richard s. adler, m.d. staff psychiatrist children’s hospital & regional medical center &...
TRANSCRIPT

RICHARD S. ADLER, M.D.
Staff Psychiatrist Children’s Hospital & Regional Medical Center
&Private Practice
Forensic & Clinical Psychiatry
Seattle, WA

WHICH IS IT?
ADHD,
BIPOLAR DISORDER OR
ASPERGER’S DISORDER?
New York Area
Florida
April – May 2003


Overview
Interactive Case – Participant Centered Learning
What differentiates these disorders? Clinical Management +/- comorbidity? Clinical strategies when the diagnosis is
uncertain Q & A

ADHD: Comorbidity In Majority
1NIMH2Milberger S et al. J Am Acad Child Adolesc Psychiatry 1997;36:37-44.3Biederman et al. J Am Acad Child Adolesc Psychiatry 1997;36:21-29.
60
55
50
45
40
35
30
25
20
15
10
5
0
(%)
OppositionalDefiantDisorder1
Anxietydisorders1
Learningdifficulties1
Mooddisorders1
Conductdisorder1
Smoking2 SubstanceUseDisorder3
Languagedisorder
40%
30-35%
20-25%
15-20% 15-20% 15-20% 19%15%

ALISSA CHAVARONE

Alissa is a youngster transferred to your care. Her prior attending is no longer on her parents’ insurance panel. In the fall of 1st grade Alissa was noted to have problems with inattention and impulsivity that interfered with her school achievement and behavior. In the home, she was difficult to manage, irritable, highly demanding and had tantrums that at times seemed entirely unprovoked. She was rough with, and sometimes completely mean to her 3-year old sister. By the spring of first grade the teacher suggested that her parents obtain an evaluation for the attention deficit.




Have you ever thought, or has anyone ever told you, that they suspected that your child might have Attention
Deficit Hyperactivity Disorder (ADHD)?
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38

Have you ever thought, or has anyone ever told you, that they suspected that your child might have Attention
Deficit Hyperactivity Disorder (ADHD)?
Total
3346
%
Yes
No
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38

Have you ever thought, or has anyone ever told you, that they suspected that your child might have Attention
Deficit Hyperactivity Disorder (ADHD)?
Total
3346
%
Yes 35
No 65
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38

Who was it that suspected that your child might have Attention Deficit Hyperactivity Disorder (ADHD)?
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38

Who was it that suspected that your child might have Attention Deficit Hyperactivity Disorder (ADHD)?
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38
Total
1143
%
Me
Doctor or other medical professional
School professional (i.e. teacher, nurse, guidance counselor)
Social worker
Friend or family member

Who was it that suspected that your child might have Attention Deficit Hyperactivity Disorder (ADHD)?
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38
Total
1143
%
Me 45
Doctor or other medical professional
School professional (i.e. teacher, nurse, guidance counselor)
Social worker
Friend or family member

Who was it that suspected that your child might have Attention Deficit Hyperactivity Disorder (ADHD)?
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38
Total
1143
%
Me 45
Doctor or other medical professional
School professional (i.e. teacher, nurse, guidance counselor)
62
Social worker
Friend or family member

Who was it that suspected that your child might have Attention Deficit Hyperactivity Disorder (ADHD)?
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, McNeil Consumer Healthcare, 2002, p. 38
Total
1143
%
Me 45
Doctor or other medical professional
30
School professional (i.e. teacher, nurse, guidance counselor)
62
Social worker 15
Friend or family member 25


Did you seek help for your child after this possibility was raised?
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, Harris Interactive, 2002, p. 39

Did you seek help for your child after this possibility was raised?
Total
1143
%
Yes
No
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, Harris Interactive, 2002, p. 39

Did you seek help for your child after this possibility was raised?
Total
1143
%
Yes 79
No 21
Cultural Attitudes & Perceptions About Attention Deficit Hyperactivity Disorder, Harris Interactive, 2002, p. 39

Alyssa's pediatrician started her on Ritalin at a low dose daily. It was remarkably helpful in all areas of Alissa’s schoolwork and behavior, but tended to wear off by mid-afternoon. Alissa’s mother went to a CHADD meeting and was urged to get a Health Impairment Form filled out by the doctor. Alissa was placed close to the teacher and had frequent breaks during the day. A parent at CHADD also told Mrs. Chavarone about Ritalin SR. Upon mother’s request the doctor switched Alissa to Ritalin SR which was somewhat less effective overall but seemed to last for more of the school day.

