resuscitative hypothermia academic industry roundtable hypothermia: future directions midori a....
TRANSCRIPT
RESUSCITATIVE HYPOTHERMIA ACADEMIC INDUSTRY ROUNDTABLE
Hypothermia: future directions
Midori A. Yenari, MDDepts. of Neurosurgery & Neurology
Stanford Stroke Center & Stanford UniversityStanford, CA

Introduction
• Hypothermia is a robust neuroprotectant.• Compelling pre-clinical data to justify
clinical trials• Questions at preclinical level:
duration/delay, permanent occlusion, combination with thrombolysis, combination with other treatments?
Summary: Hypothermia in Experimental Stroke
• Depth: 34.5C or lower results in comparable neuroprotection, but lower temperatures are associated with compromised hemodynamics; most consistent results with 30-33C
• **Duration: At least one hour, provided cooling begins soon after ischemia onset. Several hours (6-12 h) if cooling is delayed by more than several hours
• **Delay: consistent protection with 2-3 h delay with at least 2 h cooling; can delay up to 6 h provided cooling is maintained for 1-2d
• Long term: protection observed out to 2 mos with 2 h intraischemic cooling, or 1 h delay with prolonged cooling (2d); 70% protection in global model out to 6 mos, but extent of protection decreases over time
• **Permanent vs. Temporary: mixed results
Protect against permanent ischemia?
Less consistent data compared to temporary ischemia
Protects:Intraischemic hypothermia for 6 h ↓infarct size @ 6 h(Baker et al, Exp Neurol 1991)
Intraischemic hypothermia for 24 h ↓infarct size @ 48 h (Yamamoto et al, Stroke 2001)
↓ infarct size @ 24 h when cooling (30-34.5C) delayed up to 1 h & maintained for 1 h (Kader et al, Neurosurgery 1992)
Doesn’t protect:No difference in infarct size when cooling (33C) was instituted during ischemia,
and maintained for 1 h (Ridenour et al, Stroke 1992)
No protection when cooling to 30-36C was instituted shortly after occlusion and maintained for 2 h (Morikawa et al, JCBFM 1992)
Optimize duration/delay
• Brief intraischemic hypothermia (1-2 h) protects, but also protects when cooling begins 2-3 h after ischemia onset
• Prolonging the duration of cooling to several hours seems to lengthen the temporal therapeutic window
• What are the limits in rodents? In humans?
Combination hypothermia & rt-PA• Embolic model in rats• Hypothermia (32C), normothermia (37C) or hyperthermia (39C)
for 2 h pre/post embolization• rt-PA 2 h after embolization• Angiographic recanalization best @ 39C• rt-PA Rx itself ↓ inf. Size ~50%• @ 48h: largest infarcts (39C), smallest (32C), hypothermia ↓inf.
size by ~70%• No further improvement with rt-PA/hypothermia—is lack of
difference due to robust protection by hypothermia?• Interaction of rt-PA and temperature?• Can hypothermia prolong the window for rt-PA Rx? Reduce
hemorrhage?
(Meden et al, Br Res, 1994)

Effect of temperature on clot lysis
• rt-PA is the only approved treatment for acute stroke
• combination rt-PA and mild hypothermia?
• how does temperature influence clot lysis?
Effect of temperature on clot lysis
• Thrombin stabilized, 24 h aged clots from whole blood of donor rabbits.
