respiratory physiology physiology • external respiration = gas exchange • four steps of external...
TRANSCRIPT
7/5/02 Mr. Davenport 1
Respiratory Physiology
Copyright 1999, Stephen G. Davenport, No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form without prior written permission.
7/5/02 Mr. Davenport 2
Respiratory Physiology• External respiration = gas exchange• Four steps of external respiration
– pulmonary ventilation– gas diffusion across respiratory membrane– storage and transport of gases– exchange of dissolved gases
•Internal respiration = cellular respirationHypoxia - low tissue oxygen levelsAnoxia - lack of oxygen delivery
7/5/02 Mr. Davenport 3
Atmospheric pressure
• Is the pressure of air (gases) surrounding the body (760 mm Hg)
• Is a function of gravitational pull on gases that exist in a mixture. The primary atmospheric gases are nitrogen, oxygen, and carbon dioxide.
7/5/02 Mr. Davenport 4
Intrapulmonary pressure
• is the pressure within the alveoli, • changes during each inspiratory and
expiratory event,• eventually equalizes with atmospheric
pressure when inspiration or expiration terminates
7/5/02 Mr. Davenport 5
Intrapleural Pressure• Pressure within the pleural cavity • Always less than intrapulmonary pressure• Two factors which act to pull the lungs
(visceral pleura) away from thorax wall (parietal pleura)
• Tendency of lungs to recoil• Surface tension of alveolar fluid
– Factor which opposes inward pull is elasticity of chest wall
7/5/02 Mr. Davenport 6
Inspiration and Expiration
• Boyle’s Law states an inverse relationship between volume and pressure
• Inspiration and exhalation involve changes in the volume of the chest cavity and the associated lungs– Volume is changed by the action of the
diaphragm and intercostal (internal and external) muscles
7/5/02 Mr. Davenport 7
Inspiration• Inspiration involves inspiratory muscles;
diaphragm and external intercostal muscles– diaphragm (most important of two muscle
groups) moves inferiorly and flattens – intercostal muscles lift rib cage and move the
sternum forward– Thus, volume increases and pressure decreases
(intrapulmonary pressure drops 1mm Hg). Air enters lungs until intrapulmonary pressure again equals atmospheric pressure
7/5/02 Mr. Davenport 8
Expiration• Normally passive and produced by the
relaxation of inspiratory muscles and recoil of alveoli
• Forced Expiration: produced by contraction of abdominal muscles which depress the rib cage and increase abdominal pressure (push diaphragm upward)
7/5/02 Mr. Davenport 9
FACTORS AFFECTING PULMONARY VENTILATION
• Three important factors which directly affect the passage of air during pulmonary ventilation are:
• Airway resistance• Alveolar surface tension• Lung compliance
7/5/02 Mr. Davenport 10
Airway Resistance
• Friction is a major source of resistance encountered in airways
• Gas flow is – directly proportional to difference in pressure
between atmosphere and alveoli (for example, gas flow increases as pressure increases)
– inversely proportional to resistance (for example, gas flow decreases as resistance increases)
7/5/02 Mr. Davenport 11
Airway Resistance• Diameters of initial air passages are large• As individual air passages become smaller
the total cross-sectional diameter increases because of their continued branching
• Diffusion is the driving force at the respiratory bronchioles and alveoli
• Medium sized bronchi offer the greatest resistance– Branching is not extensive– Smooth muscle serves as protective
mechanism, constriction in asthma and dilation in flight or fight response
7/5/02 Mr. Davenport 12
Alveolar Surface Tension• Surface tension of water has tendency to
collapse the alveoli (resists expansion) – Produced mostly by polar water molecules
• Surfactant (produced by septal cells) reduces surface tension
• Less energy is needed to expand the lungs and prevent alveolar collapse
• Infant respiratory distress syndrome (IRDS) - premature babies (up until last two months) can not produce enough surfactant.
