rheumatic fever and rheumatic heart disease: clinical profile of 550 cases in india
TRANSCRIPT

Archives of Medical Research 34 (2003) 382–387
ORIGINAL ARTICLE
Rheumatic Fever and Rheumatic Heart Disease: Clinical Profile of550 Cases in India*
M.S. Ravisha, Milind S. Tullu and Jaishree R. KamatDepartment of Pediatrics, Seth G.S. Medical College and KEM Hospital, Parel, Mumbai, Maharashtra, India
Received for publication February 7, 2003; accepted May 26, 2003 (03/010).
Background. The aims and objectives of this paper were to analyze the clinical presentationof children with rheumatic fever (RF) and rheumatic heart disease (RHD), to determine thecardiac sequel of RF and valvular affection due to RF, and to study clinical manifestations inrecurrences of RF.
Methods. Our study, a retrospective analysis, was conducted at a tertiary-care teachinghospital with specialty follow-up clinic for patients with RF/RHD. This retrospectivestudy was conducted to include a period of 31 years (from January 1971 through December2001). Pre-completed case protocols of patients with RF/RHD were analyzed to recordthe following information: demographic data; clinical features on admission/presentation;relevant investigations; recurrences; cardiac valvular affection, and outcome. ModifiedJones’ criteria were used for diagnosis of RF.
Results. The study included 550 patients. Mean age of presentation was 9.62 years andsex ratio was 1.15:1 favoring males. A total of 250 patients presented with initial/firstattack of RF. Arthritis and carditis were seen in 169 (67.6%) and 105 cases (42%),respectively. Chorea was seen in 47 cases (18.8%) and erythema marginatum, in four. Atotal of 224 patients presented with recurrence of RF (with pre-existing RHD). Arthritisand carditis were seen in 109 (48.66%) and 178 cases (79.46%), respectively, in thesepatients; 76 cases presented with chronic RHD. Mitral regurgitation was the most commoncardiac valvular lesion observed (150 cases) followed by a combination of mitral stenosis andmitral regurgitation (98 cases). Congestive cardiac failure was seen in 201 cases (36.54%)and infective endocarditis in 30 (5.45%). 2-D echocardiography and/or color Doppler wasperformed in 201 patients (36.54%). Average duration of follow-up was 3.19 years; 74.72%of cases were lost to follow-up. Benzathine penicillin prophylaxis was regular in42.18% cases. Positive family history of RF/RHD was present in 2% of cases. Twentythree patients (4.18%) died.
Conclusions. Arthritis was the most common manifestation in the initial attack of RF,while carditis was the most common manifestation in patients presenting with rheumaticrecurrences (with pre-existing RHD) and mitral regurgitation was the most commonvalvular lesion. Rate of patient dropout from penicillin prophylaxis was high. Clinicalmanifestations in initial/first attack of RF have not significantly changed in the last 31years. � 2003 IMSS. Published by Elsevier Inc.
Key Words: Arthritis, Carditis, Chorea, Color Doppler, Penicillin, Prophylaxis.
Address reprint requests to: Dr. Milind S. Tullu, ‘Sankalp Siddhi’,Block #1, Ground floor, Kher Nagar, Bandra (East), Mumbai, 400051,Maharashtra, India. Phone: (�91) (22) 2647-3974; E-mails: [email protected] and [email protected]
*This paper was originally used at a Poster Presentation at EMBICON2002 (Annual Conference of Mumbai and Navi-Mumbai Branches of theIndian Academy of Pediatrics) and a similar abstract was published inthe Proceedings of EMBICON 2002.
0188-4409/03 $–see front matter. Copyright � 2003 IMSS. Published by Elsedoi : 10.1016/S0188-4409(03)00072-9
Introduction
Rheumatic fever (RF) and rheumatic heart disease (RHD)are still prevalent in developing countries including India.There have been very few recent studies on clinical presen-tations of patients with RF/RHD. The clinical profile ofpatients presenting with RF in developing countries has been
vier Inc.

