repercusiones de las diferencias entre las guías eas/esc y las acc/aha
TRANSCRIPT
LLUÍS MASANA
HOSPITAL UNIVERSITARI SANT JOAN
UNIVERSITAT ROVIRA i VIRGILI
CIBERDEM-IISPV
REUS
REPERCUSIONES PRÁCTICAS DE LAS DIFERENCIAS ENTRE LAS GUÍAS EAS/ESC Y LAS ACC/AHA

No se establecen recomendaciones a favor o en contra de objetivos de cLDL o cNO-HDL ni en prevención primaria ni secundaria
Las guías no establecen objetivos terapéuticos ni para LDL ni para cNO-HDL
Se cuestionan dos estrategias ampliamente implementadas en la práctica clínica al considerar que los estudios randomizados y controlados no se diseñaron para alcanzar distintos objetivos terapéuticos sino que, prácticamente todos, se realizaron con dosis fijas de estatinas:
“Treat to target” (Tratar hasta el objetivo)
“Lowest is best” (Como más bajo mejor)
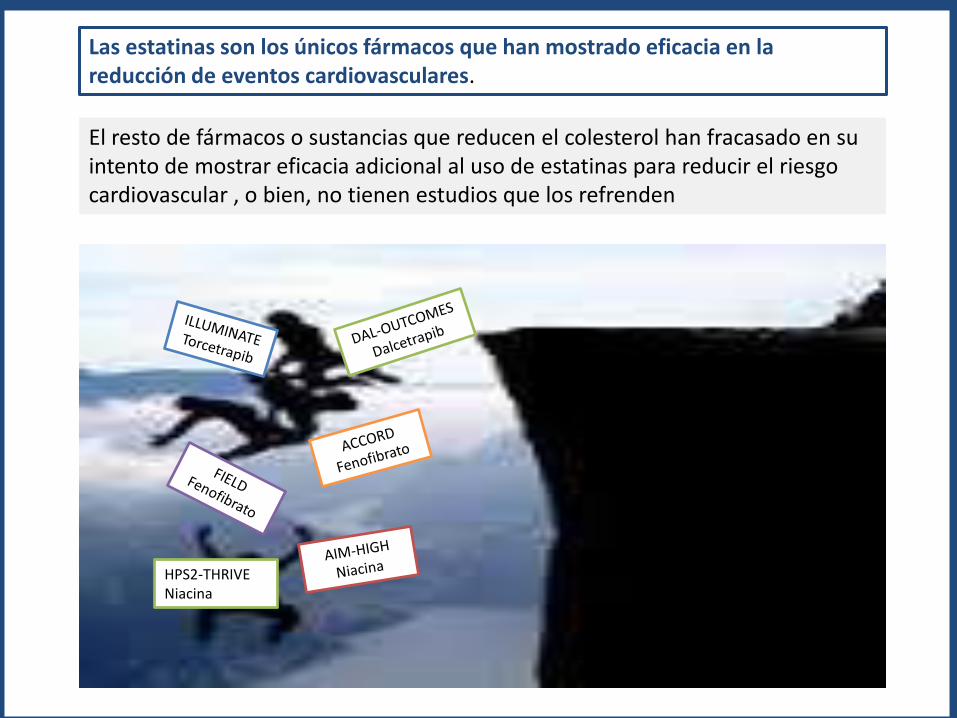
Las estatinas son los únicos fármacos que han mostrado eficacia en la reducción de eventos cardiovasculares.
