report to: executive cabinet date: commissioning board...
TRANSCRIPT

Report to: EXECUTIVE CABINET
Date: 20 June 2018
Officer of Strategic Commissioning Board
Councillor Brenda Warrington – Executive Leader
Stephanie Butterworth – Director of Adult Services
Subject: PRESENTATION OF THE DRAFT OUTLINE BUSINESS CASE THAT PRESENTS THE CASE FOR THE TRANSACTION OF A NUMBER OF ADULT SOCIAL CARE FUNCTIONS AND STAFF INTO TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
Report Summary: The attached report presents the draft Outline Business Case (OBC) for the transaction of a proportion of Adult Social Care services and staff into the ICFT. The OBC combines a high level Strategic Outline Case (SOC) and the OBC within one document as agreed with NHS Improvement.
The Council, ICFT, and CCG considered a number of integration options at the SOC stage and concluded that the options distilled in the OBC were the most effective ones to take at this time.
Details of the teams and functions that are included in the preferred option are detailed, including the benefits, dis-benefits and risks to both the Council and the ICFT.
The report describes the economic, business, financial, commercial and management cases for the transaction of the services and functions identified in the preferred option.
Recommendations: That Strategic Commissioning Board note the content of the report and support the content of the report and the proposal contained in Option 2.
Financial Implications:(Authorised by the statutory Section 151 Officer & Chief Finance Officer)
ICF Funding Stream Section 75 Decision Required By Strategic Commissioning Board Organisation and Directorate
Tameside MBC – Adult Services
CommentsThe Outline Business Case (OBC) includes assumptions on the level of Council resources that will support the transfer of the respective services to the ICFT for the five year period to 2023/24 (Section 2 of the OBC). Section 6.4 of the OBC includes the proposed details of the risk share arrangements for the transfer. The arrangements for the Council support functions related to the transfer are yet to be confirmed.Members should consider the related risks to the Council associated with the transfer alongside the share of the proposed financial risk share arrangements stated in 6.4. The financial implications of the OBC will continue to be reviewed and updated, with further updates included within the Full Business Case should the OBC be approved by NHS Improvement.
Legal Implications:(Authorised by the Borough Solicitor)
It should be noted that he approach to risk transfer set out in the report states that: “It will be based on the best practice principle of allocating risk to the party, or parties, best placed to manage that

risk. Therefore, an optimum allocation of risk rather than a maximum risk transfer will be taken.
The risk sharing agreement (which protects the ICFT from undue financial hardship until it can start to realise benefits) will be defined and agreed during the project process. After this TMBC will not cover any funding shortfalls as the ICFT will have had the opportunity to transform the service in a manner that releases savings. Risks associated with the delivery of the solution (i.e. post contract award) will be maintained in a jointly held risk register with clear assignment to the responsible party.
Hempsons Solicitors have provided an initial review of the legal feasibility and likely risks involved in this transfer.
Going forward we need to be clear that there is an appropriate risk transfer and the Council/CCG are not left exposed with an increasing demand for resources set against a lack of control whilst retaining the liability for the service. This will need to be carefully understood before any final decision is made.
How do proposals align with Health & Wellbeing Strategy?
The proposals and strategic direction are consistent and aligned.
How do proposals align with Locality Plan?
The proposals and strategic direction are consistent and aligned.
The service is consistent with the following priority transformation programmes:
Healthy Lives (early intervention and prevention) Enabling self-care Locality-based services Urgent Integrated Care Services Planned care services
How do proposals align with the Commissioning Strategy?
The service contributes to the Commissioning Strategy by:
Empowering citizens and communities Commission for the ‘whole person’ Target commissioning resources effectively
Recommendations / views of the Health and Care Advisory Group:
This document has not been presented at HCAG.
Public and Patient Implications:
It is anticipated that this proposal will improve the service offer to people living within the borough.
Quality Implications: A Quality Impact Assessment will be completed as part of the development of the FBC and the programme of transfer to ensure quality is maintained.
A robust quality assurance framework will be developed to assure the DASS that the ICFT is delivering the Council’s statutory duties.
How do the proposals help to reduce health
A primary objective of the Care Together Programme and the development of the Integrated Care Organisation (ICO) – Tameside and Glossop Integrated Care NHS Foundation Trust –

inequalities? is to reduce health inequalities.
Bringing together the health and social care functions, working in an asset based, place based way, will improve the offer to local people, with a focus on those whose health is placing them at most risk.
What are the Equality and Diversity implications?
It is anticipated that the proposal will not have a negative effect on any of the protected characteristic group(s) within the Equality Act.
An Equality Impact assessment will be completed as part of the FBC.
What are the safeguarding implications?
Safeguarding assurance is integral and essential to the service model. All safeguarding implications will be considered as part of the FBC.
What are the Information Governance implications? Has a privacy impact assessment been conducted?
As part of the development of the FBC, a data flow mapping exercise will be undertaken to understand what information will be transferred and to where; from that it will be possible to identify the requirements for robust data sharing agreements between the parties sending or receiving the data. A work stream is already considering the implications.
A Privacy Impact Assessment has not been conducted at this stage in the process.
Risk Management: The OBC details the anticipated risks to the three options proposed in the report. Further risk analysis and mitigation will be considered as part of the development of the Full Business Case.
Access to Information : The background papers relating to this report can be inspected by contacting Stephanie Butterworth, Director of Adult Services
Telephone: 0161 342 2613
e-mail: [email protected]

1. INTRODUCTION1.1 The purpose of this report is to provide a progress update to the Strategic Commissioning
Board (SCB) regarding the progress made on the transaction of transferring a sub-set of Adult Social Care (ASC) services from Tameside Metropolitan Borough Council (TMBC) into Tameside and Glossop Integrated Care NHS Foundation Trust (ICFT). This builds on the report that was received by the Health and Wellbeing Board in January 2018.
2. CONTEXT
3. OUTLINE BUSINESS CASE
3.1 The recent activity undertaken in support of this transaction has been focused upon the production of the Outline Business Case (OBC). Before the transaction can be effected it needs to receive the support of the ICFT’s Board, of Council’s Cabinet, and of NHS Improvement (one of the ICFT’s regulators). Therefore the OBC aims to set out the locality’s rationale for the transaction and a compelling case for change.
3.2 There is appended to this report the current draft of the OBC (version 12.2). There has been a significant focus over the last two months to produce a business case that will set out for NHS Improvement the benefits to the local health and care system of delivering this transaction whilst also setting out the risks and how these can be mitigated.
3.3 SCB are advised that this version of the OBC has been shared with the Board members of the ICFT who were supportive of the report, with a preference for Option 2, subject to a more detailed Full Business Case.
Strategic Outline Case3.4 This current version of the OBC (version 12.2) opens with the Strategic Outline Case and
sets out a long list of options that have been considered with regards to the services under consideration for the transaction and also the options for any new contractual basis including the implications for staff. From this long list of eight potential options there is the rationale provided as to how the OBC arrived at a short list of three options.
3.5 These three options are:
Option One – Do nothing Option Seven - Integration of a subset of in house ASC delivered services from
TMBC into the ICFT, through TUPE arrangements Option Eight - Integration of a subset of in house ASC delivered services from TMBC
into the ICFT, as detailed in Appendix B, with the LA staff seconded into the ICFT.
2.1 During 2015 analysis conducted through the Contingency Planning Team’s report concluded that in order to achieve the most improved outcomes for our local people and to be a sustainable economy the formation of an Integrated Care Organisation was required. This new organisation would be inclusive of Social Care and the principle was accepted by the locality partners.
2.2 Consequently the locality established a programme of work to define, design, and implement the transactional process to deliver Adult Social Care into the ICFT, and within agreed timescales.

ASC services for the transaction3.6 The draft OBC is proposing that only a subset of ASC services would transfer at this time.
Although it remains the intent to progress the integration in the future to include the wider scope of ASC services it has been decided to transact a smaller sub-set of services in the first instance both to prove the concept and to limit the financial and operational risk. It is considered that this stepped approach would be more amenable to NHS Improvement. It remains the intent that in future further services would still look to be transferred.
3.7 The following table sets out the services proposed for transfer at this time:
Service Area – Adult Social Care
Service Description
TMBC Urgent Care
Service Unit Manager
Integrated Urgent Care Team (IUCT) - staff and Management team
The ASC resource in IUCT is made up of Social Workers, Assessors Assistant Practitioners, Customer Care Officers. Community Care Officers and therapists, including Physios and OTs. The function of the team is to aid a speedy discharge from hospital, prevent hospital admission, deal with a wide range of situations which present within the community, the referrals that are received by the Team come from a range of sources, such as GP's, Emergency Services, other professionals, families and carers. The function of the Team is to assess a persons’ needs and requirements, provide a 72 hour wrap around service establishing on-going support requirements going forward. At present the team also carry out rehabilitation for a period of time, which should be no longer than 6 weeks.
Integrated Community Equipment Service (ICES) - Service co-ordination staff member
Integrated Community Equipment Services provides a vast range of equipment to support people either in their own homes or the establishments they live in. ICES contract has three partners – TMBC, CCG and Derbyshire County Council. It is currently a section 75 pooled budget with TMBC as the lead Commissioner. The contract is currently being reviewed to determine future commissioning arrangements. A Co-ordinator is employed to ensure appropriate ordering and prescribing by health and social care staff, and to monitor the performance of the contract.
TMBC – Localities
Assessment / Care Co-ordination (18+) Inc Locality teams and management
The Care Act 2014 provides a statutory duty on the Council to carry out an assessment of need for anyone requesting it. Once an assessment has taken place, the application of the national eligibility criteria is made and a suitable support plan is determined. People receiving a package of care must be reviewed/reassessed annually as a minimum and those with complex care packages will be care managed/care co-ordinated throughout their time with the service.
Assessment and Care Management staff undertake assessments and annual re-assessments. They hold a caseload, and will support individuals on an on-going basis, working proactively with individuals to enable them to live well in their own homes. Where an individual experiences a crisis or experiences a change in need the Social Worker/Assessor will work with the individual, carrying out a re-assessment where appropriate, and amending/changing the support
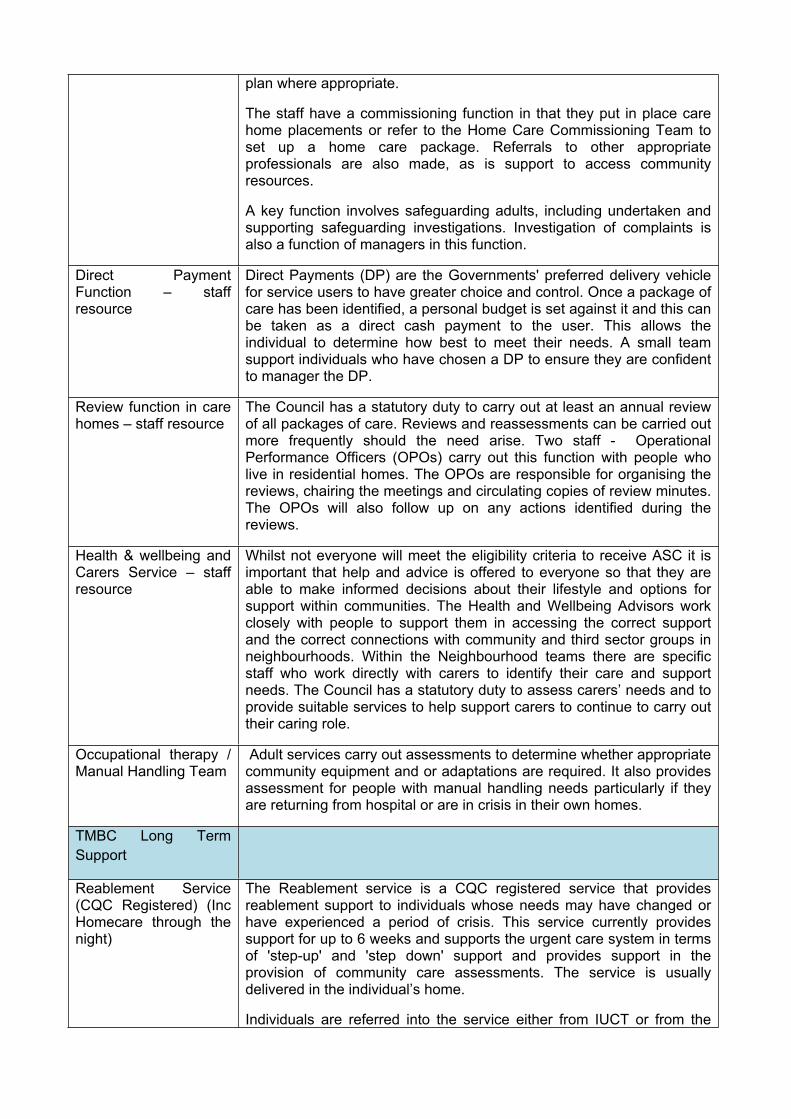
plan where appropriate.
The staff have a commissioning function in that they put in place care home placements or refer to the Home Care Commissioning Team to set up a home care package. Referrals to other appropriate professionals are also made, as is support to access community resources.
A key function involves safeguarding adults, including undertaken and supporting safeguarding investigations. Investigation of complaints is also a function of managers in this function.
Direct Payment Function – staff resource
Direct Payments (DP) are the Governments' preferred delivery vehicle for service users to have greater choice and control. Once a package of care has been identified, a personal budget is set against it and this can be taken as a direct cash payment to the user. This allows the individual to determine how best to meet their needs. A small team support individuals who have chosen a DP to ensure they are confident to manager the DP.
Review function in care homes – staff resource
The Council has a statutory duty to carry out at least an annual review of all packages of care. Reviews and reassessments can be carried out more frequently should the need arise. Two staff - Operational Performance Officers (OPOs) carry out this function with people who live in residential homes. The OPOs are responsible for organising the reviews, chairing the meetings and circulating copies of review minutes. The OPOs will also follow up on any actions identified during the reviews.
Health & wellbeing and Carers Service – staff resource
Whilst not everyone will meet the eligibility criteria to receive ASC it is important that help and advice is offered to everyone so that they are able to make informed decisions about their lifestyle and options for support within communities. The Health and Wellbeing Advisors work closely with people to support them in accessing the correct support and the correct connections with community and third sector groups in neighbourhoods. Within the Neighbourhood teams there are specific staff who work directly with carers to identify their care and support needs. The Council has a statutory duty to assess carers’ needs and to provide suitable services to help support carers to continue to carry out their caring role.
Occupational therapy / Manual Handling Team
Adult services carry out assessments to determine whether appropriate community equipment and or adaptations are required. It also provides assessment for people with manual handling needs particularly if they are returning from hospital or are in crisis in their own homes.
TMBC Long Term Support
Reablement Service (CQC Registered) (Inc Homecare through the night)
The Reablement service is a CQC registered service that provides reablement support to individuals whose needs may have changed or have experienced a period of crisis. This service currently provides support for up to 6 weeks and supports the urgent care system in terms of 'step-up' and 'step down' support and provides support in the provision of community care assessments. The service is usually delivered in the individual’s home.
Individuals are referred into the service either from IUCT or from the
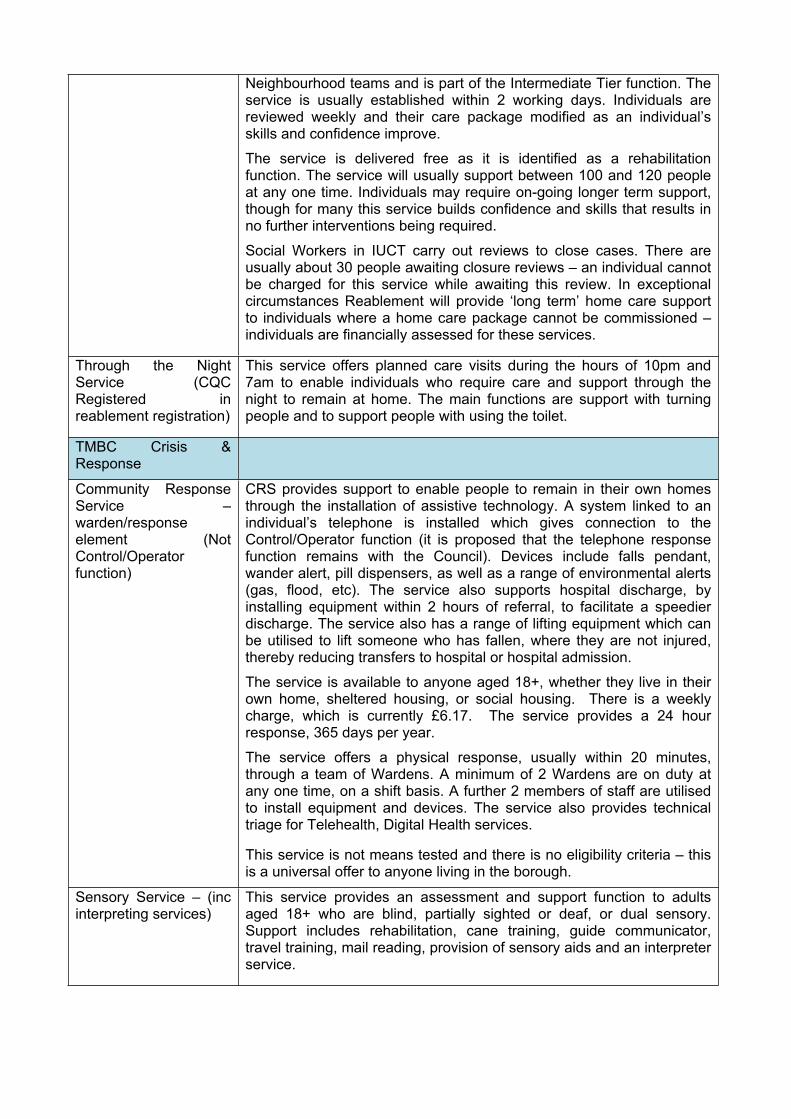
Neighbourhood teams and is part of the Intermediate Tier function. The service is usually established within 2 working days. Individuals are reviewed weekly and their care package modified as an individual’s skills and confidence improve.
The service is delivered free as it is identified as a rehabilitation function. The service will usually support between 100 and 120 people at any one time. Individuals may require on-going longer term support, though for many this service builds confidence and skills that results in no further interventions being required.
Social Workers in IUCT carry out reviews to close cases. There are usually about 30 people awaiting closure reviews – an individual cannot be charged for this service while awaiting this review. In exceptional circumstances Reablement will provide ‘long term’ home care support to individuals where a home care package cannot be commissioned – individuals are financially assessed for these services.
Through the Night Service (CQC Registered in reablement registration)
This service offers planned care visits during the hours of 10pm and 7am to enable individuals who require care and support through the night to remain at home. The main functions are support with turning people and to support people with using the toilet.
TMBC Crisis & Response
Community Response Service – warden/response element (Not Control/Operator function)
CRS provides support to enable people to remain in their own homes through the installation of assistive technology. A system linked to an individual’s telephone is installed which gives connection to the Control/Operator function (it is proposed that the telephone response function remains with the Council). Devices include falls pendant, wander alert, pill dispensers, as well as a range of environmental alerts (gas, flood, etc). The service also supports hospital discharge, by installing equipment within 2 hours of referral, to facilitate a speedier discharge. The service also has a range of lifting equipment which can be utilised to lift someone who has fallen, where they are not injured, thereby reducing transfers to hospital or hospital admission.
The service is available to anyone aged 18+, whether they live in their own home, sheltered housing, or social housing. There is a weekly charge, which is currently £6.17. The service provides a 24 hour response, 365 days per year.
The service offers a physical response, usually within 20 minutes, through a team of Wardens. A minimum of 2 Wardens are on duty at any one time, on a shift basis. A further 2 members of staff are utilised to install equipment and devices. The service also provides technical triage for Telehealth, Digital Health services.
This service is not means tested and there is no eligibility criteria – this is a universal offer to anyone living in the borough.
Sensory Service – (inc interpreting services)
This service provides an assessment and support function to adults aged 18+ who are blind, partially sighted or deaf, or dual sensory. Support includes rehabilitation, cane training, guide communicator, travel training, mail reading, provision of sensory aids and an interpreter service.

