review article review of clinical trials on effects of...
TRANSCRIPT
Review ArticleReview of Clinical Trials on Effects of OralAntioxidants on Basic Semen and Other Parameters inIdiopathic Oligoasthenoteratozoospermia
Senka Imamovic Kumalic and Bojana Pinter
ReproductiveUnit, Division ofGynecology andObstetrics, UniversityMedical Centre Ljubljana, Slajmerjeva 3, 1000 Ljubljana, Slovenia
Correspondence should be addressed to Bojana Pinter; [email protected]
Received 31 January 2014; Accepted 14 March 2014; Published 31 March 2014
Academic Editor: Irma Virant-Klun
Copyright © 2014 S. Imamovic Kumalic and B. Pinter. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
Infertility affects 50 to 80 million people worldwide. Male factor is a cause of infertility in almost half of cases, mainly due tooligoasthenoteratozoospermia (OAT). With common diagnostic methods no cause can be found in approximately 30% of casesof male infertility due to OAT and these are considered idiopathic. Reactive oxygen species (ROS) play an important role in maleinfertility and are proved to be higher in infertilemen; antioxidants could oppose their effect.The aim of this paper was to review theliterature on clinical trials in the period from year 2000 to year 2013 studying the effects of various types of antioxidant supplementson basic and other sperm parameters and pregnancy rates in subfertile males with idiopathic OAT. The majority of studies wererandomized and placebo controlled and confirmed beneficial effect of antioxidants on at least one of the semen parameters; thebiggest effect was determined on sperm motility. In many of these trials combinations of more antioxidants were assessed. Theoptimal dosages of one or more antioxidants were not defined.We concluded that antioxidants play an important role in protectingsemen from ROS and can improve basic sperm parameters in case of idiopathic OAT.
1. Introduction
Almost 15% of all couples trying to conceive are affected byinfertility, and in almost half of these cases male infertilityis the sole or a contributing factor [1]. While conditionssuch as varicocele, cryptorchidism, and hypogonadism aredefinable causes for infertility, no cause may be determinedfor an abnormal semen analysis in over 25% of cases [2]. Suchidiopathic infertility and oligoasthenoteratospermia (iOATs)is a condition in which sperm concentration, the proportionof motile sperms, and the proportion of morphologicallynormal sperms are below the World Health Organization(WHO) reference values [3].
Elevated reactive oxygen species (ROS) levels in thesemen may be an etiologic factor for male infertility [4]. Itis estimated that 25% of infertile men possess high levelsof semen ROS, whereas fertile men do not have high levelsof semen ROS [5, 6]. ROS are needed for capacitation, theacrosome reaction, and ultimately fertilization [7]. However,
their uncontrolled production is detrimental to cell functionas they damage a variety of biomolecules such as lipids, aminoacids, carbohydrates, protein, and DNA and adversely affectsperm function [8] due to DNA damage [9, 10], reducedmotility [11], and defective membrane integrity [12, 13].Spermatozoa are particularly susceptible to oxidative injurydue to the abundance of plasma membrane polyunsaturatedfatty acids. These unsaturated fatty acids provide fluidity thatis necessary for membrane fusion events (e.g., the acrosomereaction and sperm-egg interaction) and for sperm motility[14]. The human ejaculate contains a number of potentialsources of ROS. These include leukocytes, germ cells, orabnormal sperms [15]. At the same time, a number of cellularmolecules called antioxidants, which protect the cell fromexcessive ROS-induced lipid peroxidation, are also presentwithin the ejaculate [16]. Studies have shown that seminalantioxidant capacity is suppressed in infertile men with highROS levels compared to men with normal levels of ROS[17, 18].
Hindawi Publishing CorporationBioMed Research InternationalVolume 2014, Article ID 426951, 11 pageshttp://dx.doi.org/10.1155/2014/426951

2 BioMed Research International
2. Materials and Methods
We searched PubMed with keywords, including combina-tions of search terms such as “male infertility” and “antiox-idants.” We searched for reviews, controlled and random-ized controlled clinical studies. From the numerous searchresults for the period between 1st January 2000 and 31stDecember 2013, 32 primary studies on idiopathic oligoas-thenoteratozoospermia (OAT) were chosen and their datawere gathered in order to provide a complete overview ofthe literature. Given the different antioxidants used (bothalone and in combination), the different dosages, differentduration of treatment, and various number of participants(from very small groups to large researches), we looked up forstatistical significance of changes in basic sperm parametersand pregnancy rates.
3. Results and Discussion
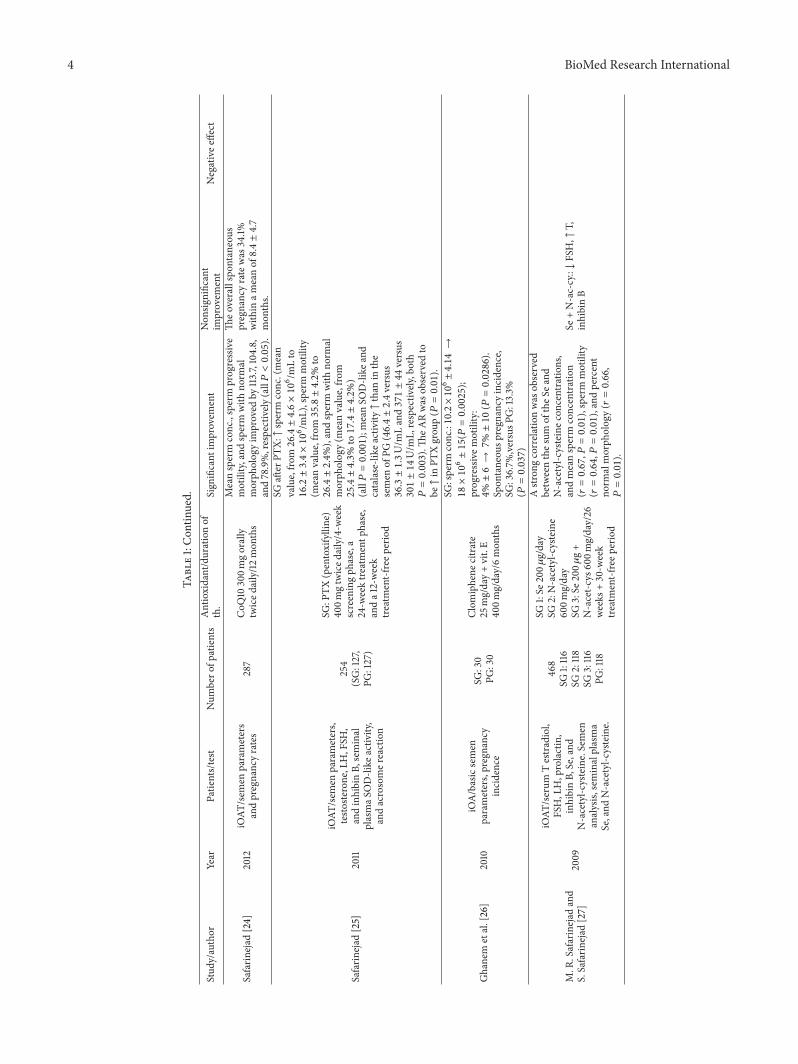
The review of the studies on antioxidants in clinical studies isillustrated in Table 1.
