right and left atrial macroreentrant tachycardias - card electrophysiol clin 2014
TRANSCRIPT

Right and Left AtrialMacroreentrant
Tachycardias Shih-Lin Chang, MD, PhD, Shih-Ann Chen, MD*KEYWORDS
� ECG � Macroreentrant tachycardias � Atrial flutter � Circuit � Mapping � Algorithm
KEY POINTS
� A 12-lead electrocardiogram (ECG) during tachycardia provides important information in the initialstrategy for the physician or specialized cardiologist.
� Catheter ablation of the cavotricuspid isthmus can eradicate typical and reverse typical atrial flutter(AFL) with a high success rate and few complications.
� For atypical AFL, catheter ablation of the isthmus between the boundaries using electroanatomicmapping can eliminate these arrhythmias.
Atrial macroreentrant tachycardia is a commontachycardia in clinical practice and its incidenceis increasing because of the aging population.1–6
It can result from structural heart disease or scar-ring from previous cardiac surgery/ablation butalso can be found in patients without obviousheart disease.2,3,7 Macroreentrant atrial tachy-cardia is characterized by an atrial tachycardiadriven by a large reentry circuit around a centralobstacle with fixed and/or functional barriers.8
Entrainment is possible in most macroreentrantatrial tachycardias. Numerous forms of macro-reentrant atrial tachycardia have been reported,and the surface electrocardiogram (ECG) patternscould correlate with the reentrant circuits. Atrialflutter (AFL) is defined by an undulating F wavein the ECG with a sawtooth appearance, whichrepresents macroreentrant atrial tachycardia insurface ECG. Therefore, the 12-lead ECG pro-vides important information for the location ofthe reentrant circuit location and mechanism.
It is crucial to understand how to determine amacroreentrant tachycardia origin based on the
The authors have nothing to disclose.Department of Medicine, Taipei Veterans General Hospi* Corresponding author.E-mail address: [email protected]
Card Electrophysiol Clin 6 (2014) 469–481http://dx.doi.org/10.1016/j.ccep.2014.05.0041877-9182/14/$ – see front matter � 2014 Elsevier Inc. All
12-lead ECG morphology of the flutter wave. Aperiod of at least 3:1 AV block during tachycardiasis suitable for flutter wave analysis. The widestflutter wave of any lead is used to define the onsetand the offset of flutter wave in all other leads.9 Theschemas of variable flutter wave morphologies on12-lead ECGs are shown in Fig. 1.
ELECTROPHYSIOLOGY STUDY AND ECGCHARACTERISTICS OF MACROREENTRANTTACHYCARDIASTypical and Reverse Typical AFL
Typical AFL is the most common type of macro-reentrant atrial tachycardia, even in patients withprior cardiac surgery/ablation.8,10 The cavotricus-pid isthmus (CTI), defined as a path bounded bythe orifice of the inferior vena cava, eustachianvalve/ridge, coronary sinus ostium, and tricuspidannulus, is a protected zone of slow conductionduring typical AFL.7 Activation mapping hasshown that the activation wave front goes down-ward in the right atrial (RA) free wall, travels
tal, 201 Section 2, Shih-Pai Road, Taipei, Taiwan
rights reserved. cardiacEP.th
eclinics.com

Fig. 1. The schemas of variable flutter wave morphol-ogies on 12-lead ECGs. The first 2 waves are monopha-sic positive (F1) and negative (F�) flutter waves. Thethird to sixth waves are biphasic flutter waves, consist-ing of dominant negative with small terminal positive(F�/f1), dominant positive with small terminal nega-tive (F1/f�), small initial negative with dominant ter-minal positive (f�/F1), and the equal amplitude ofnegative and positive waves (isoelectric). Flat polarityis amplitude less than 0.01 mV and more than�0.01 mV. (From Yuniadi Y, Tai CT, Lee KT, et al. Anew electrocardiographic algorithm to differentiateupper loop re-entry from reverse typical atrial flutter.J Am Coll Cardiol 2005;46:525; with permission.)
Chang & Chen470
through the CTI, spreads upward in the septal wall,and crosses the crista terminalis to complete thereentrant circuit (Fig. 2). Reverse slow conductionand rate-dependent conduction delay in the CTI is
Fig. 2. Activation mapping during typical AFL. Left panel shthe free wall, travels through the cavotricuspid isthmus, spterminalis. Right panel reveals the intracardiac electrogram10 to 4 are located in the free wall, and electrodes of HALarrow) activates from HAL 10 to HAL 1 with passive conducTV, tricuspid valve.
mechanistically important for the development oftypical AFL (Fig. 3). The activation sequence ofreverse typical AFL is the opposite of typical AFL.Slow conduction in the CTI may be mechanisti-
cally important for the development of typical andreverse AFL (CTI-dependent AFL). The tricuspidannulus is the anterior and fixed barrier. The cristaterminalis and eustachian ridge form the posteriorbarrier in typical AFL. Split potentials can be re-corded along the length of the crista terminalisduring pacing from the low posterior right atriumat a long cycle length in patients with clinicalAFL, suggesting that poor transverse conductionproperty in the crista terminalis may be therequisite substrate for the clinical occurrence oftypical AFL.11
Typical AFL has positive F waves in lead V1;negative F waves in lead V6; and negative F wavesin leads II, III, and aVF.8 Low-amplitude flutterwaves can be seen in leads I and aVL (Fig. 4A).Reverse typical AFL has wide, negative P wavesin lead V1; positive P waves in lead V6; and broad,positive P waves in leads II, III, and aVF (seeFig. 4B).12 However, it may present with differentECG patterns that need activation mapping todefine the exact circuit.
