richard furie, md -...
TRANSCRIPT

4/16/2018
1
SLE: Neuropsychiatric Lupus
Richard Furie, MDChief, Division of Rheumatology
Northwell HealthProfessor of Medicine
Zucker School of Medicine at Hofstra Northwell
Disclosures
Nothing to disclose in relationship to this topic
Learning Objective
1. Review the classification of neuropsychiatric lupus2. Describe mechanisms of injury in lupus3. Discuss specific neuropsychiatric complications of
lupus and the approach to treatment
4/16/2018
2
I Hate the Word Cerebritis
Neuropsychiatric Lupus Syndromes
Central Nervous SystemAcute Confusional State Cognitive DysfunctionMyasthenia Gravis Anxiety DisorderHeadache Aseptic MeningitisNeuropathy, Cranial Movement Disorder (Chorea)Psychosis Cerebrovascular DiseaseMood Disorders Seizures and Seizure DisordersDemyelinating Syndrome
Peripheral Nervous SystemAcute Inflammatory Demyelinating Polyradiculoneuropathy (Guillain-
Barré Syndrome)Myelopathy Mononeuropathy (single/multiplex)Plexopathy Autonomic DisorderPolyneuropathy
ACR Ad Hoc Committee of Neuropsychiatric Lupus Nomenclature. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. 1999;42:599–608
Ab
C’
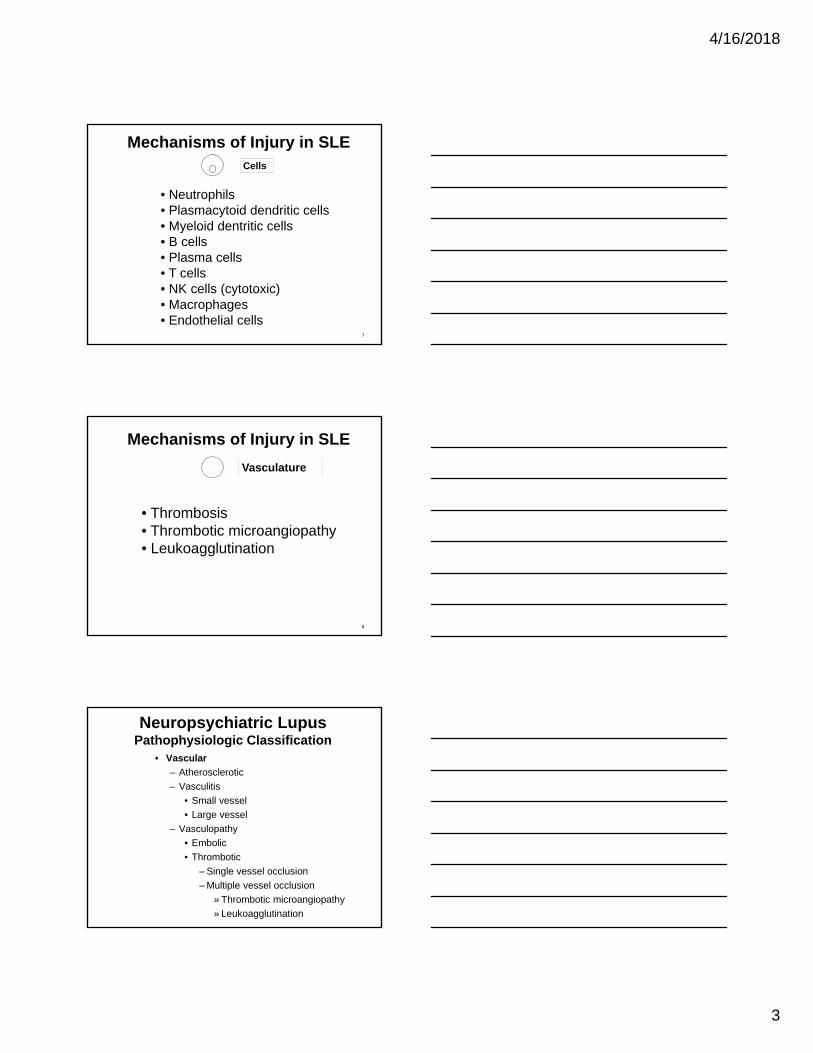
Mechanisms of Injury in SLE
CNS dysfunction
Apoptosis
Ab
Direct Binding
IC
Kidney
Immune Complex
Ab
CDCC
AHA (cold)
C’
Fc
ADCC
ATP
