richard & edith mass 15 main st 2015 income … & edith mass 15 main st chelmsford, ma 01824...
TRANSCRIPT

RICHARD & EDITH MASS15 MAIN ST
CHELMSFORD, MA 018242015 INCOME TAX RETURN

INVOICE
Description Amount
Total Invoice
Amount Paid
Balance Due
������������������������������������������������������������������������
������������������������������������������������������������������������
������������������������������������������������������������������������
������������������������������������������������������������������������
��������������������������������
��������������������������������
������������������������������������������
������������������������������������������
������������������������������������������
������
������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
��������������������������������������������
��������������������������������������������
� �� �� �� �� �� �� �
PRACTICE LAB15 PRACTICE LAB WAYWASHINGTON DC 20005
(202) 202-2022
RICHARD D MASS & EDITH M MASS15 MAIN STCHELMSFORD MA 01824(978) 251-3131
Preparer No.: 995Client No. : XXX-XX-7210Invoice Date: 10/14/2016
PREPARATION OF 2015 FEDERAL/STATE FORMS & WORKSHEETS:
FORM 1040 ASCHEDULE B (INTEREST & DIVIDENDS)FORM W-2 (WAGES AND TAX)FORM 1099-R (RETIREMENT DISTRIBUTIONS) (2)FORM 8879 (E-FILE SIGNATURE AUTHORIZATION)MA STATE RESIDENT RETURN
$0.00
$0.00
$0.00
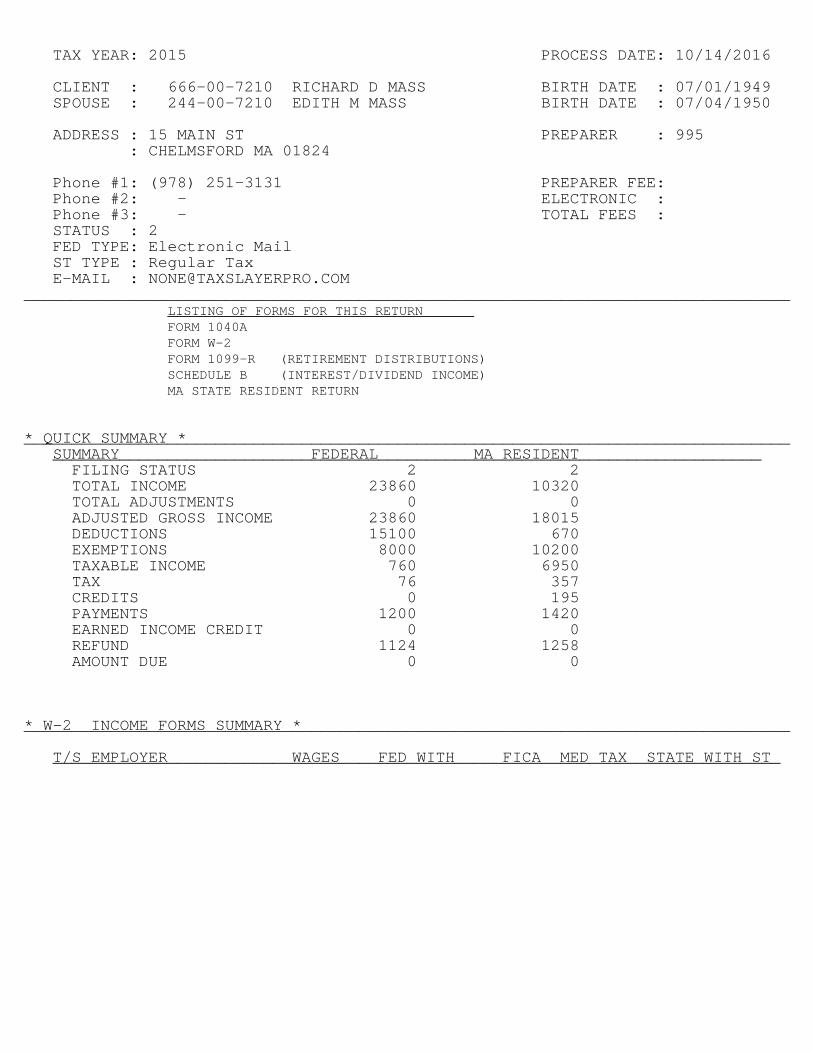
TAX YEAR: 2015 PROCESS DATE: 10/14/2016
CLIENT : 666-00-7210 RICHARD D MASS BIRTH DATE : 07/01/1949SPOUSE : 244-00-7210 EDITH M MASS BIRTH DATE : 07/04/1950
ADDRESS : 15 MAIN ST PREPARER : 995 : CHELMSFORD MA 01824
Phone #1: (978) 251-3131 PREPARER FEE: Phone #2: - ELECTRONIC : Phone #3: - TOTAL FEES : STATUS : 2FED TYPE: Electronic MailST TYPE : Regular TaxE-MAIL : [email protected]
________________________________________________________________________________LISTING OF FORMS FOR THIS RETURN________________________________FORM 1040AFORM W-2FORM 1099-R (RETIREMENT DISTRIBUTIONS)SCHEDULE B (INTEREST/DIVIDEND INCOME)MA STATE RESIDENT RETURN
* QUICK SUMMARY *________________________________________________________________________________SUMMARY__________________________________________________________________________
FILING STATUSTOTAL INCOMETOTAL ADJUSTMENTSADJUSTED GROSS INCOMEDEDUCTIONSEXEMPTIONSTAXABLE INCOMETAXCREDITSPAYMENTSEARNED INCOME CREDITREFUNDAMOUNT DUE
FEDERAL 2 23860 0 23860 15100 8000 760 76 0 1200 0 1124 0
MA RESIDENT 2 10320 0 18015 670 10200 6950 357 195 1420 0 1258 0
* W-2 INCOME FORMS SUMMARY *________________________________________________________________________________
T/S EMPLOYER WAGES FED WITH FICA MED TAX STATE WITH ST ____________________________________________________________________________