7/5/02 Mr. Davenport 13
Compliance• is an indication of lung expandability• determined by lung and thorax elasticity and
surface tension of the alveoli• is decreased by anything that
– reduces natural resilience of lungs (fibrosis)– blocks smaller passageways (pneumonia, bronchitis)– reduces production of surfactant (dehydration)– decreases flexibility of thoracic cage (ossification of
costal cartilages)
7/5/02 Mr. Davenport 14
RESPIRATORY VOLUMES
• Respiratory volume - a single respiratory event• Respiratory capacity - sum of two or more
volumes• Spirometer - instrument used to measure
respiratory volumes or capacities
7/5/02 Mr. Davenport 15
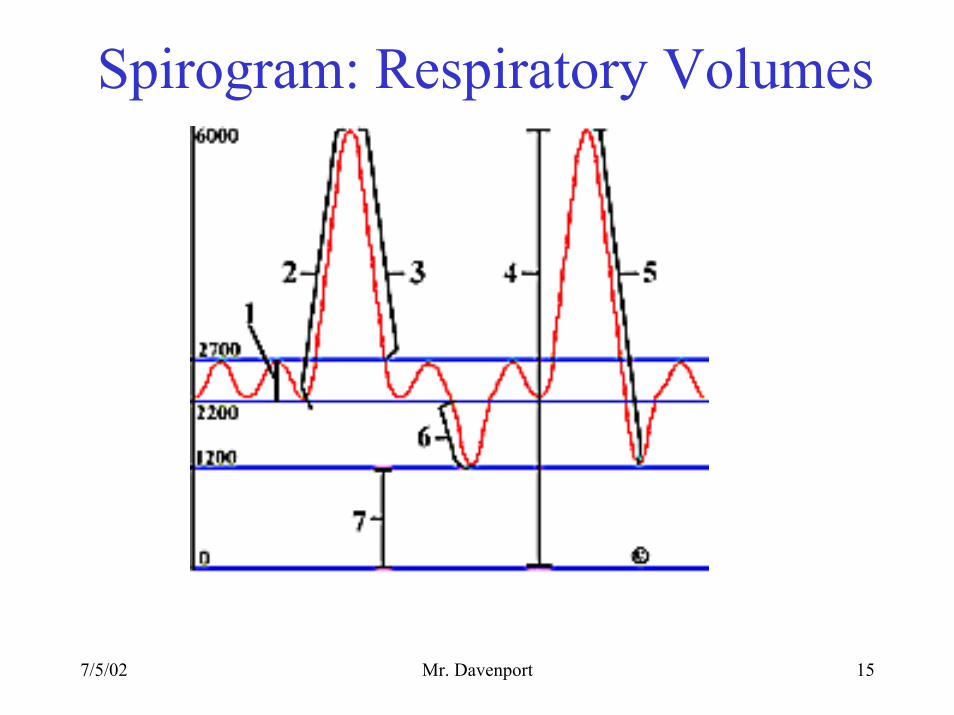
Spirogram: Respiratory Volumes
7/5/02 Mr. Davenport 16
Tidal volume (TV)
• Amount of air moved into (or out of) the lungs with each normal breath.