AHA (warm)
FcR
6
4/16/2018
3
Mechanisms of Injury in SLE
• Neutrophils• Plasmacytoid dendritic cells• Myeloid dentritic cells• B cells• Plasma cells• T cells • NK cells (cytotoxic)• Macrophages• Endothelial cells
Cells
7
Mechanisms of Injury in SLE
• Thrombosis • Thrombotic microangiopathy• Leukoagglutination
Vasculature
8
Neuropsychiatric LupusPathophysiologic Classification
• Vascular
– Atherosclerotic
– Vasculitis
• Small vessel
• Large vessel
– Vasculopathy
• Embolic
• Thrombotic
– Single vessel occlusion
– Multiple vessel occlusion
» Thrombotic microangiopathy
» Leukoagglutination
4/16/2018
4
Neuropsychiatric LupusPathophysiologic Classification
• Extra-vascular
– Ab-mediated dysfunction
– Cell-mediated injury
– Cytokine-mediated
NP Lupus TreatmentPathophysiology Treatment
• Vascular (occlusion vs hemorrhage)
– Vasculitis steroids, IS
– Vasculopathy
• Thrombotic
– Thrombotic microangiopathy plasmapheresis
eculizumab
– Leukoagglutination steroids
– Single vessel occlusion anticoagulation
• Embolic anticoagulation
• Extra-vascular
– Ab-mediated dysfunction steroids, IS
– Cell-mediated injury steroids, IS
– Cytokine-mediated steroids, IS
Embolic Complications
4/16/2018
5
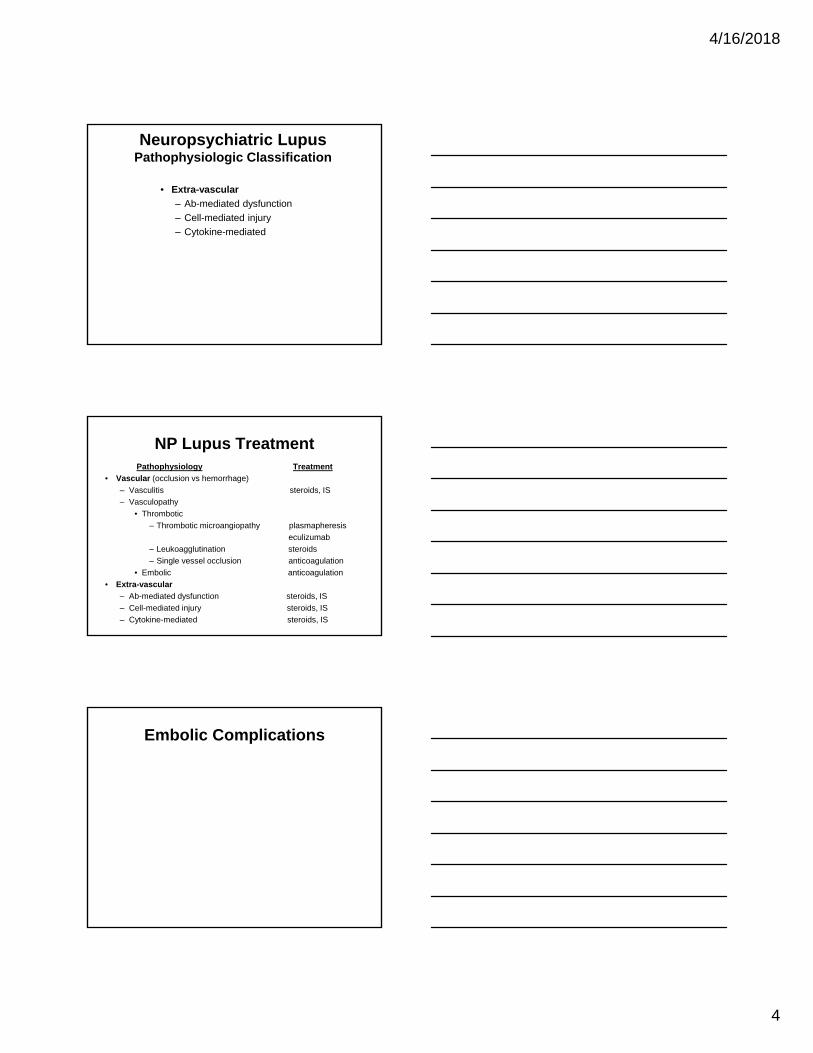
Intracardiac Thrombus
Stroke
• Case: 45 y/o F with 8-year history of SLE admitted for chest pain.
