respiratory system 3-20-14 for bb
TRANSCRIPT

• Reminders:
• Tomorrow 3/21 is the last day to withdraw from this class
• Exam 2 will be given on 4/3/14 (the Thursday after your Spring
Break) and will be composed of questions from both Dr.
Schmidt and Dr. McGinley
• The final exam is scheduled for Monday, May 5 from 10:30 am
- 12:30 pm. Location TBA

Cyclopic infant born in 2006. Survived
1 day after birth.
Most cases of cyclopia are fatal due
to breathing problems (nonfunctional
nose/mouth) or brain defects.
The drug cyclopamine is
produced by California corn lily.
Pregnant animals grazing on the
plant have cyclopic offspring like
this lamb.
Cyclopamine is currently in clinical trials as
an anti-cancer drug (Saredigib / IPI-926).

Development of the
Respiratory System

Learning Objectives
Name the parts of the adult respiratory system and their function. Which parts
conduct air and which parts do gas exchange?
Identify the germ layer origins of the respiratory system.
Describe how the developing lungs separate from the foregut.
Explain how blood is oxygenated within the alveoli of the lungs.
Describe what tissues are formed during each of the 5 stages of lung
development.
Understand the role of surfactant in lung function. What are the consequences
of having insufficient surfactant at birth?
Describe the cause, symptoms and treatments for the following congenital lung
disorders: tracheoesophageal fistula, infant respiratory distress syndrome,
alveolar capillary dysplasia, and pulmonary hypoplasia.


Trachea (windpipe) – connects the pharynx/larynx to the lungs • Lining is endoderm and the cartilage is mesoderm

Primary bronchi/lung buds
Secondary bronchi
Tertiary bronchi
Primary bronchioles
Terminal bronchioles
Respiratory bronchioles
Alveolar ducts
Alveolar sacs
Alveoli
Respiratory
airways
Conductive
airways
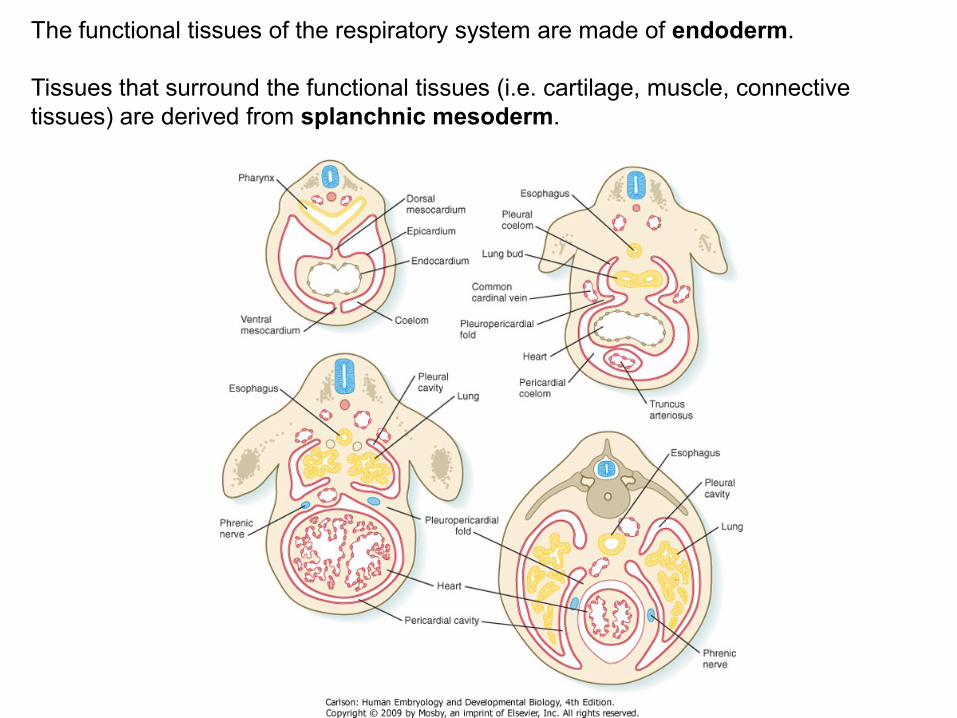
The functional tissues of the respiratory system are made of endoderm.
Tissues that surround the functional tissues (i.e. cartilage, muscle, connective
tissues) are derived from splanchnic mesoderm.

Laryngotracheal groove (respiratory diverticulum) – precursor of the lungs and
trachea.
• It is a ventral evagination from the esophageal endoderm of the foregut.
Fusion of the tracheoesophageal septum (ridge) causes separation of the trachea
and esophagus.
The diverticulum elongates and branches forming lung buds.
• The straight portion will form the trachea.
• The lung buds will give rise to the mature lung.