RF and RHD: Clinical Profile 383
Table 1. Characteristics of study group
Initial (first) attack of Recurrence of RF with Chronic RHD withoutRF (n � 250) RHD (n � 224) RF (n � 76) Total (n � 550)
Age 9.60 years (range, 3–20 years) 9.61 years (range, 4–16 years) 9.75 years (range, 6–12 years) 9.62 years (range, 3–20 years)Sex Males, 130 females, 120 Males, 126 females, 98 Males, 38 females, 38 Males, 294 females, 256Average duration 3.85 years (range, 0–19 years) 2.64 years (range, 0–18 years) 2.70 years (range, 0–22 years) 3.19 years (range, 0–22 years)
of follow-upLost to follow-up 182 (72.8%) 170 (75.89%) 59 (77.63%) 411 (74.72%)Regular prophylaxis 105 (42%) 98 (43.75%) 29 (38.15%) 232 (42.18%)
RF � rheumatic fever; RHD � rheumatic heart disease.
considered as different from profiles of patients with RFin developed countries (1). A previous study done at ourinstitution did not adequately differentiate the clinical fea-tures of initial attack of RF, recurrent attacks of RF, andchronic RHD (2). A prospective study at our Institutiondid address the issue of presenting features of RF and recur-rences of RF, but did not discuss the cardiac sequel of RF(3). Hence, the present study was planned to study clinicalpresentation of children with RF/RHD, valvular sequel ofRF, and clinical pattern of recurrences of RF. In addition,clinical features of RF/RHD were compared during twotime intervals within the study period. A comparison of ourfindings and those noted in previous studies was presentedin the Discussion section of this paper.
Patients and Methods
Case files of patients diagnosed as RF/RHD from January1971 through December 2001 were reviewed. Patients werediagnosed with RF if they fulfilled modified Jones’ criteria(4). The following information was recorded from case files-demographic data, clinical features at presentation, pasthistory of rheumatic fever, results of investigations (ESR,C-reactive protein, leukocytosis, anti-streptolysin O titer-ASLO, throat swab, and 2-D echocardiography or colorDoppler examination), duration of follow-up, and outcome.Presence of carditis was noted based on the combinationof the following findings: presence of valvulitis murmur;changing murmurs; pericardial rub; congestive cardiac fail-ure, and sleeping pulse rate �100/min. Results of 2-D echo-cardiography and/or color Doppler examination wererecorded. Cardiac valvular lesions were enlisted, and pres-ence of RF/RHD in other family members was recorded.Clinical features of recurrences of RF were noted.
Results
A total of 550 case files of patients diagnosed as having RF/RHD were analyzed retrospectively (total study period, 31years). Characteristics of the study group are presented inTable 1. The study group was analyzed in three distinct groups
