rena buckstein february 2009. using case based methods, review the current epidemiology,...
TRANSCRIPT

Case Based NHL teaching for Medical Oncologists
Rena BucksteinFebruary 2009

Objectives
Using case based methods, review the current epidemiology, classification and diagnosis of DLBCL and FL
Discuss approach to treatments with supporting evidence Immunochemotherapy Radioimmunoconjugates High dose therapy and SCT Newer approaches and agents

NHL: Incidence and Mortality
Canada6,220 new cases2650 deaths Fifth most
commontype of cancer
in females and males in
Canada 1/46 chance
lifetime risk Increasing since
early 1970s but now levelling
Year
1975 1978 1983 1988 1993 1998 20040
2.5
20.0
17.5
15.0
12.5
10.0
7.5
5.0
11.1
5.6
11.9
5.9
14.0
6.7
17.2
7.5
18.8
8.28.7
7.0
19.420.4
Rate per 100,000
Incidence
Mortality

Age-Specific Incidence of
Non-Hodgkin Lymphoma
2000-2004
Incidenceper100,000
0
110
100
90
80
70
60
50
40
30
20
10
0-4
5-9
10
-14
15
-19
20
-24
25
-29
30
-34
35
-39
40
-44
45
-49
50
-54
55
-59
60
-64
65
-69
70
-74
75
-79
80
-84
85
+
0.6 0.9 1.2 1.8 2.4 3.4 4.9 7.410.5
15.522.6
32.0
45.1
63.4
80.0
100.8
Age
NHL: DemographicsNHL: Demographics• Increases with age
102.0
112.1
<1* <16 cases per time interval
<1
*
0.0
115





Copyright ©2007 American Society of Hematology. Copyright restrictions may apply.
Hematology 2007;2007:509-520
Figure 1. Schematic representation of normal B-cell ontogeny in the germinal center

Copyright ©2007 American Society of Hematology. Copyright restrictions may apply.
Hematology 2007;2007:509-520
Figure 4. Schematic representation of t(14;18)+ B-cell clones and the genesis of follicular lymphoma

Case
A 60-year-old woman is diagnosed with stage IV FL Hemoglobin is 11 g/dL, platelets 120,
LDH upper normal limit No bulky disease She has some fatigue but no other
symptoms or other significant past medical history
What is her prognosis?



CD20 MIB 1
H & E

FL: grading and reportingGrade Grade 1: 0-5 centroblasts/hpf Grade 2: 6-15 centroblasts/hpf Grade 3: > 15 centroblasts/hpf
3a: centrocyes present 3b: solid sheets of centroblasts
Pattern reporting Follicular: > 75% follicular Follicular and diffuse: 25-75% follicular Focally follicular: < 25% follicular

FL: variants and immunophenotype
Diffuse Follicle center lymphoma Grade 1: 0-5 centroblasts/hpf Grade 2: 6-15 centroblasts/hpf Grade 3b: call DLBCL
Cutaneous follicle center lymphoma Immunophenotype
SIg+ (IgM +/- IgD, IgG or rarely IgA) Bcl2+ (except cutaneous), CD20+, CD10+,
CD5-, CD22+, CD79a+)

Follicular lymphoma: genetic abnormalities
t(14;18) 80%+7 20%+18 20%3q27-28 15%6q23-26 15%17p 15%BCL2 rearranged 80%

Agricultural pesticide use and the risk of t(14;18)-defined subtypes of NHL in Nebraska
175 tumour blocks with NHL cases T(14;18) by FISH Compared exposures to herbicides, fungicides and
fumigants in 65 + cases versus 107 negative cases with those among 1432 control subjects
Compared with farmers who never used pesticides, the risk of t(14;18) + NHL was increased in farmers who used Animal insecticides (OR 2.6; 95% CI 1.0-6.9) Crop insecticides (OR 3.0; 95% CI 1.1-8.2) Herbicides (OR 2.9; 95% CI 1.1-7.9) Fumigants (OR 5.0; 95% CI 1.7-14.5) Risk increased with longer duration of use No association with t(14;18) negative NHL

FLIPI
International initiative (27 centers US, Europe, UK)
FL patients Jan 1985-Dec 1992> 5 yrs F/up5120 registered cases, with 4167
(81%) eligibleminimum criteria for stagingperformance status, albumin, b2
microglobulin not included in Cox Model
Updated from Solal-Céligny P, et al. Ann Oncol 2002;13(Suppl. 2):18 (Abstract 54)

Risk Status: FLIPI
Factors:1. Age > 602. Ann Arbor Stage III-IV3. Number of nodal sites > 44. Serum LDH level > upper limit of
normal5. Hemoglobin < 12g/dL
FOLLICULAR Philippe Solal-Céligny et al. Blood . 2004. 104:1258-1265.