CLIENT : RICHARD MASS 666-00-7210SPOUSE : EDITH MASS 244-00-7210
PREPARER : 995 DATE : 10/14/2016________________________________________________________________________________
LISTING OF FORMS FOR THIS RETURN________________________________
* W-2 INCOME FORMS SUMMARY *________________________________________________________________________________
T/S EMPLOYER WAGES FED WITH FICA MED TAX STATE WITH ST ____________________________________________________________________________1. T TOWN OF CHELMS 9800 600 0 150 300 MA
TOTALS...... 9800 600 0 150 300
* 1099-R INCOME FORMS SUMMARY *________________________________________________________________________________
[T/S] PAYER GROSS DIST TAXABLE AMT FED WITH STATE WITH ___________________________________________________________________________1. T FIIDELITY INVESTM 7500 7500 0 502. T CAMBRIDGE RETIREM 6300 6300 600 0
TOTALS...... 13800 13800 600 50

a Employee’s social security numberOMB No. 1545-0008
This information is being furnished to the Internal Revenue Service. If you are required to file a tax return, a negligence penalty or other sanction may be imposed on you if this income is taxable and you fail to report it.
b Employer identification number (EIN)
c Employer’s name, address, and ZIP code
d Control number
e Employee’s first name and initial Last name Suff.
f Employee’s address and ZIP code
1 Wages, tips, other compensation 2 Federal income tax withheld
3 Social security wages 4 Social security tax withheld
5 Medicare wages and tips 6 Medicare tax withheld
7 Social security tips 8 Allocated tips
9 10 Dependent care benefits
11 Nonqualified plans 12a See instructions for box 12Co d e
12bCo d e
12cCo d e
12dCo d e
13 Statutory employee
Retirement plan
Third-party sick pay
14 Other
15 State Employer’s state ID number 16 State wages, tips, etc. 17 State income tax 18 Local wages, tips, etc. 19 Local income tax 20 Locality name
Form W-2 Wage and Tax Statement 2015
Department of the Treasury—Internal Revenue Service
a Employee’s social security numberOMB No. 1545-0008
This information is being furnished to the Internal Revenue Service. If you are required to file a tax return, a negligence penalty or other sanction may be imposed on you if this income is taxable and you fail to report it.
b Employer identification number (EIN)
c Employer’s name, address, and ZIP code
d Control number
e Employee’s first name and initial Last name Suff.
f Employee’s address and ZIP code
1 Wages, tips, other compensation 2 Federal income tax withheld
3 Social security wages 4 Social security tax withheld
5 Medicare wages and tips 6 Medicare tax withheld
7 Social security tips 8 Allocated tips
9 10 Dependent care benefits
11 Nonqualified plans 12a See instructions for box 12Co d e
12bCo d e
12cCo d e
12dCo d e
13 Statutory employee
Retirement plan
Third-party sick pay
14 Other
15 State Employer’s state ID number 16 State wages, tips, etc. 17 State income tax 18 Local wages, tips, etc. 19 Local income tax 20 Locality name
-----------------------------------------------------------------------------
666-00-7210
21-3333556
TOWN OF CHELMSFORD50 BILLERICA RDCHELMSFORD MA 01824
RICHARD D MASS
15 MAIN STCHELMSFORD MA 01824
9800 600
10320 150
OTHER 520
MA 213333556 10320 300

Form 8879Department of the Treasury Internal Revenue Service
IRS e-file Signature Authorization
Do not send to the IRS. This is not a tax return.
Keep this form for your records.
Information about Form 8879 and its instructions is at www.irs.gov/form8879.
OMB No. 1545-0074
2015
Submission Identification Number (SID)
Taxpayer’s name Social security number
Spouse’s name Spouse’s social security number
Part I Tax Return Information—Tax Year Ending December 31, 2015 (Whole Dollars Only)1 Adjusted gross income (Form 1040, line 38; Form 1040A, line 22; Form 1040EZ, line 4) . . . . . 1
2 Total tax (Form 1040, line 63; Form 1040A, line 39; Form 1040EZ, line 12) . . . . . . . . . 2
3 Federal income tax withheld (Form 1040, line 64; Form 1040A, line 40; Form 1040EZ, line 7) . . . 3
4 Refund (Form 1040, line 76a; Form 1040A, line 48a; Form 1040EZ, line 13a; Form 1040-SS, Part I, line 13a) 4
5 Amount you owe (Form 1040, line 78; Form 1040A, line 50; Form 1040EZ, line 14) . . . . . . . 5
Part II Taxpayer Declaration and Signature Authorization (Be sure you get and keep a copy of your return)
Under penalties of perjury, I declare that I have examined a copy of my electronic individual income tax return and accompanying schedules and statements for the tax year ending December 31, 2015, and to the best of my knowledge and belief, it is true, correct, and complete. I further declare that the amounts in Part I above are the amounts from my electronic income tax return. I consent to allow my intermediate service provider, transmitter, or electronic return originator (ERO) to send my return to the IRS and to receive from the IRS (a) an acknowledgement of receipt or reason for rejection of the transmission, (b) the reason for any delay in processing the return or refund, and (c) the date of any refund. If applicable, I authorize the U.S. Treasury and its designated Financial Agent to initiate an ACH electronic funds withdrawal (direct debit) entry to the financial institution account indicated in the tax preparation software for payment of my federal taxes owed on this return and/or a payment of estimated tax, and the financial institution to debit the entry to this account. This authorization is to remain in full force and effect until I notify the U.S. Treasury Financial Agent to terminate the authorization. To revoke (cancel) a payment, I must contact the U.S. Treasury Financial Agent at 1-888-353-4537. Payment cancellation requests must be received no later than 2 business days prior to the payment (settlement) date. I also authorize the financial institutions involved in the processing of the electronic payment of taxes to receive confidential information necessary to answer inquiries and resolve issues related to the payment. I further acknowledge that the personal identification number (PIN) below is my signature for my electronic income tax return and, if applicable, my Electronic Funds Withdrawal Consent.
Taxpayer’s PIN: check one box only
I authorize ERO firm name
to enter or generate my PIN Enter five digits, but do
not enter all zerosas my signature on my tax year 2015 electronically filed income tax return.
I will enter my PIN as my signature on my tax year 2015 electronically filed income tax return. Check this box only if you are entering your own PIN and your return is filed using the Practitioner PIN method. The ERO must complete Part III below.
Your signature Date
Spouse’s PIN: check one box only
I authorize ERO firm name
to enter or generate my PIN Enter five digits, but do
not enter all zerosas my signature on my tax year 2015 electronically filed income tax return.
I will enter my PIN as my signature on my tax year 2015 electronically filed income tax return. Check this box only if you are entering your own PIN and your return is filed using the Practitioner PIN method. The ERO must complete Part III below.
Spouse’s signature Date
Practitioner PIN Method Returns Only—continue belowPart III Certification and Authentication—Practitioner PIN Method Only
ERO’s EFIN/PIN. Enter your six-digit EFIN followed by your five-digit self-selected PIN.Do not enter all zeros
I certify that the above numeric entry is my PIN, which is my signature for the tax year 2015 electronically filed income tax return for the taxpayer(s) indicated above. I confirm that I am submitting this return in accordance with the requirements of the Practitioner PIN method and Publication 1345, Handbook for Authorized IRS e-file Providers of Individual Income Tax Returns.
ERO’s signature Date
ERO Must Retain This Form — See Instructions
Do Not Submit This Form to the IRS Unless Requested To Do So
For Paperwork Reduction Act Notice, see your tax return instructions. Form 8879 (2015)
QNA
RICHARD D MASS 666-00-7210
EDITH M MASS 244-00-7210
23860 76 1200 1124
10/14/2016
10/14/2016
X PRACTICE LAB 1 7 2 1 0
X PRACTICE LAB 1 7 2 1 0
3 6 9 2 5 8 1 9 2 5 8
PRACTICE LABIRS PREPARER
10/14/2016

