review in internal medicine 2021
TRANSCRIPT

Review in Internal Medicine 2021
Pituitary
Hypothalamus
TSH
TRH
_
_
Thyroid
T4
T3
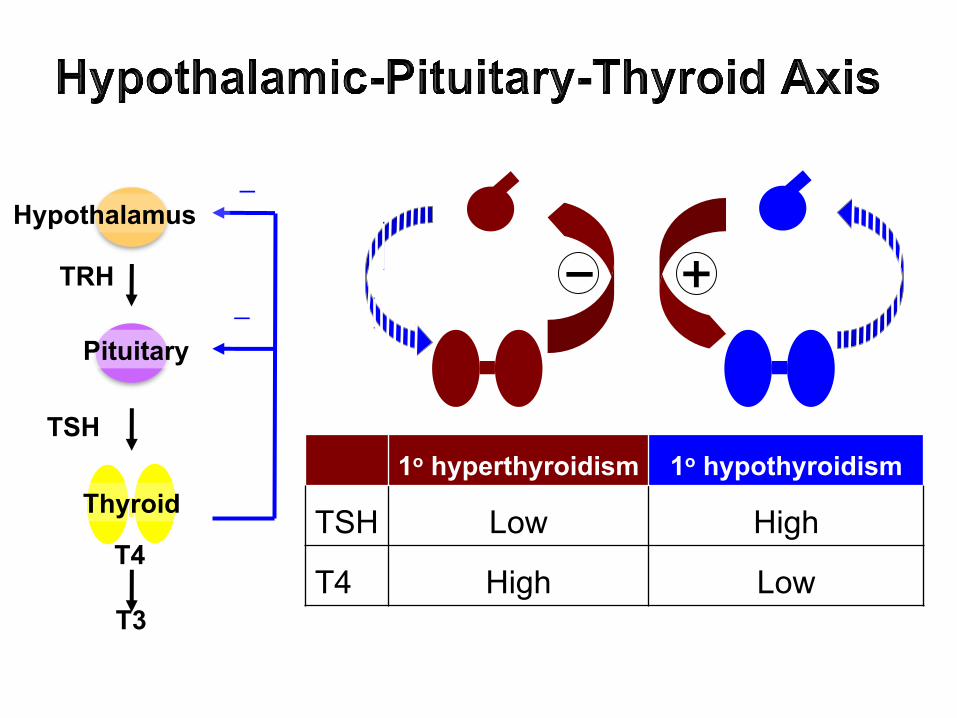
1o hyperthyroidism 1o hypothyroidism
TSH Low High
T4 High Low

TSH is the most efficient test for 1o thyroid disease.
Clinical Endocrinology 2011;74, 673-678.
A 2-fold change in FT4 will produce a 100-fold change in TSH.

Usual TFT Interpretation
!"# !$" %&'()*+&+⬆ ⬇ ,! -./012-.1*&3&+4⬇ ⬆ ,! -./*2-.1*&3&+4! ⬇ $5678&)&7'8#-./012-.1*&3&+4
! ⬆ $5678&)&7'8#-./*2-.1*&3&+4⬆ ⬆9: ;)'//1*/1&'20#!$"#+07102&*)⬇ ⬇9: <0)21'8#-./*2-.1*&3&+4 *1
:*)#2-.1*&3'8#&88)0++
Pituitary
Hypothalamus
TSH
TRH
_
_
Thyroxine binding globulin (TBG)
Receptor
Thyroid
T4
T3 Screening thyroid disorder: TSHSuspected thyrotoxicosis: TSH, FT4, TT3 (or FT3)Suspected hypothyroidism: TSH, FT4
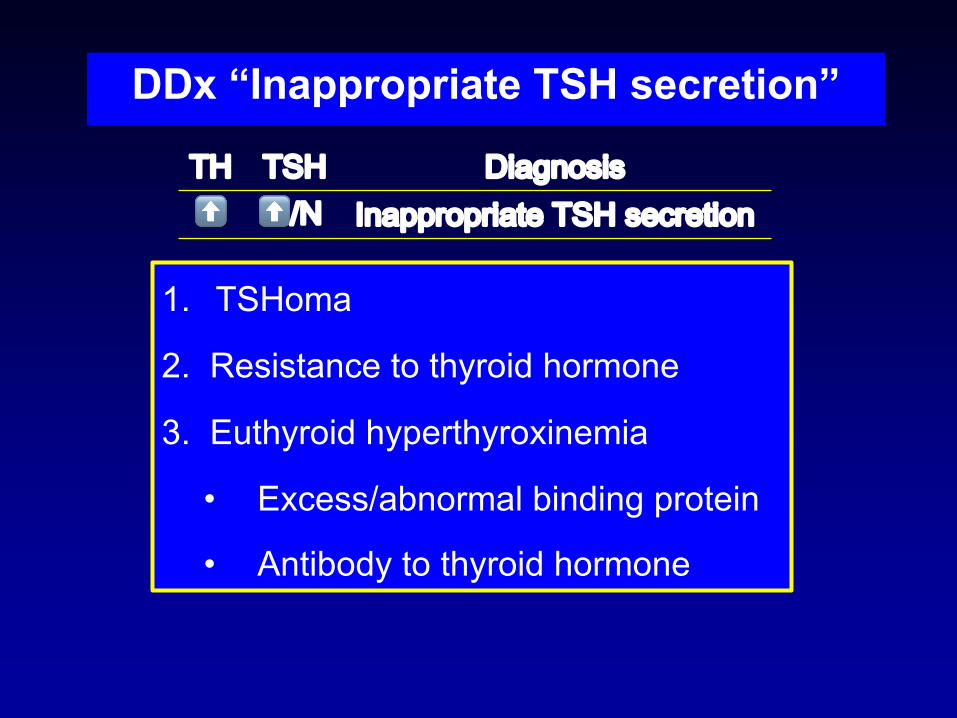
DDx “Inappropriate TSH secretion”
1. TSHoma
2. Resistance to thyroid hormone
3. Euthyroid hyperthyroxinemia
• Excess/abnormal binding protein
• Antibody to thyroid hormone
!"# !$" %&'()*+&+⬆ ⬆9: ;)'//1*/1&'20#!$"#+07102&*)
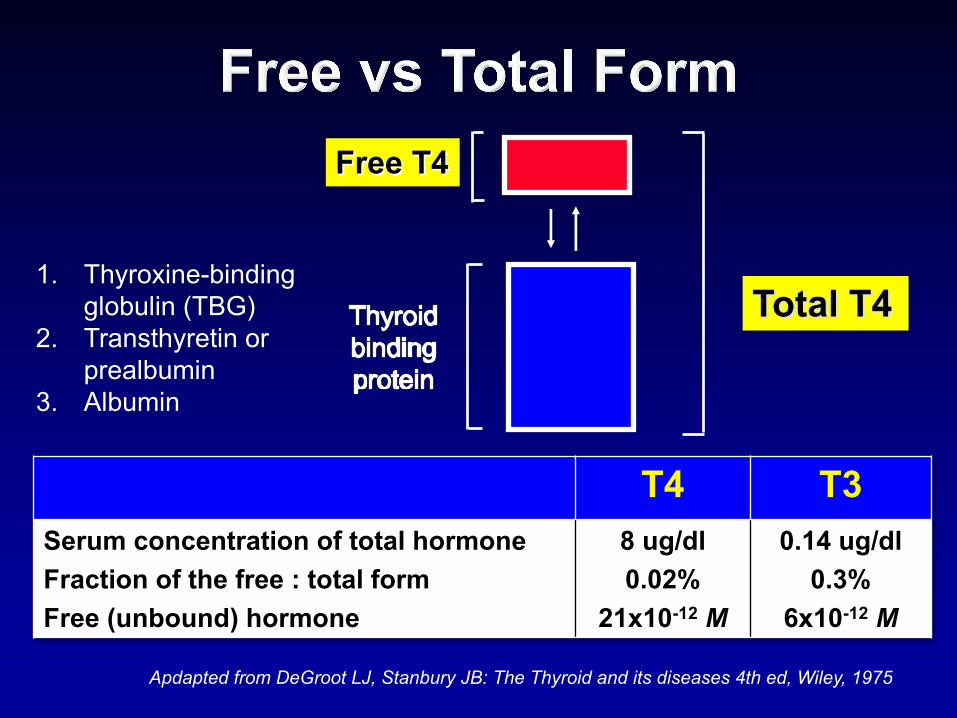
Free T4
Total T4
Apdapted from DeGroot LJ, Stanbury JB: The Thyroid and its diseases 4th ed, Wiley, 1975
T4 T3Serum concentration of total hormoneFraction of the free : total formFree (unbound) hormone
8 ug/dl0.02%
21x10-12 M
0.14 ug/dl0.3%
6x10-12 M
1. Thyroxine-binding globulin (TBG)
2. Transthyretin or prealbumin
3. Albumin
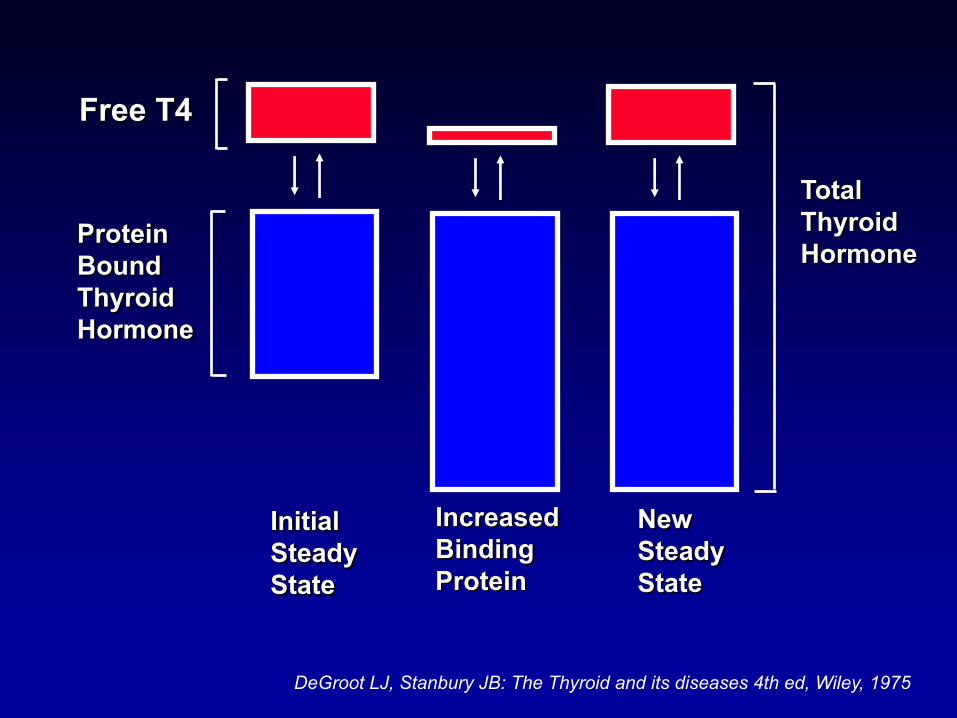
Free T4
ProteinBound ThyroidHormone
InitialSteadyState
Increased Binding Protein
New Steady State
Total Thyroid Hormone
DeGroot LJ, Stanbury JB: The Thyroid and its diseases 4th ed, Wiley, 1975
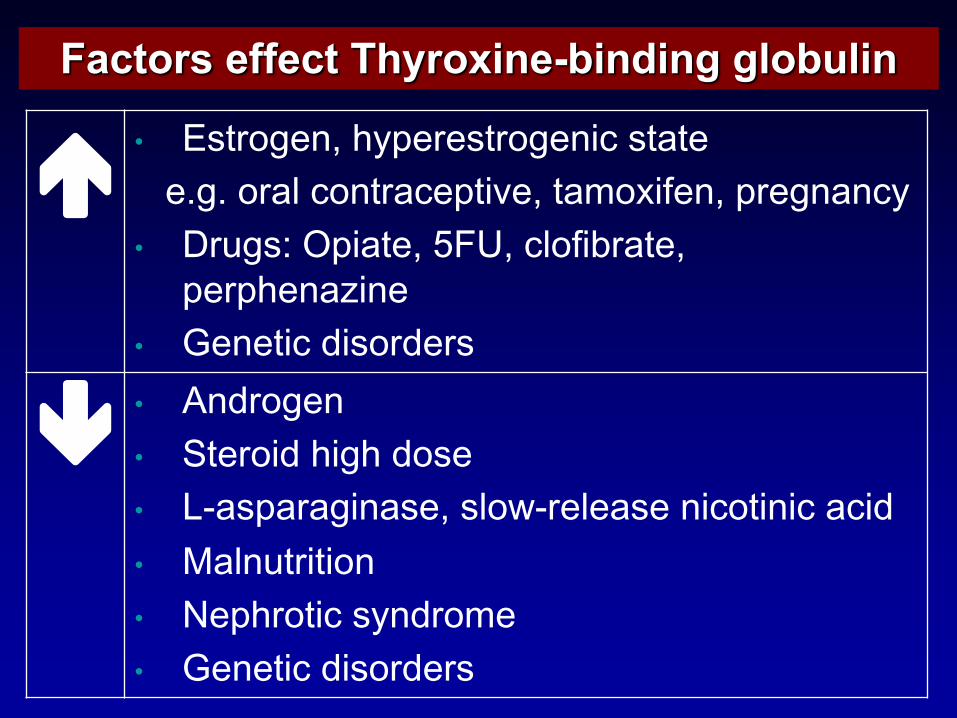
Factors effect Thyroxine-binding globulin
é• "#$%&'()*+,-.(%(#$%&'()/0 #$1$(+(2'2+&%13+0&)$%10(.$/4(*+$15&6/7()*+.%(')1)0-
• 8%9'#:+;./1$(*+<=>*+03&7/?%1$(*+.(%.,()1@/)(
• A()($/0+B/#&%B(%#
ê• C)B%&'()• D$(%&/B+,/',+B&#(• EF1#.1%1'/)1#(*+#3&GF%(3(1#(+)/0&$/)/0+10/B• H13)9$%/$/&)• !(.,%&$/0 #-)B%&5(• A()($/0+B/#&%B(%#
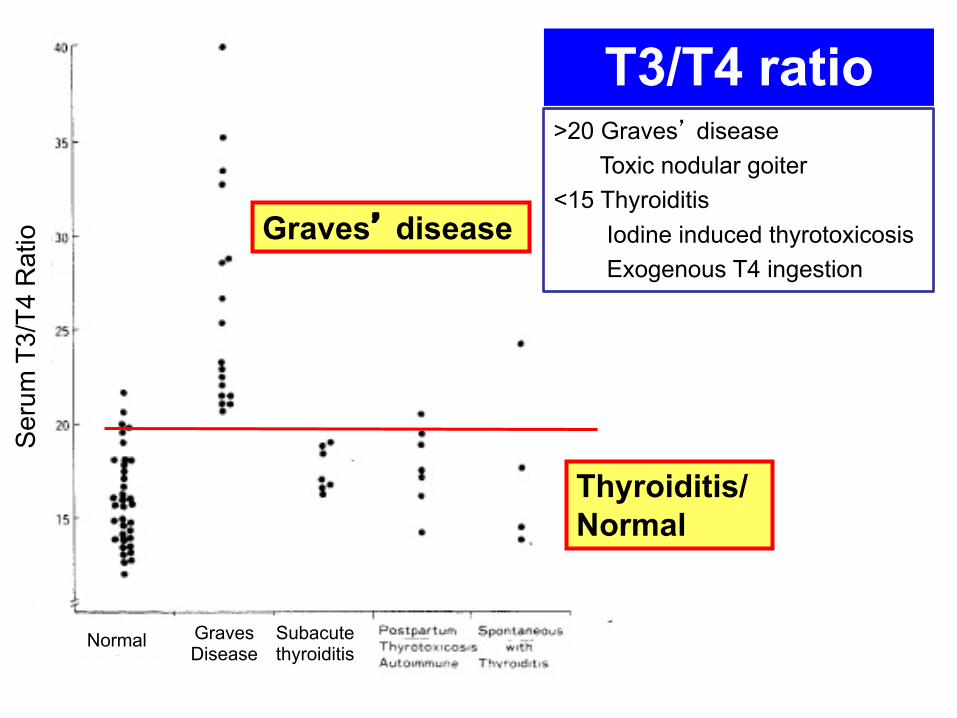
T3/T4 ratio
Graves’ disease
Thyroiditis/Normal
>20 Graves’ diseaseToxic nodular goiter
<15 ThyroiditisIodine induced thyrotoxicosisExogenous T4 ingestion
Seru
m T
3/T4
Rat
io
Normal GravesDisease
Subacutethyroiditis
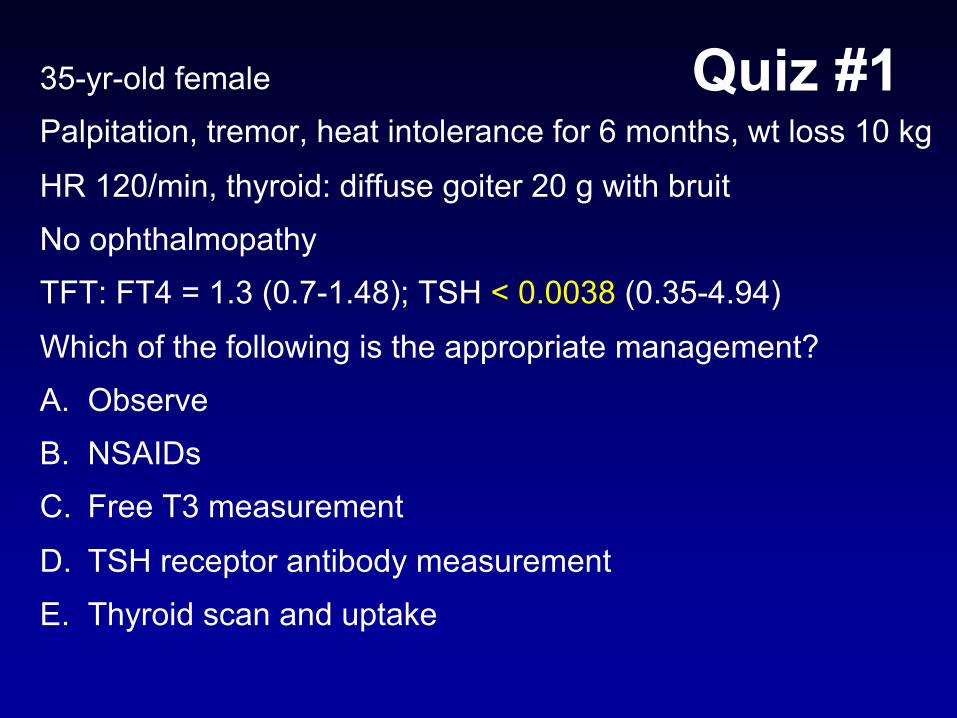
Quiz #135-yr-old femalePalpitation, tremor, heat intolerance for 6 months, wt loss 10 kg
HR 120/min, thyroid: diffuse goiter 20 g with bruitNo ophthalmopathyTFT: FT4 = 1.3 (0.7-1.48); TSH < 0.0038 (0.35-4.94)Which of the following is the appropriate management?A. ObserveB. NSAIDsC. Free T3 measurement
D. TSH receptor antibody measurementE. Thyroid scan and uptake
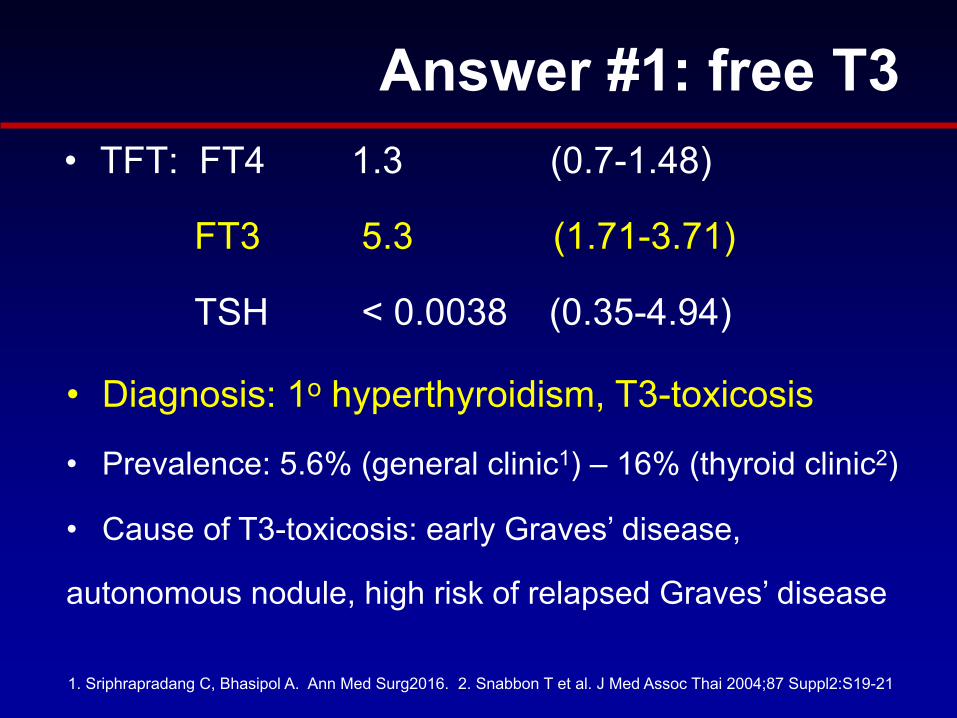
• TFT: FT4 1.3 (0.7-1.48)
FT3 5.3 (1.71-3.71)
TSH < 0.0038 (0.35-4.94)
• Diagnosis: 1o hyperthyroidism, T3-toxicosis
• Prevalence: 5.6% (general clinic1) – 16% (thyroid clinic2)
• Cause of T3-toxicosis: early Graves’ disease,
autonomous nodule, high risk of relapsed Graves’ disease
1. Sriphrapradang C, Bhasipol A. Ann Med Surg2016. 2. Snabbon T et al. J Med Assoc Thai 2004;87 Suppl2:S19-21
Answer #1: free T3
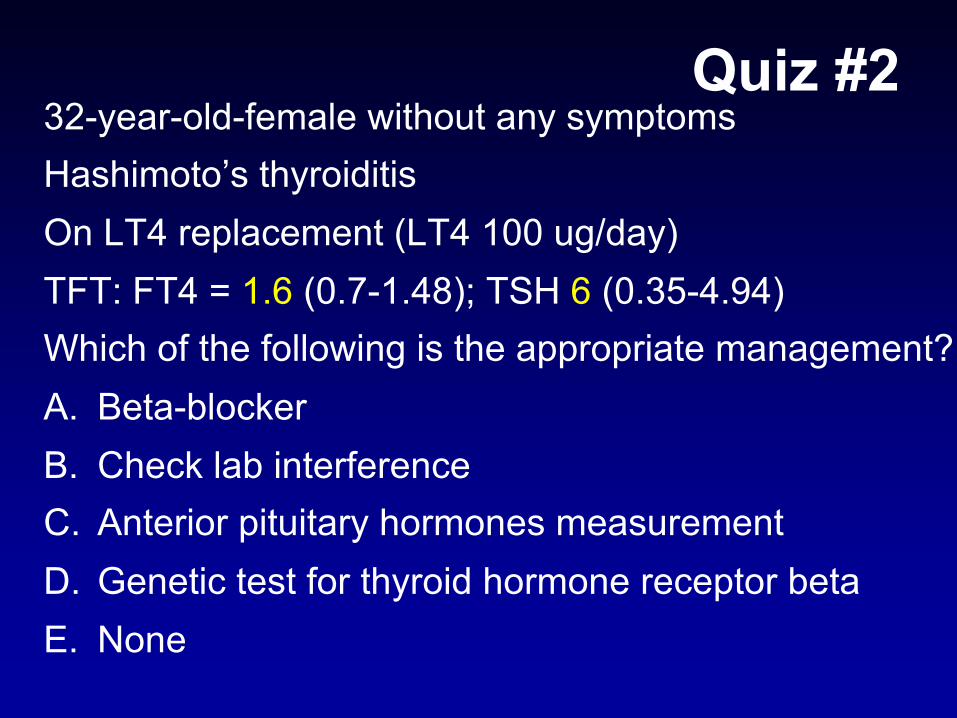
32-year-old-female without any symptomsHashimoto’s thyroiditisOn LT4 replacement (LT4 100 ug/day)TFT: FT4 = 1.6 (0.7-1.48); TSH 6 (0.35-4.94)Which of the following is the appropriate management?A. Beta-blockerB. Check lab interferenceC. Anterior pituitary hormones measurementD. Genetic test for thyroid hormone receptor betaE. None
Quiz #2