RA Upper Loop Reentry and Lower LoopReentry
Atypical RA flutters could arise from single-loopor double-loop figure-of-eight reentry.13,14
The activation wave front circulates around the
ows that the activation wave front goes downward inreads upward in the septal wall, and crosses the cristaduring typical AFL. Electrodes of halocatheter (HAL)3 to 1 are located in the CTI. The wave front (yellowtion in the coronary sinus (CS). IVC, inferior vena cava;

Fig. 3. (A) Incremental pacing from the low lateral right atrium (near H6 and H7) using a cycle length of 210 mil-liseconds produced gradual conduction delays and block in the isthmus (between H4 and H2) of the counterclock-wise wave front and initiated clockwise atrial flutter. (B) Incremental pacing from the coronary sinus ostium (OCS)using a cycle length of 180 milliseconds produced gradual conduction delays and block in the isthmus (betweenH1 and H2) of the clockwise wave front and initiated counterclockwise atrial flutter. HBE, recordings at the Hisbundle area; PCS, recordings at the proximal coronary sinus. (From Tai CT, Chen SA, Chiang CE, et al. Character-ization of low right atrial isthmus as the slow conduction zone and pharmacological target in typical atrial flutter.Circulation 1997;96:2606; with permission.)
Atrial Macroreentrant Tachycardias 471
central obstacle composed of a functional blockarea, and through a gap in the crista terminalis.The conduction channel between the crista termi-nalis and central obstacle and/or the crista termina-lis gaparecritical pathways formaintenanceofAFL.
Using a noncontact, three-dimensional mappingtechnique, the wave front of upper loop reentry
(ULR) had counterclockwise (CCW) activation (de-scending activation sequence in the free wall ante-rior to the crista) or clockwise (CW) activation(ascendingactivationsequence in the freewall ante-rior to the crista) around the central obstacle, whichwas composed of the crista terminalis, the area offunctional block and the superior vena cava (SVC)

Fig. 4. Surface ECG of RA macroreentrant tachycardias. Typical AFL is characterized by negative waves in inferiorleads and positive waves in V1 (A). Reverse typical AFL shows positive waves in inferior leads, negative waves inV1, and prominent positive polarity in lead I (arrow) (B). During upper loop reentry (ULR), lead I shows eithernegative flat (arrow) (C) or small positive (arrow) (D) polarity. Note the similarities of flutter waves in inferiorleads between reverse typical and ULR AFL. The surface ECG pattern of lower loop reentry (LLR) is similar tothe pattern of typical AFL with negative waves in inferior leads and positive waves in V1 (E). (From Yuniadi Y,Tai CT, Lee KT, et al. A new electrocardiographic algorithm to differentiate upper loop re-entry from reversetypical atrial flutter. J Am Coll Cardiol 2005;46:526; with permission.)
Chang & Chen472
(Fig. 5).9 During CCW ULR, there might be variableactivation of the left atrium by the wave front fromthe mid or low interatrial septum. Therefore, the po-larity of flutterwaves in lead I canbe flat, negative, orlow-amplitude positive. The surface ECGmorphology of lower loop reentry (LLR) resemblestypical AFL. The differences are characterized bydiminished amplitude of the late positive waves inthe inferior leads, which may be contributed fromwave front collision over the lateral RA wall.ULR has negative P waves in lead V1 and posi-
tive flutter waves in inferior leads, which is analo-gous to the ECG pattern of atypical AFL (seeFig. 4C and D). Negative or flat flutter wave polarityin lead I can differentiate ULR from reverse typicalAFL.9 The surface ECG pattern of LLR is similar tothe pattern of typical AFL (see Fig. 4E), except forthe shorter cycle length and the lower amplitude ofthe inferior limb leads.15
Left Atrial Macroreentrant Tachycardias
Various circuits were reported in left atrial (LA)macroreentrant tachycardias by electroanatomicmapping. The circuits commonly rotate aroundthe mitral annulus, pulmonary veins, or a scararea.2 LA muscular bundles or a scar area can pro-vide a conduction block line and barrier, which isimportant for the formation of LA flutter (Fig. 6).16
The ECGmorphology of LA macroreentrant tachy-cardia shows inhomogeneous and variable pat-terns resembling atrial tachycardia (discrete Pwaves and isoelectric baseline) or typical or atyp-ical AFL, and mostly reveals a positive flutterwave in lead V1.2,8,15,17
Mitral Annular AFL
The circuit of mitral flutter rotates around the mitralannulus, either CCW or CW. The boundaries of thecritical isthmus include themitral annulusanteriorly,and low-voltage zone or scars in the posterior wallof the LA posteriorly.2,3,16 CCW mitral annular AFLhas positive flutter waves in V1 and low amplitudein the inferior leads.15 Gerstenfeld and colleagues18
reported detailed surface ECG pattern for CW andCCWmitral annular AFL in patients after pulmonaryvein isolation. CCWmitral annular AFL has positiveflutter wave in the inferior and precordial leads, andpresents prominent negative flutter waves in leads Iand aVL. In contrast, CWmitral annular AFL revealsa negative flutter wave in the inferior leads andpositive flutter wave in leads I and aVL (Fig. 7A).