Form
1040A 2015U.S. Individual Income Tax ReturnDepartment of the Treasury—Internal Revenue Service
IRS Use Only—Do not write or staple in this space. (99)
OMB No. 1545-0074Your first name and initial Last name
Your social security number
If a joint return, spouse’s first name and initial Last name Spouse’s social security number
Make sure the SSN(s) above and on line 6c are correct.
Home address (number and street). If you have a P.O. box, see instructions. Apt. no.
City, town or post office, state, and ZIP code. If you have a foreign address, also complete spaces below (see instructions).
Foreign country name Foreign province/state/county Foreign postal code
Presidential Election Campaign
Check here if you, or your spouse if filing jointly, want $3 to go to this fund. Checking a box below will not change your tax or refund. You Spouse
Filing status Check only one box.
1 Single2 Married filing jointly (even if only one had income)3 Married filing separately. Enter spouse’s SSN above and
full name here.
4 Head of household (with qualifying person). (See instructions.) If the qualifying person is a child but not your dependent, enter this child’s name here.
5 Qualifying widow(er) with dependent child (see instructions)Exemptions
If more than six dependents, see instructions.
6a Yourself. If someone can claim you as a dependent, do not check box 6a.
b Spouse}
c Dependents:
(1) First name Last name
(2) Dependent’s social security number
(3) Dependent’s
relationship to you
(4) if child under age 17 qualifying for child tax credit (see
instructions)
d Total number of exemptions claimed.
Boxes checked on 6a and 6b
No. of children
on 6c who:
• lived with
you
• did not live with you due to
divorce or separation (see
instructions)
Dependents
on 6c not
entered above
Add numbers
on lines
above
Income Attach Form(s) W-2 here. Also attach Form(s) 1099-R if tax was withheld. If you did not get a W-2, see instructions.
7 Wages, salaries, tips, etc. Attach Form(s) W-2. 7
8a Taxable interest. Attach Schedule B if required. 8ab Tax-exempt interest. Do not include on line 8a. 8b
9a Ordinary dividends. Attach Schedule B if required. 9ab Qualified dividends (see instructions). 9b
10 Capital gain distributions (see instructions). 1011 a IRA
distributions. 11a11b Taxable amount
(see instructions). 11b12 a Pensions and
annuities. 12a12b Taxable amount
(see instructions). 12b
13 Unemployment compensation and Alaska Permanent Fund dividends. 1314 a Social security
benefits. 14a14b Taxable amount
(see instructions). 14b
15 Add lines 7 through 14b (far right column). This is your total income. 15Adjusted gross income
16 Educator expenses (see instructions). 1617 IRA deduction (see instructions). 1718 Student loan interest deduction (see instructions). 18
19 Tuition and fees. Attach Form 8917. 1920 Add lines 16 through 19. These are your total adjustments. 20
21 Subtract line 20 from line 15. This is your adjusted gross income. 21For Disclosure, Privacy Act, and Paperwork Reduction Act Notice, see separate instructions. Form 1040A (2015)
RICHARD D. MASS
EDITH M. MASS
666-00-7210
244-00-7210
15 MAIN ST
CHELMSFORD MA 01824
X
X
X2
0
0
0
2
9800
260 163
7500
6300
23860
23860