Representative Behavioral Half-lives
of the Stimulant Medications for ADHD
Wilens, Spencer. Child Adolesc Psychiatr Clin N Am. In press
Re
spo
nse
Hours0 2 4 6 10
MPH IR/D-AMPHMPH SRMixed AMPH saltsOROS® MPH

Alissa’s 2nd and 3rd grades progressed with numerous suspensions for misbehavior, including a number of fights, one of which involved biting another student. The Chavarone’s prior insurance did not cover mental health treatment. The pediatrician referred Alissa to the local mental health clinic, but she remained on a wait list for two years. Occasional pastoral counseling reassured Mrs. Chavarone that it was OK to have Alissa on medication. Alissa appeared to be socially immature and she had only one friend who shared her fascination with Pokeman cards. Alissa insisted that other children call her Pikachu and gave all the other children in the class names of characters from the cards. She would giggle and laugh when they expressed dislike for this habit of hers.

Qualitative impairment in social interaction, as manifested by at least two of the following:
Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction
Failure to develop peer relationships appropriate to development level
A lack of spontaneous seeking to share enjoyment, interests, and activities with other people (e.g., by a lack of showing, bringing, or pointing out of objects of interest to other people)
Lack of social or emotional reciprocity
DSM IV Diagnostic Criteria for Asperger’s Disorder

Restricted repetitive and sterotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
Encompassing preoccupation with one or more sterotyped and restricted patterns of interest that is abnormal either in intensity or focus
Apparently inflexible adherence to specific, nonfunctional routines or rituals Stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements)
Persistent preoccupation with parts of objects
DSM IV Diagnostic Criteria for Asperger’s Disorder

The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning.
There is no clinically significant general delay in language (e.g., single words used by age 2 years, communicative phrases used by age 3 years).
There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood.
Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia.
DSM IV Diagnostic Criteria for Asperger’s Disorder

In 4th grade Alissa appeared to be sad, withdrawn and angry. She did not sleep well, and reported that she feared the devil would take her soul if she slept too deeply. She appeared drawn, tired and would ask staff and students, even those she did not know: “I don’t need to sleep, do you?”

Survey of NDMDA Members
• N = 500• 59% endorsed onset during childhood or
adolescence• 48% did not get dx until consulting at least
3 professionals• 10% did not get dx until consulting at least
7 professionals
Lish JD, Dime-Meenan J, Whybrow PC. J Affective Disorders, 1994, 31(4), 281-94

“Akiskal described the profile of a child at risk to develop bipolar illness as one who experienced emotions, whether they be positive or negative, passionately and intensely and whose mood and behavior was dysregulated and disinhibited. Predictors of bipolar outcome in adolescents with major depression have been identified as a family history of bipolar disorder, sudden onset of symptoms, delusions, psychomotor retardation and hypersomnia, pharmacologically induced hypomania/mania (Akiskal and coworkers; Strober and Carlson)”.
Cogan MB. Psychiatric Times, 13 (5), 1996

DSM IV Diagnostic Criteria for Manic Episode
A distinct period of abnormally and persistently elevated, expansive, or irritable mood, lasting at least 1 week (or any duration if hospitalization is necessary).
During the period of mood disturbance, three (or more) of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree:
Inflated self-esteem or grandiosity
Decreased need for sleep (e.g. feels rested after only 3 hours of sleep)
More talkative than usual or pressure to keep talking
Flight of ideas or subjective experience that thoughts are racing distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli)
Distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli)
Increase in goal-directed activity (either socially, at work or school, or sexually) or psychomotor agitation
Excessive involvement in pleasurable activities that have a high potential for painful consequences (e.g. engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments).