El resto de fármacos o sustancias que reducen el colesterol han fracasado en su intento de mostrar eficacia adicional al uso de estatinas para reducir el riesgo cardiovascular , o bien, no tienen estudios que los refrenden
HPS2-THRIVENiacina
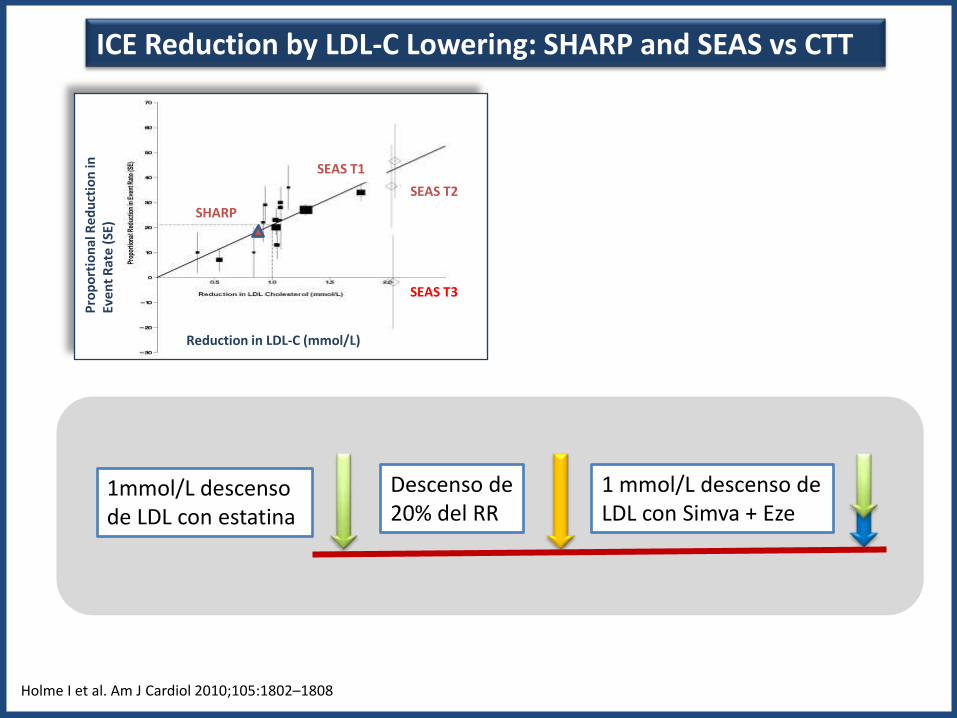
ICE Reduction by LDL-C Lowering: SHARP and SEAS vs CTT
Holme I et al. Am J Cardiol 2010;105:1802–1808
SEAS T1
SEAS T2
SEAS T3
Reduction in LDL-C (mmol/L)
Pro
po
rtio
nal
Re
du
ctio
n in
Ev
en
t R
ate
(SE)
SHARP
1mmol/L descensode LDL con estatina
Descenso de 20% del RR
1 mmol/L descenso de LDL con Simva + Eze
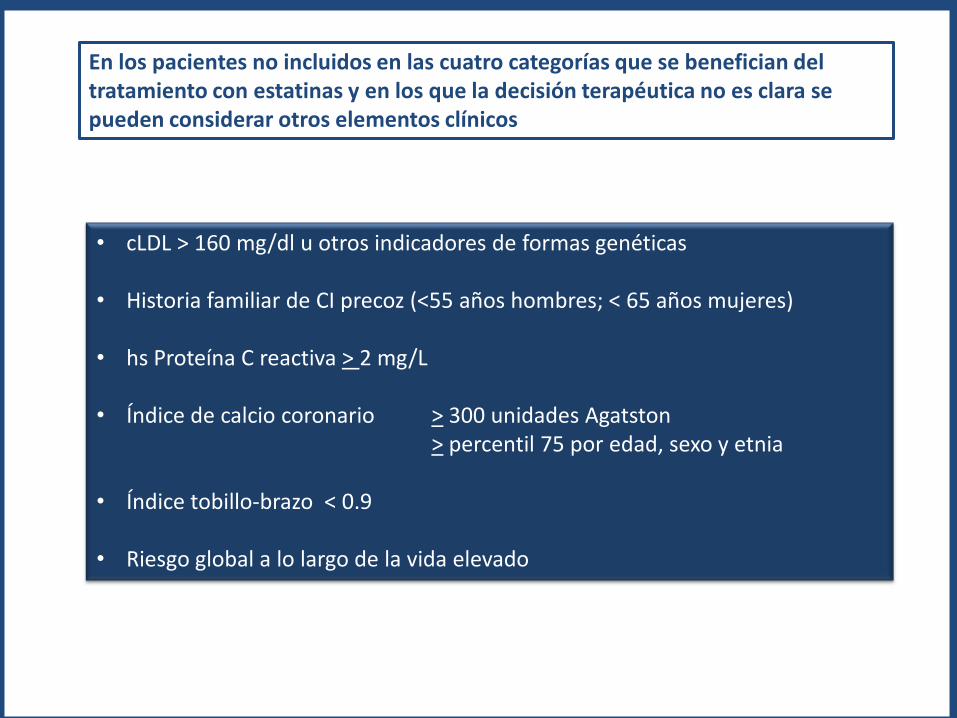
En los pacientes no incluidos en las cuatro categorías que se benefician del tratamiento con estatinas y en los que la decisión terapéutica no es clara se pueden considerar otros elementos clínicos
• cLDL > 160 mg/dl u otros indicadores de formas genéticas
