results of treatment of colorectal cancer at the peter bent brigham hospital
TRANSCRIPT
Results of Treatment of Colorectal Cancer at the Peter Bent Brigham Hospital
THOMAS ~V. BOTSFORD, M.D., Brookline, Massachuselts, MENELAOS A. AI.IAPOULIOS, M.D., AND
LON E. CURTIS, .~t.D., Boston, Masmchusetts
From the Departments of Surgery, IIan,ard Medical School, and the Peter Bent Brigham Hospital, Boston, Massachusetts,
C OLORECTAL CANCER presently is the most common visceral neoplasm. These lesions
are accessible to relatively simple but accurate diagnostic methods, and the surgical treatment of the "early" lesion in the majority of cases is adequate. Despite these favorable aspects, the number of patients who die within five years of the onset of this disease or its complications exceeds the number who are saved [1]. The purpose of this communication is to present the experience of recent years in the treatment of cancer of the colon and rectum at the Peter Bent Brigham Hospital. It is, so to speak, our present score and will be compared in part to earlier experience at this hospital ~eported by Cheever [2] in 1930.
MATERIAL
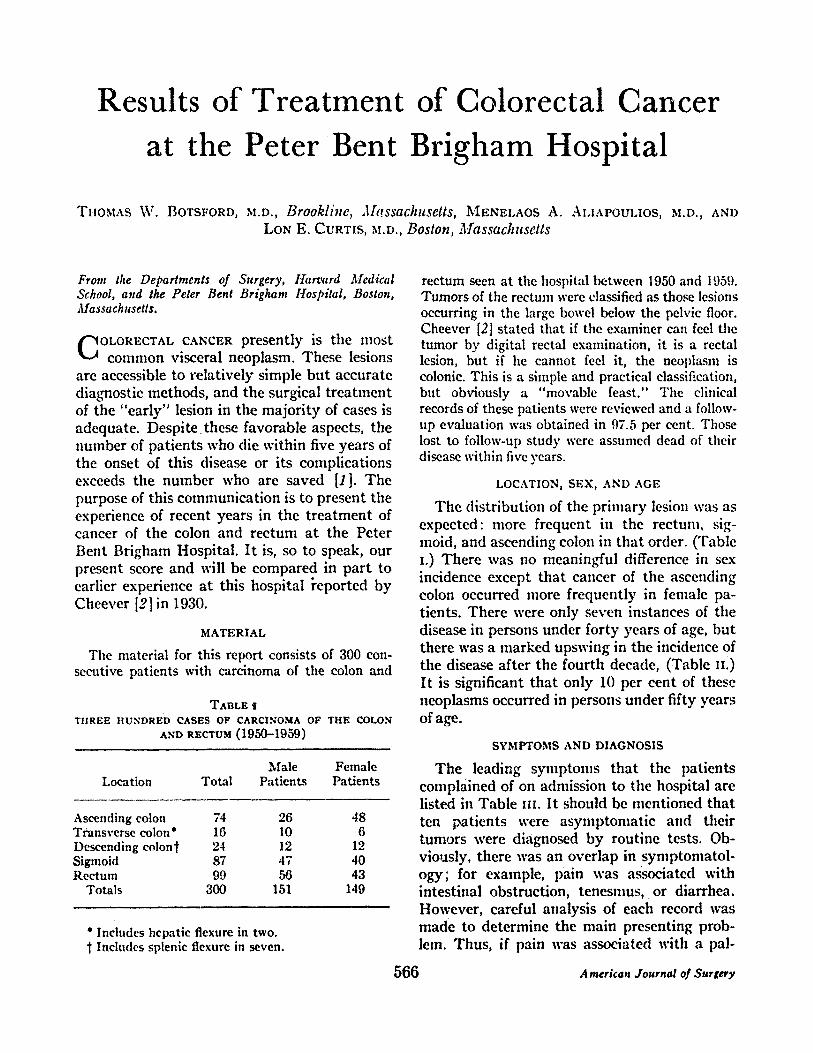
The material for this report consists of 300 con- secutive patients with carcinoma of the colon and
TABLE tI THREE HUNDRED CASES OF CARCINOMA OF' TIlE COLON
AND RECTUM (1950-1959)
Male Female Location Total Patients Patients
Ascending colon 74 26 48 Transverse colon* 16 10 6 Descending colon $ 24 12 12 Sigmoid 87 47 40 Rectum 99 56 43
Totals 300 151 149
* Includes hepatic flexure in two. Includes splenic flexure in seven.
rectum seen at the hospital between 1950 and 1959. Tumors of the rectum were classified as those lesions occurring in the large bowel below the pelvic floor. Cheerer [2] stated that if the examiner can feel tile tumor by digital rectal examination, it is a rectal lesion, but if he cannot feel it, the neolfl,~m is colonic. This is a simple and practical classification, but obviously a "movable feast." Tile clinical records of these patients were reviewed and a follow- up evaluation was obtained in 97.5 per cent. Those lost to follow-up study were assumed dead of their disease within five years.
