resin bonded bridges.modi/ labial orthodontics
TRANSCRIPT

1
Resin Bonded Fixed Partial Denture –case reports.
INDIAN DENTAL ACADEMY
Leader in continuing dental education www.indiandentalacademy.com
www.indiandentalacademy.com

2
Introduction
• The need for conservation of natural tooth structure has always been the desired but elusive goal in dentistry.
• In fixed partial prosthodontics this goal manifests itself with the continued interest and development of Resin bonded fixed partial dentures (RBFPD).
www.indiandentalacademy.com

3
Definition
• Resin bonded prosthesis
A prosthesis that is luted to tooth structure,primarily enamel,which has been etched to provide mechanical retention for the resin cement. -GPT-7
• Also called as Maryland bridges, Rochette bridges.
www.indiandentalacademy.com


5
Why a Re-Look ?
1. Sometimes Cost and other constraints make single teeth implants unfeasible.
2. Recent and further scope of Advances in adhesive dentistry.
3. Lesser failure rates of RBFPD’s found in recent studies.
www.indiandentalacademy.com

6
History and development
• Development of Acid etching of enamel by Buonocore.
• Bowen developed the BIS-GMA composite resins.
www.indiandentalacademy.com

7
Rochette bridge
• Developed in 1973.It was a complete innovation.Use of ring like retainers,with funnel shaped
perforations through them to enhance resin retention.
Silane coupling agent was used to produce adhesion to the metal.
www.indiandentalacademy.com

8
Maryland ridge
• Etched metal surface first developed by Livaditis and Thompson.
• Treatment of metal surface with acids and controlled electric current.
www.indiandentalacademy.com

9
Virginia bridge.
• Roughned surface of the retainer itself provides for retention
• Achieved by lost salt technique.
• Air abrasion with aluminium oxide.
www.indiandentalacademy.com

10
Advantages of Resin bonded bridges.
1) Reduced cost .
2) No anesthetic needed.
3) Supragingival margins.
4) Minimal tooth preparation.
5) Rebonding possible.
www.indiandentalacademy.com

11
Indications.
1) Adolescents with single missing teeth (traumatic or congenital).
2) Caries- free abutment teeth and good oral hygiene.
3) Maxillary incisor replacements (most favourble prognosis) and Mandibular incisor replacements.
4) Periodontal splints.
5) Single posterior tooth replacements.
www.indiandentalacademy.com

12
• Survival rates of FPD – 96% at 5 years – 74% at 15 years
• Creugers et al 1994.
• Survival rates of RBFPD– 74% at 4 years (meta study)– 93% at 11 years Barrack
www.indiandentalacademy.com
13
Tooth preparation The strength of bonding to prepared and
etched enamel is greater than that to etched but unprepared enamel.(Aker et al 1979)
Preparation should cover as large as area as esthetically possible
www.indiandentalacademy.com

14
Cervical margin should always be in enamel and Supragingival.
Preparation should ensure precise insertion and seating of the framework.
180 0 wraparound of the metal.
www.indiandentalacademy.com

15
Case-1
• History
www.indiandentalacademy.com

16
Examination
• Root exposure of central incisor and canine.
• Widened edentulous space mesiodistally.
• I mm over jet and overbite
www.indiandentalacademy.com

17
• Good oral hygiene and favorable periodontal status.
• Study models were made and articulated.
• Radiographs were taken.
www.indiandentalacademy.com

18
Treatment plan • Resin bonded fixed partial denture was
the treatment of choice1. As it kept the option of going for bone
grafting and implant a possibility.
2. Angulation of abutments and gingival recession made the possibility of 3 unit conventional FPD a difficult proposition.
www.indiandentalacademy.com

19
Tooth preparation
• Very conservative palatal preparation.
• Supragingival chamfer.
• Proximal groves.
www.indiandentalacademy.com

20
Laboratory procedure
• Wax pattern was made and casted in Ni-Cr alloy.
• Pontic was made in appropriate shade of ceramic.
• Holes were made on the wings to facilitate light curing of composite.
www.indiandentalacademy.com

21
Bonding steps.
• Sand blasting of metal framework.
• Acid etching
• Rinsing and drying.
• Contamination to be avoided at all cost.
www.indiandentalacademy.com

22
www.indiandentalacademy.com

23www.indiandentalacademy.com

24
www.indiandentalacademy.com

25www.indiandentalacademy.com

26www.indiandentalacademy.com

27www.indiandentalacademy.com

28
Case 2
• Missing mandibularRight central incisor
www.indiandentalacademy.com

29
• Bone loss and gingival recession in abutment teeth.
• Grade 1 mobility.
www.indiandentalacademy.com