• FT4 = 1.6 (0.7-1.48); TSH 6 (0.35-4.94)
• Poor compliance
• Owing to their differing half-lives,
intermittent hormone ingestion can result in
normal or even elevated FT4 levels,
but fails to normalize TSH
Answer #2: none
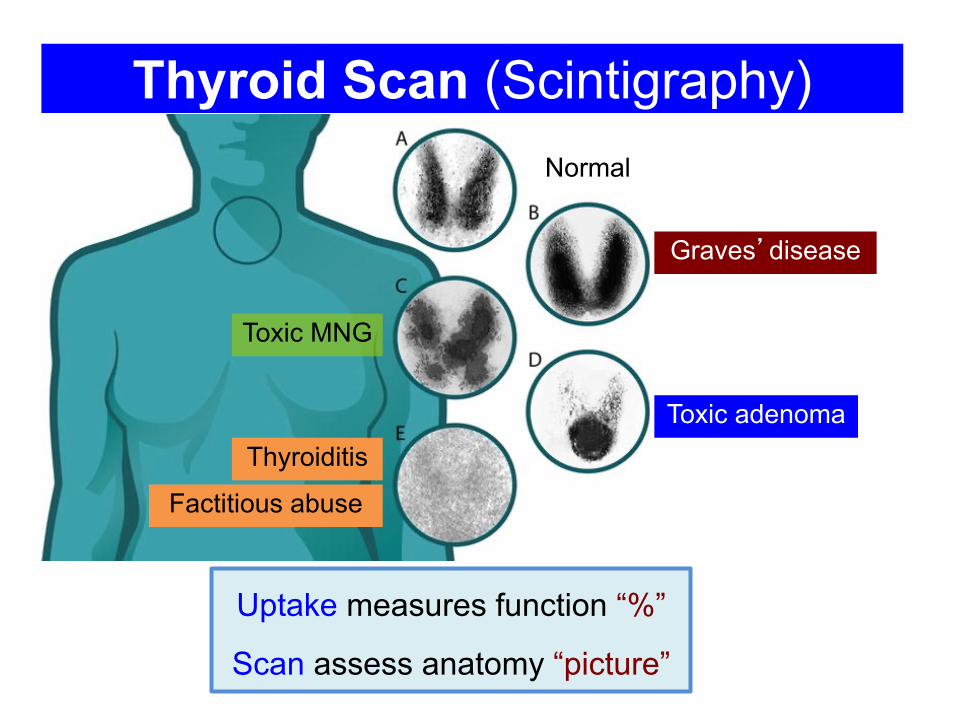
Thyroid Scan (Scintigraphy)Normal
Toxic MNG
Graves’disease
Toxic adenomaThyroiditis
Factitious abuse
Uptake measures function “%”
Scan assess anatomy “picture”
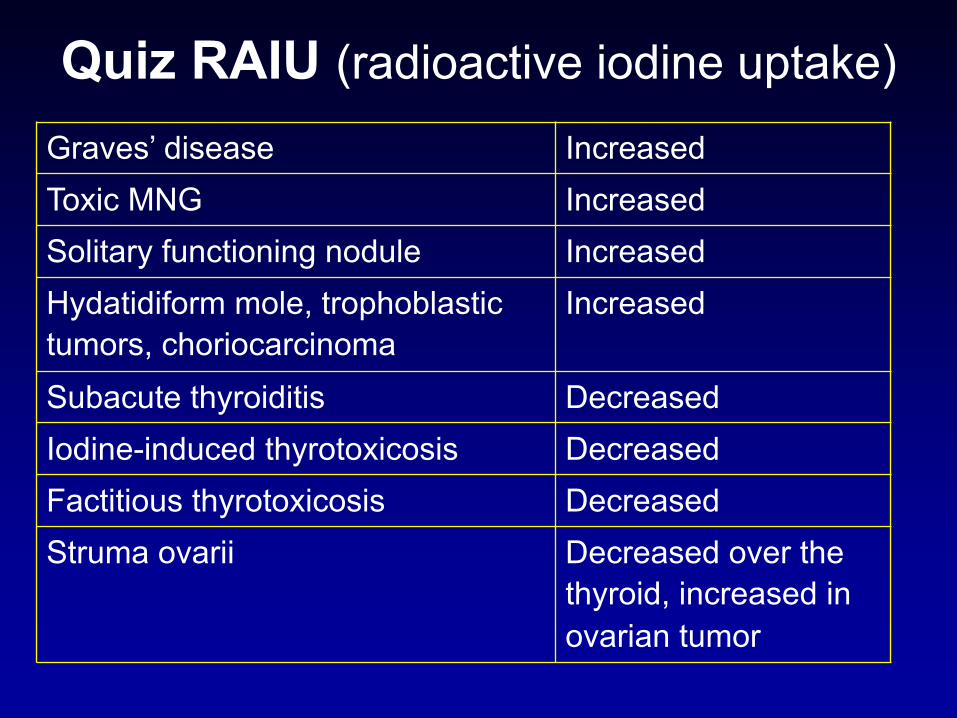
Quiz RAIU (radioactive iodine uptake) Graves’ disease IncreasedToxic MNG IncreasedSolitary functioning nodule IncreasedHydatidiform mole, trophoblastic tumors, choriocarcinoma
Increased
Subacute thyroiditis DecreasedIodine-induced thyrotoxicosis DecreasedFactitious thyrotoxicosis DecreasedStruma ovarii Decreased over the
thyroid, increased in ovarian tumor
TSH receptor Ab• DDx of etiology of thyrotoxicosis in patients with
ambiguous clinical findings
• Diagnosis of euthyroid Graves’
e.g., Exophthalmos in euthyroid pts
• Determining the risk of fetal and neonatal Graves’
• Assessing the risk of Graves’ disease relapse after ATD Rx
TPO Ab & Tg Ab• Diagnosis of autoimmune thyroid diseases• Diagnosis of postpartum thyroiditis• As a risk factor for
– AITD in pts with autoimmune disease e.g., T1DM– Thyroid dysfunction or hypothyroidism before and during
amiodarone, lithium, IFN-alpha– Hypothyroidism in Down syndrome– Thyroid dysfunction during pregnancy – Spontaneous miscarriage
• TgAb: follow-up to assess disease recurrence in thyroid cancer (combination with thyroglobulin level)
Adapted from Autoantibodies Textbook 2013

Sriphrapradang C et al. Poster Presentation in Endocrine Society Meeting 2010 San Diego, CA
TRAb
TPO AbTg Ab
Quiz #339-yr-old prisoner malePalpitation, tremor, heat intolerance for 6 months, wt loss 10 kg
HR 120/min, thyroid: no goiter, no ophthalmopathyFT3 > 7 (1.71-3.71); FT4 = 3 (0.7-1.48), TSH < 0.0038 Thyroglobulin (Tg) < 0.1 ng/mL (3.5-77), TPO Ab & Tg Ab negWhat is the most likely cause of thyrotoxicosis?A. Graves’ diseaseB. Subacute thyroiditis
C. Functioning thyroid metastasisD. TSHomaE. Thyrotoxicosis factitia
• Suppressed thyroglobulin (TgAb neg)
= No thyroid tissue
(history of total thyroidectomy + radioactive iodine)
= Exogenous thyroid hormone ingestion
• “Hamburger thyrotoxicosis”
– Meat in the neck region of slaughtered animals is ground into hamburger
– Outbreak of thyrotoxicosis
Answer #3: factitious thyrotoxicosis
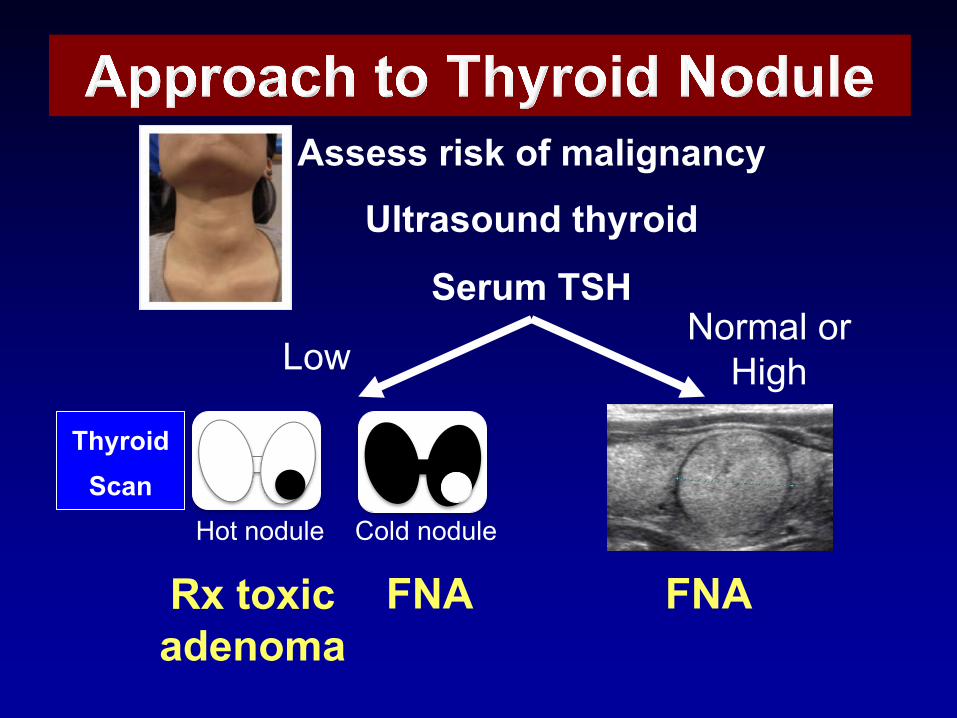
Assess risk of malignancyUltrasound thyroid
Serum TSH
LowNormal or
High
Hot nodule Cold nodule
FNA FNARx toxic adenoma
ThyroidScan
Quiz #460-yr-old female, no underlying diseaseSlow-growing right thyroid nodule for 2 yrs
Exam: BP 130/80, HR 72/min regular rhythm4-cm rubbery and movable thyroid nodule @ Rt lobeFT3 = 2 (1.71-3.71); FT4 = 1.1 (0.7-1.48), TSH < 0.0038 What is the most appropriate next step?A. Thyroid scanB. TSH receptor antibodyC. Doppler USG thyroid
D. Whole body scanE. ESR
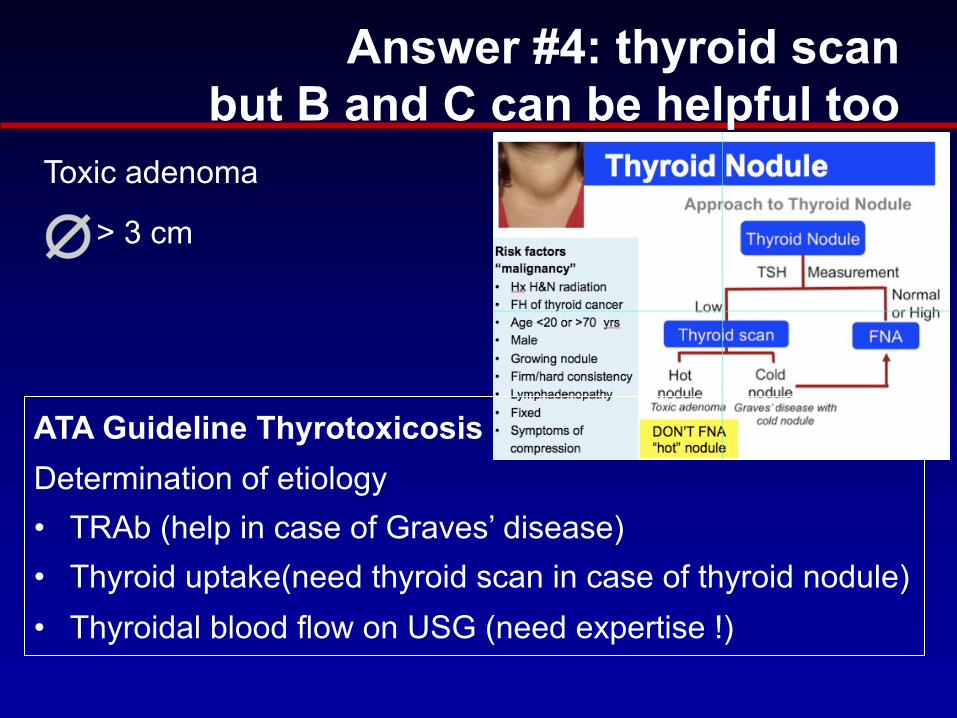
Answer #4: thyroid scan but B and C can be helpful too
ATA Guideline ThyrotoxicosisDetermination of etiology • TRAb (help in case of Graves’ disease)• Thyroid uptake(need thyroid scan in case of thyroid nodule)• Thyroidal blood flow on USG (need expertise !)
Toxic adenoma
> 3 cm
Thyroid scan
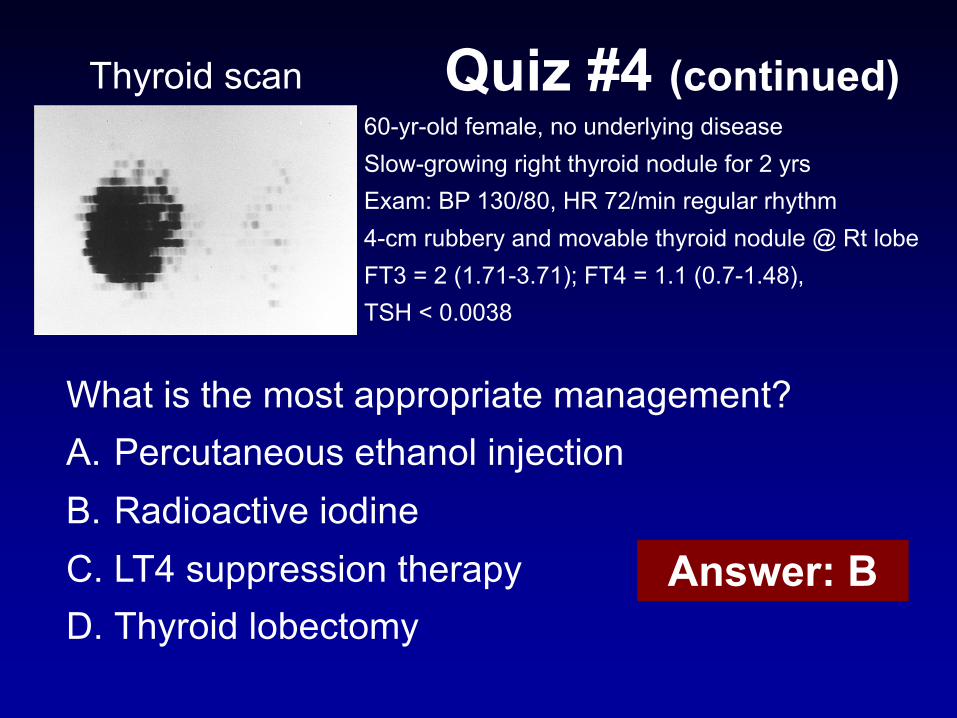
What is the most appropriate management?A. Percutaneous ethanol injectionB. Radioactive iodineC. LT4 suppression therapyD. Thyroid lobectomy
60-yr-old female, no underlying diseaseSlow-growing right thyroid nodule for 2 yrsExam: BP 130/80, HR 72/min regular rhythm4-cm rubbery and movable thyroid nodule @ Rt lobeFT3 = 2 (1.71-3.71); FT4 = 1.1 (0.7-1.48),TSH < 0.0038
Quiz #4 (continued)
Answer: B
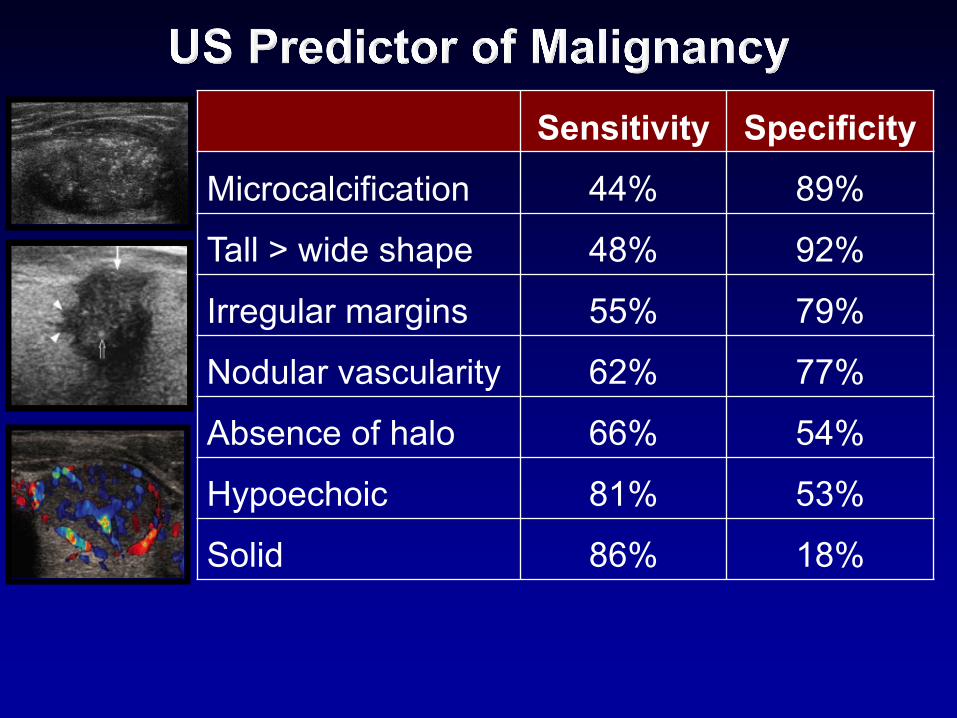
Sensitivity SpecificityMicrocalcification 44% 89%
Tall > wide shape 48% 92%
Irregular margins 55% 79%
Nodular vascularity 62% 77%
Absence of halo 66% 54%
Hypoechoic 81% 53%
Solid 86% 18%
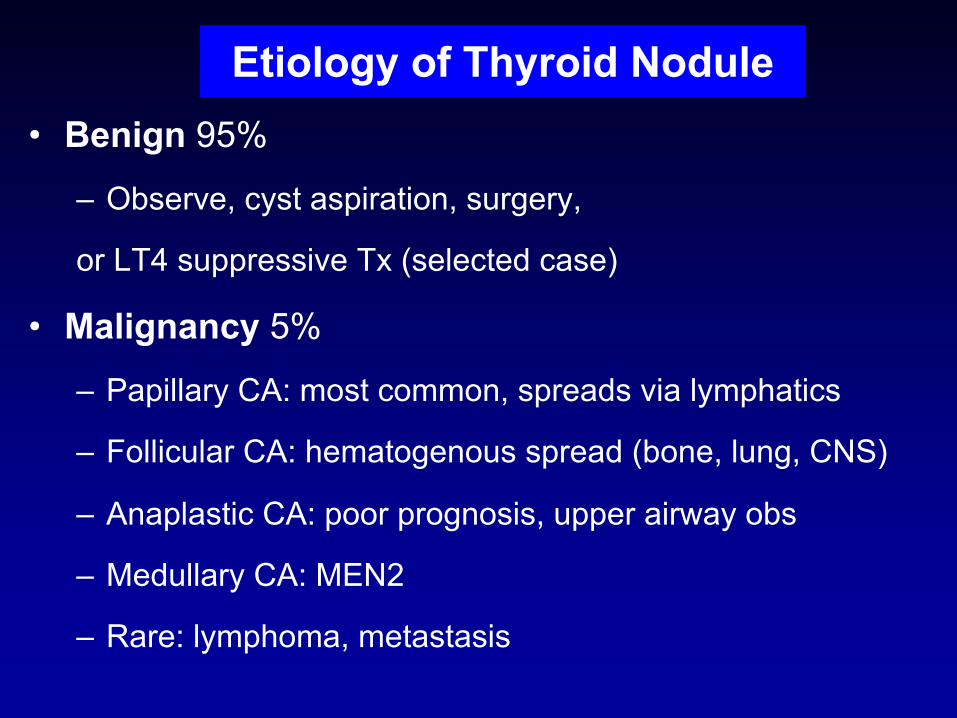
Etiology of Thyroid Nodule• Benign 95%
– Observe, cyst aspiration, surgery,
or LT4 suppressive Tx (selected case)
• Malignancy 5%
– Papillary CA: most common, spreads via lymphatics
– Follicular CA: hematogenous spread (bone, lung, CNS)
– Anaplastic CA: poor prognosis, upper airway obs
– Medullary CA: MEN2
– Rare: lymphoma, metastasis

Quiz #525-yr-old maleRight thyroid nodule ~ 2 cm
Normal TSHFNA: medullary thyroid carcinomaWhich of the following is the most appropriate next step?A. MIBG scanB. Whole body scan
C. Hemoglobin A1cD. Prolactin levelE. 24-hr urine fractionated metanephrine
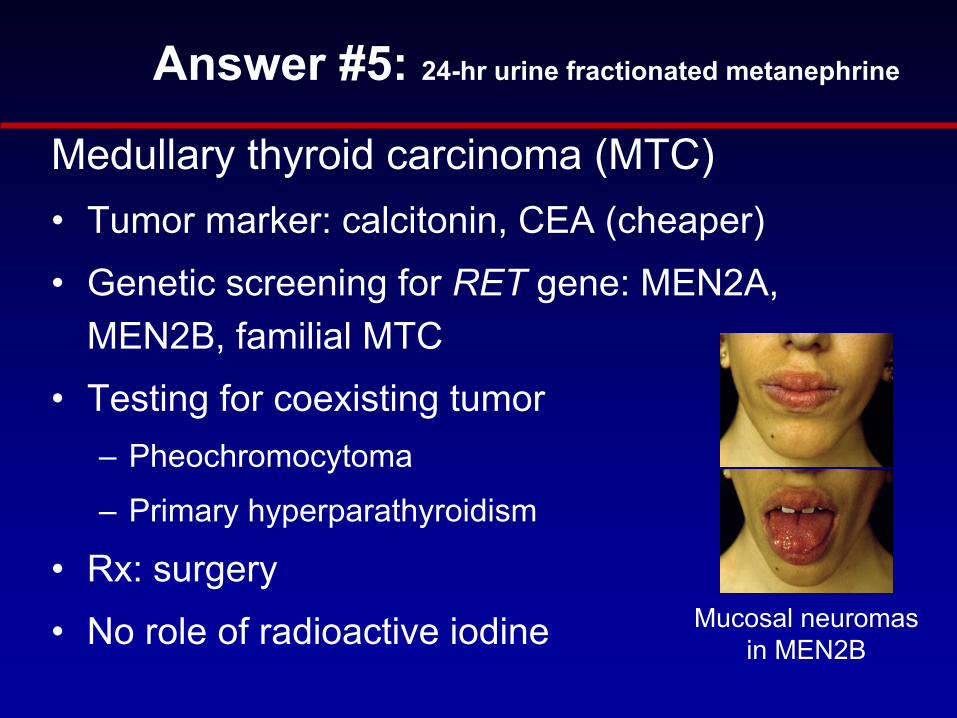
Medullary thyroid carcinoma (MTC)• Tumor marker: calcitonin, CEA (cheaper)• Genetic screening for RET gene: MEN2A,
MEN2B, familial MTC• Testing for coexisting tumor
– Pheochromocytoma
– Primary hyperparathyroidism
• Rx: surgery• No role of radioactive iodine
Answer #5: 24-hr urine fractionated metanephrine
Mucosal neuromasin MEN2B

Thyrotoxicosis vs Hyperthyroidism
Non-hyper-
thyroidism

Some Clues of Specific Causes of Thyrotoxicosis
Graves’ disease
Toxic adenoma
Toxic MNG
Subacutethyroiditis
Thyroid bruit
> 3 cm
PAINTENDERNESS
Short Duration
Family history, other autoimmune disorders
T3/T4 ratio <20
Slowly progression
S HyperàOvert Hyper

