remark from the minister of health - …indonesia.unfpa.org/sites/default/files/pub-pdf/isi_national...
TRANSCRIPT

i
REMARK FROM THE MINISTER OF HEALTH
The targets of the Millennium Development Goals (MDGs) are due to be reached in 2015, just two years after the publication of this book. The Government of Indonesia has dedicated strong attention to reaching these targets. This attention has only been strengthened by an increased allocation of health funds, with about 80% of this increase occurring in the regions. However, several MDG indicators, which are also included in the targets of the National Medium Term Development Plan (RPJMN) for 2010-2014, will be difficult to achieve under the current efforts and strategies. Various projections and estimates have found that the Maternal Mortality Rate (MMR) will not drop fast enough to achieve the target by the deadline in 2015 without a renewed approach.
The results of surveys and research conducted over the past five years have generally shown that under the current approach, the targeted decrease in the MMR will not be achieved by the deadline of the MDGs in 2015. This indicates that a more cost-effective and evidence-based approach is needed. Furthermore, the country’s stagnant Total Fertility Rate (TFR) over the past 10 years shows that the Government’s Reproductive Health Programme and Family Planning Programme require special attention. In recent years, maternal deaths have mostly occurred among women aged under 20, or over 35, and greater numbers of women have begun to have more than three children, with shorter spacing between births.
Health programme managers at the national, provincial and district levels should be able to identify the existing problems and find solutions, using the interventions that have proven to work successfully with the use of local resources. Optimization and synchronization of activities must be conducted. Every district and city must re-examine whether the action plans developed have addressed the existing problems in their region. The role of provinces should be promoted as an extended arm of the central government to assist the districts and cities in carrying out the development of public health. Strategic steps that need to be carried out to optimize efforts to accelerate the reduction of the MMR are detailed in this book.
I extend my appreciation to all stakeholders who have already, are currently, or are planning to participate in accelerating the reduction of the MMR in this country, and all who have contributed to the publication of this book. It is my hope that this book will be useful as a reference for the acceleration of the reduction of the MMR in Indonesia, and can bring the greatest possible results for the health of its
people.
Jakarta, 30 April 2013
Dr. Nafsiah Mboi, SpA, MPH, Health Minister of the Republic of Indonesia

ii
FOREWORD DIRECTOR GENERAL OF NUTRITION, MATERNAL AND CHILD HEALTH
Thanks to Almighty God for His blessings and the abundance of His grace, that the National Action Plan for the Acceleration of the Reduction of the Maternal Mortality Rate can finally be published. This book was jointly prepared by all programmes involved in the Ministry of Health, as well as professional organizations and donor agencies involved in maternal health in Indonesia.
The National Development Planning Board (Bappenas) has developed a Regional Action Plan to achieve the Millennium Development Goals, or MDGs. In 2010, this Regional Action Plan should be followed up with concrete actions, particularly because the MDG target on reducing maternal deaths is predicted to be difficult to achieve before the deadline in 2015. It is important for stakeholders to read this book, which details the principles of maternal mortality prevention, strategies and interventions − interventions that have proven to be effective for preventing maternal mortality − and the parameters that must be considered by programme managers.
It is expected that this book can serve as a set of guidelines for all actors involved in maternal health at the national and regional levels in developing the programmes and targets that suit the conditions of each region.
Thanks to all parties that have contributed to the preparation of the National Action Plan for the Acceleration of the Reduction of the Maternal Mortality Rate, and especially to Dr. Endang Achadi, MPH, who helped with the formulation of this National Action Plan.
Jakarta, March 2013Director-General of Nutrition, Maternal and Child Health
Dr. Slamet Riyadi Yuwono, DTM&H, MARS

iii
iii
LIST OF CONTENT
REMARK FROM THE MINISTER OF HEALTH .............................................................................................. i
FOREWORD DIRECTOR GENERAL OF NUTRITION, MATERNAL AND CHILD HEALTH ............................... ii
LIST OF CONTENT .................................................................................................................................... iii
LIST OF ABBREVIATIONS ......................................................................................................................... iv
LIST OF FIGURES ..................................................................................................................................... vii
LIST OF TABLES ...................................................................................................................................... viii
CHAPTER I INTRODUCTION ..................................................................................................................... 1
A. Background ....................................................................................................................... 1
B. Goal ................................................................................................................................... 1
C. Target ................................................................................................................................ 2
CHAPTER II SITUATION ANALYSIS ........................................................................................................... 3
A. Maternal Mortality .......................................................................................................... 3
B. Pathway of maternal mortality ....................................................................................... 4
C. Principles of maternal mortality prevention ................................................................... 5
D. Program Achievement ..................................................................................................... 6
CHAPTER III NATIONAL ACTION PLAN .................................................................................................. 11
A. Goal ................................................................................................................................. 11
B. Challenge, Strategy and Main Program ......................................................................... 11
CHAPER IV MONITORING AND EVALUATION ....................................................................................... 23
A. Achievement Indicator ................................................................................................... 23
B. Mechanism for monitoring of the National Action Plan for the Acceleration of Maternal Mortality Ratio Reduction ............................................................................. 24

iv
vi
LIST OF ABBREVIATIONS
ANC Antenatal Care
APBD Anggaran Pandapatan dan Belanja Daerah (Regional Budget)
APN Asuhan Persalinan Normal (Normal Delivery)
Balitbangkes Badan Penelitian dan Pengembangan Kesehatan (National Institute of Health, Research and Development)
Bappeda Badan Perencanaan Pembangunan Daerah (Regional Development Planning Board)
Bappenas Badan Perencanaan Pembangunan Nasional (National Development Planning Board)
BDRS Bank Darah Rumah Sakit (Hospital Blood Bank)
BKKBN Badan Kependudukan dan Keluarga Berencana Nasional (the National Population and Family Planning Board)
BPPSDM Badan Pengembangan dan Pemberdayaan Sumber Daya Manusia (Human Resources Development and Empowerment Board)
BPS Bidan Praktik Swasta (Private Practice Midwife)
CSR Corporate Social Responsibility
DPRD Dewan Perwakilan Rakyat Daerah (Regional Representatives Council)
DTPK Daerah Tertinggal, Perbatasan dan Kepulauan (Underdeveloped, Border and Island Regions)
GDON Gawat Darurat Obstetri dan Neonatal (Emergency Obstetrics and Neonatal Care)
GSI Gerakan Sayang Ibu (Mother-Friendly Movement)
HDK Hipertensi Dalam Kehamilan (Hypertension in Pregnancy)
HIV/AIDS Human Immuno-deficiency Virus/Acquired Immuno-deficiency Syndrome
HOGSI Himpunan Obstetri dan Ginekologi Sosial Indonesia (Indonesian Social Gynaecology and Obstetrics Association)
IAKMI Ikatan Ahli Kesehatan Masyarakat (Indonesian Public Health Association)
IBI Ikatan Bidan Indonesia (Indonesian Midwives Association)
ICD 10 International Classification of Diseases
IDAI Ikatan Dokter Anak Indonesia (Indonesian Pediatrics Society)
IDI Ikatan Dokter Indonesia (Indonesian Medical Association)
IDHS Indonesia Demographic and Health Survey
IDI Ikatan Dokter Indonesia(Indonesian Medical Association)

v
vii
IDSAI Ikatan Dokter Spesialis Anestesiologi dan Reanimasi Indonesia (Indonesian Society of Anesthesiologists and Reanimateurs)
K4 Antenatal visits occurring four times (4 kali) throughout pregnancy: once each in the first and second trimesters, and twice in the third trimester.
KARS Komisi Akreditasi Rumah Sakit (Hospital Accreditation Commission)
KB Keluarga Berencana, Family Planning
Kemenkes Kementerian Kesehatan, Health Ministry
KIA Kesehatan Ibu dan Anak (Maternal and Child Health)
KIE Komunikasi, Informasi dan Edukasi (Communication, Information and Education)
MMR Maternal Mortality Rate
MDGs Millennium Development Goals
MoU Memorandum of Understanding
NGO Non-Governmental Organization
P4K Program Perencanaan Persalinan dan Pencegahan Komplikasi (Complication
Prevention and Delivery Planning Programme)
Pemda Pemerintah Daerah (Local Government)
Perda Peraturan Daerah (Regional Regulation)
PERSI Perhimpunan Rumah Sakit Seluruh Indonesia (Indonesian Hospital Association)
PKK Pemberdayaan Kesejahteraan Keluarga (Empowerment of Family Welfare)
PMA Perinatal Mortality Audit
PMD Pemberdayaan Masyarakat Desa (Empowerment of Village Community)
PMI Palang Merah Indonesia (Indonesian Red Cross)
PODES Potensi Desa (Village Potential Statistics)
POGI Persatuan Obstetri dan Ginekologi Indonesia (Indonesian Society of Obstetrics and Gynecology)
PONED Pelayanan Obstetri Neonatal Emergensi Dasar (Basic Emergency Obstetric and Neonatal Care)
PONEK Pelayanan Obstetri Neonatal Emergensi Komprehensif (Comprehensive Emergency Obstetric and Neonatal Care)
PP AKI Percepatan Penurunan Angka Kematian Ibu (Acceleration of the Reduction of the Maternal Mortality Rate)
PPDS Program Pendidikan Dokter Spesialis (Doctorate Program in Medicines)