4. NEXT STEPS
4.1 If the OBC then receives support from the leadership at both organisations it will then be submitted to NHS Improvement for their consideration. It is expected that NHS Improvement would provide a response by September 2018.
4.2 Should the appropriate approval be given to transfer staff into the ICFT full and formal consultation will be undertaken with all affected staff.
5. RECOMMENDATIONS
5.1 As set out on the front of the report.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 9 of 64
Tameside and Glossop Integrated Care NHS Foundation Trust
Adult Social Care Transaction
OUTLINE BUSINESS CASE
Author: Suzanne Holroyd / Paul Pallister
Date: 21/03/2018File Ref: N/AVersion: v0.12.2Status: For review
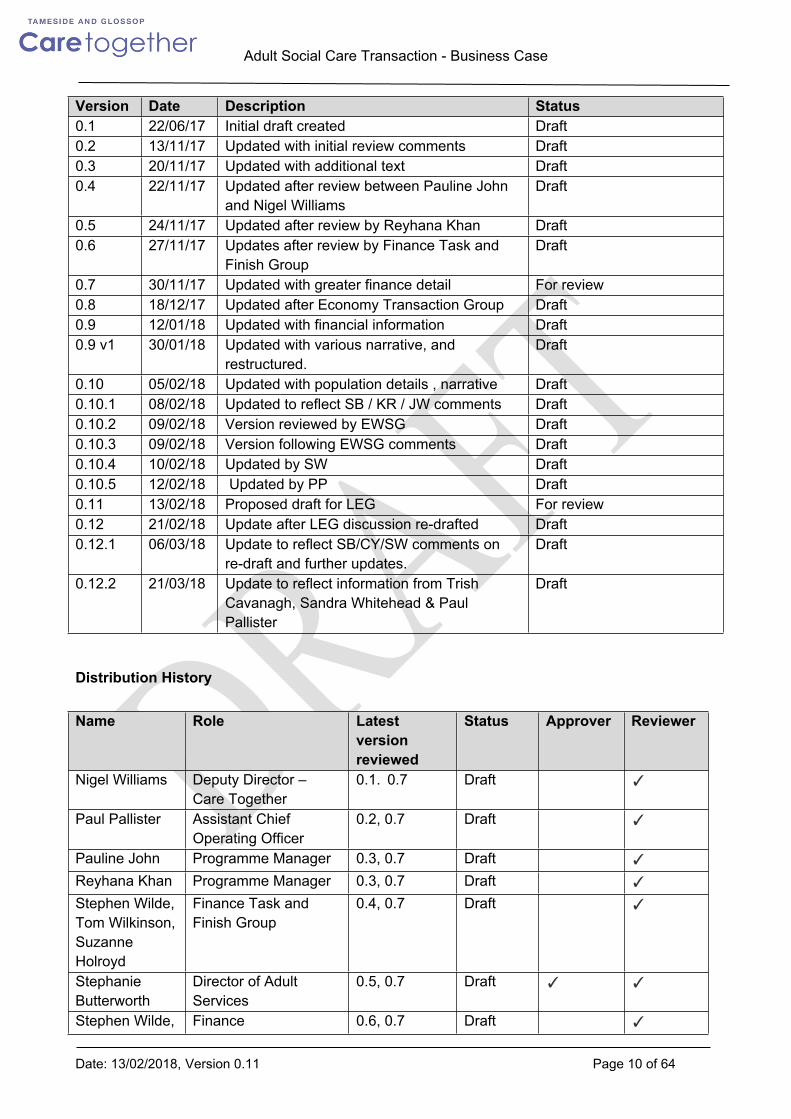
Version History
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 10 of 64
Version Date Description Status0.1 22/06/17 Initial draft created Draft0.2 13/11/17 Updated with initial review comments Draft0.3 20/11/17 Updated with additional text Draft0.4 22/11/17 Updated after review between Pauline John
and Nigel WilliamsDraft
0.5 24/11/17 Updated after review by Reyhana Khan Draft0.6 27/11/17 Updates after review by Finance Task and
Finish GroupDraft
0.7 30/11/17 Updated with greater finance detail For review0.8 18/12/17 Updated after Economy Transaction Group Draft0.9 12/01/18 Updated with financial information Draft0.9 v1 30/01/18 Updated with various narrative, and
restructured. Draft
0.10 05/02/18 Updated with population details , narrative Draft0.10.1 08/02/18 Updated to reflect SB / KR / JW comments Draft0.10.2 09/02/18 Version reviewed by EWSG Draft0.10.3 09/02/18 Version following EWSG comments Draft0.10.4 10/02/18 Updated by SW Draft0.10.5 12/02/18 Updated by PP Draft0.11 13/02/18 Proposed draft for LEG For review0.12 21/02/18 Update after LEG discussion re-drafted Draft0.12.1 06/03/18 Update to reflect SB/CY/SW comments on
re-draft and further updates.Draft
0.12.2 21/03/18 Update to reflect information from Trish Cavanagh, Sandra Whitehead & Paul Pallister
Draft
Distribution History
Name Role Latest version reviewed
Status Approver Reviewer
Nigel Williams Deputy Director – Care Together
0.1. 0.7 Draft ✓
Paul Pallister Assistant Chief Operating Officer
0.2, 0.7 Draft ✓
Pauline John Programme Manager 0.3, 0.7 Draft ✓
Reyhana Khan Programme Manager 0.3, 0.7 Draft ✓
Stephen Wilde, Tom Wilkinson, Suzanne Holroyd
Finance Task and Finish Group
0.4, 0.7 Draft ✓
Stephanie Butterworth
Director of Adult Services
0.5, 0.7 Draft ✓ ✓
Stephen Wilde, Finance 0.6, 0.7 Draft ✓

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 11 of 64
Tom Wilkinson representativesEconomy Transaction Group
Overseeing Board 0.7 Draft ✓
Economy Transaction Group
Overseeing Board 0.8 Draft ✓
ICFT Senior team, Stephanie Butterworth, Tracey Simpson
ICFT Senior TeamDirector of Adult ServicesDeputy Chief Finance Officer
0.9 Draft ✓
ICFT Senior Team
ICFT Senior Team 0.9 v1 Draft ✓
Economy Transaction Group
Overseeing Board 0.10 Draft ✓
Economy Transaction Group
Overseeing Board 0.10.2 Draft ✓
Suzanne Holroyd
Associate Director of Finance ICFT
0.12 Draft ✓
Stephanie Butterworth, Claire Yarwood
Director of Adult Social Services & DoF ICFT
0.12 Draft ✓
ICFT March Part 2 Board & TMBC April Board
Decision Making Bodies
0.12.2 Draft ✓

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 12 of 64
Glossary
Term or abbreviation Description
SOC Strategic Outline CaseOBC Outline Business CaseFBC Full Business CaseASC Adult Social Care ICFT Integrated Care Foundation TrustTMBC Tameside Metropolitan Borough CouncilCCG Clinical Commissioning GroupLA Local AuthoritySCF Strategic Commissioning FunctionDASS Director Adult Social ServicesPOPPI Projecting Older People Population Information
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 13 of 64
CONTENTS 1. Executive Summary2. Introduction3. Strategic Outline Case4. OBC Strategic Vision
4.1 Strategic Vision4.2 Strategic Context4.3 The Tameside & Glossop Case for Change4.4 Rationale for the Transaction of Adult Social Care moving into the ICFT3.5 Strategic Alignment of ASC into the ICFT’s Strategic Plan
5. OBC Options Considered6. Economic Case 5.1 Option 1 5.2 Option 2 5.3 Option 37. Finance Case 6.1 Financial Position in the Economy 6.2 Funding Regimes 6.3 Section 75 Agreement 6.4 Financial Risk Management 6.5 Benefits Realisation 6.6 Financial Option Appraisal 6.7 Financial Principles 6.8 Sensitivity Analysis8. Commercial Case 8.1 Commissioners’ Procurement Strategy 8.2 Due Diligence Summary 8.3 Contractual Arrangements9. Management Case 9.1 Introduction 9.2 Integration Principles 9.3 Management Structure 9.4 Organisational Development 9.5 Governance Arrangements 9.6 Project Management Arrangements 9.7 Summary Next Steps10. Conclusion and Recommendations
Appendices

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 14 of 64
Appendix A: SOC – Long List of OptionsAppendix B: Option Analysis of Gross Expenditure & Associated Funding GapAppendix C: Public Health Joint Needs AssessmentAppendix D: Adult Social Care Budget AnalysisAppendix E: Hempsons’ Due Diligence Report & Questionnaire

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 15 of 64
Executive SummaryThis is the Business Case for the transfer of in house Adult Social Care (ASC) services into Tameside and Glossop Integrated Care NHS Foundation Trust (ICFT) from Tameside Metropolitan Borough Council (TMBC). For the purposes of this document this transaction refers to:
The transfer of the provision of in house ASC services from TMBC into the ICFT The transfer of ASC staff from TMBC into the ICFT
TO BE COMPLETED ONCE ALL OF THE OPTIONS HAVE BEEN WORKED THROUGH AND A RECOMMENDATION MADE