FLIPI
Risk Group
# factors % of patients
5 yr OS 10 yr OS
Low 0-1 36 91 71
Int 2 37 77 51
High >3 27 52 36
Blood 2004; 104:1258-1265.Philippe Solal-Céligny et al. Blood . 2004104:1258-
1265


Pro
bab
ilit
y o
f su
rviv
alOverall survival according to FLIPI
1.0
0.8
0.6
0.4
0.2
0
0 12 24 36 48 60 72 84
Months
Good
Intermediate
Poorp <0.0001

Follicular lymphoma and the immune system
Spontaneous remissions in up to 20%
Role of alpha interferon Idiotype vaccinesTumor microenvironment immune
signature

Survival Predicted by Molecular features of Tumor Infiltrating Immune Cells
International collaborative studyGene expression profiling of 191
biopsy specimens for untreated FLConstructed molecular predictor of
survival from GEP’s in training set and validated in independent set
Two signatures called IR-1 and IR-2 were found to be significantly discriminating

Immune response signatures: can be averaged into survival predictor score
IR1: favorablegenes encoding T cell markers
(CD7, CD8B1, ITK, LEF1 and STAT4)IR2: unfavorable genes preferentially expressed in
macrophages, dendritic cells or both (TLR5, FCGR1A, SEP10, LGMN, C3AR1)

Development of a Molecular Predictor of Survival in Follicular Lymphoma.

FL: Natural history
IncurableWaxing and waning courseMultiple treatment courses over
patient lifetimeOS 10-12 yearsW&W appropriateAnthracyclines upfront provide no
survival advantage

Gallagher CJ, et al. J Clin Oncol 1986; 4:1470-80.
Follicular Lymphoma:Duration of Chemotherapy-Induced Remissions
Duration of Remission (Years)
100
0
20
40
60
80
•0 1 2 3 8
1st (N=74)
2nd (N=20)
3rd (N=18)
4th (N=8)

FL response to treatment: historical
75-85% response rates to standard chemotherapy
CR rates are short(12-36) months duration of response to chemo:
prognostic survival if CR or PR < 1 yr.: 2.4 yrs survival if CR or PR > 1 yr.: 6 yrs
response rates decline with further chemo
▪ regimen 1: 16 months▪ regimen 2: 11 months▪ regimen 3: 9 months▪ regimen 4: 3.2 months

Case
60 y.o man presents with painless single inguinal LN measuring 2x3 cm
PE and staging confirms localizedLDH and labs are normalBiopsy: follicular grade 2How to treat this patient?

Treatment options
1. watch and wait2. Radiation3. Chemotherapy alone + R
maintenance4. R-chemotherapy +/- maintenance5. Rituximab alone +/- maintenance6. Radioimmunotherapy7. HDT stem cell transplant

Is radiotherapy curative for stage I and II low grade follicular lymphoma?


Stage I and II follicular non-Hodgkin’s lymphoma: long-term follow-up of no initial therapy
Advani R. et al JCO 2004
Estimated survivals at 5, 10 and 20 years were 97%, 85% and 22%

Case history details
VPL, 35 years old, hairdresser, female, black. December 2003: cervical lymph nodes (left 3 cm, right 2
cm) with progressive increase. March 22, 2004 (first appointment): cervical lymph nodes
of 2 cm, no organ enlargements.
Lab tests Hb 13.4 g/dL; Ht 40%, WBC: 6,300/mm3 Biochemistry: normal (including LDH and ß2
microglobuline). Serology: HIV, hepatitis, CMV, HTLV I,II negative.
Bone marrow aspiration: Hypercellular - 56% lymphoid cells
Bone marrow biopsy: multifocal paratrabecular infiltration by lymphoid cells
Cytogenetics: normal Chest CT: 1-2 lymph nodes (para tracheal, para aortic and
pulmonary) Abdomen CT– small bulk extensive lymphadenopathy
Lymph node cervical biopsy: B cell follicular lymphoma grade 2 (WHO)
How to treat?