vi
viii
PPIA Pencegahan Penularan HIV dari Ibu ke Anak (Prevention of the Tranmission of HIV from Mother to Child)
PPNI Persatuan Perawat Nasional Indonesia (Indonesian National Nurses Association)
Puskesmas Pusat Kesehatan Masyarakat (Community Health Centre)
Pusrengunakes Pusat Perencanaan dan Pendayagunaan Tenaga Kesehatan (Center for Health Personnel Plannning and Utilization)
Pustanserdik Pusat Standardisasi, Sertifikasi dan Pendidikan (Center for Standardization, Certification and Education)
RAD Rencana Aksi Daerah (Regional Action Plan)
RAN Rencana Aksi Nasional (National Action Plan)
RB Rumah Bersalin (Birthing House/Maternity Hospital)
Rifaskes Riset Fasilitas Kesehatan (Health Facility Research)
Riskesdas Riset Kesehatan Dasar (Basic Health Research)
RPJMD Rencana Pembangunan Jangka Menengah Daerah (Regional Medium-Term Development Plan)
RPJMN Rencana Pembangunan Jangka Menengah Nasional (National Medium-Term Development Plan)
RPJPN Rencana Pembangunan Jangka Panjang Nasional (National Long-Term Development Plan)
RS Rumah Sakit (Hospital)
SDKI Survei Demografi dan Kesehatan Indonesia (Indonesian Demographic Health Survey)
SJSN Sistem Jaminan Sosial Nasional (National Social Security System)
SPOG Spesialis Obstetri dan Ginekologi (Gynaecology and Obstetrics Specialist)
SUSENAS Survey Sosial Ekonomi Nasional (National Socioeconomic Survey)
UKS Usaha Kesehatan Sekolah (School Health Programme)
UTD Unit Transfusi Darah (Blood Transfusion Unit)
WHO World Health Organization
WUS Wanita Usia Subur (Reproductive Age Women)

vii
ix
LIST OF FIGURES
Figure 1 : Causes of maternal mortality 2010 .......................................................................................... 3
Figure 2 : Framework of Pathway Concept of Maternal Mortality .......................................................... 5
Figure 3 : Proportion of the public hospitals that meet the 17 criteria for hospital that provide PONEK for 24 hours .............................................................................................................................. 9
Figure 4 : Proportion of mother receiving danger signs of pregnancy in 2010 .................................... 10
Figure 5 : National Action Plan Framework for the acceleration of MMR Reduction 2013 - 2015 ....... 11

viii
x
LIST OF TABLES
Table 1 : Data on normal delivery care quality ........................................................................................ 8
Table 2 : Data on Antenatal Care Quality ................................................................................................ 9

11
CHAPTER I
INTRODUCTION
A. Background Maternal mortality is a result of the interaction of various aspects, which include clinical aspects, health care system aspects and non-clinical aspect affecting the clinical service delivery and implementation of the optimal health care system. Therefore, a common perception and understanding of the stakeholders on the importance and the role of these aspects in addressing maternal mortality are required, and the strategies to address the maternal mortality should be a comprehensive integration of these various aspects. Based on the estimation derived from IDHS in 1990 until 2007 that uses the exponential calculation, the maternal mortality rate in Indonesia in 2015 is 161/100.000 live births, while the MDG target of Indonesia is 102/100,000 live births. The Presidential Instruction No. 3 of 2010 on equitable development requires all governors, head of districts and mayors to prioritize the achievement of the MDG targets in their regional development programs as outlined in the Regional Action Plan for MDGs achievement. In focusing the achievement of MDG Goal 5, that is improve maternal health, the collaboration of all stakeholders to perform effective, efficient and consistent measures is required to accelerate the maternal and neonatal mortality rate reduction in Indonesia. Therefore, the Ministry of Health establishes an action plan for the acceleration of maternal mortality rate reduction 2013-2015, which focuses on 3 strategies and 7 main programs. This Action Plan is expected to create the same understanding for all stakeholders about the concept of maternal and neonatal mortality and the effective and efficient measures to prevent them. These efforts require a strong commitment from all stakeholders to accelerate maternal mortality rate reduction in Indonesia, which is set forth in the Regional Action Plan.
B. Goal
General Achieve the maternal mortality rate target in Indonesia, which is 102/100.000 live births in 2015, and meet the maternal mortality rate target in the regions according to the Regional Action Plan/MDGs/Regional Mid-Term Development Plan for the regions that have achieved the national target.
Specific a) Describe the presidential vision, mission and program that are developed based on the
National Long-Term Development Plan 2005-2025. In this plan, the maternal mortality rate is targeted to fall from 307/100.000 live births in 2008 to 118/100.000 live births in 2014.
b) Provide guidance and directions for the implementation of maternal and neonatal health development at national, provincial, district and city levels, both for the government

2
2
institutions and the community and other stakeholders involved in the improvement of maternal and neonatal health.
c) Focus on improving the health care system to ensure the availability of access to quality obstetric and neonatal care.
C. Target Decision makers at national, provincial, district/city level; program managers; health professionals; professional organizations; community organizations; business sector; and groups that are concerned with maternal health.

3
3
CHAPTER II
SITUATION ANALYSIS
A. Maternal Mortality
1. Definition of maternal mortality According to ICD 10, maternal mortality is defined as "the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.” The definition explicitly explains that maternal mortality covers a wide scope, which is not only related to the deaths during delivery, but also includes the death of mothers during pregnancy and postpartum. The definition also distinguishes maternal deaths into two categories. The first is a death caused by direct obstetric causes, that is the death directly resulting from pregnancy and childbirth. The second is a death caused by indirect causes, that is the death resulting from previous existing diseases, and is not due to pregnancy or childbirth.
2. Direct causes of maternal mortality Globally, the five major causes of maternal death are hemorrhage, hypertension in pregnancy, infection, obstructed labor and abortion. In Indonesia, maternal mortality is still dominated by three main causes of death, which are hemorrhage, hypertension in pregnancy and infection, but the proportion of these three causes of death have changed. Hemorrhage and infection are decreasing, while hypertension in pregnancy is increasing, with almost 30% of maternal mortality in Indonesia in 2010 are due to hypertension in pregnancy.
Figure 1: Causes of maternal mortality 2010
(Source: Population Census 2010)
A. Mate 1. De
Aprthm Thonpr Thcachfr
2. DiGprstprHwpr
ernal Morta
efinition of ccording toregnant or whe site of the
management
he definitionnly related tregnancy an
he definitionaused by dirhildbirth. Throm previou
irect causeslobally, theregnancy, intill dominateregnancy anemorrhage
with almost regnancy.
ality
maternal mo ICD 10, mwithin 42 dae pregnancyt, but not fro
n explicitly eto the death
nd postpartu
n also distinrect obstetrhe second iss existing di
s of maternae five majonfection, obed by three
nd infection,and infectio32% of mat
F
SITUA
mortality maternal moays of termiy, from any om accident
explains thahs during deum.
nguishes maric causes, ths a death cseases, and
al mortalityr causes of
bstructed lae main caus, but the proon are decreternal morta
igure 1: Cau
3
CHAPTER IIATION ANA
ortality is dination of pcause relate
tal or inciden
t maternal melivery, but
aternal deathat is the decaused by in is not due t
f maternal bor and abo
ses of deathoportion of easing, whilality in Indo
uses of mate
I ALYSIS
defined as "regnancy, ir
ed to or aggntal causes.
mortality coalso include
hs into twoeath directlyndirect causto pregnanc
death are ortion. In Inh, which arethese threele hypertensonesia in 20
ernal mortal
"the death rrespective ravated by t”
overs a widees the death
categories.y resulting fses, that is cy or childbi
hemorrhagndonesia, me hemorrha causes of dsion in preg
010 are due
ity 2010
of a womaof the durathe pregnan
e scope, whih of mother
. The first isfrom pregnathe death rrth.
ge, hypertematernal mo
ge, hypertedeath have cgnancy is ince to hyperte
(Source: PopCensus 2010
an while tion and
ncy or its
ch is not rs during
a death ancy and resulting
nsion in ortality is ension in changed. creasing, ension in
pulation )
Post-partum hemorrhage
20%
Amnion defect
2%
Prolonged labour
1%Abortus
4% APB3%
Others7%
Hypertension in pregnancy
32%
Puerpural Complication
31%
3
CHAPTER II
SITUATION ANALYSIS
A. Maternal Mortality
1. Definition of maternal mortality According to ICD 10, maternal mortality is defined as "the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.” The definition explicitly explains that maternal mortality covers a wide scope, which is not only related to the deaths during delivery, but also includes the death of mothers during pregnancy and postpartum. The definition also distinguishes maternal deaths into two categories. The first is a death caused by direct obstetric causes, that is the death directly resulting from pregnancy and childbirth. The second is a death caused by indirect causes, that is the death resulting from previous existing diseases, and is not due to pregnancy or childbirth.
2. Direct causes of maternal mortality Globally, the five major causes of maternal death are hemorrhage, hypertension in pregnancy, infection, obstructed labor and abortion. In Indonesia, maternal mortality is still dominated by three main causes of death, which are hemorrhage, hypertension in pregnancy and infection, but the proportion of these three causes of death have changed. Hemorrhage and infection are decreasing, while hypertension in pregnancy is increasing, with almost 30% of maternal mortality in Indonesia in 2010 are due to hypertension in pregnancy.
Figure 1: Causes of maternal mortality 2010
(Source: Population Census 2010)