PE: possible rub
ECHO:
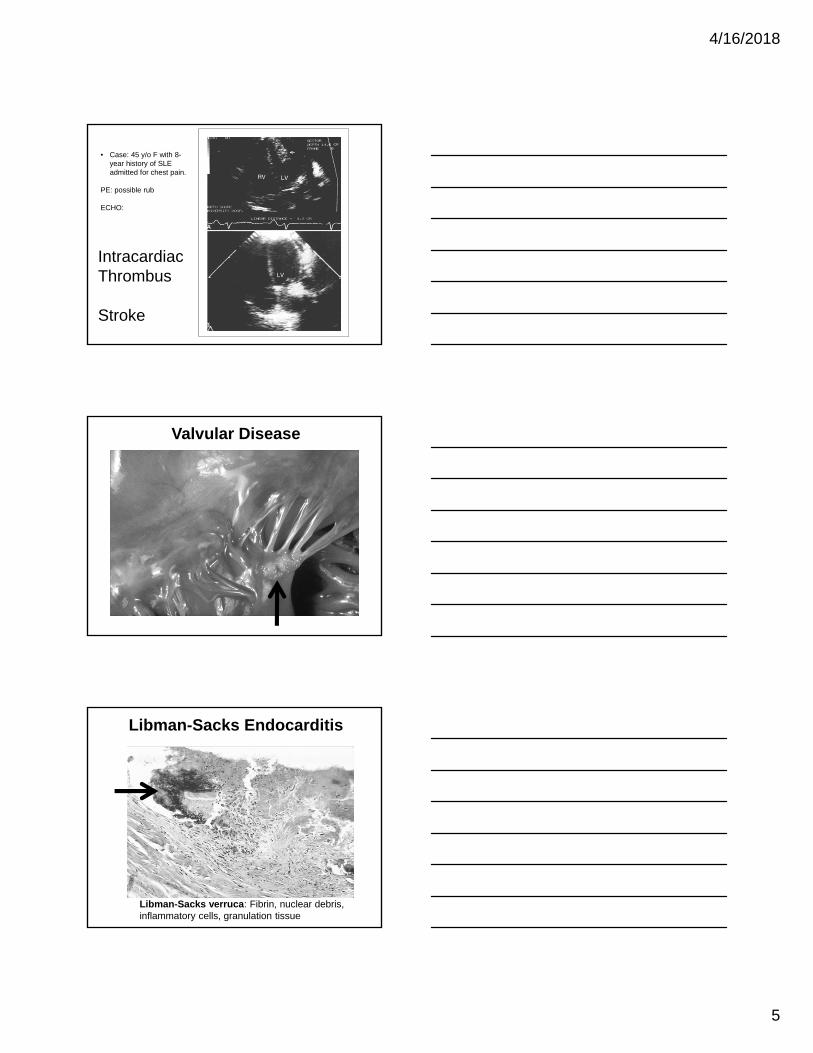
Valvular Disease
Libman-Sacks Endocarditis
Libman-Sacks verruca: Fibrin, nuclear debris, inflammatory cells, granulation tissue

4/16/2018
6
Thrombotic Complications
Thrombotic Complications
• Case: 58 y/o F– 30 year history of SLE complicated by AHA
controlled with MMF and rituximab
– Initial visit labs notable for:• Beta-2 glycoprotein I IgG Ab: >150 (<15)
• Anticardiolipin IgG Ab: 120 (<15)
– No history of miscarriage or thrombosis
• Would you advise therapy for primary prevention?
• If so, which medicine?– ASA
– Clopidogrel
– Warfarin
– Prednisone
– Something else?

4/16/2018
7
• Case continued– Placed on ASA 81 mg per day
• Stroke – Treated with heparin and then warfarin
• What are the data for secondary prevention?
• What is the appropriate INR target?
Preventing the First Clot
• Risk of thrombosis < 5% per year
• Confounded by other factors
• APLASA (Erkan 2007): ASA 81 mg vs placebo
– N=98; f/u 2.3 years
– ASA (3 events); placebo (0)
– ASA did not protect against thrombosis
• ?? ASA for primary prevention ??
• ?? HCQ for primary prevention ??