depending on the following clinical features at admission:1) patients with initial or first attack of RF (250 cases); 2)patients with recurrence of RF (in those with underlying pre-existing RHD, 224 cases), and patients with chronic RHD(76 cases, including patients admitted for establishing a diag-nosis, or cardiac failure, or for infective endocarditistherapy).
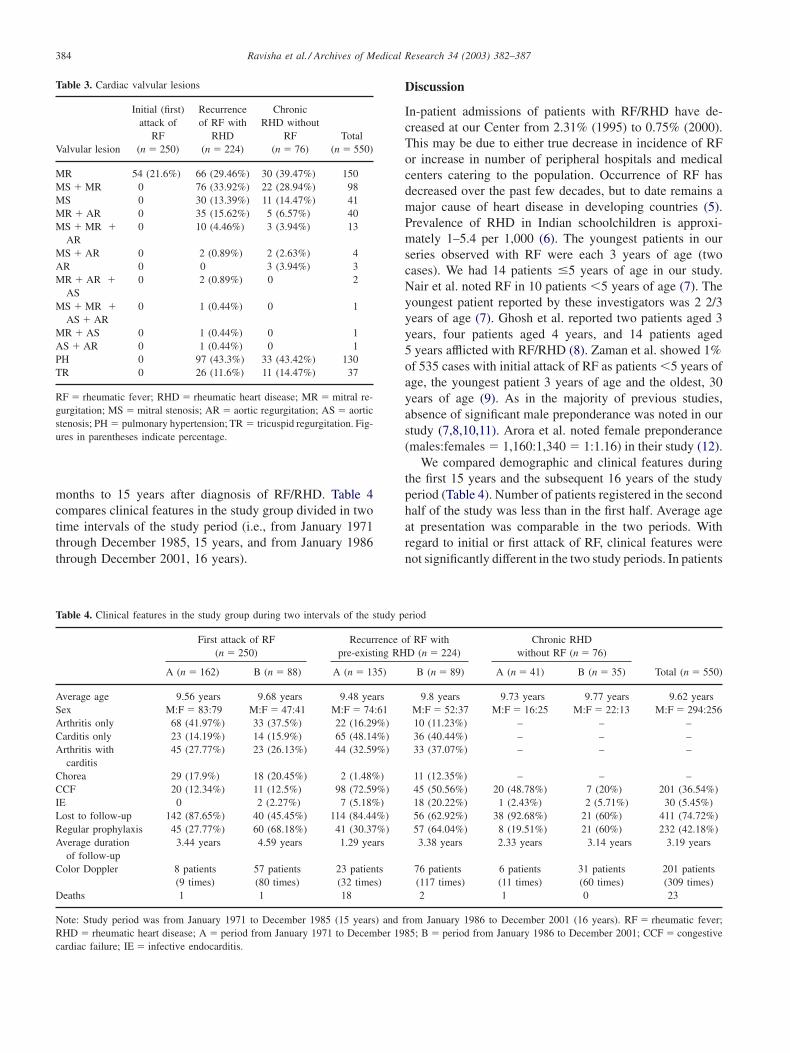
Clinical features of RF on admission to the hospital oninitial or first attack and recurrent attack (in patients withpre-existing RHD) are compared in Table 2. Cardiac valvularlesions observed are listed in Table 3. Initial mitral regurgita-tion disappeared in 32 patients over a period ranging from2 months to 9 years of follow-up, while new valvular lesionsappeared in 17 patients over a period ranging from 1 monthto 12 years. These included mitral stenosis (four cases),aortic regurgitation (five cases), mitral stenosis with mitralregurgitation (three cases), aortic regurgitation with mitralstenosis (three cases), and mitral regurgitation (two cases).A total of 127 episodes of recurrences were observed in 107patients (19.45%) during the study. Clinical manifestationsin observed recurrences of RF included arthritis in 31(24.4%), carditis in 46 (36.22%), and arthritis with carditisin 35 (27.55%). Family history of RF/RHD was present in11 patients (2%). Twenty three patients (4.18%) died 2
Table 2. Clinical features of RF in initial attack and recurrent attack(with pre-existing RHD)
Initial (first) attack Recurrent attackFeature of RF (n � 250) of RF (n � 224)
Arthritis only 101 (40.4%) 32 (14.28%)Carditis only 37 (14.8%) 101 (45.08%)Both arthritis and carditis 68 (27.2%) 77 (34.37%)Chorea 47 (18.8%) 13 (5.8%)Subcutaneous nodules 3 (1.2) 3 (1.33%)CCF 31 (12.4%) 143 (63.83%)Infective endocarditis 2 (0.8%) 25 (11.16%)Color Dopplera 65a (89 times) 99a (149 times)
RF � rheumatic fever; RHD � rheumatic heart disease; CCF � congestivecardiac failure. a� number of patients on whom 2-D echocardiographyand/or color Doppler was performed (with figure in parentheses indicatingnumber of times the study was performed). Erythema marginatum wasseen in four cases (all in initial attack of RF).
Ravisha et al. / Archives of Medical Research 34 (2003) 382–387384
Table 3. Cardiac valvular lesions
Initial (first) Recurrence Chronicattack of of RF with RHD without
RF RHD RF TotalValvular lesion (n � 250) (n � 224) (n � 76) (n � 550)
MR 54 (21.6%) 66 (29.46%) 30 (39.47%) 150MS � MR 0 76 (33.92%) 22 (28.94%) 98MS 0 30 (13.39%) 11 (14.47%) 41MR � AR 0 35 (15.62%) 5 (6.57%) 40MS � MR � 0 10 (4.46%) 3 (3.94%) 13
ARMS � AR 0 2 (0.89%) 2 (2.63%) 4AR 0 0 3 (3.94%) 3MR � AR � 0 2 (0.89%) 0 2
ASMS � MR � 0 1 (0.44%) 0 1
AS � ARMR � AS 0 1 (0.44%) 0 1AS � AR 0 1 (0.44%) 0 1PH 0 97 (43.3%) 33 (43.42%) 130TR 0 26 (11.6%) 11 (14.47%) 37
RF � rheumatic fever; RHD � rheumatic heart disease; MR � mitral re-gurgitation; MS � mitral stenosis; AR � aortic regurgitation; AS � aorticstenosis; PH � pulmonary hypertension; TR � tricuspid regurgitation. Fig-ures in parentheses indicate percentage.