At around 4 weeks, lung (bronchial) buds form at the caudal end of the respiratory
diverticulum
The lung buds become the primary bronchi
• Right primary bronchi = right lung; left primary bronchi = left lung
Secondary (lobar) bronchi grow out from the primary bronchi
• Three on the right and two on the left
• Will eventually give rise to the lobes of the lung
Tertiary bronchi grow from the secondary bronchi

Primary bronchioles grow out from
the tertiary bronchi
Terminal bronchioles grow out from
the primary bronchioles
Respiratory bronchioles grow from
the terminal bronchioles
Alveolar ducts branch from the
respiratory bronchioles and give rise
alveolar sacs
Alveolar sacs eventually give rise to
alveoli
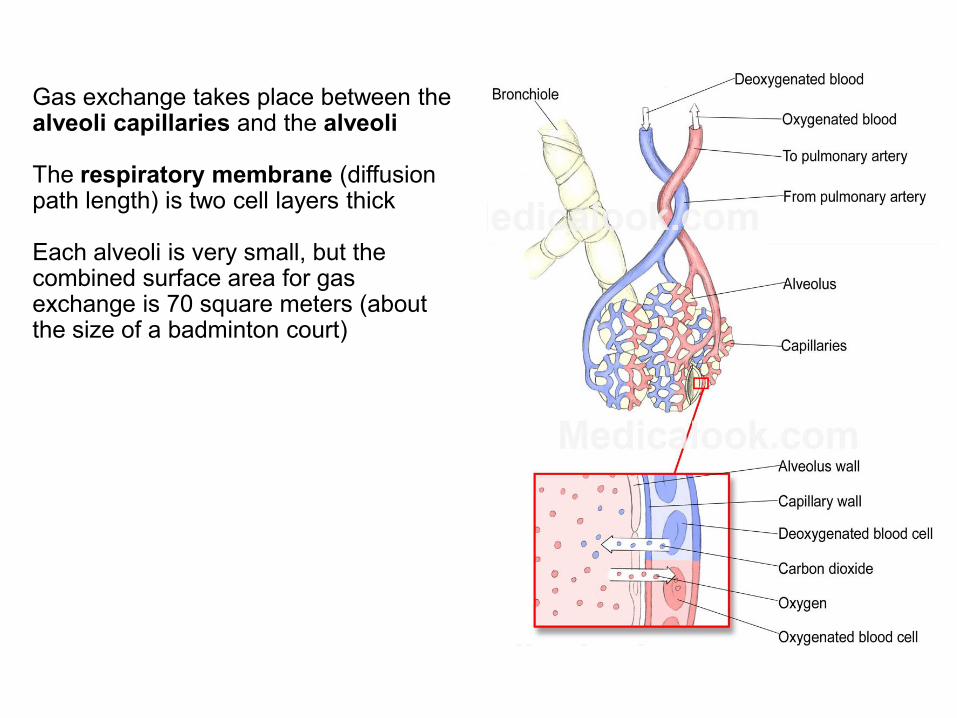
Gas exchange takes place between the alveoli capillaries and the alveoli The respiratory membrane (diffusion path length) is two cell layers thick Each alveoli is very small, but the combined surface area for gas exchange is 70 square meters (about the size of a badminton court)

Structure of the
respiratory
system
between
weeks 4 and 7:
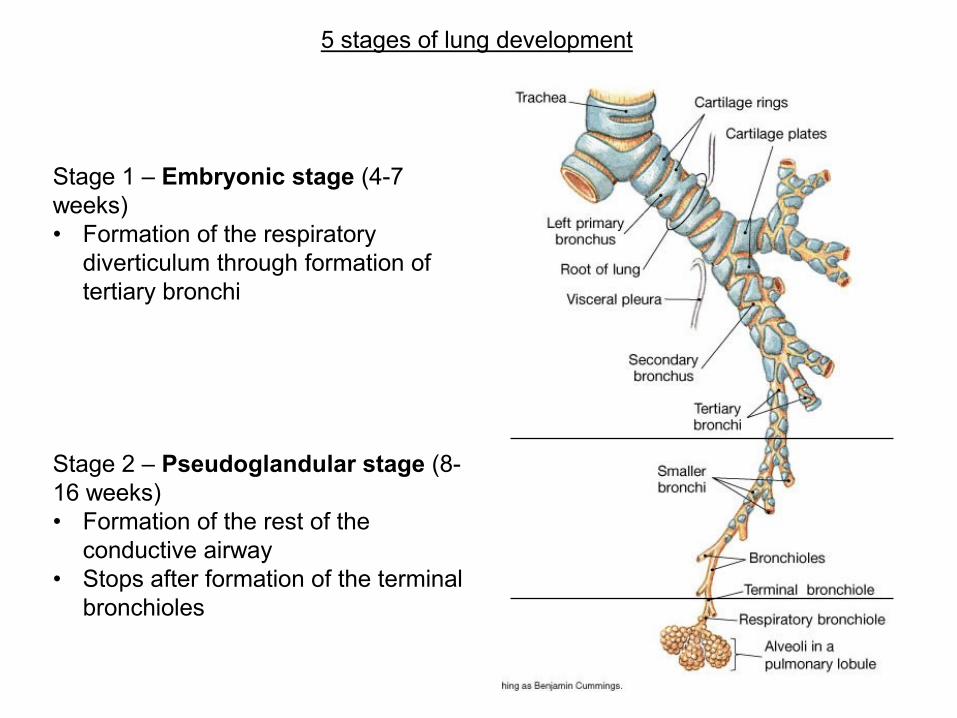
Stage 1 – Embryonic stage (4-7
weeks)
• Formation of the respiratory
diverticulum through formation of
tertiary bronchi
Stage 2 – Pseudoglandular stage (8-
16 weeks)
• Formation of the rest of the
conductive airway
• Stops after formation of the terminal
bronchioles
5 stages of lung development