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 16 of 64
1. Introduction
The Tameside and Glossop Economy consists of Tameside & Glossop Integrated Care NHS Foundation Trust (ICFT), NHS Tameside and Glossop Clinical Commissioning Group (CCG) and Tameside Metropolitan Borough Council (TMBC). TMBC provides Social Services within the Tameside area, but does not provide these services to the residents of Glossop who receive Social Services from Derbyshire County Council (DCC). Under the future models of care Glossop residents would continue to receive Social Services from DCC who will not be integrating their services into the ICFT.
The Tameside and Glossop economy has experienced significant clinical and financial sustainability challenges for a number of years. Over a number of years three external reviews have been conducted (Ernst & Young 2012, McKinsey 2013/4, and PwC via Monitor’s Contingency Planning Team process in 2015) and all concluded that improved population outcomes at reduced cost could be achieved through the integration of health and social care services. As the financial challenge continues, we have continued to develop and implement plans to maintain (and in some cases to increase) service provision but at reduced cost.
Monitor appointed Price Waterhouse Cooper (PwC) in November 2014 as a Contingency Planning Team (CPT) to test the financial and clinical sustainability of the then Tameside Hospital NHS Foundation Trust (THFT) following a number of critical reports. The CPT report was supported and published by Monitor in September 2015 and fed directly into the on-going transformation work across the economy. The CPT process provided considerable assurance on our plans as it concluded that THFT should become an Integrated Care Foundation Trust (ICFT) as the delivery vehicle for providing an integrated health and social care system.
The CPT report proposed the full integration of Community Services, Adult Social Care, Mental Health Services and Commissioning into the ICFT in order to support ongoing financial sustainability of the ICFT. The ICFT has already integrated Community Services into the Trust in April 2016 as the first stage of the integration process. This OBC intends to further progress the process with the integration of Adult Social Care Services which are currently provided by TMBC directly employed Social workers and other associated staff.
2. Strategic Outline Case
This Outline Business Case (OBC) integrates a high level Strategic Outline Case (SOC) and the OBC within one document as agreed with NHSI.
The ICFT, TMBC and CCG considered a number of various integration options at the SOC stage and concluded that the options distilled in the OBC were the most effective options at this time.
The long list of options considered within the SOC are detailed below:-
Option One – Do nothing

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 17 of 64
Option Two – Full integration of all Adult Social Care Services, and CCG Commissioned Services.
Option Three – Full integration of all Adult Social Care Services, and a subset of CCG Commissioned Services.
Option Four – Full integration of all Adult Social Care Services (including staff and funding).
Option Five – Integration of in house ASC delivered services from TMBC into the ICFT through TUPE arrangements
Option Six - Integration of in house ASC delivered services from TMBC into the ICFT with TMBC staff being seconded into the ICFT
Option Seven - Integration of a subset of in house ASC delivered services from TMBC into the ICFT, through TUPE arrangements
Option Eight: Integration of a subset of in house ASC delivered services from TMBC into the ICFT, as detailed in Appendix B, with the LA staff seconded into the ICFT.
The high level reason for excluding each of the options not taken forward are detailed below.
Option Two – Full integration of all Adult Social Care Services, and CCG Commissioned Services.The Trust engaged Hempsons Solicitors in July 2017 to undertake a review of the integration of all Adult Social Care and CCG Commissioned Services. As a result of this review it was determined that including the integration of CCG Commissioned services would slow the process down due to the proposal not being sufficiently developed and the legal issues that would need resolving in order to transfer CCG Commissioned Services, as it is not lawful for the CCG to delegate its functions to an NHS Foundation Trust. This option also transferred significant financial risk to the ICFT and under the Single Oversight Framework this may have resulted in the failure to secure an acceptable NHS Improvement risk rating
Option Three – Full integration of all Adult Social Care Services, and a subset of CCG Commissioned Services.The reasons for discounting this option were the same as option two but the financial risk had reduced but only marginally. The largest financial risk remained associated with all of adult social services transferring. There also remained potential legal issues with the sub-set of CCG Commissioned services.
Option Four – Full integration of all Adult Social Care Services (including staff and funding).This option was discounted on the level of financial risk to the ICFT. The transfer of all Adult Social Care Services had the potential to have transferred a financial gap of £x by 22/23 to the ICFT with no clear financial or operational plans to mitigate this.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 18 of 64
Option Five – Integration of in house ASC delivered services from TMBC into the ICFT through TUPE arrangementsThis option was also discounted on the level of financial risk to the ICFT.
Option Six - Integration of in house ASC delivered services from TMBC into the ICFT with TMBC staff being seconded into the ICFTThis option was also discounted on the level of financial risk to the ICFT.
A matrix of the services considered as part of each of the options can be found at Appendix A. Appendix B details the financial gap details and values of the services within each option.
The table below details for the Adult Social Service options transferring (excludes back office support functions), the 2023/24 projected financial gap associated with each option, and supports the option being discounted on the basis of financial risk.
Table:- Adult Social Care Financial Gap Associated with each of the Options
2023/2024 Projected Gap
Option 1
Option 2
Option 3
Option 4
Option 5
Option 6
Option 7
Option 8
TMBC ASC Financial gap
£m
17,318 17,318 17,318 17,318 4,312 4,312 2,264 2,264
Only options one, seven and eight have been taken forward as the shortlist of options into the OBC, as such the later parts of this OBC will be limited to the remaining three options. Section 4 details the OBC options and the services covered within the case.
3. OBC - Strategic Case
3.1 Strategic Vision
Care Together is our transformational approach to improving significantly the health and wellbeing of the 250,000 residents of Tameside and Glossop. The programme comprises three key elements:
The establishment of a Strategic Commissioning Function to ensure resources are aligned and distributed in a way which facilitates integration and most effectively meets need
The development of an Integrated Care Organisation to eliminate traditional organisational silos and boundaries
A new model of care to drive forward at pace and scale the changes required in order to achieve our ambitions of improved outcomes for our population and a financially and clinically sustainable health and care system.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 19 of 64
We aim to develop a sustainable economy by improving the healthy life expectancy (HLE) of our population. In doing this, our programme has three key ambitions which are wholly in line with both Greater Manchester and national policy:
1. To support local people to remain well by tackling the causes of ill health, supporting behaviour and lifestyle change, and maximising the role played by local communities
2. To ensure that those receiving support are equipped with the knowledge, skills, and confidence to enable them to take greater control over their own care needs and the services they receive
3. When illness or crisis occurs, to provide high quality and integrated services designed around the needs of the individual and, where appropriate, provided as close to home as possible.
We have the economy-wide leadership in place to deliver our integration agenda. We have a coherent, ambitious strategy and comprehensive governance arrangements and have already delivered a Strategic Commissioning function. Implementation is underway to transform to our new models of care. We have one health economy with all partners equally sharing the risk and burden of deficit. This Outline Business Case sets out the opportunity for delivering at pace the three key ambitions above by bringing together health and adult social care services and, in the process, transforming the local hospital into an Integrated Care Foundation Trust. This ambitious programme firmly establishes the confidence held by the Strategic Commissioners regarding the Foundation Trust’s ability to develop into a fully-fledged Integrated Care Foundation Trust by taking responsibility for the provision of Adult Social Care and integrating these services with community and acute medicine. As evidence of this confidence and in order to support the transaction the Strategic Commission has agreed to underwrite the financial risk in full for a number of years and then for a proportion for a further period of time.
We are confident that the aims of this transaction are achievable; we have taken learning from colleagues elsewhere in Greater Manchester and note for example the progress made by the Salford locality to bring together Adult Social Care and health services.
We are fully cognisant of the context within which we are operating; we know that by progressing this transaction at pace we have the opportunity to deliver Adult Social Care services to the ICFT without the requirement of undergoing a largescale procurement process.
We recognise our locality’s uniqueness both within Greater Manchester and nationally. We are rightly acknowledged as being at the forefront of integration and this transaction will further cement our reputation as visionary system leaders.
3.2 Strategic Context
The way in which the NHS and care partners provide health and care services has been the subject of review for a number of years as the UK population and its needs change. Demand for services is increasing as people live for longer with more complex health and care needs. Consequently, the current model of care which we offer is under pressure.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 20 of 64
In 2014 the NHS published a Five Year Forward View (FYFV), which recognised the scale of the challenges facing the health and care system in England and projected a funding gap of up to £30bn by 2020 if the NHS did not radically change the way it delivered services. This called for changes to the way in which health and care is provided, to better meet the needs of individuals, whilst meeting the financial and sustainability challenge. This recognised the need for a wholesale shift towards care that is; focussed on prevention as much as cure, that empowers people to manage their health and care, and is organised around the needs of the individual as well as the assets of the community.
The Greater Manchester Health and Social Care Partnership (GMH&SCP) has developed its five year plan ‘Taking Charge of our Health and Social Care in Greater Manchester’. This describes the vision for Greater Manchester (GM) ‘to deliver the fastest and greatest improvement in health and wellbeing of the 2.8 million population of GM, creating a strong, safe and sustainable health and care system that is fit for the future’.
Locally the Public Health Joint Strategic Needs Assessment (Appendix C) highlights that people in Tameside and Glossop experience particularly high levels of ill health, and shorter life expectancy, than the national average. Additionally projections indicate that the population of Tameside and Glossop will increase by 10% by 2035 to 280,000 with a greater growth in the number of older people.
The locality has some significant social issues including continuing high levels of relative deprivation as well as the impact of a reducing resource base.
The health of people in Tameside is generally worse than the England average. Tameside is one of the 20% most deprived districts/unitary authorities in England and about 24% (10,600) of children live in low income families. Life expectancy for both men and women is lower than the England average. Life expectancy locally is about 7 years lower for men and 8 years lower for women in the most deprived areas of Tameside compared to the least deprived in the borough (as at 2014/16).
In adults the recorded diabetes prevalence, excess weight, and drug and alcohol misuse is significantly worse than the England average. Rates of smoking related deaths and hospital admissions for alcohol harm are significantly higher than the England average. 70% of all preventable disease in Tameside is linked to four conditions (Liver disease, Heart disease, Respiratory disease, and Cancer).
Compared with England as a whole, Tameside and Glossop has a slightly lower proportion of people aged 20-39 and a slightly higher proportion of people aged 40-69. In addition, an ageing population is likely to increase the overall prevalence of life limiting long term illness or disability and increase demand for health services and social service interventions. The burden on and need for efficient Adult Social Care services is likely to increase over the next few years.
The table below indicates elements of Tameside population projections to 20351. The data source is POPPI (Projecting Older People Population Information), and specifically relates to Tameside, and excludes Glossop’s population.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 21 of 64
Table: TMBC POPPI Data
2018 2020 2025 2030 2035 Percentage Increase
People aged 65 and over 40,400 41,400 45,600 51,300 56,200 39%
People aged 85 and over 4,600 4,800 6,000 7,400 9,600 109%
People living with dementia 2,603 2,745 3,183 3,750 4,307 65%
People living with a limiting long term illness
22,362 23,038 25,737 28,896 31,890 43%
People 65 and over unable to manage at least one personal care task
15,842 16,423 18,511 21,038 23,477 48%
As can be seen from the table above over the next seventeen years there is projected to be a thirty nine percent increase in people over the age of 65 within the Tameside area, and a forty eight percent increase in people unable to manage at least one personal care task, and a forty three percent increase in people living with a limiting long term illness.
All of these projections will put increasing pressure on the local health and social care economy, thereby emphasising the need for transformation of the way in which services are provided.
Changes in the ageing population are already contributing to an increased demand on health and social care services. The demands on these services will continue as people live longer and the dynamics of the ageing population changes. The number of carers will also increase as more people live longer and therefore it is important to have responsive, flexible arrangements in place to support those people caring for others and to support people who want to live independently; this will create a health and social care culture where the need for secondary hospital services are a last resort.
3.3 The Tameside and Glossop Case for Change
Traditionally, the provision of ASC services within Tameside and Glossop rested with TMBC for the residents of Tameside. With the increased collaboration between TMBC, the CCG and the ICFT it was recognised that there was an opportunity to transfer the provision of in house ASC services to the ICFT. It was felt that this gave an opportunity to rationalise the service within the local health and care economy without negatively impacting patient care.
The vehicle for implementing the Care Together vision is the ICFT. The ICFT would bring together under the controlling auspices of one organization the provision of:-
In house Adult Social Care services currently provided by TMBC Community health services which are already integrated into the ICFT