• Incubate in sterile PBS at 24, 30, 33, 35, 37 & 40C.• Incubate with rt-PA (concentrations corresponding to serum levels in rabbits
given doses of 1, 3 and 6 mg/kg)
• Measure pre- and post-incubation weights
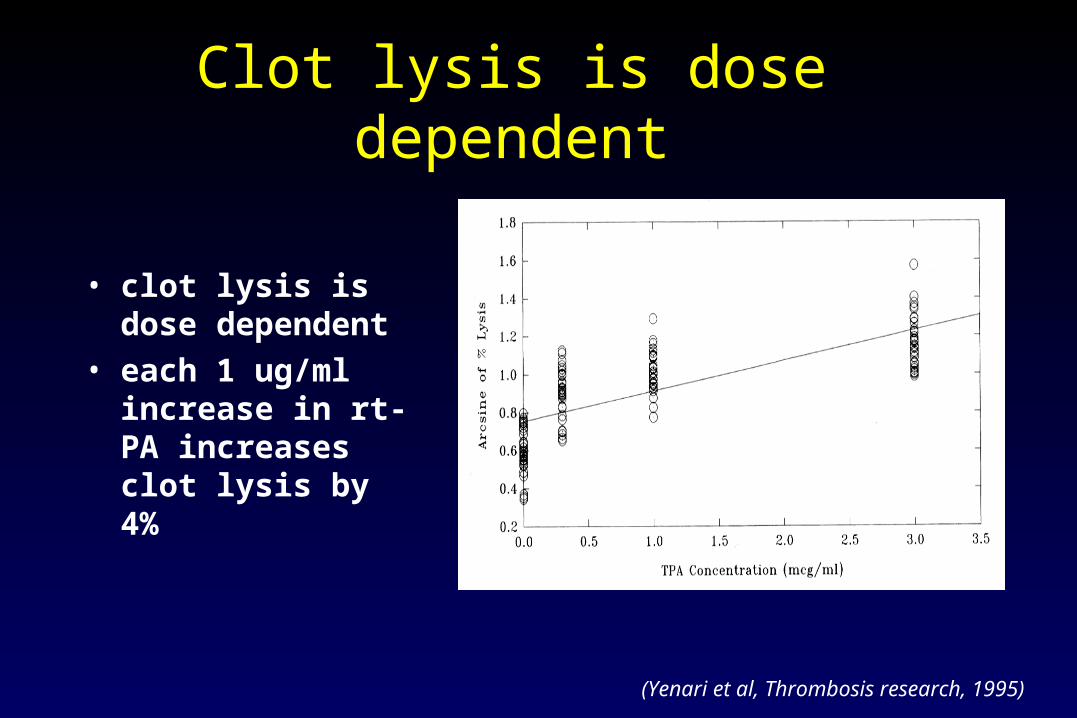
Clot lysis is dose dependent
(Yenari et al, Thrombosis research, 1995)
• clot lysis is dose dependent
• each 1 ug/ml increase in rt-PA increases clot lysis by 4%
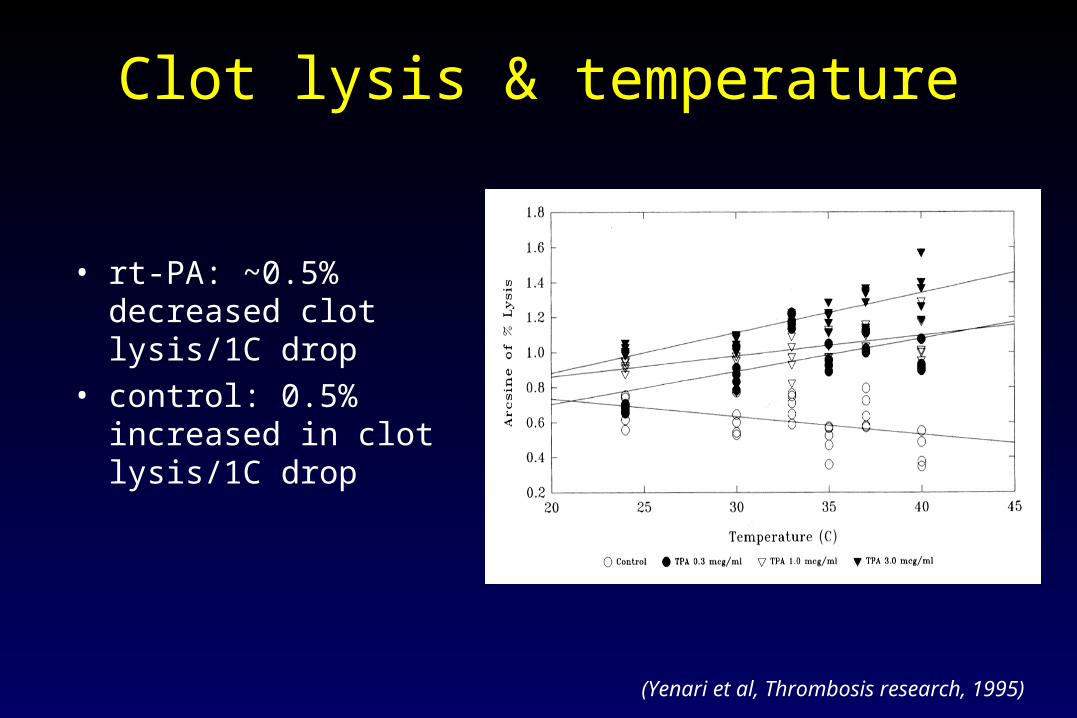
Clot lysis & temperature
• rt-PA: ~0.5% decreased clot lysis/1C drop
• control: 0.5% increased in clot lysis/1C drop
(Yenari et al, Thrombosis research, 1995)
Combination RX with hypothermia & gene therapy (Zhao et al.)