3.1. SpermConcentration. Low sperm concentration or oligo-zoospermia is defined as concentration less than 15 ×106 spermatozoa/mL according to WHO reference value
from 2010 [51] and less than 20 × 106 spermatozoa/mLaccording to WHO reference values from 1999 [52], whichwere considered in most of researches in this review. Manyresearches showed significant improvements in sperm con-centration after oral intake of different antioxidants [19–31].Most of these researches investigated combination of differentantioxidants, like L-carnitine, coenzyme Q10 (CoQ10), vita-min C, vitamin E, zinc (Zn), selenium (Se), and so forth. Butthere are also some studies that investigated only one type ofantioxidant. Safarinejad et al. showed that intake of 200mgCoQ10 daily for 26 weeks improved sperm concentration instudy group (28.7±4.6×106 spermatozoa/mL) versus placebogroup (16.8 ± 4.4 × 106 spermatozoa/mL) (𝑃 = 0.005) [23].After 6months of intake of combination of 25mg clomiphenecitrate and 400mg vitamin E per day sperm concentrationimproved from 10.2×106±4.14 spermatozoa/mL to 18×106±15 spermatozoa/mL (𝑃 = 0.0025) [26]. There was also signif-icant improvement in sperm concentration from 14.3±7.38×106 spermatozoa/mL to 32.8 ± 10.3 × 106 spermatozoa/mL
(𝑃 < 0.001) after consumption of 1 g of vitamin C twice dailytaken for 2 months as proved by Akmal et al. [28].
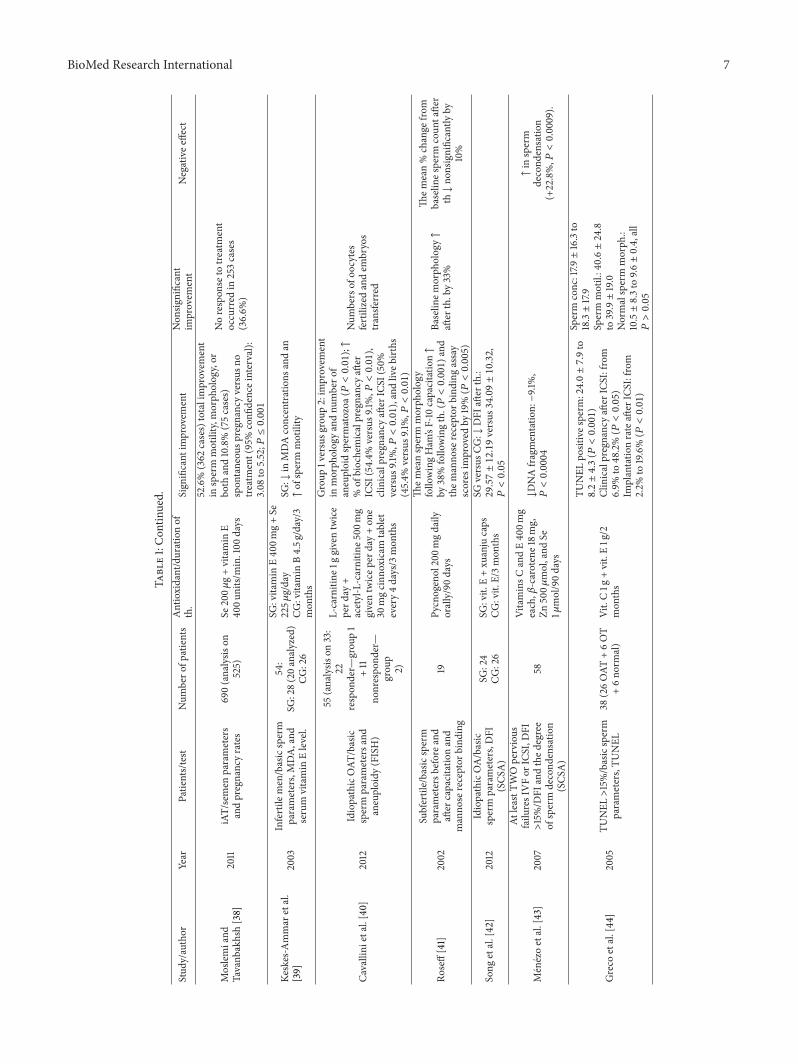
3.2. Sperm Motility. Asthenozoospermia is defined as lessthan 40% of motile spermatozoa [51] and according toWHO reference value from 1999 less than 50% of motilespermatozoa [52]. 20 out of 32 studies in our review provedsignificant improvement in sperm motility after the use ofantioxidants [19, 20, 22–39]. Improvement in sperm motilityhas been shown mostly in researches considering mixtureof more antioxidants such as selenium and vitamin E [38,39]. Most of studies with just one type of antioxidantwere about CoQ10 but in different dosages and in differentduration of consuming [22–24, 37]. Kumar et al. showed
that consumption of herbal-mineral supplement Addyzoafor 3 months improved total and progressive sperm motilityin study group. Total motility improved from 23.2 ± 17.3%before the treatment to 33.4 ± 23.2% after the treatment(𝑃 = 0.008). Progressivemotility improved from 15.7±12.6%before treatment to 22.6±18.0%after treatmentwithAddyzoa(𝑃 = 0.024) [33]. Wang et al. showed that L-carnitine incombination with vitamin E taken for 3 months significantlyimproved forward sperm motility from 28.6% ± 9.2% to45.4% ± 11.1% (𝑃 < 0.01), compared with just vitamin E[35]. After treatment with 200mg CoQ10 twice daily for 6months spermmotility improved from 9.13%± 2.50% beforethe therapy to 16.34% ± 3.43% after the therapy (𝑃 < 0.05)[37].
3.3. Sperm Morphology. WHO reference values from 1999[52] defined teratozoospermia as less than 14% of normalshape and form spermatozoa according to strict Krugercriteria. Although WHO reference values from 2010 defineteratozoospermia as less than 4% of normal shape andform spermatozoa [51] strict Kruger criteria are still used asreference value for assessing sperm morphology. L-carnitinein combinationwithCoQ10, vitamins E andC, zinc, selenium[20, 40], CoQ10 alone [23, 24], pentoxifylline [25], N-acetyl-cysteine with Se [27], vitamin C alone [28], combinationof papaya, beta-glucan, lactoferrin, vitamins C and E [36],Se, and vitamin E [38], and pycnogenol [41] significantlyimproved sperm morphology. Therapy with 200mg CoQ10daily for 26 weeks improved spermmorphology in 114 partic-ipants in study group to 17.6%± 4.4% versus 14.8%± 4.1% in114 participants in placebo group (𝑃 = 0.01) [23]. Safarinejadalso showed that intake of 400mg of pentoxifylline twicedaily for 24 weeks of treatment phase significantly improvedpercentage of sperm with normal morphology to 25.4 ± 4.3%in study group versus 17.4 ± 4.2% in placebo group (𝑃 =0.001) [25]. Combination of 20mg beta-glucan, 50mg fer-mented papaya, 97mg lactoferrin, 30mg vitamin C, and 5mgvitamin E, twice per day for 3 months, improved percentageof morphologically normal sperm in 36 participants from17.0 ± 5.2% to 29.8 ± 6.5% (𝑃 < 0.01) [36].
3.4. Sperm DNA Fragmentation and Chromatin Integrity.ROS can cause sperm DNA damage and integrity of spermDNAcan bemeasuredwithDNA fragmentation.The levels ofsperm-derived ROS (measured in sperm preparations havingminimal leukocyte contamination) have been associated withsperm DNA damage [53]. High level of denatured DNA inspermatozoa with large nuclear vacuole could arise fromprecocious decondensation and disaggregation of spermchromatin fibers [54]. Dietary antioxidants may be benefi-cial in reducing sperm DNA damage, particularly, in menwith high levels of DNA fragmentation [5]. Five out of 32studies confirmed that the usage of different antioxidants hadimportant influence on DNA fragmentation and chromatinintegrity [20, 42–46]. Song et al. showed that combination ofChinese medicine Compound Xuanju Capsule with vitaminE taken for 3months decreased degree ofDNA fragmentationindex (DFI) after therapy to 29.57 ± 12.19 compared just to

BioMed Research International 3
Table1:Stud
ycharacteris
ticsa
ndthee
ffectof
oralantio
xidantso
nbasic
andothersem
enparameters.
Stud
y/author
Year
Patients/test
Num
bero
fpatients
Antioxidant/durationof
th.
