rifampicin–fosfomycin coating for cementless endoprostheses: antimicrobial effects against...
TRANSCRIPT
Acta Biomaterialia 10 (2014) 4518–4524
Contents lists available at ScienceDirect
Acta Biomaterialia
journal homepage: www.elsevier .com/locate /ac tabiomat
Rifampicin–fosfomycin coating for cementless endoprostheses:Antimicrobial effects against methicillin-sensitive Staphylococcus aureus(MSSA) and methicillin-resistant Staphylococcus aureus (MRSA)
http://dx.doi.org/10.1016/j.actbio.2014.06.0131742-7061/� 2014 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
⇑ Corresponding author at: Department of Trauma Surgery Giessen, UniversityHospital of Giessen-Marburg, Campus Giessen, 35385 Giessen, Germany.
E-mail address: [email protected] (V. Alt).
Volker Alt a,b,⇑, Kristin Kirchhof c, Florian Seim a,b, Isabelle Hrubesch a,b, Katrin S. Lips b, Henrich Mannel c,Eugen Domann d, Reinhard Schnettler a,b
a Department of Trauma Surgery Giessen, University Hospital of Giessen-Marburg, Campus Giessen, 35385 Giessen, Germanyb Laboratory of Experimental Trauma Surgery Giessen, Justus-Liebig-University Giessen, 35394 Giessen, Germanyc Biomet Deutschland GmbH, 14167 Berlin, Germanyd Institute of Medical Microbiology, University Hospital of Giessen-Marburg, Campus Giessen, 35392 Giessen, Germany
a r t i c l e i n f o a b s t r a c t
Article history:Received 17 February 2014Received in revised form 7 May 2014Accepted 9 June 2014Available online 16 June 2014
Keywords:InfectionProsthesisStaphylococcus aureusMRSA
New strategies to decrease infection rates in cementless arthroplasty are needed, especially in the contextof the growing incidence of methicillin-resistant Staphylococcus aureus (MRSA) infections. The purpose ofthis study was to investigate the antimicrobial activity of a rifampicin–fosfomycin coating against meth-icillin-sensitive Staphylococcus aureus (MSSA) and MRSA in a rabbit infection prophylaxis model.Uncoated or rifampicin–fosfomycin-coated K-wires were inserted into the intramedullary canal of thetibia in rabbits and contaminated with an inoculation dose of 105 or 106 colony-forming units of MSSAEDCC 5055 in study 1 and MRSA T6625930 in study 2, respectively. After 28 days the animals were killedand clinical, histological and microbiological assessment, including pulse-field gel electrophoresis, wasconducted. Positive culture growth in agar plate testing and/or clinical signs and/or histological signswere defined positive for infection. Statistical evaluation was performed using Fisher’s exact test. Bothstudies showed a statistically significant reduction of infection rates for rifampicin–fosfomycin-coatedimplants compared to uncoated K-wires (P = 0.015). In both studies none of the 12 animals that weretreated with a rifampicin–fosfomycin-coated implant showed clinical signs of infection or a positive agarplate testing result. In both studies, one animal of the coating group showed the presence of sporadic bac-teria with concomitant inflammatory signs in histology. The control groups in both studies exhibited aninfection rate of 100% with clear clinical signs of infection and positive culture growth in all animals. Insummary, the rifampicin–fosfomycin-coating showed excellent antimicrobial activity against both MSSAand MRSA, and therefore warrants further clinical testing.
� 2014 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Infections in total arthroplasty such as total knee and total hiparthroplasty are devastating situations with a negative impact bothon the quality of life for the patient and on the cost to the health-care system [1]. Frequently, surgical treatment to exchange theinfected prosthesis is the only option for treatment of the infection.However, failure rates with reinfection or persistence of the infec-tion of this extensive surgical treatment of �20% have beenreported [2].
The virulence of methicillin-resistant Staphylococcus aureus(MRSA) has turned this pathogen not only into the most deadlybacteria in North America [3] but also into a complex problem inthe context of total joint infections. Previous reports have shownthat the treatment outcome for patients with infections with mul-tiresistant bacteria such as MRSA is significantly worse comparedto infections with non-multiresistant bacteria with higher recur-rence of infection of up to 61%, resulting in resection arthroplastyor even amputation [4,5]. Therefore, all efforts should be under-taken to optimize infection prophylaxis in total joint arthroplasty,including prophylaxis against MRSA.
The principle of local delivery of antibiotics by antibiotic-loaded bone cement was introduced by Buchholz and Engelbrecht[6] and was intended to optimize infection prophylaxis by highconcentrations of the antibiotic in direct vicinity to the implant

V. Alt et al. / Acta Biomaterialia 10 (2014) 4518–4524 4519
and in the adjacent tissue, while at the same time minimizingsystemic concentrations and systemic side effects. Clinical datafrom the Norwegian Arthroplasty Register show a significantreduction of infection rates in primary cemented hip arthroplasty[7] when comparing systemic antibiotics plus antibiotic-loadedbone cement to systemic antibiotics plus antibiotic-free bonecement.
In cementless arthroplasty, which is performed without bonecement, the local delivery of antibiotics is currently not possible.Coating the surface of cementless implants with antibiotics orother anti-infective agents is an interesting and promising optionfor this complex problem.