months to 15 years after diagnosis of RF/RHD. Table 4compares clinical features in the study group divided in twotime intervals of the study period (i.e., from January 1971through December 1985, 15 years, and from January 1986through December 2001, 16 years).
Discussion
In-patient admissions of patients with RF/RHD have de-creased at our Center from 2.31% (1995) to 0.75% (2000).This may be due to either true decrease in incidence of RFor increase in number of peripheral hospitals and medicalcenters catering to the population. Occurrence of RF hasdecreased over the past few decades, but to date remains amajor cause of heart disease in developing countries (5).Prevalence of RHD in Indian schoolchildren is approxi-mately 1–5.4 per 1,000 (6). The youngest patients in ourseries observed with RF were each 3 years of age (twocases). We had 14 patients �5 years of age in our study.Nair et al. noted RF in 10 patients �5 years of age (7). Theyoungest patient reported by these investigators was 2 2/3years of age (7). Ghosh et al. reported two patients aged 3years, four patients aged 4 years, and 14 patients aged5 years afflicted with RF/RHD (8). Zaman et al. showed 1%of 535 cases with initial attack of RF as patients �5 years ofage, the youngest patient 3 years of age and the oldest, 30years of age (9). As in the majority of previous studies,absence of significant male preponderance was noted in ourstudy (7,8,10,11). Arora et al. noted female preponderance(males:females � 1,160:1,340 � 1:1.16) in their study (12).
We compared demographic and clinical features duringthe first 15 years and the subsequent 16 years of the studyperiod (Table 4). Number of patients registered in the secondhalf of the study was less than in the first half. Average ageat presentation was comparable in the two periods. Withregard to initial or first attack of RF, clinical features werenot significantly different in the two study periods. In patients
Table 4. Clinical features in the study group during two intervals of the study period
First attack of RF Recurrence of RF with Chronic RHD(n � 250) pre-existing RHD (n � 224) without RF (n � 76)
A (n � 162) B (n � 88) A (n � 135) B (n � 89) A (n � 41) B (n � 35) Total (n � 550)
Average age 9.56 years 9.68 years 9.48 years 9.8 years 9.73 years 9.77 years 9.62 yearsSex M:F � 83:79 M:F � 47:41 M:F � 74:61 M:F � 52:37 M:F � 16:25 M:F � 22:13 M:F � 294:256Arthritis only 68 (41.97%) 33 (37.5%) 22 (16.29%) 10 (11.23%) – – –Carditis only 23 (14.19%) 14 (15.9%) 65 (48.14%) 36 (40.44%) – – –Arthritis with 45 (27.77%) 23 (26.13%) 44 (32.59%) 33 (37.07%) – – –
carditisChorea 29 (17.9%) 18 (20.45%) 2 (1.48%) 11 (12.35%) – – –CCF 20 (12.34%) 11 (12.5%) 98 (72.59%) 45 (50.56%) 20 (48.78%) 7 (20%) 201 (36.54%)IE 0 2 (2.27%) 7 (5.18%) 18 (20.22%) 1 (2.43%) 2 (5.71%) 30 (5.45%)Lost to follow-up 142 (87.65%) 40 (45.45%) 114 (84.44%) 56 (62.92%) 38 (92.68%) 21 (60%) 411 (74.72%)Regular prophylaxis 45 (27.77%) 60 (68.18%) 41 (30.37%) 57 (64.04%) 8 (19.51%) 21 (60%) 232 (42.18%)Average duration 3.44 years 4.59 years 1.29 years 3.38 years 2.33 years 3.14 years 3.19 years
of follow-upColor Doppler 8 patients 57 patients 23 patients 76 patients 6 patients 31 patients 201 patients
(9 times) (80 times) (32 times) (117 times) (11 times) (60 times) (309 times)Deaths 1 1 18 2 1 0 23
Note: Study period was from January 1971 to December 1985 (15 years) and from January 1986 to December 2001 (16 years). RF � rheumatic fever;RHD � rheumatic heart disease; A � period from January 1971 to December 1985; B � period from January 1986 to December 2001; CCF � congestivecardiac failure; IE � infective endocarditis.