Sign
ificant
improvem
ent
Non
significant
improvem
ent
Negativee
ffect
Wirleitner
etal.[19]
2012
OAT
versus
non-OAT
,MSO
ME
147
Fertilo
vitM
plus/2–12
mon
ths
↑concentrationandmotilityof
sperm
Morph
olog
y
Abad
etal.[20]
2013
AT/D
FI,basicsperm
parameters
20
L-Ca
rnitine
1500
mg;
vitamin
C60
mg;CoQ
1020
mg;vitamin
E10mg;
Zn10mg;vitamin
B9200𝜇
g;Se
50𝜇g;vitamin
B121𝜇g/3mon
ths
DNAintegrity
(𝑃<0.01),the
prop
ortio
nof
DDS↓(𝑃<0.05).↑in
concentration,
motility,vita
lity,and
morph
olog
yparameters.
Safarin
ejad
[21]
2011
iOAT
238(analysis
on211)
SG:106
PG:105
SG:eicosapentaenoic
(EPA
)and
docosahexaenoica
cids
(DHA),1.8
4gperd
ayversus
PG/32weeks
SG:↑
ofsperm
celltotalcou
nt(fr
om38.7±8.7×106to61.7±11.2×106,
𝑃=0.001)a
ndsperm
cell
concentration(fr
om15.6±4.1×106/m
Lto
28.7±4.4×106/m
L,𝑃=0.001).
SeminalplasmaE
PAandDHAconc.
werep
ositivelycorrelated
with
seminalplasmaS
OD-like
and
catalase-like
activ
ity(both
𝑃=0.001).
Inseminalplasma,bo
thSO
D-like
andcatalase-like
activ
itywerep
ositively
correlated
with
sperm
coun
t,sperm
motility,and
sperm
morph
ology.
Safarin
ejad
[22]
2009
iOAT
/sem
enanalyses,
AR,
immun
obeadtestfor
antisperm
antib
ody,and
determ
inationof
resting
levelsof
LH,FSH
,prolactin
,testoste
rone,
andinhibinB
212
(SG:106,versusP
G:
106)
CoQ
10300m
g/26
weeks
follo
wed
bya3
0-week
treatment-freep
hase
SG:↑
insperm
density
andmotility
(each𝑃=0.01).↓FSHandLH
atthe
26-w
eektre
atmentp
hase
(each
𝑃=0.03).By
thee
ndof
the
treatmentp
hase
them
eanARhad
increasedfro
m14%±8%
and
15%±8%
to31%±11%
and
16%±10%
intheC
oQ10
andplacebo
grou
ps,respectively
(𝑃=0.01).
Safarin
ejad
etal.[23]
2012
iOAT
/sem
enparameters,
seminalplasmaT
AC,
FSH,and
inhibinB
228
SG:114
PG:114
CoQ
10200m
g/day/26
weeks
SG:↑
insperm
density
(28.7±4.6×106/m
Lversus
16.8±4.4×106/m
L(𝑃=0.005)),
sperm
motility(35.8%±2.7%
versus
25.4%±2.1%
(𝑃=0.008)),and
sperm
morph
ology(17.6%±4.4%
versus14.8%±4.1%
(𝑃=0.01)).
FSH↓(𝑃=0.02),inhibinB↑
(𝑃=0.01)
4 BioMed Research International
Table1:Con
tinued.
Stud
y/author
Year
Patients/test
Num
bero
fpatients
Antioxidant/durationof
th.
Sign
ificant
improvem
ent
Non
significant
improvem
ent
Negativee
ffect
Safarin
ejad
[24]
2012
iOAT
/sem
enparameters
andpregnancyrates
287
CoQ
10300m
gorally
twiced
aily/12
mon
ths
Meansperm
conc.,s
perm
progressive
motility,and
sperm
with
norm
almorph
olog
yim
proved
by113.7,104.8,
and78.9%,respectively
(all𝑃<0.05).
Theo
verallspon
taneou
spregnancyratewas
34.1%
with
inam
eanof
8.4±4.7
mon
ths.
Safarin
ejad
[25]
2011
iOAT
/sem
enparameters,
testo
sterone,LH,FSH
,andinhibinB,
seminal
plasmaS
OD-like
activ
ity,
andacrosomer
eaction
254
(SG:127,
PG:127)
SG:P
TX(pentoxifylline)
400m
gtwiced
aily/4-w
eek
screeningph
ase,a
24-w
eektre
atmentp
hase,
anda1
2-week
treatment-freep
eriod
SGaft
erPT
X:↑sperm
conc.(mean
value,fro
m26.4±4.6×106/m
Lto
16.2±3.4×106/m
L),sperm
motility
(meanvalue,fro
m35.8±4.2%
to26.4±2.4%),andsperm
with
norm
almorph
olog
y(m
eanvalue,fro
m25.4±4.3%
to17.4±4.2%)
(all𝑃=0.001);meanSO
D-like
and
catalase-like
activ
ity↑than
inthe
semen
ofPG
(46.4±2.4versus
36.3±1.3U/m
Land371±44versus
301±14U/m
L,respectiv
ely,both
𝑃=0.003).Th
eARwas
observed
tobe↑in
PTXgrou
p(𝑃=0.01).
Ghanem
etal.[26]
2010
iOA/basicsemen
parameters,pregnancy
incidence
SG:30
PG:30
Clom
iphene
citrate
25mg/day+vit.E
400m
g/day/6mon
ths
SG:sperm
conc.:10.2×106±4.14→
18×106±15(𝑃=0.0025);
progressivem
otility:
4%±6→7%±10(𝑃=0.0286).
Spon
taneou
spregn
ancy
incidence,
SG:36.7%
,versusP
G:13.3%
(𝑃=0.037)
M.R
.Safarinejad
and
S.Safarin
ejad
[27]
2009
iOAT
/serum
Testradiol,
FSH,LH,prolactin,
inhibinB,
Se,and
N-acetyl-c
ysteine.Semen
analysis,
seminalplasma
Se,and
N-acetyl-c
ysteine.
468
SG1:116
SG2:118
SG3:116
PG:118
SG1:Se
200𝜇
g/day
SG2:N-acetyl-c
ysteine
600m
g/day
SG3:Se
200𝜇
g+
N-acet-c
ys60
0mg/day/26
weeks
+30-w
eek
treatment-freep
eriod
Astr
ongcorrelationwas
observed
betweenthes
umof
theS
eand
N-acetyl-c
ysteinec
oncentratio
ns,
andmeansperm
concentration
(𝑟=0.67,𝑃=0.01),sperm
motility
(𝑟=0.64,𝑃=0.01),andpercent
norm
almorph
olog
y(𝑟=0.66,
𝑃=0.01).
Se+N-ac-cy.:↓FSH,↑
T,inhibinB

BioMed Research International 5
Table1:Con
tinued.
Stud
y/author
Year
Patients/test
Num
bero
fpatients
Antioxidant/durationof
th.
Sign
ificant
improvem
ent
Non
significant
improvem
ent
Negativee
ffect
Akm
aletal.[28]
2006
O/sem
enparameters
13vitamin
C1g
twiced
aily/2
mon
ths
Meansperm
coun
t:14.3±7.38×106
sperms/mLto32.8±10.3×106
sperms/mL(𝑃<0.001),meansperm
motility:31.2±9.61%
to60.1±8.47%
(𝑃<0.001),andmean
spermsw
ithno
rmalmorph
ology:
43±7.87%
to66.7±4.77%
(𝑃<0.001).
Shietal.[29]
2004
OA/sem
inalroutine
analysis
34
Xinx
ibao
(ZnandSe
tablets)threetim
esa
day/90
days
+fivetablets
atatim
efor
90days
insuccessio
n
Thes
perm
quality
was
improved
60days
and90
days
after
treatment.5
cases(14.7%)sho
wed
remarkable
effect,25
(73.5%
)improved.
4cases(11.8%
)did
not
respon
d.