Preventing the Second Clot
• Retrospective Studies– Warfarin better than ASA– Warfarin HD better than LD
• Prospective Studies– Warfarin Mod Intensity = High Intensity
Targeting a specific INR is easier said than done
4/16/2018
8
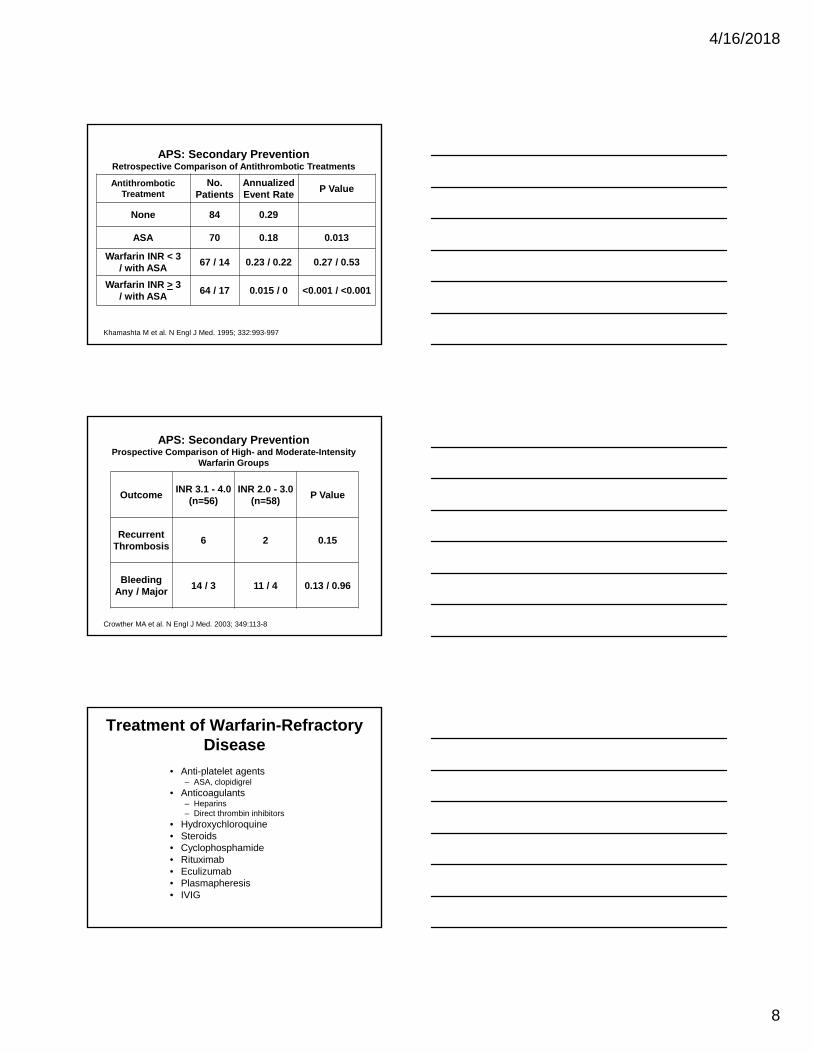
Antithrombotic Treatment
No. Patients
Annualized Event Rate
P Value
None 84 0.29
ASA 70 0.18 0.013
Warfarin INR < 3/ with ASA
67 / 14 0.23 / 0.22 0.27 / 0.53
Warfarin INR > 3/ with ASA
64 / 17 0.015 / 0 <0.001 / <0.001
APS: Secondary PreventionRetrospective Comparison of Antithrombotic Treatments
Khamashta M et al. N Engl J Med. 1995; 332:993-997
OutcomeINR 3.1 - 4.0
(n=56)INR 2.0 - 3.0
(n=58)P Value
RecurrentThrombosis
6 2 0.15
BleedingAny / Major
14 / 3 11 / 4 0.13 / 0.96
APS: Secondary PreventionProspective Comparison of High- and Moderate-Intensity
Warfarin Groups
Crowther MA et al. N Engl J Med. 2003; 349:113-8
Treatment of Warfarin-Refractory Disease
• Anti-platelet agents– ASA, clopidigrel
• Anticoagulants– Heparins– Direct thrombin inhibitors
• Hydroxychloroquine• Steroids• Cyclophosphamide• Rituximab• Eculizumab• Plasmapheresis• IVIG

4/16/2018
9
Thrombotic Microangiopathy
Medical History
27 year old female with a 5 year history of SLE was admitted to the hospital because of confusion and fever.