RF and RHD: Clinical Profile 385
with recurrence of RF (with pre-existing RHD), co-existenceof arthritis with carditis was observed more commonly inthe latter half as compared to the first half of the studyperiod. Benzathine penicillin prophylaxis was more regularin the latter half of the study. 2-D echocardiography and/or color Doppler were used more commonly (for evaluation ofpatients) in the second half of the study period (due to easyavailability of these investigations). Number of deaths wasalso lower in the second half of the study period. Thesedifferences may reflect better diagnostic and treatment facili-ties at our Institution during the latter half of the study period.
Table 5 summarizes the clinical presentation of patientswith initial attack of RF in various developing (includingthe present study) and developed countries. In the presentseries, �67% of cases with initial attack of RF had arthritis.This is a slightly lower incidence compared to previous stud-ies. Bitar et al. (17) recently showed a very high incidence ofcarditis and arthralgia/arthritis (�90% for both) in pediatricpatients with RF admitted to a tertiary-care hospital in Leba-non. Carditis was the most common manifestation in recur-rences of RF (in patients with pre-existing RHD who arrivedat the hospital with recurrences as well as in recurrencesobserved in the study group on follow-up in our study).Recurrences of RF were noted in patients not receivingregular benzathine penicillin prophylaxis. Erythema mar-ginatum has been rarely reported in Indian studies (1,8,10),with only four cases reported to date.
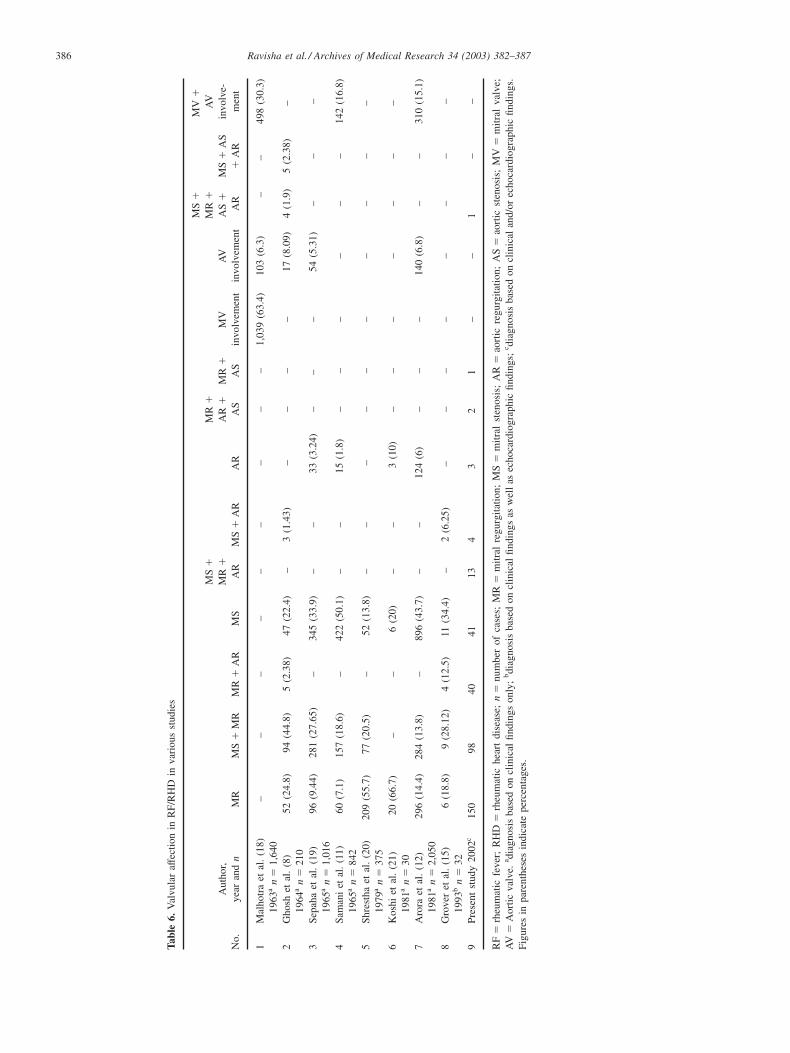
Mitral regurgitation followed by mitral stenosis withmitral regurgitation was the most common valvular lesionseen by our group. Valvular involvement in various previousstudies is presented in Table 6. Rheumatic mitral stenosiswas noticed as early as 5 years of age by Ghosh et al. (8). Wealso had five patients aged 5 years with mitral stenosis.Three had mitral regurgitation in addition to mitral steno-sis. Such early development of chronic RHD in children �5years of age contributed to high morbidity of RF/RHD indeveloping countries. Mitral regurgitation disappeared in 32
cases over a period ranging from 2 months to 9 years in ourstudy. Kassem et al. (22) showed disappearance of mitralregurgitation in 31 cases over a period ranging from 6 monthsto 14 years after initial attack; the investigators also reportedbetter compliance and fewer rheumatic recurrences in thisgroup of patients (22).