Suzukietal.[30]
2003
OandAversus
norm
ozoo
spermia/sperm
parameters,serum
horm
ones,and
SOD
activ
ityin
thes
erum
and
thes
eminalplasma+
the
testiculara
rtery
SG:47
CG:16
Saire
i-to9g
/day/3
mon
ths
SG:totalsperm
conc.(17.1±20.0to
28.7±35.5×106/m
L,𝑃=0.02)a
ndsperm
motility(30.1%±21.6to
45.8%±24.4,𝑃<0.0001)a
ndthe
pulsa
tility
indexof
thetestic
ular
artery↓(2.03±0.84to1.64±0.48,
𝑃=0.04)
Afterth.serum
horm
ones
andSO
Dactiv
itydidno
tchange
significantly
ineither
grou
p.CG
:nosig
nificantchange
insperm
cond
ition
sor
testiculara
rteryflo
w.
Gup
taandKu
mar
[31]
2002
Idiopathicno
nobstructiv
eO/A
/Tspermia/sem
enanalysis
30Lycopene
2000
mcg,twice
aday/3
mon
ths
20patie
nts(66
%):↑sperm
conc.,16
(53%
)↑motility.Th
emedianchange
inconcentrationwas
22million/mL,
motility25%.H
igherb
aseline
concentra
tions
(morethan5
million/mL)
werea
ssociatedwith
significantimprovem
entand
resulted
insix
spon
taneou
spregn
ancies
in26
patie
nts(23%).
14patie
nts(46
%)↑
insperm
morph
ology
(medianchange
10%).
Baselin
esperm
concentra
tionlessthan
5million/mLwas
associated
with
nosig
nificant
improvem
ent.
Busetto
etal.[32]
2012
IdiopathicAT
/basicsperm
parameters
114(96fin
ished)
L-Ca
rnitine
145m
g,acetyl-L-carnitin
e64m
g,fructose
250m
g,citric
acid
50mg,Se
50𝜇g,
CoQ
1020
mg,Zn
10mg,
ascorbicacid
90mg,
cyanocob
alam
in1.5𝜇g,
andfolic
acid
200m
cgon
cead
ay/4
mon
ths
↑Meansperm
progressivem
otility:
18.3±3.8to42.1±5.5,
16patientsa
chievedpregnancy
durin
gthes
tudy.
Con
centratio
nand
morph
olog
y

6 BioMed Research International
Table1:Con
tinued.
Stud
y/author
Year
Patients/test
Num
bero
fpatients
Antioxidant/durationof
th.
Sign
ificant
improvem
ent
Non
significant
improvem
ent
Negativee
ffect
Kumar
etal.[33]
2011
Atleasto
neparameter
ofOAT
/basicsemen
parameters,RO
S,TA
C,andDFI
(SCS
A)
SG:21
PG:23
herbal-m
ineral
supp
lementA
ddyzoa/3
mon
ths
SG:totalmotility:
23.2±17.3%→33.4±23.2%
(𝑃=0.008)
Progressivem
otility:
15.7±12.6%→22.6±18.0%
(𝑃=0.024)
Chen
etal.[34]
2012
O,A
/sperm
concentration
and%of
progressively
motile
sperm,the
rateof
clinicalpregn
ancy
Oligosp:
64(SG:33+CG
:31)
Asth
eno:42
(SG:22+CG
:20)
Oligosperm
ia:
CG:tam
oxifen10mgbid
SG:tam
oxifen10mgbid+
vit.E100m
gtid
Asth
enosperm
ia:
CG:levocarnitin
eoral
solutio
n1b
ottle
bid
SG:levocarnitin
eoral
solutio
n1b
ottle
bid+vit.
E100m
gtid
/3mon
ths
Oligosperm
ia:
then
umbero
fspo
ntaneous
pregnanciesa
fterth.wereC
G:0,and
SG:6
(𝑃<0.01).
Asth
enosperm
ia:
after
th.the
numbersof
cases
evaluatedas
with
noor
slight
improvem
entinthe%
ofprogressively
motile
sperm
were7
and2(𝑃<0.01),4and8(𝑃<0.01),
andthen
umbero
fspo
ntaneous
pregnanciesC
G:5,and
SG:9
(𝑃<0.01).
Asth
enosperm
:afte
rth,
then
umbero
fcases
evaluatedas
with
mod
erateo
rmarked
improvem
entinthe
percentage
ofprogressively
motile
sperm
was
3and2
(𝑃>0.05)a
nd1and
1(𝑃>0.05)
Wangetal.[35]
2010
A/basicsperm
parameters
135
Group
A(𝑛=68)
andB(𝑛=67)
Group
A:L-carnitin
e2g
/day
+vitamin
EGroup
B:vitamin
E/3
mon
ths
Group
A:↑
%of
forw
ardmotile
sperm
(28.6%±9.2%
to45.4%±11.1%,𝑃<0.01),ther
ateo
fspon
taneou
spregn
ancy↑(31.1%)
than
ingrou
pB(3.8%)a
fterthe
treatment(𝑃<0.01).
Group
A:sperm
density
andthe%
ofthes
perm
ofno
rmalmorph
olog
y(𝑃>0.05).
Piom
boni
etal.[36]
2008
AT+leuk
ocytosis/sperm
parameters,DNAdamage
(acridineo
range)
51(SG:36+CG
:15)
SG:beta-glucan
20mg,
ferm
entedpapaya
50mg,
lactoferrin
97mg,vit.C
30mg,andvit.E5m
g,twicep
erday/3mon
ths
SG:%
ofmorph
ologicallyno
rmal
sperm
(17.0±5.2to29.8±6.5)a
ndtotalprogressiv
emotility(19.0±7.8
to34.8±6.8),↓in
leuk
ocytec
onc.
(2.2±0.9to0.9±0.2),all𝑃<0.01
Structuralsperm
characteris
ticsa
swellas
chromatin
integrity
were
also
improved
after
treatment.
Balerciaetal.[37]
2004
iA(W
HO1999)/basic
sperm
parameters,
seminalplasmaa
ndsperm
CoQ
10,and
phosph
atidylcholine(PC
)
22CoQ
10200m
g2x/day/6
mon
ths
CoQ
10sem.plasm
a(ng
/mL:
42.0±5.1to127.1±1.9(𝑃<0.005))
CoQ
10sperm
cells
(ng/10
6cells):
3.1±0.4to6.5±0.3(𝑃<0.05)
PCsem.plasm
a(𝜇M):1.49±0.50to
5.84±1.15(𝑃<0.05)
PCsperm
cells
(nmol/10
6cells):
6.83±0.98to9.67±1.23(𝑃<0.05)
Sperm
cellmotility9.13±2.50%
to16.34±3.43%
after
th.(𝑃<0.05)
Sperm
conc.and
sperm
morph
olog
y
BioMed Research International 7
Table1:Con
tinued.
Stud
y/author
Year
Patients/test
Num
bero
fpatients
Antioxidant/durationof
th.
Sign
ificant
improvem
ent
Non
significant
improvem
ent
Negativee
ffect
Moslemiand
Tavanb
akhsh[38]
2011
iAT/semen
parameters
andpregnancyrates
690(analysis
on525)
Se200𝜇
g+vitamin
E40
0units/
min.100
days
52.6%(362
cases)totalimprovem
ent
insperm
motility,m
orph
ology,or
both
and10.8%(75cases)
spon
taneou
spregn
ancy
versus
notre
atment(95%confi
denceinterval):
3.08
to5.52;𝑃≤0.001
Norespon
seto
treatment
occurred
in253cases
(36.6%
)
Keskes-Ammar
etal.
[39]
2003
Infertile
men/basicsperm
parameters,MDA,and
serum
vitamin
Elevel.