Bipolar Disorder in Youth:• M>F
• Mixed>manic or depressed, esp. prepubertal [DeLong & Aldershof 1987]
• Mixed phase: dysphoria, hypomania and agitation intermixed
• Incr. freq. of psychotic sxs, grandiosity, bizarre
delusions Of those with MDD pre-
pubertally, 20-33% incidence of Bipolar Disorder

The pediatrician increased the Ritalin SR to address Alissa’s worsening behavior but it was assumed that this was causing insomnia. Mrs. Chavarone urged the pediatrician to give Alissa something to help her sleep. The pediatrician prescribed imipramine for sleep. Initially it was helpful. Alissa’s mood improved. She began to play with her sister, even if the sister forgot to call her Pikachu.

In 5th grade Alissa had worsening difficulties. In September it was attributed to transitioning back to school, and a change in teachers due to an unexpected illness in teaching staff. By October, Alissa frequently left class and the playground on a whim. She seemed to be in constant motion, almost frantic. At times she would shriek at the top of her lungs, or sing “Happy Birthday” in the middle of class. Her mother initiated a referral for Special Education services after chatting with another mother on the MSN ADHD chat room. When the examining School Psychologist asked Alissa why she insisted that he call her Pikachu, she turned over his laptop and threw a vase out his window. The vase hit a child in a wheelchair below.

The school called the police, who took Alissa in handcuffs to the Emergency Room. The psychiatrist on duty told Alissa that she was misbehaving terribly and would not likely get many toys for Christmas if she persisted in this way. She told him: “My father spanks me everyday with a belt and I still won’t behave, so kiss my ass doctor.” Mrs. Chavarone confirmed that her husband often used this form of discipline. The Emergency Room social worker insisted on reporting the family to CPS. The psychiatrist wrote a 10-day prescription for Mellaril to help Alissa “calm down.”

The new medication was initially helpful and the pediatrician continued the Mellaril. Alissa appeared a bit sluggish and cognitively less sharp, but her aggression decreased. The pediatrician discontinued the imipramine because the Mellaril had been helpful for sleep. Alissa told a classmate: “OK, I’m not really Pikachu, I just like Pikachu.”

After your initial visit with the patient, the parents tell you that Alissa is starting to “outgrow her ADD”, they have limited funds and would like to discontinue her medications.

Discussion Issue 1:What is the most likely
diagnosis?

Telling one from the other: Why isn’t it easier?
Many symptoms in common Some illnesses develop over time (like a Polaroid picture – fuzzy at first, obvious after the fact) Denial & minimization, lack of clinician expertise, patient access to care

How does the clinician differentiate one disorder from the other?
Inclusion and exclusion criterion (DSM-IV) Pattern recognition (experience) Family history Progression of illness ? Response to interventions
Positive and negative “Pharmacological dissection”

Differential DiagnosisADHD MDI ASP
INCIDENCE 5-7%
M:F::1-3:1
< 1%
M>F
< 0.5%
M>F
MEDIAN AGE FOR CLINICAL PRESENTATION
9 M
11 F
? 11
COURSE OF ILLNESS HYPERACTIVITY DECREASES, COMORBIDITY INCREASES, RESPONSE TO ADD MEDS PERSIST
PSYCHOSIS NOT UNCOMMON
EXACERBATION IN ADOLESCENCE
FH & GENETICS HERED = 0.75 HERED =
0.4-0.75
MZ CONCORD FOR PDD SPECTRUM IS 90%, INCR FH MDI
ASSOCIATED FEATURES
LD, ODD, CD, MOOD, ANX, SUBST AB
SUBST ABUSE ADD SXS, OCD SXS. MOOD 50%
TREATMENT STIM, NON-STIM ADD MOOD STABIL,ANTI
PSYCHOTICS, APS (COMPLEX REGIMENS)
SSRIs, ANTIPSYCHOTICS, STIMS

Differential Diagnosis
ADHD MDI ASP
PROGNOSIS FAIRLY GOOD WITH TX
GUARDED MINIMAL CHANGE WITH
TX
PSYCHOSOCIAL TREATMENT
ROLE OF DECREASED
EE
FOCUS ON STRUCTURE, DECREASED
EE

Discussion Issue 2:What further workup
is indicated?