LOCATION, SEX, AND AGE
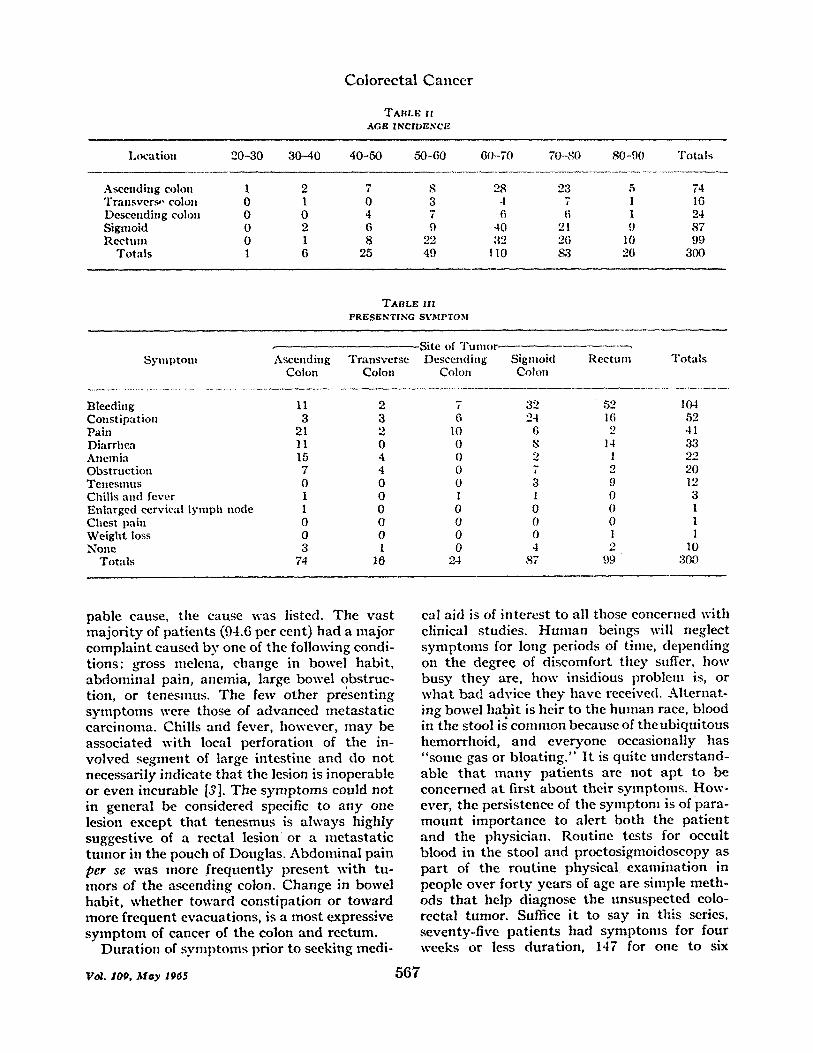
The distribution of the primary lesion was as expected: more frequent in the rectmn, sig- moid, and ascending colon in that order. ('Fable I.) There was no meaningful difference in sex incidence except that cancer of the ascending colon occurred more frequently in female pa- tients. There were only seven instances of the disease in persons under forty years of age, but there was a marked upswing in the incidence of the disease after the fourth decade, (Table II.) It is significant that only 10 per cent of these neoplasms occurred in persons under fifty years of age.