7/5/02 Mr. Davenport 17
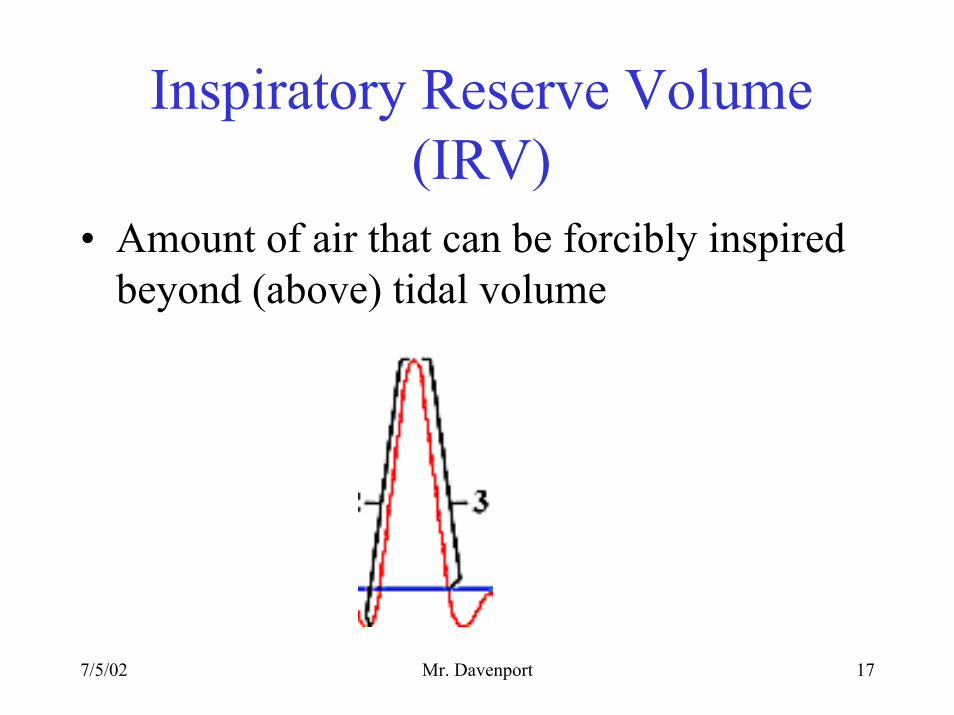
Inspiratory Reserve Volume (IRV)
• Amount of air that can be forcibly inspired beyond (above) tidal volume
7/5/02 Mr. Davenport 18
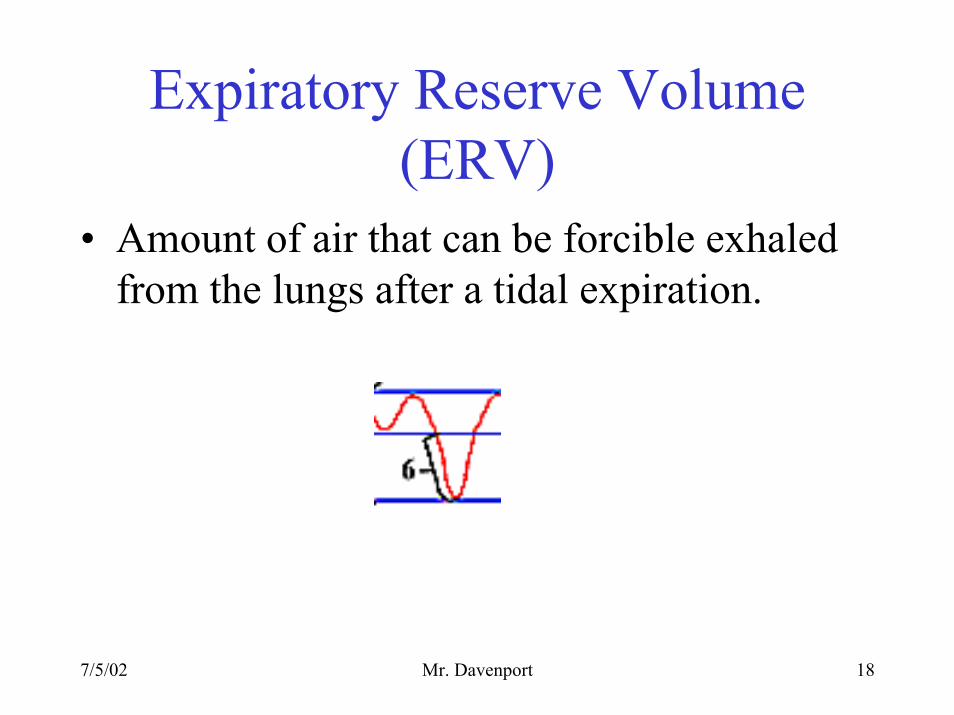
Expiratory Reserve Volume (ERV)
• Amount of air that can be forcible exhaled from the lungs after a tidal expiration.