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 22 of 64
Hospital services.
This proposal supports that intention by moving a defined set of ASC services into the ICFT and is in alignment with recommendations contained within the Contingency Planning Report (2015).
Through strong leadership, pooling our resources, and redesigning how our health and social care provision works collectively we aim to improve financial sustainability. This will be achieved by a continued focus on:
Reducing growth in health and social care demand Avoiding unplanned admissions Preventing ill health Use of the Voluntary sector and communities Efficiency and unlocking the potential of enabling work streams.
Our transformation plans describe how health and social care services will contribute towards our whole system ambition of improving health, wellbeing and prosperity.
The local health and social care economy has delivered significant transformation over the last two years culminating in the formation of the Strategic Commissioning Function and the continued development of the Integrated Care Organisation to deliver the economy vision. TMBC, Tameside and Glossop ICFT, and the CCG have a significant track record in the delivery of substantial strategic change programmes. We are therefore in a strong position to drive ahead at both pace and scale with the programme identified in this Outline Business Case.
3.4 Rationale for the Transaction of ASC moving into the ICFT
The Tameside and Glossop locality has created a compelling case for the development of the local health and care economy (social care, health, primary care, mental health, voluntary and community sector and others) to deliver a significantly improved offer and outcomes for local people. The vision is predicated on a fully integrated model that promotes good health, great outcomes for local people and manages the demographic challenges faced by the locality. The locality has received external assurance (from the CPT report commissioned by then Monitor) that this is the appropriate strategy.
The model of care that is currently being implemented through our local transformation programme is fundamentally about an offer:
to activate and empower local people and communities to look after their own health to do so in the context of wider determinants of health reaching across to leisure,
housing, education, employment and training, and local economic development to deliver care in or as close to people’s homes as possible developing five
neighbourhood community care teams bringing together professional expertise, including primary care, offering a range of services for preventative and proactive care interventions and support for people living with long term conditions. Hospital based services would only be provided where there is no other suitable setting of care.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 23 of 64
In order to maximise the benefits of this model and to deliver against the transformation programme, it is crucial that health and social care services are delivered in a fully integrated manner. This will ensure maximum flexibility in the movement of funding and resources across the whole system to support and enable people to remain in good health and to delay the need for more intensive interventions. It is only by bringing health and social care services into an integrated system that the opportunities to transform services can be maximised.
Our vision for Adult Social Care is as an integral element of a system that delivers our ambitions for local people, maximises the opportunities to maintain and develop people to live well in their own homes, supports and promotes independence, minimises social isolation and develops a local offer where people expect to self-care when appropriate and to engage with local community assets to ensure personal resilience and self-determination.
Other ASC services and functions are integral to the delivery of the model, and being part of a single economic entity ensure maximum flexibility in how these resources are deployed to impact positively on system priorities. An example of this is the Community Response Service that delivers a physical response to individuals via a pendant alarm system. This service works collaboratively with Digital Health Service and forms an integral part of the falls prevention agenda, the frailty programme across Integrated Neighbourhoods and the Support at Home model.
The creation of an ICO requires a higher level of service integration that cannot be delivered through collaboration alone. Bringing the full range of care within a unified, aligned management structure and contractual arrangement enables more efficient, effective and person-centred services.
Although care can be integrated without transfer to the ICFT the advantage of this approach is that a unified organisation with one funding envelope, an agreed set of objectives and a shared vision of integration for the future of Tameside and Glossop’s health and social care economy is better able to avoid the problems of fragmentation and duplication. An ICFT should be able to more effectively ensure:
Consistency in applying operational policies and procedures Consistency in applying risk, governance and performance principles The spread and sustaining of improvements to practice across the whole economy The improvement of communication, information and reporting systems Faster reaction to changes in demand and times of pressure More innovation in developing new services Provide more assurance to staff and improve sickness and retention rates Collectively deliver improved outcomes for local people it serves Efficient and effective use of resources
3.5 Strategic Alignment of Adult Social Care into ICFT’s Strategic Plan
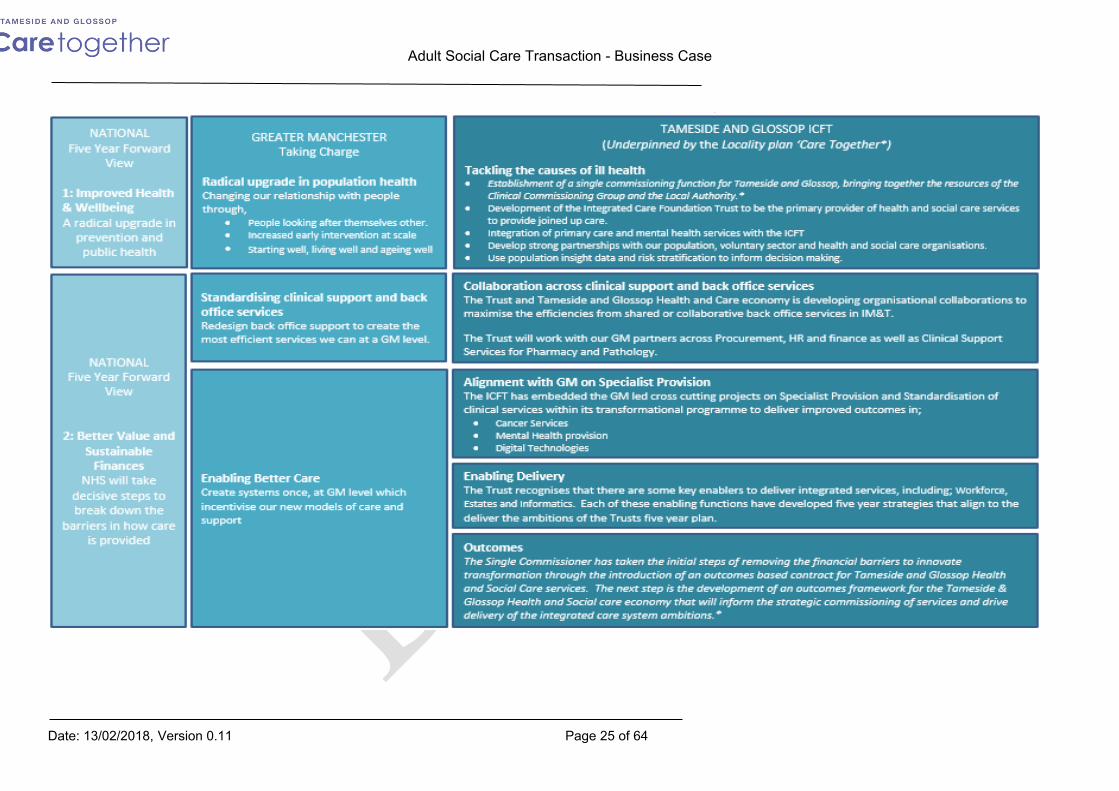
The integration of ASC forms an integral element of the ICFT’s five year strategic plan. The table below demonstrates how the Trust’s five year strategic plan is aligned to and enables the

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 24 of 64
delivery of the triple aims of the national five year forward view and the Greater Manchester plan, Taking Charge and Locality plans. (* denotes locality plans)
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 25 of 64

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 26 of 64
N A T I O N A L
F i v e Y e a r F o r w a r d
V i e w
3: Transformed Quality of Care
DeliveryWhen people do
need health servi ces, pati ents
wi ll gai n far gr eater contr ol of thei r own care.
GREATER MANCHESTERTaki ng Char ge
Transforming community based care and supportTransform care in localities by integrating primary, community, acute, social and third sector care through the development of new local Care Organisations (LCO’s) focussing on; Managing care at home and in the
community Providing alternatives to A&E when
crisis occurs Supporting effective discharge from
Hospital Helping people return home and stay
well
TAMESI DE AND GL OSSOP ICFT (Underpinned by the Locality plan ‘Care Together*)Supporting People with Greater ControlThe support people need to stay healthy and well is not always medical or based on treatments. It can be practical help with tasks of daily living, emotional support, or information so that people can better manage their own health. This will be delivered through System-Wide Self-Care, which includes;
Social Prescribing Asset Based Approaches Self-management education Person-centred care and support
Standardising acute and specialist careStandardise and create consistent evidence based hospital services so that; Care that does not require a hospital
stay will be provided locally In-patient emergency care and all in-
patient surgery would be organised at a cluster or group level.
Highly specialised services requiring specialist skills and infrastructure will be organised at a GM level.
Integrated services closer to homeThe ICFT has committed to bringing together health and social care services within Tameside and Glossop, to provide seamless care to meet all of an individual’s needs rather than treating each condition or need as an isolated episode and where possible to delivering services within the communities or in people’s homes. Our approach will be to;
Adopt a Home First principle to support effective and timely discharge from hospital and avoid unnecessary admissions. Create integrated neighbourhood teams (INTs) made up of a range of health and social care professionals to provide co-
ordinated care and support to people who live in their neighbourhood. INT multi-disciplinary team will work closely with community, including carers, the local voluntary sector, and wider statutory services.
Provide specialised health or social care services through the Intermediate Tier services Develop innovative and integrated end of life and frailty care pathways. Develop the home care service in Tameside and Glossop to provide individualised patient centred care that gives
individuals greater control.
Developing Local Hospital ServicesThe Integrated Care Trust will continue to provide and develop seamless and joined-up Local Hospital Services to the population of Tameside and Glossop. Including:
Development of an Urgent Care Treatment Centre on the Hospital site to provide alternatives to A&E* Collaboration with Mental Health Partners to simplify and improve mental health provision for our populations.* Development of Maternity Services and network arrangements with other organisations to deliver high quality maternity
services for a wider geographical population. Development of collaborative and network arrangements with other organisations to provide high quality specialist care
for our population. Enhance the Trusts Research and Development programme and participation in clinical trials. Contributing to wider work on the standardisation of clinical services across Greater Manchester to look at how services
in key clinical areas can be provided in a more standardised way across GM.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 27 of 64
4.0 OBC - Options considered
The three partner organisations considered various options at the SOC stage as discussed in section two. Although it remains the intent to progress the integration in the future to include the wider scope of Adult Social Care services it was decided to transact of smaller sub-set of Adult social care in the first instance to both prove the concept and limit the financial and operational risk. It remains the intent that in future further services would still look to be transferred. The following short list of options taken forward therefore reflects a staged approach and an agreed initial configuration of the ICFT.
This Outline Business Case considers the following five options for the transaction of Adult Social Care services into the ICFT.
Option One: Do Nothing
Option Two: Transfer the provision of a subset of ASC delivered services from TMBC into the ICFT, as detailed in Appendix B, through TUPE arrangements
Option Three: Transfer the provision of a subset of ASC delivered services from TMBC into the ICFT, as detailed in Appendix B, with the LA staff seconded into the ICFT.
For clarity, the definition of ‘ASC delivered services’ is staff and services that are delivered directly by the Council (that is, TMBC employed staff) not services that are commissioned by TMBC to meet need (such as residential and nursing care beds, home care services). These have not been considered for transaction at this time but will be considered for a separate transaction at a later date.
Both options two and three would see the same services transferring across to the ICFT but just under differing operational models.
The services that would transfer under both options two and three are detailed below with a brief service description in order to aid understanding of the options.
Service Area – Adult Social Care
Service Description
TMBC Urgent CareService Unit ManagerIntegrated Urgent Care Team (IUCT) - staff and Management team
The ASC resource in IUCT is made up of Social Workers, Assessors Assistant Practitioners, Customer Care Officers. Community Care Officers and therapists, including Physios and OTs. The function of the team is to aid a speedy discharge from hospital, prevent hospital admission, deal with a wide range of situations which present within the community, the referrals that are received by the Team come from a range of sources, such as GP's, Emergency Services, other professionals, families and carers. The function of the Team is to assess a persons’ needs and requirements, provide a 72 hour wrap around service establishing on-going support requirements going forward. At present the team also carry out rehabilitation for a period of time, which should be no longer than 6 weeks.
Integrated Community Integrated Community Equipment Services provides a vast range of equipment

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 28 of 64
Equipment Service (ICES) - Service co-ordination staff member
to support people either in their own homes or the establishments they live in. ICES contract has three partners – TMBC, CCG and Derbyshire County Council. It is currently a section 75 pooled budget with TMBC as the lead Commissioner. The contract is currently being reviewed to determine future commissioning arrangements. A Co-ordinator is employed to ensure appropriate ordering and prescribing by health and social care staff, and to monitor the performance of the contract.
TMBC – LocalitiesAssessment / Care Co-ordination (18+) Inc Locality teams and management
The Care Act 2014 provides a statutory duty on the Council to carry out an assessment of need for anyone requesting it. Once an assessment has taken place, the application of the national eligibility criteria is made and a suitable support plan is determined. People receiving a package of care must be reviewed/reassessed annually as a minimum and those with complex care packages will be care managed/care co-ordinated throughout their time with the service.
Assessment and Care Management staff undertake assessments and annual re-assessments. They hold a caseload, and will support individuals on an on-going basis, working proactively with individuals to enable them to live well in their own homes. Where an individual experiences a crisis or experiences a change in need the Social Worker/Assessor will work with the individual, carrying out a re-assessment where appropriate, and amending/changing the support plan where appropriate.
The staff have a commissioning function in that they put in place care home placements or refer to the Home Care Commissioning Team to set up a home care package. Referrals to other appropriate professionals are also made, as is support to access community resources.
A key function involves safeguarding adults, including undertaken and supporting safeguarding investigations. Investigation of complaints is also a function of managers in this function.
Direct Payment Function – staff resource
Direct Payments (DP) are the Governments' preferred delivery vehicle for service users to have greater choice and control. Once a package of care has been identified, a personal budget is set against it and this can be taken as a direct cash payment to the user. This allows the individual to determine how best to meet their needs. A small team support individuals who have chosen a DP to ensure they are confident to manager the DP.
Review function in care homes – staff resource
The Council has a statutory duty to carry out at least an annual review of all packages of care. Reviews and reassessments can be carried out more frequently should the need arise. Two staff - Operational Performance Officers (OPOs) carry out this function with people who live in residential homes. The OPOs are responsible for organising the reviews, chairing the meetings and circulating copies of review minutes. The OPOs will also follow up on any actions identified during the reviews.
Health & wellbeing and Carers Service – staff resource
Whilst not everyone will meet the eligibility criteria to receive ASC it is important that help and advice is offered to everyone so that they are able to

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 29 of 64
make informed decisions about their lifestyle and options for support within communities. The Health and Wellbeing Advisors work closely with people to support them in accessing the correct support and the correct connections with community and third sector groups in neighbourhoods. Within the Neighbourhood teams there are specific staff who work directly with carers to identify their care and support needs. The Council has a statutory duty to assess carers’ needs and to provide suitable services to help support carers to continue to carry out their caring role.
Occupational therapy / Manual Handling Team
Adult services carry out assessments to determine whether appropriate community equipment and or adaptations are required. It also provides assessment for people with manual handling needs particularly if they are returning from hospital or are in crisis in their own homes.
TMBC Long Term Support
Reablement Service (CQC Registered) (Inc Homecare through the night)
The Reablement service is a CQC registered service that provides reablement support to individuals whose needs may have changed or have experienced a period of crisis. This service currently provides support for up to 6 weeks and supports the urgent care system in terms of 'step-up' and 'step down' support and provides support in the provision of community care assessments. The service is usually delivered in the individual’s home.
Individuals are referred into the service either from IUCT or from the Neighbourhood teams and is part of the Intermediate Tier function. The service is usually established within 2 working days. Individuals are reviewed weekly and their care package modified as an individual’s skills and confidence improve.
The service is delivered free as it is identified as a rehabilitation function. The service will usually support between 100 and 120 people at any one time. Individuals may require on-going longer term support, though for many this service builds confidence and skills that results in no further interventions being required.
Social Workers in IUCT carry out reviews to close cases. There are usually about 30 people awaiting closure reviews – an individual cannot be charged for this service while awaiting this review. In exceptional circumstances Reablement will provide ‘long term’ home care support to individuals where a home care package cannot be commissioned – individuals are financially assessed for these services.
Through the Night Service (CQC Registered in reablement registration)
This service offers planned care visits during the hours of 10pm and 7am to enable individuals who require care and support through the night to remain at home. The main functions are support with turning people and to support people with using the toilet.
TMBC Crisis & Response
Community Response Service – warden/response element (Not Control/Operator function)
CRS provides support to enable people to remain in their own homes through the installation of assistive technology. A system linked to an individual’s telephone is installed which gives connection to the Control/Operator function (it is proposed that the telephone response function remains with the Council). Devices include falls pendant, wander alert, pill dispensers, as well as a range of environmental alerts (gas, flood, etc). The service also supports hospital discharge, by installing equipment within 2 hours of referral, to facilitate a

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 30 of 64
speedier discharge. The service also has a range of lifting equipment which can be utilised to lift someone who has fallen, where they are not injured, thereby reducing transfers to hospital or hospital admission.
The service is available to anyone aged 18+, whether they live in their own home, sheltered housing, or social housing. There is a weekly charge, which is currently £6.17. The service provides a 24 hour response, 365 days per year.
The service offers a physical response, usually within 20 minutes, through a team of Wardens. A minimum of 2 Wardens are on duty at any one time, on a shift basis. A further 2 members of staff are utilised to install equipment and devices. The service also provides technical triage for Telehealth, Digital Health services.
This service is not means tested and there is no eligibility criteria – this is a universal offer to anyone living in the borough.
Sensory Service – ( inc interpreting services)
This service provides an assessment and support function to adults aged 18+ who are blind, partially sighted or deaf, or dual sensory. Support includes rehabilitation, cane training, guide communicator, travel training, mail reading, provision of sensory aids and an interpreter service.
The table below details both the number of staff employed in each of these services, and where appropriate, details the activity levels associated with the service.
Table :- Transferring Staff Numbers and Service ActivitySERVICE/FUNCTION NUMBER OF
STAFFING POSTS
ACTIVITY
Integrated Urgent Care Staff & Management Team
47
ICES Service co-ordination 1
Assessment / Care Co-ordination (18+) 48 2,515
Direct Payment Function - staff resource 2 315 service users
Review function in care homes - staff resource 2 386 residents
Health & Wellbeing and Carers Service (Inc Management)
9 929 includes carers and wellbeing
Community Occupational Therapy / Manual Handling Team
19 1,321
Reablement Service 131 115
Through the Night Service 11 43
Community Response Service 50 3,42518,000 in-bound calls on CRS per month 1,300 in-bound calls on Control per month (approximately 342 relating to ASC)