Form 1040A (2015) Page 2
Tax, credits,
and
payments
22 Enter the amount from line 21 (adjusted gross income). 2223 a Check
if: { You were born before January 2, 1951, BlindSpouse was born before January 2, 1951, Blind }Total boxes
checked 23ab If you are married filing separately and your spouse itemizes
deductions, check here 23bStandard Deduction for—
• People who check any box on line 23a or 23b or who can be claimed as a dependent, see instructions. • All others: Single or Married filing separately, $6,300 Married filing jointly or Qualifying widow(er), $12,600 Head of household, $9,250
24 Enter your standard deduction. 2425 Subtract line 24 from line 22. If line 24 is more than line 22, enter -0-. 2526 Exemptions. Multiply $4,000 by the number on line 6d. 2627 Subtract line 26 from line 25. If line 26 is more than line 25, enter -0-.
This is your taxable income. 2728 Tax, including any alternative minimum tax (see instructions). 2829 Excess advance premium tax credit repayment. Attach
Form 8962. 2930 Add lines 28 and 29. 3031 Credit for child and dependent care expenses. Attach
Form 2441. 3132 Credit for the elderly or the disabled. Attach
Schedule R. 3233 Education credits from Form 8863, line 19. 3334 Retirement savings contributions credit. Attach Form 8880. 3435 Child tax credit. Attach Schedule 8812, if required. 3536 Add lines 31 through 35. These are your total credits. 3637 Subtract line 36 from line 30. If line 36 is more than line 30, enter -0-. 3738 Health care: individual responsibility (see instructions). Full-year coverage 3839 Add line 37 and line 38. This is your total tax. 3940 Federal income tax withheld from Forms W-2 and 1099. 4041 2015 estimated tax payments and amount applied
from 2014 return. 41If you have a qualifying child, attach Schedule EIC.
42a Earned income credit (EIC). 42ab Nontaxable combat pay election. 42b
43 Additional child tax credit. Attach Schedule 8812. 4344 American opportunity credit from Form 8863, line 8. 4445 Net premium tax credit. Attach Form 8962. 4546 Add lines 40, 41, 42a, 43, 44, and 45. These are your total payments. 46
Refund Direct deposit? See instructions and fill in 48b, 48c, and 48d or Form 8888.
47 If line 46 is more than line 39, subtract line 39 from line 46. This is the amount you overpaid. 47
48a Amount of line 47 you want refunded to you. If Form 8888 is attached, check here 48a
b Routing number
c Type: Checking Savings
d Account number
49 Amount of line 47 you want applied to your 2016 estimated tax. 49
Amount you owe
50 Amount you owe. Subtract line 46 from line 39. For details on how to pay, see instructions. 50
51 Estimated tax penalty (see instructions). 51
Third party
designee
Do you want to allow another person to discuss this return with the IRS (see instructions)? Yes. Complete the following. No
Designee’s name
Phone no.
Personal identification number (PIN)
Sign here Joint return? See instructions. Keep a copy for your records.
Under penalties of perjury, I declare that I have examined this return and accompanying schedules and statements, and to the best of my knowledge and belief, they are true, correct, and accurately list all amounts and sources of income I received during the tax year. Declaration of preparer (other than the taxpayer) is based on all information of which the preparer has any knowledge.
Your signature Date Your occupation Daytime phone number
Spouse’s signature. If a joint return, both must sign. Date Spouse’s occupation If the IRS sent you an Identity Protection PIN, enter it here (see inst.)
Paid
preparer
use only
Print/type preparer's name Preparer’s signature DateCheck if self-employed
PTIN
Firm's name
Firm's address
Firm's EIN
Phone no.
Form 1040A (2015)
MASS 666-00-7210
23860XX 2
15100 8760 8000
760 76
76
76X
76 1200 FORM 1099
1200
1124 1124
X X X X X X X X X
X X X X X X X X X X X X X X X X X
RETIRED 978-251-3131
RETIRED
10/14/2016
10/14/2016
10/14/2016IRS PREPARER S12345678
PRACTICE LAB15 PRACTICE LAB WAY WASHINGTON DC 20005 202-202-2022
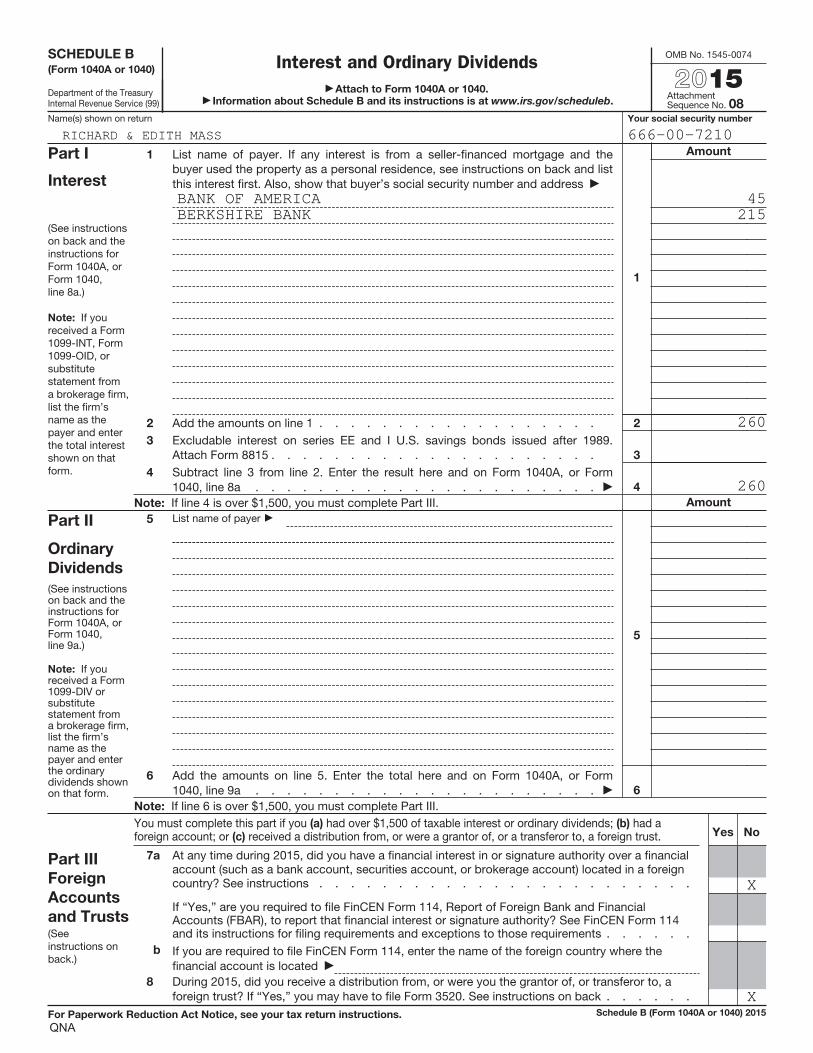
SCHEDULE B (Form 1040A or 1040)
Department of the Treasury Internal Revenue Service (99)
Interest and Ordinary Dividends Attach to Form 1040A or 1040.
Information about Schedule B and its instructions is at www.irs.gov/scheduleb.
OMB No. 1545-0074
2015Attachment Sequence No. 08
Name(s) shown on return Your social security number
Part I
Interest
(See instructions on back and the instructions for Form 1040A, or Form 1040, line 8a.)
Note: If you received a Form 1099-INT, Form 1099-OID, or substitute statement from a brokerage firm, list the firm’s name as the payer and enter the total interest shown on that form.
1 List name of payer. If any interest is from a seller-financed mortgage and the buyer used the property as a personal residence, see instructions on back and list this interest first. Also, show that buyer’s social security number and address
1
Amount
2 Add the amounts on line 1 . . . . . . . . . . . . . . . . . . 2
3 Excludable interest on series EE and I U.S. savings bonds issued after 1989. Attach Form 8815 . . . . . . . . . . . . . . . . . . . . . 3
4 Subtract line 3 from line 2. Enter the result here and on Form 1040A, or Form 1040, line 8a . . . . . . . . . . . . . . . . . . . . . . 4
Note: If line 4 is over $1,500, you must complete Part III. Amount
Part II
Ordinary
Dividends
(See instructions on back and the instructions for Form 1040A, or Form 1040, line 9a.)
Note: If you received a Form 1099-DIV or substitute statement from a brokerage firm, list the firm’s name as the payer and enter the ordinary dividends shown on that form.
5 List name of payer
5
6 Add the amounts on line 5. Enter the total here and on Form 1040A, or Form 1040, line 9a . . . . . . . . . . . . . . . . . . . . . . 6
Note: If line 6 is over $1,500, you must complete Part III.
Part III
Foreign
Accounts
and Trusts (See instructions on back.)
You must complete this part if you (a) had over $1,500 of taxable interest or ordinary dividends; (b) had a foreign account; or (c) received a distribution from, or were a grantor of, or a transferor to, a foreign trust. Yes No
7a At any time during 2015, did you have a financial interest in or signature authority over a financial account (such as a bank account, securities account, or brokerage account) located in a foreign country? See instructions . . . . . . . . . . . . . . . . . . . . . . . .
If “Yes,” are you required to file FinCEN Form 114, Report of Foreign Bank and Financial Accounts (FBAR), to report that financial interest or signature authority? See FinCEN Form 114 and its instructions for filing requirements and exceptions to those requirements . . . . . .
b If you are required to file FinCEN Form 114, enter the name of the foreign country where the financial account is located
8 During 2015, did you receive a distribution from, or were you the grantor of, or transferor to, a foreign trust? If “Yes,” you may have to file Form 3520. See instructions on back . . . . . .
For Paperwork Reduction Act Notice, see your tax return instructions. Schedule B (Form 1040A or 1040) 2015
QNA
RICHARD & EDITH MASS 666-00-7210
BANK OF AMERICA 45BERKSHIRE BANK 215
260
260
X
X