• Historia familiar de CI precoz (<55 años hombres; < 65 años mujeres)
• hs Proteína C reactiva > 2 mg/L
• Índice de calcio coronario > 300 unidades Agatston> percentil 75 por edad, sexo y etnia
• Índice tobillo-brazo < 0.9
• Riesgo global a lo largo de la vida elevado

En pacientes con hipercolesterolemias primarias con cifras de cLDL > 190 mg/dl iniciar tratamiento con estatinas de alta intensidad
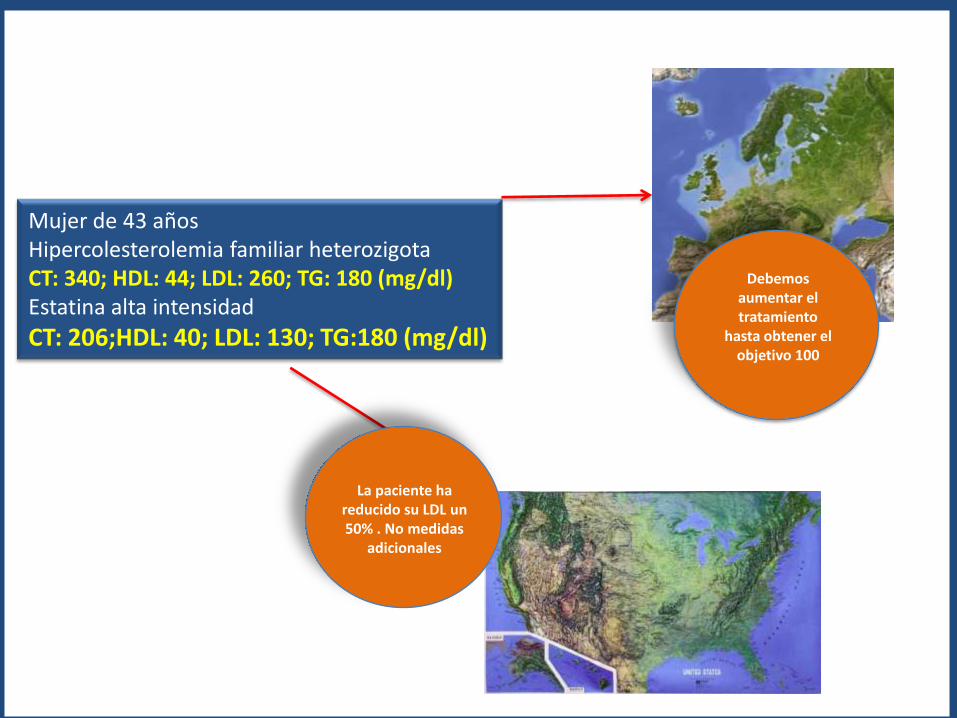
Mujer de 43 añosHipercolesterolemia familiar heterozigotaCT: 340; HDL: 44; LDL: 260; TG: 180 (mg/dl)Estatina alta intensidad
CT: 206;HDL: 40; LDL: 130; TG:180 (mg/dl)
Debemosaumentar el tratamiento
hasta obtener el objetivo 100
La paciente ha reducido su LDL un 50% . No medidas
adicionales
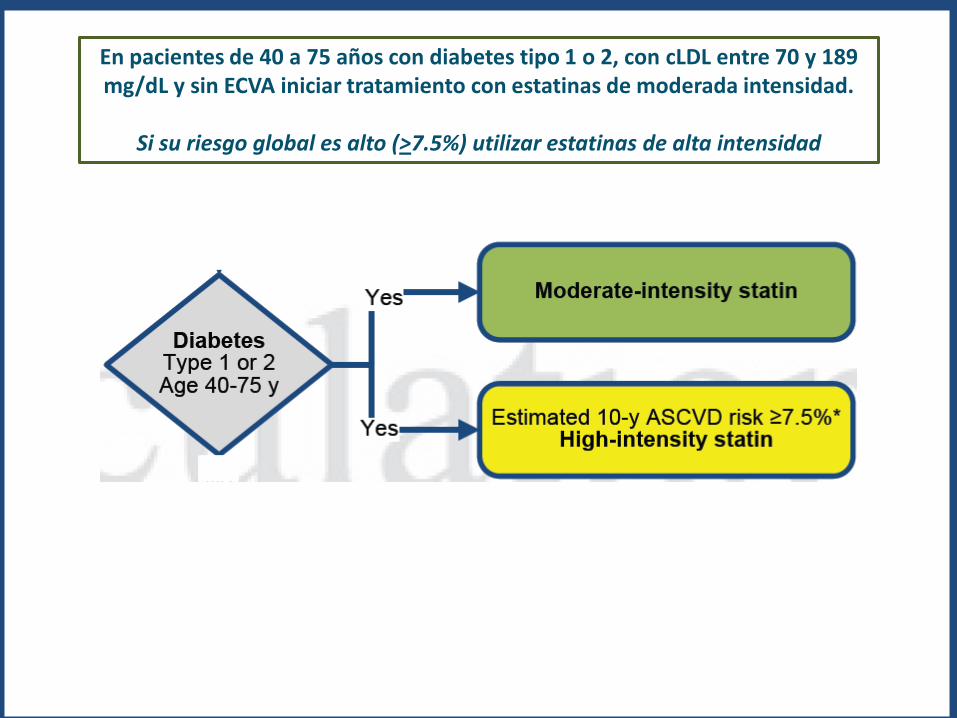
En pacientes de 40 a 75 años con diabetes tipo 1 o 2, con cLDL entre 70 y 189 mg/dL y sin ECVA iniciar tratamiento con estatinas de moderada intensidad.