Newly Diagnosed Advanced Stage Patient: Asymptomatic

How would you treat her?
1. Watch and wait2. CVP + R3. CHOP + R4. Rituximab monotherapy +/-
maintenance5. Bexxar or Zevalin6. Autologous Stem Cell Transplant7. Allogeneic Stem Cell Transplant

Initial Therapy
Watch and Wait 3 randomized trials to support this in low
tumour burden NHL▪ GELF 1997: no rx vs prednimustine vs
interferon alfa▪ NCI 1988: no rx vs. ProMACE-MOPP▪ BNLI 2003: no rx vs. chlorambucil

Ardeshna et al. Lancet 2003; 362: 516-22
Overall
Cause- specific

Time to Treatment
Ardeshna et al. Lancet 2003; 362: 516-22Median time to first treatment 2.6 yrs

Patient history continues
2 years later, patient complains of B symptoms
CT re-imaging: extensive bulky retroperitoneal and peri-renal LN’s
HB 110, plt 100

How would you treat her?
1. Watch and wait2. CVP + R3. CHOP + R4. Rituximab monotherapy +/-
maintenance5. Bexxar or Zevalin6. Autologous Stem Cell Transplant7. Allogeneic Stem Cell Transplant

Newly Diagnosed Patient with Advanced Disease: Symptomatic

Criteria for starting cytotoxic therapy
GELF CRITERIA
High tumor bulk any of: Tumor > 7 cm 3 nodes in 3 distinct areas
> 3 cm each Symptomatic
splenomegaly Organ compression Ascites or pleural effusion Systemic symptoms ECOG > 1 Increased LDH or
B2microglobulin
BNLI CRITERIA
Any of: Rapid generalized disease
progression in preceding 3 mos
Life threatening organ involvement
Renal or macroscopic liver infiltration
Bone lesions Symptoms Hgb < 10 or WBC < 3 or
plt < 100 if do to BMI


target cell
plus antibody
antigen
naturalkillercell
targetcell
macrophageFc receptor
FcFab
Fc receptor


Rituximab
Infusional side effects tolerableDepletes B cells for about 6 monthsNot myelosuppressiveDoes not increase infectious riskCan be re-used with equal efficacy in
respondersAdditive or synergistic effects with
chemotherapy

Study Design: CVP +/- R
Follicular NHL (IWF B, C, D)
Stage III–IV ³18 years No prior treatment Measurable disease Central histology
review
RANDOMIZED
CVP x 4 cycles(every 3 weeks)
Rituximab + CVP x 4 cycles
(every 3 weeks)
RESTAGING
CVP x 4 cycles(every 3 weeks)
Rituximab + CVP x 4 cycles
(every 3 weeks)
SD, PD off treatment
CR, PR
Rituximab 375mg/m2 i.v. day 1Cyclophosphamide 750mg/m2 i.v. day 1Vincristine 1.4mg/m2 i.v. day 1Prednisone 40mg/m2 p.o. days 1–5
Marcus R. et al. Blood. 2005; 105: 1417-1423

Patient Characteristics
Variable
CVP (n=159)
R-CVP (n=162)
Age (Median)
53
52
IPI Low Int High
44% 49% 2%
45% 47% 1%
FLIPI 0-2 3-5
47% 47%
49% 44%
Imrie K. et al. Proc. ASCO 2005; abstract 6525

Summary of outcomesmedian follow-up: 30 months
Endpoint CVP(n-159)
R-CVP(n=162) p
Response rate
Median time to treatment failure(months)
57%
7
81%
27
<0.0001
<0.0001
Median duration of response(months) 14 35 <0.0001
Median disease-free survival(months) 21 not
reached 0.0009
Median time to new anti-lymphoma treatment or death (months)
12 not reached <0.0001
KM estimates for overall survivalat 30 months 85 89 NS
KM = Kaplan-Meier; NS = not statistically significantImrie K. et al. Proc. ASCO 2005; abstract 6525

CVP ± Rituximab in Previously Untreated Follicular NHL: Time to Treatment Failure
CVP
Rituximab + CVP
Patients at risk: 30 months follow-up
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0 3 6 9 12 15 18 21 24 27 30 33
Months
Pro
bab
ility
of
even
t-fr
ee
surv
ival
Rituximab + CVP: median 27 months
CVP: median 7 months
p<0.0001
Risk reduction: 67%
159 100 87 67 43 29 14 13 9 1 0 0
162 140 123 114 95 73 50 37 20 8 3 0
Marcus et al. Blood. 2005;105:1417-1423