Treatment Advantages Disadvantages
Antithyroiddrugs
• Conservative Rx• Hospitalization • Low risk of subsequent
hypothyroidism• Radiation exposure• No effect on GO• Safe to use during pregnancy
and breastfeeding
• High relapse rate• Frequent clinic visits • Poor adherence• Adverse events (rarely major)
131I • Definitive Rx• Low cost• Hospitalization• No need for surgery or
anaesthetic
• Lifelong hypothyroidism• Radiation exposure• Slow control of hyperthyroidism• Possible progression or de novo
occurrence of GO
Thyroidec-tomy
• Definitive Rx• Radiation exposure• Prompt control of
hyperthyroidism
• Lifelong hypothyroidism• Adverse events related to
surgical procedure and anaesthetic
• Hospitalization• High cost• Permanent scar
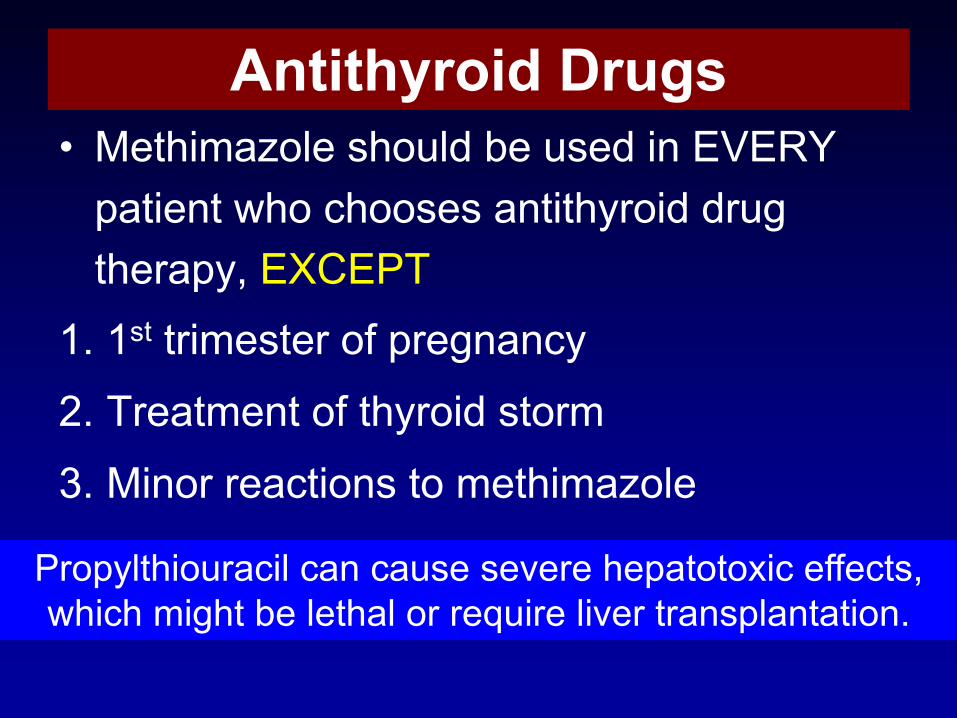
Antithyroid Drugs• Methimazole should be used in EVERY
patient who chooses antithyroid drug therapy, EXCEPT
1. 1st trimester of pregnancy2. Treatment of thyroid storm3. Minor reactions to methimazole
Propylthiouracil can cause severe hepatotoxic effects, which might be lethal or require liver transplantation.
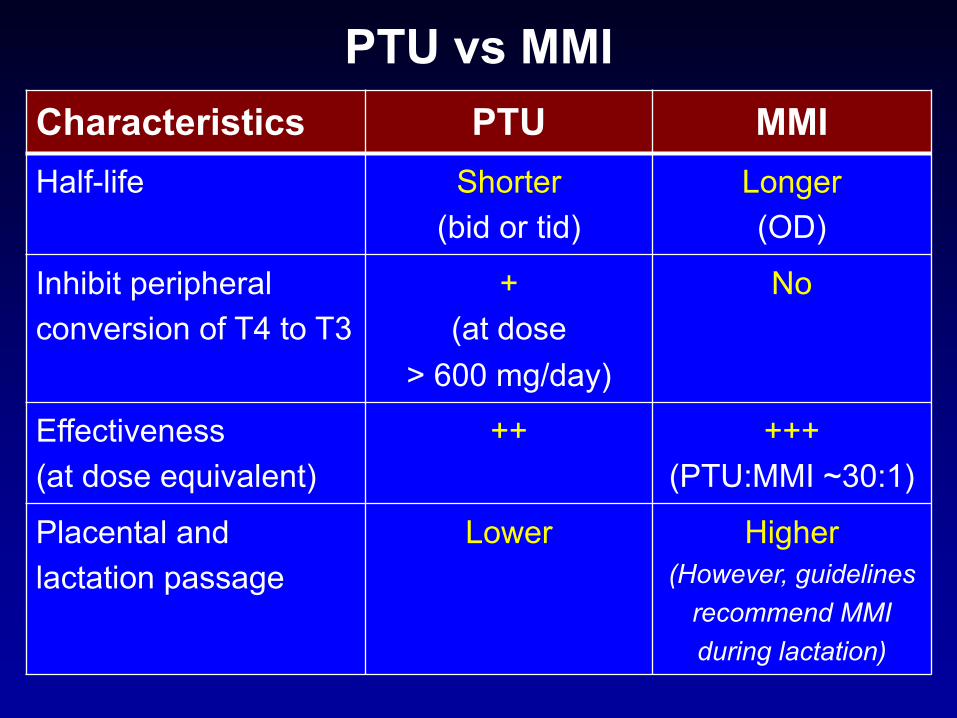
PTU vs MMICharacteristics PTU MMIHalf-life Shorter
(bid or tid)Longer(OD)
Inhibit peripheral conversion of T4 to T3
+(at dose
> 600 mg/day)
No
Effectiveness (at dose equivalent)
++ +++(PTU:MMI ~30:1)
Placental and lactation passage
Lower Higher(However, guidelines
recommend MMI during lactation)
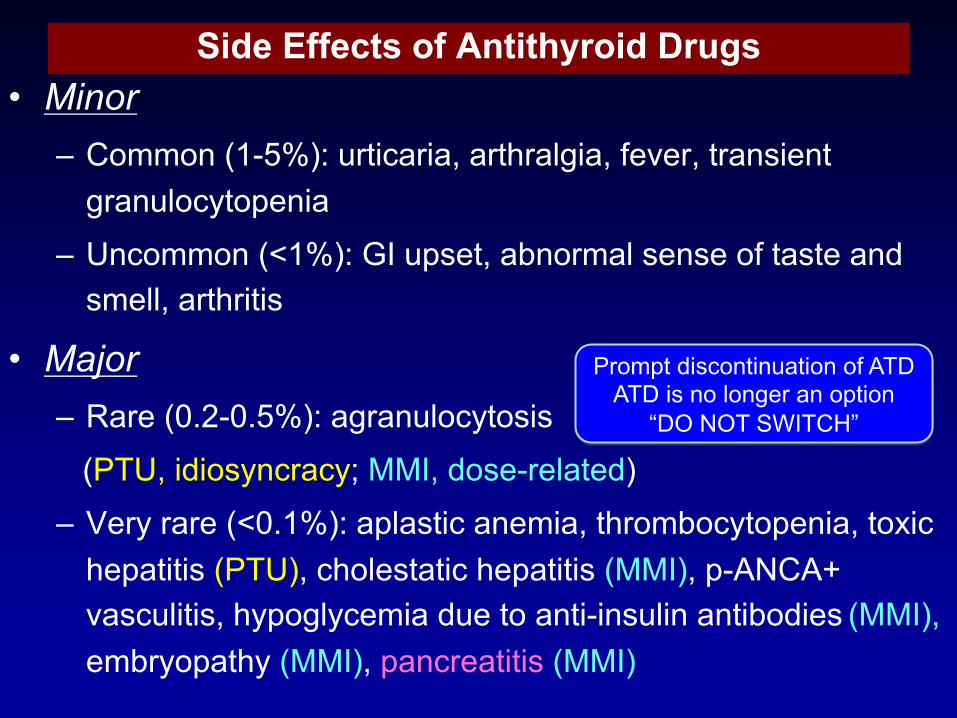
Side Effects of Antithyroid Drugs• Minor
– Common (1-5%): urticaria, arthralgia, fever, transient granulocytopenia
– Uncommon (<1%): GI upset, abnormal sense of taste and smell, arthritis
• Major– Rare (0.2-0.5%): agranulocytosis
(PTU, idiosyncracy; MMI, dose-related)– Very rare (<0.1%): aplastic anemia, thrombocytopenia, toxic
hepatitis (PTU), cholestatic hepatitis (MMI), p-ANCA+ vasculitis, hypoglycemia due to anti-insulin antibodies (MMI), embryopathy (MMI), pancreatitis (MMI)
Prompt discontinuation of ATDATD is no longer an option
“DO NOT SWITCH”
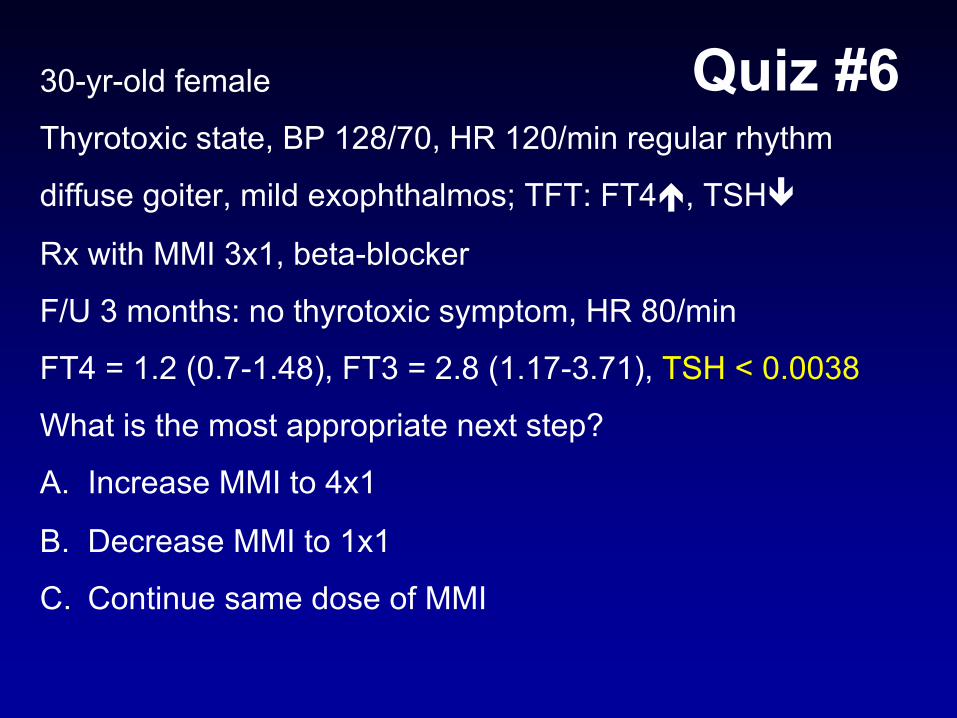
Quiz #630-yr-old female
Thyrotoxic state, BP 128/70, HR 120/min regular rhythm
diffuse goiter, mild exophthalmos; TFT: FT4é, TSHê
Rx with MMI 3x1, beta-blocker
F/U 3 months: no thyrotoxic symptom, HR 80/min
FT4 = 1.2 (0.7-1.48), FT3 = 2.8 (1.17-3.71), TSH < 0.0038
What is the most appropriate next step?
A. Increase MMI to 4x1
B. Decrease MMI to 1x1
C. Continue same dose of MMI

Thyroid 2003; 13:1-126.
Quiz #6 Answer: B decrease MMI
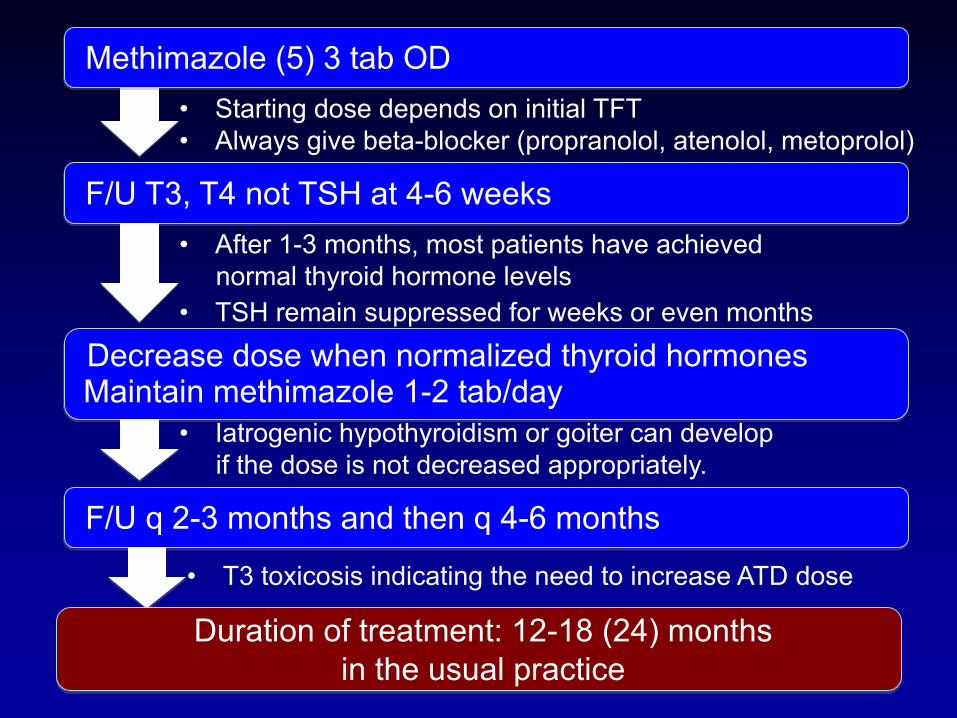
• Starting dose depends on initial TFT• Always give beta-blocker (propranolol, atenolol, metoprolol)
F/U T3, T4 not TSH at 4-6 weeks• After 1-3 months, most patients have achieved
normal thyroid hormone levels
Decrease dose when normalized thyroid hormonesMaintain methimazole 1-2 tab/day
• Iatrogenic hypothyroidism or goiter can develop if the dose is not decreased appropriately.
F/U q 2-3 months and then q 4-6 months
• TSH remain suppressed for weeks or even months
• T3 toxicosis indicating the need to increase ATD dose
Duration of treatment: 12-18 (24) monthsin the usual practice
Methimazole (5) 3 tab OD
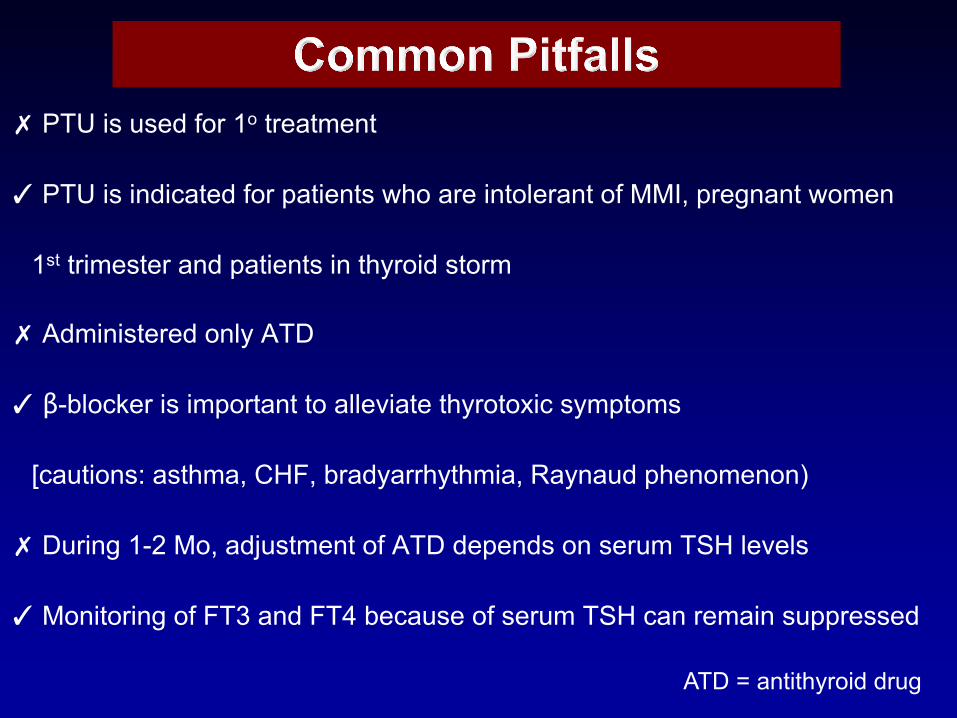
✗ PTU is used for 1o treatment
✓ PTU is indicated for patients who are intolerant of MMI, pregnant women
1st trimester and patients in thyroid storm
✗ Administered only ATD
✓ β-blocker is important to alleviate thyrotoxic symptoms
[cautions: asthma, CHF, bradyarrhythmia, Raynaud phenomenon)
✗ During 1-2 Mo, adjustment of ATD depends on serum TSH levels
✓Monitoring of FT3 and FT4 because of serum TSH can remain suppressed
ATD = antithyroid drug

Factors associated with a high rate of relapse after antithyroid drug treatment
• Severe hyperthyroidism• Large goiter• T3 predominance• Prior relapse• High levels of TSH receptor antibody • Young age• Male sex• Cigarette smoking• Postpartum period
Adapted from Nat Rev Endocrinol. 2013 Dec;9(12):724-34.
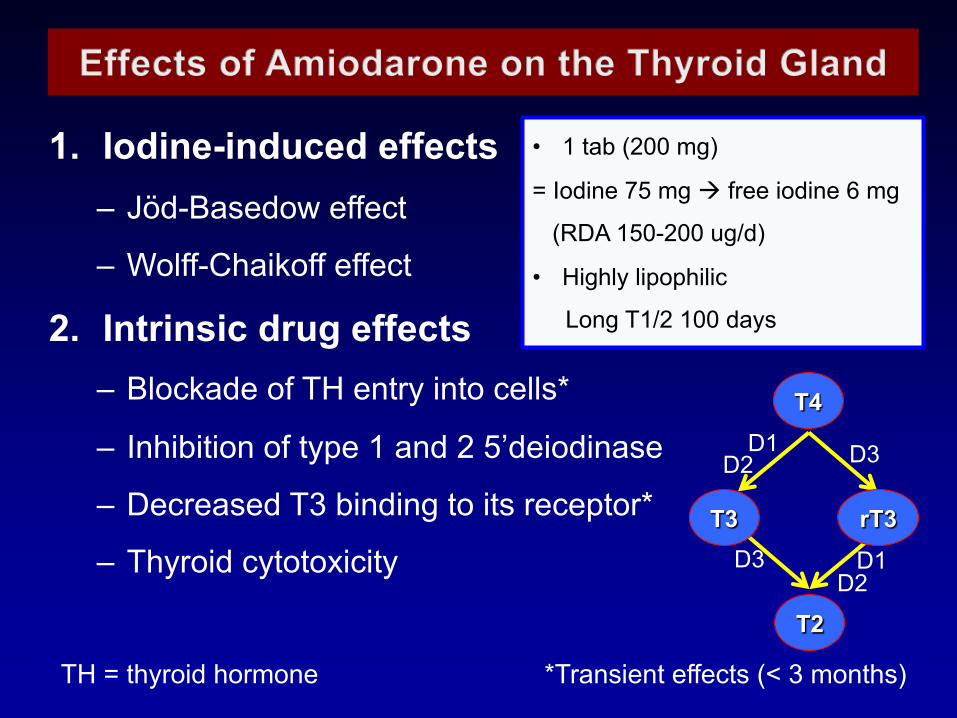
1. Iodine-induced effects– Jöd-Basedow effect
– Wolff-Chaikoff effect
2. Intrinsic drug effects– Blockade of TH entry into cells*
– Inhibition of type 1 and 2 5’deiodinase
– Decreased T3 binding to its receptor*
– Thyroid cytotoxicity
TH = thyroid hormone *Transient effects (< 3 months)
D1 D3D2
D3 D1D2
T4
rT3T3
T2
• 1 tab (200 mg)
= Iodine 75 mg à free iodine 6 mg
(RDA 150-200 ug/d)
• Highly lipophilic
Long T1/2 100 days
• Amiodarone-induced thyrotoxicosis (AIT)
• Type 1: iodine-induced hyperthyroidism
• Type 2: drug-induced destructive thyroiditis
• Amiodarone-induced hypothyroidism (AIH)
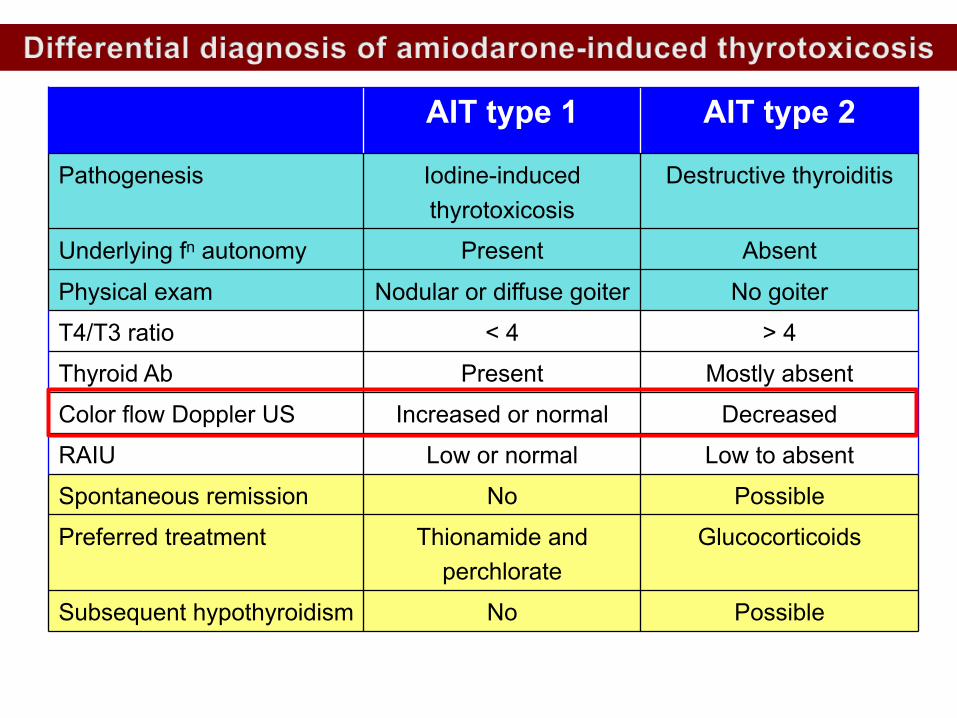
AIT type 1 AIT type 2
Pathogenesis Iodine-induced thyrotoxicosis
Destructive thyroiditis
Underlying fn autonomy Present Absent
Physical exam Nodular or diffuse goiter No goiter
T4/T3 ratio < 4 > 4
Thyroid Ab Present Mostly absent
Color flow Doppler US Increased or normal Decreased
RAIU Low or normal Low to absent
Spontaneous remission No Possible
Preferred treatment Thionamide and perchlorate
Glucocorticoids
Subsequent hypothyroidism No Possible
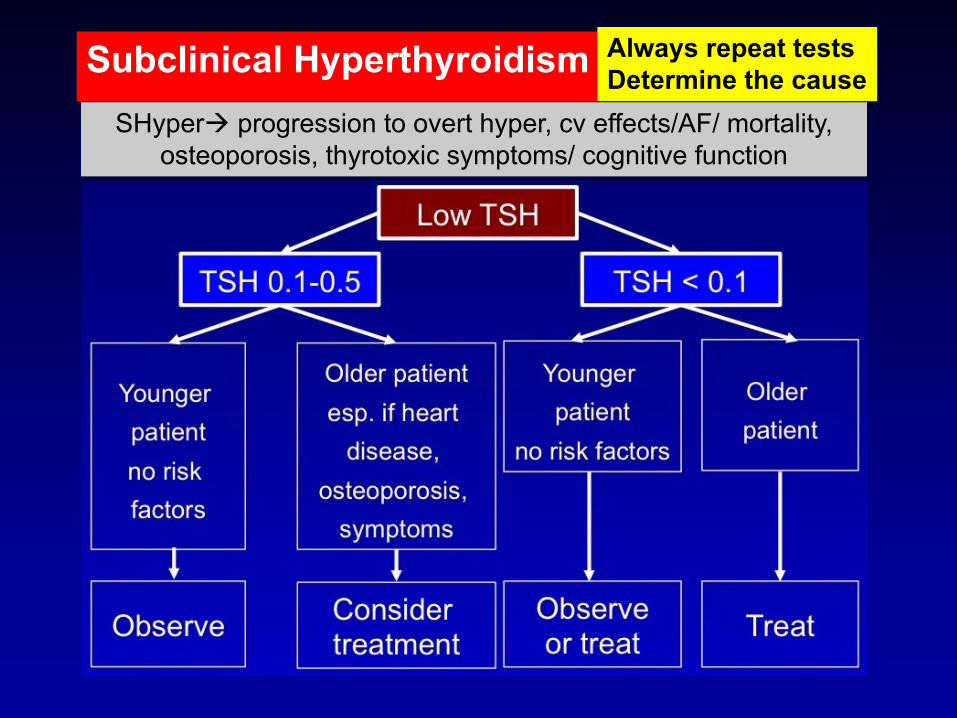
Subclinical Hyperthyroidism Always repeat testsDetermine the cause
SHyperà progression to overt hyper, cv effects/AF/ mortality, osteoporosis, thyrotoxic symptoms/ cognitive function

Hypothyroidism• Etiology: Hashimoto’s thyroiditis, Post Sx/I-131
Graves’ disease, drug (amiodarone, lithium)
• Always evaluate Hypo in bilat CTS, dementia
• éLDL, anemia, hypoNa, éPRL
• Suspected central hypothyroidism à check
cortisol before initiate LT4
Treatment of Hypothyroidism• L-thyroxine (LT4) replacement
– Dose 1.6 ug/kg/day, once daily; before meal
– Absorption site: duodenum, jejunum
• Interference: calcium, iron, PPI, sucralfate, cholestyramine, soybean formula, IBD
– T1/2 7 days: F/U TSH at 4-6 weeks after start LT4
then q 3-6 months
– Old age, CAD risk: start low and slowly titrate up
– Pregnancy: 25-30% édose prepregnancy doseIBD = inflammatory bowel disease

Quiz #760-yr-old maleFatigue, constipation, cold intoleranceSquamous cell CA of tonsil Rx with radiation 3 yrs agoExam: dry skin, mild periorbital edema, no goiter, hyporeflexiaLab: Hb 11 g/dL, Na 129, TSH 1.4 mU/L (0.3-4)
What is the most appropriate next step?A. FT4 measurementB. Repeat TSH measurement in 4 wksC. TPO Ab measurementD. Thyroid scintigraphyE. Thyroid ultrasound