LA Septal Flutter
In LA septal flutter, the macroreentrant circuit ro-tates around the left septum primum, either CCWor CW.2,13,17 The critical isthmus is located

Fig. 5. (A) Isopotential maps showing the activation sequence (frames 1–6) of counterclockwise ULR in the rightposterior oblique view. Color scale for each isopotential map has been set so that white indicates the most nega-tive potential. The activation wave front propagates down the anterolateral RA near the SVC (frame 1) to themiddle and inferior anterolateral RA (frame 2), then splits into 2 wave fronts (frame 3); one passes around thearea of functional block, and the other passes through the cavotricuspid isthmus. The wave front in the lateralRA continues through the gap in the crista terminalis (CT) (frame 4) to the superior posterior RA (frame 5) andactivates the atrial wall surrounding the SVC before reactivation of the anterolateral RA. (B) The virtual electro-grams from the area of functional block (virtuals 11–15) and the CT (virtuals 16–20) including the conduction gap(virtuals 16–18) show double potentials. The numbers 1 to 6 represent the time points at which the isopotentialmaps are displayed in panel A. (From Tai CT, Huang JL, Lin YK, et al. Noncontact three dimensional mappingand ablation of upper loop reentry originating in the right atrium. J Am Coll Cardiol 2002;40:749; withpermission.)
Atrial Macroreentrant Tachycardias 473
between the septum primum and the pulmonaryveins or between the septum primum and themitral annulus ring. LA septal AFL reveals promi-nent, large, positive waves in V1 with almost flat
waves in other leads, suggesting that thismorphology could be the result of a septal circuitwith anterior-posterior forces projecting on V1and cancellation of caudocranial forces.

Fig. 6. LA macroreentrant tachycardia with double circuits. (A, B) The typical activation pattern during sinusrhythm in the LA. The wave fronts propagate around the gray zone, where isochrone lines are crowded togetherand double potentials were recorded during sinus rhythm in the anteroposterior and left posteromedial view,respectively. (C, D) Activation of a figure-of-eight LA flutter with a cycle length of 199 milliseconds. Arrows indi-cate circuit loop(s). The brown lesion indicates the pulse of circumferential ablation. One loop rotates around themitral annulus and the other rotates around the left pulmonary veins with a common channel conductedthrough the mitral isthmus. The reentrant circuits of atrial flutter were bordered anteriorly and posteriorly bylines of conduction block (gray zone), which were in similar locations during sinus rhythm (A, B). (D) The localbipolar electrograms along the circuit of double-loop reentry. Recording positions are shown in the isochronesmap. During LA flutter, clockwise atrial activation around the mitral annulus was manifested by atrial electro-grams in the middle posterior wall (site 1), lower posterior wall (site 8), medial mitral isthmus (site 9), and loweranterior wall (site 10), followed by activation in the lateral mitral isthmus (sites 5, 11, and 7). A slow conductionzone with fractionated electrograms was recorded at site 5. Another counterclockwise atrial activation aroundthe left pulmonary vein was manifested by atrial electrograms in the middle posterior wall (site 1), upper poste-rior wall (site 2), roof (site 3), and upper anterior wall (site 4), followed by activation in the lateral mitral isthmus(sites 5, 6, and 7). Labeled anatomic locations include the mitral valve (MV), right superior pulmonary vein (RSPV),right inferior pulmonary vein (RIPV), left superior pulmonary vein (LSPV), left inferior pulmonary vein (LIPV).(From Chang SL, Tai CT, Lin YJ, et al. The role of left atrial muscular bundles in catheter ablation of atrial fibril-lation. J Am Coll Cardiol 2007;50:967; with permission.)