Apt. no.State Election Campaign Fund: $1 You $1 Spouse TOTAL 3Fill in if veteran of U.S. armed forces who served in Operation Enduring Freedom, Iraqi Freedom or Noble Eagle 3 You 3 SpouseTaxpayer deceased 3 You SpouseFill in if under age 18 3 You 3 Spouse
3 Name/address changed since 2014Federal adjusted gross income 3 3 Fill in if noncustodial parent
1. Filing status (select one only): 3 Single 3 Fill in if filing Schedule TDSMarried filing jointlyMarried filing separate returnHead of household 3 You are a custodial parent who has released claim to exemption for child(ren)
2. Exemptionsa. Personal exemptions 2ab. Number of dependents. (Do not include yourself or your spouse.) Enter number 3 × $1,000 = 2bc. Age 65 or over before 2016 You + Spouse = 3 × $700 = 2cd. Blindness You + Spouse = 3 × $2,200 = 2de. 1. Medical/dental 3 2. Adoption 3 1 + 2 = 2ef. Total exemptions. Add lines 2a through 2e. Enter here and on line 18 3 2f
3. Wages, salaries, tips 3 34. Taxable pensions and annuities 3 45. Mass. bank interest: a. 3 – b. exemption = 56. Business/profession or farm income or loss 3 67. Rental, royalty and REMIC, partnership, S corp., trust income/loss 3 7
8a. Unemployment 3 8a8b. Mass. lottery winnings 3 8b
9. Other income from Schedule X, line 5 3 910. TOTAL 5.15% INCOME 10
SIGN HERE. Under penalties of perjury, I declare that to the best of my knowledge and belief this return and enclosures are true, correct and complete.Your signature Date Spouse’s signature Date
May the Department of Revenue discuss this return with the preparer shown here? 3 YesI do not want preparer to file my return electronically 3 (this may delay your refund)Print paid preparer’s name Date Check if self-employed Paid preparer’s SSN
3
Paid preparer’s signature Paid preparer’s phone Paid preparer’s EIN3
PRIVACY ACT NOTICE AVAILABLE UPON REQUEST
2015 Form 1Massachusetts Resident Income Tax ReturnFOR FULL YEAR RESIDENTS ONLY
For the year January 1–December 31, 2014 or other taxable
Year beginning Ending
MA1500111038
RICHARD D MASS 666007210EDITH M MASS 24400721015 MAIN ST CHELMSFORD MA 01824-
23860
X
8800
X X 2 1400
10200 10320
195 200
7500 17820
10142016 10142016
IRS PREPARER 10142016 S12345678
202-202-2022
10/14/2016 09:45:24 AM

2015 Form 1, pg. 2Massachusetts Resident Income Tax Return
11a. Amount paid to Soc. Sec. Medicare, R.R., U.S. or Mass. Retirement 3 11a11b. Amount your spouse paid to Soc. Sec., Medicare, R.R., U.S. or Mass. Retirement 3 11b
12. Child under age 13, or disabled dependent/spouse care expenses 3 1213. Number of dependent member(s) of household under age 12, or dependents age 65 or over (not you or your spouse) as of
12/31/15, or disabled dependent(s)Not more than two. a. 3 × $3,600 =3 13
14. Rental deduction. a. 3 ÷ 2 =3 1415. Other deductions from Schedule Y, line 18 3 1516. Total deductions. Add lines 11 through 15 3 1617. 5.15% INCOME AFTER DEDUCTIONS. Subtract line 16 from line 10. Not less than “0” 1718. Exemption amount 1819. 5.15% INCOME AFTER EXEMPTIONS. Subtract line 18 from line 17. Not less than “0” 1920. INTEREST AND DIVIDEND INCOME 3 2021. TOTAL TAXABLE 5.15% INCOME. Add lines 19 and 20 2122. TAX ON 5.15% INCOME. Note: If choosing the optional 5.85% tax rate, fill in and multiply line 21 and the
amount in Schedule D, line 21 by .0585 3 2223. 12% INCOME. Not less than “0.” a. 3 × .12 = 2324. TAX ON LONG-TERM CAPITAL GAINS. Not less than “0.” Fill in if filing Schedule D-IS 3 3 24
Fill in if any excess exemptions were used in calculating lines 20, 23 or 24 3
25. Credit recapture amount 3 BC EOA LIH HR 3 2526. Additional tax on installment sale 3 2627. If you qualify for No Tax Status, fill in and enter “0” on line 28 3
28. TOTAL INCOME TAX. Add lines 22 through 26 2829. Limited Income Credit 3 2930. Other credits from Schedule Z, line 15 3 3031. INCOME TAX AFTER CREDITS. Subtract the total of lines 29 and 30 from line 28. Not less than “0” 31
BE SURE TO INCLUDE THIS PAGE WITH FORM 1, PAGE 1
MA1500121038
666007210
670
670 17150 10200 6950
6950
357
357 195
162
10/14/2016 09:45:24 AM

2015 Form 1, pg. 3Massachusetts Resident Income Tax Return
32. Voluntary Contributionsa. Endangered Wildlife Conservation 3 32ab. Organ Transplant Fund 3 32bc. Massachusetts AIDS Fund 3 32cd. Massachusetts U.S. Olympic Fund 3 32de. Massachusetts Military Family Relief Fund 3 32ef. Homeless Animal Prevention and Care 3 32fTotal. Add lines 32a through 32f 32
33. Use tax due on Internet, mail order and other out-of-state purchases 3 3334. Health care penalty a. You 3 + b. Spouse 3 – c. Fed. health care penalty 3 3435. INCOME TAX AFTER CREDITS PLUS CONTRIBUTIONS AND USE TAX. Add lines 31 through 34 3536. Massachusetts income tax withheld 3 3637. 2014 overpayment applied to your 2015 estimated tax 3 3738. 2015 Massachusetts estimated tax payments 3 3839. Payments made with extension 3 3940. Earned Income Credit. a. Number of qualifying children 3 Amount from U.S. return 3 × .15 = 3 4041. Senior Circuit Breaker Credit 3 4142. Other Refundable Credits 3 4243. TOTAL. Add lines 36 through 42 4344. Overpayment. Subtract line 35 from line 43 3 4445. Amount of overpayment you want applied to your 2016 estimated tax 3 4546. Refund. Subtract line 45 from line 44. Mail to: Massachusetts DOR, PO Box 7001, Boston, MA 02204 3 46
Direct deposit of refund. Type of account 3 checkingsavings
RTN # 3 account # 3
47. Tax due. Pay online at www.mass.gov/dor/payonline. Mail to: Mass. DOR, PO Box 7002, Boston, MA 02204 3 47Interest 3 Penalty 3 M-2210 amt. 3 3 EX enclose
Form M-2210
BE SURE TO INCLUDE THIS PAGE WITH FORM 1, PAGE 1
MA1500131038
666007210
162 350
1070
1420 1258
1258
10/14/2016 09:45:24 AM