• HSV viral vectors
• Overexpress potentially neuroprotective genes
• Bcl-2 as a prototypical anti-apoptosis, anti-necrosis gene
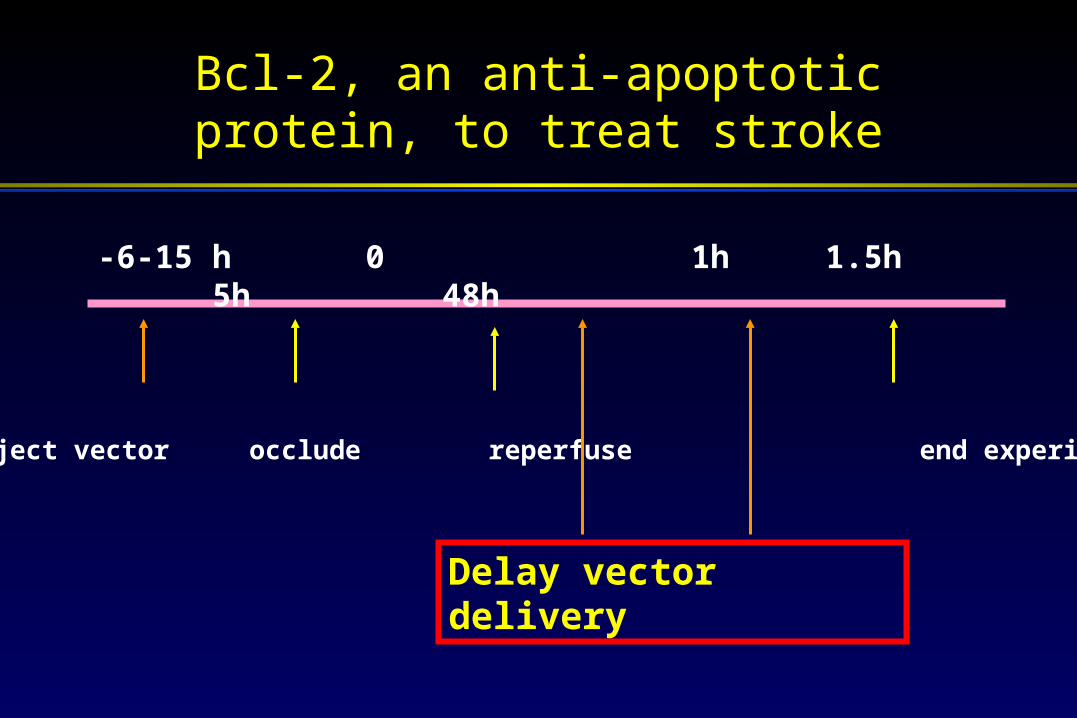
Bcl-2, an anti-apoptotic protein, to treat stroke
-6-15 h 0 1h 1.5h 5h 48h
Inject vector occlude reperfuse end experiment*
Delay vector delivery

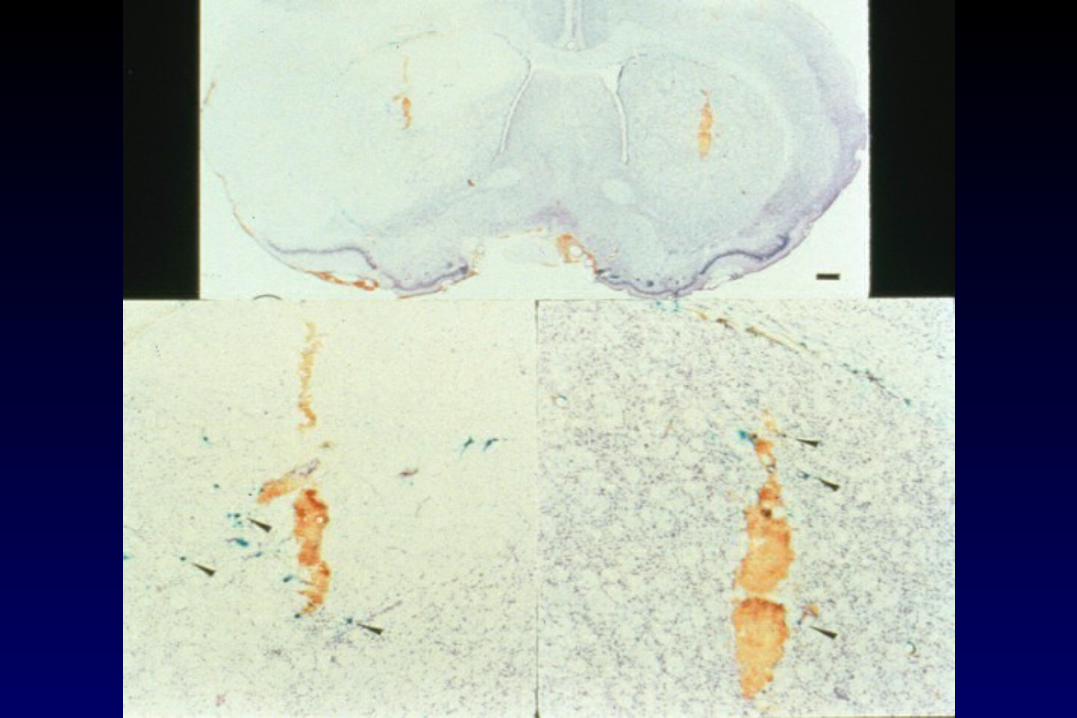
Striatal Bcl-2 overexpression protects neurons from tMCAO (Lawrence et al, JCBFM, 1995)