7/5/02 Mr. Davenport 19
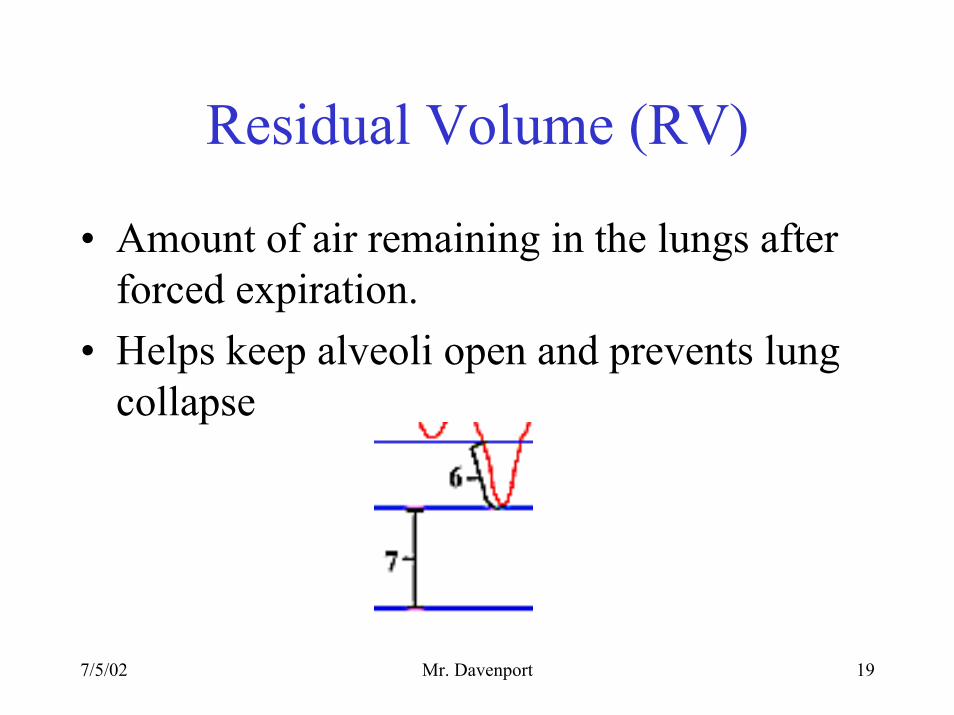
Residual Volume (RV)
• Amount of air remaining in the lungs after forced expiration.
• Helps keep alveoli open and prevents lung collapse
7/5/02 Mr. Davenport 20
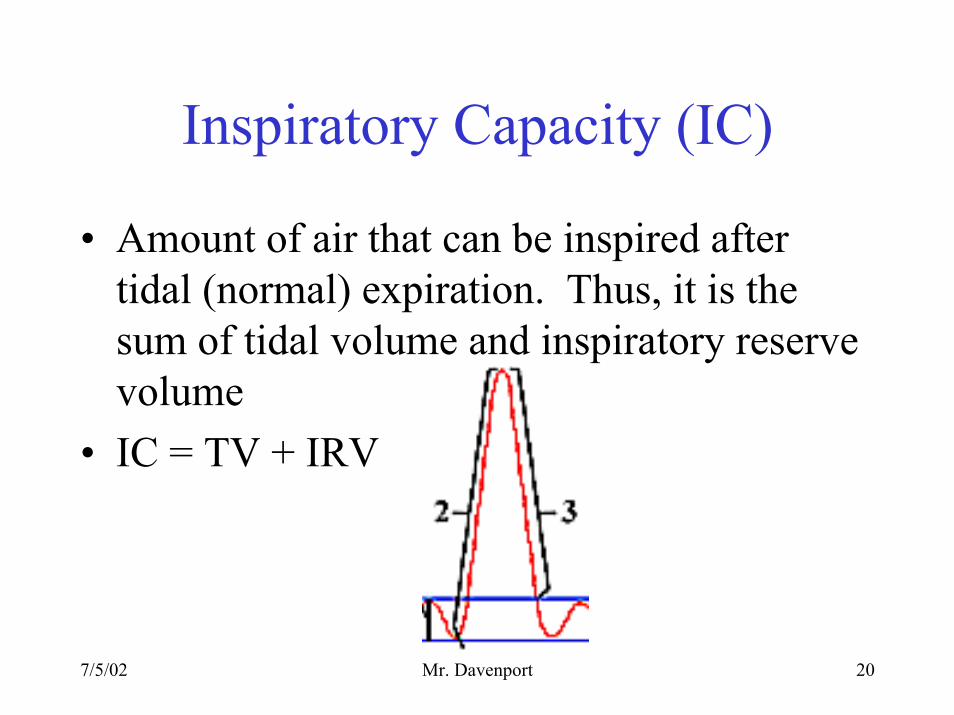
Inspiratory Capacity (IC)
• Amount of air that can be inspired after tidal (normal) expiration. Thus, it is the sum of tidal volume and inspiratory reserve volume
• IC = TV + IRV
7/5/02 Mr. Davenport 21
Vital Capacity (VC)
• Total amount of exchangeable air• The sum of tidal, inspiratory reserve volume
and expiratory reserve volume.• VC = TV + IRV + ERV• VC = IC + ERV
7/5/02 Mr. Davenport 22
Pulmonary Function Tests
• Forced vital capacity (FVC) measures amount of total exhalation. Should be at least 80% of the value in table (laboratory)
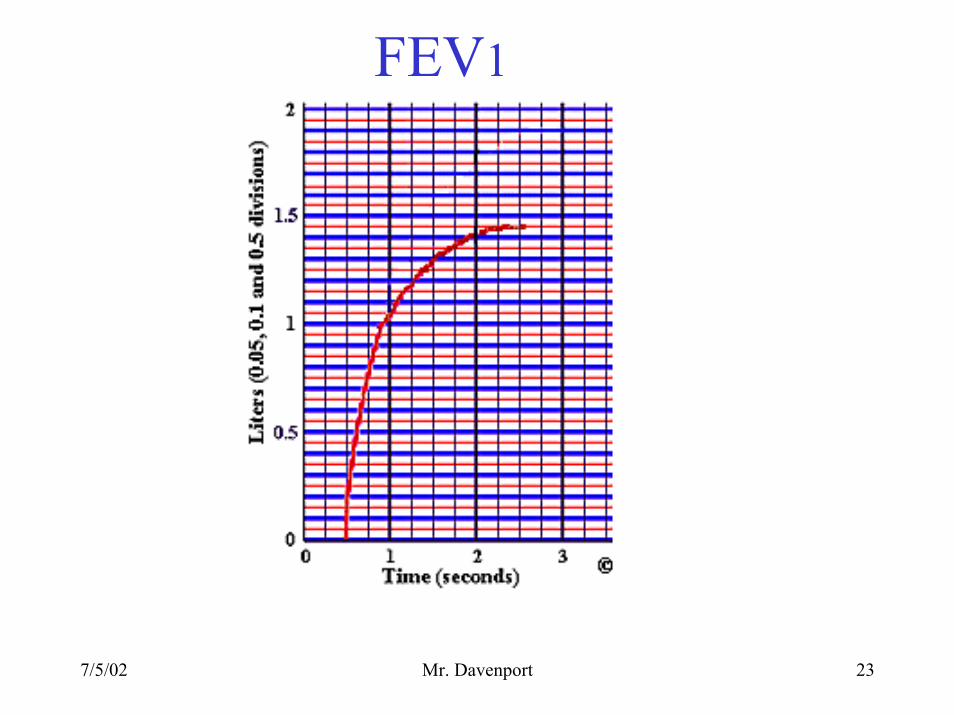
• Forced expiratory volume - timed (FEVt)measures as a percentage the amount of air forcibly expired in one second. Should be at least 75% of the volume measured.
7/5/02 Mr. Davenport 23
FEV1
7/5/02 Mr. Davenport 24
GAS EXCHANGE IN THE BODY
• Dalton’s law - the total pressure exerted by a mixture of gases is the sum of pressures exerted independently by each gas in the mixture
• Pressure exerted is called partial pressure• Pressure of gas is directly proportional to its
percentage in the total gas mixture
7/5/02 Mr. Davenport 25
Atmospheric Pressure• Nitrogen is 78.6% of atmospheric gas
– Partial pressure of nitrogen (written as PN2) is 597mm Hg (78.6% x 760mm Hg)
• Oxygen is 20.9% of atmospheric gas – Partial pressure of oxygen (PO2) is 159mm Hg
• Nitrogen and oxygen contribute 99% of total atmospheric pressure. Carbon dioxide contributes 0.04% , water vapor 0.5%, etc.