30
Treatment plan.
• Resin bonded fixed partial denture was the treatment of choice.As patient wanted a fixed replacement of
the missing teeth.
Need for splinting the lower anteriors.
www.indiandentalacademy.com
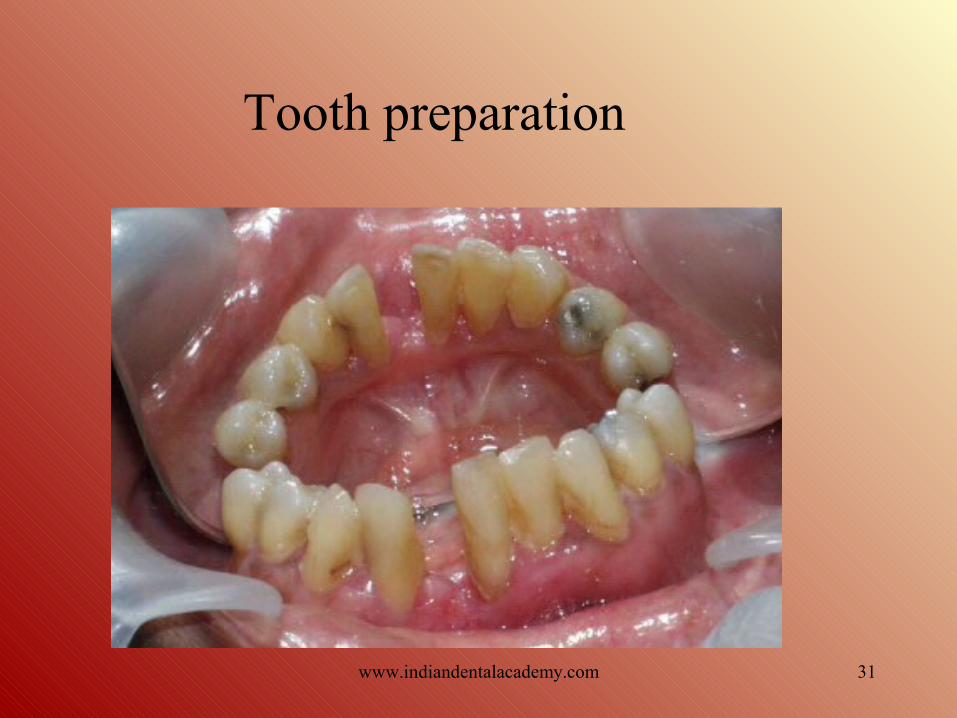
31
Tooth preparation
www.indiandentalacademy.com

32
• Conventional Maryland bridge fabricated with porcelain fused to metal pontic.
www.indiandentalacademy.com

33
• Bonded with resin cement.
www.indiandentalacademy.com

34www.indiandentalacademy.com

35www.indiandentalacademy.com

36
Case 3• 16 year old
female patient.
• Traumatic loss of maxillary left central incisors .
• Using RPD for 3 years.
www.indiandentalacademy.com

37
• Ridge resorption.
• Widened pontic space.
www.indiandentalacademy.com

38
Treatment plan
Resin bonded bridge was the treatment of choice.
• Taking into consideration age of the patient.
• Need for the conservative treatment.
www.indiandentalacademy.com

39www.indiandentalacademy.com

40
Case –4 Metal free resin bonded bridge
• Loss due to trauma.
• Highly reduced pontic space.
www.indiandentalacademy.com

41
Treatment plan.
Metal free resin bonded bridge was the treatment of choice
• As patient had edge to edge bite - less unfavourable stresses transmitted to the prosthesis.
• Superior esthetics.
www.indiandentalacademy.com

42
Treatment plan• Proximal
slicing of the abutments was done to distribute the space evenly.
• Diagnostic wax up was shown to the patient
www.indiandentalacademy.com

43www.indiandentalacademy.com

44
Temporization
www.indiandentalacademy.com

45
Laboratory procedures• Hardcore porcelain fired on refractory cast.(Hi –
ceram) • Porcealin build up done on the coping .
www.indiandentalacademy.com

46www.indiandentalacademy.com

47www.indiandentalacademy.com

48www.indiandentalacademy.com

49www.indiandentalacademy.com

50
Disadvantages
• Irreversible.
• Uncertain longevity.
• No space correction.
• No alignment correction.
• Difficult temporization.
www.indiandentalacademy.com

51
Contraindications.
• Extensive caries.
• Nickel sensitivity.
• Deep vertical overbite.
• Extensive restoration on abutment teeth.
• Parafuncitonal habits
www.indiandentalacademy.com

52
Conclusion
• Rapid development in adhesive technology holds a promising future for RBFPDs, which were originally developed as an interim restoration. Today high success rate and reducing cost is fast making RBFPD’s as a treatment alternative for permanent oral rehabilitation.
www.indiandentalacademy.com

53
• Furthermore in a developing country like India this esthetic approach, which is cost effective too, holds promising future.
www.indiandentalacademy.com