54:
SG:28(20analyzed)
CG:26
SG:vitamin
E40
0mg+Se
225𝜇
g/day
CG:vitamin
B4.5g
/day/3
mon
ths
SG:↓
inMDAconcentrations
andan
↑of
sperm
motility
Cavallini
etal.[40
]2012
IdiopathicOAT
/basic
sperm
parametersa
ndaneuploidy
(FISH)
55(analysis
on33:
22respon
der—
grou
p1
+11
nonrespo
nder—
grou
p2)
L-carnitine
1ggiventwice
perd
ay+
acetyl-L-carnitin
e500
mg
giventwicep
erday+on
e30
mgcinn
oxicam
tablet
every4days/3
mon
ths
Group
1versusg
roup
2:im
provem
ent
inmorph
ologyandnu
mbero
faneuploidspermatozoa
(𝑃<0.01);↑
%of
biochemicalpregnancyaft
erICSI
(54.4%
versus
9.1%,𝑃<0.01),
clinicalpregn
ancy
after
ICSI
(50%
versus
9.1%,𝑃<0.01),andliveb
irths
(45.4%
versus
9.1%,𝑃<0.01)
Num
bersof
oocytes
fertilizedandem
bryos
transfe
rred
Roseff[41]
2002
Subfertile/basic
sperm
parametersb
eforea
ndaft
ercapacitatio
nand
manno
sereceptor
bind
ing
19Py
cnogenol200m
gdaily
orally/90days
Them
eansperm
morph
olog
yfollo
wingHam
’sF-10
capacitatio
n↑
by38%follo
wingth.(𝑃<0.001)a
ndthem
anno
sereceptor
bind
ingassay
scores
improved
by19%(𝑃<0.005)
Baselin
emorph
olog
y↑
after
th.by33%
Them
ean%change
from
baselin
esperm
coun
tafter
th↓no
nsignificantly
by10%
Song
etal.[42]
2012
IdiopathicOA/basic
sperm
parameters,DFI
(SCS
A)
SG:24
CG:26
SG:vit.
E+xu
anju
caps
CG:vit.
E/3mon
ths
SGversus
CG:↓
DFI
after
th.:
29.57±12.19versus34.09±10.32,
𝑃<0.05
Menezoetal.[43]
2007
AtleastT
WOpervious
failu
resIVFor
ICSI,D
FI>15%/D
FIandthed
egree
ofsperm
decond
ensatio
n(SCS
A)
58
VitaminsC
andE40
0mg
each,𝛽
-carotene18m
g,Zn
500𝜇
mol,and
Se1𝜇
mol/90days
↓DNAfragmentatio
n:−9.1
%,
𝑃<0.0004
↑in
sperm
decond
ensatio
n(+22.8%,𝑃<0.0009).
Greco
etal.[44
]2005
TUNEL>15%/basicsperm
parameters,TU
NEL
38(26OAT
+6OT
+6no
rmal)
Vit.C1g
+vit.E1g/2
mon
ths
TUNEL
positives
perm
:24.0±7.9to
8.2±4.3(𝑃<0.001)
Clinicalpregnancyaft
erICSI:from
6.9%
to48.2%(𝑃<0.05)
Implantatio
nrateaft
erICSI:from
2.2%
to19.6%(𝑃<0.01)
Sperm
conc:17.9±16.3to
18.3±17.9
Sperm
motil.:40.6±24.8
to39.9±19.0
Normalsperm
morph
.:10.5±8.3to
9.6±0.4,all
𝑃>0.05

8 BioMed Research International
Table1:Con
tinued.
Stud
y/author
Year
Patients/test
Num
bero
fpatients
Antioxidant/durationof
th.
Sign
ificant
improvem
ent
Non
significant
improvem
ent
Negativee
ffect
Greco
etal.[45]
2005
TUNEL>15%/basicsperm
parameters,TU
NEL
SG:32
PG:32
Vit.C1g
+vit.E1g/2
mon
ths
SG:↓
fragm.D
NA:
22.1±7.7→9.1±7.2(𝑃<0.001)
PG:T
UNEL
:22.4±7.8
→22.9±7.9
Raiganietal.[46]
2013
OAT
/sperm
quality,
sperm
mito
chon
drial
functio
n,sperm
chromatin
status,semen
andbloo
dfolate,zinc,B12,
TAC,
andMDAconcentr.
83Fo
licacid
5mg/day±Zn
sulphate220m
g/day
versus
placebo/16
weeks
Sperm
chromatin
integrity
(%)↑
ingrou
preceivingon
lyZn
sulphate
treatment(𝑃=0.048)
Sperm
conc.↑
ingrou
preceivingthec
ombinedth.
offolic
acid
andZn
sulphateandalso
inthe
grou
preceivingon
lyfolic
acid
th.;(𝑃=0.056and
𝑃=0.05,respectively
).
Trem
ellenetal.[47]
2007
Malefactorinfertility,
TUNEL>25%/embryo
quality,pregn
ancy
and
fertilizatio
nrateaft
erIV
F-ICSI
SG:36
PG:16
Menevit(likopen,
vit.C,
vit.E,
Zn,Se,folate,and
garlic)/3
mon
ths
Pregnancyrateaft
erICSI
inSG
:38.5%,versusP
G:16%
(𝑃=0.046)
Safarin
ejad
etal.[48]
2011
iOAT
/sem
enparameters
andTA
Cof
seminal
plasma
260
(SG:130,
PG:130)
Saffron
60mg/day/26
weeks
Nosta
tistic
allysig
nificant
improvem
entsin
either
grou
pin
anyof
the
studied
semen
parameters
Nadjarzadeh
etal.[49]
2011
iOAT
/basicsperm
parameters,TA
C47
CoQ
10200m
g/day/12
weeks
versus
placebo
SG:↑
TAC(𝑃<0.05)
Semen
parameterso
fCoQ
10grou
p
Com
haire
etal.[50]
2000
Infertile
men/sperm
characteris
tics,RO
S,fatty
acidso
fsperm
mem
brane
phosph
olipids,sperm
oxidized
DNA
(8-O
H-dG),andindu
ced
AR
27N-acetyl-c
ysteineo
rvitaminsA
+Eand
essentialfattyacids
↓RO
S,↑AR
Noim
provem
entinsperm
motilityandmorph
olog
yor↓of
roun
dcells
and
whitebloo
dcells
insemen.Sperm
concentration↑in
oligozoo
sp.m
en(7.4±1.3
to12.5±1.9
million/mL).
Legend
:Add
yzoa:G
okshura(Trib
ulus
terrestris)200m
g,Ashtavarga200m
g,Gud
uchi
(Tinospora
cordifolia)150
mg,
Ashwagandh
a(W
ithania
Somnifer
a)150m
g,Amalaki(Em
blica
officin
alis)
75mg,
Balamoo
l(Sidacordifolia)7
5mg,
Vridhadh
aru(Argyreia
speciosa)7
5mg,
Shatavari(Asparagusracem
osus)7
5mg,
Shwet
musli(Chlorophytum
arun
dina
ceum
)150
mg,
Shud
dhakapikachchhu
(Purified
Mucun
aprurien
s)150m
g,Va
rahikand
(Tacca
aspera)30
mg,
Chop
chin
(Smila
xchina)
30mg,
Vidarik
and(Ip
omoeadigitata)30
mg,
Mun
jatak(Eulophiacampestris)
15mg,
Purnachand
rodaya
rasa
45mg,
Suvarnavang30
mg,
Muk
tashuk
tibh
asma30
mg,
Suvarnam
akshik
bhasma30
mg,
Shilajit
shud
dha30
mg,
Abhrak
bhasma15mg,
Makardh
wajrasa
15mg,
Rasa
sindu
r5mg;AR:
acrosomereactio
n;CG
:con
trolg
roup
;DDS:DNA
degraded
sperm;D
FI:D
NAfragmentatio
nindex;Fertilo
vitM
plus:L-citrullin
e(20.2%),L-carnitine-L-ta
rtrate,D
-alpha-to
coph
erylacetate,hydroxypropylm
ethylcellulose
(capsulecoating),acidifiertartaric
acid,
L-ascorbicacid
(6.7%),partingcompo
undsilicon
dioxide,calcium
carbon
ate,lycopene,N
-acetyl-L
-cysteine,glutathion
e(redu
ced),cornsta
rch,zinc
oxide,coenzymeQ
10,vegetableoil,shellacc
oatin
g,pteroyl-L
-glutam
ate,sodium
selenite,coloringagenttitanium
dioxide(
capsule),coloringagento
rangey
ellow
S(capsule);CoQ
10:coencym
eQ10,FISH:fluo
rescentinsituhybridization;
FSH:follicle-stim
ulatingho
rmon
e;ICSI:intracytoplasmicsperm
injection;
iOAT
:idiop
athicOAT
;IVF:
invitro
fertilizatio
n;LH
:luteinizing
horm
one;MDA:m
alon
dialdehyde;M
SOME:
motile
sperm
organelle
morph
olog
yexam
ination;
OAT
:oligoastheno
teratozoosperm
ia;PG:placebo
grou
p;RO
S:reactiv
eoxygenspecies;Saire
i-to:aC
hinese
herbaldrug;SCS
A:sperm
chromatin
structureassay;Se:sele
nium
;SG:study
grou
p;T:
testo
sterone;TAC
:total
antio
xidant
capacity;T
UNEL
:TdT
(term
inaldeoxyribon
ucleotidyltransfe
rase)—
mediateddU
TPnick-end
labelin
g;Xu
anju:Formica
fusca,Herba
epim
edii,Fructusc
nidii,andFructuslycii;Zn
:zinc.