Beck-Peccoz P, et al. Nat Rev Endocrinol. 2017;13(10):588-598.
Central hypothyroidism
FT4
TSH
Quiz #7 Answer: A. FT4 measurement
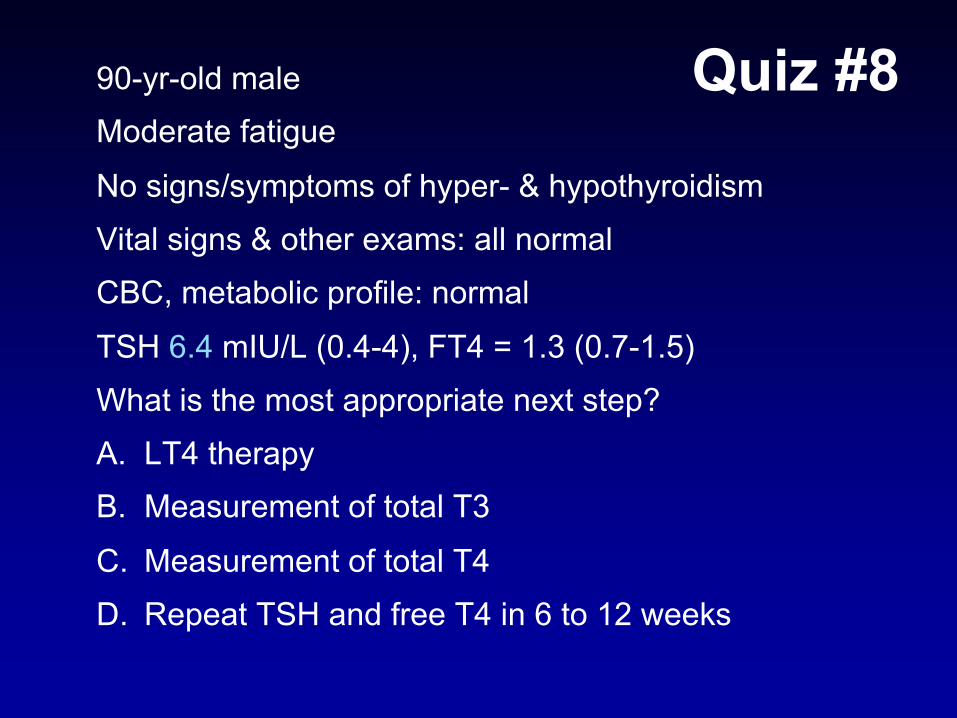
Quiz #890-yr-old maleModerate fatigue
No signs/symptoms of hyper- & hypothyroidismVital signs & other exams: all normalCBC, metabolic profile: normalTSH 6.4 mIU/L (0.4-4), FT4 = 1.3 (0.7-1.5)What is the most appropriate next step?A. LT4 therapyB. Measurement of total T3
C. Measurement of total T4D. Repeat TSH and free T4 in 6 to 12 weeks
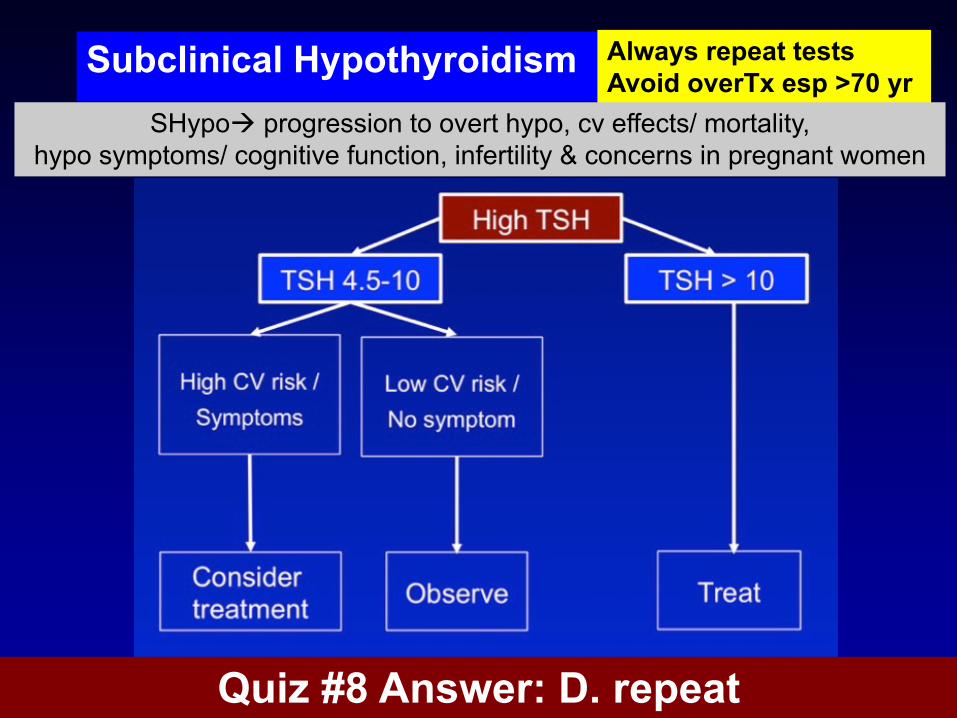
Subclinical Hypothyroidism Always repeat testsAvoid overTx esp >70 yr
SHypoà progression to overt hypo, cv effects/ mortality, hypo symptoms/ cognitive function, infertility & concerns in pregnant women
Quiz #8 Answer: D. repeat
Changes in Thyroid Physiology in Gestation• Increased renal iodide clearance
– Effect on goiter (depending on dietary iodine)
• Binding protein changes (éTBG, êalbumin)– Increase total T4 and total T3
– FT4 assay issue
• First trimester increase in beta-hCG– Decrease in TSH concentration
• Increased degradation of T4 and T3 by placental type 3 deiodinase
TBG, thyroxine-binding globulin
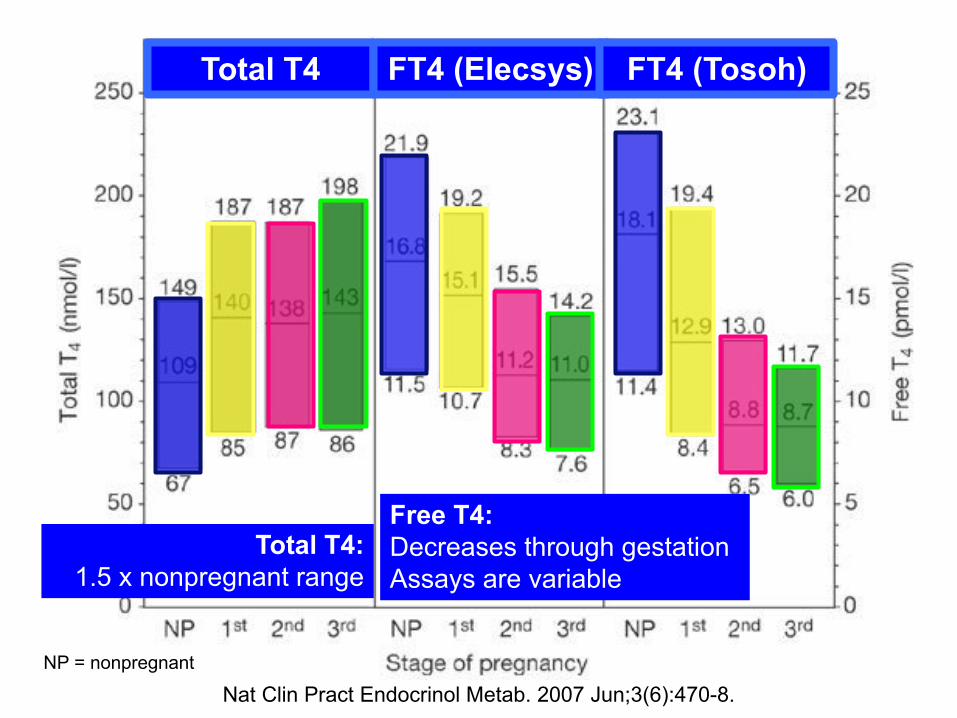
Nat Clin Pract Endocrinol Metab. 2007 Jun;3(6):470-8.
Total T4: 1.5 x nonpregnant range
Free T4: Decreases through gestationAssays are variable
Total T4 FT4 (Elecsys) FT4 (Tosoh)
NP = nonpregnant

0-7 weeks 7-16 weeks 17 - 40 weeks
FT4 FT4TT4 (GA-specific range)
TT4 (GA-specific range)
TT4 pregnant range = 1.5 X nonpregnant rangeTT4 é
5 % per w
k
5%X10 weeks = 50 %
50%
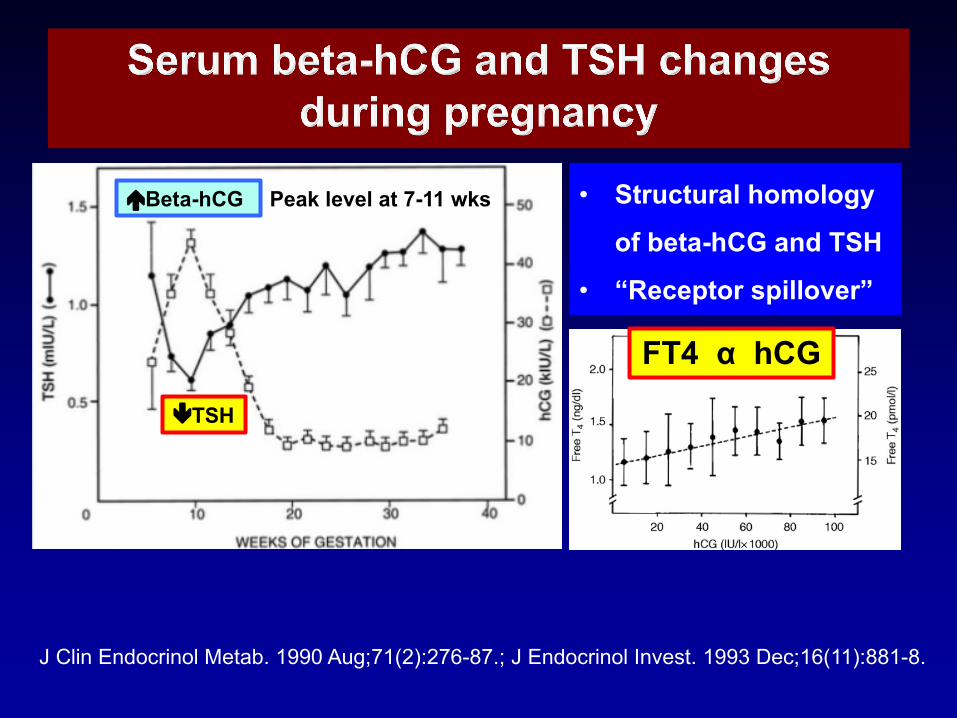
J Clin Endocrinol Metab. 1990 Aug;71(2):276-87.; J Endocrinol Invest. 1993 Dec;16(11):881-8.
éBeta-hCG
êTSH
• Structural homology
of beta-hCG and TSH
• “Receptor spillover”
Peak level at 7-11 wks
FT4 α hCG
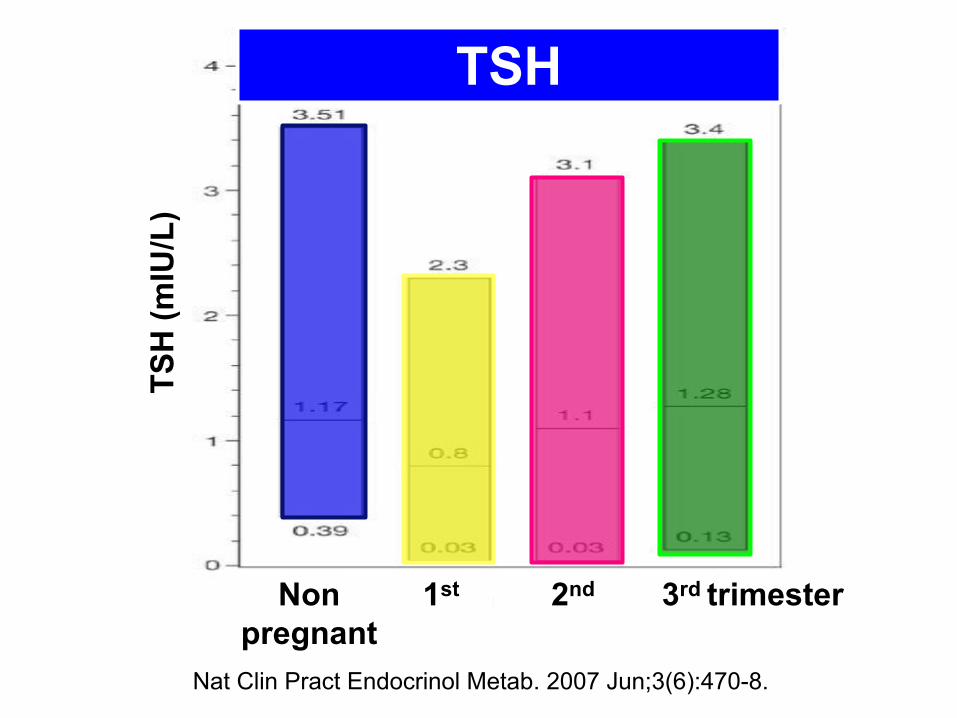
Nat Clin Pract Endocrinol Metab. 2007 Jun;3(6):470-8.
TSHTS
H (m
IU/L
)
Nonpregnant
1st 2nd 3rd trimester
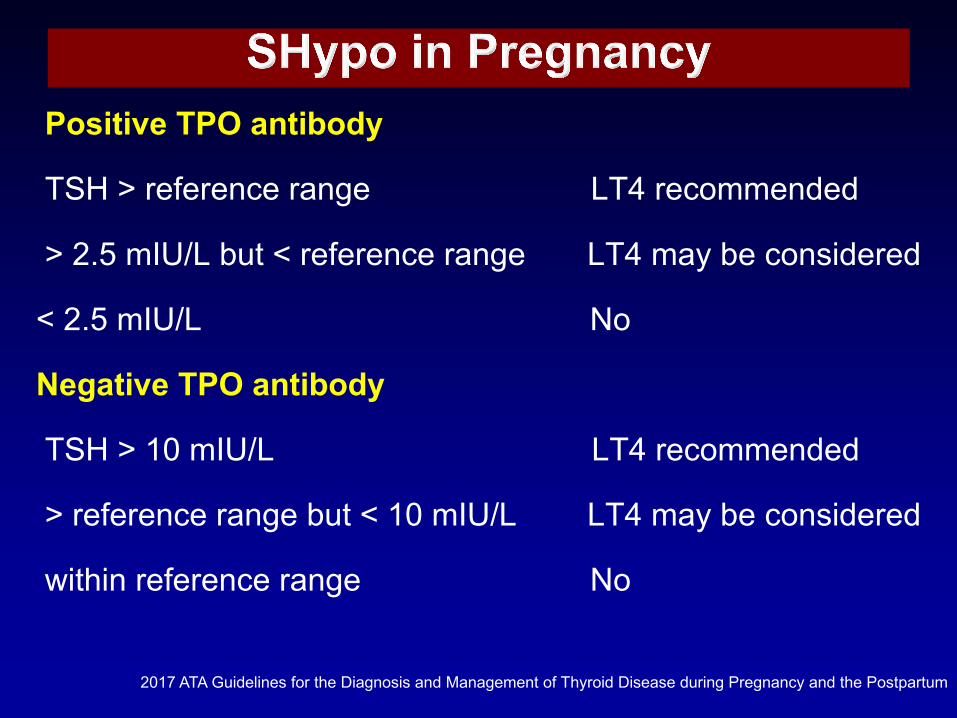
Positive TPO antibody
TSH > reference range LT4 recommended
> 2.5 mIU/L but < reference range LT4 may be considered
< 2.5 mIU/L No
Negative TPO antibody
TSH > 10 mIU/L LT4 recommended
> reference range but < 10 mIU/L LT4 may be considered
within reference range No
2017 ATA Guidelines for the Diagnosis and Management of Thyroid Disease during Pregnancy and the Postpartum
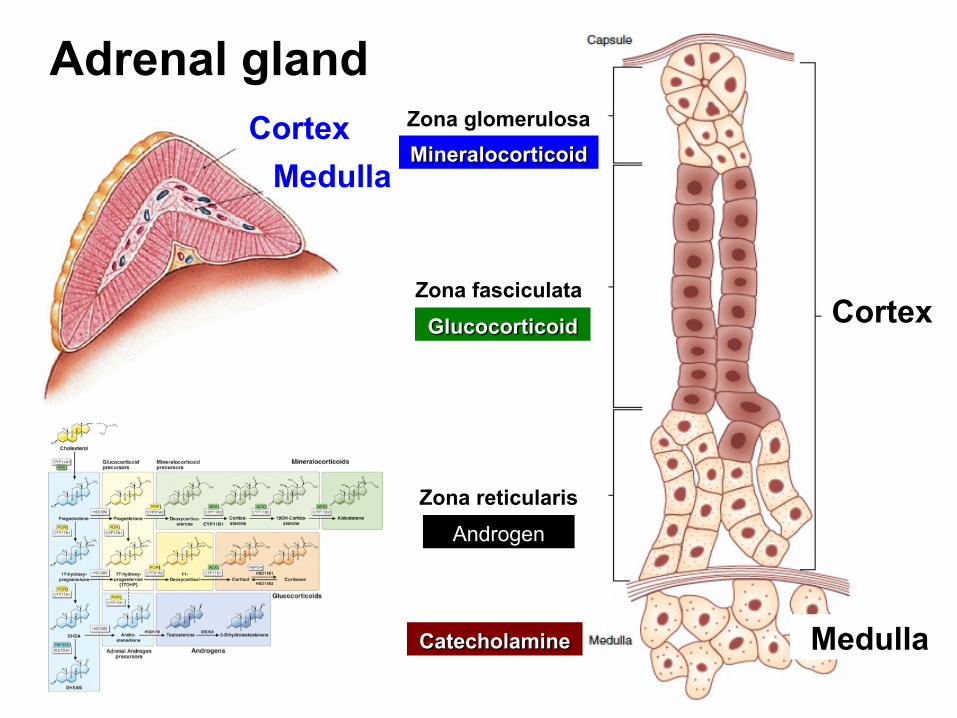
CortexMedulla
Cortex
Medulla
Zona glomerulosa
Zona fasciculata
Zona reticularis
Adrenal gland
Mineralocorticoid
Glucocorticoid
Androgen
Catecholamine
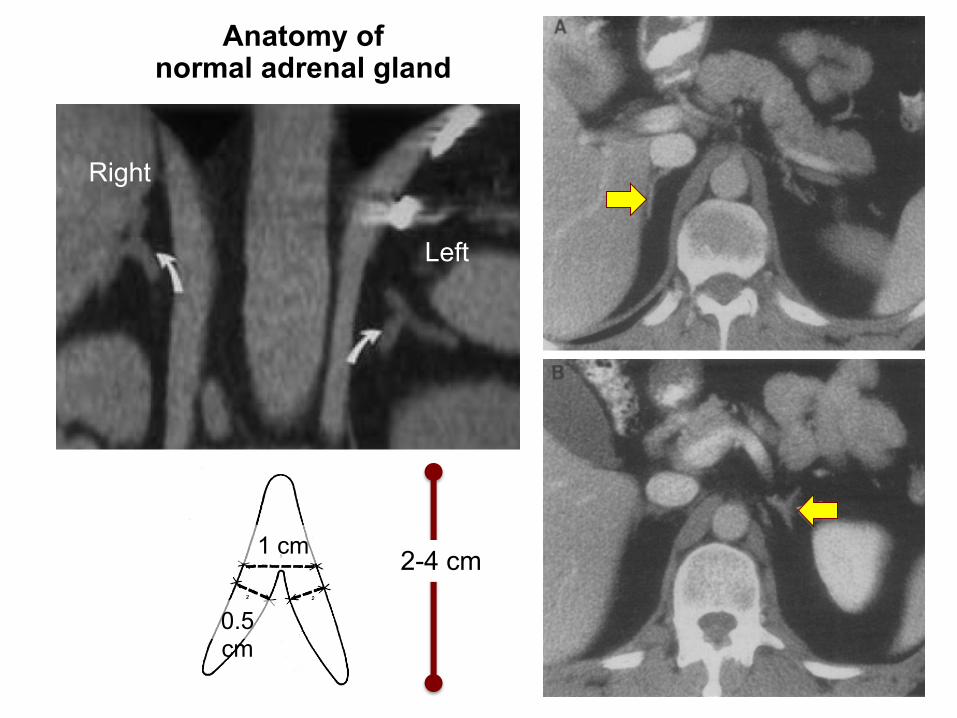
Anatomy of normal adrenal gland
Right
Left
2-4 cm1 cm
0.5 cm
Adrenal gland disorders that internists should know
• Adrenal cortex– Cushing’s syndrome– Primary hyperaldosteronism– Adrenal incidentaloma– Adrenal insufficiency– Congenital adrenal hyperplasia (CAH)
• Adrenal Medulla– Pheochromocytoma

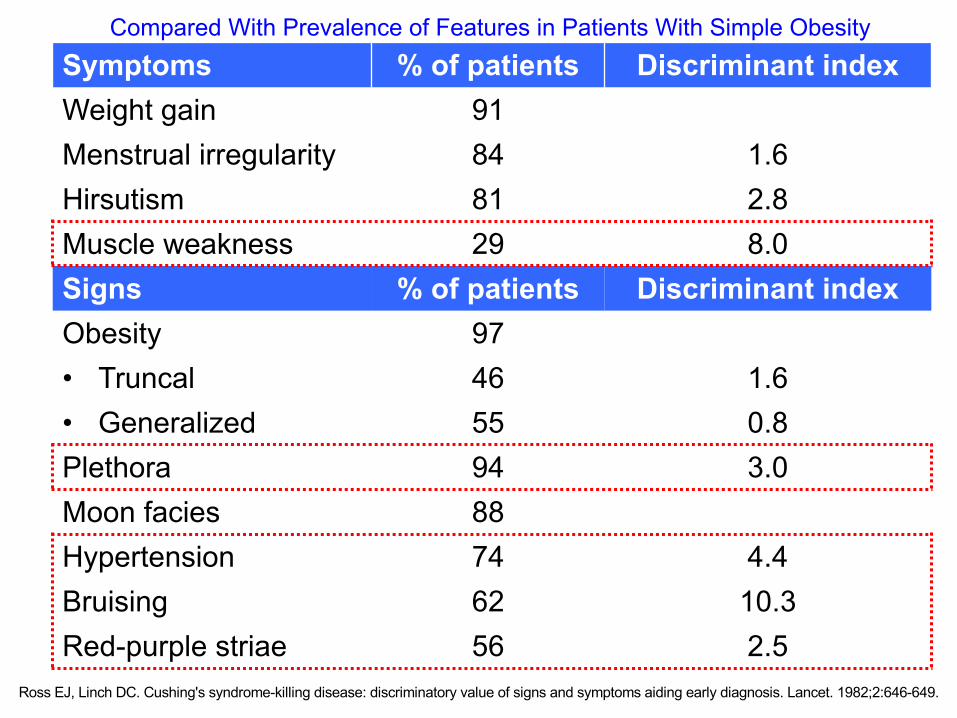
Ross EJ, Linch DC. Cushing's syndrome-killing disease: discriminatory value of signs and symptoms aiding early diagnosis. Lancet. 1982;2:646-649.
Symptoms % of patients Discriminant indexWeight gain 91Menstrual irregularity 84 1.6Hirsutism 81 2.8Muscle weakness 29 8.0Signs % of patients Discriminant indexObesity 97• Truncal 46 1.6• Generalized 55 0.8Plethora 94 3.0Moon facies 88Hypertension 74 4.4Bruising 62 10.3Red-purple striae 56 2.5
Compared With Prevalence of Features in Patients With Simple Obesity