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 31 of 64
Sensory Service including Interpreter Services 8 136541 Interpreting sessions182 Mail Reading
Total Staff 328
In addition to the service departments transferring it will be necessary to transfer either function or funding to support back office functions. If operationally it is better to retain the function with TMBC in order to maintain economies of scale funding will transfer and a service level agreement will be put in place for the ICFT to purchase the service from TMBC. Alternatively funding and staff will transfer and the service will be integrated into the ICFT. The table below identifies the functions:-
Function Service descriptionAssistant Director AdultsHead of Service Assessment and Care ManagementFinanceHuman ResourcesLegalInformationPayrollIT & SystemsPerformance ManagementQuality Governance
Further work will be required between approval of the OBC and FBC to develop the options and values associated with back office functions, as it is only proposed to transfer a sub-set of ASC which will mean that it is more difficult to disaggregate roles and responsibilities as most staff will support the whole of ASC services. Any agreements will need to ensure value for money and aim to avoid any increases in economy costs.
TMBC will still maintain legal responsibility for the provision of ASC services (although they will choose to discharge this responsibility through using the ICFT as their provider). This responsibility will be protected by the introduction of a Service Level Agreement. There will need to be appropriate additional controls around safeguarding, and assurance to TMBC that the ICFT is delivering social care effectively, ensuring TMBC duties are being delivered in accordance with the law.
Further detail on the options and the benefits and dis-benefits of each of the options taken forward in the OBC are included in the economic case below.
5.0 Economic Case
5.1 Option One – Do NothingThe three partners (CCG, ICFT and TMBC) could do nothing. This would leave the responsibility for providing Adult Social Care with TMBC. Nothing would be changed.
5.1.1 Benefits
Lowest risk option in the short term

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 32 of 64
No additional risk of disruption to patients/clients No additional risk of disruption to the hospital or staff – at the moment the ICFT and
ASC is undergoing considerable change and transformation. This would be an additional significant change
5.1.2 Dis-benefits
No opportunity to change and improve the service (financial) Ignores the wider integration agenda Fragmentation of services Duplication of service provision Whole economy gap will remain and money will not flow through the system Less scope to improve the quality of services, as organisations work in silos. Less opportunity to improve user experience Lose opportunity to develop organisational development activities Reputational damage in terms of money already spent on forming partnerships. Opportunities to maximise early intervention, prevention and community based
interventions will be lost Limited opportunities to develop a ‘think family’ and place based approach to meet
people’s needs Lose opportunity to access and share skills and knowledge across the organisation
5.1.3 Risks of this option
The significant drawback of the ‘Do nothing’ option is that is does not help the partners to address the whole economy financial gap. Under this option none of the three statutory partners to the Tameside and Glossop Locality Plan will be in financial balance by the end of the time period. Also there will be no significant progress made to deliver the required improvements in healthy life expectancy.
5.2 Option 2 – Transfer the provision of a subset of ASC delivered services from TMBC into the ICFT, as detailed in appendix A, through TUPE arrangements.
5.2.1 RationaleThere are a range of services that have a close interface between the ICFT and social care. These services identified as transferring as a subset of ASC are those that are more easily recognised as supporting the individual’s journey through the health and social care system, since they impact more directly on the transition of care between the acute sector and neighbourhood provision. Several operate to support people to remain at home through an admission avoidance function or ensure that an individual’s care is supported on discharge from hospital care.
The transformational work already commenced as part of the Care Together Programme has demonstrated the synergies/co-dependencies between these services and the benefits to the system and individuals that can be gained when pathways are streamlined and care better co-ordinated. It becomes more difficult to articulate a rationale for managing all

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 33 of 64
services under the current ASC remit the further along a continuum that those services are away from that health/social care interface.
It is therefore proposed that a subset of ASC services are transferred (as listed in Section four and in appendix A) along with the funds/staff required to perform them. It has been established that operationally the majority of these services are already closely aligned and that further integration would be beneficial to ensuring that standardisation of policies and working practices could be completed. Services that are partially aligned rather than fully integrated do present some issues as this alignment leads in some instances to clear lines of responsibility and accountability becoming more blurred. Whilst this is not necessarily a disadvantage for service users it can become complex for staff operating in the service and attempting to respond to the different organisational requirements.
Whilst it is unlikely that full integration of these services would result in significant cash releasing benefits in the short term, it would assist in supporting workforce redesign within health and social care in the medium to long term. The opportunities for exploiting the potential for developing apprenticeships and new roles and career paths is unlikely to occur in the absence of fully integrated services but would be an advantage given the predicted future shortfall in workforce across these sectors.
The need for data sharing presents further rationale for the transfer of these services. The interventions with the client group served by these services currently requires complex data sharing arrangements and access to and recording on multiple information systems. This would be more streamlined within a fully integrated service having the potential for the development of single assessment documentation between professional disciplines. This would enhance quality, potentially reduce risk and avoid duplication.
A number of considerations relating to governance issues could also be addressed and simplified with one organisation having a single line of sight on incidents and opportunities for improvement in the quality of services. This may present some risks, if not regulatory then reputational, as the ICFT develops a more in-depth understanding of service delivery and the potential risks inherent within them. To some extent this could be covered in part by a risk-sharing agreement though any public perception of a poor quality of service would be unlikely to be resolved even if this were in place. Given the high degree of regulation of health services, there may be some differences in the risk appetite between organisations. That said, the services recently reviewed by the CQC have been positively rated.
The services not included in this option are the longer term provision of care and mental health services. Whilst there is some risks that the flexibility gained by the transfer of ASC to the ICFT would be at the expense of the loss of the same flexibility between those ASC services remaining and those transferring, it is likely that greater benefits would be gained from the transfer.
Further information is available in the detailed benefit profiles below.
5.2.2 Benefits
This option in part mitigates the risk deriving from a transaction the size of the whole of Adult Social Care; it is more likely that both organisations would more easily be able to continue to meet their statutory duties.
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 34 of 64
The scale of change would be less likely to distract from the transformational programme and would enhance the work undertaken to date.
Operational teams are currently working in a partially integrated manner and there are further operational benefits that would be realised with the standardisation of policies and procedures. It is likely that staff would have more clarity on lines of reporting, responsibility and accountability.
Data sharing would be less complex and there is potential for streamlining assessment processes and avoidance of duplication.
Governance arrangements could be more easily determined and opportunities for learning and improvement accelerated and risk reduced.
Workforce planning could be completed in an integrated manner creating the potential for new roles which would be unlikely to occur if services remained separate. This is important given the future reductions in workforce across both health and social care sector.
5.2.3 Dis-benefits
There would be a separation in ASC services which does not currently exist and a potential loss of flexibility in TMBCs ability to flex resources as it does at present.
The ICFT may have a different risk appetite than TMBC and determine risks to be greater than is currently perceived.
5.2.4 Risks of this option
However leading from this specific option is the risk that the functions identified for transfer will either not be sufficient to address the locality’s financial challenge and / or be unable to enable the delivery of significant service transformation to deliver the Locality Plan’s objectives.
This option also carries the risk of failing to agree an appropriate financial value of the transaction as only a subset of services is to transfer. Under this option the ICFT holds the risk for the transfer of the identified staff.
5.3 Option 3 – Transfer the provision of a subset of ASC delivered services from TMBC into the ICFT, as detailed in Appendix A, with the LA staff seconded into the ICFT.
5.3.1 Rationale
The rationale for this option are the same as those discussed in section 5.2.1.
5.3.2 Risks of this option
This option contains the same risk profile as Option Two above but without the ICFT taking on the same degree of staffing risk. There continues to be the risk of having two cohorts of

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 35 of 64
staff on different terms and conditions.
5.4 Adult Social Care - Support Functions
In terms of the back office functions that support the new organisational form there are three key options to be considered.
No back office functions transfer from TMBC to the ICFT and instead there is a range of Service level agreements put in place to cover the requirements.
Transfer all of the back office functions from TMBC into the ICFT Transfer a subset of back office functions dependent on which option is
recommended.
6.0 Finance Case
6.1 Financial Position within the EconomyIn 2015 the ICFT, CCG and TMBC worked together to develop their locality plan. As part of that locality plan the three organisations developed a projected financial gap by 2020/21. At that time the projected gap was £70 million assuming that the ICFT could deliver £30 million pounds of cash releasing savings across that period. As such the economy do nothing gap was circa £100m. It should be noted that TMBC’s financial gap included Children’s services which no longer forms part of the integration plans.
The table below identifies the latest projected economy gap (still incorporating TMBC’s Children’s Services.
Economy Financial Gap 2018/19 £000
2019/20 £000
2020/21 £000
2021/22 £000
2022/23 £000
CCG 21,877 21,036 21,232 21,232Council – Social Care & Population Health
12,131 12,944 17,926 18,251
Strategic Commissioner 34,008 33,980 39,158 39,483ICFT 29,500 28,666 31,655 31,349Health; Social Care & Population Health Gap
63,508 62,646 70,813 70,833
ICFT TEP savings required
Other Council Services Savings 5,115 7,477 14,820 18,717

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 36 of 64
Strategic Commissioning Total Gap 39,123 41,456 53,978 58,200
Total Commissioner & Provider Gap – assuming ICFT TEP achieved
68,623 70,122 85,633 89,549
Total Commissioner & Provider Gap – assuming ICFT TEP not achieved
77,123 78,224 91,799 93,756
6.2 Funding Regimes
Funding and accounting mechanisms vary between the Local Authorities and the NHS. The funding flows within the NHS are depicted below.
CCG’s purchase activity from hospitals and, in the main, pay for it using a set of nationally set tariffs. As such funding follows the patients who receive the services free of charge. NHS Trusts are performance managed by NHSI, and are required to deliver against nationally set performance targets, and quality standards set by inspection regimes (Care Quality Commission – CQC). NHS Trusts account for income and expenditure on a gross basis.
Local Authorities receive their funding from four main sources; funding from central government, business rates, local council tax and fees and charges levied for Council Services. Councils which provide Social Care to Adults have been allowed to increase their share of Council tax by a maximum of an extra 6% between 2017/18 and 19/20, if it is all used to fund the increasing costs of Adult Social Care services. This is referred to as the ‘Adult Social Care precept’. The extent of total Council expenditure is dictated by the amount of income or funding received, as the Council has to balance income and expenditure on an annual basis. They cannot have a deficit, as such if income falls for any reason the Council has to cut back on its planned levels of expenditure. As such the Council has to align its limited resources with key Council priorities, which are influenced by local priorities, input from public consultation, consultation with local businesses, Government
Department of Health
NHS England
Clinical Commissioning Groups
NHS Trusts

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 37 of 64
policies, performance information and external inspections. Councils are able to charge for Adult Social Services, based upon means testing, in accordance with the Care Act 2014. Councils report income and expenditure on a net basis, and also operate under different sections of the VAT Act to the NHS.
TMBC spends its money on the services depicted below.
0
20
40
60
80
100
120
140
Council Planned Net Spend (£m) 2018/19
It is only elements of Adult services that would be integrated into the ICFT in the first instance, and TMBC would continue to collect any client charges.
6.3 Section 75 Agreement
The funding for Adult Social Care services is held within the integrated Commissioning Fund (ICF) which is a pooled arrangement between the CCG and TMBC. Within the Tameside and Glossop ICF there are three pooling mechanisms; a section 75 pooling arrangement, ‘aligned’ funds, and ‘in collaboration’ funds. It is anticipated that the Adult Social Care transfer will be funded from the section 75 element of the ICF but there may be a small minority of services which may be funded from the ‘aligned’ funds due to the limitation of the section 75 legislation. This will be fully identified prior to the transaction being undertaken. The ICFT contract is funded from the ICF in which it is proposed that this Adult Social Care transfer will be included.
The transfer of this sub-section of adult Social Care services to the ICFT will be funded from the local authority contributions into the ICF. The ICF is underpinned by a robust Financial Framework which incorporates a mechanism for sharing financial risk between the two Strategic Commissioners and this will be separate from the risk share arrangement proposed for Adult Social Care between the Strategic Commission and the ICFT. This flow of funds in