4
4
3. Indirect causes of maternal mortality The definition of maternal mortality indicates that maternal mortality does not only include the deaths caused by delivery, but is also related to deaths caused by non-obstetric causes. An example is a pregnant woman who dies from tuberculosis, anemia, malaria, heart disease, etc. These diseases are considered to aggravate pregnancy, increase the risk of morbidity and mortality. The proportion of indirect causes of maternal deaths in Indonesia is quite significant, which is about 22%, so attention should be given to prevention and treatment. In dealing with the indirect causes, coordination with other medical disciplines in a hospital or between hospitals, such as with internal medicine and surgery, is required.
4. Maternal mortality in Millenium Development Goals Indicator for improved maternal health in the Millennium Development Goals (MDGs) is a reduction of maternal mortality rate associated with improved childbirths attended by skilled health personnel (MDG Target 5a). But this effort is not enough, because reducing maternal mortality rate can not be done simply by addressing the direct causes, but also by overcoming the indirect causes. Therefore, the efforts to reduce maternal mortality rate should also be supported by other reproductive health-related efforts, including increased antenatal care coverage, declined adolescent birth rate, increased contraceptive prevalence rate and declined unmet need of family planning. The four indicators are set forth in the MDG Target 5b: universal access to reproductive health, while the last two additional indicators are the efforts of the family planning program. The "4 Too" factor (too young, too close, too many and too old) is one of the indirect causes of maternal mortality that can be overcome with family planning services.
B. Pathway of maternal mortality
It is estimated that 15% pregnancy and birth will have complications. Most of these complications can be life-threatening, but most of them can be prevented and treated if: 1) the mothers immediately seek medical treatment, 2) the health personnel perform the appropriate treatment procedures, including using a partograph to monitor the progress of labor and implementation of the active management stage III to prevent postpartum hemorrhage; 3) the health personnel are able to identify early complications; 4) if complications occur, the health personnel are able to provide first aid and perform stabilization to the patients prior to making referral; 5) the referral process is effective; 6) the hospital services are prompt and appropriate. Thus, the complications that require treatment in a hospital need a continuum of care, covering the basic services through hospital services. The above mentioned step 1 through step 5 will not be helpful if the step 6 is inadequately performed. On the contrary, the adequate hospital care will not be beneficial if the patient suffering from complications is not referred to hospital services (Figure 2)

5
5
Figure 2. Framework of Pathway Concept of Maternal Mortality
C. Principles of maternal mortality prevention Most of the maternal deaths should be preventable, because most obstetric complications can be handled. At least there are three conditions that need to be observed to save a mother:
a) First, obstetric complications are unpredictable, so they will occur to any pregnant
woman at any time (during pregnancy, childbirth or postpartum, especially the first 24 hours after delivery). This condition puts any pregnant woman at risk of having obstetric complications that may threaten their life.
b) Secondly, every pregnancy has a risk, so every pregnant woman should have an
access to adequate services required when complications occur. Most complications can be life-threatening and should be immediately attended at the hospitals that can provide obstetric and neonatal emergency care.
c) Thirdly, most of the maternal deaths occur during delivery and in the first 24 hours after delivery, which are a very short period, so the access and quality of care in this period should be prioritized to give high leverage in reducing maternal mortality.
In reality, preventive measures and treatment of complications mentioned above are not usually performed, because of the delays, which include:
A pregnant/giving birth mother dies because the complications they are suffering from are not attended in timely and appropriate manner
Family Planning
Soruce: Endang Achadi
6. PrincMostcan moth a) Fi
whoco
b) Se
adthob
c) Th
desh
In reusua
KeluargaBerenca
F
ciples of mat of the mabe handledher:
irst, obstetrwoman at an
ours after domplication
econdly, evedequate serhreatening bstetric and
hirdly, mostelivery, whihould be pri
eality, preveally performe
A pregnan
a na
Figure 2. Fram
aternal mortternal deat. At least t
ric complicny time (duelivery). Thi
ns that may
ery pregnanrvices requiand should
d neonatal e
t of the match are a veoritized to g
entive meased, because
t/giving birtfrom are
mework of P
tality prevenhs should bthere are th
ations are ring pregnais condition threaten th
ncy has a riskired when c
d be immedmergency ca
ternal deathery short pegive high lev
sures and tre of the delay
th mother dnot attende
5
Pathway Co
ntion be preventahree condit
unpredictaancy, childb
puts any preir life.
k, so every pcomplicatiodiately atteare.
hs occur dureriod, so theverage in red
reatment ofys, which in
dies becaused in timely
ncept of Ma
ble, becausions that n
ble, so theirth or postregnant wo
pregnant woons occur. Mended at th
ring deliverye access andducing mate
f complicaticlude:
e the compy and appro
aternal Mort
e most obsteed to be o
ey will occutpartum, esman at risk
oman shoulMost complihe hospitals
y and in thed quality of
ernal mortal
ions mentio
plications thopriate man
tality
tetric compobserved to
ur to any ppecially the
k of having o
ld have an aications cans that can
e first 24 hof care in thiity.
oned above
hey are suffenner
Soruce:Endang
plications o save a
pregnant e first 24 obstetric
access to n be life-
provide
urs after s period
are not
ering
: g Achadi
Family Planning
I. Skilled birth attendants in health facilities
III. Quality of care at hospital
Timely access to hospital
II. Effective Referral
Mothers saved
15% of complication cannot be predicted but can be prevented
85% normal
Fees
?
Quality of Care• Complication prevention• Complication Identification• First Aid to complication and stabilization prior to refer
Pregnancy

6
6
a) Delays in making a decision Delays in making a decision at the community level are attributed to the following conditions: 1) The mother is late to seek assistance from health professionals despite the available
access to them for 24 hours a day and 7 days a week due to the constraints of traditions/beliefs in decision-making in the family, and the inability to provide non-medical costs and other medical costs (particular type of medicines, blood type check, transportation to find blood/medicines, etc.).
2) The family is late to refer the mother to health professionals due to lack of understanding about the life-threatening signs.
3) The health professionals are late to perform the preventive measures and/or identify the complications early due to lack of optimal competence, such as handling normal delivery care according to the standard and providing first aid for obstetric and neonatal emergency.
4) The health professionals are not able to advocate the importance of making a prompt referral to the patient and her families to save the mother's life.
b) Delays in reaching the referral hospitals and ineffective referral, which can be caused
by: 1) Geographical issues 2) Constraints of means of transport 3) Stabilization of patients with complications (such as pre-shock) is not
performed/not effective, because the health professionals’ skills are not optimal and/or the medicines/medical devices are not available.
4) Monitoring of the referred patients is not performed or performed but is not followed by necessary actions.
c) Delays in getting adequate care in referral hospitals, which can be caused by
1) Ineffective administrative system of emergency care in hospitals. 2) The required health professionals (obstetrician/gynecologist, anesthesiologist,
paediatrician, etc.) are not available. 3) Lack of skillful health professionals despite available access to them 4) Incomplete/unavailable infrastructure, such as emergency room, delivery room,
medical instruments and medicines. 5) Blood is not immediately available 6) Patients arrive at the hospital in a critical condition that is difficult to save. 7) Lack of clear admission procedure for emergency cases to prevent rejection of
patients or to make an effective referral to other hospitals. 8) Lack of information for the community about the capacity of the health care
facilities that are referred to in handling obstetric and neonatal emergency, so adequate service is not obtained
D. Program Achievement
One of the massive government efforts to reduce maternal mortality rate is the program that assigns midwives in the villages, which has been initiated since the 1990s. The program aims to bring people's access closer to the health services for mothers and newborns, especially during pregnancy and childbirth. However, since the midwife education only

7
7
takes a short time, approximately 54,000 in 6 years, the quality of some midwives still needs to be improved to meet the standards of competence Based on the regular reports on maternal health from the Provincial Health Office in 2011, until today there are 66,442 village midwives that are registered, but only about 54,369 of them (82%) live in the villages. In addition, village midwives’ ability in providing standardized delivery care is hampered by housing facilities that also serve as a village health post. The Indonesia Health Profile Data of 2011 shows that the number of village health posts in 2011 are only 53,152. In addition, the number of midwives who have received training on normal delivery care is only 35,367 (52.6%). The training components include the active management stage III to prevent partial postpartum hemorrhage and the use of partograph to detect problems in delivery process. Since not all villages have a midwife, and only some midwives are trained to have adequate skills, delivery care that meets the standards can be performed in health care facilities (community health centers that provides inpatient care or basic obstetric and neonatal emergency care/PONED). Delivery in health care facilities has several advantages: there are more than one health personnel to attend the delivery, especially in the case of complications, and thus monitoring of patients can be done more intensively by turns; overcome the shortage of midwives as rotational assignments can be done in a health care facility; since the delivery is not taken place at the patient’s home, family pressure and unfavorable conditions of the house for the midwife can be avoided; the availability of equipment and medicines in the health care facilities is more certain; health care facilities are usually located in the area from which it is more convenient to reach the hospital. The implementation of normal delivery care standards in basic health facilities has met the expectation as shown by the declining proportion of hemorrhage and infection. However, the quality of maternity care still needs to be improved. The results of Quality Maternal Health Services Study in 2012, which was conducted in 20 districts/cities in Indonesia, show that the adherence of health professionals in using a partograph, performing a physical examination and documenting the examination results is still low, whereas a thorough physical examination and proper use of a partograph can prevent delivery complications. (Table 1)