Chang & Chen474
CCW septal flutter shows a prominent positiveflutter wave in lead V1 and flat flutter or low-amplitude positive wave in the limb leads (seeFig. 7B). CW septal flutter has a prominentnegative deflection in lead V1 and flat flutter orlow-amplitude positive F wave in limb leads.17
Other LA Flutters
Macroreentrant circuits can rotate around one ormore pulmonary veins and a scar in the posteriorwall or roof of LA.2,3 These circuits may have
multiple loops (see Fig. 6). In LA posterior flutter,the circuit rotates around low-voltage or scarredareas on the LA posterior wall.17
The ECG pattern of pulmonary vein flutter ischaracterized by a positive wave in V1 with posi-tive wave in lead I and isoelectric wave in aVL forright pulmonary vein flutter; and an isoelectric Pwave in lead I and negative wave in aVL for left pul-monary vein flutter (see Fig. 7C). LA posterior wallAFL is less commonly seen, and its ECGmorphology resembles typical AFL with dimin-ished amplitude in the inferior leads.15
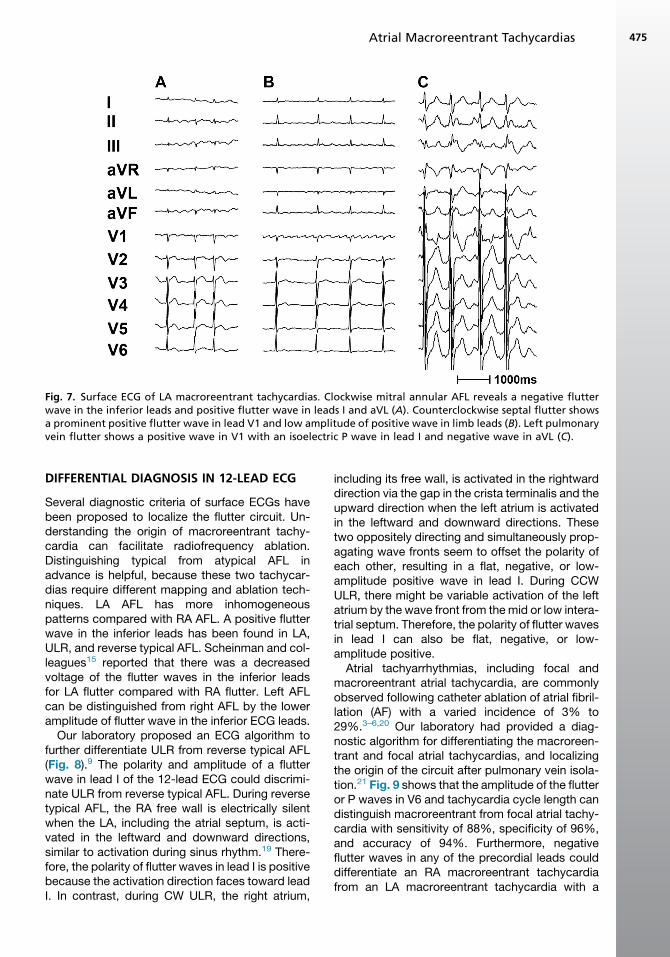
Fig. 7. Surface ECG of LA macroreentrant tachycardias. Clockwise mitral annular AFL reveals a negative flutterwave in the inferior leads and positive flutter wave in leads I and aVL (A). Counterclockwise septal flutter showsa prominent positive flutter wave in lead V1 and low amplitude of positive wave in limb leads (B). Left pulmonaryvein flutter shows a positive wave in V1 with an isoelectric P wave in lead I and negative wave in aVL (C).
Atrial Macroreentrant Tachycardias 475
DIFFERENTIAL DIAGNOSIS IN 12-LEAD ECG
Several diagnostic criteria of surface ECGs havebeen proposed to localize the flutter circuit. Un-derstanding the origin of macroreentrant tachy-cardia can facilitate radiofrequency ablation.Distinguishing typical from atypical AFL inadvance is helpful, because these two tachycar-dias require different mapping and ablation tech-niques. LA AFL has more inhomogeneouspatterns compared with RA AFL. A positive flutterwave in the inferior leads has been found in LA,ULR, and reverse typical AFL. Scheinman and col-leagues15 reported that there was a decreasedvoltage of the flutter waves in the inferior leadsfor LA flutter compared with RA flutter. Left AFLcan be distinguished from right AFL by the loweramplitude of flutter wave in the inferior ECG leads.
Our laboratory proposed an ECG algorithm tofurther differentiate ULR from reverse typical AFL(Fig. 8).9 The polarity and amplitude of a flutterwave in lead I of the 12-lead ECG could discrimi-nate ULR from reverse typical AFL. During reversetypical AFL, the RA free wall is electrically silentwhen the LA, including the atrial septum, is acti-vated in the leftward and downward directions,similar to activation during sinus rhythm.19 There-fore, the polarity of flutter waves in lead I is positivebecause the activation direction faces toward leadI. In contrast, during CW ULR, the right atrium,
including its free wall, is activated in the rightwarddirection via the gap in the crista terminalis and theupward direction when the left atrium is activatedin the leftward and downward directions. Thesetwo oppositely directing and simultaneously prop-agating wave fronts seem to offset the polarity ofeach other, resulting in a flat, negative, or low-amplitude positive wave in lead I. During CCWULR, there might be variable activation of the leftatrium by the wave front from themid or low intera-trial septum. Therefore, the polarity of flutter wavesin lead I can also be flat, negative, or low-amplitude positive.
Atrial tachyarrhythmias, including focal andmacroreentrant atrial tachycardia, are commonlyobserved following catheter ablation of atrial fibril-lation (AF) with a varied incidence of 3% to29%.3–6,20 Our laboratory had provided a diag-nostic algorithm for differentiating the macroreen-trant and focal atrial tachycardias, and localizingthe origin of the circuit after pulmonary vein isola-tion.21 Fig. 9 shows that the amplitude of the flutteror P waves in V6 and tachycardia cycle length candistinguish macroreentrant from focal atrial tachy-cardia with sensitivity of 88%, specificity of 96%,and accuracy of 94%. Furthermore, negativeflutter waves in any of the precordial leads coulddifferentiate an RA macroreentrant tachycardiafrom an LA macroreentrant tachycardia with a

Fig. 8. Diagnostic algorithm to differ-entiate between ULR and reversetypical atrial flutter (RTAFL). Flat po-larity is defined as polarity of lessthan 0.01 mV but more than�0.01 mV. Isoelectric is defined asbiphasic polarity in which negativeand positive deflection have equalamplitude. (From Yuniadi Y, Tai CT,Lee KT, et al. A new electrocardio-graphic algorithm to differentiateupper loop re-entry from reversetypical atrial flutter. J Am Coll Cardiol2005;46:527; with permission.)