Diagnostic Options for Asperger’s Disorder
Hearing Evaluation Vision Evaluation IQ Testing Speech and Language Evaluation Chemistries, CBC, Thyroid Function Tests Lead Level Fragile X Testing Amino Acids/Organic Acids Chromosome karyotype EEG Brain MRI Neurology Consultation Genetics Consultation
Source: Posey, DJ, McDougle CJ.Autism:A Three-step Practical Approach to making the Diagnosis. Current Psychiatry 2002;1:20-28.

Discussion Issue 3:What would an ideal treatment plan look
like for Alyssa?


Educate and engage parents re: uncertainty Develop a cascade of interventions (e.g. Plan A, Plan B,
Plan C) Assess level of parental support (e.g. respite, NAMI, CHADD) Address parental psychopathology Visit and re-visit FH of psychiatric illnessSet reasonable goals and timelines for interventions, target specific symptoms, then follow closely Involve multiple informants Get consultation, especially peer-to-peer
Strategies for managing when the diagnosis is uncertain

EDUCATIONAL INTERVENTIONS


Classroom Strategy and Effectiveness Rating [ADHD]
26%2.32.6Sensory Modulation Techniques
31%2.53.0Time Out
65%3.03.0Peer Tutoring
42%3.53.2Assistance During Transitions
56%3.53.2Use of Quiet Work Area
59%3.63.3Environmental Modifications
55%3.53.4Alternative Evaluations
40%3.63.5Individual Behavior Program
70%3.73.5Teach Self-Monitoring of Behavior
42%3.53.6Assignment Modifications
54%3.63.6Curriculum Modifications
61%3.73.6Use of Motor Breaks
76%4.14.0Frequent Contact
76%4.34.1Routine and Structure
53%3.94.2Preferential Seating
% OF TEACHERS USING ON REGULAR STUDENTS
EFFECTIVENESSFREQUENCYSTRATEGY
Source: Mulligan, S. Classroom Strategies Used by Teachers of Students with Attention Deficit Hyperactivity Disorder. Physical & Occupational Therapy in Pediatrics, Vol. 20(4) 2001, 25-44.

INSTRUCTION
Adjust reading level Allow student to tape lectures Permit child to submit typed or word-processed
homework Provide a written outline for work when feasible Use peer tutoring Preprint chalkboard and oral instructions so that
students may refer to them later
Classroom Accommodations To Consider In ADHD
Source: A Guide to the Educational Rights of Children with ADHD [pamphlet]. Shire US Inc. Florence, Kentucky, July 2002.

Classroom Accommodations To Consider In ADHD
TESTING
Allow open-book tests Provide practice questions for study Give multiple-choice instead of short-answer questions Permit the use of a dictionary or calculator during test Provide extra time to complete work
Source: A Guide to the Educational Rights of Children with ADHD [pamphlet]. Shire US Inc. Florence, Kentucky, July 2002.

Classroom Accommodations To Consider In ADHD
COMMUNICATION
Create a daily/weekly journal Schedule periodic parent/teacher meetings Provide parents and students with a duplicate set of
texts that they can use at home for the school year Develop weekly progress reports Mail a schedule of classroom and homework
assignments to student’s parents
Source: A Guide to the Educational Rights of Children with ADHD [pamphlet]. Shire US Inc. Florence, Kentucky, July 2002

Classroom Accommodations to Consider in Asperger's Disorder
CONSIDERATIONS Visual Schedules Oral Presentations provided in written form Routine Predictable Schedule Sensory Outlet Breaks Placement in classroom offering least sensory
distraction Facilitate Social Relationships

A SIDE-BY SIDE COMPARISON OF SECTION 504 AND IDEA
Source: A Guide to the Educational Rights of Children with ADHD [pamphlet]. Shire US Inc. Florence, Kentucky, July 2002.
IDEASECTION 504
•In order to receive special education services, ADHD must result in a child’s heightened alertness to stimuli in the classroom that limits his or her alertness in academic tasks
•A child is considered eligible for Section 504 if ADHD substantially limits a major life activity
ADHD must result in an adverse effect on academic performance, and the student must require special education services in order to address his or her ADHD and its impact
Since learning is considered a major life activity, a child is eligible under Section 504 if ADHD substantially limits his or her ability to learn
•The effects of ADHD must be long lasting (chronic) or have a substantial impact (acute)
•A child not eligible for special education may still receive related services if he or she meets the eligibility requirements