Etiologies of Cushing’s Syndrome
ACTH-dependent• Pituitary CS
• Ectopic ACTH
• Ectopic CRH
• Exogenous ACTH
ACTH-independent• Adrenal adenoma• Adrenal CA
• Micronodular hyperplasia– PPNAD
• Macronodular hyperplasia– BMAH
Pituitary Cushing = Cushing’s disease
PPNAD Primary pigmented nodular adrenal disease
BMAH bilateral macronodular adrenal hyperplasia
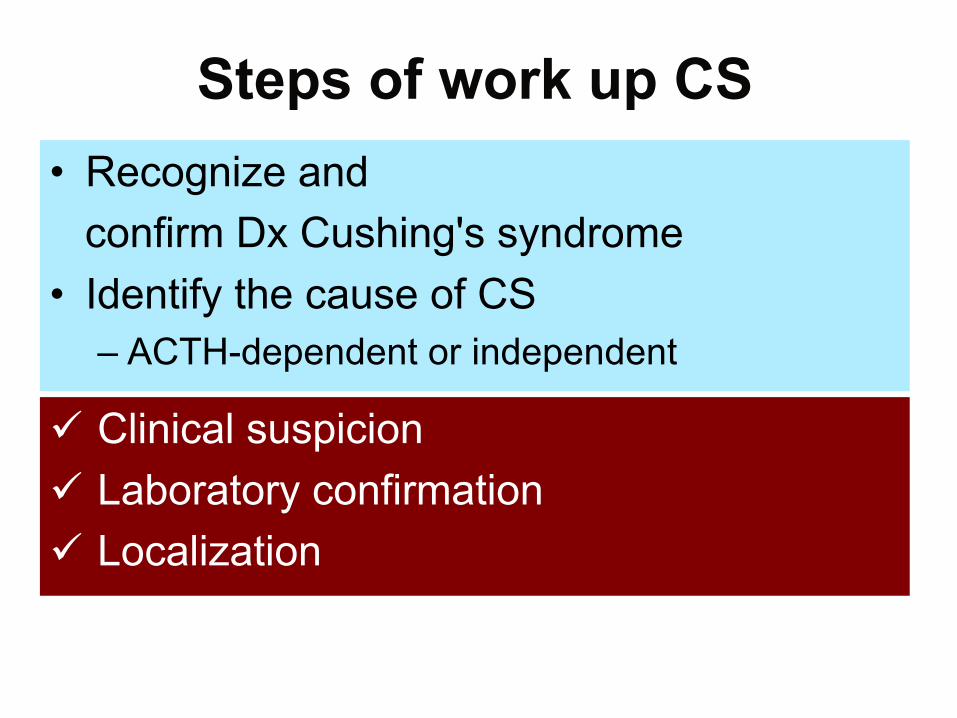
Steps of work up CS• Recognize and
confirm Dx Cushing's syndrome• Identify the cause of CS
– ACTH-dependent or independent
ü Clinical suspicionü Laboratory confirmationü Localization
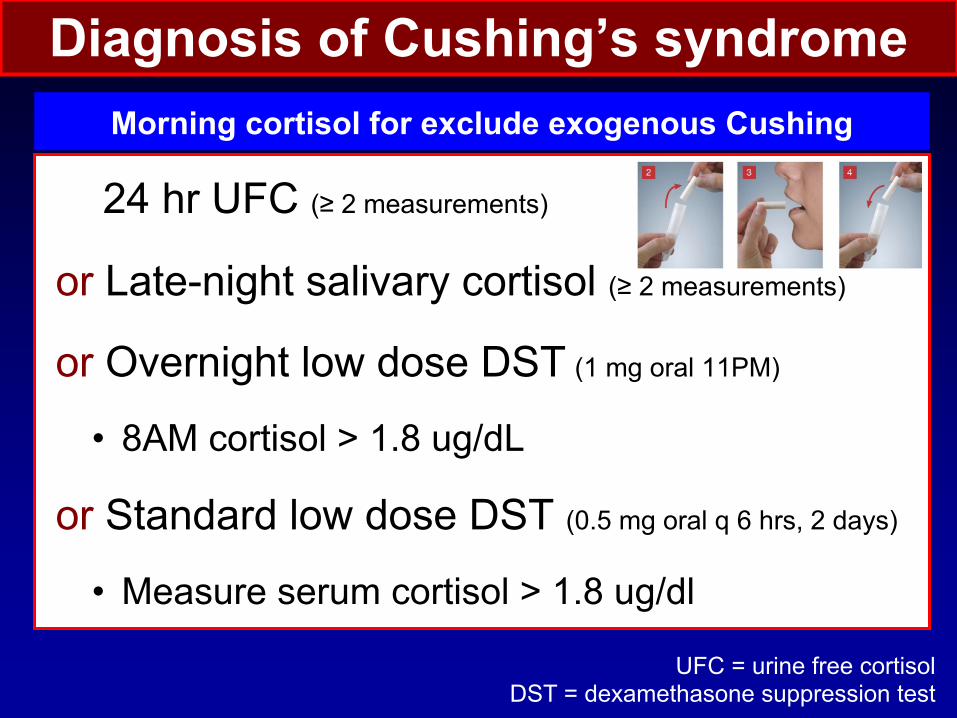
Diagnosis of Cushing’s syndrome
24 hr UFC (≥ 2 measurements)
or Late-night salivary cortisol (≥ 2 measurements)
or Overnight low dose DST (1 mg oral 11PM)
• 8AM cortisol > 1.8 ug/dL
or Standard low dose DST (0.5 mg oral q 6 hrs, 2 days)
• Measure serum cortisol > 1.8 ug/dl
UFC = urine free cortisolDST = dexamethasone suppression test
Morning cortisol for exclude exogenous Cushing
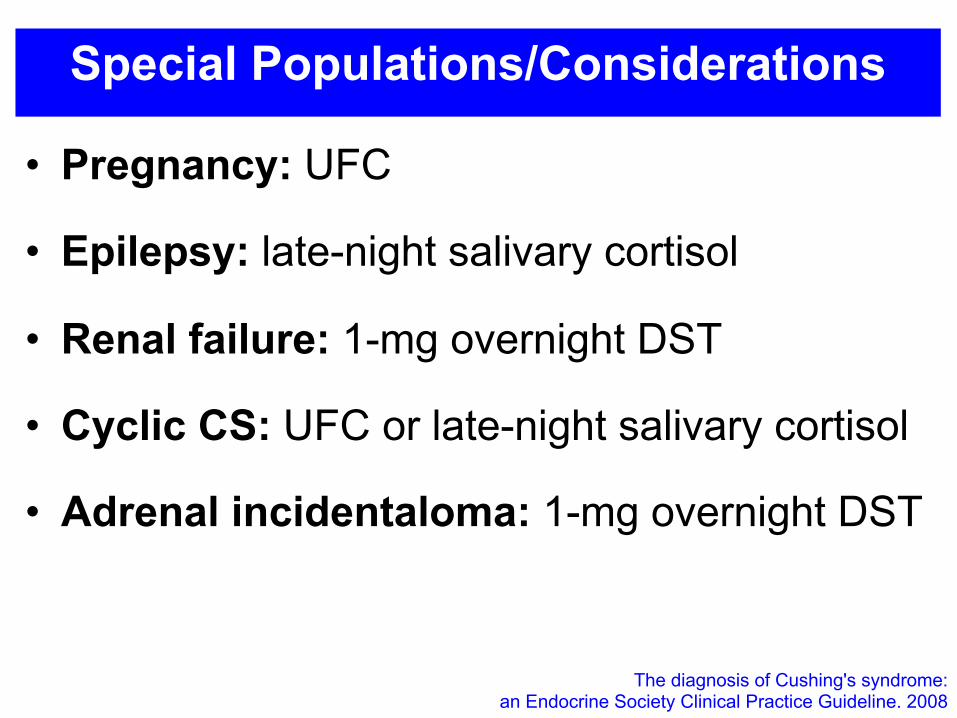
Special Populations/Considerations
• Pregnancy: UFC
• Epilepsy: late-night salivary cortisol
• Renal failure: 1-mg overnight DST
• Cyclic CS: UFC or late-night salivary cortisol
• Adrenal incidentaloma: 1-mg overnight DST
The diagnosis of Cushing's syndrome: an Endocrine Society Clinical Practice Guideline. 2008

ACTH dependent vs independent
ACTH
ACTH dependent
ACTH > 20 pg/ml
Pituitary adenoma
Ectopic ACTH or
CRH producing tumors
Adrenal adenoma
Adrenal carcinoma
ACTH independent
ACTH < 10 pg/ml
CT adrenal
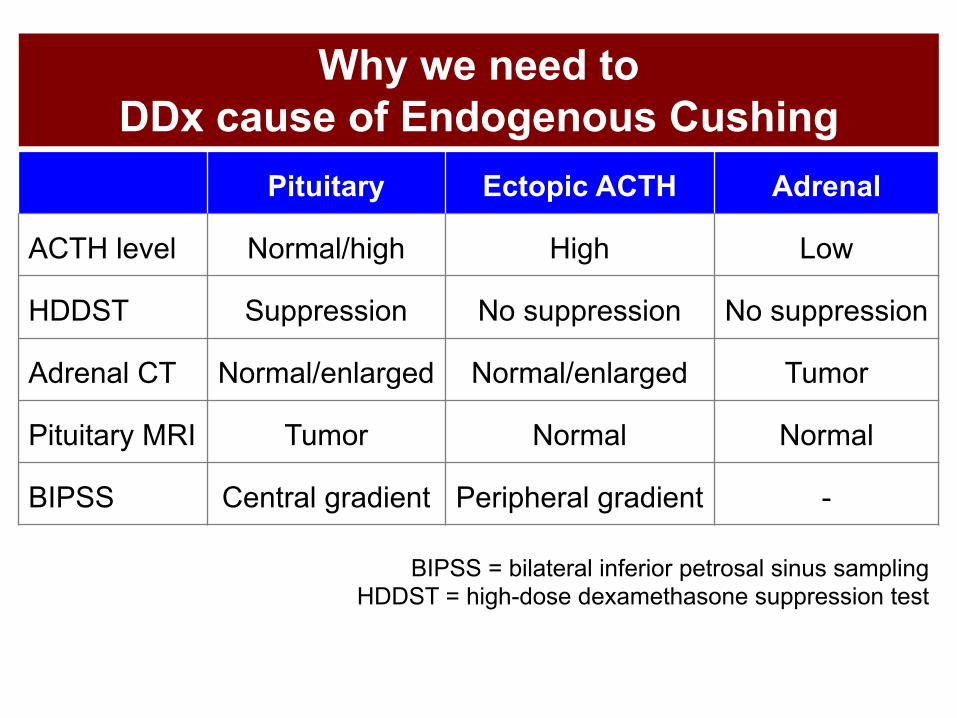
Why we need to DDx cause of Endogenous Cushing
Pituitary Ectopic ACTH Adrenal
ACTH level Normal/high High Low
HDDST Suppression No suppression No suppression
Adrenal CT Normal/enlarged Normal/enlarged Tumor
Pituitary MRI Tumor Normal Normal
BIPSS Central gradient Peripheral gradient -
BIPSS = bilateral inferior petrosal sinus samplingHDDST = high-dose dexamethasone suppression test
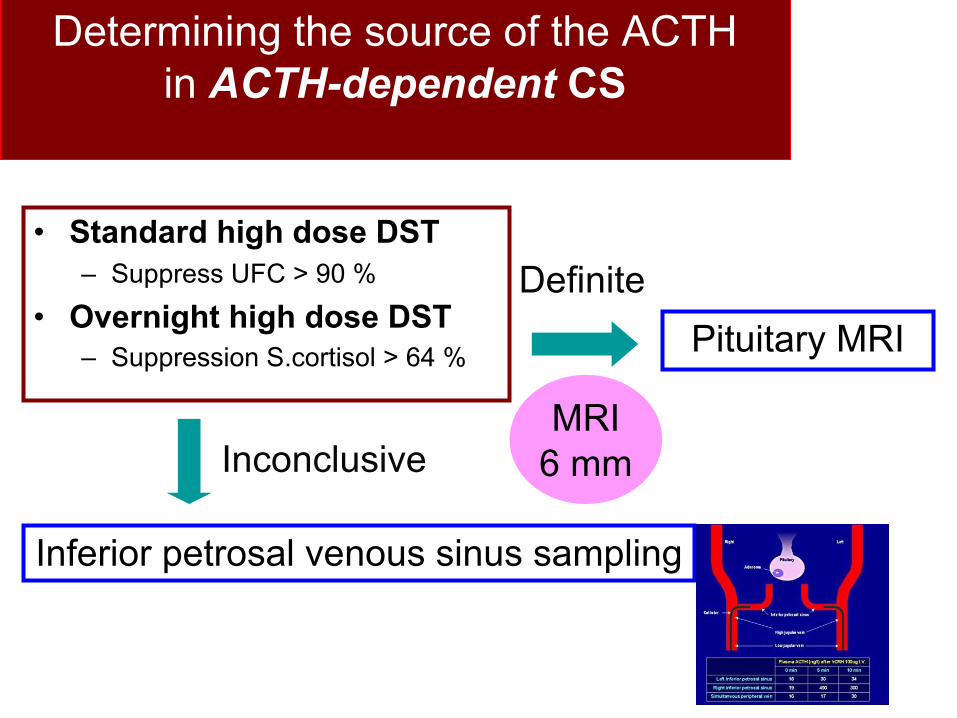
Determining the source of the ACTH in ACTH-dependent CS
• Standard high dose DST– Suppress UFC > 90 %
• Overnight high dose DST– Suppression S.cortisol > 64 %
Inferior petrosal venous sinus sampling
Inconclusive
DefinitePituitary MRI
MRI6 mm
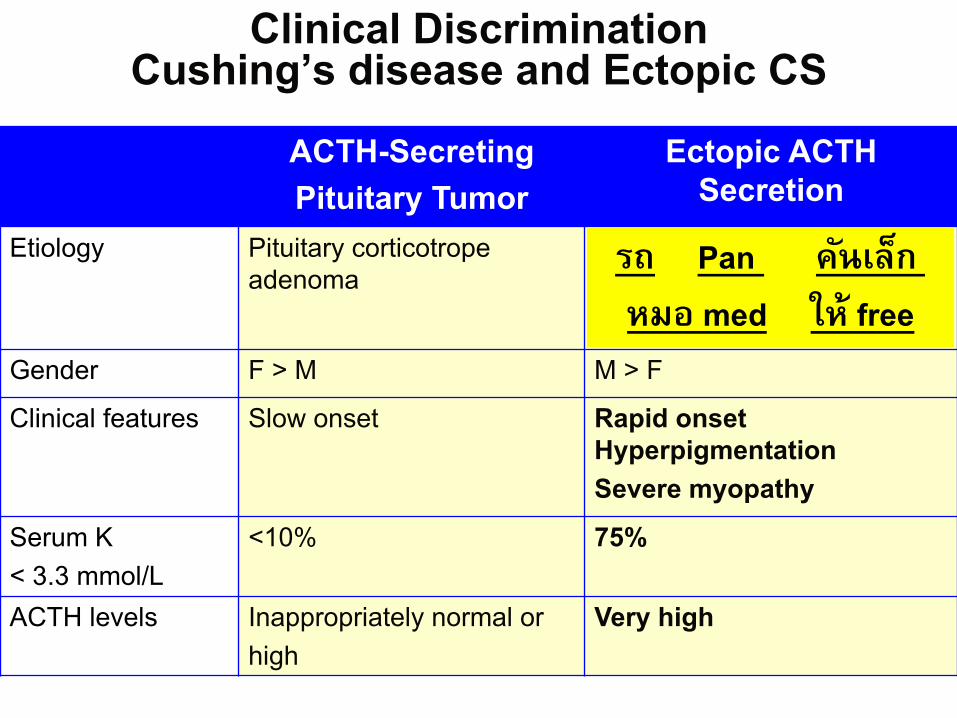
Clinical Discrimination Cushing’s disease and Ectopic CS
ACTH-Secreting Pituitary Tumor
Ectopic ACTH Secretion
Etiology Pituitary corticotrope adenoma
Bronchial, abdominal carcinoidSC lung cancer Thymoma
Gender F > M M > F
Clinical features Slow onset Rapid onsetHyperpigmentation Severe myopathy
Serum K < 3.3 mmol/L
<10% 75%
ACTH levels Inappropriately normal or high
Very high
รถ Pan คนัเลก็
หมอ med ให้ free
Treatment• Surgery• Pituitary irradiation• Medical therapy
– KetoconazoleSE: Elevated hepatic transaminases, gynecomastia, impotence, GI upset, edema
– Metyrapone
– Mitotane– Aminoglutethimide– Etomidate; IV form
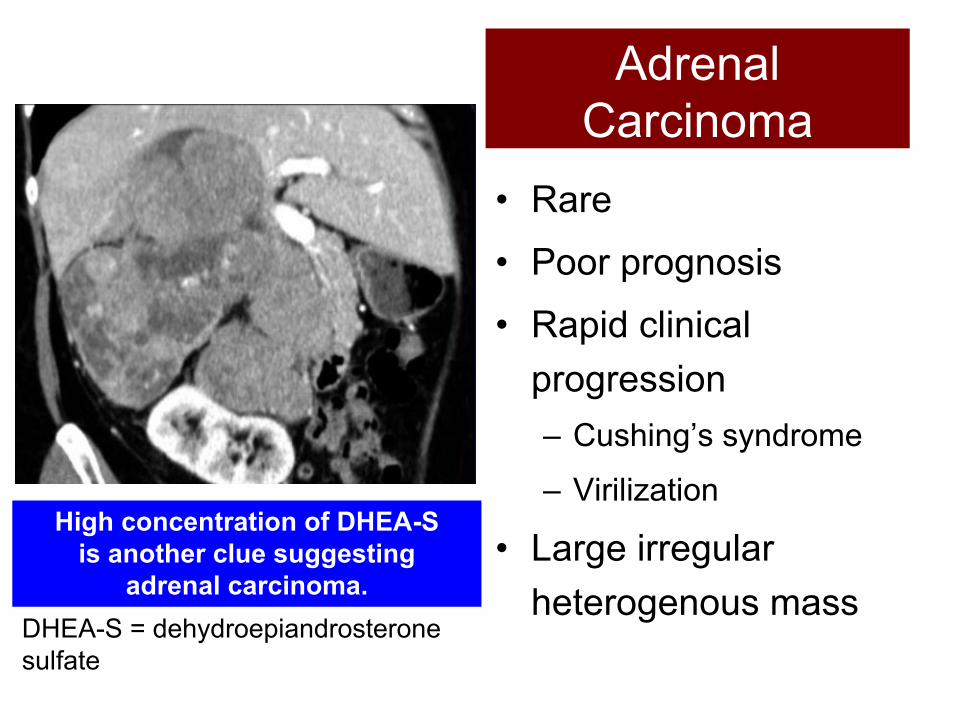
Adrenal Carcinoma
• Rare• Poor prognosis• Rapid clinical
progression– Cushing’s syndrome
– Virilization
• Large irregular heterogenous mass
High concentration of DHEA-S is another clue suggesting
adrenal carcinoma.DHEA-S = dehydroepiandrosterone sulfate
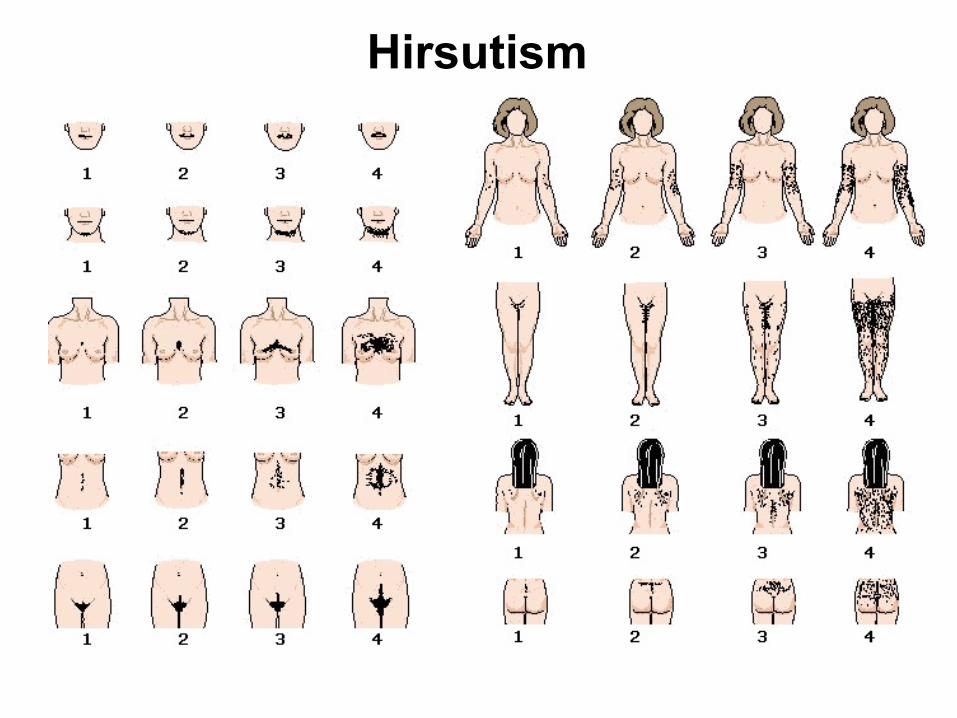
Hirsutism
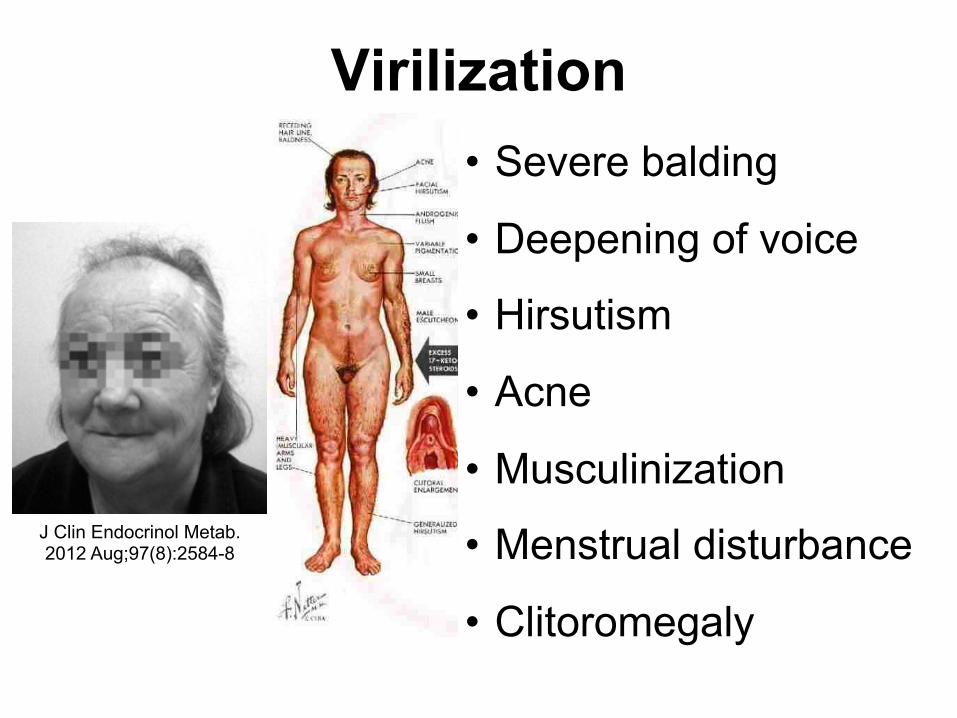
Virilization
J Clin Endocrinol Metab. 2012 Aug;97(8):2584-8
• Severe balding
• Deepening of voice
• Hirsutism
• Acne
• Musculinization
• Menstrual disturbance
• Clitoromegaly
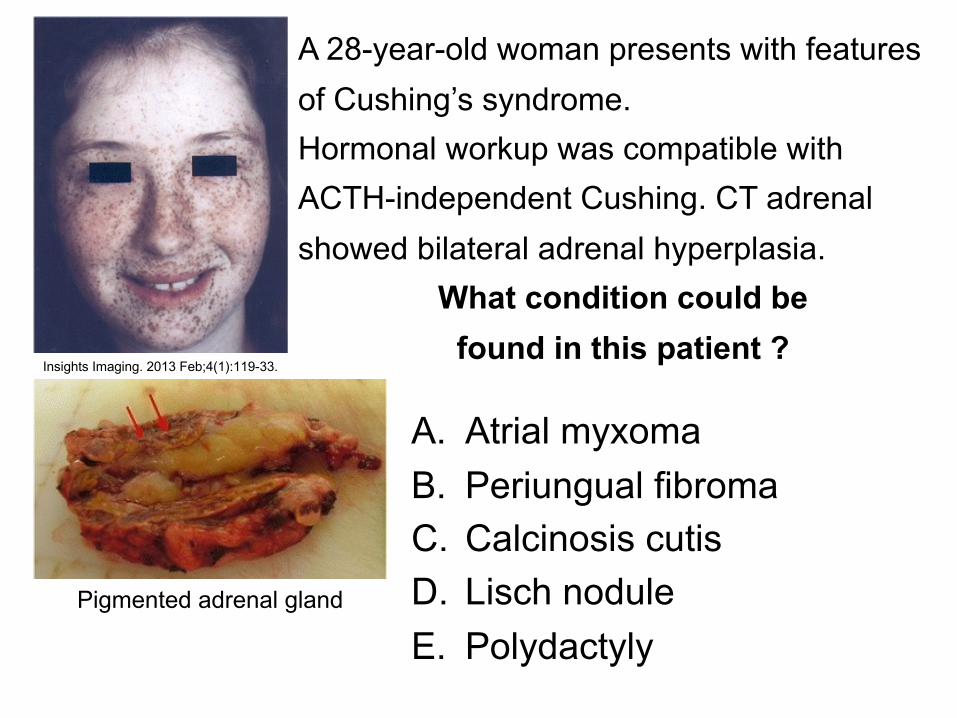
Insights Imaging. 2013 Feb;4(1):119-33.
A 28-year-old woman presents with features of Cushing’s syndrome. Hormonal workup was compatible with ACTH-independent Cushing. CT adrenal showed bilateral adrenal hyperplasia.
What condition could be found in this patient ?
A. Atrial myxomaB. Periungual fibromaC. Calcinosis cutisD. Lisch noduleE. Polydactyly
Pigmented adrenal gland

Insights Imaging. 2013 Feb;4(1):119-33.
Answer: A. Atrial MyxomaSpotty skin pigmentation
Epithelioid blue-nevi
Atrial myxoma Primary pigmented nodular adrenocortical
disease (PPNAD)
Carney complex: a rare multiple familial neoplasia syndrome that is characterized by multiple types of skin tumors and pigmented lesions, endocrine neoplasms, myxomas and schwannomas
Acromegaly Mammary myxoma
Schwannoma Testicular tumor
Cutaneous myxoma