FOR YOUR RECORDS ONLYMassachusetts AGI Worksheet
Form 1, Line 27 Massachusetts AGI Worksheet. No Tax Status (Only if Single, Head of Household or Married Filing Jointly.)
1. Enter your total 5.2% income form Form 1, line 10. Not less then "0". (Add back any Abandoned Building
Renovation deduction claimed on Schedule(s) C and/or E before entering an amount in line 1.).......... 1.
2. Add Schedule Y, line 1-10............................................ 2.
3. Subtract line 2 from line 1. Not less than “0”................................... 3.
4. Enter total Massachusetts bank interest or the interest exemption amount, whichever is smaller,
from Form 1, line 5a or line 5b.......................................... 4.
Note: If Form 1, line 10 is a loss, combine Form 1, line 10 with the amaller amount of total Massachusetts bank interest or
the interest exemption amount. Enter the result in line 4, unless the result is a loss. If the result is a loss, enter "0".
5. Enter amount from Schedule B, line 35. If there is no entry in Schedule B, line 35 or if
not filing Schedule B, enter the amount from Form 1, line 20 ........................... 5.
6. Enter the amount from Schedule D, line 19. Not less than "0". (If filing Schedule D-IS, Installment Sales, see
the Schedule D-IS instructions, available at www.mass.gov/dor, for the amount to enter in line 6.)......... 6.
7. Add lines 3 through 6 .............................................. 7.
1038
������������
������������
������������
������������
������������
������������
������������
666007210RICHARD D MASS
17820
17820
195
18015

1a. Date of birth 3 1b. Spouse’s date of birth 3 1c. Family size 3
2. Federal adjusted gross income 3 2
3. Indicate the time period that you were enrolled in a Minimum Creditable Coverage (MCC) health insurance plan(s). The Form MA 1099-HC from your insurerwill indicate whether your insurance met MCC requirements. Note: MassHealth, Commonwealth Care, Medicare, and health coverage for U.S. Military,including Veterans Administration and Tri-Care, meet the MCC requirements. If you did not receive a Form MA 1099-HC from your insurer, or you hadinsurance that did not meet MCC requirements, see the special section on MCC requirements in the instructions.
See instructions if, during 2015, you turned 18, you 3 3a You: Full-year MCC Part-year MCC No MCC/Nonewere a part-year resident or a taxpayer was deceased. 3 3b Spouse: Full-year MCC Part-year MCC No MCC/NoneIf you filled in the full-year or part-year MCC oval, go to line 4. If you filled in No MCC/None, go to line 6.
4. Indicate the health insurance plan(s) that met the Minimum Creditable Coverage (MCC) requirements in which you were enrolled in 2015, as shown on Form MA 1099-HC (check all that apply). If you did not receive this form, fill in line(s) 4f and/or 4g and see instructions. Fill in if you were enrolled in private insurance and MassHealth or Commonwealth Care and enter your private insurance information in line(s) 4f and/or 4g and goto line 5.4a. Private insurance, including ConnectorCare (completes line(s) 4f and/or 4g below) You Spouse4b. MassHealth or Commonwealth Care. Fill in and go to line 5 You Spouse4c. Medicare (including a replacement or supplemental plan). Fill in and go to line 5 You Spouse4d. U.S. Military (including Veterans Administration and Tri-Care). Fill in and go to line 5 You Spouse4e. Other government program (enter the program name(s) only in lines 4f and/or 4g below). Note: Health Safety Net You Spouseis not considered insurance or minimum creditable coverage.
4f. Your Health Insurance. Complete if you answered line(s) 4a or 4e and go to line 5. Fill in if you were not issued Form MA 1099-HC.
4g. Spouse’s Health Insurance. Complete if you answered line(s) 4a or 4e and go to line 5. Fill in if you were not issued Form MA 1099-HC.
5. If you had health insurance that met MCC requirements for the full-year, including private insurance, MassHealth, Commonwealth Care or ConnectorCare,you are not subject to a penalty. Skip the remainder of this schedule and continue completing your tax return. Other wise, go to line 6.
If you had Medicare (including a replacement or supplemental plan), U.S. Military (including Veterans Administration and Tri-Care), or other governmentinsurance at any point during 2015, you are not subject to a penalty. Skip the remainder of this schedule and continue completing your tax return. Other -wise, go to line 6.
2015 Schedule HC
Schedule HC, Health Care Information, must be completed by allfull-year residents and certain part-year residents (see instructions).Note: Schedule HC must be enclosed with your Form 1 or Form1-NR/PY. Failure to do so will delay the processing of your return.
MA1502911038
RICHARD D MASS 666007210
07011949 07041950 2
23860
XX
X X
BCBS 96-0000001 98765431
BCBS 96-0000001 98765432
10/14/2016 09:45:24 AM

2015 Schedule HC, pg. 2
Uninsured for All or Part of 20156. Was your income in 2015 at or below 150% of the federal poverty level? 3 6 Yes No
If you answer Yes, you are not subject to a penalty in 2015. Skip the remainder of this schedule and complete your tax return. If you answer No and you were enrolledin a health insurance plan that met the MCC requirements for part, but not all, of 2015, go to line 7. If you answer No and you had no insurance or you were enrolled ina plan that did not meet the MCC requirements during the period that the mandate applied, go to line 8a.
7. Complete this section only if you, and/or your spouse if married filing jointly, were enrolled in a health insurance plan(s) that met the Minimum CreditableCoverage (MCC) requirements for part, but not all of 2015. Fill in below the months that met the MCC requirements, as shown on Form MA 1099-HC. If youdid not receive this form, fill in the months you were covered by a plan that met the MCC requirements at least 15 days or more. If, during 2015, you turned18, you were a part-year resident or a taxpayer was deceased, fill in the oval(s) below for the month(s) that met the MCC requirements during the periodthat the mandate applied. See instructions.You may only fill in the month(s) you had health insurance that met MCC requirements. If you had health insurance, but it did not meet MCC requirements,you must skip this section and go to line 8a.
Months Covered By Health InsuranceYou Jan. Feb. March April May June July Aug. Sept. Oct. Nov. Dec.Spouse Jan. Feb. March April May June July Aug. Sept. Oct. Nov. Dec.
If you had four or more consecutive months either with no insurance or insurance that did not meet the MCC requirements (four or more blank months in a row),go to line 8a. Otherwise, a penalty does not apply to you in 2015. Skip the remainder of this schedule and complete your tax return.
Religious Exemption and Certificate of Exemption8a. Religious exemption: Are you claiming an exemption from the requirement to purchase health insurance based 3 8a You Yes No
on your sincerely held religious beliefs that cause you to object to substantially all forms of treatment covered by health insurance? Spouse Yes No
If you answer Yes, go to line 8b. If you answer No, go to line 9.8b. If you are claiming a religious exemption in line 8a, did you receive medical health care during the 2015 tax year? 3 8b You Yes No
Spouse Yes NoIf you answer No to line 8b, skip the remainder of this schedule and continue completing your tax return. If you answer Yes to line 8b, go to line 9.
9. Certificate of exemption: Have you obtained a Certificate of Exemption issued by the Massachusetts Health 3 9 You Yes NoConnector for the 2015 tax year? Spouse Yes No
If you answer Yes, enter the certificate number, skip the remainder of this schedule and continue completing your taxreturn. If you answer No to line 9, go to line 10.
MA1502921038666007210
10/14/2016 09:45:24 AM