Stupor turned to coma
Thrombotic Microangiopathy
Laboratory Results
Hb 6.8 g/dLPlt 12 K/uL
PT / PTT 12 / 66 secondsDIC screen normalLAC positive
Creatinine 1.9 mg/dL
LDHHaptoglobinReticulocyte countDirect Coombs testBlood smear
1200not detectable15.5 %negative
Thrombotic Microangiopathy
Treatment: Plasmapheresis: complete response within 1 week

4/16/2018
10
Thrombotic Microangiopathy1
1. Thrombocytopenia2. Microangiopathic hemolytic anemia (schistocytes)3. Organ dysfunction (kidney; brain; heart; GB)
Issues:1. Relationship to aHUS, to CAPS2. Role of eculizumab in treating TMA3. Need for chronic anticoagulation
Thrombotic Microangiopathy
1Symmers W. Br Med J, 2 (1952), pp. 897-903
SLE/APS Vasculopathy
Venous thrombosis (large vessel)
Thrombotic Microangiopathy
Occlusive Arteriopathy
Venous Thrombosis small ; large vessel
Headache
• Case: 28 y/o F with a 4-year history of SLE complicated by rash and Raynauds. She was admitted because of acute headache
PE: unremarkable
Labs: unremarkable except for RNP Ab
Imaging studies: normal
4/16/2018
11
Differential Diagnosis
1.Stroke2.Venous sinus thrombosis3. Intracranial hemorrhage4.Meningitis5.Aseptic meningtis (NSAIDs)6.Central nervous system lupus
Headache in SLE
SLEDAI definition:
"severe, persistent headache; may be migrainous, but must be nonresponsive to narcotic analgesia”
Epratuzumab (EMBLEMTM) and Lupus Headache
• 227 patients in dose-ranging study
• At baseline:– 15 headache (8 points)
Petri et al. ACR 2011.

4/16/2018
12
Headache in SLE
Prevalence:
All headache: 33-78%Migraine: 32%Tension: 24%
Davey R et al. Cephalagia 2008; Davey R et al. Arthritis Rheum 2007
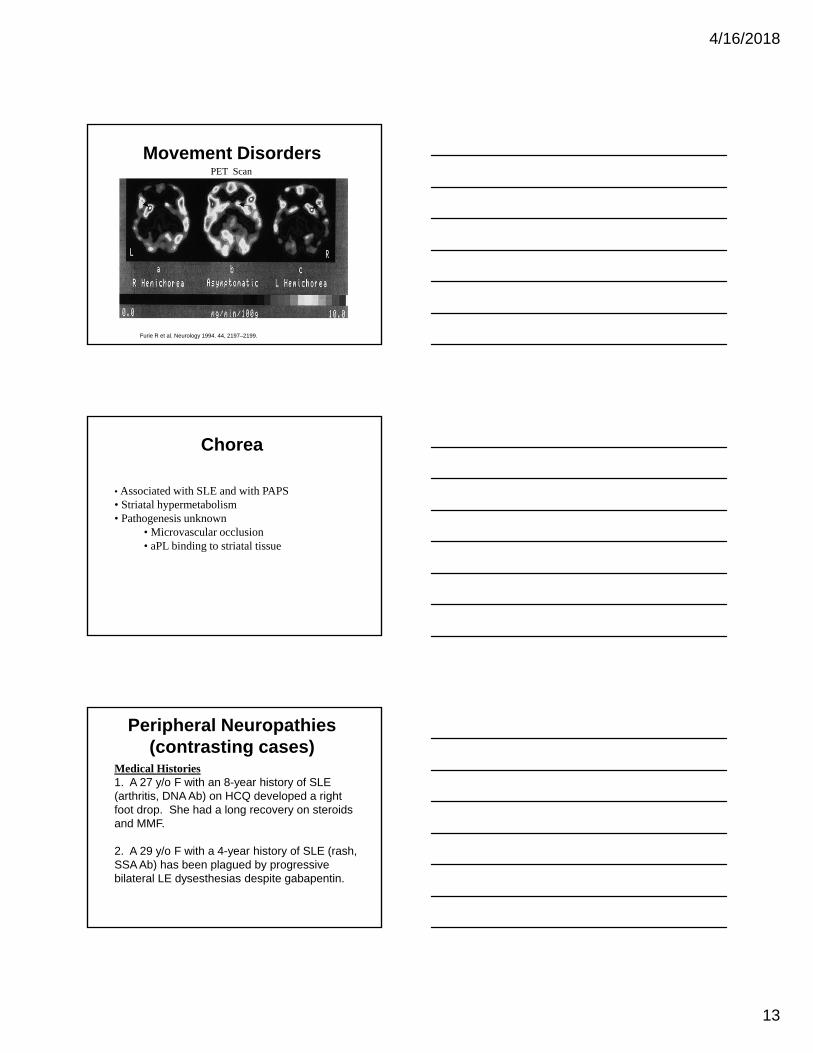
Movement Disorders
Case: A 24 y/o F with steroid-responsivethrombocytopenia was referred for evaluationof possible SLE. She had no otherinflammatory manifestations. During theinterview, she had spontaneous flailingmovements of the right wrist as well as choreicmovements of the fingers of the right hand.