8
8
The maternal and neonatal deaths are highly influenced by the promptness and and accuracy of the measures taken during emergency. The existence of the community health centers that have a capacity to provide PONED is a solution to bring the public access closer to obstetric and neonatal care to prevent complications and/or get a first aid during obstetric and neonatal emergency on the conditon that the service provided meets the adequate standards of care. However, the coverage and quality of basic services still need to be improved. The data from the 2011 health facilities research shows that 241 districts in Indonesia (60%) do not have 4 community health centers that provide PONED per district as required. Only 69.7% of community health centers have a medical device to check the hemoglobin (Hb) and only 42.6% of community health centers that provide PONED have MgSO4, while hemorrhage and eclampsia are two major causes of maternal death. Of all the community health centers that provide emergency care, including PONED, only 76.5% have a means of transportation (ambulance or motor boat). Most obstetric and neonatal emergency cases can be treated in a basic health care facility using a simple technology, so the improved emergency obstetric and neonatal emergency care at community health centers should provide a substantial contribution to the prevention of maternal and neonatal mortality. Hospital as a final referral place of obstetric and neonatal cases has an important role in saving mothers and newborns, because about 5-15% of complications cases require actions that can only be performed at hospitals, such as caesarean sectio and blood transfusions. The 2011 Health Care Facilities Research shows that only 7.6% of public hospitals meet the 17 criteria for hospitals which have the capacity to provide PONEK for 24 hours and 7 days a week (Figure 3). Lack of means and retention of Obstetrician and Gyneacologist is the major cause that makes a hospital unable to provide PONEK for 24 hours and 7 days a week.
NORMAL DELIVERY CARE Hospital* Community health center*
Complete the medical record 68,6% 61,4% Complete the general physical and obstetric examination
52,1% 57,3%
Use a partograph 41,0% 68,3% Use a cardiotography (CTG) 19,0% 2,5%
Perform delivery care stage I 73,8% 83,8%
Observe indication and symptom stage II 80,0% 85,0% Prepare delivery care 60,6% 65,8% Ensure full opening of the cervix 72,5% 77,5% Ensure good condition of the fetus 77,5% 75,0%
Document the examination results 20,0% 42,5%
Table 1: data on normal delivery care quality
(Source: Quality maternal health services study, Min. of Health- WHO-HOGSI, 2012)

9
9
Figure 3: Proportion of the public hospitals that meet the 17 criteria for hospitals that
provide PONEK for 24 hours (Source: Basic Health Care Facilities Research 2011)
One of the successful prevention of maternal mortality lies in the accuracy of decision making in the event of complications. It can be achieved if the family has a good basic knowledge about pregnancy and childbirth, so they can make a delivery planning and are prepared to face the complications as early as possible.
Table 2: Data on Antenatal Care Quality
ANTENATAL CARE Hospital* Community
health center*
Complete the medical record 33,86% 48,52% Complete the general physical and obstetric examination
50,00% 59,38%
Provide counseling and education 24,17% 45,00%
Perform regular supporting examination 39,38% 19,69%
Perform supporting examination in the event of indications
49,00% 52,50%
Provide supplements and vaccination 62,50% 73,13%
The results of the 2010 Basic Health Research shows that about 45% of mothers claim to receive information about the danger signs of pregnancy during ANC (Figure 4). This is reinforced by the results of the 2012 Maternal Care Quality Study that shows that only 24% of hospitals and 45% of community health centers perform appropriate counseling and education according to the current standard during ANC. Both of these indicate that the role of health professionals in providing information and advocacy to mothers and families during ANC is still weak, so the knowledge of families and communities to develop a childbirth planning is also poor (Table 2).
(Source: Maternal Care Quality Study, Min. of Health-WHO-HOGSI, 2012)

10
10
Figure 4: Proportion of mothers receiving danger signs of pregnancy in 2010 (Source: Basic Health Care Research 2010)
Delivery Planning and Complications Prevention Program, which was introduced in 2007, was implemented in 63,000 villages across Indonesia in 2011. It is necessary to ensure the implementation of this program in these villages to help families develop a delivery planning and realize the plan well in time.
Other activities prior to this program that involve the community is Mother Friendly Movement which was popular in the year 2000s. Unfortunately this activity has faded lately, whereas it is considered to be quite capable of raising the maternal health issues in the community because it increases the decision makers’ concern at all government levels. The integration of strengthened delivery planning and complication prevention program, alert villages and Mother Friendly Movement is one of the solutions to empower families and communities in maternal health.
The measures to reduce maternal mortality rate can not be separated from the family planning
services, as they are related to the prevention of unwanted pregnancy and the 4-too factors. But in the last 10 years the participation rate of modern family planning (Contraceptive Prevalence Rate/CPR) only increases very slightly, which is from 56.7 % (2002) to 57.9% (2012). The rate of unmet need of family planning participants also declines very slightly, from 8.6% (2002) to 8.5% (2012). The measures taken to increase CPR and reduce unmet need among others are including
family planning services in the maternity insurance package which has eliminated financial barriers in obtaining family planning services, and utilizing an integrated antenatal care,
maternal class and Delivery Planning and Pregnancy Prevention Program to improve mothers’ and families’ knowledge about family planning.
Mothers receive information about the danger signs of pregnancy

11
11
CHAPTER III
NATIONAL ACTION PLAN
A. Goal
Accelerate the reduction of maternal and neonatal mortality and morbidity rate in Indonesia.
B. Challenge, Strategy and Main Program The National Action Plan is implemented in the decentralization context in the form of the Regional Action Plan, which ensures a steady integration in health development planning and budget allocation process. It focuses on mothers and newborns health care according to the current standard, which is cost-effective and based on the evidence at all health care levels and health referrals in both government and private sectors.
Figure 5: National Action Plan Framework for the Acceleration of MMR Reduction 2013 – 2015
11
CHAPTER III
NATIONAL ACTION PLAN
A. Goal
Accelerate the reduction of maternal and neonatal mortality and morbidity rate in Indonesia.
B. Challenge, Strategy and Main Program The National Action Plan is implemented in the decentralization context in the form of the Regional Action Plan, which ensures a steady integration in health development planning and budget allocation process. It focuses on mothers and newborns health care according to the current standard, which is cost-effective and based on the evidence at all health care levels and health referrals in both government and private sectors.
Figure 5: National Action Plan Framework for the Acceleration of MMR Reduction 2013 – 2015
Challenges :
1.Community access to health facilities already increased but coverage and quality of care are not optimal yet
2.Limited strategic resources for maternal and neonatal health
3.Community knowledge and awareness on maternal health are still low
Strategy :
1.Improve coverage and quality of maternal health care
2.Enhance local government and private sector’s role in maternal health efforts
3.Family and community empowerment
MMR 102/ 100,000 LB (2015)
Main program :1. Assurance of village midwifecompetence according to the standard
2. Assurance of the availability of health care facilities that can provide delivery care 24/7 according to the standard
3. Assurance of the function of all PONED community health centers and PONEK hospitals in at district/city level to work 24/7 in accordance with the standard
4. Assurance of the implementation of effective referral for complications cases
5. Assurance of Local Governments Support for the Implementation of the Acceleration of Maternal Mortality Rate Reduction Program
6. Improvecross-sectoral and private sector partnership
7. Improved Understanding and Implementation Program of the Delivery Planning and Complications Prevention Program (P4K) inthe Community

12
12
1. Challenges Three main challenges related to the acceleration of maternal mortality rate reduction are access to the quality services in health care facilities that is not optimal, limited strategic resources for maternal and neonatal health, and community knowledge and
awareness on maternal health are still low.
2. Strategies used to achieve the maternal mortality target in 2015 2.1. Improved coverage and quality of maternal health care
Very strong evidences suggest that the life safety of women during pregnancy, childbirth and puerperium is strongly influenced by the access to quality obstetric care at all times, especially since every pregnancy and childbirth have a risk of life-threatening complications. The concept of continuum of obstetric care that is delivered in the previous chapter underlies the significance of the improved coverage and quality of care as such that every woman who is undergoing complications during pregnancy and childbirth has an access to the quality health care in a timely and appropriate manner. This continuum of care is particularly important during the period of laboring process and during the first 24 hours after delivery for in these very short periods the majority of maternal deaths occur. Access to health care for certain cases that can aggravate the condition of women during pregnancy, childbirth and puerperium, and for the cases that have widespread health and social implications in the future, namely anemia, malaria in endemic areas, HIV and AIDS, post abortion care and teen pregnancy, needs attention significantly.
2.2. Enhancing the role of local governments in the regulations that can effectively support the implementation of the program Health care system is a part of a public service system that is in some aspects is highly regulated by local policies and regulations, such as the provision and placement of health professionals and supporting health personnel, and the provision of health infrastructure. Health professionals are at the forefront of the implementation of health care programs. Therefore, the policy on health professional assignment has a very strategic position that needs to be regulated clearly and firmly. The policy needs to be complemented with a clear application of reward and punishment, both for specialists, medical doctors, midwives, and other health-related personnel. Since the optimal health care outcomes are strongly influenced by the quality of service, the assurance of health professional competence requires attention through various actions, including adequate pre-service education, in-service training for health professionals, appropriate implementation of health

13
13
professionals’ authorities, certification for health professionals and health care facilities, and audit of health professionals’ services and health care facilities. The role of local and central government in the regulation about the availability and quality of health professionals is expected to function effectively. The availability of competent personnel is not enough without the support of adequate means and infrastructure, including the availability of blood 24/7. Good coordination between the blood transfusion unit of general hospitals at district level and the Indonesian Red Cross, the blood transfusion unit of genral hospitals at provincial level and the blood transfusion unit of private hospitals in the provision of blood for patients is necessary. Strengthening the referral system requires a strong support from the local governments and other stakeholders as such that patients who are referred are attended immediately. Support is very much needed given the referral process requires involvement of various stakeholders, namely the community, health professionals and basic health care faclities, hospitals (public and private) including blood transfusion unit of hospitals and the Indonesian Red Cross. Regionalization which is adapted to the conditions of each region needs to be considered to clarify the referred destination. Regionalization include clusters of island, coast, urban area and the nearest district, etc. In this case, support through gubernatorial regulations may help the referral regionalization efforts. The role of private sector in health care to public can not be ignored given the capacity of the government health care facilities is limited and lately people tend to choose the health care provided by private sector, especially in urban areas. Therefore, private sector should have an active role in jointly delivering the best health care that suits the public needs, regulated by a regional regulation. The explanation above indicates that a strong role of the local governments in regulating the optimal implementation of health care for public is essential, including regulating the role of various government sectors, the role of civil society organizations and private sector. The central government’s role needs to be coordinated in order to mutally complement the good implementation of health care in the regions.
2.3. Family and Community Empowerment
Decision on pregnancy and childbirth arrangement should be made together by a mother with her husband and her family. It is not a decision that is not desired by the mother, either because of medical reasons or other reasons related to readiness. Families should have an understanding that every pregnancy is desired by the mother, including when pregnancy is wanted and how many children are desired. It is also necessary to improve the knowledge and attitudes of family and society in general regarding the importance of understanding that every pregnancy has a risk of life-threatening complications, and therefore a planning for good delivery and