2015 Schedule HC, pg. 3
Affordability as Determined By State GuidelinesNote: This section will require the use of worksheets and tables found in the instructions. You must complete the worksheet(s) to determine if health insurance wasaffordable to you during the 2015 tax year.
10. Did your employer offer affordable health insurance that met minimum creditable coverage requirements 3 10 You Yes Noas determined by completing the Schedule HC Worksheet for Line 10 in the instructions? Spouse Yes No
Fill in No if your employer did not offer health insurance that met minimum creditable coverage requirements, you were not eligible for health insurance offered byyour employer, you were self-employed or you were unemployed.
11. Were you eligible for government-subsidized health insurance as determined by completing the Schedule HC 3 11 You Yes NoWorksheet for Line 11 in the instructions? Spouse Yes No
If you answer No, go to line 12. If you answer Yes, go to the Health Care Penalty Worksheet in the instructions to calculate your penalty amount.12. Were you able to purchase affordable private health insurance that met minimum creditable coverage requirements 3 12 You Yes No
as determined by completing the Schedule HC Worksheet for Line 12 in the instructions? Spouse Yes NoIf you answer No, you are not subject to a penalty. Continue completing your tax return. If you answer Yes, go to the Health Care Penalty Worksheet in theinstructions to calculate your penalty amount.
Complete Only If You Are Filing An AppealYou must complete the Health Care Penalty Worksheet to determine your penalty amount before completing this section.You may have grounds to appeal if you were unable to obtain affordable insurance that meets the minimum creditable coverage requirements in 2015 due to ahardship or other circumstances. The grounds for appeal are explained in more detail in the instructions. If you believe you have grounds for appealing the penalty,fill in the field(s) below. The appeal will be heard by the Massachusetts Health Connector. By filling in the field below, you (or your spouse if married filing jointly) areauthorizing DOR to share information from your tax return, including this schedule, with the Massachusetts Health Connector for purposes of deciding your appeal.You will receive a follow-up letter asking you to state your grounds for appeal in writing, and submit supporting documentation. Failure to respond to thatletter within the time specified in the letter will lead to dismissal of your appeal and will result in a future assessment of a penalty. Once your documenta tionis received, it will be reviewed by the Massachusetts Health Connector and you may be required to attend a hearing on your case. You will be required to file yourclaims under the pains and penalties of perjury.Note: If you are filing an appeal, make sure you have calculated the penalty amount that you are appealing, but do not assess yourself or enter a penalty amounton your Form 1 or Form 1-NR/PY. Also, do not include any hardship documentation with your original return. You will be required to submit substantiating hardshipdocumentation at a later date during the appeal process.
You I wish to appeal the penalty. I authorize DOR to share this tax return including this schedule with the Massachusetts Health Connectorfor purposes of deciding this appeal.
Spouse I wish to appeal the penalty. I authorize DOR to share this tax return including this schedule with the Massachusetts Health Connectorfor purposes of deciding this appeal.
MA1502931038
RICHARD D MASS 666007210
10/14/2016 09:45:24 AM
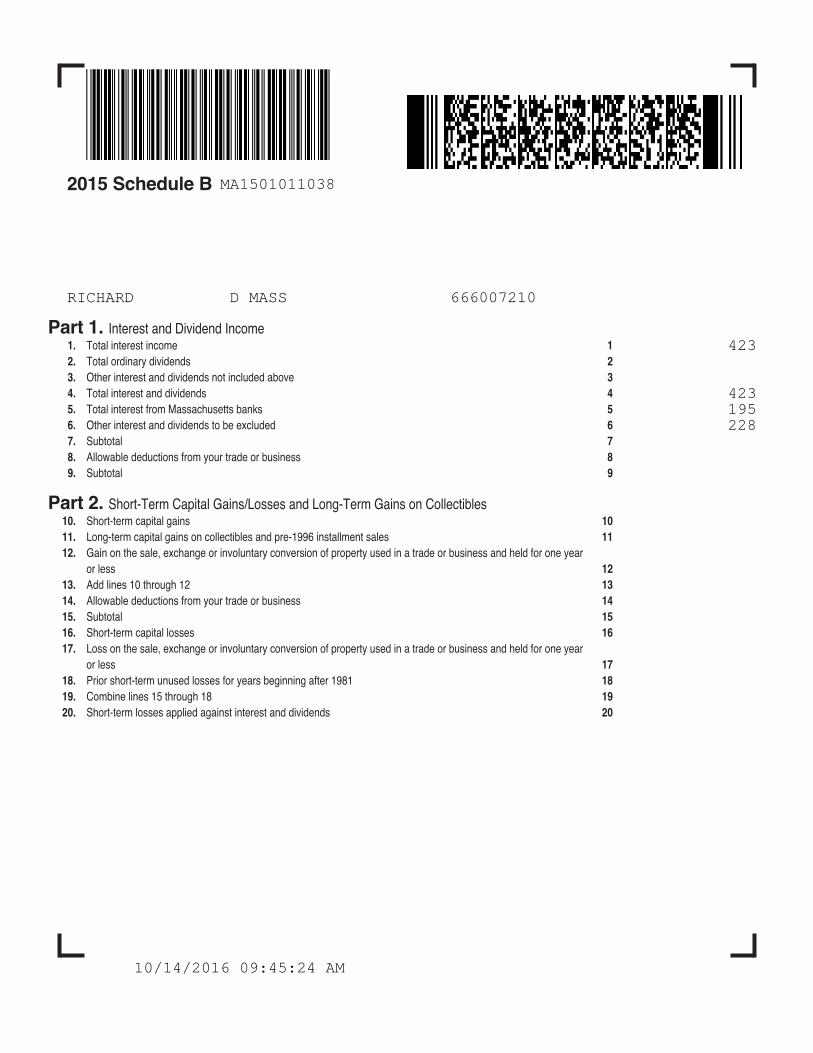
2015 Schedule B
Part 1. Interest and Dividend Income1. Total interest income 12. Total ordinary dividends 23. Other interest and dividends not included above 34. Total interest and dividends 45. Total interest from Massachusetts banks 56. Other interest and dividends to be excluded 67. Subtotal 78. Allowable deductions from your trade or business 89. Subtotal 9
Part 2. Short-Term Capital Gains/Losses and Long-Term Gains on Collectibles10. Short-term capital gains 1011. Long-term capital gains on collectibles and pre-1996 installment sales 1112. Gain on the sale, exchange or involuntary conversion of property used in a trade or business and held for one year
or less 1213. Add lines 10 through 12 1314. Allowable deductions from your trade or business 1415. Subtotal 1516. Short-term capital losses 1617. Loss on the sale, exchange or involuntary conversion of property used in a trade or business and held for one year
or less 1718. Prior short-term unused losses for years beginning after 1981 1819. Combine lines 15 through 18 1920. Short-term losses applied against interest and dividends 20
MA1501011038
RICHARD D MASS 666007210
423
423 195 228
10/14/2016 09:45:24 AM