Livedo Reticularis
4/16/2018
13
Movement DisordersPET Scan
Furie R et al. Neurology 1994. 44, 2197–2199.
Chorea
• Associated with SLE and with PAPS• Striatal hypermetabolism• Pathogenesis unknown
• Microvascular occlusion• aPL binding to striatal tissue
Peripheral Neuropathies(contrasting cases)
Medical Histories1. A 27 y/o F with an 8-year history of SLE (arthritis, DNA Ab) on HCQ developed a right foot drop. She had a long recovery on steroids and MMF.
2. A 29 y/o F with a 4-year history of SLE (rash, SSA Ab) has been plagued by progressive bilateral LE dysesthesias despite gabapentin.

4/16/2018
14
Peripheral Neuropathies in 4924 Chinese SLE Patients
Overall frequency: 1.5%
Wang X et al. Medicine (Baltimore). 2015 Mar; 94(11): e625.
Nerve Fiber Classification
• Large nerve fibers– A-alpha fibers
• Myelinated
• Mediate motor strength
– A-beta fibers• Mediate vibratory and touch sensation
Tavee J, Zhou L. Clev Clin J Med 2009; 76: 297-305
• Medium-sized fibers– A-gamma fibers
• Myelinated
• Innervate muscle spindles
Nerve Fiber Classification
4/16/2018
15
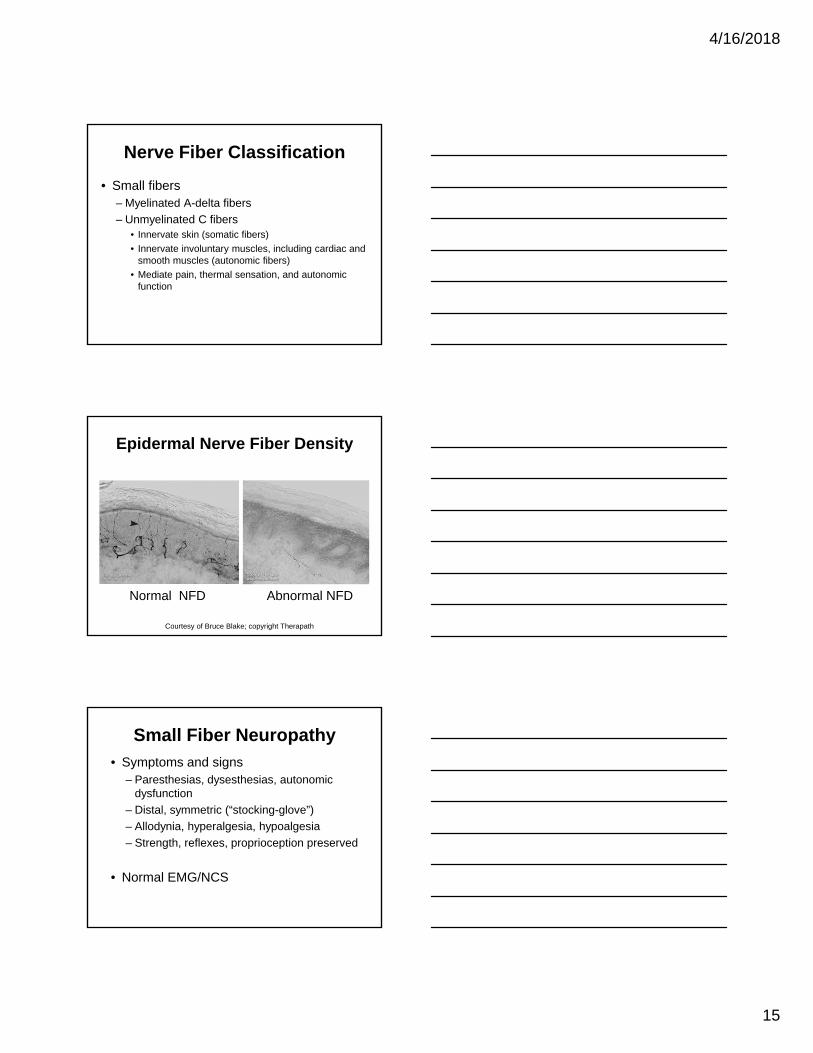
• Small fibers– Myelinated A-delta fibers
– Unmyelinated C fibers• Innervate skin (somatic fibers)
• Innervate involuntary muscles, including cardiac and smooth muscles (autonomic fibers)
• Mediate pain, thermal sensation, and autonomic function
Nerve Fiber Classification
Epidermal Nerve Fiber Density
Courtesy of Bruce Blake; copyright Therapath
Normal NFD Abnormal NFD
Small Fiber Neuropathy
• Symptoms and signs– Paresthesias, dysesthesias, autonomic
dysfunction
– Distal, symmetric (“stocking-glove”)
– Allodynia, hyperalgesia, hypoalgesia
– Strength, reflexes, proprioception preserved
• Normal EMG/NCS

4/16/2018
16
Small Fiber Neuropathy
• Skin biopsy: measure intra-epidermal nerve fiber density (few labs perform)
• Nerve biopsy not justified
• Therapy– Gabapentin, pregabalin
– Amitriptyline, nortriptyline
– Lidocaine patch
– Analgesics
– ? Role of steroids, IS
Complications of Treatment