CVP ± Rituximab in Previously Untreated Follicular NHL: Time to Progression, Relapse or Death
Rituximab + CVP: median 32 months
CVP: median 15 months
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 3 6 9 12 15 18 21 24 27 30 33
Months
Pro
bab
ility
of
even
t-fr
ee
surv
ival
p<0.0001
CVP
Rituximab + CVP
Patients at risk
159 140 130 106 75 49 31 24 16 2 0 0
162 156 143 134 110 83 60 44 25 9 3 0
Marcus et al. Blood. 2005;105:1417-1423
30 months follow-up

Conclusions
The addition of rituximab to first-line treatment with CVP improves response rate, response duration and time to progression without increasing toxicity
The benefit in terms of TTP of adding rituximab is observed in all prognostic groups.
In the presence of treatment with R-CVP, only the FLIPI score has additional predictive value Imrie K. et al. Proc. ASCO 2005; abstract 6525

GLSG: CHOP vs R-CHOPFor First Line Therapy of Follicular Lymphoma
Randomization
6 - 8 x CHOP
6 - 8 x CHOP +
Ritux
CR, PR
CR, PR
Randomization
PBSCT
standard IFN-maintenance
intensive IFN-maintenance
standard IFN-maintenance
Hiddemann W et al. Blood. 2005;106; 3725-32
pts. < 60 yrs.
pts. > 60 yrs.
N=187
N=201

Copyright ©2005 American Society of Hematology. Copyright restrictions may apply.
Hiddemann, W. et al. Blood 2005;106:3725-3732
Figure 2. Time to treatment failure and duration of response after CHOP and R-CHOP
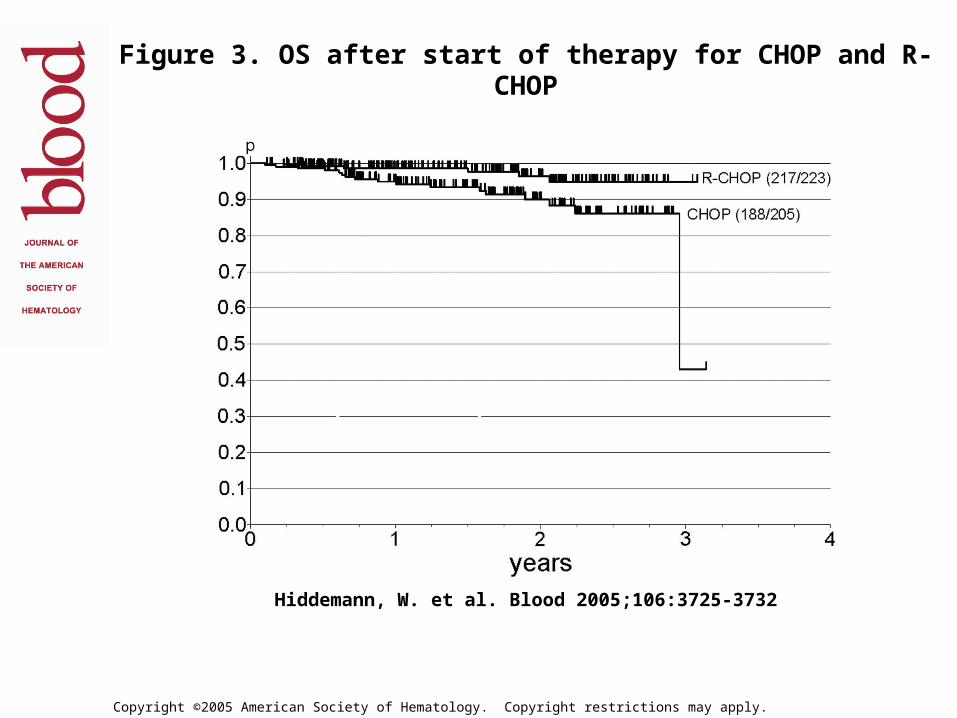
Copyright ©2005 American Society of Hematology. Copyright restrictions may apply.
Hiddemann, W. et al. Blood 2005;106:3725-3732
Figure 3. OS after start of therapy for CHOP and R-CHOP
(P = .016).