SYMPTOMS AND DIAGNOSIS
The leading symptoms that the patients complained of on admission to the hospital are listed in Table Ul. It should be mentioned that ten patients were asymptomatic and their tumors were diagnosed by routine tests. Ob- viously, there was an overlap in symptonmtol- ogy; for example, pain was a~ociated with intestinal obstruction, tenesmus, or diarrhea. However, careful analysis of each record was made to determine the main presenting prob- lem. Thus, if pain was associated with a pal-
566 American Journal o/Surgery
C o l o r e c t a l C a n c e r
"/'AnL~ H AGI~ INCIDENC/~
I,ocation 20-30 30-40 40-50 50-60 60-70 70-S0 80-9(I Totals
Ascending colon 1 2 7 S 28 23 5 74 Transver~. colon 0 1 0 3 .l 7 I 16 Descending colon 0 0 4 7 6 6 1 24 Sigmoid 0 2 6 9 40 21 9 87 Rectum 0 1 8 22 ;¢2 26 10 99
Totals 1 6 25 49 110 83 26 300
TABLt¢ l I l
PRi~S~NTING SI 'MPTOM
Site of Tumor Synu~totn Ascending Transverse Descending Sigmoid Rectum Totals
Colon Colon Colon Co|oil
Bleeding 11 2 7 32 52 104 Constipation 3 3 6 24 16 52 Pain 21 2 10 6 '2 41 Diarrhea 11 0 0 S 14 33 Anemia 15 4 0 2 1 '22 Obstruction 7 4 0 7 2 20 Tenesmus 0 0 0 3 9 12 Chills and fever I 0 1 I 0 3 Enlarged eervi~d lymph node I 0 0 0 0 1 Chest pain 0 0 0 0 0 I Weight loss 0 0 0 0 1 1 None 3 1 0 4 2 10
Totals 74 16 24 87 99 300
pable cause, the cause was listed. The vast ma jo r i ty of pat ients (94.6 per cent) had a major compla in t caused by one of the following condi- t ions: gross melena, change in bowel habi t , abdominal pain, anemia, large bowel obstruc- tion, or tenesmus. The few other present ing symp toms were those of advanced metas ta t i c carcinoma. Chills and fever, however, m a y be associated with local perforat ion of the in- volved seganent of large intest ine and do not necessarily indicate t h a t the lesion is inoperable or even incurable [3]. The symp toms could not in general be considered specific to any one lesion except t h a t tenesmus is always highly suggestive of a rectal lesion or a me tas t a t i c t u m o r in the pouch of Douglas. Abdominal pain per se was more f requent ly present with tu- mors of the ascending colon. Change in bowel habi t , whether toward const ipat ion or toward more f requent evacuations, is a mos t express,.'ve s y m p t o m of cancer of the colon and rectum.
Dura t ion of syml)tOms prior to seeking medi-
cal aid is of in teres t to all those concertled with clinical studies. H u n m n beings will neglect symptoms for long periods of time, depending on the degree of discomfort they suffer, how bus)" t hey are, how insidious problem is, or wha t bad advice they have received. Al teruat- ing bowel habi t is heir to the h u m a n race, blood in the stool is common because of theub iqu i tous hemorrhoid, and everyone occasionally has " some gas or b loa t ing ." I t is quite unders tand- able t h a t m a n y pa t ien ts are not ap t to be concerned a t first abou t their symptoms. How- ever, the persistence of the symptom is of para- m o u n t impor tance to aler t both the pa t ien t and the physician. Rout ine tests for occul t blood in the stool and proctosigmoidoscopy as pa r t of the rout ine physical examinat ion in people over fort)" years of age are simple meth- ods t h a t help diagnose the unsuspected eolo- rectal tumor. Suffice i t to say in this series, seventy-five pa t ien ts had symptoms for four weeks or less dura t ion , 147 for one to six
Vo2. 1oo, May 1q65 5 6 7
Botsford, Aliapoulios, and Curtis