Chang & Chen476
sensitivity and specificity of 83% and 100%(Fig. 10), respectively, and an accuracy of 98%.Opposite polarity of flutter wave could befound clinically in V1 and V6 in cavotricuspidisthmus–dependent AFL. Precordial negativitymay represent an RA origin. Regarding the LAmacroreentrant tachycardia, most macroreentrantatrial tachycardias were terminated during theablation of the mitral isthmus and roof.3,21 Promi-nent positive flutter waves in V1 were morecommonly seen in roof/mitral isthmus–dependentthan non–roof/mitral isthmus–dependent macro-reentrant atrial tachycardias, suggesting that V1is useful for differentiation (Figs. 11 and 12). Thesensitivity and specificity were 80% and 83%,
Fig. 9. A new diagnostic algorithm for differentiating mwave is defined as a polarity of the flutter or P wave ofto �0.05 mV. Numbers indicates numbers of patients withage indicates the percentage of patients with accurate preand colleagues.21 CL, cycle length. (From Chang SL, Tsao Hfocal atrial tachycardias occurred after circumferential p2011;22:753; with permission.)
respectively, with an accuracy of 81%.21 Gersten-feld and colleagues18 showed that mitral annularAFL following pulmonary vein isolation had a pos-itive P wave in V1 with a small initial negative depo-larization in the other precordial leads. Positiveflutter waves in leads I and aVL can differentiateCW mitral AFL from CCW RA flutter and left pul-monary vein atrial tachycardia after AF ablation.
MANAGEMENT
Three methods of treatment can be used toconvert AFL to sinus rhythm: antiarrhythmic drugs,electrical cardioversion, or catheter ablation.Catheter ablation has a higher success rate in
acroreentrant and focal atrial tachycardia (AT). A flatless than or equal to 0.05 and greater than or equalaccurate prediction/total number of patients; percent-diction/total number of patients in the study by ChangM, Lin YJ, et al. Differentiating macroreentrant fromulmonary vein isolation. J Cardiovasc Electrophysiol

Fig. 10. Diagnostic algorithm for differentiating RAand LA macroreentrant AT. Number indicates numberof patients with accurate prediction/total number ofpatients; percentage indicates the percentage ofpatients with accurate prediction/total number of pa-tients in the study by Chang and colleagues.21 (FromChang SL, Tsao HM, Lin YJ, et al. Differentiatingmacroreentrant from focal atrial tachycardiasoccurred after circumferential pulmonary vein isola-tion. J Cardiovasc Electrophysiol 2011;22:753; withpermission.)
Atrial Macroreentrant Tachycardias 477
elimination of AFL and maintenance of sinusrhythm.2,3,6,8 The CTI is the target for radiofre-quency ablation of typical and reverse typicalAFL, in which it is easiest to obtain complete bidi-rectional isthmus block via a venous approach.However, atypical AFL could arise from the RA orLA. Electroanatomic mapping and transseptalapproach are sometimes needed. Radiofrequencyablation of the isthmus between the boundariescan eliminate these arrhythmias. It is more timeconsuming and difficult to eliminate atypical AFLcompared with typical AFL. Therefore, it is impor-tant to identify the origin of reentrant tachycardias
Fig. 11. A new diagnostic algorithm for differentiatingdependent macroreentrant AT. Number indicates numberpatients; percentage indicates the percentage of patientsthe study by Chang and colleagues.21 (From Chang SL, Tfrom focal atrial tachycardias occurred after circumferentia2011;22:754; with permission.)
using 12-lead ECG in management of AFL. Recog-nizing the location of macroreentrant tachycardiafrom the 12-lead ECG is useful for (1) determiningan initial treatment (pharmacologic or ablationtherapy), (2) facilitating mapping and navigatingablation, and (3) monitoring and understandingthe possible mechanism of recurrence from priorcatheter ablation of tachyarrhythmias.