14
14
prevention, and for finding immediate help in the event of complications is required (the availability of transportation, funding and potential blood donors). Knowledge of the risk of complications in pregnancy, childbirth and puerperium as well as information about family planning are important to gain since adolescence, so teenagers can plan the right age to get married, the number of children desired and arrange the pregnancy interval. Education to improve the knowledge, understanding and participation of youth/community including teachers is given through youth friendly health service program that aims to prevent teens from having risky sexual behavior, such as unwanted pregnancy, whch may result in unsafe abortion and may ultimately lead to maternal death.
3. Main Program
The selected main program is the program that is considered to have high leverage for accelerating maternal mortality rate reduction, because it ensures the availability of quality services that can be accessed at any time, which include: 1. Mother and child health service delivery at village level in accordance with the
standards 2. Provision of basic health care facilities which are able to provide delivery care
according to the standard for 24 hours 7 days a week 3. Assurance of the entire PONED community health center and PONEK hospital for 24
hours 7 days a week to work according to the standard. 4. Implementation of effective referral in case of complications 5. Strengthening the district/city government in decentralized health governance
programs (regulation, financing, etc.). 6. Implementation of cross-sectoral and private partnership. 7. Improved behavior change and community empowerment through understanding
and implementation of delivery planning and complications prevention program and integrated service posts.
4. Program and Activities
4.1. Assurance of village midwife competence according to the standard 4.1.1. Provide health care facilities in the village (village health posts) at the
locations where access to a more complete service has not been met. Clarification about the functions of village health posts is needed based on the conditions of each region.
a. Provision of health care facilities at village health posts b. Provision of midwife kits, including Hb checking device
4.1.2. Improve midwife skills on delivery care and integrated antenatal care
a. Normal delivery care training: for village midwives who have not receive such training (including adequate hands-on training) and for midwives whose competence has not met the standards.
15
15
b. Integrated training on normal delivery care c. Training for midwives in providing counseling and education to the
community about maternal and infant health and nutrition, so the midwives can be more effective in changing people's attitudes and make them more vigilant in dealing with pregnancy and better prepared in the event of complications. The training programs must be equipped with the post-training evaluation component and periodic monitoring, for example through self assessment using checklists.
4.1.3. Maintain/improve the quality of mother and child health care by increasing facilitative supervision on village midwives.
4.2. Assurance of the availability of health care facilities that can provide delivery care 24/7 according to the standard
4.2.1. Improve detection and first aid for complications cases and effective referrals
a. Increase the number of community health centers which can provide delivery
care in accordance with the working standard 24/7 Complement/add maternity room at community health centers Complement the infrastructures, including medicines Train the community health centers’ team to work 24/7, including
performing detection and first aid for complications cases and effective referrals.
b. Conduct an integrated antenatal care, including prevention of HIV transmission from mother to child.
c. Conduct screening of hemoglobin examination for any mother who checks their pregnancies at health care facilities.
4.2.2. Increase the number of health care facilities that can handle complications:
a. Increase the number of community health centers that provide PONED 24/7 : Fill/add PONED trained team. Ideally, 2 trained teams are available in
every community health center that provides PONED, so the service is available for 24 hours 7 days a week. In circumstances where two teams can not be afforded, it is expected that an in-house training can be given to the staff of community health centers.
Complement the facilities and infrastructures of community health centers that provide PONED, including medicines
Conduct a refreshment training for the existing PONED team given complications cases are rarely encountered
Ensure the availability of referred means of transportation and adequate communication

16
16
b. Establish community health centers which can provide PONED 24/7 in remote areas and islands, with special guidance and supervision from PONEK hospitals, so community health centers that provide PONED and effective referral can function properly.
4.2.2.1. Build coordination and cooperation with referral hospitals, which are located
in the same region and in other regions (provincial hospitals, hospitals in border regions, military hospitals, private hospitals) to expand the access to complications case referrals in hospitals.
4.2.3. Optimize the utilization of health insurance for eligible people (maternity insurance, national social security system) by: a. Building coordination with various stakeholders to implement maternity
insurance/national social security system at every level of service, so the main tasks and functions of every stakeholder are clear.
b. Providing information to the public about the rights and obligations related to health insurance.
4.2.4. Improve quality of service
a. Improve the skills of health professionals at basic level using a variety of approaches, including training, apprenticeship, and in-house training, to make them competent in performing normal delivery care, including prevention of complications, so the cases referred to the hospitals are not normal delivery cases. Conversely, improve the ability of health professionals to be able to identify complications cases early, provide first aid for complications cases and make a referral for cases that require effective treatment in hospital, including monitoring and stabilizing the patients during referral process so they arrive at the hospital in timely and appropriate manner.
b. PONEK hospitals provides guidance for PONED community health centers c. Perform the Maternal Perinatal Audit on maternal and neonatal mortality
cases and provide the follow-up actions. d. Implement back referral to allow the referrers learn from the results of
their actions and continue to perform the monitoring of post-hospitalized patients.
e. Conduct facilitative supervision on PONED services performed by a coordinating district midwife or other designated health professionals.
4.3. Assurance of the function of all PONED community health centers and PONEK hospitals in at district/city level to work 24/7 in accordance with the standard 4.3.1. Improve the quality of health personnel in referral hospitals in handling
complications cases in a timely and appropriate manner, including the availability of service standards guidelines for complication cases
4.3.2. Build coordination and cooperation with other referral hospitals, either in the same region or the nearest region, which are the hospitals of higher type, private hospitals/maternity hospitals and military hospitals, to expand
17
17
the access for complications cases to the hospitals as part of a referral network.
4.3.3. Ensure the access to safe blood a. Improve and strengthen the cooperation with the Indonesian Red Cross. b. Improve the function of blood transfusion unit c. Ensure all hospitals have a hospital blood bank d. Establish a network of inter-hospital blood provision, both between
hospitals in the same region and or in different region, to improve the cooperation between hospitals, both in the same region and outside the region (province or district and other cities) on blood provision.
4.3.4. Improve postpartum family planning services in collaboration with other
relevant sectors, notably hospitals and the National Family Planning Coordinating Board.
4.3.5. Ensure the availability of obstetric and neonatal care at any time (24 hours 7 days) a. Complement/add personnel to ensure the service delivery for 24/7:
At least 1 team that is able to perform PONEK or handle emergency cases is available with such arrangement that the services are available for 24 hours 7 days. In circumstances where a full team can not always be available, it is expected that an in-house training is given by the trained team/staff to other hospital staff, so the service can still be provided. In circumstances where there is no PONEK team or team that can provide emergency care, especially in remote areas and islands, it is necessary to consider specific approach, including building cooperation with post-graduate training institutions and provincial hospitals. The team includes caesarean section operators (obstetrician and gynecologist/post-graduate student of obstetrics), anesthesia operators (anesthesiologist/post-graduate student of anesthesiology, assistant), midwives and nurses.
b. Complement/add the facilities and infrastructure: operating room and its priority use arrangement, C-section kits, medicines, blood, etc.
c. Conduct innovative approaches for the hospitals undergoing human resources shortage, particularly in remote border areas and islands. Provision of guidance model and assignment of personnel from larger hospitals in the same region or outside the region (provincial hospitals or nearest hospitals) in regional hospitals are an alternative to be explored. For example is the sister hospital program which supports mother and child health revolution program in East Nusa Tenggara, so the continuum of care can be provided.
4.3.6. Improve the quality of mother and child health care
a. Improve the skills of health professionals: midwives, physicians and specialists, through trainings, apprenticeships, in-house trainings and guidance.

18
18
b. Conduct audits on every maternal and neonatal death occurring in the hospitals.
c. Optimize supervision and quality assurance in the hospitals. d. Use a service edict to increase the role of the society in improving the
service quality.
4.3.7. Strengthen the health care system in hospitals a. Develop/modify policies in health care facilities: admission flow and
handling of obstetric and neonatal emergency cases, availability and proper functioning of the emergency room, etc.
b. Implement back referral made by the hospitals to the referrers, so the referrers can get a learning and perform monitoring of the post-hospitalized patients.
4.4. Assurance of the implementation of effective referral for complications cases 4.4.1. Ensure the availability of referral guidelines.
a. Develop/establish clear referral guidelines at national level. b. Develop/establish clear referral guidelines and operations at local level,
including the function and role of every level of service, as such that the service is utilized as needed.
c. Develop guidelines for back referral, which is made by the hospitals to the referrers.
d. Develop guidelines for referral system for patients who use the maternity insurance program/National Social Security System or other government health insurance programs.
4.4.2. Ensure the availability of firm referral system: a. Develop/strengthen a mutually agreed networking system, which includes
"Vertical Reference Network" between basic services and services at a higher level (hospital services), and "Horizontal Referral Network" between hospitals (public and private); between village midwives or midwives at a community health center and the Central Statistics Agency, between a PONED community health center and a maternity hospital, etc.
b. Develop/strengthen a mutually-agreed regional networking system, especially to handle remote and border areas.
c. Develop a referral communication system that has two objectives as follows: a. Provide service guidance (by an obstetrician/gynecologist to general
practitioners or midwives in the field, by a senior midwife to midwives in the field, etc. )
b. Obtain a confirmation about the availability of the referral hospital services (the availability of doctor, bed, blood, medicines, etc.).
d. Strengthen the admission and handling system for emergency cases in the hospitals, including handling flow, coordination with obstetrician or post-graduate students of obstetrics, and coordination with other specialists associated with maternal deaths due to indirect causes.
e. Develop/strengthen a mutually-agreed networking system for remote areas and islands.