Stage 3 – Canalicular stage (17-26 weeks)
• Formation of respiratory bronchioles and alveolar ducts from the terminal bronchioles
• Blood vessels begin to grow into the lungs, and capillaries become associated with
the respiratory bronchioles
Stage 4 – Terminal/saccular/alveolar stage (26 weeks – birth)
• Alveoli (terminal air sacs) bud from the alveolar ducts
• Type I alveolar cells – gas exchange
• Type II alveolar cells – production of pulmonary surfactant

Stage 5 – Postnatal stage (birth – approximately 8 years old)
• Mature lungs contain about 300 million alveoli, about 90% of which are formed
after birth
• This is due to the formation of secondary septa that divide the alveoli
1. Alveolar duct
2. Primary septum
3. Alveolar sac
4. Type I pneumocyte
5. Type II pneumocyte
6. Capillaries
1. Alveolar duct
2. Secondary septum
3. Alveolar sac
4. Type I pneumocyte
5. Type II pneumocyte
6. Capillaries
http://www.embryology.ch/anglais/rrespiratory/phasen06.html

http://www.embryology.ch/anglais/rrespiratory/phasen01.html

Lungs are not needed for respiration in utero, but are necessary immediately upon
birth
Before birth, the fetus’ lungs are filled with liquid
• Liquid is usually composed of surfactant and amniotic fluid
Upon birth, the fluid needs to be quickly removed and replaced with oxygen
Fluid is removed by the lungs in three ways:
1. Pressure on the fetus’ chest as it moves through the birth canal
2. Entrance into the pulmonary circulation via the alveolar capillaries
3. Entrance into the lymphatic system via the bronchioles
An infant takes a first breath as a reflex, and this breath causes all of the respiratory
passageways to open
Hydrostatic test – used to determine if a fetus was alive at the time of birth
The theory:
• if the fetus was alive at the time of birth, it would have taken a breath, the lungs
would fill with air, and they would therefore float when placed in water
• If the fetus was stillborn at the time of birth, it would not take a breath, the lungs
would not inflate and would sink when placed into water

Malformations of the Lungs
Tracheoesophageal fistula (TEF) – an
• Abnormal connection between the trachea and the esophagus, usually due to a
failure of the tracheoesophageal ridges to fuse.
• Co-occurs with esophageal atresia (EA)
• Symptoms = problems feeding and abdominal distention
• Treatment = surgical repair

Malformations of the Lungs, continued
Infant Respiratory Distress Syndrome
• Formerly called hyaline membrane disease because of lung histology
• Symptoms = difficulty breathing, cyanosis
• Associated with premature infants, gestational diabetes. Due to lack of surfactant.
• 1% of all births. Leading cause of death for premature infants.
• Treatments = artificial surfactant, oxygen via breathing machines. Corticosteroids
given before birth can speed lung maturation.
Alveolar capillary dysplasia –
• Capillaries fail to properly form
around the alveoli
• Shortly after birth, infants experience
respiratory distress
• Usually results in death of the
newborn
• In July 2012, the first newborn with
ACD was kept alive via use of an
artificial lung followed by a lung
transplant

Malformations of the Lungs, continued
Pulmonary hypoplasia
• Underdevelopment of the lungs
• Found frequently in premature infants.
• Can be caused by diaphragm hernias, cysts/tumors , dextrocardia, hydrops fetalis.
• Symptoms = Reduced lung volume leads to respiratory distress, often death
• Treatment = oxygenation, surgical repair of causal disorder, corticosteroids.