INTERVENTION OUTCOME
The acute and long-term outcomes of macroreen-trant atrial tachycardia are shown in Table 1. Ra-diofrequency ablation of the CTI can eliminatetypical and reverse AFL with low recurrence andcomplication rates.22–24 However, AF continuesto be a long-term risk for patients undergoing thisprocedure, with incidence of 20% to 50%.22,25
The presence of structural heart disease and priorspontaneous or inducible sustained AF increasesthe risk of developing AF. For atypical RA AFL, ra-diofrequency ablation of the free-wall channel and/or the crista terminalis gap is effective in elimi-nating these macroreentrant tachycardias.14
Regarding LA macroreentrant tachycardia, theprotected isthmus between 2 anatomic barriersis amenable to radiofrequency ablation. Identifyingthe conduction block line and further creatingadditional line(s) crossing the isthmus of thereentry barrier may contribute to a better clinicaloutcome.2,20,26
With increasingly aggressive treatments of AF,postablation macroreentrant atrial tachycardiasare expected to increase in number andcomplexity in daily clinical practice. Detailed
roof/mitral isthmus (R/M)–dependent from non–R/M-of patients with accurate prediction/total number ofwith accurate prediction/total number of patients in
sao HM, Lin YJ, et al. Differentiating macroreentrantl pulmonary vein isolation. J Cardiovasc Electrophysiol

Fig. 12. Three-dimensional activationmap and surface ECG of macroreentrant atrial tachycardias. The white arrowindicates the activation circuit, and red arrowhead the P or flutter wave of the macroreentrant atrial tachycardias.(A) A mitral macroreentrant atrial tachycardia (CL, 225 milliseconds) rotating clockwise around the mitral annulus.The surface ECG of the tachycardia shows positive flutter waves in V1 and V6. The amplitude of the flutter wavesin V6 is 0.5 mV. (B) A left pulmonary vein (LPV) macroreentrant atrial tachycardia rotating around the LPV with aCL of 205 milliseconds. The surface ECG of the tachycardia shows positive flutter waves in V1 and V6. The ampli-tude of the flutter waves in V6 is 0.6 mV. (C) A double macroreentrant atrial tachycardia rotating around the LPVand mitral annulus with a CL of 236 milliseconds. The surface ECG of the tachycardia shows positive flutter wavesin V1 and flat waves in V6. (D) A right pulmonary vein (RPV) macroreentrant atrial tachycardia rotating around theRPV with a CL of 199 milliseconds. The surface ECG of the tachycardia shows positive flutter waves in V1 and V6.The amplitude of the flutter waves in V6 is 0.1 mV. (E) A double macroreentrant atrial tachycardia rotating aroundthe LPV and LA appendage (LAA) with a CL of 237 milliseconds. The surface ECG of the AT shows flat flutter wavesin V1 and positive waves in V6. The amplitude of the flutter waves in V6 is 0.25 mV. LVZ, low-voltage zone. (FromChang SL, Tsao HM, Lin YJ, et al. Differentiating macroreentrant from focal atrial tachycardias occurred aftercircumferential pulmonary vein isolation. J Cardiovasc Electrophysiol 2011;22:751; with permission.)
Chang & Chen478
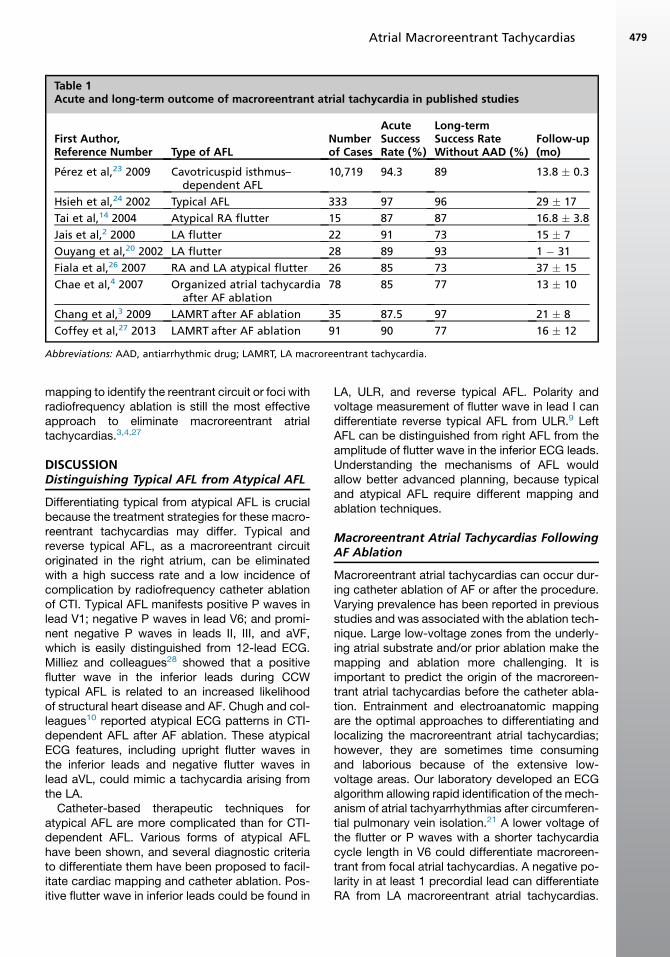
Table 1Acute and long-term outcome of macroreentrant atrial tachycardia in published studies
First Author,Reference Number Type of AFL
Numberof Cases
AcuteSuccessRate (%)
Long-termSuccess RateWithout AAD (%)
Follow-up(mo)
Perez et al,23 2009 Cavotricuspid isthmus–dependent AFL
10,719 94.3 89 13.8 � 0.3
Hsieh et al,24 2002 Typical AFL 333 97 96 29 � 17
Tai et al,14 2004 Atypical RA flutter 15 87 87 16.8 � 3.8
Jais et al,2 2000 LA flutter 22 91 73 15 � 7
Ouyang et al,20 2002 LA flutter 28 89 93 1 � 31
Fiala et al,26 2007 RA and LA atypical flutter 26 85 73 37 � 15
Chae et al,4 2007 Organized atrial tachycardiaafter AF ablation
78 85 77 13 � 10
Chang et al,3 2009 LAMRT after AF ablation 35 87.5 97 21 � 8
Coffey et al,27 2013 LAMRT after AF ablation 91 90 77 16 � 12
Abbreviations: AAD, antiarrhythmic drug; LAMRT, LA macroreentrant tachycardia.