Follow-up rate and percentage of patients taking regularpenicillin prophylaxis was low in our study despite adequatecounseling. Although adequacy of counseling in the presentstudy has not been objectively evaluated, the low rate ofprophylaxis may be related to poor health awareness, resid-ing in remote villages far from tertiary-care health centers,and the low literacy rate in India. Good short-term prophy-laxis at the end of 3.5 years of surveillance was reportedby Koshi et al. (21). Kumar et al. (23) reported exceptionalcompliance of 92% over 12 years in patients with RF/RHD.It is possible that patients lost to follow-up in our study maybe receiving benzathine penicillin prophylaxis at their localdispensaries or from their family physicians.
Family history of RF/RHD was seen in 2% of patientsin our study, although �1% was reported by Arora et al.(12), and �4 and 5% reported by Nair et al. (7) and Bena-kappa et al. (10), respectively. Ghosh et al. (8) had positivefamily history of arthritis with fever in 12 of 404 cases(2.97%). Sanyal et al. had a sole patient with positive familyhistory (14). Of the 550 patients in our study, 76 (13.81%) hadchronic RHD while 224 cases (40.72%) arrived at the hospitalwith recurrence of RF in presence of pre-existing RHD,indicating that patients arrived late at tertiary-care centers.Death rate of 4.18% in our study was similar to 5.7% notedby Ghosh et al. (8). Deaths in the present study may beunderestimated due to suboptimal follow-up.
Limitations of a retrospective study applied to the presentstudy as well. All investigations, especially 2-D echocardio-graphic or color Doppler examination, were not possible inall cases, especially during the early years of the study
Table 5. Comparison of clinical manifestations of initial attack of RF in various studies
Arthritis and/or Carditis � Subcutaneous ErythemaNo. Author and year No. of cases Carditis (%) arthralgia (%) arthritis (%) Chorea (%) nodules (%) marginatum (%)
1 Bland et al.* (13)–1951a 1,000 65.3 81.1 – 51.8 8.8 –2 Ghosh et al. (8)–1964a 262 60 86 – 6 1 03 Sanyal et al. (14)–1974a 102 33.3 86.3 25.5 20.5 1.9 1.94 Benakappa et al. (10)–1978a 100 68 68 – 15 3 05 Arora et al. (12)–1981a 450 42 72 – 2.6 6 0.26 Agarwal et al. (1)–1986a 100 51 80 31 16 5 07 Nair et al. (7)–1990b 100 57 88 – 10 4 08 Grover et al. (15)–1993b 48 37.5 75 – 8.3 4.1 29 Abbag et al. (16)–1998b 34 attacks of RF 67.6 – – – – –
10 Bitar et al. (17)–2000b 91 93 94 — 2 1 411 Present study–2002c 250 42 67.6 27.2 18.8 1.2 1.6
Studies conducted in developed countries are marked with an asterisk (*) in superscript after the authors’ name (column 2). RF � rheumatic fever; a � diag-nosis based on clinical findings only; b � diagnosis based on clinical findings as well as echocardiographic findings; c � diagnosis based on clinical and/or echocardiographic findings.