Alt and co-workers were the first to reveal the successful in vivoantimicrobial activity of an antibiotic coating for cementlessprostheses coated with combined gentamicin–hydroxyapatitelayers [8]. Since then, several articles have been published on thein vivo results of a number of other coatings for cementless jointimplants such as tobramycin–periapatite [9], vancomycin [10],minocycline–rifampicin [11,12], teicoplanin–clindamycin [13]and various silver coatings [14,15] or cationic steroidal antimicro-bial coating [16].
New developments for coating of orthopaedic implants shouldtarget solutions that cover the most relevant bacteria strains forimplant-associated infections such as Staphylococci includingMRSA and gram-negative strains, e.g. Pseudomonas aeruginosaand Escherichia coli. Rifampicin is a bactericidal antibiotic thatfulfils this requirement by inhibiting bacterial RNA polymerasewith both extracellular and intracellular activity which is superiorcompared to vancomycin and teicoplanin [17]. One of the draw-backs of rifampicin use is the fast development of resistance in caseof monotherapy, and therefore it should only be used with a sec-ond antibiotic agent [18]. Fosfomycin can act as ‘‘second antibioticagent’’ in combination with rifampicin as it has been shown toexhibit excellent antibiotic activity against gram-negative andgram-positive strains including MRSA [19,20]. The synergisticeffects of rifampicin and fosfomycin have been reported forsystemic use [21], and this systemic combination was recentlyfound to be highly effective in an in vivo subcutaneous implant-associated foreign body infection model [22].
The aim of this work is to investigate the in vivo antimicrobialeffects of rifampicin–fosfomycin-coated titanium K-wires in animplant-associated bone infection prophylaxis model againstmethicillin-sensitive Staphylococcus aureus (MSSA) and MRSA.
2. Materials and methods
Two studies for antimicrobial testing of rifampicin–fosfomycin-coated K-wires were undertaken, using an MSSA in the first and anMRSA in the second study. All experiments were approved beforesurgery by the local animal committee (RP Thüringen, Erfurt,Germany, Registration No. 14-002/07).
2.1. Study design
2.1.1. Study 1: MSSAStudy 1 included 12 3 month old New Zealand White Rabbits.
Inoculation doses of 105 or 106 colony-forming units (CFUs) ofMSSA EDCC 5055 were used for this study. Six animals receiveda rifampicin–fosfomycin-coated K-wire. Three of these were inoc-ulated with 105 and the remaining three rabbits with 106 CFUs.In the control group, in which the uncoated K-wire was inserted,three animals received an inoculation dose of 105 and three of106 CFUs. One animal of the control group with an inoculation doseof 105 CFUs was precluded from the study because of anatomicaldeformity of the lower limb.
2.1.2. Study 2: MRSAA similar study design was chosen for study 2. Inoculation doses
of 105 or 106 CFUs of MRSA T6625930 were used to contaminatethe intramedullary canal of the tibia. In six animals a rifampicin–fosfomycin-coated K-wire was implanted. Three of these rabbitswere inoculated with 105 and three with 106 CFUs. In the controlgroup, in which the uncoated K-wire was used, three animals wereinoculated with 105 and three with 106 CFUs. In the control groupone animal with an inoculation dose of 105 CFUs died duringsurgery due to anesthesia complications.
2.2. Bacteria
2.2.1. Bacterial strainsMSSA EDCC 5055 strain was used in a previous study for testing
the antimicrobial effect of different gentamicin coatings forcementless endoprostheses in the same animal model [8]. MSSAEDCC 5055 is a clinical isolate from a patient with a wound infec-tion. The isolate was identified by API biochemical characteristictesting (bioMerieux, Marcy L’Etoile, France), by sequencing the16S rDNA gene, and by specific polymerase chain reactions (PCRs)to detect the femB and coa genes. This strain exhibited stronghemolytic activity and very strong biofilm formation capacity aspublished before [23] based on the technology of O’Toole et al.[24].
The MRSA T6625930 is a clinical isolate from a patient with aperiprosthetic hip joint infection. It also shows in vitro biofilm for-mation. The strain was identified by sequencing the 16S rDNAgene, and by specific PCRs to detect the femB and mecA genes.
To determine the minimal inhibitory concentration (MIC), bac-terial colonies were picked out from blood–agar plates, mixed in atube containing sterile saline and diluted to obtain a turbidityequivalent to the 0.5 McFarland test standard. Using a sterile swab,bacteria were streaked on Mueller–Hinton agar plates. MIC evalu-ator strips™ (OXOID, Wesel, Germany) were aseptically applied tothe agar plates, which were further incubated overnight at 37 �C.MICs were read the following day. The MIC of MSSA EDCC 5055against rifampicin was found to be 6 0.5 lg ml�1 and against fosfo-mycin 6 16 lg ml�1; the MIC of MRSA T6625930 against rifampi-cin was 6 0.5 lg ml�1 and against fosfomycin 6 8 lg ml�1.
2.2.2. Bacteria cultivationAll bacteria were grown in brain heart infusion broth (BHI) at
37 �C under vigorous shaking for 16 h. The culture was diluted1:50 in BHI and further incubated as described above for 4 h. Theculture was diluted 1:10 in phosphate-buffered salie (PBS) and pla-ted on BHI agar plates using a spiral plater for the enumeration of S.aureus in CFUs ml�1. Several suspensions with a final volume of160 ll for inoculations with the required concentrations of 105 or106 CFUs per 20 ll in BHI/20% glycerol were generated and storedat �80 �C until use. Each inoculation volume for the infection trialwas 20 ll, equivalent to 105 or 106 CFUs.