Complications of Cushing’s Syndrome
Lancet Diabetes Endocrinol. 2016 Jul;4(7):611-29.
Quiz #930-yr-old maleCushingoid appearance, new-onset DM
BP 160/90, BMI 30Overnight low dose DEX suppression: cortisol 9 ug/dL24-hr urine free cortisol > 5xULNUndetectable ACTH level Which of the following is the most appropriate next step?A. MRI pituitaryB. CT adrenal
C. Late-night salivary cortisolD. Inferior petrosal sinus sampling
Quiz #9 Answer: B. CT adrenal
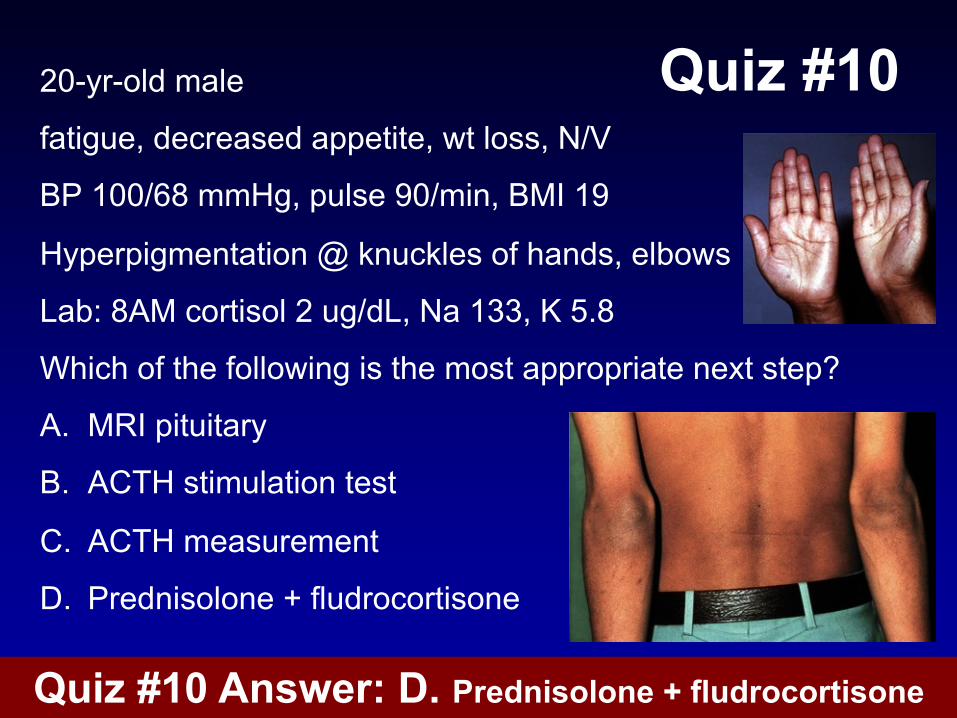
Quiz #1020-yr-old male
fatigue, decreased appetite, wt loss, N/V
BP 100/68 mmHg, pulse 90/min, BMI 19
Hyperpigmentation @ knuckles of hands, elbows
Lab: 8AM cortisol 2 ug/dL, Na 133, K 5.8
Which of the following is the most appropriate next step?
A. MRI pituitary
B. ACTH stimulation test
C. ACTH measurement
D. Prednisolone + fludrocortisone
Quiz #10 Answer: D. Prednisolone + fludrocortisone
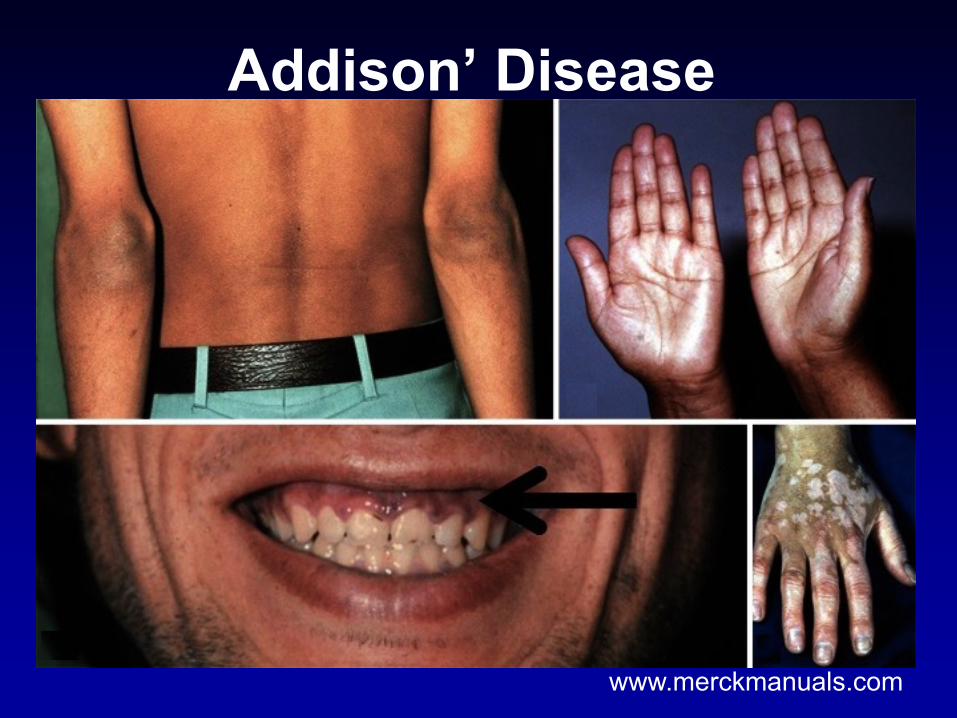
Addison’ Disease
www.merckmanuals.com
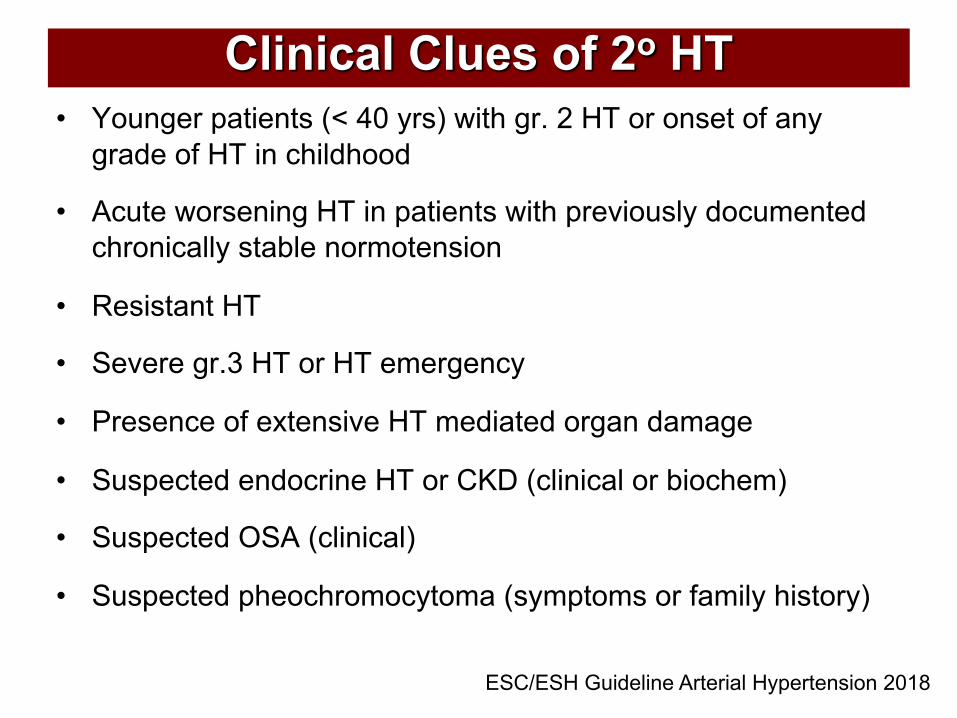
Clinical Clues of 2o HT• Younger patients (< 40 yrs) with gr. 2 HT or onset of any
grade of HT in childhood
• Acute worsening HT in patients with previously documented chronically stable normotension
• Resistant HT
• Severe gr.3 HT or HT emergency
• Presence of extensive HT mediated organ damage
• Suspected endocrine HT or CKD (clinical or biochem)
• Suspected OSA (clinical)
• Suspected pheochromocytoma (symptoms or family history)
ESC/ESH Guideline Arterial Hypertension 2018

Clinical evaluation of 2o HT• Drugs
• Family history
• Pulse, BP 4 extremities
• Orthostatic hypotension
• Abdominal bruit
• Bimanual palpation
• Hx hypoK/proximal m weakness
• Paroxysm
• OSA symptoms
• Signs of Cushing, hyper-, hypothyroidism
• Hx hyperCa (hyperPTH)
NSAIDsOral contraceptivesSympathomimeticCyclosporineTacrolimusErythropoietinVEGF inhibitorTKIAlcoholCocaineAmphetamineAntidepressantsGlucocorticoidMineralocorticoidLiquorice
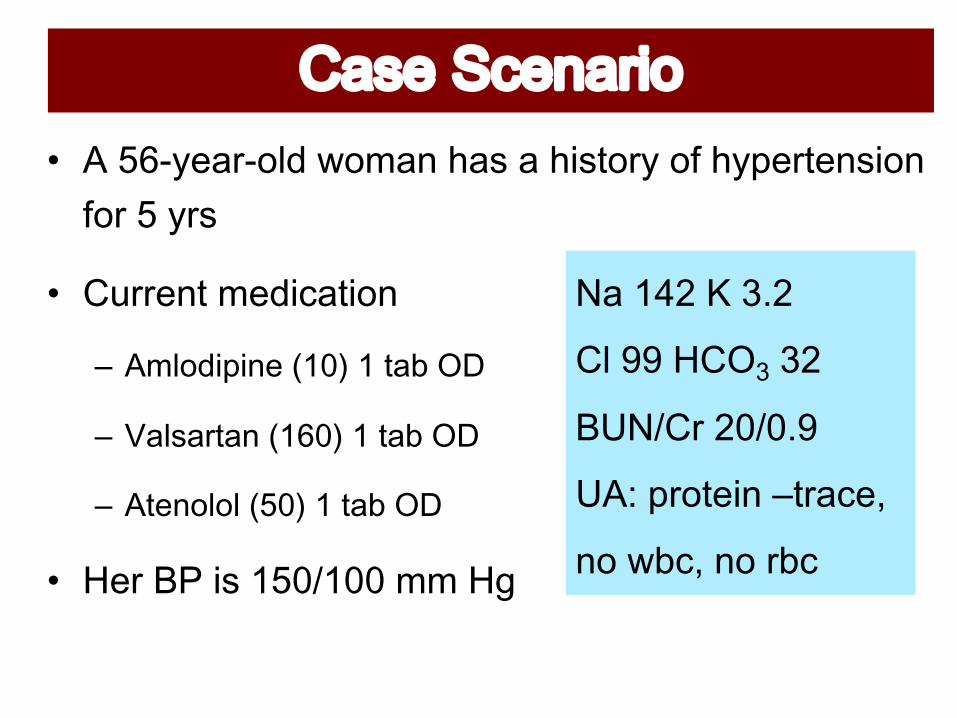
!"#$%&'$(")*+• C+<IF-(1%F&3B+G&51)+,1#+1+,/#$&%-+&7+,-.(%$()#/&)+7&%+<+-%#
• J9%%()$+5(B/01$/&)
– =48*3&/&)0#>,?@#,#2'6#A%
– B'8+'12')#>,C?@#,#2'6#A%
– =20)*8*8#>D?@#,#2'6#A%
• K(%+LM+/#+N<OPNOO+55+K'+
Na 142 K 3.2
Cl 99 HCO3 32
BUN/Cr 20/0.9
UA: protein –trace,
no wbc, no rbc
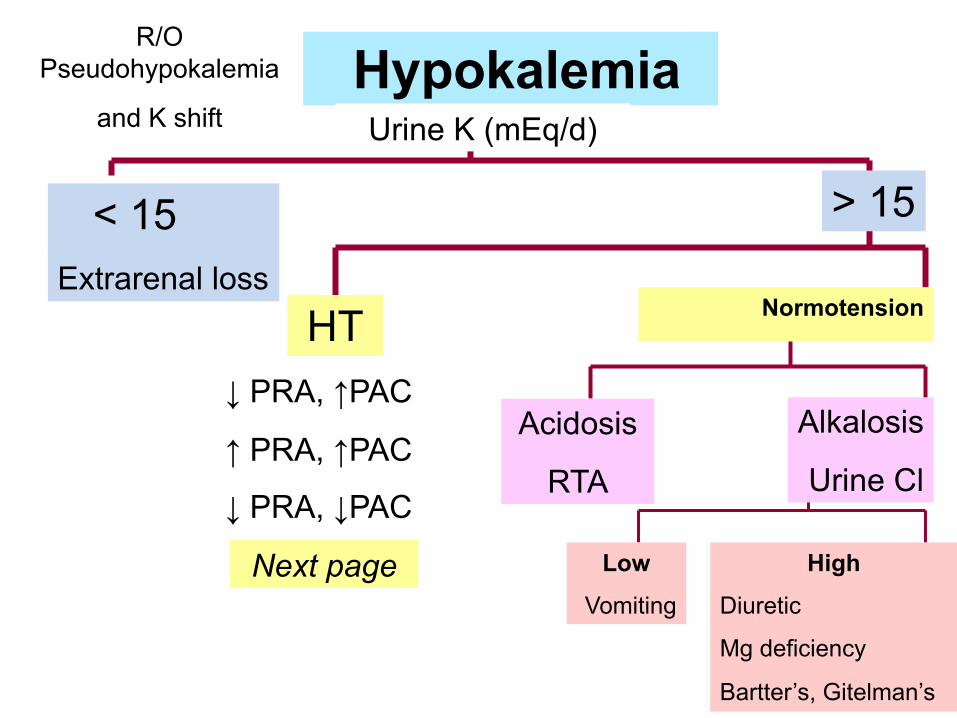
HypokalemiaR/O
Pseudohypokalemia
and K shift Urine K (mEq/d)
< 15Extrarenal loss
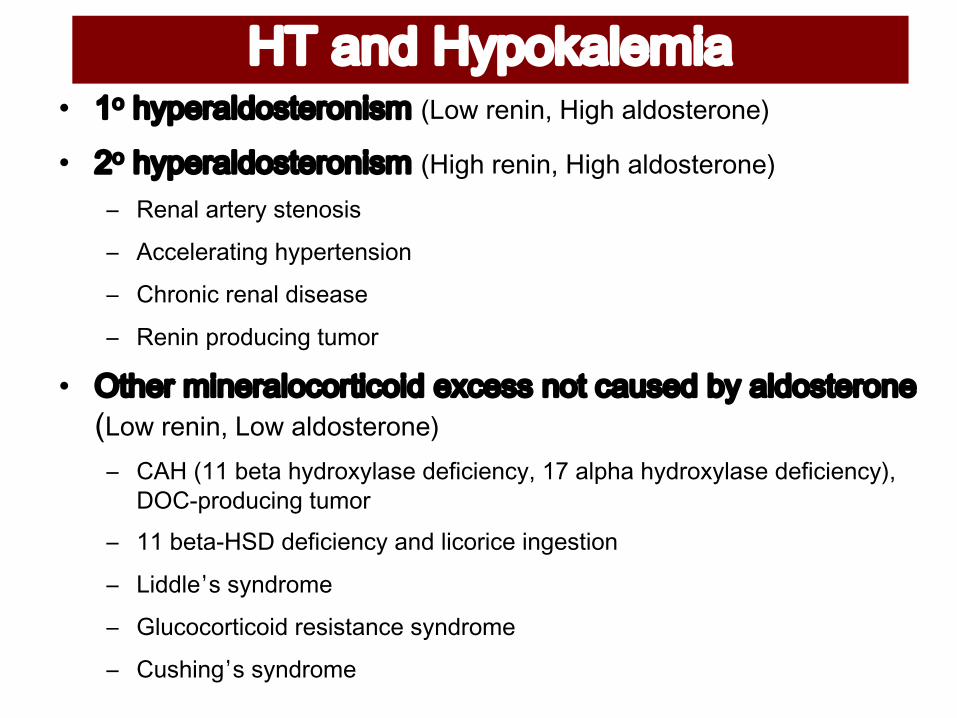
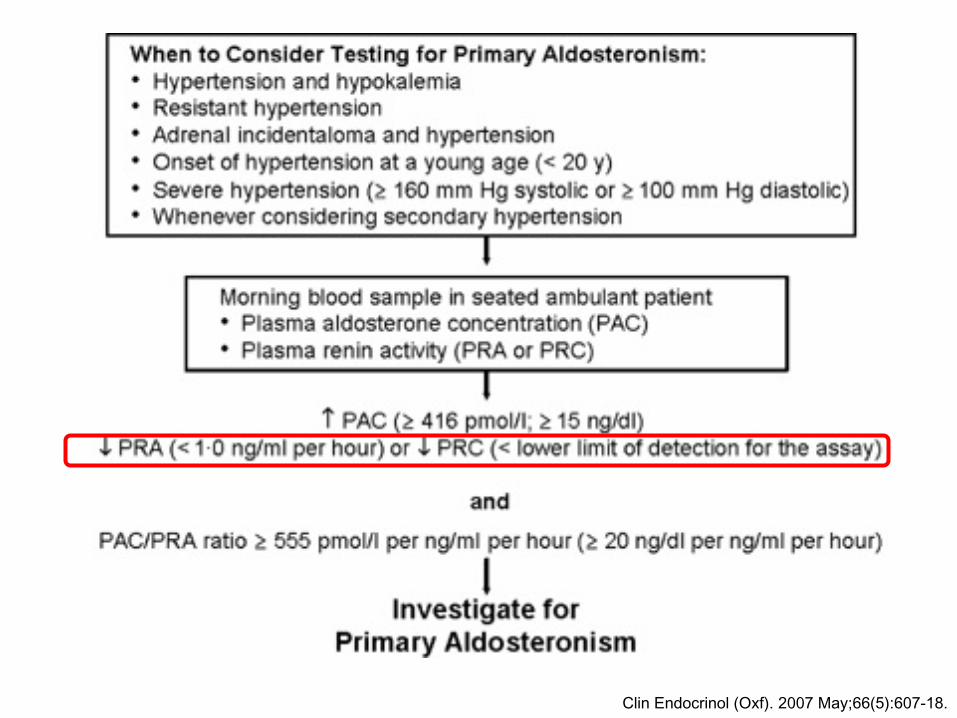
HT↓ PRA, ↑PAC
↑ PRA, ↑PAC
↓ PRA, ↓PAC
Acidosis
RTA
LowVomiting
HighDiuretic
Mg deficiency
Bartter’s, Gitelman’s
> 15
Alkalosis
Urine Cl
Normotension
Next page
!"#$%&#!'()*$+,-.$E ,! -./01'83*+201*)&+4 !"#$%&'()(*%+),-%./0#12'&#('3E F! -./01'83*+201*)&+4#!+),-%&'()(*%+),-%./0#12'&#('3
! "#$%&'%()#(*'+)#$,+-+
! .//#&#(%)-$0'1*2#()#$+-,$
! 31(,$-/'(#$%&'4-+#%+#
! "#$-$'2(,45/-$0')56,(
E A2-01#4&)01'8*7*12&7*&3#0G70++#)*2#7'5+03#6.#'83*+201*)0>"#$%&'()(*%"#$%./0#12'&#('3! 3.7'899':#)%'1*4(,;*&%+#'4#<-/-#$/*='9>'%&21%'1*4(,;*&%+#'4#<-/-#$/*?='@A3B2(,45/-$0')56,(
! 99':#)%B7C@'4#<-/-#$/*'%$4'&-/,(-/#'-$0#+)-,$
! D-44&#’+'+*$4(,6#
! E&5/,/,()-/,-4'(#+-+)%$/#'+*$4(,6#
! 35+1-$0’+'+*$4(,6#
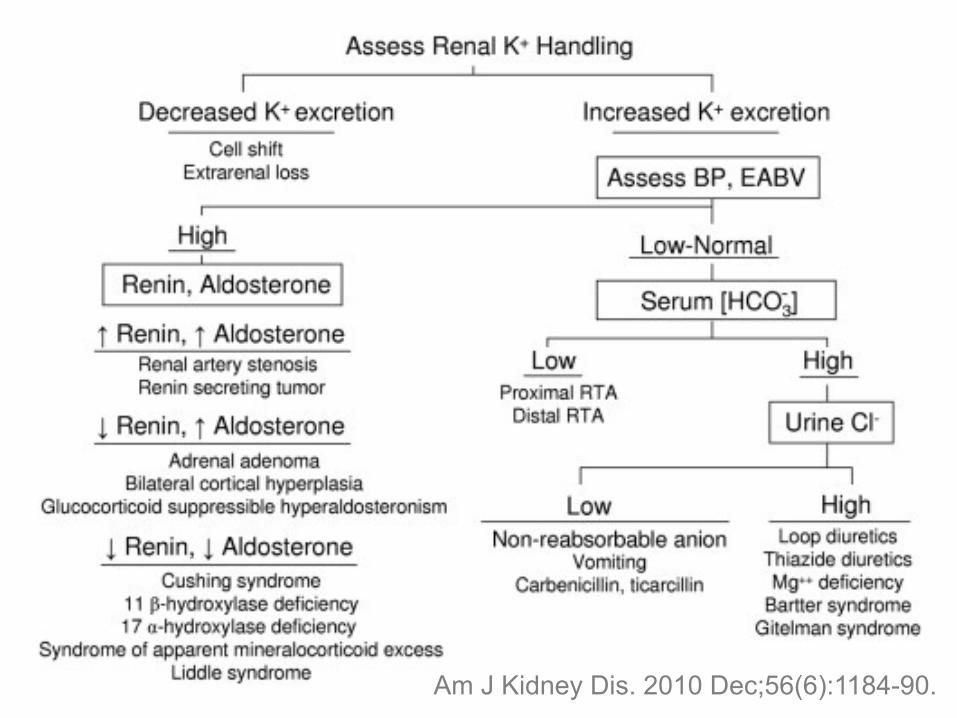
Am J Kidney Dis. 2010 Dec;56(6):1184-90.
M%(.1%1$/&)+&7+$,(+13B&#$(%&)(F%()/)+%1$/&+5(1#9%(5()$
• J&%%(0$+,-.&Q13(5/1+RQ((.+STUV
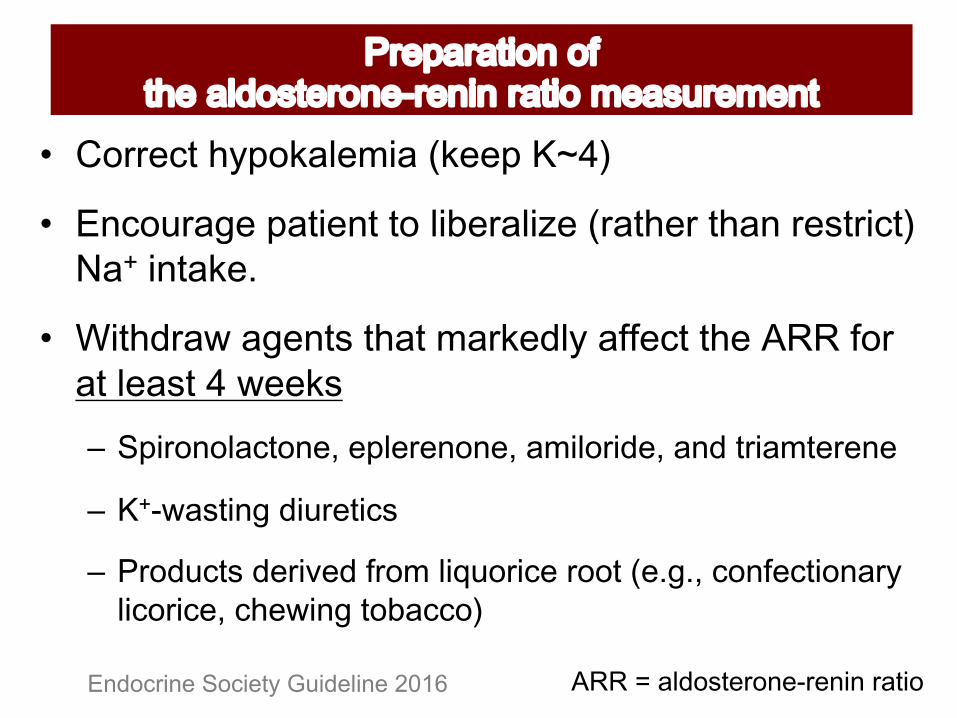
• ")0&9%1'(+.1$/()$+$&+3/?(%13/@(+R%1$,(%+$,1)+%(#$%/0$V+!1! /)$1Q(2
• W/$,B%1G+1'()$#+$,1$+51%Q(B3-+177(0$+$,(+CXX+7&%+1$+3(1#$+U+G((Q#– $/&1*)*8'72*)0H#0/8010)*)0H#'4&8*1&30H#')3#21&'42010)0
– I"JK'+2&)(#3&5102&7+
– L1*3572+#301&M03#N1*4#8&O5*1&70#1**2#>0P(PH#7*)N072&*)'1.#8&7*1&70H#7-0K&)(#2*6'77*@
455%6%./0#12'&#('7&'()(%&.2)#Endocrine Society Guideline 2016
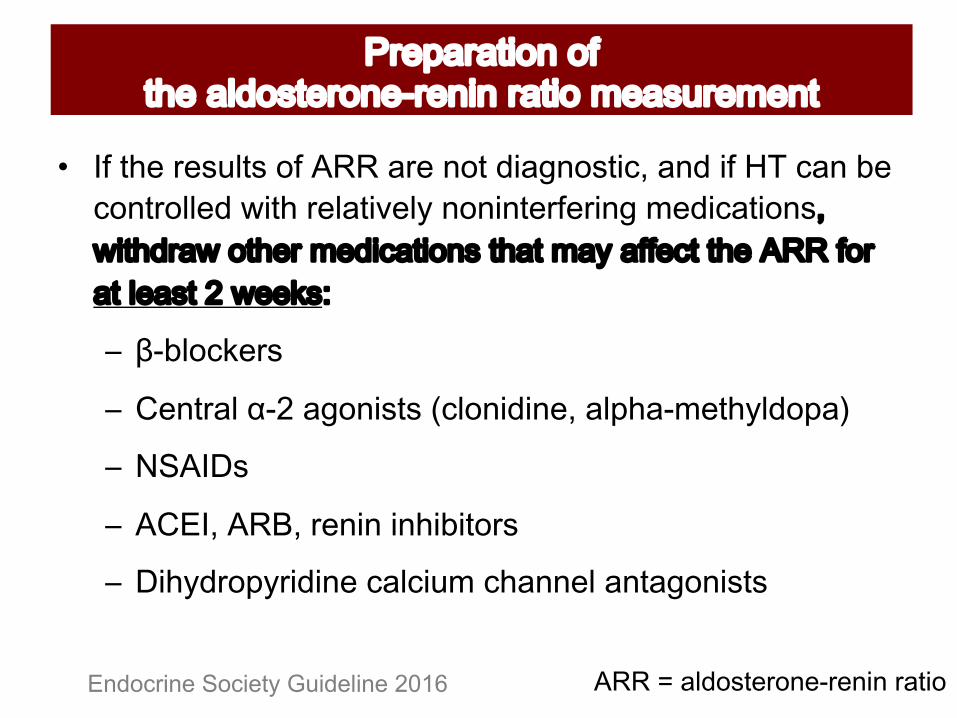
E ;N#2-0#10+582+#*N#=QQ#'10#)*2#3&'()*+2&7H#')3#&N#"!#7')#60#7*)21*8803#K&2-#108'2&M08.#)*)&)201N01&)(#403&7'2&*)+H#K&2-31'K#*2-01#403&7'2&*)+#2-'2#4'.#'NN072#2-0#=QQ#N*1#'2#80'+2#F#K00R+S
T UJ68*7R01+
T <0)21'8#VJF#'(*)&+2+#>78*)&3&)0H#'8/-'J402-.83*/'@
T :$=;%+
T =<W;H#=QXH#10)&)#&)-&6&2*1+
T %&-.31*/.1&3&)0#7'87&54#7-'))08#')2'(*)&+2+
455%6%./0#12'&#('7&'()(%&.2)#Endocrine Society Guideline 2016
M%(.1%1$/&)+&7+$,(+13B&#$(%&)(F%()/)+%1$/&+5(1#9%(5()$
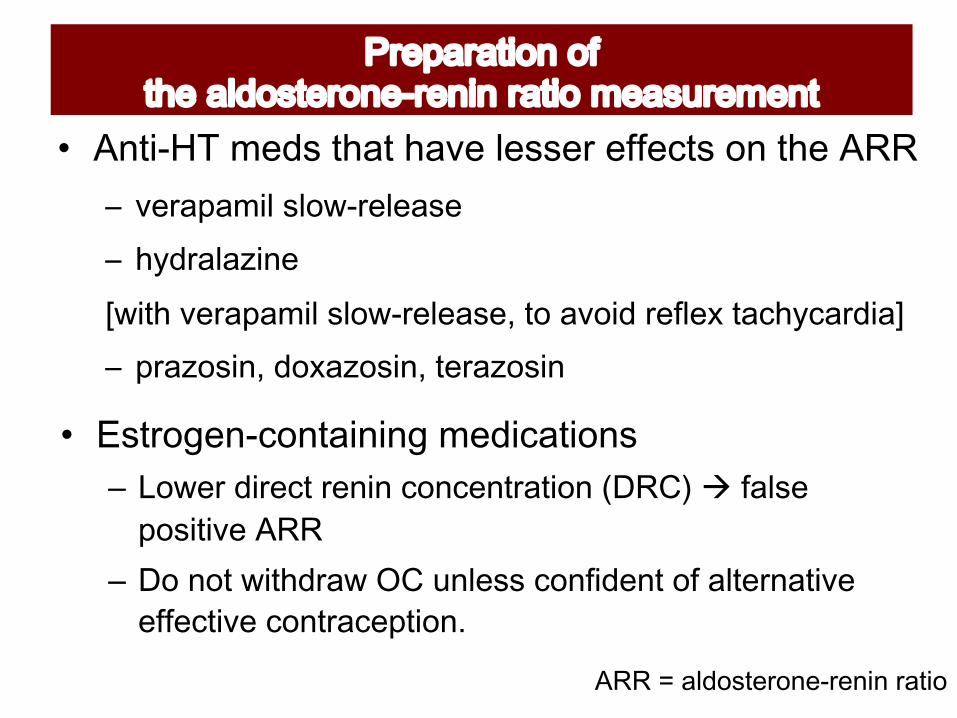
Y C)$/FKZ+5(B#+$,1$+,14(+3(##(%+(77(0$#+&)+$,(+CXX+T M01'/'4&8#+8*KJ1080'+0T -.31'8'Y&)0#ZK&2-#M01'/'4&8#+8*KJ1080'+0H#2*#'M*&3#10N80G#2'7-.7'13&'[T /1'Y*+&)H#3*G'Y*+&)H#201'Y*+&)
• "#$%&'()F0&)$1/)/)'+5(B/01$/&)#+– \*K01#3&1072#10)&)#7*)70)21'2&*)#>%Q<@#à N'8+0#/*+&2&M0#=QQ#
– %*#)*2#K&2-31'K#A<#5)80++#7*)N&30)2#*N#'8201)'2&M0#0NN072&M0#7*)21'70/2&*)P
455%6%./0#12'&#('7&'()(%&.2)#
M%(.1%1$/&)+&7+$,(+13B&#$(%&)(F%()/)+%1$/&+5(1#9%(5()$