19
19
4.5. Assurance of Local Governments Support for the Implementation of the Acceleration of Maternal Mortality Ratio Reduction Program.
The local government support is generated through the District Team Problem Solving (DTPS) approach, which includes
4.5.1. Regulation on the procurement and assignment of health professionals a. Submit a proposal to the central and local governments to meet the manpower
needs at various levels of health care facilities, so people have access to maternity and neonatal services required at all times. The proposal includes Completing the manpower at PONED and PONEK health care facilities that do
not have trained personnel. Gradually assigning at least 1 PONED team, and if possible 2 teams PONED
health care facilities in certain areas gradually. Gradually assigning at least 1 PONEK team, and if possible 2 teams at PONEK
hospitals in certai areas. Ensuring the availability of medical specialists at PONEK hospitals or public
hospitals that have not obtained PONEK status. b. Submit a proposal to the local governments to secure the assignment of health
professionals who have received PONED/PONEK training, so they will not be transferred or replace them with other personnel who have equal capacity and have been previously prepared.
4.5.2. Regulation on the procurement and assurance of the availability of necessary
equipment and medicines in every health care facility. a. Improve and strengthen coordination with the national and local
governments, so the availability of necessary equipment and medicines is assured at all times, including the process of application, procurement, distribution, and storage
b. Improve and strengthen coordination with the Indonesian Red Cross regarding the blood provision, if necessary through a Memorandum of Understanding at local level.
c. Improve and strengthen coordination between hospitals, public and and private, both within the region and outside the region (provincial hospitals or the nearest hospital), in the provision of equipment, medicines and blood, if necessary through a Memorandum of Understanding at local level.
4.5.3. Regulation on the administrative and financial governance
a. Submit a proposal to the local governments to increase the regional budget allocation to support health activities that have a high leverage to achieve the MDG 5, that is the availability of continuum of care, which includes the availability of competent midwives, health care facilities capable of providing PONED and hospitals capable of providing PONEK

20
20
b. Submit a proposal to the local governments about the need for breakthrough efforts related to maternal and neonatal care, including considering the emergency aspects in service delivery (after working hours).
c. Submit a proposal to the local governments to make clear regulations for border and remote areas, including the regulation governing the referral system of obstetric and neonatal cases to facilitate the people in these areas to access the health care facilities nearby.
4.5.4. Regulation on improved quality/skills of health professionals
a. Submit a proposal to the local governments to improve the quality and clinical skills of health professionals through training, apprenticeship or other training programs.
b. Recommend licensing for establishing schools and colleges in the regions that refer to the applicable standards of professional competence. The local government can work together with the relevant professional organizations. Ministry of Health also oversees the implementation of teaching-learning process in medical educational institutions.
c. Conduct socialization of the Health Minister Decree of 2009 on health training through the board of human resources development and empowerment.
4.5.5. Regulation on maternal and neonatal health information system a. Develop guidelines on integrated recording and reporting system (vertically
and horizontally). b. Establish key indicators for monitoring and evaluation purposes c. Conduct an analysis and utilization of information as a basis for determining
policies and programs.
4.5.6. Assurance of support for other required regulations 1. Develop macro and fundamental policies related to community health
center. These policies include the concept of community health center, specific workforce and financial governance.
2. Develop regulations to determine priority health care areas. 3. Conduct socialization of the national referral guidelines (Health Minister
Regulation No. 1/2012). 4. Develop regulations on the referral system at district/city level. 5. Conduct advocacy on delayed marriage based on health considerations.
4.6. Cross-Sectoral and Private Partnership Improvement Program
Work with other sectors as follows:
1. Medical education institutions to work in local hospitals to ensure the availability of adequate service 24 hours/7 days, such as through the assignment of post-graduate students of obstetrics program.

21
21
2. Private sector which directly provides obstetric care (maternity hospitals, clinics, general hospitals) is expected to build coordination in providing obsetric care to the community, including in the referral system, through a Memorandum of Understanding (MoU) on Cooperation.
3. Private sector which has indirect roles (medical educational institutions, companies’ CSR program) is expected to work together to improve the obstetric coverage and care, either through the improved quality of students of health-related program based on the national standards, or through the utilization of CSR funds.
4. The National Family Planning Coordinating Board, to improve access for all women of childbearing age to information on reproductive health and access to family planning methods.
5. Primary and secondary education sectors, to increase access for all adolescents, especially girls, in schools (school health unit) to information on reproductive health. The implementation of 12-year compulsory education is expected to be utilized by the health sector to convey the information related to reproductive health and other health-related information.
6. Professional organization, to increase its role in improving the quality of services of its members, such as through training, apprenticeship, coaching and arrangement of professional licence registration. The local governments and the local health offices are expected to work with the professional organizations in accordance with their respective roles as agreed upon.
7. Religious sector, to improve access for all girls in religion-based schools, madrasah (school health unit) and all brides-to-be who register their marriage at the office of religious affairs, to information on reproductive health, including body readiness for first pregnancy.
8. Religious organizations can play a role in at least two aspects Delivery of health information, such as information on reproductive health and
health insurance (maternity insurance, national social security system), through the existing organization networks, and As part of the Local Health Service Network
9. Develop/improve other partnerships according to the circumstances and conditions of the regions.
4.7. Improved Understanding and Implementation Program of the Delivery Planning and Complications Prevention Program in the Community
4.7.1. Conduct a reorientation and reactivate the concept of community
preparedness in facing the delivery a. Conduct a reorientation for all relevant health personnel regarding the
delivery planning and complications prevention program to create the same and appropriate understanding about the program concept, including the purpose and benefits of the program, and the measures that must be taken.
b. Conduct an orientation for health cadres and communities about the danger signs of pregnancy and childbirth as well as their role in the delivery planning and complications prevention program.

22
22
c. Reactivate the mother friendly movement at all levels (national, provincial, and district)
4.7.2. Conduct an orientation about the importance of necessary measure during
pregnancy and childbirth a. Conduct maternal class using mother and child health guide book b. Socialize the danger signs of pregnancy and childbirth through appropriate
media to every segment of society in accordance with the acceptable culture and norms.

23
23
CHAPER IV
MONITORING AND EVALUATION
A. Achievement Indicator
1. Achievement of the Acceleration of Maternal Mortality Ratio Reduction Program a) Outcome Indicator
Maternal Mortality Ratio: The total number of maternal deaths (according to the definition of ICD 10) in a region divided by the total number of live births in the same region in a specified period of time, represented in unit per 100,000 live births
Delivery assisted by skilled attendants: The total number of births attended by health professionals in a region divided by the total number of women giving birth in the same region in a specified period of time, represented in percent.
Age Specific Fertility Rate, 15-19 years old
The total number of birth to women of a specified age group (15-19 years) per 1000 women of the same age group in the same region in a specified period of time, represented in per mil.
Antenatal care visit in 4 times during pregnancy : The total number of antenatal care visits in 4 times in a region, which are at least 1 time in Trimester 1, 1 time in Trimester 2 and 2 times in Trimester 3, divided by the total number of pregnant women in the same region in a specified period of time, represented in percent.
Delivery in health care facilities: The total number of births assisted by health professionals in health facilities (community health centers and hospitals) in a region divided by the number of women giving birth in the same region in a specified period of time, represented in percent. It is necessary to distinguish delivery in non-hospital health care facilities from delivery in hospitals.
Proportion of obstetric complications attended in the hospitals that provide obstetric and neonatal emergency care (PONEK hospitals or hospitals that have

24
24
not gained/do not gain PONEK status, but capable of providing emergency care): The total number of obstetric complications attended in a hospital (PONEK hospitals or hospitals that have not gained/do not gain PONEK status, but capable of providing emergency care) in a region, divided by the estimated total complications (= number of pregnancies * 15%) in the same region in a specifed period of time, represented in percent.
b) Output/Process Indicator: As outlined in the attached matrix, including policies and
regional regulations.
2. Regional Budget Allocation: trend and amount of the allocation in accordance with the needs of maternal and neonatal health programs.
3. Cross-sectoral and Private Cooperation: a cross-sectoral and private cooperation
document (MoU). B. Mechanism for monitoring of the National Action Plan for the Acceleration of
Maternal Mortality Ratio Reduction Monitoring of the National Action Plan for the acceleration of maternal mortality ratio reduction can be done using the monthly activity report of maternal health programs on
1) Strengthening and development of integrated recording and reporting system which
becomes the consensus on the data/information that needs to be collected regularly or periodically. It has a simple format but contains important information about maternal health (MDG 5 indicators and other output/outcome indicators which is considered important) and reporting flow (vertical from community health centers to the health office, and horizontal between hospitals and the health office).
2) Analysis of regular reports from provincial and district/municipal health offices on the key indicators, including health professionals’ delivery coverage, delivery at health care facilities, delivery location, number of maternal deaths and activity reports according to the established indicators.
3) Periodic dissemination of information on the development of key indicators of maternal and neonatal health to various stakeholders.
4) Supervision conducted in stages for provinces and districts/cities to directly identify the problems on the acceleration of maternal mortality rate reduction and try to solve them.
5) Monitoring and evaluation team meeting on the acceleration of maternal and neonatal mortality reduction that involves all relevant stakeholders, namely: Ministry of Internal Affairs, Ministry of Health, Ministry of National Development Planning/National Development Planning Board, Ministry of Women's Empowerment and Child Protection, National Family Planning Coordinating Board, Family Welfare Empowerment Movement Team, professional organizations (POGI, IDAI, IDSAI, IDI, IBI, PPNI, IAKMI), KARS, PERSI, Arsada, NGOs and maternal health oberservers organizations.
6) Data-based annual planning that is integrated with all of the available funding resources

25
25
In addition to regular/periodic data collection, other data that is available can be used for evaluation, such as SP, IDHS, SUSENAS, PODES, basic health research and health care facilities research.