2.3. Implants
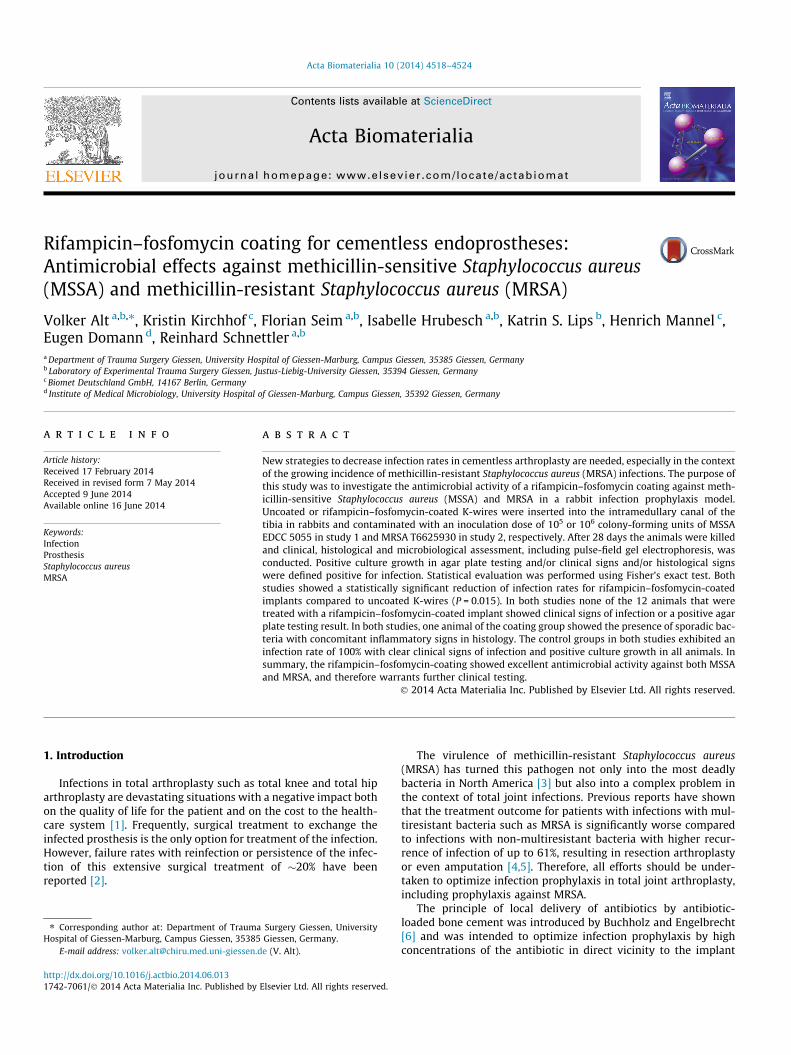
c-sterilized titanium alloy Ti6Al4 V K-wires with a diameter of2.0 mm that were either uncoated or coated with rifampicin–fosfo-mycin were used for the study (Fig. 1). All implants were providedby Biomet Deutschland GmbH (Berlin, Germany). The implants hada total length of 12 cm of which 10 cm were coated. The coatingwas applied via an ink-jet technology in analogy to a gentamicincoating as published before [8]. The concentrations of rifampicinand fosfomycin were 50 and 250 lg cm�2, respectively, with a totalamount of 307 lg rifampicin and 1522 lg fosfomycin per implant.
Fig. 1. Rifampicin–fosfomycin-coated K-wire (top) and uncoated titanium K-wire(bottom (a). Scanning electron microscope image of a rifampicin–fosfomycin-coated Ti6Al4V alloy disc sample (K-wire and disc have the identical grit blastedsurface finishing); 10,000-fold magnification, scale bar 1 lm (b).
Fig. 2. Postoperative X-ray of implanted rifampicin–fosfomycin-coated K-wire.
4520 V. Alt et al. / Acta Biomaterialia 10 (2014) 4518–4524
2.4. Surgery
Anesthesia was performed using ketamine (60 mg kg�1
bodyweight), xylazine (6 mg kg�1 bodyweight) and atropine
(0.1 mg kg�1 bodyweight). Surgery was carried out under asepticconditions according to the previously published model [8]. Nosystemic antibiotics were utilized.
After disinfection of the right lower limb, the knee region wasdraped in a sterile manner. The tibial tuberosity was approachedvia a 1 cm infrapatellar incision followed by splitting of the patellartendon and opening of the distal part of the knee joint. The supe-rior cortex of the tibial tuberosity was perforated and the K-wirewas subsequently introduced into the intramedullary canal. TheK-wire was driven to the distal part of the intramedullary canaland was shortened to fit the length of the tibia. Shortening wasalways performed in the non-coated proximal 2 cm of the implant.A 16G needle was also introduced into the intramedullary tibiacanal next to the K-wire over which 20 ll of the suspension withthe number of CFUs of S. aureus according to the study protocolwere inoculated into the midshaft area of the intramedullary canal.After injection of the bacteria, 20 ll of the remaining inoculum wasstreaked out on agar plates to confirm the intended inoculationdose. The wound was closed and post-operative X-ray controlwas performed (Fig. 2).