Response Rate

2-Year Event Free Survival

Case continued…
Patient achieves a 4 year remission after CVP-R but relapses with similar clinical presentation
How to treat?
How would you treat her?
1. Watch and wait2. CVP + R3. CHOP + R +/- maintenance4. Rituximab monotherapy +/-
maintenance5. Bexxar or Zevalin6. Autologous Stem Cell Transplant7. Allogeneic Stem Cell Transplant

Rituximab in remission induction and maintenance treatment of relapsed follicular NHL ASH 2005 - EORTC/Intergroup
(Final analysis)
M.H.J. van OersM. Van Glabbeke
I. TeodorovicC. Rozewicz
R.KlasaR.E.Marcus
M.WolfE Kimby
A.Hagenbeek

RANDOMIZED
CHOP every21 days
maximum 6 cycles
Rituximab + CHOP every
21 daysmaximum 6
cycles
Intergroup phase III trial – Final analysis
RANDOMIZED
Observation
Rituximab maintenance*
CRPR
MR - Rituximab 375 mg/m2 q 3 mos for 2 years
n = 319 evaluable (median F/U 33 mos)

Intergroup Study - PFS (2nd Randomization)
Overall log-rank test: p<0.0001Hazard ratio: 0.40
O N Number of patients at risk
110 167 90 42 17 5 Observation66 167 126 86 47 12 MabThera
Treatment
100
90
80
70
60
50
40
30
20
10
0
0 1 2 3 4 5Years
MR 52 mos
Observation: 15 mos
Pro
gre
ssio
n-f
ree
surv
ival
(%
)

(years)
0 1 2 3 4 5
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment55 69 31 11 4 1
32 76 61 38 20 4
Observation
Mabthera
Progression free survivalafter CHOP
Overall Logrank test: p<0.0001
(years)
0 1 2 3 4 5
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment55 98 59 31 13 4
34 91 65 48 27 8
Observation
Mabthera
Progression free survivalafter R-CHOP
Overall Logrank test: p=0.004
Intergroup phase III trial Progression free survival (2nd randomization)
median: 42.2 months
med. 11.6 monthsmed. 23.1 months
median: 51.9 months
Subgroups according to induction treatment
Hazard ratio: 0.30 Hazard ratio: 0.54

(years)
0 1 2 3 4 5 6
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment39 167 148 99 50 14 2
23 167 155 112 69 19 4
Observation
Mabthera
Overall survivalfrom 2nd randomization
Overall Logrank test: p=0.011
Intergroup phase III trial Overall survival (2nd randomization)
MR at 3 years - 85%
Observation at 3 years - 77%

(years)
0 1 2 3 4 5 6
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment19 69 61 42 23 7 2
12 76 75 49 30 8 2
Observation
Mabthera
Overall survivalafter CHOP
Overall Logrank test: p=0.073
(years)
0 1 2 3 4 5 6
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment20 98 87 57 27 7 0
11 91 80 63 39 11 2
Observation
Mabthera
Overall survivalafter R-CHOP
Overall Logrank test: p=0.059
OS from 2nd randomization: subgroup analysis
Hazard ratio: 0.52 Hazard ratio: 0.49
Intergroup phase III trial Overall survival (2nd randomization)

Copyright restrictions may apply.
Schulz, H. et al. J. Natl. Cancer Inst. 2007 99:706-714; doi:10.1093/jnci/djk152

Summary: Rituximab + chemotherapy in follicular NHL
Recommended for first or second line combination (> 6 randomized trials support)
No one regimen clearly superior to another
Role of re-treatment combination unknown
Maintenance Rituximab is associated with improved PFS and OS after CVP alone first line and after CHOP or CHOP-R second line
Case continued alternate scenario
Patient gets CVP-R and enters complete remission.
4 years later, presents with night sweats and rapidly progressive axillary and inguinal nodes
LDH is elevated and patient has widespread bulky adenopathy
What would you do?

Transformed FL
Population based series from BC lymphoma database (n=600) median follow up 109 months
28% developed transformation at median of 40 months (63% by biopsy)
Annual rate 3% per year continuously
Advanced stage at diagnosis only RFMedian post transformation survival
1.7 years (better if limited with 5 yr OS 66% vs. 19%)

Copyright © American Society of Clinical Oncology
Al-Tourah, A. J. et al. J Clin Oncol; 26:5165-5169 2008
Fig 1. The actuarial risk of transformation in patients with follicular lymphoma

Copyright © American Society of Clinical Oncology
Al-Tourah, A. J. et al. J Clin Oncol; 26:5165-5169 2008
Fig 2. The impact of transformation on the overall survival

What about high dose therapy?