26
26
Attachment:
Explanation about Matrix Strategy, Output, Program/Activities, Indicators, Targets and Implementation Actor
The following matrix describes the sub-programs or activities of the 7 main programs that need to be done in the period of 2013-2015 to accelerate the achievement of maternal and neonatal mortality rate target. The main programs selected for the National Action Plan 2013-2015 are the programs that focus on the continuum of care, which, if implemented entirely, has proven to have high leverage for reducing maternal and neonatal mortality rate. Therefore, although other programs are also important, within the next 3 years it is expected that the programs focus and activities refer to the 7 main programs. Each activity will have the indicators that will be used as the basis for periodic progress evaluation, which are conducted quarterly, annually or in other periods of time. Baseline data can be filled with the achievements in 2012 according to the available data. In circumstances where there is not any data at all, it should be denoted by "no data", then the data in 2013 is used as a baseline for evaluation in subsequent years. Annual achievement targets need to be filled in accordance with the existing conditions. Since the reduction of maternal and neonatal maternity rate involves cross programs and cross-sectors, including the government at national, provincial, district and city level, private sector, universities, professional organizations and communitis, the responsible party of every activity should be clarified. Thus the efficiency and effectiveness of the program can be achieved. It is expected that every province, district and city can fill in the Matrix in its Regional Action Plan

2725
Mat
rix
of S
trat
egy,
Out
put,
Pro
gram
/Act
ivit
y, In
dica
tor,
Tar
get,
and
Exe
cuto
r
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
Init
ial A
ctiv
ity
O
rien
tatio
n of
pat
hway
con
cept
and
con
tinuu
m o
f car
efor
all
heal
th
pers
onne
lare
nec
essa
ry, s
o th
ey h
ave
the
sam
e re
fere
nce
and
perc
eptio
ns a
bout
the
dire
ctio
n of
the
polic
y an
d pr
ogra
m
Impl
emen
tatio
n of
the
orie
ntat
ion
for
heal
th p
erso
nnel
at
nat
iona
l, pr
ovin
cial
and
di
stri
ct le
vel
All
dist
rict
s an
d ci
ties
have
rece
ived
th
e or
ient
atio
n by
the
end
of s
econ
d qu
arte
r 201
3
Stra
tegy
1: I
mpr
ovin
g co
vera
ge a
nd q
ualit
y of
mat
erna
l hea
lth s
ervi
ce d
eliv
ery
1.
A
ssur
ance
of
villa
ge m
idw
ife
com
pete
nce
acco
rdin
g to
the
stan
dard
1.1.
Prov
ide
heal
th
care
faci
litie
s in
vi
llage
s(vi
llage
he
alth
pos
ts)
1.1.
1. P
rovi
sion
of v
illag
e he
alth
pos
ts
Num
ber o
f vi
llage
hea
lth
post
s av
aila
ble
in a
sub
dist
rict
The
num
ber
of v
illag
e he
alth
pos
ts
incr
ease
s ev
eryy
eara
ccor
ding
to th
e ta
rget
of e
ach
regi
on, a
ndin
201
5the
nu
mbe
r of
vill
age
heal
th p
osts
ha
vein
crea
seda
t lea
stby
30%
co
mpa
red
to 2
012
(10%
per
year
)
Cent
er fo
r he
alth
pr
omot
ion
Min
. of H
ealth
, H
ealth
Off
ice
at
Prov
inci
al,
Dis
tric
t and
City
, Lo
cal
Gov
ernm
ent,
Re
gion
al
Dev
elop
men
t Pl
anni
ng B
oard
; pr
ofes
sion
al
orga
niza
tion

2826
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
1.
1.2.
Pro
visi
on o
f mid
wife
ki
ts e
quip
ped
with
H
b ch
ecki
ng d
evic
e
Num
ber o
f m
idw
ives
who
ha
s m
idw
ife k
its
in a
dis
tric
t and
ci
ty
By th
e en
d of
201
3 or
the
late
st a
t the
be
ginn
ing
of 2
014
all m
idw
ives
al
read
y ha
ve m
idw
ife k
its a
ccor
ding
to
the
stan
dard
Dir
ecto
rate
of
Mat
erna
l Hea
lth
1.2.
Impr
ove
mid
wife
sk
ills
on
child
birt
h an
d in
tegr
ated
an
tena
tal c
are
1.2.
1. N
orm
al d
eliv
ery
care
trai
ning
for
villa
ge m
idw
ives
Num
ber o
f m
idw
ives
who
ha
s at
tend
ed
the
norm
al
deliv
ery
care
tr
aini
ng a
nd/o
r ot
her s
kills
im
prov
emen
t tr
aini
ngs
Num
ber
of m
idw
ives
who
have
ad
equa
te
com
pete
ncet
hrou
ghtr
aini
ngsi
ncre
ase
ever
yyea
r acc
ordi
ng to
the
targ
et o
f ea
ch re
gion
.By
2015
allm
idw
ives
alre
ady
have
appr
opri
atec
ompe
tenc
e ac
cord
ing
to th
e st
anda
rd
Dir
ecto
rate
of
Mat
erna
l Hea
lth
1.
2.2.
Tra
inin
g on
in
tegr
ated
AN
C
Num
ber o
f in
tegr
ated
AN
C tr
aini
ngs
whi
ch
have
bee
n co
nduc
ted
Num
ber o
f the
inte
grat
edA
NCt
rain
ings
th
at h
ave
been
con
duct
ed in
crea
se
ever
yyea
r acc
ordi
ng to
the
targ
et o
f ea
ch r
egio
n. In
2015
the
AN
Cint
egra
tedt
rain
ing
has
been
im
plem
ente
dfor
allp
erso
nnel
Dir
ecto
rate
of
Mat
erna
l Hea
lth
1.
2.3.
Tra
inin
g fo
r vi
llage
m
idw
ives
in g
ivin
g co
unse
ling
and
educ
atio
n to
the
com
mun
ity to
mak
e th
em m
ore
aler
t
Num
ber o
f vi
llage
mid
wiv
es
trai
ned
in g
ivin
g co
unse
ling
and
educ
atio
n
Trai
ning
for v
illag
e m
idw
ives
in g
ivin
g co
unse
ling
and
educ
atio
n be
gins
in
2013
and
incr
ease
s ev
ery
year
ac
cord
ing
to th
e ta
rget
of e
ach
regi
on.
In 2
015
the
coun
selin
g an
d ed
ucat
ion
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Dir
ecto
rate
of
nurs
ing
serv
ice
and
publ
ic
heal
th M
in. o
f H
ealth
,

2927
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
trai
ning
is c
ondu
cted
for 3
0% o
f vill
age
mid
wiv
es
Prov
inci
al, ,
D
istr
ict/
City
Le
vel
1.3.
Mai
ntai
n/in
crea
se
the
qual
ity o
f m
othe
r and
chi
ld
heal
th c
are
1.3.
1. I
mpr
ove
faci
litat
ive
supe
rvis
ion
for
villa
ge m
idw
ives
Num
ber o
f co
mm
unity
he
alth
cen
ters
co
nduc
ting
faci
litat
ive
supe
rvis
ion
Num
ber o
f com
mun
ity h
ealth
cen
ters
co
nduc
ting
faci
litat
ive
supe
rvis
ion
incr
ease
s ev
ery
year
in a
ccor
danc
e w
ith th
e ta
rget
of e
ach
area
. In
2015
al
l com
mun
ity h
ealth
cen
ters
hav
e co
nduc
ted
faci
litat
ive
supe
rvis
ion
for
all v
illag
e m
idw
ives
reg
ular
ly
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Dir
ecto
rate
of
nurs
ing
serv
ice
and
publ
ic
heal
th M
in. o
f H
ealth
, Pr
ovin
cial
, ,
Dis
tric
t/Ci
ty
Leve
l
2.
A
ssur
ance
of
the
avai
labi
lity
of h
ealth
car
e fa
cilit
ies
capa
ble
of
prov
idin
g de
liver
y ca
re
24/7
in
acco
rdan
ce
with
the
wor
king
st
anda
rd
2.1.
Impr
ove
dete
ctio
n an
d fir
st a
id fo
r co
mpl
icat
ions
ca
ses
and
effe
ctiv
e re
ferr
als
2.1.
1.
Incr
ease
the
num
ber o
f com
mun
ity
heal
th c
ente
rs c
apab
le o
f pr
ovid
ing
deliv
ery
care
ac
cord
ing
to th
e w
orki
ng
stan
dar
24/7
Com
plem
ent/
add
mat
erni
ty
room
at
co
mm
unity
he
alth
ce
nter
s
Com
plem
ent
mea
ns a
nd
infr
astr
uctu
res,
inc
ludi
ng
med
icin
es
Tr
ain
the
com
mun
ity
Num
ber o
f co
mm
unity
he
alth
cen
ter
capa
ble
of
prov
idin
g m
ater
nity
car
e 24
/7
Num
ber o
f com
mun
ity h
ealth
cen
ters
ca
pabl
e of
pro
vidi
ng m
ater
nity
and
ne
onat
al c
are
incr
ease
s ev
ery
year
in
acco
rdan
ce w
ith th
e ta
rget
of e
ach
regi
on. I
n 20
15 5
0% o
f the
com
mun
ity
heal
th c
ente
rs in
dis
tric
t are
as a
nd
100%
in c
ity a
reas
are
cap
able
of
prov
idin
g m
ater
nity
and
neo
nata
l ca
re.
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t (B
UKD
)
Prov
inci
al,
Dis
tric
t and
City
H
ealth
Off
ice,
Lo
cal
Gov
ernm
ent,
Re
gion
al
Dev
elop
men
t Pl
anni
ng B
oard
; ho
spita
ls;
prof
essi
onal
or
gani
zatio
n