After 4 weeks the animals were killed under general anaesthe-sia (ketamine: 60 mg kg�1 bodyweight; T61: 4–5 ml intracardial).The tibiae were then harvested under sterile conditions. TheK-wire was removed and the tibia was then sagitally cut. Thelateral and the medial half were used for microbiological andhistological evaluations, respectively.
2.5. Evaluation methods
2.5.1. Clinical assessment for infectionThe lower extremity and the adjacent knee and ankle joint were
evaluated for any clinical signs of inflammation or swelling beforeharvesting of the bone. During dissection for bone harvest the softtissue and after longitudinal section of the tibia the intramedullarycavity were assessed for pus, abscess formation and cortical lysis.
2.5.2. Microbiological assessment for infectionThe K-wires were removed carefully under sterile conditions
and rolled out on BHI agar plates. For the bone samples, the bonemarrow of one tibial half was removed and weighed. The bonemarrow tissue sample was suspended in PBS and vortexed to dis-perse potential bacteria in the sample. The suspension was subse-quently diluted (1:1, 1:10, 1:100) and 10 ll of each dilution werestreaked on BHI plates and incubated at 37 �C for 24 h. The numberof colonies was counted on each agar plate. In order to confirm theidentity of the inoculated S. aureus and the S. aureus isolates onagar plates, randomly collected colonies from agar plates weregenetically compared with the inoculated strains using PFGE andthe CHEF-DR II system (Biorad, Munich, Germany) as describedbefore [8].
2.5.3. Histological evaluationThe medial half of the tibia was immersed in 4% paraformalde-
hyde solution for 24 h and subsequently 5 lm longitudinal sec-tions were cut using the grinding technique as previouslydescribed [8]. These sections were stained with toluidine blueand hematoxylin–eosin. The identification of bacteria with con-comitant inflammatory signs such as sequester formation, pres-ence of immune-competent cells, periost reaction and/orperiosteal reaction was defined as infection.
2.6. Statistical analysis
Sample size calculation was based on the hypothesis that rifam-picin–fosfomycin coating can reduce infection rates by 50% com-pared to standard implants (null hypothesis). This targeted 50%
V. Alt et al. / Acta Biomaterialia 10 (2014) 4518–4524 4521
reduction of infection rate would indicate a great clinical successand was therefore considered as the target for statistical differencein the current study. Statistical analysis was done with Fisher’sexact test using a two sided v2-test using SPSS for Windows(version 21.0). Differences with a P-value < 0.05 were consideredto be statistically significant.
3. Results
3.1. Study 1: MSSA
Inoculation doses of 105 or 106 CFUs of MSSA EDCC 5055 wereused for this study.
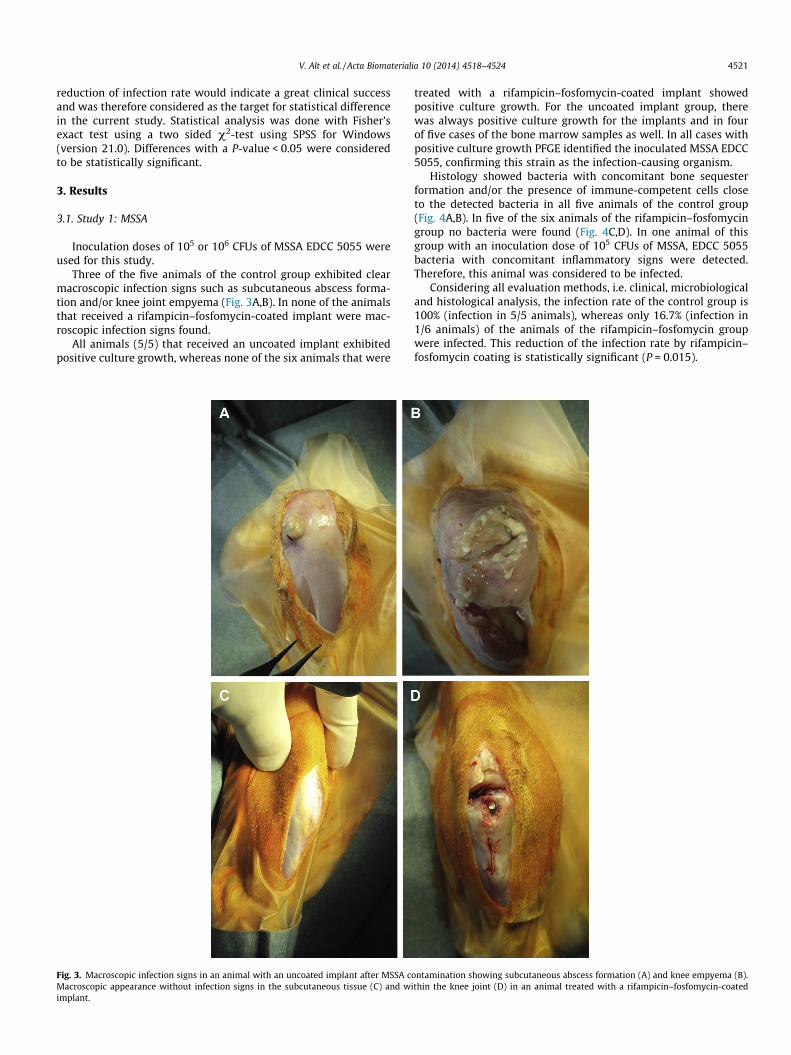
Three of the five animals of the control group exhibited clearmacroscopic infection signs such as subcutaneous abscess forma-tion and/or knee joint empyema (Fig. 3A,B). In none of the animalsthat received a rifampicin–fosfomycin-coated implant were mac-roscopic infection signs found.