Si su riesgo global es alto (>7.5%) utilizar estatinas de alta intensidad
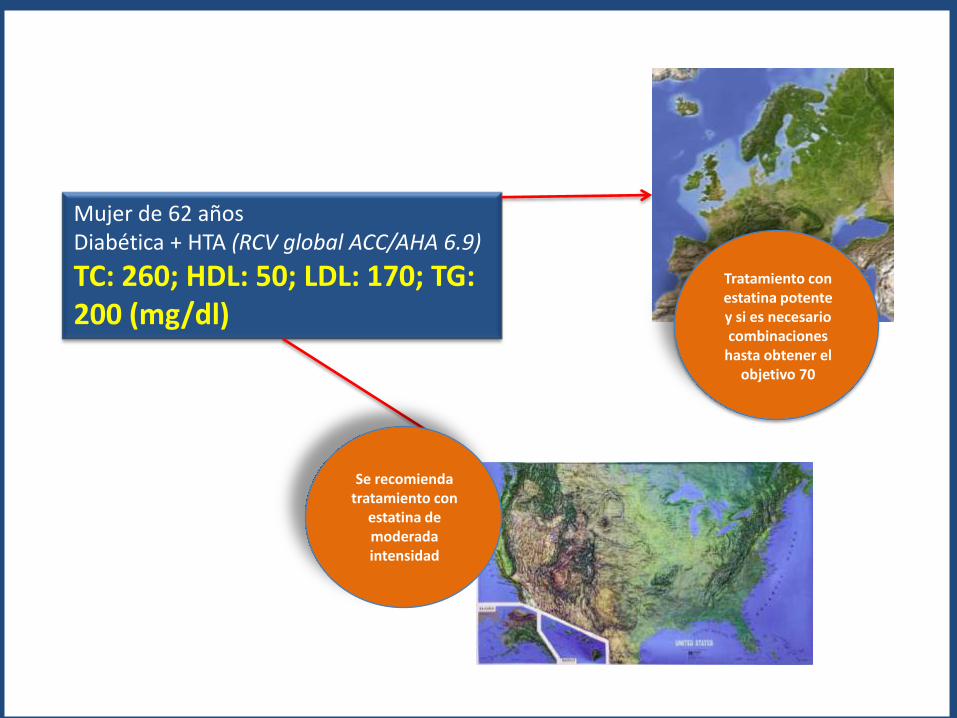
Mujer de 62 añosDiabética + HTA (RCV global ACC/AHA 6.9)
TC: 260; HDL: 50; LDL: 170; TG: 200 (mg/dl)
Tratamiento con estatina potentey si es necesariocombinaciones
hasta obtener el objetivo 70
Se recomiendatratamiento con
estatina de moderadaintensidad
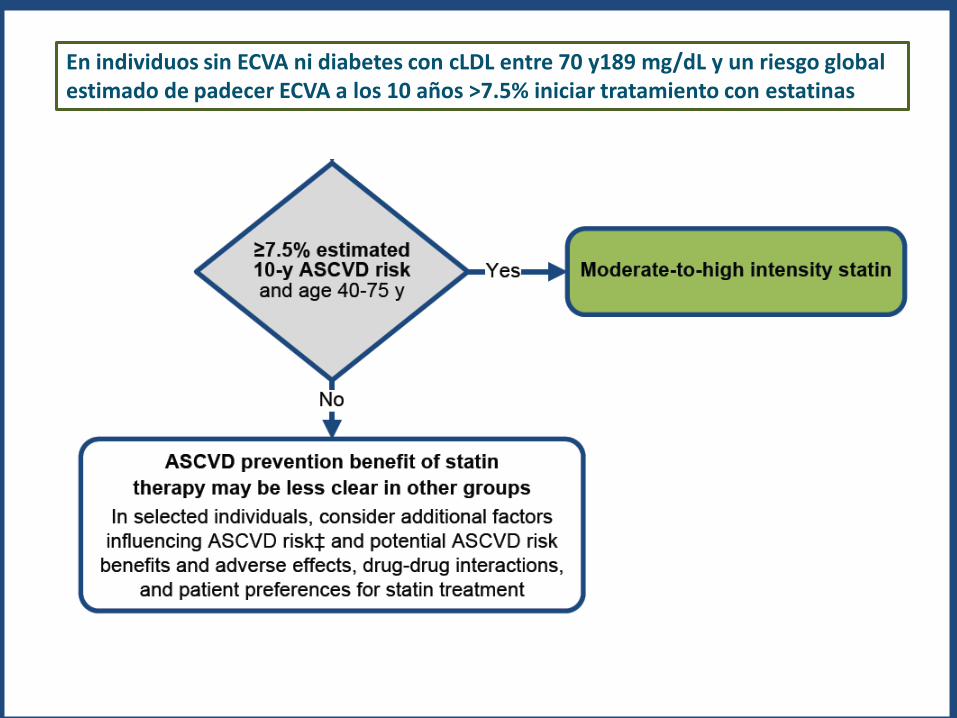