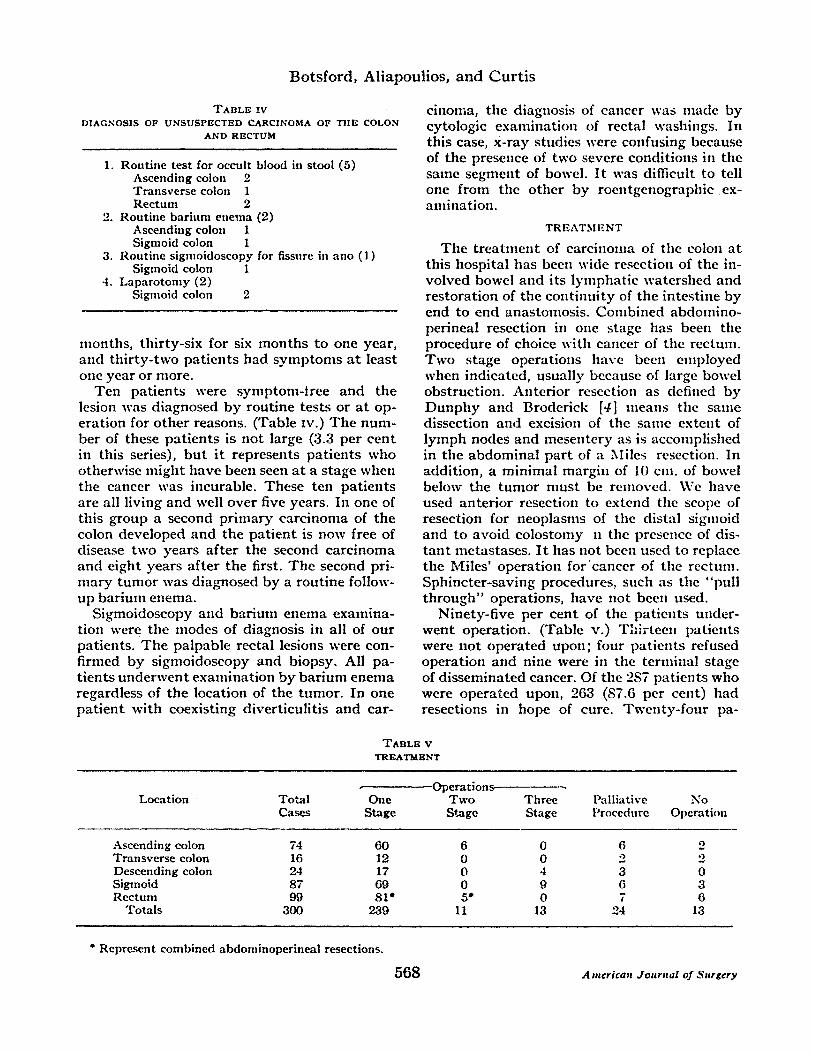
TABLE Iv DIAGNOSIS OF UNSUSPECTED CARCINOMA OF TIlE COLON
AND RECTUM
1. Rou t ine tes t for occult blood in stool (5) Ascending colon 2 Transverse colon 1 Rec tum 2
2. Routine barium enema (2) Ascending colon 1 Sigmoid colon 1
3. Routine sigmoidoscopy for fissure in ano (1) Sigmoid colon 1
4. Laparotomy (2) Sigmoid colon 2
months, thirty-six for six months to one year, and th i r ty- two pat ients had symptoms a t least one year or more.
Ten pat ients were symptom-tree and the lesion was diagnosed by routine tests or at op- eration for o ther reasons. (Table Iv.) The num- ber of these pat ients is not large (3.3 per cent in this series), bu t it represents pat ients who otherwise might have been seen a t a stage when the cancer was incurable. These ten pat ients are all living and well over five years. In one of this group a second pr imary carcinoma of the colon developed and the pat ient is now free of disease two years af ter the second carcinoma and eight years af ter the first. The second pri- nmry tumor was diagnosed by a routine follow- up bar ium enema.
Sigmoidoscopy and barium enema examina- tion were the modes of diagnosis in all of our patients. The palpable rectal lesions were con- firmed by sigmoidoscopy and biopsy. All pa- t ients underwent examination by bar ium enema regardless of the location of the tumor. In one pat ient with coexisting diverticulitis and car-
cinoma, the diagnosis of cancer was made by cytologic examination of rectal washings. In this case, x-ray studies were confusing because of the presence of two severe conditions in the same segment of bowel. I t was difficult to tell one from the other by roentgenographic ex- aufination.
TREATMENT
The t r ea tmen t of carcinoma of the colou at this hospital has been wide resection of tile in- volved bowel and its lymphat ic watershed and restoration of the cont inui ty of the intestine by end to end anastomosis. Combined abdomino- perineal resection in one stage has been the procedure of choice with cancer of the rectum. Two stage operations have been employed when indicated, usually because of large bowel obstruction. Anterior resection as defined by D u n p h y and Broderick [4] means the same dissection and excision of the same extent of lymph nodes and mesentery as is accomplished in the abdominal par t of a Miles resection. In addition, a minimal margin of 10 cm. of bowel below the tumor must be removed. We have used anterior resection to extend the scope of resection for neoplasms of the distal sigmoid and to avoid colostomy n the presence of dis- t an t metastases. I t has not been used to replace the Miles' operat ion f o r c a n c e r of the rectum. Sphincter-saving procedures, such as the "pull th rough" operations, have not been used.
Ninety-five per cent of the pat ients under- went operation. (Table v.) Thir teen patients were not operated upon; four pat ients refused operation and nine were in the ternfinal stage of disseminated cancer. Of the 2S7 pat ients who were operated upon, 263 (87.6 per cent) had resections in hope of cure. Twenty- four pa-
TABLE V TREATMENT
Location To ta l One Cases Stage
Operations Two Stage
Three Stage
Pall ia t ive Procedure
No Operat ion
Ascending colon 74 60 6 0 6 2 Transverse colon 16 12 0 0 2 2 Descending colon 24 17 0 4 3 0 Sigmoid 87 69 0 9 6 3 Rec tum 99 81" 5" 0 7 6
Tota l s 800 239 11 13 24 13
* Represent combined abdominoperineal resections.