Atrial Macroreentrant Tachycardias 479
mapping to identify the reentrant circuit or foci withradiofrequency ablation is still the most effectiveapproach to eliminate macroreentrant atrialtachycardias.3,4,27
DISCUSSIONDistinguishing Typical AFL from Atypical AFL
Differentiating typical from atypical AFL is crucialbecause the treatment strategies for these macro-reentrant tachycardias may differ. Typical andreverse typical AFL, as a macroreentrant circuitoriginated in the right atrium, can be eliminatedwith a high success rate and a low incidence ofcomplication by radiofrequency catheter ablationof CTI. Typical AFL manifests positive P waves inlead V1; negative P waves in lead V6; and promi-nent negative P waves in leads II, III, and aVF,which is easily distinguished from 12-lead ECG.Milliez and colleagues28 showed that a positiveflutter wave in the inferior leads during CCWtypical AFL is related to an increased likelihoodof structural heart disease and AF. Chugh and col-leagues10 reported atypical ECG patterns in CTI-dependent AFL after AF ablation. These atypicalECG features, including upright flutter waves inthe inferior leads and negative flutter waves inlead aVL, could mimic a tachycardia arising fromthe LA.
Catheter-based therapeutic techniques foratypical AFL are more complicated than for CTI-dependent AFL. Various forms of atypical AFLhave been shown, and several diagnostic criteriato differentiate them have been proposed to facil-itate cardiac mapping and catheter ablation. Pos-itive flutter wave in inferior leads could be found in
LA, ULR, and reverse typical AFL. Polarity andvoltage measurement of flutter wave in lead I candifferentiate reverse typical AFL from ULR.9 LeftAFL can be distinguished from right AFL from theamplitude of flutter wave in the inferior ECG leads.Understanding the mechanisms of AFL wouldallow better advanced planning, because typicaland atypical AFL require different mapping andablation techniques.
Macroreentrant Atrial Tachycardias FollowingAF Ablation
Macroreentrant atrial tachycardias can occur dur-ing catheter ablation of AF or after the procedure.Varying prevalence has been reported in previousstudies and was associated with the ablation tech-nique. Large low-voltage zones from the underly-ing atrial substrate and/or prior ablation make themapping and ablation more challenging. It isimportant to predict the origin of the macroreen-trant atrial tachycardias before the catheter abla-tion. Entrainment and electroanatomic mappingare the optimal approaches to differentiating andlocalizing the macroreentrant atrial tachycardias;however, they are sometimes time consumingand laborious because of the extensive low-voltage areas. Our laboratory developed an ECGalgorithm allowing rapid identification of the mech-anism of atrial tachyarrhythmias after circumferen-tial pulmonary vein isolation.21 A lower voltage ofthe flutter or P waves with a shorter tachycardiacycle length in V6 could differentiate macroreen-trant from focal atrial tachycardias. A negative po-larity in at least 1 precordial lead can differentiateRA from LA macroreentrant atrial tachycardias.

Chang & Chen480
This novel algorithm can accurately diagnose themechanism and origin of atrial tachyarrhythmiasafter pulmonary vein isolation. To facilitate themapping and ablation, simple and accurate algo-rithms using the surface ECG are always welcome.
SUMMARY
With improved mapping techniques and moreaggressive treatment in management of macro-reentrant atrial tachycardias, a 12-lead ECG dur-ing tachycardia provides important information inthe initial strategy for the physician or specializedcardiologist. Catheter ablation of CTI can eradi-cate typical and reverse typical AFL with a highsuccess rate and few complications. For atypicalAFL, catheter ablation of the isthmus betweenthe boundaries using electroanatomic mappingcan eliminate these arrhythmias.
REFERENCES
1. Granada J, Uribe W, Chyou PH, et al. Incidence and
predictors of atrial flutter in the general population.
J Am Coll Cardiol 2000;36:2242–6.
2. Jais P, Shah DC, Haissaguerre M, et al. Mapping
and ablation of left atrial flutters. Circulation 2000;
101:2928–34.
3. Chang SL, Lin YJ, Tai CT, et al. Induced atrial tachy-
cardia after circumferential pulmonary vein isolation
of paroxysmal atrial fibrillation: electrophysiological
characteristics and impact of catheter ablation on
the follow-up results. J Cardiovasc Electrophysiol
2009;20:388–94.
4. Chae S, Oral H, Good E, et al. Atrial tachycardia af-
ter circumferential pulmonary vein ablation of atrial
fibrillation: mechanistic insights, results of catheter
ablation, and risk factors for recurrence. J Am Coll
Cardiol 2007;50:1781–7.
5. Gerstenfeld EP, Callans DJ, Dixit S, et al. Mecha-
nisms of organized left atrial tachycardias occurring
after pulmonary vein isolation. Circulation 2004;110:
1351–7.
6. Gerstenfeld EP, Callans DJ, Sauer W, et al. Reen-
trant and nonreentrant focal left atrial tachycardias
occur after pulmonary vein isolation. Heart Rhythm
2005;2:1195–202.