BioMed Research International 9
vitamin E with degree of DFI of 34.09±10.32 (𝑃 < 0.05) [42].Greco et al. [44, 45] had proved that 1 g of vitamin C and 1 g ofvitamin E together taken for 2months significantly decreasedthe degree of DNA fragmentation from 22.1 ± 7.7 to 9.1 ± 7.2(𝑃 < 0.001) [45]. Raigani et al. showed that zinc sulphatesignificantly improved sperm chromatin integrity [46].
3.5. Pregnancy Rate. CoQ10 [24], clomiphene citrate withvitamin E [26], lycopene [31], L-carnitine with vitamin E [34,35], and selenium with vitamin E [38] significantly improvedspontaneous pregnancy rates during duration of treatment,while L-carnitine with cinnoxicam [40] and vitamins C andE together [44] significantly improved pregnancy rates percycle after assisted reproductive technology with intracyto-plasmic sperm injection (ICSI). Ghanem et al. proved higherspontaneous pregnancy rate in 30 participants after the intakeof combination of 25mg clomiphene citrate and 400mgvitamin E per day for 6months (36.7%) than in placebo group(13.3%) with 𝑃 = 0.037 [26]. L-Carnitine, 2 g, with vitamin Etaken for 3 months improved spontaneous pregnancy rate to31.1% compared to vitamin E group with pregnancy rate of3.8% (𝑃 < 0.01) [35]. Another example in study by Greco etal. confirmed higher pregnancy rate after 2 months therapywith 1 g of vitamin C and 1 g of vitamin E daily. After ICSIclinical pregnancy rate was 48.2% after therapy versus 6.9%before therapy (𝑃 < 0.05) [44].
3.6. Negative or No Effect on Sperm Parameters. In this reviewwe find out also rare negative effects of antioxidants on spermparameters or no effect. Pycnogenol caused nonsignificantfall in baseline sperm count by 10% [41]. Similarly, treatmentwith vitamins C and E, ß-carotene, zinc, and selenium signif-icantly increased sperm decondensation [43]. Large researchon saffron showed no statistically significant improvementsin any of the studied semen parameters [48].
3.7. Other Parameters. We looked at the basic sperm param-eters but there were also many other positive influences; forexample, CoQ10 and pentoxifylline caused improvements intotal antioxidant capacity and acrosome reaction [22, 25, 49,50]; FSH value [22, 23] decreased after CoQ10 treatment,semen leucocyte concentration decreased [36], and level ofROS [50] decreased after antioxidant mixtures. Antioxidantsprotect unsaturated fatty acids and so provide fluidity thatis necessary for membrane fusion events like the acrosomereaction. Although hormonal abnormalities are not alwaysevident, iOAT is sometimes associated with lower serumtestosterone and inhibin levels and higher serum estradiol,LH, and FSH levels [55, 56].The increased serumFSH level inmen with azoospermia or severe oligozoospermia indicatesdamaged seminiferous tubule [57] and is inversely associatedwith sperm concentration, motility, and morphology [58].ROS has been found in the seminiferous tubules and seminalplasma of most patients with iOAT [59]. Decreased levels ofROS due to antioxidant consumption can cause fall in serumFSH level. Leukocytes are potential source of ROS and due toprotective influence of antioxidants their concentration maydecrease [15]. In addition, studies have found an increase in
inhibin B value [23] and in superoxide-dismutase- (SOD-)like and catalase activity [21, 25], which among others rep-resent the total antioxidant capacity of seminal plasma [60].Inhibin B in positively correlated with sperm concentrationand is, like FSH, thought to be a marker of spermatogenesisand Sertoli cell function [61, 62].
4. Conclusions
Most of the published studies were randomized and placebocontrolled. The majority of studies confirmed beneficialeffect of different antioxidants on at least one of the semenparameters and the biggest effect was determined on spermmotility. In many of these trials combinations of moreantioxidants were assessed. The optimal dosages of one ormore antioxidants were not defined.
Most commonly antioxidants studied were vitamin E,vitamin C, selenium, CoQ10, N-acetyl-cysteine, L-carnitine,and zinc and their favorable effect was confirmed. Accordingto this review favorable effects on iOAT have been deter-mined with CoQ10, vitamin E, selenium, and also vitamin CandN-acetyl-cysteine treatments. In case of oligozoospermiavitamin E and CoQ10 were most often proved to be effective.Favorable effects on asthenozoospermia havemost often beendeterminedwith vitamin E, CoQ10, and selenium treatments.In teratozoospermia selenium and CoQ10 treatments weremost often proved to be effective. In addition, combination ofvitamin C and E showed the biggest favorable effect on DNAfragmentation; similar effects were determined with zinc andselenium treatments.
In conclusion, antioxidants play an important role inprotecting semen from ROS and can improve basic spermparameters in case of idiopathic oligoasthenoteratozoosper-mia.
Conflict of Interests
The authors declare that they have no conflict of interestsregarding the publication of this paper.
References
[1] I. D. Sharlip, J. P. Jarow,A.M. Belker et al., “Best practice policiesfor male infertility,” Fertility and Sterility, vol. 77, no. 5, pp. 873–882, 2002.
[2] F. M. Siddiq and M. Sigman, “A new look at the medicalmanagement of infertility,” Urologic Clinics of North America,vol. 29, no. 4, pp. 949–963, 2002.
[3] T. G. Cooper, E. Noonan, S. von Eckardstein et al., “WorldHealth Organization reference values for human semen char-acteristics,” Human Reproduction Update, vol. 16, no. 3, ArticleID dmp048, pp. 231–245, 2009.
[4] N. Desai, R. Sharma, K. Makker, E. Sabanegh, and A. Agarwal,“Physiologic and pathologic levels of reactive oxygen species inneat semen of infertile men,” Fertility and Sterility, vol. 92, no.5, pp. 1626–1631, 2009.
[5] A. Zini, M. San Gabriel, and A. Baazeem, “Antioxidants andsperm DNA damage: a clinical perspective,” Journal of AssistedReproduction and Genetics, vol. 26, no. 8, pp. 427–432, 2009.

10 BioMed Research International
[6] A. Agarwal, K. P. Nallella, S. S. R. Allamaneni, and T. M.Said, “Role of antioxidants in treatment of male infertility: anoverview of the literature,” Reproductive BioMedicine Online,vol. 8, no. 6, pp. 616–627, 2004.
[7] J. F. Griveau and D. Le Lannou, “Reactive oxygen species andhuman spermatozoa: physiology and pathology,” InternationalJournal of Andrology, vol. 20, no. 2, pp. 61–69, 1997.