All animals (5/5) that received an uncoated implant exhibitedpositive culture growth, whereas none of the six animals that were
Fig. 3. Macroscopic infection signs in an animal with an uncoated implant after MSSA cMacroscopic appearance without infection signs in the subcutaneous tissue (C) and wiimplant.
treated with a rifampicin–fosfomycin-coated implant showedpositive culture growth. For the uncoated implant group, therewas always positive culture growth for the implants and in fourof five cases of the bone marrow samples as well. In all cases withpositive culture growth PFGE identified the inoculated MSSA EDCC5055, confirming this strain as the infection-causing organism.
Histology showed bacteria with concomitant bone sequesterformation and/or the presence of immune-competent cells closeto the detected bacteria in all five animals of the control group(Fig. 4A,B). In five of the six animals of the rifampicin–fosfomycingroup no bacteria were found (Fig. 4C,D). In one animal of thisgroup with an inoculation dose of 105 CFUs of MSSA, EDCC 5055bacteria with concomitant inflammatory signs were detected.Therefore, this animal was considered to be infected.
Considering all evaluation methods, i.e. clinical, microbiologicaland histological analysis, the infection rate of the control group is100% (infection in 5/5 animals), whereas only 16.7% (infection in1/6 animals) of the animals of the rifampicin–fosfomycin groupwere infected. This reduction of the infection rate by rifampicin–fosfomycin coating is statistically significant (P = 0.015).
ontamination showing subcutaneous abscess formation (A) and knee empyema (B).thin the knee joint (D) in an animal treated with a rifampicin–fosfomycin-coated

Fig. 4. Histological evaluation of an animal that received an uncoated implant (control group) of the MSSA study with abscess formation (arrow) in the intramedullary canal(A) (scale bar: 1 mm). In detail histology (B): presence of bacteria (arrow) within the abscess surrounded by a wall of immune competent cells (arrow head) (scale bar 20 lm).Intact cortical and intact bone marrow structure of an animal of the rifampicin–fosfomycin group of the MSSA study (C) (scale bar: 200 lm) without signs of infectionreactions in Haversian (arrow) or Volkmann channels (arrow head) and intact osteocytes (D) (scale bar: 50 lm).
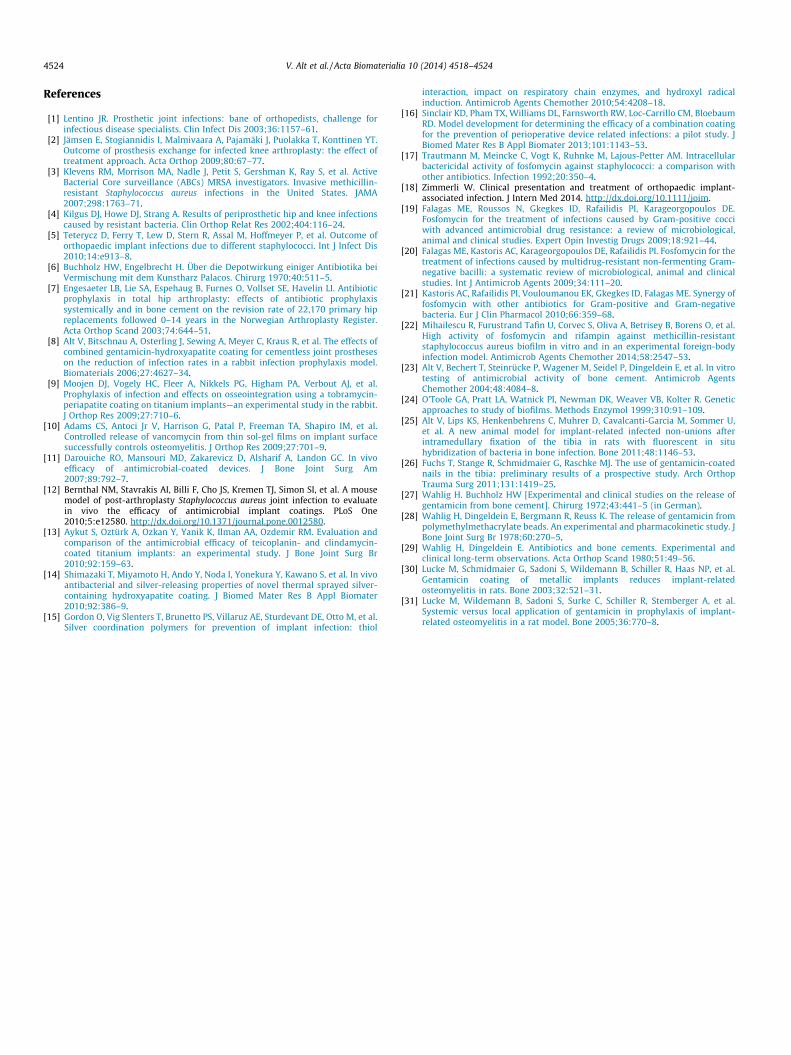
Fig. 5. Macroscopic appearance of an animal treated with an uncoated implant after MRSA contamination with extensive pus formation in the knee joint infection signs in ananimal with an uncoated implant after MRSA contamination showing knee empyema (A). Macroscopic appearance without infection signs within the knee joint (B) in ananimal treated with a rifampicin–fosfomycin-coated implant.