568 A merica~l Journal of Surgery
C o l o r e c t a l C a n c e r
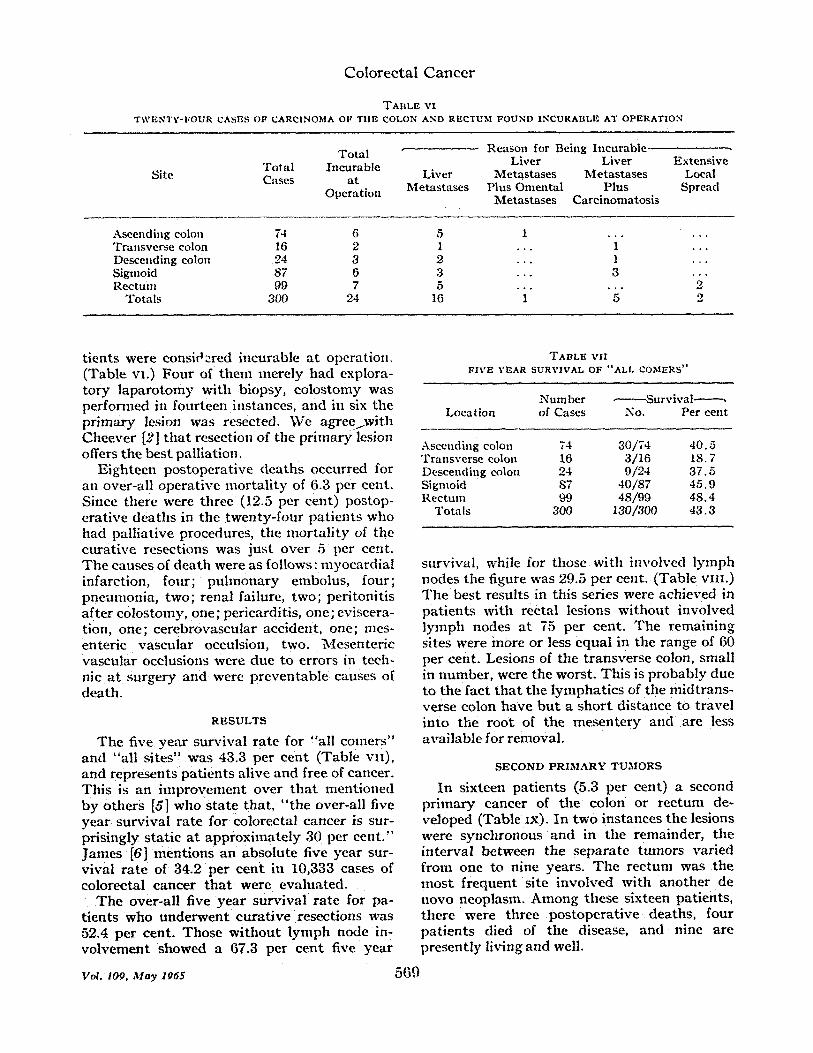
TABLE vI T~VENTV-FOUR CASES OF CAR(21NObIA OF TIIF. COLON AND RECTUM FOUND INCURAELIg. AT OPERATION
T o t a l ~ R e a s o n for B e i n g h i c u r a b l e ~ - . T o t a l h i c u r a b l e L i v e r L i v e r E x t e n s i v e
S i te Cases a t L i v e r M e t a s t a s e s l~{e tas t a ses Loca l O p e r a t i o n M e t a s t a s e s P l u s O m e n t a t P l u s S p r e a d
M e t a s t a s e s C a r c i n o m a t o s i s
A s c e n d i n g co lon 74 6 5 1 . . . . . . T r a n s v e r s e co lon 16 2 1 . . . 1 . . . D e s c e n d i n g co lon 24 3 2 . . . 1 . . .
Sigmoid 87 6 3 . . . 3 • • R e c t u m 99 7 5 2"
T o t a l s 35)0 24 16 " 1" "5" 2
t ients were considered incurable a t operat ion. (Table vI.) F o u r of them mere ly had explora- to ry l a p a r o t o m y wi th b iopsy , co los tomy was per formed in four teen instances, and in six the p r ima ry lesion was resected. W e agree~wi th C h e e r e r [2] t h a t resection of the p r imary lesion offers the bes t paUiation.