[8] J. Rivlin, J. Mendel, S. Rubinstein, N. Etkovitz, and H. Breitbart,“Role of hydrogen peroxide in sperm capacitation and acro-some reaction,” Biology of Reproduction, vol. 70, no. 2, pp. 518–522, 2004.
[9] S. Lopes, A. Jurisicova, J.-G. Sun, and R. F. Casper, “Reactiveoxygen species: potential cause for DNA fragmentation inhuman spermatozoa,” Human Reproduction, vol. 13, no. 4, pp.896–900, 1998.
[10] R. J. Aitken, G. N. De Iuliis, J. M. Finnie, A. Hedges, and R.I. McLachlan, “Analysis of the relationships between oxidativestress, DNA damage and sperm vitality in a patient population:development of diagnostic criteria,” Human Reproduction, vol.25, no. 10, pp. 2415–2426, 2010.
[11] S.-H. Kao, H.-T. Chao, H.-W. Chen, T. I. S. Hwang, T.-L. Liao,and Y.-H. Wei, “Increase of oxidative stress in human spermwith lowermotility,”Fertility and Sterility, vol. 89, no. 5, pp. 1183–1190, 2008.
[12] R. J. Aitken, J. S. Clarkson, and S. Fishel, “Generation of reactiveoxygen species, lipid peroxidation, and human sperm function,”Biology of Reproduction, vol. 41, no. 1, pp. 183–197, 1989.
[13] A. Agarwal, R. A. Saleh, and M. A. Bedaiwy, “Role of reactiveoxygen species in the pathophysiology of human reproduction,”Fertility and Sterility, vol. 79, no. 4, pp. 829–843, 2003.
[14] A. Zini and N. Al-Hathal, “Antioxidant therapy in male infer-tility: fact or fiction?” Asian Journal of Andrology, vol. 13, no. 3,pp. 374–381, 2011.
[15] J. G. Alvarez, J. C. Touchstone, L. Blasco, and B. T. Storey,“Spontaneous lipid peroxidation and production of hydrogenperoxide and superoxide in human spermatozoa. Superoxidedismutase as major enzyme protectant against oxygen toxicity,”Journal of Andrology, vol. 8, no. 5, pp. 338–348, 1987.
[16] R. K. Sharma and A. Agarwal, “Role of reactive oxygen speciesin male infertility,” Urology, vol. 48, no. 6, pp. 835–850, 1996.
[17] R. Smith, D. Vantman, J. Ponce, J. Escobar, and E. Lissi,“Total antioxidant capacity of human seminal plasma,” HumanReproduction, vol. 11, no. 8, pp. 1655–1660, 1996.
[18] P. P. Pahune, A. R. Choudhari, and P. A. Muley, “The totalantioxidant power of semen and its correlation with the fertilitypotential of human male subjects,” Journal of Clinical andDiagnostic Research, vol. 7, no. 6, pp. 991–995, 2013.
[19] B. Wirleitner, P. Vanderzwalmen, A. Stecher et al., “Dietarysupplementation of antioxidants improves semen quality ofIVF patients in terms of motility, sperm count, and nuclearvacuolization,” International Journal for Vitamin and NutritionResearch, vol. 82, no. 6, pp. 391–398, 2012.
[20] C. Abad, M. J. Amengual, J. Gosalvez et al., “Effects of oralantioxidant treatment upon the dynamics of human spermDNA fragmentation and subpopulations of sperm with highlydegraded DNA,” Andrologia, vol. 45, no. 3, pp. 211–216, 2013.
[21] M. R. Safarinejad, “Effect of omega-3 polyunsaturated fatty acidsupplementation on semen profile and enzymatic anti-oxidantcapacity of seminal plasma in infertile men with idiopathicoligoasthenoteratospermia: a double-blind, placebo-controlled,randomised study,” Andrologia, vol. 43, no. 1, pp. 38–47, 2011.
[22] M. R. Safarinejad, “Efficacy of coenzyme Q10 on semen param-eters, sperm function and reproductive hormones in infertilemen,” Journal of Urology, vol. 182, no. 1, pp. 237–248, 2009.
[23] M. R. Safarinejad, S. Safarinejad, N. Shafiei, and S. Safarinejad,“Effects of the reduced form of coenzyme Q10 (ubiquinol)on semen parameters in men with idiopathic infertility: adouble-blind, placebo controlled, randomized study,” Journal ofUrology, vol. 188, no. 2, pp. 526–531, 2012.
[24] M. R. Safarinejad, “The effect of coenzyme Q10
supplemen-tation on partner pregnancy rate in infertile men with idio-pathic oligoasthenoteratozoospermia: an open-label prospec-tive study,” International Urology and Nephrology, vol. 44, no.3, pp. 689–700, 2012.
[25] M. R. Safarinejad, “Effect of pentoxifylline on semen parame-ters, reproductive hormones, and seminal plasma antioxidantcapacity in men with idiopathic infertility: a randomizeddouble-blind placebo-controlled study,” International Urologyand Nephrology, vol. 43, no. 2, pp. 315–328, 2011.
[26] H. Ghanem, O. Shaeer, and A. El-Segini, “Combinationclomiphene citrate and antioxidant therapy for idiopathic maleinfertility: a randomized controlled trial,” Fertility and Sterility,vol. 93, no. 7, pp. 2232–2235, 2010.
[27] M. R. Safarinejad and S. Safarinejad, “Efficacy of seleniumand/or N-Acetyl-Cysteine for improving semen parameters ininfertile men: a double-blind, placebo controlled, randomizedstudy,” Journal of Urology, vol. 181, no. 2, pp. 741–751, 2009.
[28] M. Akmal, J. Q. Qadri, N. S. Al-Waili, S. Thangal, A. Haq, andK. Y. Saloom, “Improvement in human semen quality after oralsupplementation of vitamin C,” Journal of Medicinal Food, vol.9, no. 3, pp. 440–442, 2006.
[29] Y. Shi, Y. Huang, X. Shang, P. Zhu, and G. Liu, “Effects ofxinxibao on sperm quality in oligoasthenozoospermic men,”Zhonghua Nan Ke Xue, vol. 10, no. 10, pp. 758–760, 2004.
[30] M. Suzuki, T. Kurabayashi, Y. Yamamoto, K. Fujita, and K.Tanaka, “Effects of antioxidant treatment in oligozoospermicand asthenozoospermic men,” Journal of Reproductive Medicinefor the Obstetrician and Gynecologist, vol. 48, no. 9, pp. 707–712,2003.
[31] N. P. Gupta and R. Kumar, “Lycopene therapy in idiopathicmale infertility—a preliminary report,” International Urologyand Nephrology, vol. 34, no. 3, pp. 369–372, 2002.
[32] G. M. Busetto, A. Koverech, M. Messano, G. Antonini, E. DeBerardinis, and V. Gentile, “Prospective open-label study on theefficacy and tolerability of a combination of nutritional supple-ments in primary infertile patients with idiopathic astenoter-atozoospermia,” Archivio Italiano Di Urologia, Andrologia, vol.84, no. 3, pp. 137–140, 2012.
[33] R. Kumar, V. Saxena, M. B. Shamsi, S. Venkatesh, and R.Dada, “Herbo-mineral supplementation in men with idio-pathic oligoasthenoteratospermia: a double blind randomizedplacebo-controlled trial,” Indian Journal of Urology, vol. 27, no.3, pp. 357–362, 2011.
[34] X. F. Chen, Z. Li, P. Ping, J. C. Dai, F. B. Zhang, and X. J. Shang,“Efficacy of natural vitaminE on oligospermia and asthenosper-mia: a prospective multi-centered randomized controlled studyof 106 cases,” Zhonghua Nan Ke Xue, vol. 18, no. 5, pp. 428–431,2012.