4522 V. Alt et al. / Acta Biomaterialia 10 (2014) 4518–4524
3.2. Study 2: MRSA
Three of five animals of the control group exhibited clear mac-roscopic infection signs such as subcutaneous abscess formationand/or knee joint empyema (Fig. 5). These were the animals thatreceived the dose of 106 CFUs of MRSA T6625930. All animalsof the rifampicin–fosfomycin group were free of macroscopicinfection signs.
As in study 1, all animals (5/5) that received an uncoatedimplant were found to have positive culture growth on the agarplates whereas none of the six animals that received a rifampi-cin–fosfomycin-coated implant showed positive culture growth.
PFGE confirmed the inoculated MRSA T6625930 in all cases withpositive culture growth.
Histological analysis identified bacteria with concomitantbone sequester formation and/or the presence of immune-competent cells close to the detected bacteria in all five animalsof the control group. One animal of the rifampicin–fosfomycingroup with an inoculation dose of 106 CFUs MRSA T6625930was also found to have sporadic bacteria in the bone marrowand cortical bone (Fig. 6) with concomitant inflammatory signs.Therefore, this animal was also considered to be infected. All fiveother animals of this group were free of bacteria based on histo-logical assessment.

V. Alt et al. / Acta Biomaterialia 10 (2014) 4518–4524 4523
Based on clinical, microbiological and histological evaluation,the infection rate of the control group and the rifampicin–fosfomy-cin coating group is 100% (infection in 5/5 animals) and 16.7%(infection in 1/6 animals), respectively, which also means a statis-tically significant reduction of the infection rate (P = 0.015) due tothe rifampicin–fosfomycin coating.
4. Discussion
The goal of antimicrobial coatings for cementless prostheses isto reduce infection rates. The rifampicin–fosfomycin coating testedhere showed excellent antimicrobial activity against both MSSAand MRSA, with statistically significant reduction of infection ratescompared to uncoated control implants.
Currently, there is no published animal model for the assess-ment of the antimicrobial activity of antibiotic-coated K-wires tomimic the human situation after implantation of a cementless jointprosthesis. Animal models in orthopedics should in general try totarget the human situation as accurately as possible [25]. Thismeans for antimicrobial testing of implant coatings for cementlessjoint prostheses that the models should enable osseous implanta-tion with joint contact of the coated device. Anatomical and biome-chanical preconditions between bone and soft tissue are quitedifferent, and therefore total joint implants intended for boneanchorage in the joint environment should be tested in osseousand not in soft tissue environment.
Several studies concerning the in vivo antimicrobial activity ofantibiotic-coated implants in animal models have been reported[8–16]. Gordon et al. [15] and Shimazaki et al. [14] used rat modelswith only subcutaneous implantation of the coated device, whichhence exhibit the above-mentioned serious limitations. The otherabove-mentioned models [8–13,16] fulfil at least some importantprerequisites for a more realistic testing of joint prosthesescomponents as all of them allow for osseous implantation withintra-articular contact of the device. It is accepted that thesemodels do not allow articulation between implants and thereforedo not fully mimic the human joint arthroplasty situation. In thesestudies the implants coated with antibiotics such as minocycline–rifampicin [11,12], tobramycin–periapatite [9] or teicoplanin plusclindamycin [13] were challenged only against MSSA strains andnot against MRSA. The reported activity of thermal sprayed sil-ver-containing hydroxyapatite coating against MRSA was obtainedas mentioned above only in a subcutaneous implantation model[14,15]. Sinclair et al. [16] found in vivo activity of a cationicsteroidal antimicrobial coating which is not based on an antibioticdrug technology. Therefore, the present work with the rifampicin–fosfomycin coating is the first one that successfully shows theactivity of an antibiotic coating in an implant-associated boneand joint infection model against MRSA.
We have used this model previously for the assessment of theantimicrobial activity of gentamicin-coated implants [8]. This
Fig. 6. Bacteria (arrow) in cortical erosion tunnels in a rifampicin–fosfomycin-treated animal (scale bar: 20 lm).
model reliably leads to implant-associated bone and knee jointinfection in the uncoated control group with infection rates of88% as shown previously [8] and 100% in this study with clear mac-roscopic signs of infection. Therefore, this model is suitable for thetesting of antibiotic-coated implants for cementless arthroplasty.