E ighteen pos tope ra t ive d e a t h s occurred for an over-al l opera t ive mor t a l i t y of 6.3 per cent . Since there were th ree (12.5 per cent ) postop- e ra t ive dea ths in the twen ty - fou r pa t i en t s who had pal l ia t ive procedures, the m o r t a l i t y of the cu ra t ive resect ions was jus t ove r 5 per cent. T h e causes of dea th were as fol lows: myoca rd ia l infarction, four; p u h n o n a r y embolus , four; pneumonia , two; renal failure, two; per i toni t i s a f te r co los tomy, one; pericardit is , one ; eviscera- tion, one; ce rebrovascu la r accident , one; rues- enteric vascu la r occulsion, two. Mesen te r i c vascula r occlusions were due to errors in tech- nic a t su rgery and were p r even t ab l e causes of dea th .
R E S U L T S
The five yea r surv iva l ra te for "al l comer s " and "all s i tes" was 43.:3 per cen t (Table vi i) , and represents pa t i en t s al ive and free of cancer. This is an i m p r o v e m e n t over t h a t ment ioned b y o thers [5] who s ta te that , " t h e over-all five y e a r su rv iva l ra te for colorectal cancer is sur- pris ingly s ta t ic a t a p p r o x i m a t e l y 30 per cen t . " J a m e s [6] men t ions an abso lu te five year sur- vival r a t e of 34.2 per c en t in 10,333 cases of colorectal cancer t h a t were eva lua ted .
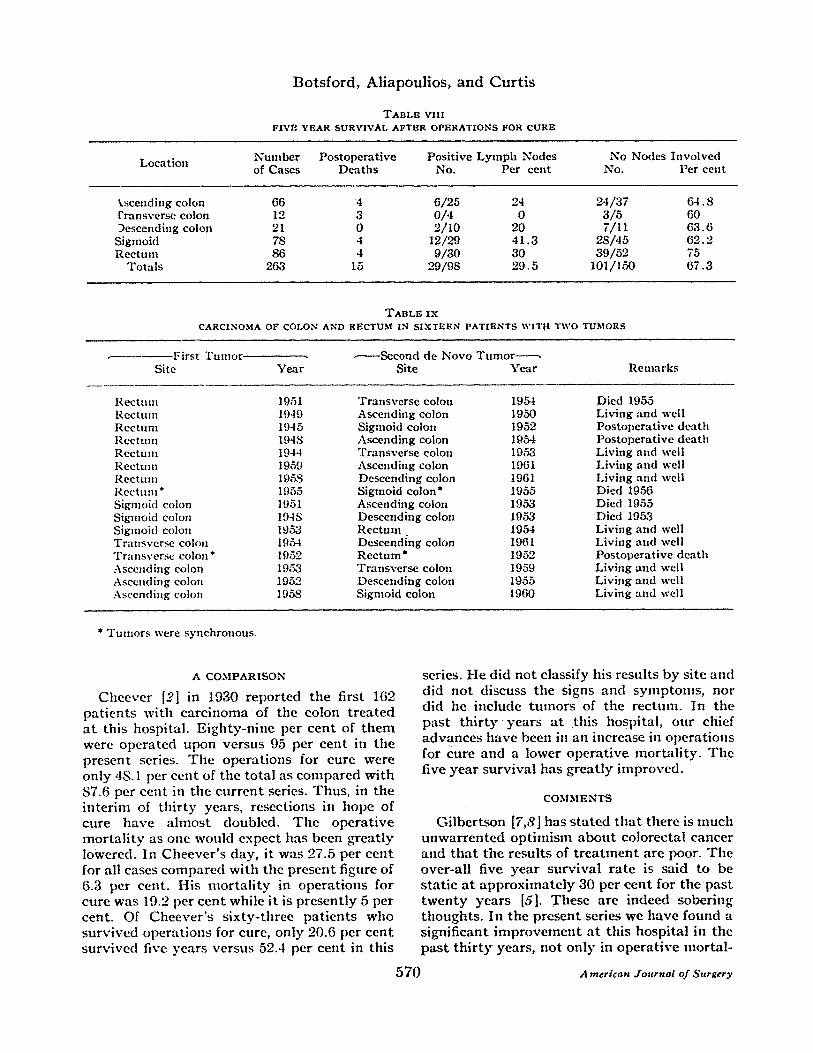
T h e over-al l five y e a r su rv iva l r a t e for pa- t ients who u n d e r w e n t cu ra t i ve resect ions was 52.4 per cent . Those w i t h o u t lymph node in- vo lvemen t showed a 67.3 per cen t five yea r
TABLE VII FIVE YI?,AR SURVIVAL OF "ALL COMERS"
N u m b e r ¢ - S u r v i v a l - - - - - - . L o c a t i o n of C a s e s No. P e r c e n t
A s c e n d i n g co lon 74 3 0 / 7 4 4 0 . 5 T r a n s v e r s e co lon 16 3 / 1 6 1 8 . 7 D e s c e n d i n g co lon 24 9 / 2 4 3 7 . 5 S i g m o i d 87 4 0 / 8 7 4 5 . 9 R e c t u m 99 4 8 / 9 9 4 8 . 4
T o t a l s 300 1 3 0 / 3 0 0 4 3 . 3
survival , while for those wi th involved l y m p h nodes the figure was 29.5 per cent. (Table vi i i . ) T h e bes t results in this series were achieved in pa t i en t s wi th rectal lesions w i t h o u t iuvolved l y m p h nodes a t 75 per cent . The remaining sites were more or less equa l in the range of 60 per cent . Lesions of the t r ansverse colon, small in number , were the worst . Th is is p robab ly due to the fac t t h a t the l y m p h a t i c s of the mid t rans- verse colon h a v e b u t a sho r t d is tance to t ravel into the roo t of the m e s e n t e r y and are less ava i lab le for removal .