[35] Y.-X. Wang, S.-W. Yang, C.-B. Qu et al., “L-carnitine: safe andeffective for asthenozoospermia,” Zhonghua Nan Ke Xue, vol.16, no. 5, pp. 420–422, 2010.
[36] P. Piomboni, L. Gambera, F. Serafini, G. Campanella, G.Morgante, and V. De Leo, “Sperm quality improvement after
BioMed Research International 11
natural anti-oxidant treatment of asthenoteratospermic menwith leukocytospermia,” Asian Journal of Andrology, vol. 10, no.2, pp. 201–206, 2008.
[37] G. Balercia, F. Mosca, F. Mantero et al., “Coenzyme Q10 supple-mentation in infertile men with idiopathic asthenozoospermia:an open, uncontrolled pilot study,” Fertility and Sterility, vol. 81,no. 1, pp. 93–98, 2004.
[38] M. K. Moslemi and S. Tavanbakhsh, “Selenium-vitamin Esupplementation in infertile men: effects on semen parametersand pregnancy rate,” International Journal of General Medicine,vol. 4, pp. 99–104, 2011.
[39] L. Keskes-Ammar, N. Feki-Chakroun, T. Rebai et al., “Spermoxidative stress and the effect of an oral vitamin e and seleniumsupplement on semen quality in infertile men,” Systems Biologyin Reproductive Medicine, vol. 49, no. 2, pp. 83–94, 2003.
[40] G. Cavallini, M. C. Magli, A. Crippa, A. P. Ferraretti, and L.Gianaroli, “Reduction in sperm aneuploidy levels in severeoligoasthenoteratospermic patients after medical therapy: apreliminary report,” Asian Journal of Andrology, vol. 14, no. 4,pp. 591–598, 2012.
[41] S. J. Roseff, “Improvement in sperm quality and function withFrenchmaritime pine tree bark extract,” Journal of ReproductiveMedicine for theObstetrician andGynecologist, vol. 47, no. 10, pp.821–824, 2002.
[42] B. Song, X. J. He, H. H. Jiang, Y. W. Peng, H. Wu, and Y. X.Cao, “Compound Xuanju Capsule combined with vitamin Eimproves sperm chromatin integrity,” Zhonghua Nan Ke Xue,vol. 18, no. 12, pp. 1105–1107, 2012 (Chinese).
[43] Y. J. R. Menezo, A. Hazout, G. Panteix et al., “Antioxidantsto reduce sperm DNA fragmentation: an unexpected adverseeffect,” Reproductive BioMedicine Online, vol. 14, no. 4, article2669, pp. 418–421, 2007.
[44] E. Greco, S. Romano, M. Iacobelli et al., “ICSI in cases of spermDNA damage: beneficial effect of oral antioxidant treatment,”Human Reproduction, vol. 20, no. 9, pp. 2590–2594, 2005.
[45] E. Greco, M. Iacobelli, L. Rienzi, F. Ubaldi, S. Ferrero, and J.Tesarik, “Reduction of the incidence of sperm DNA fragmen-tation by oral antioxidant treatment,” Journal of Andrology, vol.26, no. 3, pp. 349–353, 2005.
[46] M. Raigani, B. Yaghmaei, N. Amirjannti et al., “Themicronutri-ent supplements, zinc sulphate and folic acid, did not amelioratesperm functional parameters in oligoasthenoteratozoospermicmen,” Andrologia, 2013.
[47] K. Tremellen, G. Miari, D. Froiland, and J. Thompson, “Arandomised control trial examining the effect of an antioxidant(Menevit) on pregnancy outcome during IVF-ICSI treatment,”Australian andNew Zealand Journal of Obstetrics and Gynaecol-ogy, vol. 47, no. 3, pp. 216–221, 2007.
[48] M. R. Safarinejad, N. Shafiei, and S. Safarinejad, “A prospectivedouble-blind randomized placebo-controlled study of the effectof saffron (Crocus sativus Linn.) on semen parameters and sem-inal plasma antioxidant capacity in infertilemenwith idiopathicoligoasthenoteratozoospermia,” Phytotherapy Research, vol. 25,no. 4, pp. 508–516, 2011.
[49] A. Nadjarzadeh, M. R. Sadeghi, N. Amirjannati et al., “Coen-zyme Q10 improves seminal oxidative defense but does notaffect on semen parameters in idiopathic oligoasthenoterato-zoospermia: a randomized double-blind, placebo controlledtrial,” Journal of Endocrinological Investigation, vol. 34, no. 8, pp.e224–e228, 2011.
[50] F. H. Comhaire, A. B. Christophe, A. A. Zalata,W. S. Dhooge, A.M. A. Mahmoud, and C. E. Depuydt, “The effects of combined
conventional treatment, oral antioxidants and essential fattyacids on sperm biology in subfertile men,” ProstaglandinsLeukotrienes and Essential Fatty Acids, vol. 63, no. 3, pp. 159–165, 2000.
[51] World Health Organization, WHO Laboratory Manual for theExamination and Processing of Human Semen, WHO Press,Geneva, Switzerland, 5th edition, 2010.
[52] World Health Organization, WHO Laboratory Manual for theExamination of Human Semen and Sperm-Cervical MucusInteraction,WHOPress, Geneva, Switzerland, 4th edition, 1999.
[53] D. S. Irvine, J. P. Twigg, E. L. Gordon, N. Fulton, P. A. Milne,and R. J. Aitken, “DNA integrity in human spermatozoa:relationships with semen quality,” Journal of Andrology, vol. 21,no. 1, pp. 33–44, 2000.
[54] J. G. Franco Jr., R. L. R. Baruffi, A. L. Mauri, C. G. Petersen,J. B. A. Oliveira, and L. Vagnini, “Significance of large nuclearvacuoles in human spermatozoa: implications for ICSI,” Repro-ductive BioMedicine Online, vol. 17, no. 1, pp. 42–45, 2008.
[55] E. H. Yanushpolsky, J. A. Politch, J. A. Hill, and D. J. Anderson,“Is leukocytospermia clinically relevant?” Fertility and Sterility,vol. 66, no. 5, pp. 822–825, 1996.
[56] K. C. Cheng, D. S. Cahill, H. Kasai, S. Nishimura, and L. A.Loeb, “8-Hydroxyguanine, an abundant form of oxidative DNAdamage, causes G → T and A → C substitutions,”The Journalof Biological Chemistry, vol. 267, no. 1, pp. 166–172, 1992.
[57] M. Bergmann, H. M. Behre, and E. Nieschlag, “Serum FSH andtesticular morphology in male infertility,” Clinical Endocrinol-ogy, vol. 40, no. 1, pp. 133–136, 1994.
[58] J. D. Meeker, L. Godfrey-Bailey, and R. Hauser, “Relationshipsbetween serum hormone levels and semen quality among menfrom an infertility clinic,” Journal of Andrology, vol. 28, no. 3, pp.397–406, 2007.
[59] A.Agarwal andL.H. Sekhon, “Oxidative stress and antioxidantsfor idiopathic oligoasthenoteratospermia: is it justified,” IndianJournal of Urology, vol. 27, no. 1, pp. 74–85, 2011.
[60] R. Mahfouz, R. Sharma, D. Sharma, E. Sabanegh, and A.Agarwal, “Diagnostic value of the total antioxidant capacity(TAC) in human seminal plasma,” Fertility and Sterility, vol. 91,no. 3, pp. 805–811, 2009.
[61] T. K. Jensen, A.-M. Andersson, N. H. I. Hjollund et al.,“Inhibin B as a serum marker of spermatogenesis: correlationto differences in sperm concentration and follicle-stimulatinghormone levels. A study of 349 Danish men,” Journal of ClinicalEndocrinology and Metabolism, vol. 82, no. 12, pp. 4059–4063,1997.
[62] F. H. Pierik, A. Burdorf, F. H. De Jong, and R. F. A. Weber,“Inhibin B: a novel marker of spermatogenesis,” Annals ofMedicine, vol. 35, no. 1, pp. 12–20, 2003.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com