The rifampicin–fosfomycin coating exhibited excellent antimi-crobial activity against both MSSA and MRSA with statistically sig-nificant reduction of infection rates compared to uncoated controlimplants in the current study. Moreover, the coating proved itsantimicrobial performance when applying a relatively high con-centration of bacteria in the inoculum, leaving behind only spo-radic bacteria. In clinical practice the desired aim is to minimizethe exposure to bacteria as much as possible (disinfection) so thatthe host defence is able to cope with the remaining bacteria. There-fore, the rifampicin–fosfomycin coating can serve as an importantpart of the prophylaxis concept enabling the disinfection of thewound in cementless arthroplasty.
One limitation of the study is the small sample size number ofonly six animals per subgroup. Furthermore, the two animals lostwere not replaced during the study. Therefore, the limited statisti-cal power of the study should be kept in mind when interpretingthe results.
The transferability of preclinical experimental data into clinicalpractice always needs to be discussed. Currently, there are no anti-biotic-coated implants in cementless arthroplasty available, whichmakes the comparison between results from animal models andclinical trials impossible. However, the principle of local deliveryof antibiotics from implants has been clinically established inorthopedic surgery for antibiotic-loaded bone cement [7], and cur-rently for gentamicin-coated intramedullary nails for tibia frac-tures [26]. In both cases preclinical testing in animal modelsshowed the successful translation of the principle of local deliveryof antibiotics by the antibiotic-loaded implants. For poly(methylmethacrylate) bone cement, the original preclinical studies in dif-ferent animal models [27–29] revealed successful release of differ-ent antibiotics such as gentamicin on which the further clinicaltesting was based. The preclinical antimicrobial activity for genta-micin– poly-DL-lactic acid (PDLLA) coating has been established ina rat model [30,31]. which led to the development of a gentamicin–PDLLA-coated tibia nail for human application. This should pavethe way for transferring results from experimental trials with ade-quate models into clinical practice in the context of local deliveryof antibiotics in orthopedic surgery.
5. Conclusion
There is a tremendous need for new strategies to improve infec-tion prophylaxis and reduce infection rates in total joint replace-ment including cementless arthroplasty. The growing incidenceof MRSA-related total joint infection, worsening the outcome aftertotal joint infections, shows the importance of extending prophy-laxis strategies against MRSA strains. The rifampicin–fosfomycincoating presented here shows excellent antimicrobial activityagainst MSSA and MRSA that warrants further clinical testing.
Acknowledgement
The study was supported by Biomet Deutschland GmbH.
Appendix A. Figures with essential color discrimination
Certain figures in this article, particularly Figs. 1 and 3–6, aredifficult to interpret in black and white. The full color images canbe found in the on-line version, at http://dx.doi.org/10.1016/j.actbio.2014.06.013.
4524 V. Alt et al. / Acta Biomaterialia 10 (2014) 4518–4524
References
[1] Lentino JR. Prosthetic joint infections: bane of orthopedists, challenge forinfectious disease specialists. Clin Infect Dis 2003;36:1157–61.
[2] Jämsen E, Stogiannidis I, Malmivaara A, Pajamäki J, Puolakka T, Konttinen YT.Outcome of prosthesis exchange for infected knee arthroplasty: the effect oftreatment approach. Acta Orthop 2009;80:67–77.
[3] Klevens RM, Morrison MA, Nadle J, Petit S, Gershman K, Ray S, et al. ActiveBacterial Core surveillance (ABCs) MRSA investigators. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA2007;298:1763–71.
[4] Kilgus DJ, Howe DJ, Strang A. Results of periprosthetic hip and knee infectionscaused by resistant bacteria. Clin Orthop Relat Res 2002;404:116–24.
[5] Teterycz D, Ferry T, Lew D, Stern R, Assal M, Hoffmeyer P, et al. Outcome oforthopaedic implant infections due to different staphylococci. Int J Infect Dis2010;14:e913–8.
[6] Buchholz HW, Engelbrecht H. Über die Depotwirkung einiger Antibiotika beiVermischung mit dem Kunstharz Palacos. Chirurg 1970;40:511–5.
[7] Engesaeter LB, Lie SA, Espehaug B, Furnes O, Vollset SE, Havelin LI. Antibioticprophylaxis in total hip arthroplasty: effects of antibiotic prophylaxissystemically and in bone cement on the revision rate of 22,170 primary hipreplacements followed 0–14 years in the Norwegian Arthroplasty Register.Acta Orthop Scand 2003;74:644–51.
[8] Alt V, Bitschnau A, Osterling J, Sewing A, Meyer C, Kraus R, et al. The effects ofcombined gentamicin-hydroxyapatite coating for cementless joint prostheseson the reduction of infection rates in a rabbit infection prophylaxis model.Biomaterials 2006;27:4627–34.
[9] Moojen DJ, Vogely HC, Fleer A, Nikkels PG, Higham PA, Verbout AJ, et al.Prophylaxis of infection and effects on osseointegration using a tobramycin-periapatite coating on titanium implants—an experimental study in the rabbit.J Orthop Res 2009;27:710–6.
[10] Adams CS, Antoci Jr V, Harrison G, Patal P, Freeman TA, Shapiro IM, et al.Controlled release of vancomycin from thin sol-gel films on implant surfacesuccessfully controls osteomyelitis. J Orthop Res 2009;27:701–9.
[11] Darouiche RO, Mansouri MD, Zakarevicz D, Alsharif A, Landon GC. In vivoefficacy of antimicrobial-coated devices. J Bone Joint Surg Am2007;89:792–7.