SECOND P R I M A R Y TUMORS
In sixteen pa t ien ts (5.3 per cent) a second p r imary cancer of the co lon or r e c t u m de- veloped (Table Ix). i n t w o ins tances the lesions were synchronous and in the remainder , t he in te rva l be tween the s epa ra t e tumors var ied f rom one to nine years. T h e r e c t u m was the m o s t f r equen t site involved wi th ano ther de novo neoplasm. A m o n g these sixteen pat ients , there were three pos tope ra t i ve deaths , four pa t i en t s died of the disease, and nine are p re sen t ly living and well.
rot . wq . M a y 106S 569
Bots ford , A l iapou l io s , a nd Curt i s
T A B L E VIII FIVE YEAR SURVIVAL AFTER OPERATIONS FOR CURE
Location Number Postoperative Positive Lymph Nodes No Nodes Involved of Cases Deaths No. Per cent No. Per cent
kscending colon 66 4 6/25 24 24/37 64.8 t'ransverse colon 12 3 0/4 0 3/5 60 Descending colon 21 0 2/10 20 7/11 63.6
Sigmoid 78 4 12/29 41.3 28/45 62.2 Rectum 86 4 9/30 30 39/52 75
Totals 263 15 .o9/98 29.5 101/150 67.3
T A B L E I X CARCINOMA OF COLON AND RECTUM 1N S I X T E E N P A T I E N T S WITtt TWO TUMORS
........... First T u m o r Site
,. ,------Second de Novo Tumor ...... Year Site Year Remarks
Rectum Rectum Rectum Rectum Rectum Rectum Rectum Reetnm* Sigmokt colon Sigmoid colon Sigmoid colou Transverse colon Transverse colotl * Ascending colot~ Ascending colotl Ascending cololl
1951 Transverse colon 1954 Died 1955 1949 Ascending colon 1950 Living and well 1945 Sigmoid colon 1952 Postoperative death 194S Ascending colon 1954 Postoperative death 1 9 4 4 :rransverse colon 1953 Living and well 1959 Ascending colon 1961 Living and well 1 9 ~ S Descending colon 1961 Living and well 1955 Sigtnoid colon* 1955 Died 1956 1 9 5 1 Ascending colon 1953 Died 1955 194S Descending colon 1953 Died 1953 1953 Rectum 1954 Living and well 1 9 5 4 Descending colon 1961 Living and well 1952 Rectum* 1952 Postoperative death 1 9 F ~ Transverse colon 1959 Living and well 1952 Descending colon 1955 Living and well 195S Sigmoid colon 1960 Living and well
* Tumors were synchronous,
A C O M P A R I S O N
Cheerer [2] in 1930 reported the first 162 patients with carcinoma of the colon t reated a t this hospital. Eighty-nine per cent of them were operated upon versus 95 per cent in the present series. The operations for cure were only 4S. 1 per cent of the total as compared with $7.6 per cent in the current series. Thus, in the interim of thir ty years, resections in hope of cure have almost doubled. The operat ive mortal i ty as one would expect has been greatly lowered. In Cheever 's day, it was 27.5 per cent for all cases compared with the present figure of 6.3 per cent. His mortal i ty in operations for cure was 19.2 per cent while it is presently 5 per cent. Of Cheerer ' s sixty-three patients who survived operations for cure, only 20.6 per cent survived five years versus 52.4 per cent in this
series. He did not classify his results by site and did not discuss the signs and symptoms, nor did he include tumors of the rectum. In the past thir ty y e a r s a t this hospital, our chief advances have been in an increase in operations for cure and a lower operat ive mortali ty. The five year survival has greatly improved.