Requires that an evaluation be performed, without undue delay, to determine if a child requires special education services
Requires a local district to make an individualized determination of child’s educational needs for regular or special education, or related aids and services, if the child is found eligible under Section 504
Requires that the rights and protections provided by IDEA are extended to children with ADHD and their parents
Requires that a free appropriate public education (FAPE) be provided to each qualified child who is disabled, but does not require special education services under IDEA. FAPE includes regular or special education and related aids and services that are designed to meet an individual student’s needs and are based on adherence to the regulatory requirements for education setting, evaluation, placement, and procedural safeguards
IDEASECTION 504
•Requires that state and local districts make a free appropriate public education available to all eligible children with disabilities
•Prohibits discrimination on the basis of disability by recipients of federal funds
SUMMARY OF LEGAL REQUIREMENTS
Source: A Guide to the Educational Rights of Children with ADHD [pamphlet]. Shire US Inc. Florence, Kentucky, July, 2002.
A SIDE-BY SIDE COMPARISON OF SECTION 504 AND IDEA

A SIDE-BY SIDE COMPARISON OF SECTION 504 AND IDEA
Requires that an evaluation be performed, without undue delay, to determine if a child requires special education services
Requires a local district to make an individualized determination of child’s educational needs for regular or special education, or related aids and services, if the child is found eligible under Section 504
Requires that the rights and protections provided by IDEA are extended to children with ADHD and their parents
Requires that a free appropriate public education (FAPE) be provided to each qualified child who is disabled, but does not require special education services under IDEA. FAPE includes regular or special education and related aids and services that are designed to meet an individual student’s needs and are based on adherence to the regulatory requirements for education setting, evaluation, placement, and procedural safeguards
IDEASECTION 504
•Requires that state and local districts make a free appropriate public education available to all eligible children with disabilities
•Prohibits discrimination on the basis of disability by recipients of federal funds
SUMMARY OF LEGAL REQUIREMENTS
Source: A Guide to the Educational Rights of Children with ADHD [pamphlet]. Shire US Inc. Florence, Kentucky, July, 2002.

Treating ADD Symptoms
• PDDs:
– Expect less robust results with stimulants
– Anticipate lower mg/kg/d dosing for stimulants than in ADHD
– Be alert for worsening of anxiety with stimulants
• Bipolar Disorder:
– Mood stabilization is #1 priority.
– ADD meds are added later.


OROS® Methylphenidate HCI qd (ConcertaTM) Versus Methylphenidate HCI tid (Ritalin®)
PlasmaConcentration
(ng/mL)
Time (h)
0 1 2 3 4 5 6 7 8 9 10 11 12
6
5
4
3
2
1
0
OROS MPH 1x/dMPH 3x/dN = 61 ADHD children
Swamson JM et al. Comparison of efficacy and safety of ConcertaTM (methylphenidate HCL) with Riralin® and placebo in children with ADHD. Presented at Region IX and X Annual Meeting of the Ambulatory Pediatric Association: February 12-13, 2000: Carmel, CA.

CONCERTA®: Dosing
The 27mg tablet The 27mg tablet is now available is now available
for increased for increased dosing flexibilitydosing flexibility
CONCERTA®: Dosing• Results from a pivotal initiation study showed that 84%
of patients titrated to their optimal dose required doses above 18 mg:1
– 16% of patients were titrated to 18 mg– 40% of patients were titrated to 36 mg– 44% of patients were titrated to 54 mg
• Appropriate to initiate therapy with CONCERTA®1
– In truly naïve patients– In patients who have previously used other therapies
– 96% of treated patients were successfully dose titrated
1 Swanson J et al. J Clin Res 2000;3:59-76.