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 38 of 64
respect of the transferred services will be managed, monitored, and reported in line with the governance set out within the ICF’s Financial Framework.
The risk share arrangement between the Strategic Commission and the ICFT is proposed in section 6.4 below.
6.4 Financial Risk ManagementTo ensure greater confidence in the ongoing sustainability of both the ICFT and the provision of ASC services, there will need to be a risk sharing agreement with TMBC that guarantees the ICFT will not endure a further deficit on it in the first three years of implementation (starting in 19/20); additionally there will need to be detailed plans that identify how and when benefits can be released which will make the service more financially sustainable.
The following Risk Sharing Agreement has been proposed:
Financial Year FY 19/20 FY 20/21 FY 21/22 FY 22/23 FY 23/24
TMBC contribution to funding shortfall
100% 100% 100% 50% 25%
Funding would commence from the point of implementation in the Finance Year 19/20 and cover the remainder of that year. As part of the risk share agreement it will be necessary to identify any proposed caps on the risk share taking account of the projected activity risks.
6.5 Benefits Realisation
6.6 Financial Option Appraisal
The tables below detail the finances associated with each of the three options proposed. In all cases it is the intention to transfer the gross expenditure budgets for the services, and TMBC will continue to recover and retain all client chargeable income. The detail supporting the expenditure budgets can be found in Appendix D.
It should be noted that at this time the figures reflected in the tables below have been provided by TMBC, and as yet there has been no agreement as to the methodology proposed to determine the allocation of the Adult Social Care financial gap down to the sub-set of transferring services. As such the financial gap could reduce pending discussions between now and production of the full business case.
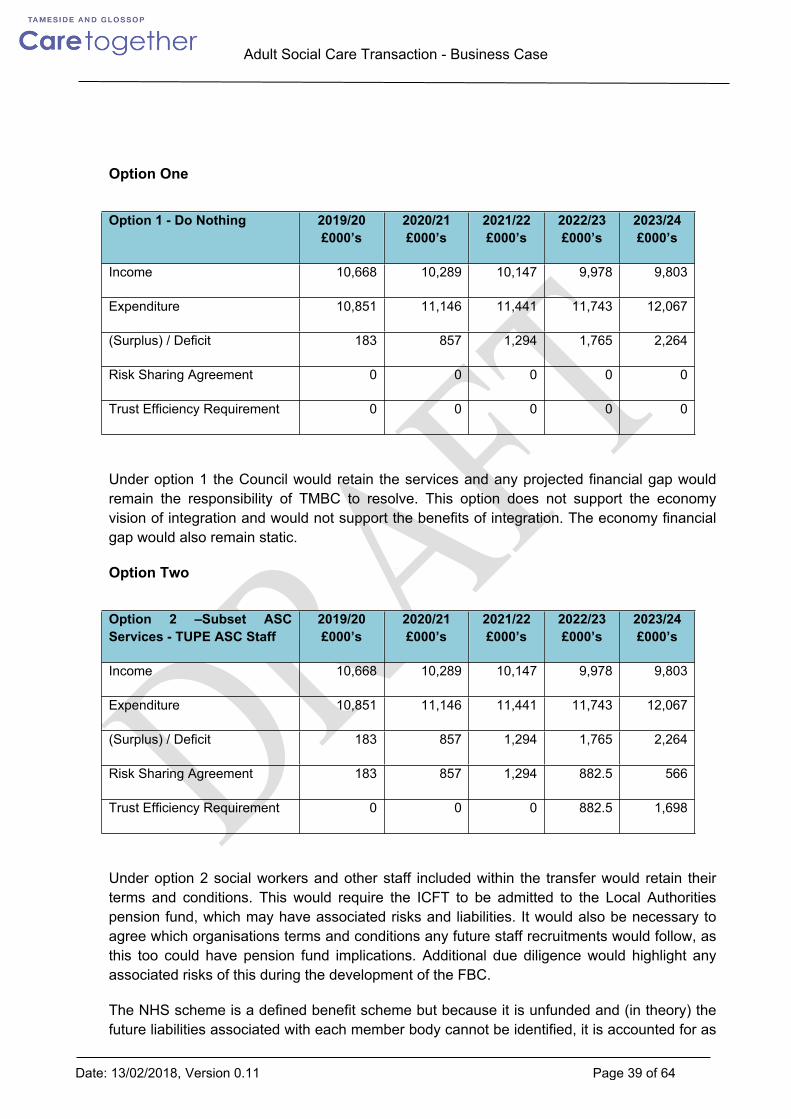
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 39 of 64
Option One
Option 1 - Do Nothing 2019/20 £000’s
2020/21 £000’s
2021/22 £000’s
2022/23 £000’s
2023/24 £000’s
Income 10,668 10,289 10,147 9,978 9,803
Expenditure 10,851 11,146 11,441 11,743 12,067
(Surplus) / Deficit 183 857 1,294 1,765 2,264
Risk Sharing Agreement 0 0 0 0 0
Trust Efficiency Requirement 0 0 0 0 0
Under option 1 the Council would retain the services and any projected financial gap would remain the responsibility of TMBC to resolve. This option does not support the economy vision of integration and would not support the benefits of integration. The economy financial gap would also remain static.
Option Two
Option 2 –Subset ASC Services - TUPE ASC Staff
2019/20 £000’s
2020/21 £000’s
2021/22 £000’s
2022/23 £000’s
2023/24 £000’s
Income 10,668 10,289 10,147 9,978 9,803
Expenditure 10,851 11,146 11,441 11,743 12,067
(Surplus) / Deficit 183 857 1,294 1,765 2,264
Risk Sharing Agreement 183 857 1,294 882.5 566
Trust Efficiency Requirement 0 0 0 882.5 1,698
Under option 2 social workers and other staff included within the transfer would retain their terms and conditions. This would require the ICFT to be admitted to the Local Authorities pension fund, which may have associated risks and liabilities. It would also be necessary to agree which organisations terms and conditions any future staff recruitments would follow, as this too could have pension fund implications. Additional due diligence would highlight any associated risks of this during the development of the FBC.
The NHS scheme is a defined benefit scheme but because it is unfunded and (in theory) the future liabilities associated with each member body cannot be identified, it is accounted for as
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 40 of 64
if it were a defined contribution scheme, with employer pension costs being charged to expenditure as and when they become due. Effectively the only cost in the Trust’s accounts will be the employer contributions payable for the financial year in question.
The Local Authority pension scheme charges the discounted present value of future benefits to expenditure each year, but then reverse this out through the statutory override so the charge to expenditure is just the employer cost in year. The Local Authority also reflect the future liabilities and share of the fund assets on their balance sheet (the NHS doesn’t recognise anything on the balance sheet). This means that Local Authorities have a charge to expenditure that is generally greater than the actual cash cost in year, and depending on the valuation point, generally a significant net pensions liability on the balance sheet. The ICFT needs to understand how if they are admitted to the Local Authority pension fund they will be required to account for these pensions and its potential impact on the charges to expenditure being in excess of the budgets transferred, and any impact of the Trust’s balance sheet.
The Local Authorities also maintain a reserve in relation to any future shortfalls in the local authority pension scheme. The ICFT would need to understand if this would be a requirement for the ICFT, or if TMBC would retain this in relation to the staff transferred.
If staff are TUPE across to the ICFT, this will result in staff being employed within the ICFT on differing terms and conditions. Any potential integration of staff onto NHS terms and conditions could increase the costs to the system, as the two organisations have differing staff and employer pension contributions and differing levels of sickness pay. The impact of any such proposal would need to be financially assessed to determine the impact on the economy and staff.
If staff are transferred this will result in staff following the same organisational policies and procedures, and will help to develop a single cultural and organisational identity. I should also support the streamlining of management processes and ensure equity. It should also enable the reduction in duplication of processes, allowing more time for direct care.
The transfer of staff to the ICFT would also potentially impact adversely on TMBC in relation to their Civil Contingency duties. Currently all staff employed by TMBC can be called on to support any local civil contingency. If the staff are TUPE, TMBC would lose this potential resource, unless this was covered within any future contract arrangements. If not it could have a potential cost to TMBC.
The transfer of staff has the potential to impact on adherence to the Care Act in that pressures within the ICFT could result in social workers priorities being shifted to the hospital which may impact on the delivery of TMBC’s statutory responsibilities such as re-assessments being undertaken within twelve months, or safeguarding duties being completed within the set timescales.
Both options two and three, by the nature of only a sub-set of adult social care services transferring, have the potential to risk management fragmentation, as current service managers will support or manage both ASC services transferred and ASC services retained by TMBC. This will need to be resolved as part of the management and back office support discussions which will be resolved as part of the FBC.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 41 of 64
Another potential risk which applies to both options two and three, is the fact that the staff which would form part of this transfer will be commissioning services against budgets and contracts retained by TMBC such as residential home placements, nursing homes, and home care, and as such these costs could increase due to differing management priorities. This could result in cost shunting between organisations, but this could be resolved as part of the future financial principles and risk share arrangements.
Option Three
Option 3 – Subset ASC services - Seconded ASC Staff
2019/20 £000’s
2020/21 £000’s
2021/22 £000’s
2022/23 £000’s
2023/24 £000’s
Income 10,668 10,289 10,147 9,978 9,803
Expenditure 10,851 11,146 11,441 11,743 12,067
(Surplus) / Deficit 183 857 1,294 1,765 2,264
Risk Sharing Agreement 183 857 1,294 882.5 566
Trust Efficiency Requirement 0 0 0 882.5 1,698
Under option 3 staff would remain employed and paid by TMBC, but would be seconded to the ICFT who would then pay TMBC for the staff. This would negate any pension fund issues, but could potentially have VAT issues, although initial VAT advice is that this would be recoverable by the ICFT. As part of stage two due diligence any VAT issues would need to be further explored, and resolved such there are no increases in costs to the economy of this option. If VAT were to be an issue in respect of this option it could increase costs across the economy by circa £2m.
The secondment option arrangement is easier to withdraw from if the ‘proof of concept’ does not materialise. If the ‘proof of concept’ does work this would support future TUPE of staff and the future transfer of further services.
Secondment of staff may not support the creation of an organisational identity, as staff will be on differing terms and conditions, which could not be changed if staff were seconded. It also could make transformation of services more difficult if any staff related proposals have to go through governance at both the ICFT and TMBC. If staff are seconded it would be necessary to clarify whose policies and procedures they would follow, which could result in a team manager having to follow differing policies and procedures for different staff in their team.
This option may also make it more difficult to re-align budgets and services in the future as part of the integration and transformation process.
Both options two and three have the same financial impact on the ICFT, subject to further due diligence work at FBC.
The tapering risk share agreement would mean that the ICFT would need to find integration benefits starting in 2022/23 of 7.5% of Adult Social Care expenditure, rising to 14%

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 42 of 64
cumulatively in 2023/24. This level of benefits exceeds that normally expected and delivered within the NHS, and is the same for both options two and three.
6.7 Financial Principles
As part of any transaction the partners would need to agree some financial principles such as:-
- Financial transparency and co-operation between organisations.
- Fair and proportionate transfer of resources to support back office functions, while maintaining services at no additional costs where ever possible.
- No transfer of historic liabilities these will be retained by the transferring organisation
- No increase in service requirements either in terms of activity levels, or specification without agreement of all parties.
- No in year reductions in funding without prior agreement, and agreement to corresponding reductions or efficiencies in service provision.
- Any national changes to terms and conditions over and above those in the financial modelling to be funded by the Single Commissioners.
- No cost shunting between partners in the economy unless fully discussed and agreed as it reduces the economy financial gap.
6.8 Sensitivity AnalysisFull sensitivity analysis will be completed as part of the full business case.
7.0 Commercial Case
7.1 Commissioners’ Procurement StrategyThe Contingency Planning Team report of 2015 (the Monitor-sponsored review by PwC) proposed the creation of an Integrated Care Organisation as the best opportunity for the locality to deliver the most significant improvements to the health and outcomes of our population.
The Strategic Commission is, therefore, convinced that the best way to achieve our vision and to deliver our priorities is by delivering via the ICO a new service model of which adult social care is a key component. It is therefore critical that the procurement strategy facilitates the development of the ICO and enables it to deliver a system of care that effectively responds to and impacts on population health outcomes whilst reducing costs.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 43 of 64
It is therefore the intention of the Strategic Commission to transfer this subset of Adult Social Care services to Tameside and Glossop Integrated Care NHS Foundation Trust. This approach has been formed through discussions with a colleague at NHS Improvement.
7.2. Due Diligence Summary
The ICFT and the Strategic Commissioners agreed to undertake due diligence in two phases. The first phase has been undertaken to support the completion of the OBC, and was commissioned on behalf of all parties. This work was undertaken by Hempsons. The second phase of due diligence will be required to support the FBC and will require the parties to the agreement to seek independent due diligence to provide the required assurance to the parties Boards.
The creation of a fully integrated Health and Social Care system is a complex undertaking that carries significant risks potentially to both TMBC who retain the statutory responsibility, and to the ICFT in terms of financial and delivery risks. As such the economy engaged Hempsons, as legal advisors in July 2017 to undertake due diligence into the integration of Adult social Care and some Commissioning functions. Hempsons were engaged to act on behalf of all partners to identify any areas of risk in expanding the ICFT services.
Due diligence has been identified as the basis of identifying both the risks and the available mitigation of those risks in expanding the ICFT. Formal due diligence will need to be performed to cover: Legal Financial Operational Quality
At the current time the first stage of external due diligence has only been undertaken by Hempsons in respect of legal issues, as it was assessed as being the areas with the highest areas of risk. The first stages of due diligence for the other areas has been undertaken internally for the first stage. At the FBC stage the ICFT will undertake formal external due diligence on the proposed option as the receiving organisation, which will comprise of legal, financial and operational due diligence.
7.2.1 Hempsons Due Diligence Report
Hempsons were engaged by the partner organisations in May 2017 and provided their findings in July 2017. Hempsons were engaged to cover the following areas:- Corporate, commercial, governance and contracts Employment and pensions Estates and Equipment Health and Safety / Environmental
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 44 of 64
IM&T and intellectual property Disputes, clinical governance and indemnity Information governance
Hempsons review process aimed to highlight the main areas of risk including those requiring the need for greater clarity. As such the following areas were covered.
System wide governance and accountability arrangements, including statutorypowers of TMBC to transfer ASC and SCT functions to TGICFT, and the role ofTMBC following completion of the arrangements
Commissioned contracts with third parties, assuming these will transfer toTGICFT
Procurement law compliance by TMBC and TGCCG as commissioners, and byTGICFT in respect of commissioned contracts with third parties
Governance issues including role of Boards of Directors and Council of Governors Regulatory issues including NHS Improvement compliance requirements for
transactions and the ISAP process, and CQC requirements Pensions liabilities in relation to TMBC staff transferring to TGICFT TUPE implications including employment liabilities of transferring staff Estates implications where there will be a change of use of existing estate IM&T implications where partners intend to integrate IM&T systems Disputes/claims – existing material disputes, civil and criminal claims of the partners
and regulatory concerns (with CQC, NHS Improvement, Information Commissioners’Office, Health and Safety Executive)
Indemnity arrangements for transferring services.
The final report was based on information provided by the three partner organisations and can be found within Appendix E. The report highlights the risks and recommends actions / mitigations that should be instigated. It should be noted that the report was produced to reflect the SOC longlist option two, where all Adult Social Services and an element of Commissioning functions would transfer.
7.2.2 Hempsons Phase One – Key Findings Report
Hempsons first phase due diligence report for inclusion within the OBC was produced based on information received from the partner organisations. The due diligence questionnaire is attached at Appendix C along with the full final report.
The key findings of the report were:- There are no legal showstoppers which will prevent the transfer of functions/services
and the award of contract.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 45 of 64
There are a number of legal, commercial and practical steps that need to be undertaken to allow the proposed transfer to happen.
There are some material risks of which 7 are red risks and 29 amber for which actions and mitigations have been identified.
Most risks affect the ICFT, as the organisation which will acquire responsibility to Commissioners for the services.
All risks can be rated ‘green’ or in a few cases ‘amber’ following the next stage of the project if actions and mitigations are followed.
Recommended that partners carry out further due diligence on the matters identified and implement suggested actions and mitigations.
7.2.3 Partnership Response
As part of the ongoing partnership working each risk has been allocated to an individual or working group to address. The output should then support the stage two formal due diligence in order to mitigate the red and amber rated risks.
7.3 Contractual Arrangements
7.3.1 Statutory Responsibility
Tameside Metropolitan Borough Council will continue to retain legal responsibility for the provision of all Adult Social Care services. For the subset of services transferring under this Outline Business Case the local authority is choosing to discharge this responsibility through the ICFT as the provider.
The Council is required to appoint a Director of Adult Social Services under section 6 of the Local Authority Social Services Act 1970 (as amended) who is accountable for the delivery of TMBC’s social services functions (except those the responsibility of the Director of Children’s Services) listed in Schedule 1 of the Local Authority Social Services Act 1970 (as amended). The Director of Adult Social Services is directly accountable to the Chief Executive of the Council, appointed by the Council to a politically restricted Statutory Chief Officer post under section 2 of the Local Government Act 1989 (as amended), and from where they are required to deliver a key leadership role on behalf of the Council. This is not a role capable of novation or delegation to another organisation. It must remain part of the statutory chief officer team employed by the Council.
The position of Director of Adult Social Services is a leadership role to deliver the local authority’s part in:
- improving preventative services and delivering earlier intervention- managing the necessary cultural change to give people greater choice and control over services- tackling inequalities and improving access to services- increasing support for people with the highest levels of need.
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 46 of 64
One of the key aspects of the Director of Adult Social Services role is to deliver an integrated ‘whole systems’ approach to supporting communities. This is at the very heart of our locality’s approach to neighbourhood working and for bringing together and transforming services.
The Director of Adult Social Services will seek assurances from the ICFT regarding the quality and timeliness of service delivery, regarding the application of the agreed eligibility criteria, and for the arrangements for the safeguarding of vulnerable adults. It is expected that these will be monitored through the existing contract review meetings.
TMBC will maintain the legal obligation to fulfil these services but will enter a contractual arrangement with the ICFT to be the provider.
7.3.2 Contract Form
The NHSE Contracting Team has verbally advised the ICFT that the standard NHS contract, as currently used by the Trust in its contract with the Single Commissioning Function, may not be the most suitable contract form in which to incorporate the provision of ASC. Instead, the NHS Standard Contract for Accountable Care Organisations (ACO) may be more appropriate.
The ICFT has raised a series of additional queries with the NHSE Contracts team. Without pre-empting any subsequent advice there is likelihood that the ICFT will continue to use the NHS standard form contract and adapt this to include the provision of ASC; this is for several reasons including:
the model contract for Accountable Care Organisations is still not finalised and appears to be essentially for the provision of primary medical services with the addition of selected local authority services such as social care and/or public health
At least one other GM NHS acute provider that also provides social care has continued to use the standard form contract without any issues
The vast majority of the ICFT’s income will continue to relate to the provision of acute and community healthcare
Regardless of the type of contract, any agreement will have a defined lifespan with the usual exit clauses which will be identified during the project process. Additionally, the provision of ASC will be fully specified in the contract, including the performance and quality requirements necessary to ensure that TMBC meets its legal obligations.
Required ServicesThe exact list of services that need to be performed, the volume and associated Service Level Agreements along with associated costs will be detailed in greater depth within any Full Business Case and later contractual documentation that will be agreed by the three partner organisations.
7.3.3 Risk Mitigation
This NHS contract will also include a risk sharing agreement which will ensure that TMBC is responsible for funding shortfalls within the first three years of the ICFT operating the ASC