Ravisha et al. / Archives of Medical Research 34 (2003) 382–387386
Tabl
e6.
Val
vula
raf
fect
ion
inR
F/R
HD
inva
riou
sst
udie
s
MS
�M
V�
MS
�M
R�
MR
�A
VA
utho
r,M
R�
AR
�M
R�
MV
AV
AS
�M
S�
AS
invo
lve-
No.
year
and
nM
RM
S�
MR
MR
�A
RM
SA
RM
S�
AR
AR
AS
AS
invo
lvem
ent
invo
lvem
ent
AR
�A
Rm
ent
1M
alho
tra
etal
.(1
8)–
––
––
––
––
1,03
9(6
3.4)
103
(6.3
)–
–49
8(3
0.3)
1963
an
�1,
640
2G
hosh
etal
.(8
)52
(24.
8)94
(44.
8)5
(2.3
8)47
(22.
4)–
3(1
.43)
––
––
17(8
.09)
4(1
.9)
5(2
.38)
–19
64a
n�
210
3Se
paha
etal
.(1
9)96
(9.4
4)28
1(2
7.65
)–
345
(33.
9)–
–33
(3.2
4)–
––
54(5
.31)
––
–19
65a
n�
1,01
64
Sam
ani
etal
.(1
1)60
(7.1
)15
7(1
8.6)
–42
2(5
0.1)
––
15(1
.8)
––
––
––
142
(16.
8)19
65a
n�
842
5Sh
rest
haet
al.
(20)
209
(55.
7)77
(20.
5)–
52(1
3.8)
––
––
––
––
––
1979
an
�37
56
Kos
hiet
al.
(21)
20(6
6.7)
––
6(2
0)–
–3
(10)
––
––
––
–19
81a
n�
307
Aro
raet
al.
(12)
296
(14.
4)28
4(1
3.8)
–89
6(4
3.7)
––
124
(6)
––
–14
0(6
.8)
––
310
(15.
1)19
81a
n�
2,05
08
Gro
ver
etal
.(1
5)6
(18.
8)9
(28.
12)
4(1
2.5)
11(3
4.4)
–2
(6.2
5)–
––
––
––
–19
93b
n�
329
Pres
ent
stud
y20
02c
150
9840
4113
43
21
––
1–
–
RF
�rh
eum
atic
feve
r;R
HD
�rh
eum
atic
hear
tdi
seas
e;n
�nu
mbe
rof
case
s;M
R�
mitr
alre
gurg
itatio
n;M
S�
mitr
alst
enos
is;
AR
�ao
rtic
regu
rgita
tion;
AS
�ao
rtic
sten
osis
;M
V�
mitr
alva
lve;
AV
�A
ortic
valv
e.a di
agno
sis
base
don
clin
ical
findi
ngs
only
;b di
agno
sis
base
don
clin
ical
findi
ngs
asw
ell
asec
hoca
rdio
grap
hic
findi
ngs;
c diag
nosi
sba
sed
oncl
inic
alan
d/or
echo
card
iogr
aphi
cfin
ding
s.Fi
gure
sin
pare
nthe
ses
indi
cate
perc
enta
ges.

RF and RHD: Clinical Profile 387
when these investigations were not available. Although meanfollow-up period was considerable, some patients barelyfollowed up for one or two visits after discharge despitehaving received counseling regarding the nature of the dis-ease and the need for regular follow-up. This may suggestthat healthcare workers need to be more vigorous in ex-plaining the nature of the disease (and the need for adequatebenzathine penicillin prophylaxis) to patients.
In conclusion, arthritis was the most common manifesta-tion in the initial attack of RF, carditis was the most frequentmanifestation in patients presenting with rheumatic recur-rences (with pre-existing RHD), and mitral regurgitation wasthe most common valvular lesion. Rate of dropouts frompenicillin prophylaxis was high. Clinical manifestations inthe initial/first attack of RF have not changed significantlyduring the last 31 years.
AcknowledgmentsThe authors wish to thank Dr. N.A. Kshirsagar, Dean of SethG.S. Medical College and KEM Hospital, Mumbai for grantingpermission to submit this paper for publication.