!"##$%&#""'&()#*
• Z/5(:+5/BF5&%)/)'
• 17$(%+$,(+.1$/()$+,1#+?(()+
9.+R#/$$/)'*+#$1)B/)'*+&%+
G13Q/)'V+7&%+1$+3(1#$+[+,%#
1)B+#(1$(B+7&%+<FN<+5/)#2
Endocrine Society Guideline 2016
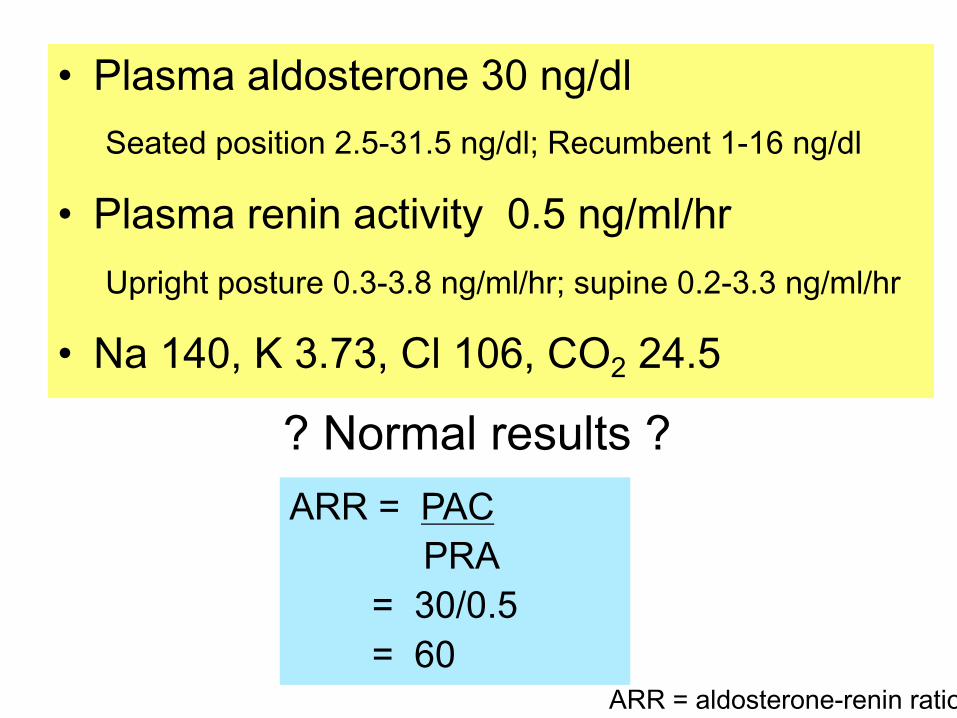
• +",-.,%,"$#-('/#*'%01%*23$"%$0'203#/*+&2&*)#FPDJ],PD#)(938^#Q075460)2#,J,C#)(938
• +",-.,%/'*)*%,&()4)(5%%167%*23."38/_/1&(-2#/*+2510#?P]J]P`#)(9489-1^#+5/&)0#?PFJ]P]#)(9489-1
• 9,%:;1<%=%06>0<%?"%:1@<%?A! B;67
? Normal results ?ARR = PAC
PRA = 30/0.5 = 60
455%6%./0#12'&#('7&'()(%&.2)#
!"#$%&$'()*#$("%+,-./0%1223%456788+9/:823;<=0
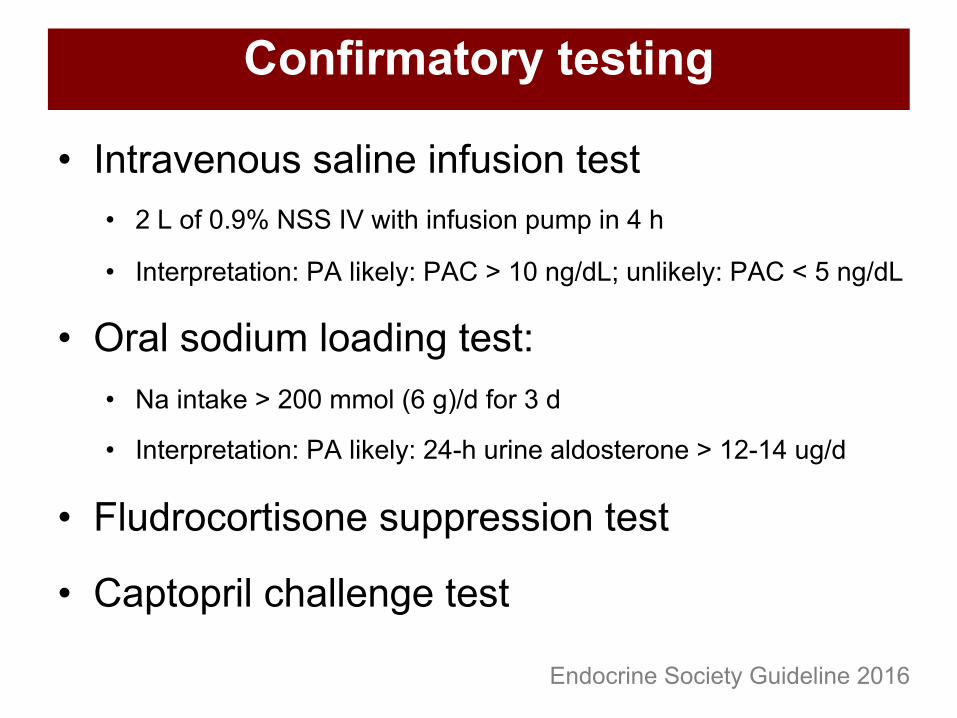
• Intravenous saline infusion test• 2 L of 0.9% NSS IV with infusion pump in 4 h
• Interpretation: PA likely: PAC > 10 ng/dL; unlikely: PAC < 5 ng/dL
• Oral sodium loading test: • Na intake > 200 mmol (6 g)/d for 3 d
• Interpretation: PA likely: 24-h urine aldosterone > 12-14 ug/d
• Fludrocortisone suppression test
• Captopril challenge test
Confirmatory testing
Endocrine Society Guideline 2016
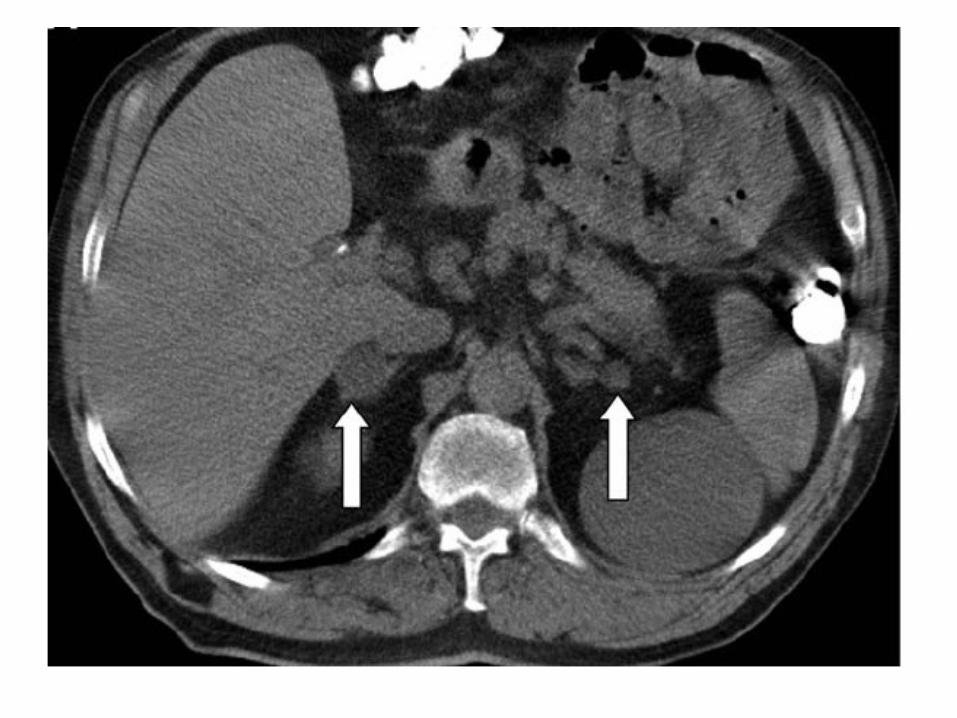
Subtypes of Primary Aldosteronism
• Adrenal adenoma
• Bilateral adrenal hyperplasia
• Glucocorticoid-remediable hyperaldosteronism: very rare
TreatmentAdenomaà Surgery
• Unilateral adrenalectomy
Hyperplasiaà
Medication- Spironolactone
- 12.5-25 mg initially and increase to 400 mg/day to normokalemia- Spironolactone Û T1/2 digoxin- Antagonism at testosterone receptor : painful gynecomastia, ED, Ü libido in men
- Agonist activity at progesterone receptor: menstrual irregularity
Aldosterone-specific CV morbidity and mortality : Stroke, MI, AF

Adrenal Venous Sampling

Results of Bilateral Adrenal Venous Sampling
Left adrenalectomy
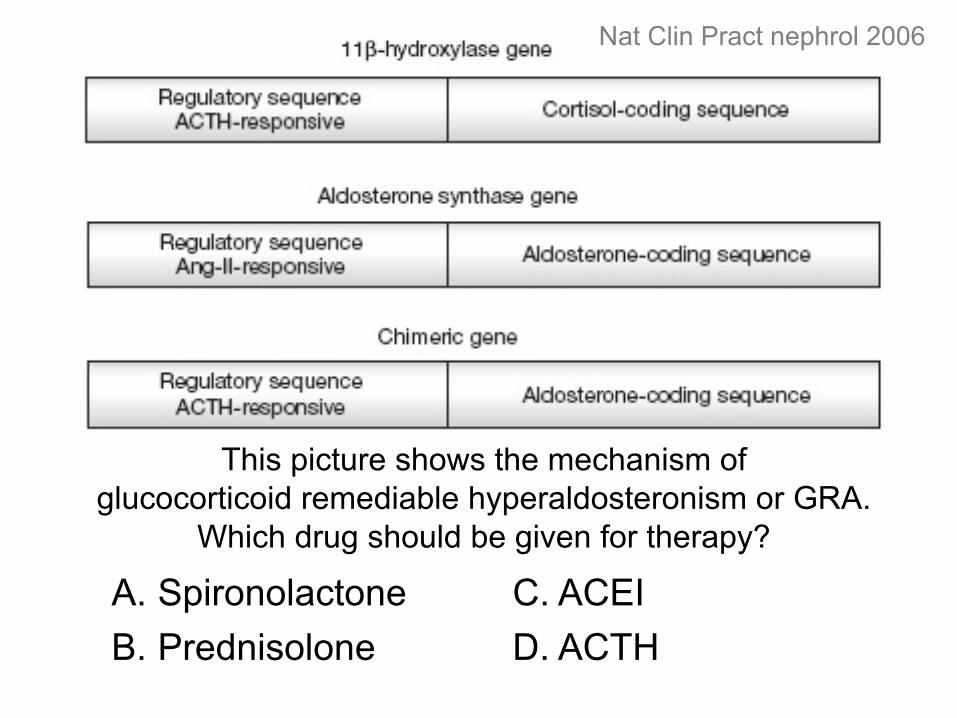
Nat Clin Pract nephrol 2006
This picture shows the mechanism of glucocorticoid remediable hyperaldosteronism or GRA.
Which drug should be given for therapy?
A. SpironolactoneB. Prednisolone
C. ACEID. ACTH
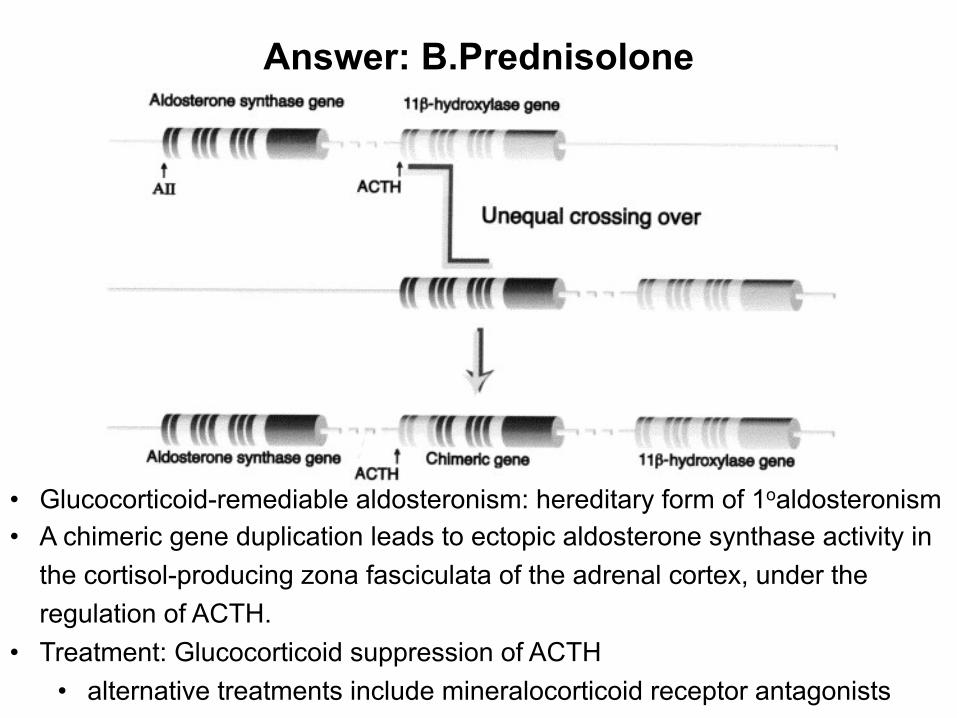
Answer: B.Prednisolone
• Glucocorticoid-remediable aldosteronism: hereditary form of 1oaldosteronism • A chimeric gene duplication leads to ectopic aldosterone synthase activity in
the cortisol-producing zona fasciculata of the adrenal cortex, under the regulation of ACTH.
• Treatment: Glucocorticoid suppression of ACTH • alternative treatments include mineralocorticoid receptor antagonists

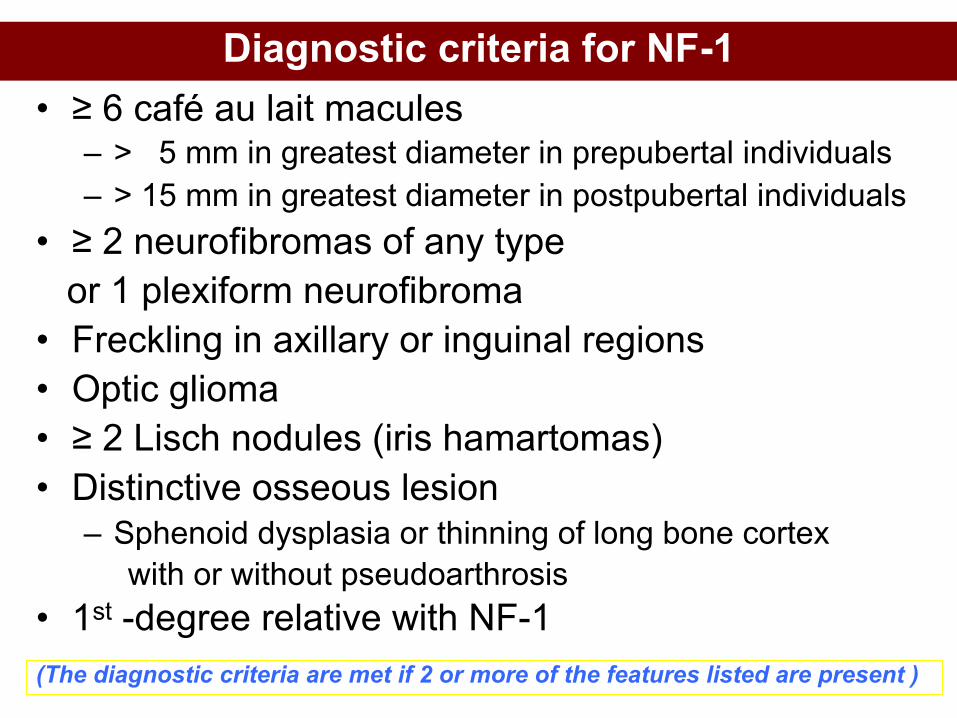
Diagnostic criteria for NF-1• ≥ 6 café au lait macules
– > 5 mm in greatest diameter in prepubertal individuals – > 15 mm in greatest diameter in postpubertal individuals
• ≥ 2 neurofibromas of any type or 1 plexiform neurofibroma
• Freckling in axillary or inguinal regions• Optic glioma• ≥ 2 Lisch nodules (iris hamartomas)• Distinctive osseous lesion
– Sphenoid dysplasia or thinning of long bone cortexwith or without pseudoarthrosis
• 1st -degree relative with NF-1(The diagnostic criteria are met if 2 or more of the features listed are present )