2015 Schedule B, pg. 2
21. Available short-term losses 2122. Short-term losses applied against long-term gains 2223. Short-term losses available for carryover in 2016 2324. Short-term gains and long-term gains on collectibles 2425. Long-term losses applied against short-term gain 2526. Subtotal 2627. Long-term gains deduction 2728. Short-term gains after long-term gains deduction 28
Part 3. Adjusted Gross Interest, Dividends, Short-Term Capital Gains and Long-Term Gains on Collectibles29. Enter the amount from line 9 2930. Short-term losses applied against interest and dividends 3031. Subtotal interest and dividends 3132. Long-term losses applied against interest and dividends 3233. Adjusted interest and dividends 3334. Enter the amount from line 28 34
Part 4. Taxable Interest, Dividends and Certain Capital Gains35. Adjusted gross interest, dividends and certain capital gains 3 3536. Excess exemptions 3637. Subtract line 36 from line 35 3738. Interest and dividends taxable at 5.15% 3 3839. Taxable 12% capital gains 3 3940. Available short-term losses for carryover in 2016 40
MA1501021038666007210
10/14/2016 09:45:24 AM

2015 Schedule CBCircuit Breaker Credit
ADDRESS OF PRINCIPAL RESIDENCE IN MASSACHUSETTS (DO NOT ENTER PO BOX) CITY/TOWN STATE ZIP + 4
1. Living quarters status during 2015: 3 Homeowner Multi-use or multi-family property Yes NoRenter
2. Homeowners only, enter assessed value of principal residence as of January 1, 2015 3 2
Income Calculation3. Massachusetts adjusted gross income 34. Total Social Security benefits 45. Pensions/annuities/IRA/Keogh distributions not taxed on your Massachusetts tax return 56. Miscellaneous income, including cash public assistance 67. Massachusetts total income. Add lines 3 through 6 3 78. Exemptions from income. From Form 1, lines 2b through 2d or Form 1-NR/PY, lines 4b through 4d 89. Qualifying income. Subtract line 8 from line 7 3 9
Credit CalculationIf you filled in “Homeowner” in line 1, complete lines 10–17; if “Renter,” skip to line 18
10. Real estate taxes paid in calendar year 2015 for your principal residence. See instructions 1011. Adjustments to real estate taxes 1112. Subtract line 11 from line 10 1213. Enter 50% (.50) of water and sewer use charges paid in 2015 1314. Add lines 12 and 13 1415. Income threshold. Multiply line 9 by 10% (.10) 1516. Subtract line 15 from line 14. If “0” or less, you do not qualify for this credit 1617. Enter the lesser of line 16 or $1,070 here and on Form 1, line 41 or Form 1-NR/PY, line 46 3 17
If you filled in “Renter” in line 1, complete lines 18–2118. Enter total amount of rent paid for your principal residence in 2015: a. ÷ 4 = 18
Landlord’s name and address19. Income threshold. Multiply line 9 by 10% (.10) 19
20. Subtract line 19 from line 18. If “0” or less, you do not qualify for this credit 2021. Enter the lesser of line 20 or $1,070 here and on Form 1, line 41 or Form 1-NR/PY, line 46 3 21
MA1502611038
RICHARD D MASS 666007210
15 MAIN ST CHELMSFORD MA 01824X X
32500
18243
6300
24543 1400 23143
5500
5500 300 5800 2314 3486
1070
10/14/2016 09:45:24 AM

2015 Schedule X & Y
Schedule X. Other Income1. Alimony received 3 12. Taxable IRA/Keogh and Roth IRA conversion distributions 3 23. Other gambling winnings. Not less than “0.” Certain gambling losses are deductible under Massachusetts law 3 34. Fees and other 5.15% income. Not less than “0” 3 45. Total other 5.15% income. Add lines 1 through 4. Not less than “0” 3 5
Schedule Y. Other Deductions1. Allowable employee business expenses 3 12. Penalty on early savings withdrawal 3 23. Alimony paid 3 34. Amounts excludible under MGL Ch. 41, sec. 111F or U.S. tax treaty incl. in Form 1, line 3 or Form 1-NR/PY, line 5 3 4
Income received by a firefighter or police officer incapacitated in the line of duty, per MGL Ch. 41, sec. 111FIncome exempt under U.S. tax treaty
5. Moving expenses 3 56. Medical savings account deduction 3 67. Self-employed health insurance deduction 3 78. Health care accounts deduction 3 89. Certain qualified deductions from U.S. Form 1040
Certain business expenses from U.S. Form 1040 3 910. Student loan interest 3 1011. College Tuition Deduction 3 1112. Undergraduate student loan interest deduction 3 1213. Deductible amount of qualified contributory pension income from another state or political subdivision included
in Form 1, line 4 or Form 1-NR/PY, line 6 3 1314. Claim of right deduction 3 1415. Commuter deduction 3 1516. Human organ donation deduction (full-year residents only) 3 1617. Certain gambling losses 3 1718. Total other deductions. Add lines 1 through 17 3 18
MA15SXY11038
RICHARD D MASS 666007210
7500
7500
10/14/2016 09:45:24 AM

2015 Schedule INC
Form W-2 and 1099 InformationA. FEDERAL ID NUMBER B. STATE TAX WITHHELD C. STATE WAGES/INCOME D. TAXPAYER SS WITHHELD E. SPOUSE SS WITHHELD F. SOURCE OF WITHHOLDING
TOTALS
MA15INC11038
666007210RICHARD D MASS
21-3333556 300 10320 W204-3276267 50 7500 1099R
350 17820
10/14/2016 09:45:24 AM