Autologous Stem Cell Transplants in relapsed FL
In 2nd or 3rd remission: 1 small RCT (CUP trial n=140) Schouten JCO 2003)
4 yr Survival advantage (46 vs 77%): Role of purging unknown
Multiple Phase 2 studies: PFS benefit Curative?
Pooled St Barts and MSK experience (n=121) Median f/up 13.5 years Plateau in PFS @ 12 years of 48% Best in second remission RD and OS better compared with age matched controls not
transplanted CY/TBI: secondary leukemia and MDS (n=15)
Molecular remissions predict for better RFS Rituximab or RIT may change durability of
remissions (cure?)

Fig 1. Remission duration of all patients.
Rohatiner et al. JCO 2007

Auto versus Allo?
Registry data: No proven survival benefit of allo
over auto RFS 80% but TRM 30% in some series
Allo has early plateau in PFS curve In 1 study, no difference between
syngeneic or allo….??? DLI has been shown to work
Allo may play a role in chemoinsensitive young patients with short remissions
Allo can rescue a relapsed auto failure

Radioimmunoconjugates

Efficacy of Unlabeled Tositumomab Enhanced Through the Crossfire Effect of
Iodine-131
Unlabeled “cold” Antibody Radiolabeled Antibody
Courtesy of Andrew Zelenetz, MD.

Radio-immunoconjugates
Zevalin BexxarSource 90Y 131IType ß mixed ß, Energy (MeV) 2.3 0.6Path (mm) 5 1T1/2 (d) 2.6 8Setting out-pt out-
ptImaging no yesThyrotoxic no yes

Radioimmunoconjugates
Advantages
Effective in heavily pre treated patients May surpass preceding
responses Effective in Rituximab
refractory patients Patients who achieve CR
have long RD Toxicity mild Treatment short Can be re-used Radiosensitive disease
Disadvantages
Limited # centers Some require dosimetry Not recommended for Plts
< 100 or BM > 30% % prior marrow radiation
may limit AML/MDS? Delayed hematologic
toxicity Expense Some require isolation for
5-8 days Used early: long term
effects? Effects on re-treatment?

Efficacy of single-regimen RIT for relapsed/refractory FL.
Reference Agent Phase n Patient selection Response rates
Duration of response
Kaminski et al (2000)
Bexxar®
I/II 42 Relapsed or refractory CD20+ B-cell low- and intermediate-grade NHL
ORR 71%CR32%
Median PFS 12 months (for CR 20 months)
Vose et al (2000)
Bexxar®
II 47 Relapsed or refractory CD20+ B-cell low-grade and transformed NHL
ORR 57%CR 32%
Median DR 9·9 months (for CR 19·9 months)
Kaminski et al (2001)
Bexxar®
II 60 Relapsed or refractory CD20+ B-cell low-grade and transformed NHL
ORR 65%CR 20%
Median DR 6·5 months
Witzig et al (1999)
Zevalin®
I/II 51 Relapsed or refractory CD20+ B-cell low- and intermediate-grade NHL or MCL
ORR 67%CR 26%
Estimated DR 11·7 + months
Witzig et al (2002a)
Zevalin®
III 143 Relapsed or refractory low-grade FL or transformed NHL
ORR 80%CR 30%CRu 4%
Estimated DR 14·2 months
Wiseman et al (2002)
Zevalin®
II 30 Relapsed or refractory low-grade FL or transformed NHL and mild thrombocytopenia
ORR 83%CR 37%CRu 6%
Estimated TTP 9·4 months (for responders 12·6 months)
Witzig et al (2002b)
Zevalin®
II 54 Rituximab-refractory FL ORR 74%CR 15%
Estimated TTP 6·8 months (for responders 8·7 months)

New agents and approaches
Anti-idiotype vaccines……????BendamustineLenalidomideVelcadeZevalin for consolidationRituxan re-treatmentGaliximab (anti-CD80), epratuzumab
(anti CD22), anti CD40

Copyright © American Society of Clinical Oncology
Liu, Q. et al. J Clin Oncol; 24:1582-1589 2006
Fig 2. Overall survival according to treatment regimen

AlgorithmNew
diagnosis
Limited stage: XRT
Advanced stage:
•W + W
•CVP-R+M
•CHOP-R+M
•Clinical trial
First Relapse
•CVP-R +M
•CHOP-R+M
•FCM-R + M
•ASCT
•Allo BMT
•RIT
•Clinical Trial
Second Relapse
•CVP +/-R
•CHOP +/- R
•FCM +/- R
•ASCT
•Allo BMT
•RIT
•Clinical Trial