7. Tai CT, Chen SA, Chiang CE, et al. Characterization
of low right atrial isthmus as the slow conduction
zone and pharmacological target in typical atrial
flutter. Circulation 1997;96:2601–11.
8. Saoudi N, Cosio F, Waldo A, et al. Classification of
atrial flutter and regular atrial tachycardia according
to electrophysiologic mechanism and anatomic ba-
ses: a statement from a joint expert group from the
Working Group of Arrhythmias of the European Soci-
ety of Cardiology and the North American Society of
Pacing and Electrophysiology. J Cardiovasc Electro-
physiol 2001;12:852–66.
9. Yuniadi Y, Tai CT, Lee KT, et al. A new electrocardio-
graphic algorithm to differentiate upper loop re-entry
from reverse typical atrial flutter. J Am Coll Cardiol
2005;46:524–8.
10. Chugh A, Latchamsetty R, Oral H, et al. Characteris-
tics of cavotricuspid isthmus-dependent atrial flutter
after left atrial ablation of atrial fibrillation. Circulation
2006;113:609–15.
11. Tai CT, Chen SA, Chen YJ, et al. Conduction prop-
erties of the crista terminalis in patients with typical
atrial flutter: basis for a line of block in the reen-
trant circuit. J Cardiovasc Electrophysiol 1998;9:
811–9.
12. Tai CT, Chen SA, Chiang CE, et al. Electrophysio-
logic characteristics and radiofrequency catheter
ablation in patients with clockwise atrial flutter.
J Cardiovasc Electrophysiol 1997;8:24–34.
13. Tai CT, Lin YK, Chen SA. Atypical atrial flutter
involving the isthmus between the right pulmonary
veins and fossa ovalis. Pacing Clin Electrophysiol
2001;24:384–7.
14. Tai CT, Liu TY, Lee PC, et al. Non-contact mapping to
guide radiofrequency ablation of atypical right atrial
flutter. J Am Coll Cardiol 2004;44:1080–6.
15. Bochoeyer A, Yang Y, Cheng J, et al. Surface elec-
trocardiographic characteristics of right and left
atrial flutter. Circulation 2003;108:60–6.
16. Chang SL, Tai CT, Lin YJ, et al. The role of left atrial
muscular bundles in catheter ablation of atrial fibril-
lation. J Am Coll Cardiol 2007;50:964–73.
17. Marrouche NF, Natale A, Wazni OM, et al. Left septal
atrial flutter: electrophysiology, anatomy, and results
of ablation. Circulation 2004;109:2440–7.
18. Gerstenfeld EP, Dixit S, Bala R, et al. Surface electro-
cardiogram characteristics of atrial tachycardias
occurring after pulmonary vein isolation. Heart
Rhythm 2007;4:1136–43.
19. Ndrepepa G, Zrenner B, Weyerbrock S, et al. Activa-
tion patterns in the left atrium during counterclock-
wise and clockwise atrial flutter. J Cardiovasc
Electrophysiol 2001;12:893–9.
20. Ouyang F, Ernst S, Vogtmann T, et al. Characteriza-
tion of reentrant circuits in left atrial macroreentrant
tachycardia: critical isthmus block can prevent
atrial tachycardia recurrence. Circulation 2002;
105:1934–42.
21. Chang SL, Tsao HM, Lin YJ, et al. Differentiating
macroreentrant from focal atrial tachycardias
occurred after circumferential pulmonary vein isola-
tion. J Cardiovasc Electrophysiol 2011;22:748–55.
22. Tai CT, Chen SA, Chiang CE, et al. Long-term
outcome of radiofrequency catheter ablation for
typical atrial flutter: risk prediction of recurrent ar-
rhythmias. J Cardiovasc Electrophysiol 1998;9:
115–21.

Atrial Macroreentrant Tachycardias 481
23. Perez FJ, Schubert CM, Parvez B, et al. Long-term
outcomes after catheter ablation of cavo-tricuspid
isthmus dependent atrial flutter: a meta-analysis.
Circ Arrhythm Electrophysiol 2009;2:393–401.
24. Hsieh MH, Tai CT, Chiang CE, et al. Recurrent atrial
flutter and atrial fibrillation after catheter ablation of
the cavotricuspid isthmus: a very long-term follow-
up of 333 patients. J Interv Card Electrophysiol
2002;7:225–31.
25. Mittal S, Pokushalov E, Romanov A, et al. Long-term
ECG monitoring using an implantable loop recorder
for the detection of atrial fibrillation after cavotricus-
pid isthmus ablation in patients with atrial flutter.
Heart Rhythm 2013;10:1598–604.
26. Fiala M, Chovancik J, Neuwirth R, et al. Atrial macro-
reentry tachycardia in patients without obvious
structural heart disease or previous cardiac surgical
or catheter intervention: characterization of arrhyth-
mogenic substrates, reentry circuits, and results of
catheter ablation. J Cardiovasc Electrophysiol
2007;18:824–32.
27. Coffey JO, d’Avila A, Dukkipati S, et al. Catheter
ablation of scar-related atypical atrial flutter. Euro-
pace 2013;15:414–9.
28. Milliez P, Richardson AW, Obioha-Ngwu O, et al.
Variable electrocardiographic characteristics of
isthmus-dependent atrial flutter. J Am Coll Cardiol
2002;40:1125–32.