• Reversible Posterior Leukoencephalopathy Syndrome• Progressive Multifocal Leukoencephalopathy• Peripheral neuropathy
• Thalidomide
Reversible Posterior Leukoencephalopathy Syndrome
• Background– 1996: 15 cases reported (Hinchey J et al. NEJM 1996)
• Clinical Presentation– Headache, altered mental status– Hypertension– Seizures, cortical blindness
• Causes– Malignant hypertension (4), eclampsia (3)– Tacrolimus or cyclosporin (7), interferon (1)– Hypercalcemia
4/16/2018
17
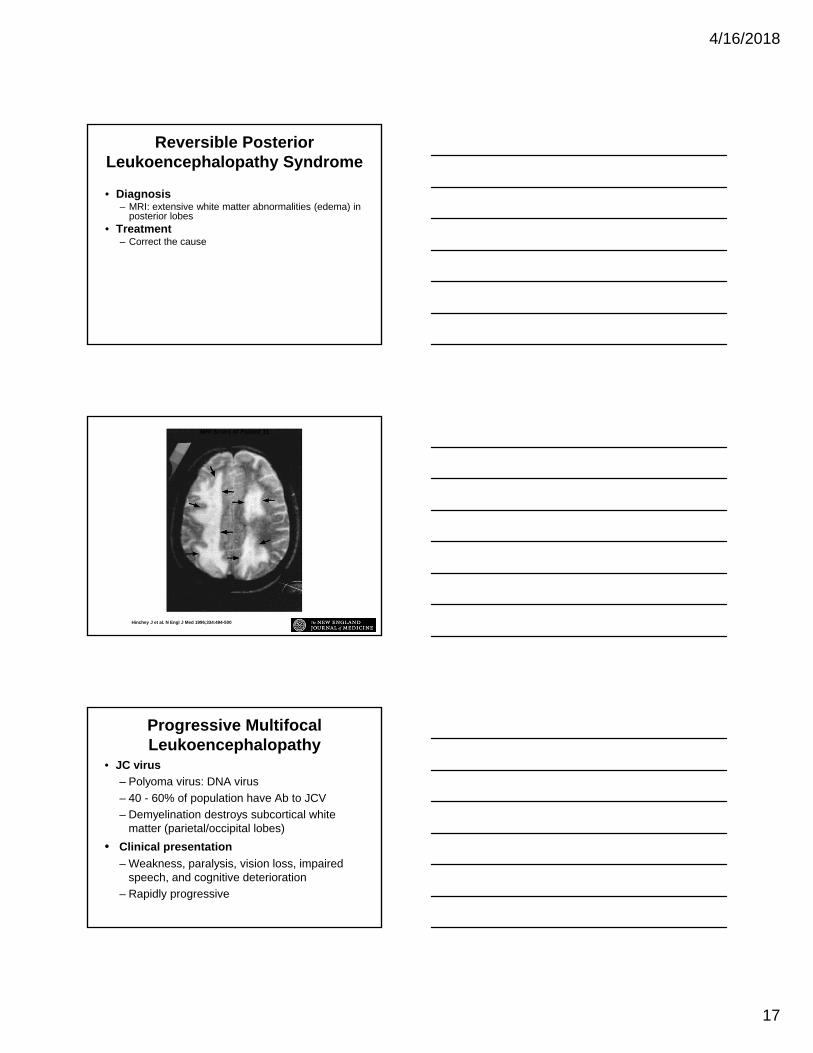
Reversible Posterior Leukoencephalopathy Syndrome
• Diagnosis– MRI: extensive white matter abnormalities (edema) in
posterior lobes• Treatment
– Correct the cause
Hinchey J et al. N Engl J Med 1996;334:494-500
MRI Scans of Patient 11
Progressive Multifocal Leukoencephalopathy
• JC virus
– Polyoma virus: DNA virus
– 40 - 60% of population have Ab to JCV
– Demyelination destroys subcortical white matter (parietal/occipital lobes)
• Clinical presentation
– Weakness, paralysis, vision loss, impaired speech, and cognitive deterioration
– Rapidly progressive
4/16/2018
18
Progressive Multifocal Leukoencephalopathy
• Diagnosis– MRI:
• Multifocal hyperintense lesions on T2W images
• Non-enhancing with IV contrast
• Cortical white matter, but brainstem and cerebellum may be involved
– Test for JC virus DNA in CSF or brain bx
Progressive Multifocal Leukoencephalopathy
• Prevalence in Autoimmune Rheumatic Diseases1
– 34 cases in FDA AE Reporting System DB
– SLE (17); RA (10); Vasculitis (4); DM (3)
– 15 treated with > 1 biologic• Rituximab (14); 10 on concomitant IS
• TNF inhibitor (6)
– 19 treated with non-biologic IS• 14 had received an alkylating agent
1Molloy E and Calabrese L; Arthritis Rheum 2012
Progressive Multifocal Leukoencephalopathy
• Prevalence in SLE1
– 17 cases in FDA AE Reporting System DB• Rituximab (5);
– 5 on IS; 3 had received alkylating agents
• Non-biologic agents (12)– 10 had received an alkylating agent
– 2 on IS alone (MTX; AZA)
1Molloy E and Calabrese L; Arthritis Rheum 2012
4/16/2018
19