METADATE CD:


ADDERALL XR
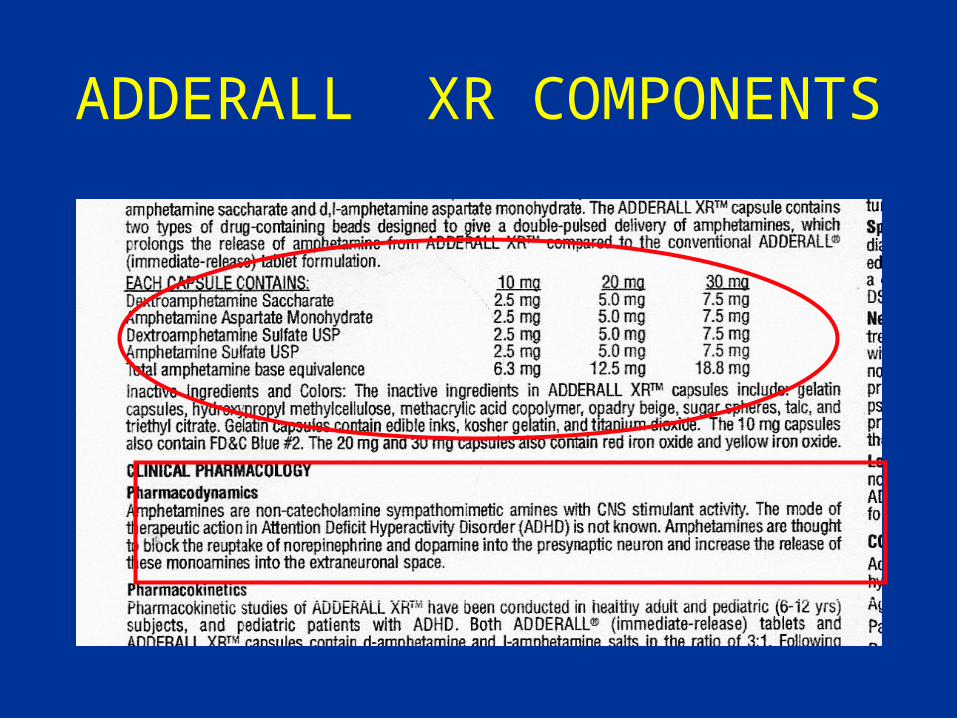
ADDERALL XR COMPONENTS

ATOMOXETINE(Strattera)
Highly selective noradrenergic reuptake inhibitor FDA approval 12/02 for children, adolescents & adults Non-stimulant 2/3 as impactful as suggested by Connors rating No significant insomnia, tics, minimal appetite impact Sexual side effects, somnolence, dyspepsia, urinary retention Metabolized via CYP450 2D6
Inhibited strongly by fluoxetine, paroxetine Buproprion and St. John’s Wort are weaker inhibitors
Dose initiated at 0.5 mg/kg/d x 3d, then 1.4 mg/kg/d Deepening effect over the course of weeks May need to cross taper or augment with stimulants

The Medical LetterOn Drugs and Therapeutics
Strattera ‘may be worth trying in patients who Have not responded to stimulants Cannot tolerate stimulants Do not want to take a controlled substance.’
The Medical Letter, V45, February 3, 2003, pp. 11 – 13.

Monthly Retail Cost
The Medical Letter, V45, February 3, 2003, p. 11.
AGENT COST DOSE (MG)
COMMENT
ATOMOXETINE $ 90 ANY ONE CAP
10, 18, 25, 40, 60 MGS
ADDERALL XR $ 73.20 20
CONCERTA $ 74.70 36


Strategies for Managing Asperger's Disorder
Behavioral Treatment: Parent Education, Structure, Decreased EE
Psychopharmacologic Treatment Speech and Occupational Therapy Social skills training Assist Parents in obtaining “guaranteed”
appropriate education (i.e. Special Education) either within district or elsewhere


Richard S. Adler, M.D.
2910 E. Madison St., Suite #202
Seattle, WA 98112
(206) 621-9325
www.RichardAdlerMD.com
THANK YOU !
COMMENTS? QUESTIONS?



www.citizen.org/hrgwww.fda.govhttp://jama.ama-assn.org