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 47 of 64
services starting 19/20 and a decreasing percentage after the initial three years. The percentage available to the ICFT is covered in the table in Section 6.4.
The risk mitigation strategy outlined in section 6.4 may need to be reconsidered if the final arrangements for the TMBC ASC staff affected by the transfer changes the balance of risk. For example, if TMBC retains the employment of ASC staff, and their services are provided to the ICFT under a service level agreement or secondment arrangement then it this potentially creates a conflict as the ICFT:
takes on increasing responsibility for any funding shortfalls from TMBC, and is dependent on TMBC for the supply of staff
In other words TMBC would have control over both the ICFT’s ASC income and costs potentially creating a significant financial risk
7.3.4 Risk TransferThe approach to risk transfer will be based on the best practice principle of allocating risk to the party, or parties, best placed to manage that risk. Therefore, an optimum allocation of risk rather than a maximum risk transfer will be taken.
The risk sharing agreement (which protects the ICFT from undue financial hardship until it can start to realise benefits) will be defined and agreed during the project process. After this TMBC will not cover any funding shortfalls as the ICFT will have had the opportunity to transform the service in a manner that releases savings.
Risks associated with the delivery of the solution (i.e. post contract award) will be maintained in a jointly held risk register with clear assignment to the responsible party.
Hempsons have provided an initial review of the legal feasibility and likely risks involved in this transfer. These issues are being captured within the Project Risk Register and will be documented in greater detail in the Project Initiation Document (PID).
8. Management Case
8.1 Introduction
This section addresses how the expansion of services within the ICO sits within the broader transformation programme within the ICFT. The integration transaction in its own right will not deliver financial or operational benefits. It will be the subsequent ability to integrate and transform services to provide a more streamlined end to end service that will provide efficiencies and a better patient experience.
To support the integration vision the Locality partners bid for and were successful in securing £23.2m of non-recurrent transformation monies from Greater Manchester Health and Social Care Partnership over a three year period from 2016. This funding will be used to transform services to better support people in their own homes, reducing the likelihood of hospital attendance and admissions, and to ensure that people are as well supported as possible to live healthy and independent lives.

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 48 of 64
All of the schemes aim to change behaviours or services within the Tameside & Glossop health and social care system, to contribute to delivery of the proposed system benefits, and impact on the successful delivery of the locality ambitions of financial sustainability and healthy life expectancy. The integration of Adult Social Care supports this ambition as reflected in the ICFT strategy as detailed in section 3.5. The aim is to fully integrate Social Service staff into the developing Neighbourhood structure which is aimed at reducing secondary care activity, and integrate them into the Hospital structure to support effective patient discharge.
8.2 Integration PrinciplesFurther work required (Stephanie, Sandra W, Trish, Suzanne to discuss)
- E.g. secure vfm for the economy- Transparency- Co-operation and commitment

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 49 of 64
- Effective integrated working between the partners- Positive health and social care outcomes- Positive communication, integration and engagement of Social Care staff
8.3 Management StructureThe operational structure would require to be reviewed in order to ensure that this transaction resulted in integration of services rather than the development of a silo within the ICFT in which social care operates. This was the approach adopted with the transfer of community services in April 2016 and there are benefits in replicating this. It should be noted that the transfer of services from one health provider to another, in which expertise in the receiving organisation already exists, differs from the transfer of functions from social care to a health care provider who is inexperienced in this. The statutory responsibility of the DASS also requires consideration in this context.
It is envisaged that a senior management team with the capability to operationally lead the delivery of services and contribute to the on-going transformational work would be required to supplement the existing management structure within the ICFT. It is proposed that this team would sit alongside the existing operational teams reporting to the Executive Director of Operations. In the first instance it is unlikely that structures within services which are already integrated would change significantly but rather that this would be an iterative process as the workforce model develops.
There would also need to be further support provided by corporate services e.g IM&T, finance, human resources, Governance to support the expanded functions of operations.
8.4 Organisational DevelopmentThe workforce within the locality has been working collaboratively for a number of years in order to transform the delivery of health and social care services to enable improvement and seamless services to our residents.
Whole workforce engagement, including trade union colleagues has been undertaken to raise awareness of our transformation plans and to ensure that all colleagues are sighted on our vision and priorities and how they will contribute to this.
A detailed development programme has been commissioned and delivered by Rothwell Douglas. The focus of this has enabled us to drive forward our vision and transformation plans:
strategic leadership and management whole workforce engagement neighbourhood and localities.
Neighbourhood teams are already co-located with colleagues from the Council and ICFT and plans are in place for this to be further developed to include primary care, voluntary sector and other wider public services.
To further support workforce transformation, a detailed workforce plan has been developed and dedicated resource put in place to ensure that the transformation is delivered. It is envisaged that the transaction of the Council workforce to the ICFT will provide significant

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 50 of 64
opportunities to accelerate transformation and new ways of working. Such benefits may include:
ability for colleagues in NHS/Council to work even more closely together to reduce duplication
develop improved ways of working enhance health and social care roles and to ensure improved outcomes for our
residents are achieved colleagues are better equipped, able and expected to work and operate on a whole
system approach improve understanding of whole system and enable priority and resource to be
directed to areas of greatest transformation/improvement support and develop improved working/collaboration with primary care and voluntary
sector enable improved career pathways to health and social care roles – improving
recruitment and retention etc. improved user experience as workforce are better connected with our priorities and
able to navigate the system better.
8.5 Governance ArrangementsGovernance arrangements will be further developed as part of the full business case but will be required to cover arrangements at the ICFT, and how it sits within the economy wider governance structure, and continues to fulfil Statutory organisational requirements.
8.6 Project Management ArrangementsThe SRO for the project is the Director of Adult Social Services at TMBC, whilst within the ICFT the Executive Lead for the project is the Director of Operations supported by the Executive management team, with the Director of Finance being the Executive lead for the transaction. The size and complexity of the project warrants significant management resource and oversight. The overall progress of the project will be overseen by the Care Together Programme Board.
The Care Together Programme Board will be collectively responsible for ensuring that:
the project is adequately resourced the project achieves its objectives that risks are well managed that partner organisations undertake their responsibility to identify and release
benefits the project is managed within budget, time and quality tolerances
8.7 Summary of Next Steps

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 51 of 64
To progress the OBC the economy partners would need to:-- Undertake individual phase two due diligence work to satisfy Boards/Cabinet as to
the benefits of the transaction- Develop formal staff communication and TUPE consultation with affected staff
(dependant on the preferred option)- Agree either staff transfers or develop SLA’s for back office functions, with
associated finances and KPI’s.- Identify any additional costs to the ICFT resulting from the transaction (e.g. IM&T)- Develop a long term strategic workforce plan- Develop service and contractual obligations and KPI’s- Develop heads of terms- Commence work on the Business transfer agreement- Produce a detailed integration plan
Work to be completed to take the OBC up to a FBC – all
9. Conclusion and recommendations
Appendix A
Strategic Outline Case Long List of Options
Service Area – Adult Social Care
Option 1
Option 2
Option 3 Option 4
Option 5
Option 6 Option 7
Option 8
TMBC Urgent Care

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 52 of 64
Service Unit Manager x √ √ √ √ √ √ √
Integrated Urgent Care staff and Management team x
√ √ √ √ √ √ √
ICES Service co-ordination staff member
x √ √ √ √ √ √ √
TMBC – LocalitiesAssessment / Care Co-ordination (18+) Inc Locality teams and management x √ √ √ √ √ √ √
Direct Payment Function – staff resource
x √ √ √ √ √ √ √
Review function in care homes – staff resource
x √ √ √ √ √ √ √
Health & wellbeing and Carers Service – staff resource x √ √ √ √ √ √ √
Occupational therapy / Manual Handling Team
x √ √ √ √ √ √ √
Home Care Commissioning Team
x √ √ √ √ √ √ √
Property Management Function – staff resource
x √
√ √ x x x x
TMBC Long Term SupportService Unit Manager x √ √ √ √ √ x x
Homemakers staff and management (24 hour Long term supported housing - LD) CQC Registered
x √ √ √ √ √ x x
LDS Support Clerks x √ √ √ √ √ x x
Shared Lives (Carer Approval, training & support) CQC Registered
x √ √ √√ √
x x
Learning Disability Day Services (including transport) x √ √ √
√ √x x
Reablement Service (CQC Registered) (Inc Homecare through the night)
x √ √ √ √ √ √ √
Through the Night Service (CQC Registered in reablement registration)
x √ √ √ √ √ √ √
Loxley House – Day service for people with physical disabilities / Development Trust
x √ √ √ √ √ x x
TMBC Crisis & ResponseService Unit Manager
x √ √ √ √ √ x xCommunity Response Service – warden/response element (Not Control/Operator function)
x √ √ √ √ √ √ √

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 53 of 64
Sensory Service – ( inc interpreting services) x √ √ √ √ √ √ √Out of Hours Social work function inc statutory MH duty
x √ √ √ √ √ x x
Mental Health Service - TMBC Provision (social workers in Pennine Care) CMHT
x √ √ √ √ √ x x
Opt-In Servicex √ √ √ √ √ x x
MCA and AMHP co-ordination inc Deprivation of Liberty Safeguards
x √ √ √ √ √ x x
TMBC ContractsAge UK Core Funding
x √ √ √ x x x xCommunity Support Service / Buddying (Age UK) x √ √ √ x x x xAdvocacy (Cloverleaf)
x √ √ √ x x x xIndividual Service Fund (Tameside Link) x √ √ √ x x x xMind Core Funding (Mind)
x √ √ √ x x x xWillow Wood Hospice
x √ √ √ x x x xIntegrated Community Equipment Service (Rosscare)
x √ √ √ x x x x
Minor Adaptations and Handy Person Service (Age Uk / NCHT)
x √ √ √ x x x x
Garden Maintenance and Daytime Support (Greenscape)
x √ √ √ x x x x
Home Care Pre-Placement "Framework" Contract (Comfort Call; Mears Group; MRL Healthcare; Allied)
x √ √ √ x x x x
Home Care Pre-Placement Approved list (Able Care; Direct Care; Person Centred Care; CRG; Laurel Bank + Others)
x √ √ √ x x x x
Mencapx √ √ √ x x x x
Older People Day Support - List of Approved Services x √ √ √ x x x xLearning Disability Day Support - List of Approved ServicesPhysical Disability Day Support - List of Approved Services
x √ √ √ x x x x
Mental Health Alternative Accommodation x √ √ √ x x x xMental Health Community Recovery Service (Turning Point)
x √ √ √ x x x x
Specialist Day Service for people with a Dementia (Creative Support - Wilshaw House)
x √ √ √ x x x x

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 54 of 64
Supported Accommodation for Adults with a Learning Disability (24 hour Support) (Alternative Futures Group)
x √ √ √ x x x x
Provision of short-term and respite care to people with a learning disability plus alternative respite (Community Integrated Care)
x √ √ √ x x x x
Supported Accommodation for people with Mental Health Needs (Bendix Court, Mottram Road, Lyne View) (Creative Support)
x √ √ √ x x x x
Support with Independent Living – Lomas Court (Alternative Futures Group)
x √ √ √ x x x x
Supported Accommodation for young adults with a learning disability (Alternative Futures Group)
x √ √ √ x x x x
IMCAx √ √ √ x x x x
Residential & Nursing Care Home “On Framework” Contract (26 Care homes)
x √ √ √ x x x x
Stroke Care Deliveryx √ √ √ x x x x
Senior Management TeamAssistant Director Adults
x √ √ √ √ √ √ √Head of Service - Operations
x √ √ √ √ √ x xHead of Service – Assessment and Care Management
x √ √ √ √ √ √ √
Back Office Functionsx √ √ √ √ √ √ √
Service Area – CCG Commissioned Services
Option 1
Option 2
Option 3 Option 4
Option 5
Option 6 Option 7
Option 8
Public Healthx √ x x x x x x
Prescribingx √ √ x x x x x
Primary Care - PCQS, OOH, central drugs, LES, home oxygen, GPIT, Broomwell
x √ x x x x x x
Urgent Primary Carex √ √ x x x x x
Individualised Commissioning – CHC etc x √ x x x x x x3rd Sector Grants & Services
x √ x x x x x xMental Health
x √ x x x x x xPatient Transport
x √ x x x x x x