[12] Bernthal NM, Stavrakis AI, Billi F, Cho JS, Kremen TJ, Simon SI, et al. A mousemodel of post-arthroplasty Staphylococcus aureus joint infection to evaluatein vivo the efficacy of antimicrobial implant coatings. PLoS One2010;5:e12580. http://dx.doi.org/10.1371/journal.pone.0012580.
[13] Aykut S, Oztürk A, Ozkan Y, Yanik K, Ilman AA, Ozdemir RM. Evaluation andcomparison of the antimicrobial efficacy of teicoplanin- and clindamycin-coated titanium implants: an experimental study. J Bone Joint Surg Br2010;92:159–63.
[14] Shimazaki T, Miyamoto H, Ando Y, Noda I, Yonekura Y, Kawano S, et al. In vivoantibacterial and silver-releasing properties of novel thermal sprayed silver-containing hydroxyapatite coating. J Biomed Mater Res B Appl Biomater2010;92:386–9.
[15] Gordon O, Vig Slenters T, Brunetto PS, Villaruz AE, Sturdevant DE, Otto M, et al.Silver coordination polymers for prevention of implant infection: thiol
interaction, impact on respiratory chain enzymes, and hydroxyl radicalinduction. Antimicrob Agents Chemother 2010;54:4208–18.
[16] Sinclair KD, Pham TX, Williams DL, Farnsworth RW, Loc-Carrillo CM, BloebaumRD. Model development for determining the efficacy of a combination coatingfor the prevention of perioperative device related infections: a pilot study. JBiomed Mater Res B Appl Biomater 2013;101:1143–53.
[17] Trautmann M, Meincke C, Vogt K, Ruhnke M, Lajous-Petter AM. Intracellularbactericidal activity of fosfomycin against staphylococci: a comparison withother antibiotics. Infection 1992;20:350–4.
[18] Zimmerli W. Clinical presentation and treatment of orthopaedic implant-associated infection. J Intern Med 2014. http://dx.doi.org/10.1111/joim.
[19] Falagas ME, Roussos N, Gkegkes ID, Rafailidis PI, Karageorgopoulos DE.Fosfomycin for the treatment of infections caused by Gram-positive cocciwith advanced antimicrobial drug resistance: a review of microbiological,animal and clinical studies. Expert Opin Investig Drugs 2009;18:921–44.
[20] Falagas ME, Kastoris AC, Karageorgopoulos DE, Rafailidis PI. Fosfomycin for thetreatment of infections caused by multidrug-resistant non-fermenting Gram-negative bacilli: a systematic review of microbiological, animal and clinicalstudies. Int J Antimicrob Agents 2009;34:111–20.
[21] Kastoris AC, Rafailidis PI, Vouloumanou EK, Gkegkes ID, Falagas ME. Synergy offosfomycin with other antibiotics for Gram-positive and Gram-negativebacteria. Eur J Clin Pharmacol 2010;66:359–68.
[22] Mihailescu R, Furustrand Tafin U, Corvec S, Oliva A, Betrisey B, Borens O, et al.High activity of fosfomycin and rifampin against methicillin-resistantstaphylococcus aureus biofilm in vitro and in an experimental foreign-bodyinfection model. Antimicrob Agents Chemother 2014;58:2547–53.
[23] Alt V, Bechert T, Steinrücke P, Wagener M, Seidel P, Dingeldein E, et al. In vitrotesting of antimicrobial activity of bone cement. Antimicrob AgentsChemother 2004;48:4084–8.
[24] O’Toole GA, Pratt LA, Watnick PI, Newman DK, Weaver VB, Kolter R. Geneticapproaches to study of biofilms. Methods Enzymol 1999;310:91–109.
[25] Alt V, Lips KS, Henkenbehrens C, Muhrer D, Cavalcanti-Garcia M, Sommer U,et al. A new animal model for implant-related infected non-unions afterintramedullary fixation of the tibia in rats with fluorescent in situhybridization of bacteria in bone infection. Bone 2011;48:1146–53.
[26] Fuchs T, Stange R, Schmidmaier G, Raschke MJ. The use of gentamicin-coatednails in the tibia: preliminary results of a prospective study. Arch OrthopTrauma Surg 2011;131:1419–25.
[27] Wahlig H. Buchholz HW [Experimental and clinical studies on the release ofgentamicin from bone cement]. Chirurg 1972;43:441–5 (in German).
[28] Wahlig H, Dingeldein E, Bergmann R, Reuss K. The release of gentamicin frompolymethylmethacrylate beads. An experimental and pharmacokinetic study. JBone Joint Surg Br 1978;60:270–5.
[29] Wahlig H, Dingeldein E. Antibiotics and bone cements. Experimental andclinical long-term observations. Acta Orthop Scand 1980;51:49–56.
[30] Lucke M, Schmidmaier G, Sadoni S, Wildemann B, Schiller R, Haas NP, et al.Gentamicin coating of metallic implants reduces implant-relatedosteomyelitis in rats. Bone 2003;32:521–31.
[31] Lucke M, Wildemann B, Sadoni S, Surke C, Schiller R, Stemberger A, et al.Systemic versus local application of gentamicin in prophylaxis of implant-related osteomyelitis in a rat model. Bone 2005;36:770–8.