COM,",I E N T S
Gilbertson [7,8] has s ta ted that there is nmeh unwarrented optinfism about colorectal cancer and that the results of treatment are poor. The over-all five year survival rate is said to be static at approximately 30 per cent for the past twenty years [5]. These are indeed sobering thoughts. In the present series we have fotmd a significant improvement at this hospital in the past thirty years, not only in operative mortal-
5 7 0 A merlcan Journal of Surgery
Coloree ta l C a n c e r
i ty and operations for cure bu t also in five year survival. I t is true that we have no interim comparison and that the five year survival is far from ideal. ~oreover , we are anything bu t complacent about the results of t rea tment of colorectal cancer and for tha t mat te r cancer of any site. However, our results are closely com- parable to those reported by Swinton [9] and by Welch and Burke [10]. Welch and Burke in a recent report have indicated tha t the problem is not entirely static and reported a definite improvement in five year survival over the past ten years.
At present the answer to the problem is to diagnose the disease a t an early stage and adequately remove the lesion by an established surgical procedure. To obtain this goal the symptomat ic pat ient must prompt ly report to a physician who will perform the proper examina- tion for the vaguest symptom. In addition, the physician should routinely perform a-d?~ital rectal examination and tes t the stool for occult blood in all patients, and perform proctosig- moidoscopy on patients over for ty years of age. All patients with either symptoms, gross or occult melena, should have a barium enema. In other words the patietitg~and physician must be alert, first to the signs and symptoms and second to the procedures necessary, bu t too often neglected. I t is significant t ha t the ten pa- tients iu this series who were asymptomat ic are all living and well.
Finally, the possibility of the development of a second de novo lesion of the colon o r rectum must be kept in mind. This happened to sixteen pat ients in this series, and the new tumor was diagnosed from one to nine years 'af ter the first. Thus, these patients must not only be followed up closely for the possibility of a recurrence bu t for the occurrence of a new tmnor.
SUMMARY
Cancer of the colon and rectum is the most common visceral cancer. Three hundred in- stances are reported; 95 per cent underwent opera t ion . Eighty-seven p e r c e n t had o p e r a - tions in hope of cure. The opera t ive mortal i ty was 5 pe r cent. The five year survival fo r ',all comers" was 43.8 per cent and for tli0se with operations for cure was 52,4 p e r cent. Signifi- cant improvements have been achieved ill the management of colorectal cancer, bu t the five year survival has not as ye t reached an optimal level. An increased alertness on the par t of the patient and the physician as to the diagnosis o f coloreetal cancer is imperative.
REFERENCES 1. DUNPHY, J . E . Cancer of the Colon and Rectum.
Fourth National Cancer Conference Proceedings, p. 453. Philadelphia,:1961, J. B. Lippincott Co .
2. CI[EEVER, D. The results of t rea tment of carcinoma of the colon a t the Peter Bent Brigham Hospital. New England.[. 3fed , 203: 462, 1930.
3. DONALDSON, G. A. The management of perforutive carcinoma of the colon. :Nedw England dr. 3Ied. 258: 201, 1958.
4. DUNPHY, J . E . and BEODERZCK, E . G . A critique of anterior resection in the t reatment of cancer of the rectum and pelvic colon:Surgery, 30::106; 1 9 5 ! /
5. FLETCHER, W. S., KRIPPAEtINE~ W, W., and DUCHY. J . E.~ Current considerations in surgery of cancer of the Colo~.and rectum, S=Clin. North America, 42: 1219, ~62.
6. JAMES, A. G. Cancer Prognosis Manual. NewYork, 1961. American Cancer Society: Inc.
7. GIL~ERTSON. V. A. Adenocarcinoma of the large bowel. J.A~3I.A, ,174: 1789, 1960,
8. GILBERTSON, V: A. A plea fo r imProvement of t h e results of bowel cancer therapy. Cancer, i 1: 82. 1961.
9. SWINTON, N. W.~ MOSZKOWSKI, E,; and SNOW, J. O. Cancer of colon and rectum: statistical study of 608patients. S. Clin. North Anierica,39: 745, 1959.
10. WELCH, C. E, and BURKE, J: F. Carcinoma of the colon and rectum. Ne'w England J.12~ted, 266: 82, 1062.
vo:. wg, ,~1a~ ~6s 571