En individuos sin ECVA ni diabetes con cLDL entre 70 y189 mg/dL y un riesgo global estimado de padecer ECVA a los 10 años >7.5% iniciar tratamiento con estatinas
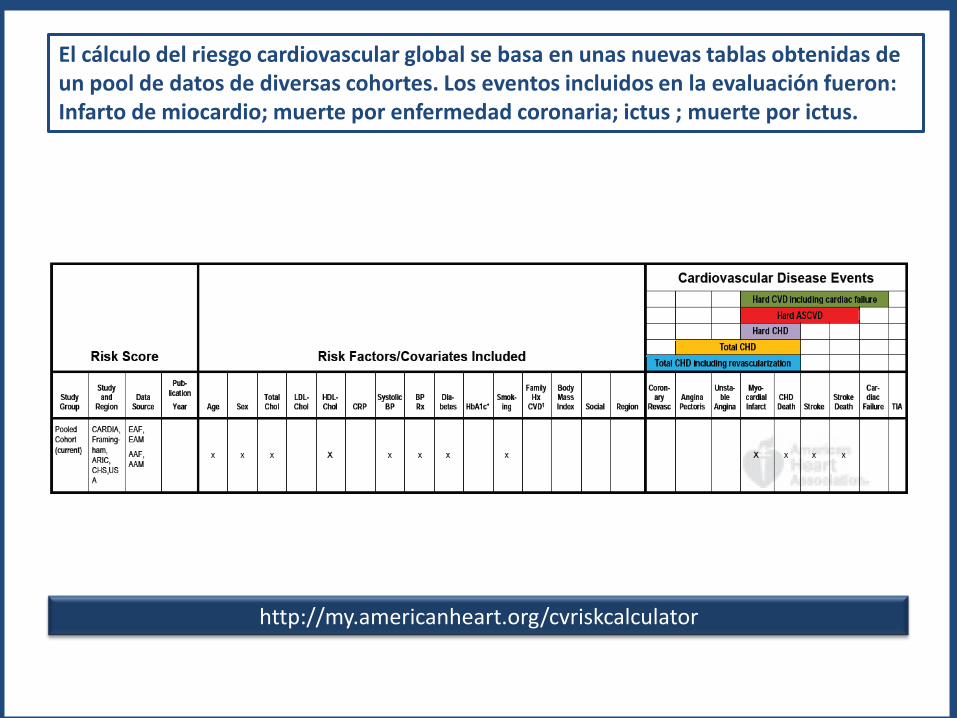
El cálculo del riesgo cardiovascular global se basa en unas nuevas tablas obtenidas de un pool de datos de diversas cohortes. Los eventos incluidos en la evaluación fueron: Infarto de miocardio; muerte por enfermedad coronaria; ictus ; muerte por ictus.