1
2
3
2
4
5
6Optic glioma
7) 1st degree relative NF1
Harrison’s Principles of Internal Medicine
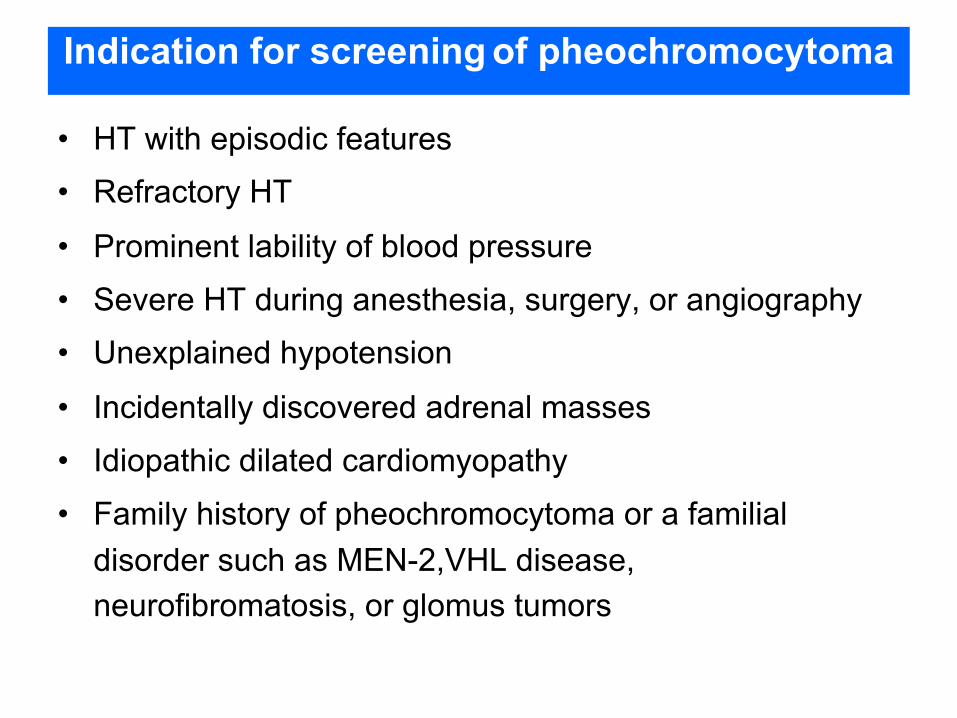
Indication for screening of pheochromocytoma
• HT with episodic features• Refractory HT
• Prominent lability of blood pressure• Severe HT during anesthesia, surgery, or angiography• Unexplained hypotension
• Incidentally discovered adrenal masses• Idiopathic dilated cardiomyopathy• Family history of pheochromocytoma or a familial
disorder such as MEN-2,VHL disease, neurofibromatosis, or glomus tumors
Familial Pheochromocytoma• MEN 2A
– 50% Pheo (usually bilateral), MTC, HPT
– RET
• MEN 2B– 50% Pheo (usually bilateral),
MTC, mucosal neuroma, marfanoid habitus
– RET
• Von Hippel-Landau– 50% Pheo (usually bilateral),
retinoblastoma, cerebellar hemangioma, nephroma, renal/pancreas cysts
– VHL
• NF1 (Von Recklinghausen's)– 2% Pheo
(50% if NF-1 and HT)– Café-au-lait spots,
neurofibroma, optic glioma– NF1
• Familial paraganglioma– SDH
MEN 2MEN2A• Medullary CA thyroid
(>90%)• Pheochromocytoma
(40-50%)• Parathyroid hyperplasia
(10-20%)• Cutaneous lichen
amyloidosis• Hirschprung’s disease
MEN2B• Medullary CA thyroid
• Pheochromocytoma
• Other
– Mucosal neuromas
– Intestinal
ganglioneuromas
– Marfanoid habitus
VHL• Major complications:
– Retinal angioma (58%) – visual loss– Cerebellar hemangioblastoma (56%)– Spinal cord hemangioblastoma (14%)– Renal cell carcinoma (25%)– Pheochromocytoma (17%)
• Other associated complications:– Pancreatic neuroendocrine tumours and cysts– Epididymal (male) or broad ligament (female)
cystadenomas– 2o polycythemia (hemangioblastoma and RCC)
VHL; 3p
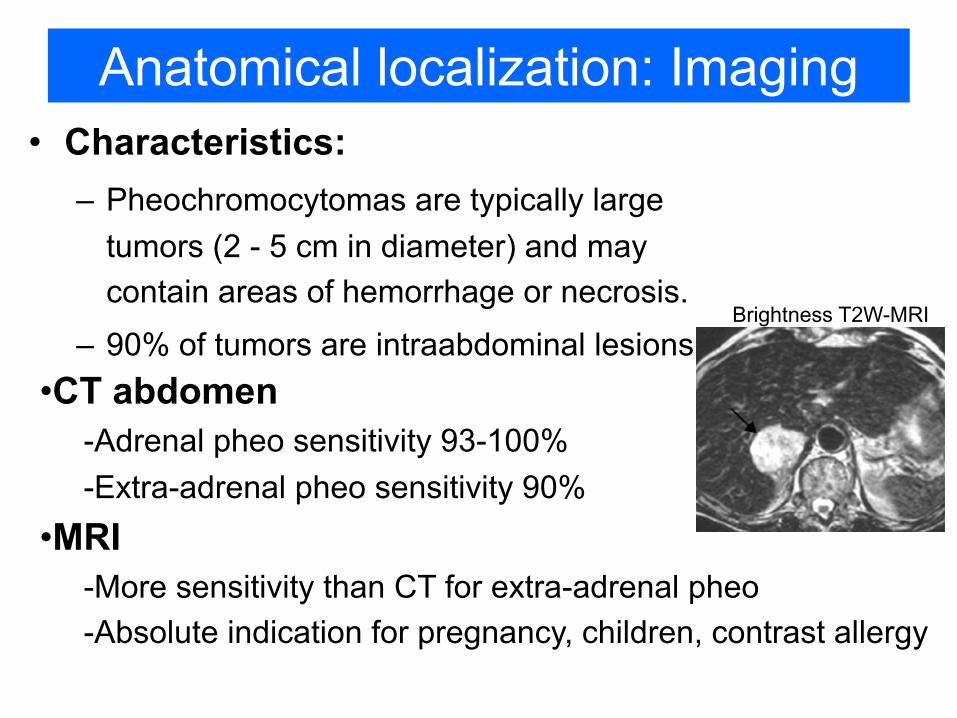
Anatomical localization: Imaging• Characteristics:
– Pheochromocytomas are typically large tumors (2 - 5 cm in diameter) and may contain areas of hemorrhage or necrosis.
– 90% of tumors are intraabdominal lesions•CT abdomen
-Adrenal pheo sensitivity 93-100%-Extra-adrenal pheo sensitivity 90%
•MRI-More sensitivity than CT for extra-adrenal pheo-Absolute indication for pregnancy, children, contrast allergy
Brightness T2W-MRI

Case vignette• 62-yr-old woman
• underwent CT coronary for check up in the private hospital
• found a 1.8-cm left adrenal mass
• underlying of DM type 2 and hypertension
How should she be evaluated ?
Adrenal incidentaloma
Questions need to be answered
True adrenal mass ?
Malignant ?
Hormonally active ?
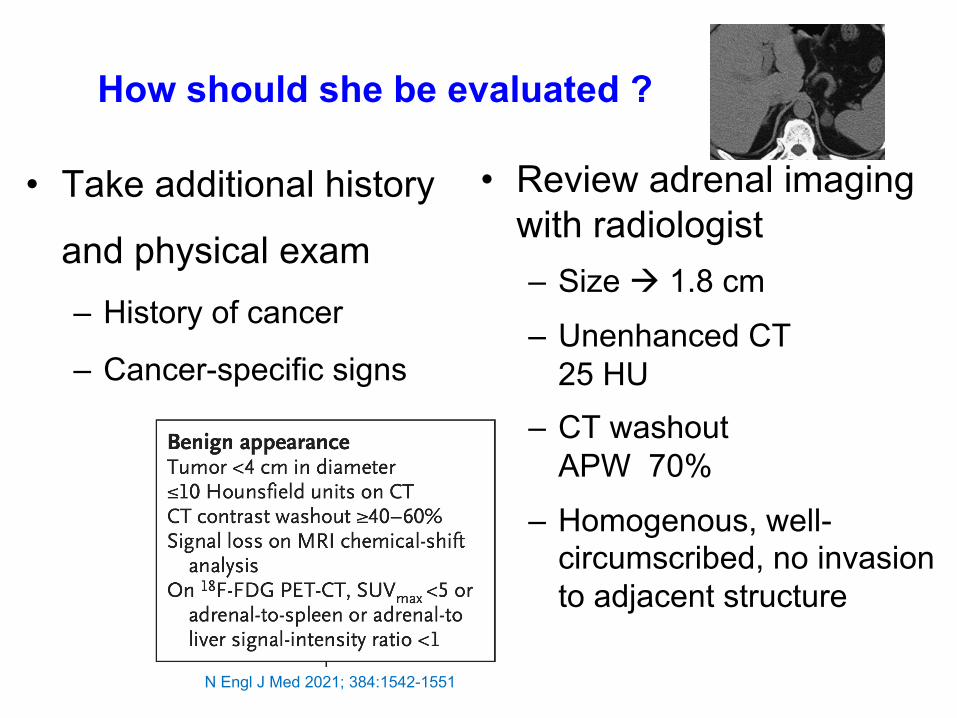
How should she be evaluated ?
• Take additional history
and physical exam– History of cancer
– Cancer-specific signs
• Review adrenal imaging with radiologist– Size à 1.8 cm
– Unenhanced CT 25 HU
– CT washout APW 70%
– Homogenous, well-circumscribed, no invasion to adjacent structure
N Engl J Med 2021; 384:1542-1551
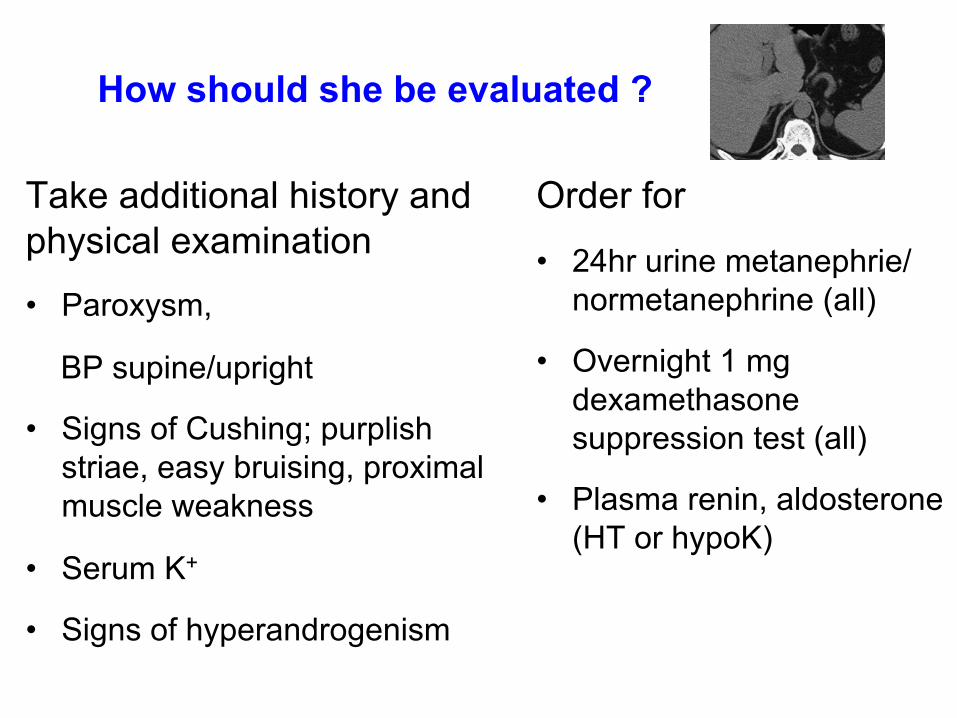
How should she be evaluated ?
Take additional history and physical examination• Paroxysm,
BP supine/upright
• Signs of Cushing; purplish striae, easy bruising, proximal muscle weakness
• Serum K+
• Signs of hyperandrogenism
Order for
• 24hr urine metanephrie/ normetanephrine (all)
• Overnight 1 mg dexamethasone suppression test (all)
• Plasma renin, aldosterone (HT or hypoK)
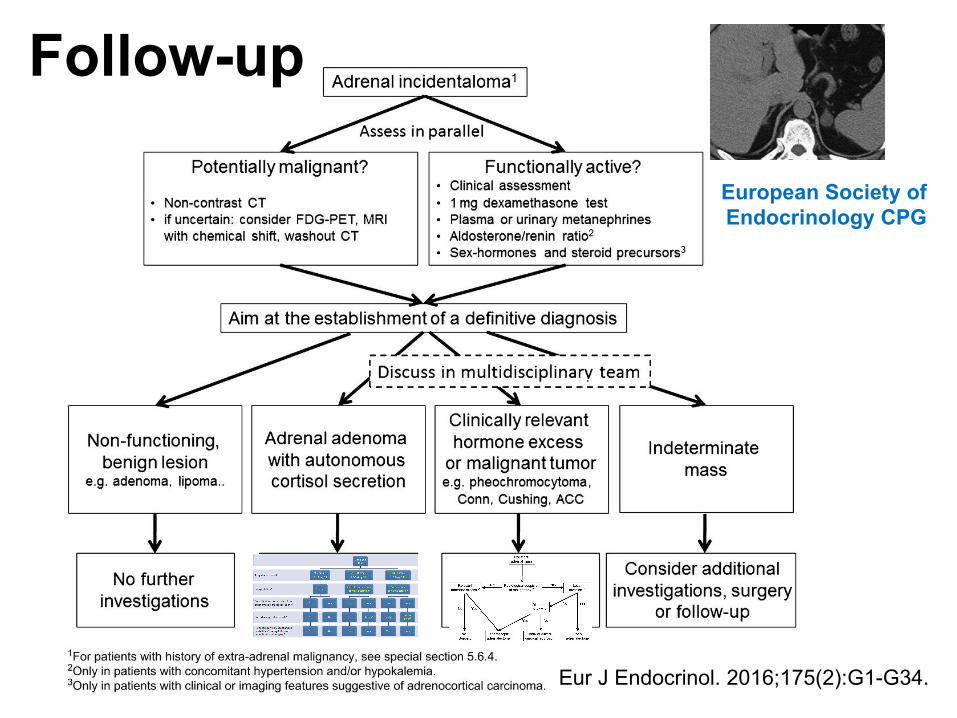
Follow-up
Eur J Endocrinol. 2016;175(2):G1-G34.
European Society of Endocrinology CPG

Quiz #1165-yr-old femaleIncidentally discovered left adrenal mass 2 cm, 5 HU
T2DM diet control, osteoporosis Dx 4 yr on alendronateNa 139, K 4.1In addition to screening test for pheo,which of the following is the most appropriate Dx test?A. Low-dose dexamethasone suppression testB. Plasma renin and aldosteroneC. DHEA-s
D. MRI adrenal glandE. No further testing
Quiz #11 Answer: A. LDDST
A 70-yr-old male
Problem: suspected adrenal insufficiency
Underlying CA rectum Dx 6 Mo S/P surgery
• Not tolerated to chemotherapy
• 3 Mo PTA, received abccdaebabcfghijhbklmnoaNimotuzumab, Opdivo, Chinese herb
• Admitted to many hospitals due to fatigue, hemiballismdue to metabolic cause
• Chronic hyponatremia (Na ~120)
– Currently euvolemic status
– 8AM cortisol < 1 ug/dL, normal TFT
Quiz #12
• Chronic hyponatremia (Na ~120)
– Currently euvolemic status
– 8AM cortisol < 1 ug/dL, normal TFT
• No Cushingoid appearance
• No hyperpigmentation
• Na 123, K 3.86, Cl 89, CO2 25, on NaCl tab 4x3
• ACTH < 5 pg/mL
• Review MRI brain: sellar region looked normal
What is the cause of adrenal insufficiency?
Quiz #12
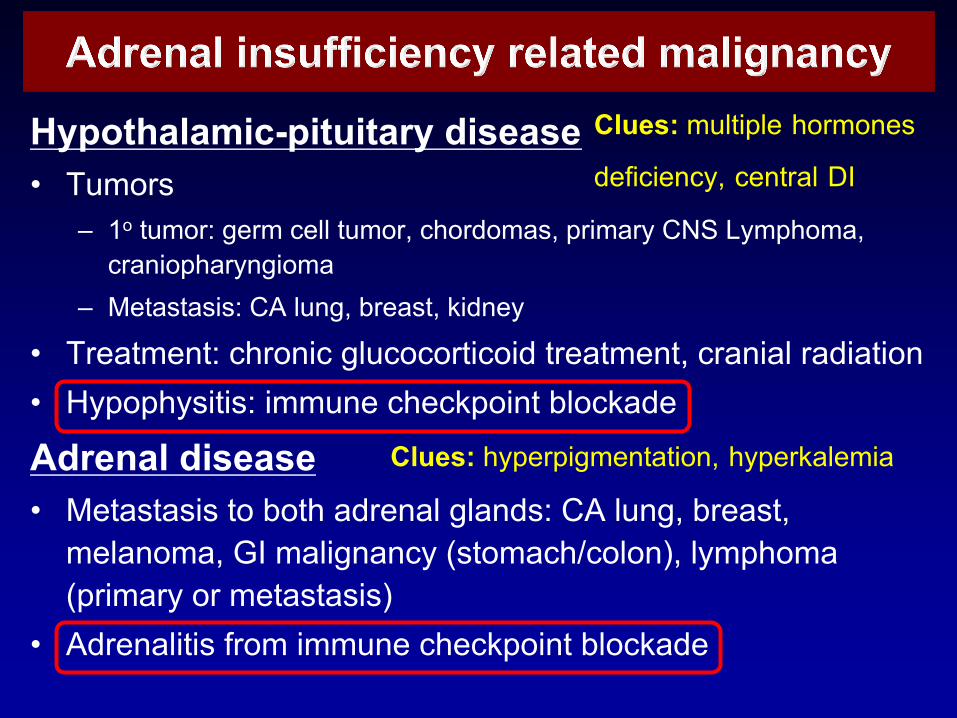
Hypothalamic-pituitary disease• Tumors
– 1o tumor: germ cell tumor, chordomas, primary CNS Lymphoma, craniopharyngioma
– Metastasis: CA lung, breast, kidney
• Treatment: chronic glucocorticoid treatment, cranial radiation• Hypophysitis: immune checkpoint blockade
Adrenal disease• Metastasis to both adrenal glands: CA lung, breast,
melanoma, GI malignancy (stomach/colon), lymphoma (primary or metastasis)
• Adrenalitis from immune checkpoint blockade
Clues: multiple hormones
deficiency, central DI
Clues: hyperpigmentation, hyperkalemia
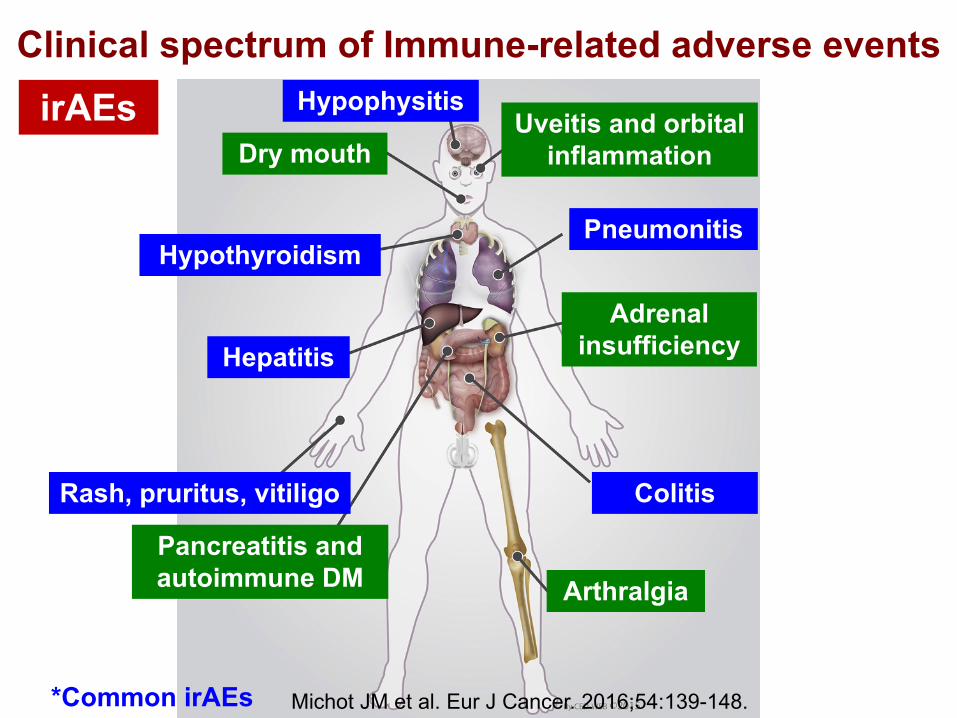
Clinical spectrum of Immune-related adverse events
Michot JM et al. Eur J Cancer. 2016;54:139-148.
Hypophysitis
Dry mouth
Hypothyroidism
Hepatitis
Rash, pruritus, vitiligo
Pancreatitis and autoimmune DM Arthralgia
Colitis
Adrenal insufficiency
Pneumonitis
Uveitis and orbital inflammation
*Common irAEs
irAEs
Congenital Adrenal Hyperplasia
1 หน้าHT, 1 หลงั virilization

Steroid synthesis
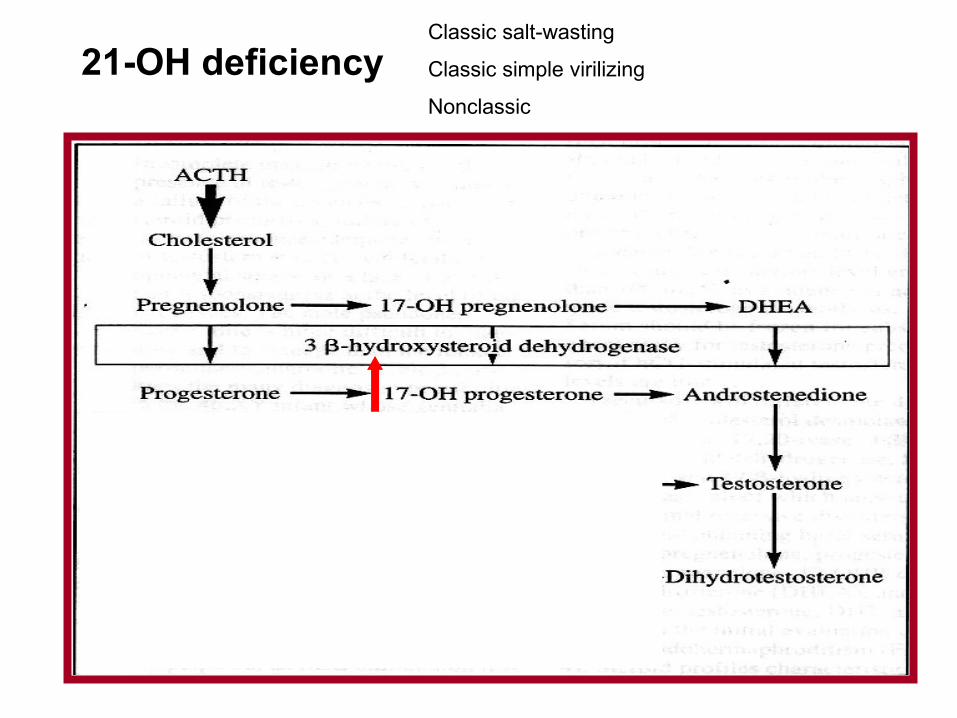
21-OH deficiencyClassic salt-wasting
Classic simple virilizing
Nonclassic
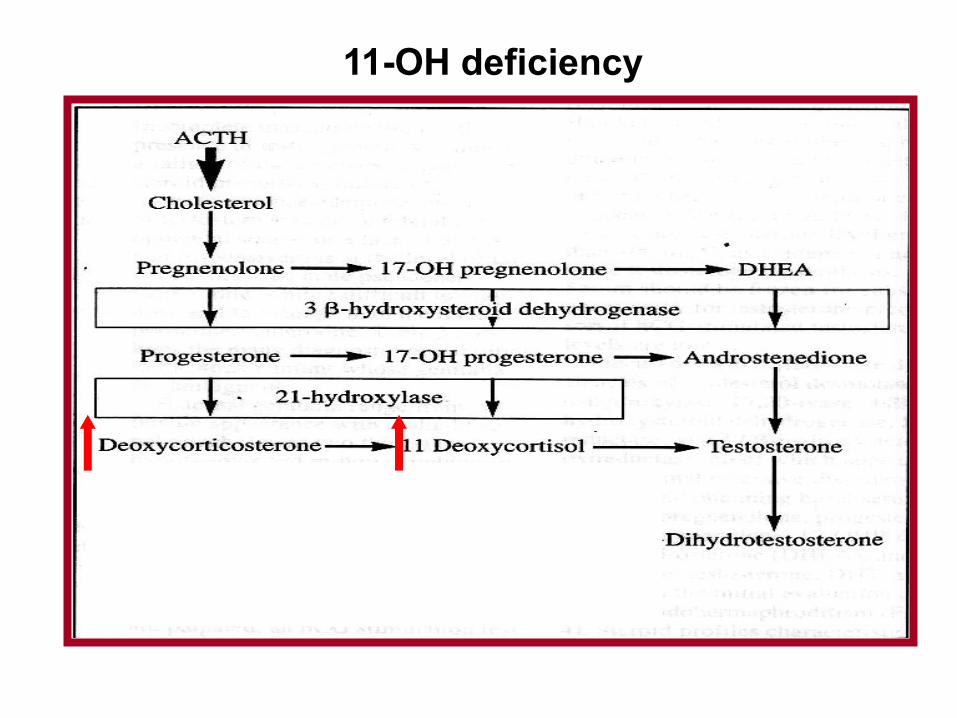
11-OH deficiency
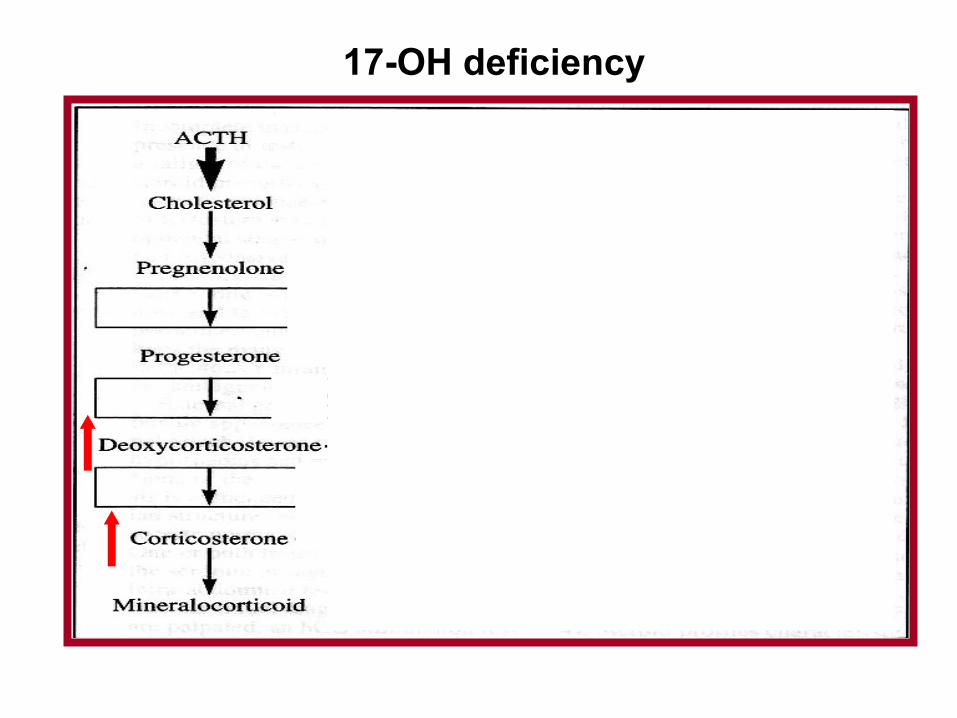
17-OH deficiency
The Hard WorkPuts YouWhere
the Good LuckCan Find You