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 55 of 64

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 56 of 64
Appendix B
Option Analysis of Gross Expenditure and Associated Funding Gap
Service Area – AdultSocial Care
Option 1 - Do Nothing
Option 2 - Full integration of all
Adult Social Care Services, and CCG
Commissioned Services.
Option 3 - Full integration of all
Adult Social Care Services, and a subset of CCG Commissioned
Services.
Option 4 - Full integration of all
Adult Social Care Services (including staff and funding).
Option 5 - Integration of in
house ASC delivered services from TMBC into the
ICFT through TUPE
arrangements
Option 6 - - Integration of in
house ASC delivered services from TMBC into the
ICFT with TMBC staff being
seconded into the ICFT
Option 7 - Integration of a
subset of in house ASC delivered services from TMBC into the ICFT, through
TUPE arrangements
Option 8 - : Integration of a
subset of in house ASC delivered services from TMBC into the
ICFT, as detailed in Appendix B, with
the LA staff seconded into the
ICFT.
Total Expenditure73,979 73,979 73,979 73,979 17,976 17,976 10,556 10,556
2023-24 Financial Gap relating to ASC transfer (£'000) 17,318 17,318 17,318 17,318 4,312 4,312 2,264 2,264Financial Gap as a % of Expenditure 23% 23% 23% 23% 24% 24% 21% 21%

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 57 of 64
Appendix C
Public Health Joint Needs Assessment
Summary of Tameside Joint Strategic Needs Analysis 2015/16
Key statistics for Tameside (compared to the England average);
Highest premature death rate for heart disease in England For premature deaths from heart disease and stroke, Tameside is ranked 148th out of 150
Local Authorities in England For overall premature deaths, Tameside is ranked 142nd out of 150 Local Authorities in
England (<75 years) For premature deaths from cancer, Tameside is ranked 133rd out of 150 Local Authorities in
England Life expectancy at birth for both males and females is lower than the England average (76.9
years males, 80.3 years females) Life expectancy locally is 8.7 years lower for men and 7.4 years lower for women in the most
deprived areas of Tameside compared to the least deprived areas. Healthy life expectancy at birth is currently 57.9 years for males in Tameside and 58.6 years for
females in Tameside. This is significantly lower than the England averages. In year 6, 33.3% of children are classified as being overweight or obese, under 18 alcohol
specific hospital admissions, breast feeding initiation and at 6 to 8 weeks and smoking in pregnancy are all worse than the England average.
In adults the recorded diabetes prevalence, excess weight and drug and alcohol misuse are significantly worse than the England average
Rates of smoking related deaths and hospital admissions for alcohol harm are significantly higher than the England average and many of our statistical neighbours
Life expectancy with Males in Tameside living 3 years less than the England average and nearly 7 years less than the England best.
Females live on average just over 2 years less than the England average and 6 years less than the England best.
Healthy life expectancy for women is nearly a year less than for men, and close to the worst in England.
Premature mortality for women has not improved as fast as the NW and England. Circulatory diseases including heart disease are the commonest cause of early death and rates
are 55% higher than the national average. Disability free life expectancy at 65 years is significantly worse than the England average (6.8
years compared to 10.2 years in England (males)) and 7.1 years compared to 10.9 years (females))
Nearly 20% of Tameside residents are living in fuel poverty compared to the 16% England average
Significantly higher emergency admissions for both males and females People returning to their own homes after a stroke is significantly worse than the England
average, 28% less people return to their own homes after a stroke compared to the England average.
Summary of Glossop Socio-economic status 2014
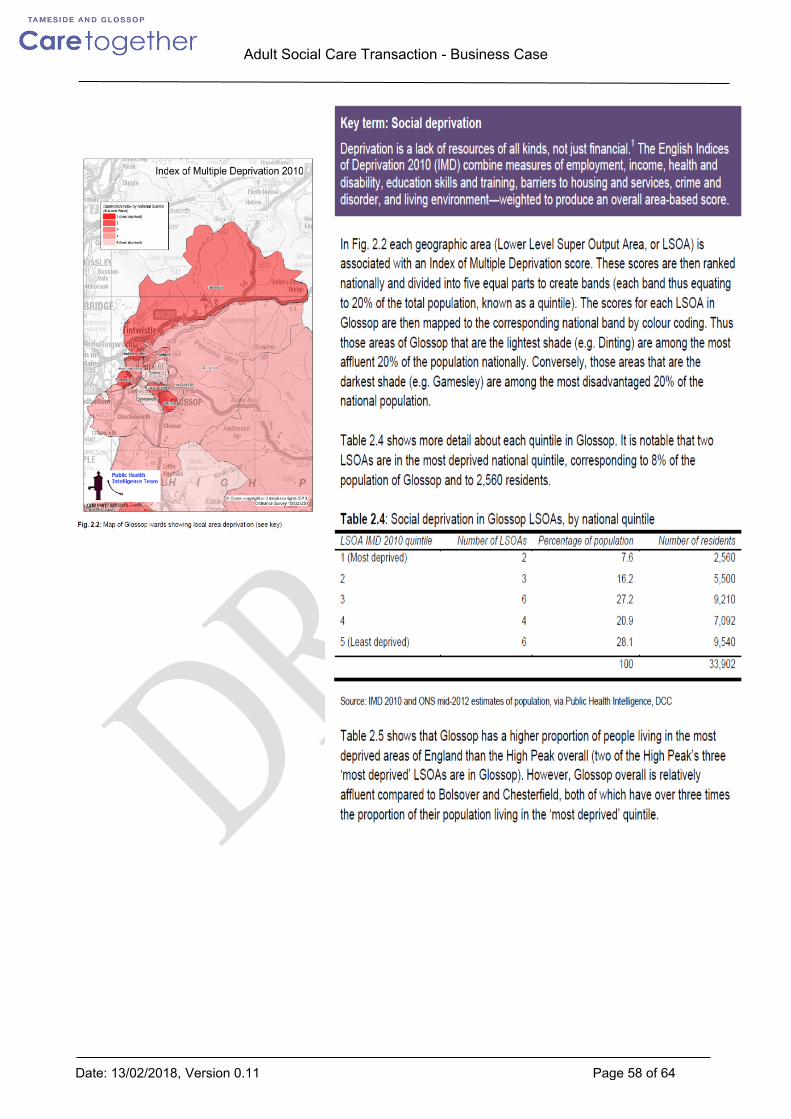
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 58 of 64

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 59 of 64
For the full report see; https://observatory.derbyshire.gov.uk/IAS/Custom/resources/HealthandWellbeing/Health_Needs_Assessments/Needs_and_assets_in_Glossop.pd
Appendix D
Adult Social Care Budget Analysis
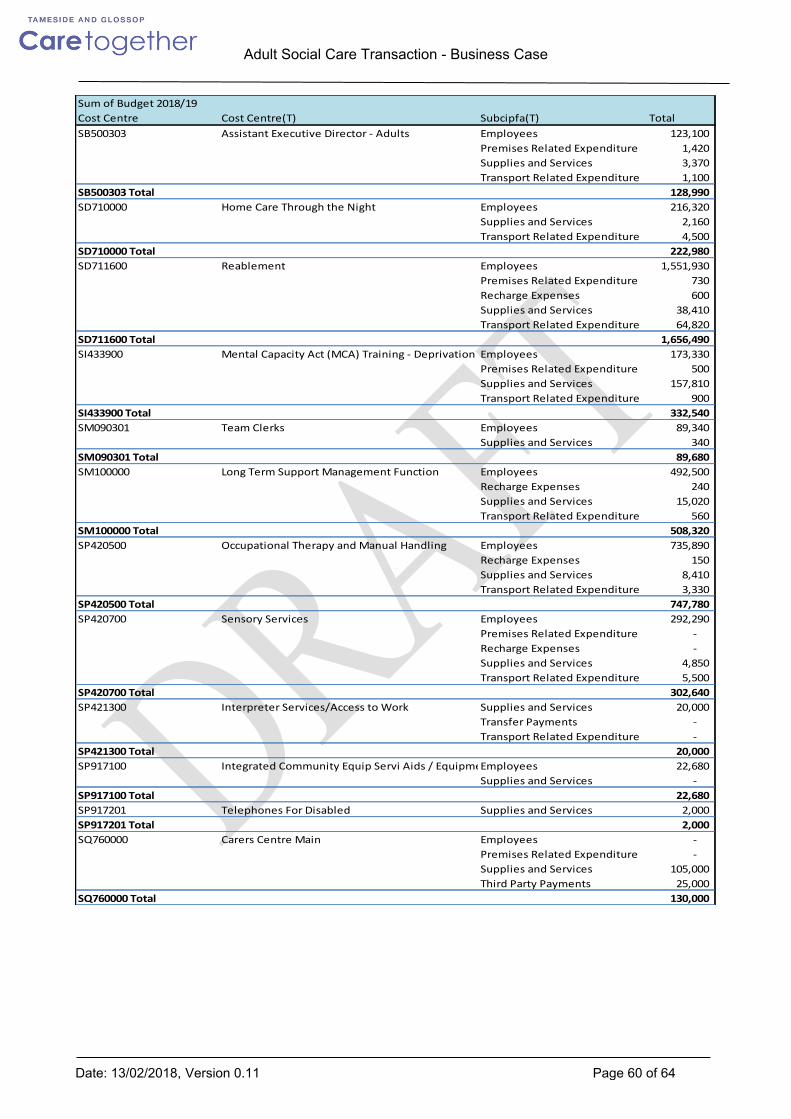
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 60 of 64
Sum of Budget 2018/19Cost Centre Cost Centre(T) Subcipfa(T) TotalSB500303 Assistant Executive Director - Adults Employees 123,100
Premises Related Expenditure 1,420Supplies and Services 3,370Transport Related Expenditure 1,100
SB500303 Total 128,990SD710000 Home Care Through the Night Employees 216,320
Supplies and Services 2,160Transport Related Expenditure 4,500
SD710000 Total 222,980SD711600 Reablement Employees 1,551,930
Premises Related Expenditure 730Recharge Expenses 600Supplies and Services 38,410Transport Related Expenditure 64,820
SD711600 Total 1,656,490SI433900 Mental Capacity Act (MCA) Training - Deprivation of Liberty Safeguards (DOLS)Employees 173,330
Premises Related Expenditure 500Supplies and Services 157,810Transport Related Expenditure 900
SI433900 Total 332,540SM090301 Team Clerks Employees 89,340
Supplies and Services 340SM090301 Total 89,680SM100000 Long Term Support Management Function Employees 492,500
Recharge Expenses 240Supplies and Services 15,020Transport Related Expenditure 560
SM100000 Total 508,320SP420500 Occupational Therapy and Manual Handling Employees 735,890
Recharge Expenses 150Supplies and Services 8,410Transport Related Expenditure 3,330
SP420500 Total 747,780SP420700 Sensory Services Employees 292,290
Premises Related Expenditure -Recharge Expenses -Supplies and Services 4,850Transport Related Expenditure 5,500
SP420700 Total 302,640SP421300 Interpreter Services/Access to Work Supplies and Services 20,000
Transfer Payments -Transport Related Expenditure -
SP421300 Total 20,000SP917100 Integrated Community Equip Servi Aids / EquipmentEmployees 22,680
Supplies and Services -SP917100 Total 22,680SP917201 Telephones For Disabled Supplies and Services 2,000SP917201 Total 2,000SQ760000 Carers Centre Main Employees -
Premises Related Expenditure -Supplies and Services 105,000Third Party Payments 25,000
SQ760000 Total 130,000

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 61 of 64
Appendix DSum of Budget 2018/19Cost Centre Cost Centre(T) Subcipfa(T) TotalSQ760200 Health and Wellbeing Staff Employees 215,870
Premises Related Expenditure -Recharge Expenses 300Supplies and Services 16,180Transport Related Expenditure 1,000
SQ760200 Total 233,350SW500300 HOS - Head of Transformation Employees 101,390
Recharge Expenses -Supplies and Services 45,310
SW500300 Total 146,700SW752000 Localities Management Function Employees 655,280
Premises Related Expenditure -Recharge Expenses 150Supplies and Services 3,220Transport Related Expenditure 500
SW752000 Total 659,150SW752300 Adult Social Care Locality Teams Employees 1,881,250
Premises Related Expenditure 3,000Recharge Expenses 1,000Supplies and Services 32,100Third Party Payments 123,680Transfer Payments -Transport Related Expenditure 18,050
SW752300 Total 2,059,080SW752500 Urgent Integrated Care Team Employees 1,623,140
Premises Related Expenditure 2,000Recharge Expenses -Supplies and Services 17,850Transfer Payments -Transport Related Expenditure 8,420
SW752500 Total 1,651,410SW752600 Urgent Intergrated Care Service Management TeamEmployees 308,890
Supplies and Services 1,800Transport Related Expenditure -
SW752600 Total 310,690SW752700 Reablement Operational Employees 502,510
Recharge Expenses 100Supplies and Services 4,770Transport Related Expenditure 2,900
SW752700 Total 510,280SW754200 Community Response and Emergency Control ServiceEmployees 821,250
Premises Related Expenditure -Recharge Expenses -Supplies and Services -Transport Related Expenditure -
SW754200 Total 821,250Grand Total 10,556,010
Appendix E
In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 62 of 64
Hempsons Legal Due Diligence Report – Stage One
TG DD Report FINAL.pdf
Hempsonsdocx-V1DD Questionaire.docx
DELETE
Finance case

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 63 of 64
Economy Financial Gap 2018/19 2019/20 2020/21 2021/22 £000 £000 £000 £000CCG 21,877 21,036 21,232 21,232Council - Social Care & Pop Health 12,131 12,944 17,926 18,251Strategic Commissioner 34,008 33,980 39,158 39,483ICFT 29,500 28,666 31,655 31,349Health & Social Care & Pop Health Gap 63,508 62,646 70,813 70,833
ICFT TEP savings required 8,500 8,102 6,166 4,207
Other Council Services Savings 5,115 7,477 14,820 18,717
Strategic Commissioning Total Gap 39,123 41,456 53,978 58,200
Total Gap Commissioner & Provider - assuming ICFT TEP achieved 68,623 70,122 85,633 89,549
Total Gap Commissioner & Provider - assuming ICFT TEP not achieved 77,123 78,224 91,799 93,756

In Progress
Adult Social Care Transaction - Business Case
Date: 13/02/2018, Version 0.11 Page 64 of 64
APPENDIX E: INDIVIDUAL SERVICE BENEFIT TEMPLATES