7/5/02 Mr. Davenport 26
Henry’s Law
• Henry’s Law - when a mixture of gases is in contact with a liquid, each gas will dissolve in the liquid in proportion to its partial pressure
7/5/02 Mr. Davenport 27
Solubility of the Gas• Each gas will dissolve according to its
solubility • Carbon dioxide is most soluble (in plasma)• Oxygen is 1/20th as soluble as carbon
dioxide• Nitrogen is 1/2 as soluble as oxygen• Hyperbaric oxygen chambers increase the
partial pressure of oxygen. Thus, force more oxygen into blood
7/5/02 Mr. Davenport 28
Composition of Alveolar Air
• A mixture of newly inspired gases and gases remaining in the lungs between breaths
• Alveolar air contains more carbon dioxide and water vapor and less oxygen than atmospheric air
7/5/02 Mr. Davenport 29
Diffusion at Respiratory Membrane
• Differences in partial pressures across membrane are substantial
• Distances involved are small• Gases are lipid soluble• Total surface area is large• Blood flow and airflow are coordinated
7/5/02 Mr. Davenport 30
Gas Pickup and Delivery• Oxygen and carbon dioxide have limited
solubilities in plasma• Red blood cells solve problem by binding
(oxygen) or producing soluble compounds (RBCs use carbonic anhydrase to produce carbonic acid from CO2 + H2O)
• Reactions are temporary and reversible
7/5/02 Mr. Davenport 31
Oxygen Transport
• Transported in two ways– bound to hemoglobin (98.5%)– dissolved in plasma (1.5%)
• Oxyhemoglobin = HbO2
• Deoxyhemoglobin (reduced) = HHb• HHb + O2 HbO2 + H+
7/5/02 Mr. Davenport 32
Hemoglobin Saturation• At most each Hb can carry four O2 molecules• Four factors affecting hemoglobin are
– PO2 (almost complete saturation of a partial pressure of 70 mm Hg.
– blood pH – temperature – RBC metabolism
Generally speaking an increase of H+ (decreased pH), temperature, and metabolism enhance unloading of oxygen from Hb.
7/5/02 Mr. Davenport 33
Carbon Dioxide Transport
• Three things can happen to carbon dioxide:– converted to a molecule of carbonic acid– bound to protein portion of Hb– dissolved in plasma
7/5/02 Mr. Davenport 34
Carbonic Acid Formation
• Red blood cells supply enzyme called carbonic anhydrase
• 70% of CO2 is transported as HCO3-
CO2 + H2O H2CO3 H+ + HCO3-
CO2 + H2O H + + HCO3-
7/5/02 Mr. Davenport 35
CO2 Binding to Hb
• Binding forms carbaminohemoglobin Hb-CO2
• 23% of CO2 is transported in this form
7/5/02 Mr. Davenport 36
CO2 Dissolved in Plasma
• 7% is transported in this form
7/5/02 Mr. Davenport 37
Respiratory Centers in Brain
• Voluntary control is by cortical influences which affect respiratory centers
• Respiratory centers are located in medulla and pons
• Medulla contains– dorsal respiratory group (DRG) controls
diaphragm and external intercostal muscles– ventral respiratory group (VRG) controls forced
respiration
7/5/02 Mr. Davenport 38
DRG
• DRG is pacesetting region– Called inspiratory center– Activates inspiration at 12 – 15 breaths per minute
(expiration is passive)– Innervates phrenic and inspiratory nerves– Eupnea is normal breathing
7/5/02 Mr. Davenport 39
Pons
• Pons contains apneustic and pneumotaxic centers
• Adjust output of medulla’s rhythmicity centers
• Controls rate and depth of respiration
7/5/02 Mr. Davenport 40
Respiratory reflexes
• Sensory information is received from– chemoreceptors: PO2, pH, PCO2 of blood and CSF– blood pressure (aorta and carotid sinuses)– stretch receptors respond to changes in lung volume– irritating physical and chemical stimuli-nasal, larynx,
bronchial– other sensations include pain, temperature, etc.