http://my.americanheart.org/cvriskcalculator
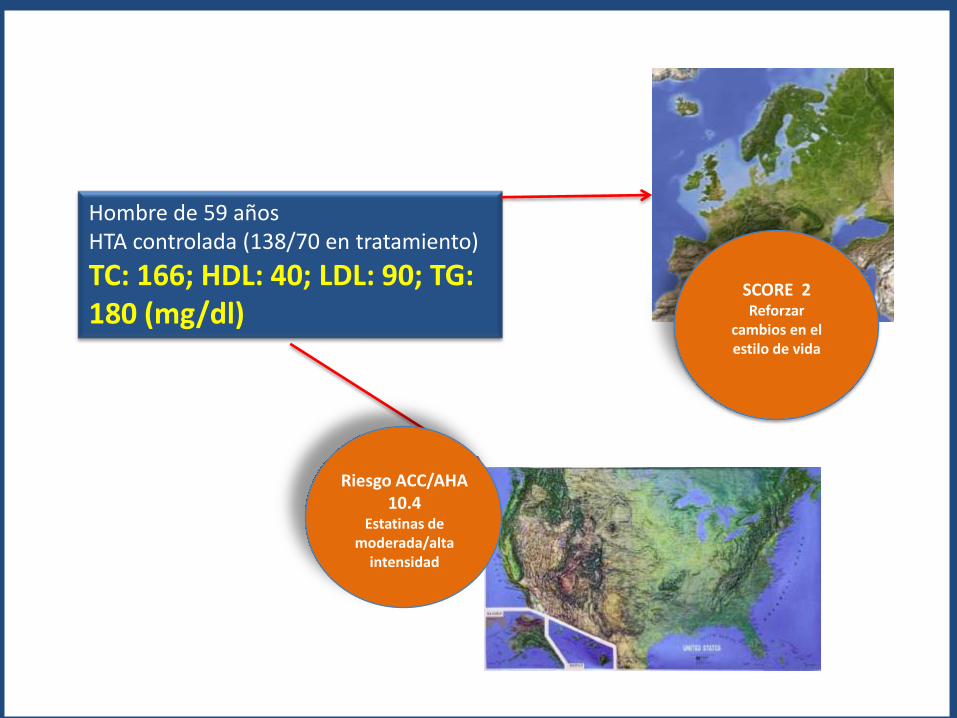
Hombre de 59 añosHTA controlada (138/70 en tratamiento)
TC: 166; HDL: 40; LDL: 90; TG: 180 (mg/dl)
SCORE 2Reforzar
cambios en el estilo de vida
Riesgo ACC/AHA 10.4
Estatinas de moderada/alta
intensidad
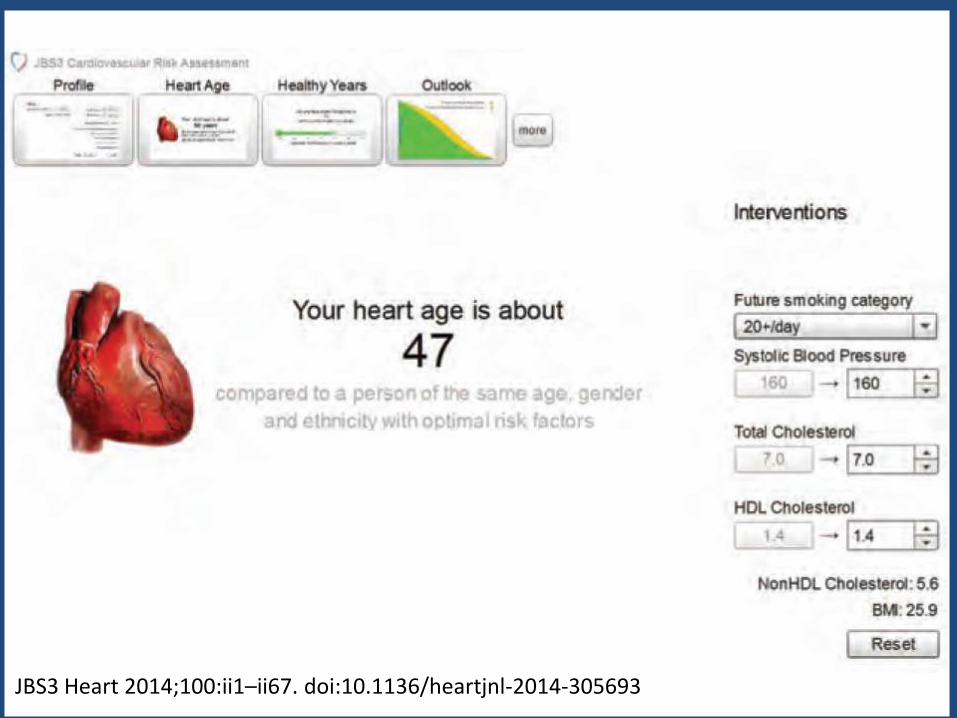
JBS3 Heart 2014;100:ii1–ii67. doi:10.1136/heartjnl-2014-305693
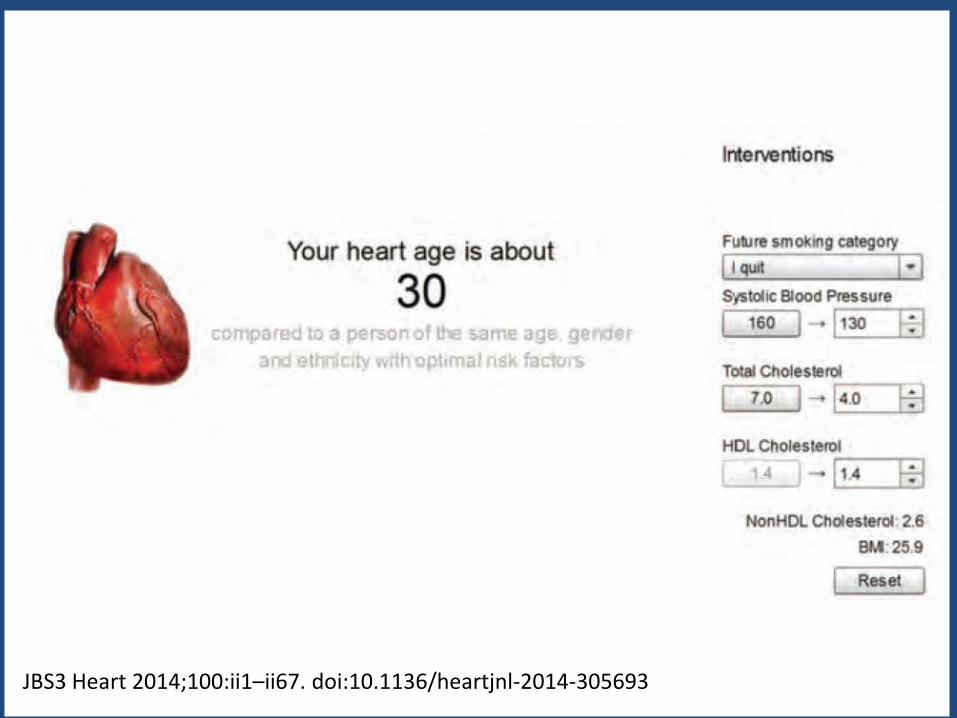
JBS3 Heart 2014;100:ii1–ii67. doi:10.1136/heartjnl-2014-305693
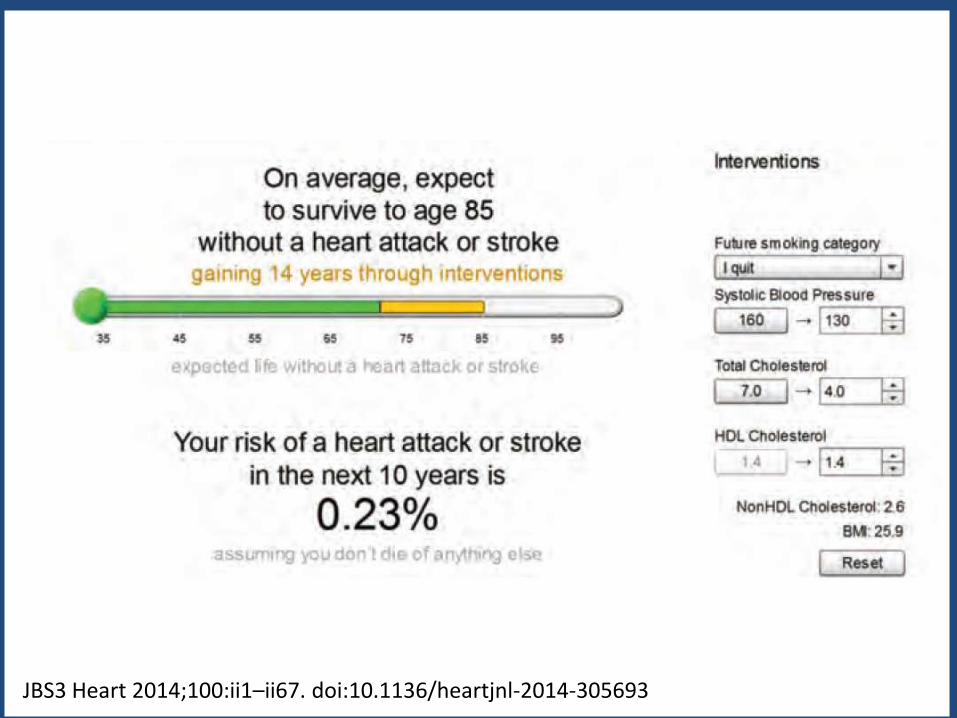
JBS3 Heart 2014;100:ii1–ii67. doi:10.1136/heartjnl-2014-305693
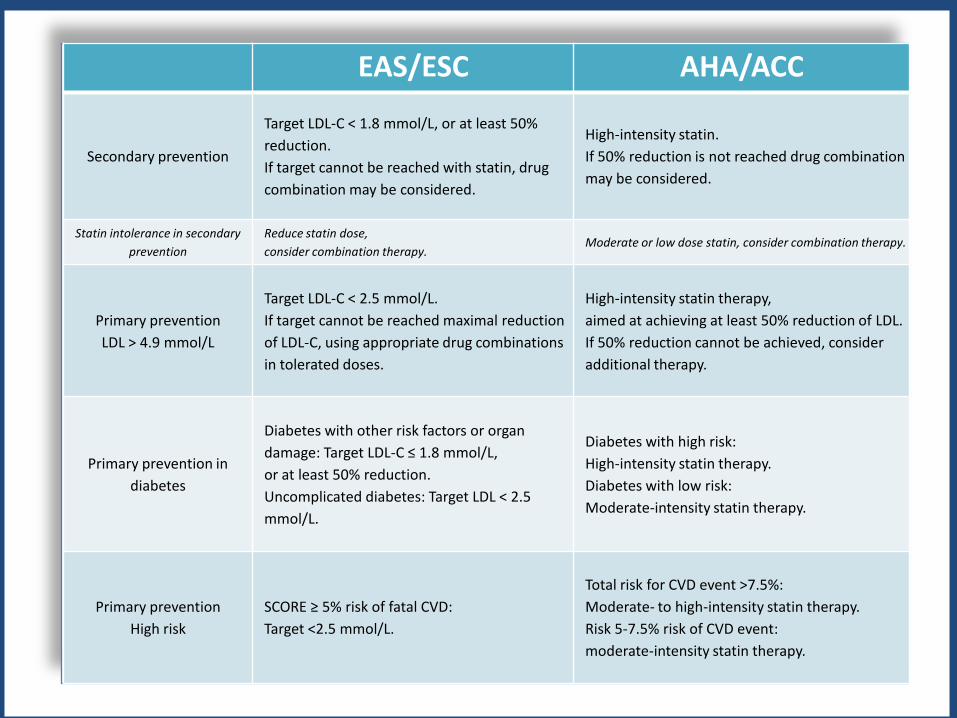
EAS/ESC AHA/ACC
Secondary prevention
Target LDL-C < 1.8 mmol/L, or at least 50%
reduction.
If target cannot be reached with statin, drug
combination may be considered.
High-intensity statin.
If 50% reduction is not reached drug combination
may be considered.
Statin intolerance in secondary