Progressive Multifocal Leukoencephalopathy
• Risk factors for PML (natalizumab-treatment) 1
– 212 cases in nearly 100,000 treated patients
– Risk:• Natalizumab: 2.1 cases/1000)
– Seronegative patients: 0.09 cases/1000
– Seropositive and IS use and natalizumab for 2-4 years: 11 cases/1000
– Should we be evaluating JC serologies?
1Bloomgren G et al. N Engl J Med 2012
I Need Help With…
1. TIA: 47 y/o F chronically serologically active (low C’, high DNA Ab) and leukopenia on HCQ with acute RUE weakness. History of migraine.
CT negativeReceived TPAMRI/MRA normal, TEE normalaPL Ab negative
Treatment: ASA, clopidogrel? Immunosuppressives
I Need Help With…
2. Psychosis: 42 y/o F with 6-year history of SLE consisting of arthritis treated with MTX. Labs notable for mild elevation of DNA Ab. She became acutely psychotic but responded to haloperidol. She has continued to have intermittent psychotic episodes.
? Immunosuppressives
4/16/2018
20
I Need Help With…
3. Carotid stenosis/stroke: 37 y/o F with SLE (DLE, arthritis, Raynauds) and APS (DVT) chronically treated with steroids, HCQ, MMF, and rivaroxaban. She has been serologically active (Sm Ab) and aPL Ab positive.
She had an acute cerebral infarct resulting in right hemiplegia
MRI: left MCA and PCA territory infarctsAngio: severe left carotid stenosis (Moya-Moya like)
Treatment:1. Left superficial temporal artery to MCA microanastomosis2. Warfarin3. ? Immunosuppressives
I Need Help With…
4. Transverse myelitis5. Fatigue6. Cognitive dysfunction7. Psychosis8. Peripheral sensory neuropathies
NP Lupus TreatmentPathophysiology Treatment
• Vascular (occlusion vs hemorrhage)
– Vasculitis steroids, IS
– Vasculopathy
• Thrombotic
– Thrombotic microangiopathy plasmapheresis
eculizumab
– Leukoagglutination steroids
– Single vessel occlusion anticoagulation
• Embolic anticoagulation
• Extra-vascular
– Ab-mediated dysfunction steroids, IS
– Cell-mediated injury steroids, IS
– Cytokine-mediated steroids, IS
4/16/2018
21
Thank You
Questions?
Answers?
more questions than answers