7/5/02 Mr. Davenport 41
Hypercapnia• An abnormally high arterial PCO2
• Homeostatic mechanism is hyperventilation until normal PCO2 is restored
• Hypercapnia may be produced by hypo-ventilation which conserves too much CO2 – Thus conserves carbonic acid (H+)– Blood ph is decreased - respiratory acidosis– Corrected by hyperventilation which results in
increased rate and depth of breath
CO2 + H2O H2CO3 H+ + HCO3-
This respiratory event (alveolar) is increased
7/5/02 Mr. Davenport 42
Hypocapnia• An abnormally low PCO2
• Homeostatic mechanism is hypoventilation or apnea until normal PCO2 is restored
• Hypocapnia may be caused by hyper-ventilation (anxiety attack) which removes too much CO2 – Thus removes carbonic acid (H+)– Blood pH is increased - respiratory alkalosis – Corrected by hypoventilation or apnea which
results in decreased rate and depth of breath
CO2 + H2O H2CO3 H+ + HCO3-
This respiratory event (alveolar) is slowed
7/5/02 Mr. Davenport 43
Chronic Obstructive Pulmonary Disease (COPD)
• History of smoking or exposure to respiratory irritant such as asbestos or silicates (pollution)
• Dyspnea (disp ne ah) – difficulty in breathing• Coughing• Frequent infections• Usually results in respiratory failure
– with respiratory acidosis (CO2 retention) – hypoxia.
7/5/02 Mr. Davenport 44
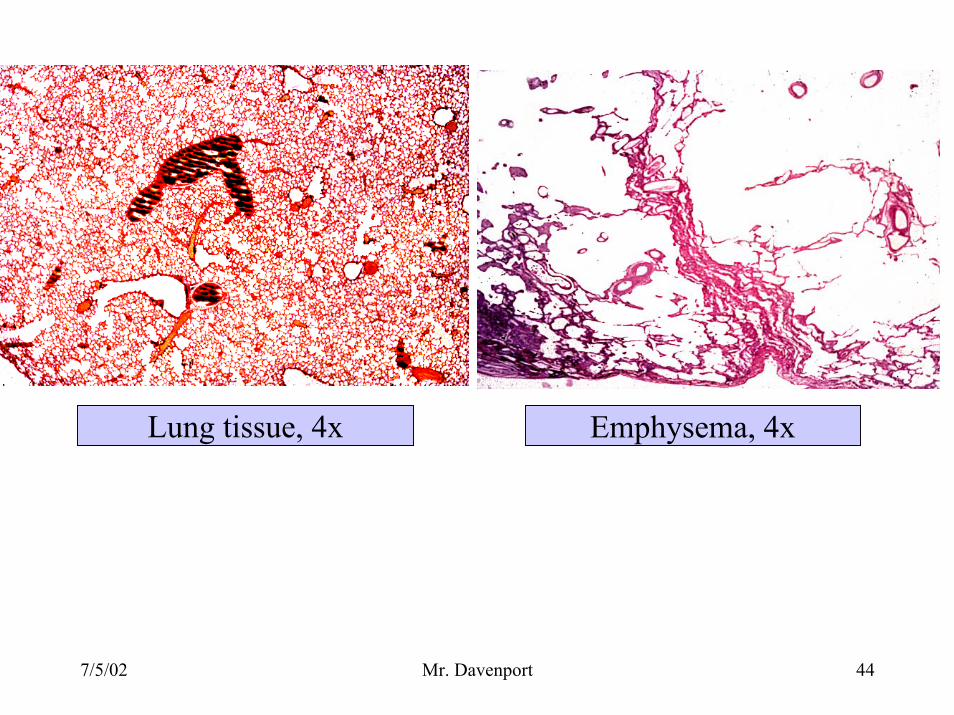
Lung tissue, 4x Emphysema, 4x