References1. Agarwal BL, Agarwal R. Rheumatic fever: clinical profile of the initial
attack in India. Bull WHO 1986;64:573–578.2. Joshi MK, Kandoth PW, Barve RJ, Kamat JR. Rheumatic fever. Clinical
profile of 339 cases with long term follow up. Indian Pediatr 1983;20:849–853.
3. Bavdekar SB, Soloman R, Kamat JR. Rheumatic fever in children. JIndian Med Assoc 1999;97:489–492.
4. Taranta A, Markowitz M. Rheumatic fever. 2nd ed. Hingham, MA,USA: Kluwer Academic Publishers;1989.
5. Rullan E, Sigal LH. Rheumatic fever. Curr Rheumatol Rep 2001;3:445–452.
6. Padmavati S. Present status of rheumatic fever and rheumatic heartdisease in India. Indian Heart J 1995;47:395–398.
7. Nair PM, Philip E, Bahuleyan CG, Thomas M, Shanmugham JS, SugunaBai NS. The first attack of acute rheumatic fever in childhood—clinicaland laboratory profile. Indian Pediatr 1990;27:241–246.
8. Ghosh S, Mangat R. Acute rheumatic fever and rheumatic heart diseasein childhood. Indian Pediatr 1964;1:226–230.
9. Zaman MM, Rouf MA, Haque S, Khan LR, Chowdhury NA, RazzaqueSA, Yoshiike N, Tanaka H. Does rheumatic fever occur usually betweenthe ages of 5 and 15 years? Int J Cardiol 1998;66:17–21.
10. Benakappa DG, Gangadharappa N, Kasthuri AV. Review of 100 casesof rheumatic fever in children. Indian Pediatr 1978;15:379–384.
11. Samani OT, Chandalia HB. Rheumatic heart disease in Bombay: astudy of 917 cases. Indian Heart J 1965;17:283–292.
12. Arora R, Subramanyam G, Khalilullah M, Gupta MP. Clinical profileof rheumatic fever and rheumatic heart disease: a study of 2,500 cases.Indian Heart J 1981;33:264–269.
13. Bland EF, Jones TD. Rheumatic fever and rheumatic heart disease: atwenty year report on 1000 patients followed since childhood. Circu-lation 1951;4:836–843.
14. Sanyal SK, Thapar MK, Ahmed SH, Hooja V, Tewari P. The initialattack of acute rheumatic fever during childhood in North India: aprospective study of the clinical profile. Circulation 1974;49:7–12.
15. Grover A, Dhawan A, Iyengar SD, Anand IS, Wahi PL, GangulyNK. Epidemiology of rheumatic fever and rheumatic heart disease ina rural community in northern India. Bull WHO 1993;71:59–66.
16. Abbag F, Benjamin B, Kardash MM, al Barki A. Acute rheumaticfever in southern Saudi Arabia. East Afr Med J 1998;75:279–281.
17. Bitar FF, Hayek P, Obeid M, Gharzeddine W, Mikati M, Dbaibo GS.Rheumatic fever in children: a 15-year experience in a developingcountry. Pediatr Cardiol 2000;21:119–122.
18. Malhotra RP, Gupta SP. Rheumatic heart disease in Punjab with specialemphasis on clinical patterns that differ from those reported abroad:a study based on 1745 cases of rheumatic heart disease. Indian HeartJ 1963;15:107–113.
19. Sepaha GC, Jain SR, Jain IM. Rheumatic heart disease in MadhyaPradesh: a report of 1016 cases. Indian Heart J 1965;17:276–282.
20. Shrestha NK, Padmavati S. Prevalence of rheumatic heart disease inDelhi school children. Indian J Med Res 1979;69:821–833.
21. Koshi G, Benjamin V, Cherian G. Rheumatic fever and rheumatic heartdisease in rural South Indian children. Bull WHO 1981;59:599–603.
22. Kassem AS, El-Walili TM, Zaher SR, Ayman M. Reversibility ofmitral regurgitation following rheumatic fever: clinical profile andechocardiographic evaluation. Indian J Pediatr 1995;62:717–723.
23. Kumar R, Raizada A, Aggarwal AK, Ganguly NK. A community-based rheumatic fever/rheumatic heart disease cohort: twelve-year ex-perience. Indian Heart J 2002;54:54–58.