prevention
Reduce statin dose,
consider combination therapy.Moderate or low dose statin, consider combination therapy.
Primary prevention
LDL > 4.9 mmol/L
Target LDL-C < 2.5 mmol/L.
If target cannot be reached maximal reduction
of LDL-C, using appropriate drug combinations
in tolerated doses.
High-intensity statin therapy,
aimed at achieving at least 50% reduction of LDL.
If 50% reduction cannot be achieved, consider
additional therapy.
Primary prevention in
diabetes
Diabetes with other risk factors or organ
damage: Target LDL-C ≤ 1.8 mmol/L,
or at least 50% reduction.
Uncomplicated diabetes: Target LDL < 2.5
mmol/L.
Diabetes with high risk:
High-intensity statin therapy.
Diabetes with low risk:
Moderate-intensity statin therapy.
Primary prevention
High risk
SCORE ≥ 5% risk of fatal CVD:
Target <2.5 mmol/L.
Total risk for CVD event >7.5%:
Moderate- to high-intensity statin therapy.
Risk 5-7.5% risk of CVD event:
moderate-intensity statin therapy.
Civeira F, Ascaso J, Masana L, Letter to the Editor: “Should we forget about LDL cholesterol?”, Journal of the American College of Cardiology (2014), doi: 10.1016/j.jacc.2013.11.054.
“The document has, according to the Spanish Atherosclerosis Society, many positives aspects: the systematic review of the literature, the definition of the groups susceptible to treatment, the classification of the statins effects, and the new calculation of cardiovascular risk. However, the uncertainty and nihilism in many important issues is worrisome and may harm many patients; leaving behind the concept of intensive reduction of LDL-c will confuse many doctors; and being focused on statins will be detrimental to the investigation and development of other lipid-lowering drugs. For these reasons, the Spanish Society of Arteriosclerosis does not support this document, and better recommends the guidelines from the ESC/EAS”