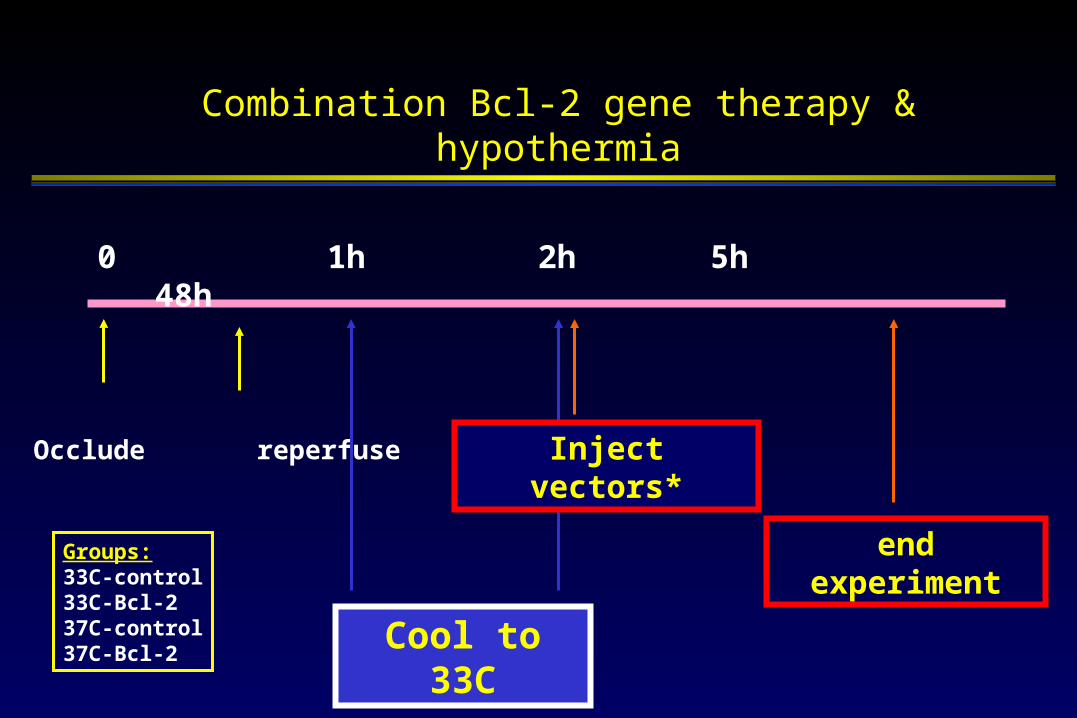
0 1h 2h 5h 48h
Occlude reperfuse
Combination Bcl-2 gene therapy & hypothermia
Cool to 33C
end experiment
Inject vectors*
Groups:33C-control33C-Bcl-237C-control37C-Bcl-2

*vs 37ºC-Bcl-2, p<0.01#vs. 33C-control, p<0.01
Hypothermia prolongs the temporal therapeutic for Bcl-2 gene therapy

Conclusions
• Permanent occlusion?
• Optimal duration/delay?
• Combination Rx with thrombolytics?
• Combination Rx with neuroprotectants?