3028
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
heal
th c
ente
rs’ t
eam
to
wor
k 24
/7, i
nclu
ding
pe
rfor
min
g de
tect
ion
and
first
aid
for
com
plic
atio
ns c
ases
and
ef
fect
ive
refe
rral
s
2.1.
2. C
ondu
ct a
n in
tegr
ated
AN
C,
incl
udin
g pr
even
tion
of H
IV tr
ansm
issi
on
from
mot
her
to c
hild
% o
f com
mun
ity
heal
th c
ente
rs in
di
stri
ct a
nd c
ity
area
s im
plem
entin
g th
e in
tegr
ated
A
NC
Num
ber o
f com
mun
ity h
ealth
cen
ters
in
ditr
ict a
nd c
ity a
reas
impl
emen
ting
the
inte
grat
ed A
NC
incr
ease
s ev
ery
year
in a
ccor
danc
e w
ith th
e ta
rget
of
each
reg
ion.
In 2
015
all c
omm
unity
he
alth
cen
ters
hav
e im
plem
ente
d th
e in
tegr
ated
AN
C
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Min
. of H
ealth
, H
ealth
off
ice
at
prov
inci
al,
dist
rict
and
city
le
vel
Dir
ecto
rate
of
nurs
ing
serv
ice
and
publ
ic
heal
th M
in. o
f H
ealth
, Pr
ovin
cial
, ,
Dis
tric
t/Ci
ty
Leve
l
2.
1.3.
Con
duct
Hb
scre
enin
g fo
r ev
ery
preg
nant
wom
an
chec
king
thei
r pr
egna
ncy
at h
ealth
ca
re fa
cilit
ies
% o
f com
mun
ity
heal
th c
ente
rs
cond
uctin
g H
b ex
amin
atio
n an
d re
port
ing
the
annu
al a
nem
ia
prev
alen
ce
Num
ber o
f com
mun
ity h
ealth
cen
ters
co
nduc
ting
Hb
exam
inat
ion
and
repo
rtin
g th
e an
emia
pre
vale
nce
of
preg
nant
mot
hers
incr
ease
s ev
ery
year
. By
the
end
of 2
013
or th
e la
test
at
the
begi
nnin
g of
201
4 al
l co
mm
unity
hea
lth c
ente
rs h
ave
cond
ucte
d H
b ex
amin
atio
n re
gula
rly
and
repo
rted
the
annu
al a
nem
ia
prev
alen
ce e
very
yea
r
Cent
er o
f Dat
a an
d In
form
atio
n
An
inte
grat
ed
mot
her a
nd
An
inte
grat
ed m
othe
r and
chi
ld h
ealth
Ce
nter
of D
ata
Prov
inci
al,

3129
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
child
hea
lth
info
rmat
ion
syst
em is
es
tabl
ishe
d
info
rmat
ion
syst
em is
ava
ilabl
e in
20
13
and
Info
rmat
ion
Dis
tric
t and
City
Le
vel
2.2.
Incr
ease
the
num
ber o
f fa
cilit
ies
whi
ch
can
prov
ide
trea
tmen
t for
co
mpl
icat
ions
2.2.
1.
Incr
ease
the
num
ber o
f com
mun
ity
heal
th c
ente
rs w
hich
pr
ovid
es P
ON
ED 2
4/7,
pr
iori
tizin
g th
e re
mot
e ar
eas:
Fill
/add
trai
ned
PON
ED
team
Com
plem
ent t
he m
eans
an
d in
fras
truc
ture
, in
clud
ing
med
icin
es, a
t co
mm
unity
hea
lth
cent
ers
Co
nduc
t a re
fres
hmen
t tr
aini
ng fo
r the
exi
stin
g PO
NED
team
giv
en
com
plic
atio
ns c
ases
are
ra
rely
enc
ount
ered
En
sure
the
avai
labi
lity
of
refe
rred
mea
ns o
f tr
ansp
orta
tion
and
adeq
uate
co
mm
unic
atio
n
% o
f com
mun
ity
heal
th c
ente
rs
capa
ble
of
prov
idin
g PO
NED
24/
7 in
di
stri
ct a
nd c
ity
area
s
All
of th
e ex
isiti
ng P
ON
ED c
omm
unity
he
alth
cen
ters
are
func
tioni
ng 2
4/7
by
the
end
of 2
013.
N
umbe
r of c
omm
unity
hea
lth c
ente
rs
capa
ble
of p
rovi
ding
PO
NED
incr
ease
s ev
ery
year
in a
ccor
danc
e w
ith th
e ta
rget
of e
ach
regi
on, a
nd in
201
5 al
l co
mm
unity
hea
lth c
ente
rs th
at
prov
ide
emer
genc
y ca
re c
an p
rovi
de
PON
ED24
/7
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t

3230
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
2.3.
Build
coor
dina
tion
and
coop
erat
ion
with
re
ferr
al
hosp
itals
, whi
ch
are
loca
ted
in
the
sam
e re
gion
an
d in
oth
er
regi
ons
(pro
vinc
ial
hosp
itals
, ho
spita
ls in
bo
rder
regi
ons,
m
ilita
ry
hosp
itals
, pri
vate
ho
spita
ls) t
o ex
pand
the
acce
ss to
co
mpl
icat
ions
ca
se re
ferr
als
in
hosp
itals
2.3.
1. B
uild
coo
rdin
atio
n w
ith th
e re
leva
nt
sect
ors
to e
stab
lish
a sy
stem
of r
efer
ral
from
com
mun
ity
heal
th c
ente
rs to
ho
spita
ls.
Num
ber o
f di
stri
cts
and
citie
s th
at h
ave
a re
ferr
al s
yste
m
and
MoU
Gui
delin
efor
ref
erra
l sys
tem
is
com
plet
ed b
y M
in. o
f Hea
lth in
201
3,
and
dist
ribu
ted
to a
ll pr
ovin
ces.
A
t pro
vinc
ial l
evel
, the
gui
debo
ok is
ad
apte
d to
the
loca
l con
ditio
ns o
f ea
ch re
gion
(inc
ludi
ng d
evel
opm
ent o
f M
oU, c
oope
ratio
n/co
ordi
natio
n w
ith,
stak
ehol
ders
, nam
ely
the
loca
l go
vern
men
ts, d
istr
ict h
ospi
tals
, hea
lth
offic
es, p
riva
te h
ospi
tals
and
pri
vate
cl
inic
s) a
nd th
en d
istr
ibut
ed to
the
dist
rict
s an
d ci
ties
in m
id/t
he e
nd o
f 20
13.
The
MoU
is is
sued
and
the
refe
rral
G
uide
lines
tart
s to
be
used
by
all
regi
ons
at th
e be
ginn
ing
of 2
014.
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s (B
UKR
)
The
inte
grat
ed
mot
her a
nd
child
in
form
atio
n sy
stem
is
esta
blis
hed
The
inte
grat
ed m
othe
r and
chi
ld
heal
th in
form
atio
n sy
stem
(ver
tical
an
d ho
riso
ntal
) is
avai
labl
e by
the
end
of 2
013
Cent
er o
f Dat
a an
d In
form
atio
n

3331
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
2.4.
Opt
imiz
e ut
iliza
tion
of
heal
th in
sura
nce
for e
ligib
le
peop
le
(mat
erni
ty
insu
ranc
e,
natio
nal s
ocia
l se
curi
ty s
yste
m)
2.4.
1. B
uild
coo
rdin
atio
n w
ith v
ario
us
stak
ehol
ders
to
impl
emen
t m
ater
nity
in
sura
nce/
natio
nal
soci
al s
ecur
ity
syst
em a
t eve
ry le
vel
of s
ervi
ce, s
o th
e m
ain
task
sand
fu
nctio
ns o
f eve
ry
stak
ehol
der a
re
clea
r
The
coor
dina
ting
mec
hani
sm fo
r th
e im
plem
enta
tion
of m
ater
nity
in
sura
nce/
natio
nal s
ocia
l se
curi
ty s
yste
m
is e
stab
lishe
d
Coor
dina
ting
mec
hani
sm fo
r the
im
plm
enta
tion
of m
ater
nity
in
sura
nce/
natio
nal s
ocia
l sec
urity
sy
stem
in d
istr
ict a
nd c
ity a
reas
is
esta
blis
hed
in 2
013
Cent
er fo
r H
ealth
Sec
urity
Fi
nanc
ing
2.
4.2.
Pro
vide
info
rmat
ion
to th
e pu
blic
abo
ut
the
righ
ts a
nd
oblig
atio
ns re
late
d to
hea
lth in
sura
nce
Dis
sem
inat
ion
of
info
rmat
ion
to
publ
ic a
bout
the
righ
ts a
nd
oblig
atio
ns
rela
ted
to h
ealth
in
sura
nce
has
be
en d
one
Dis
sem
inat
ion
of in
form
atio
n to
pub
lic
abou
t the
rig
hts
and
oblig
atio
ns
rela
ted
to h
ealth
insu
ranc
e h
as b
een
cond
ucte
d in
all
subd
istr
icts
and
vi
llage
s by
hea
lth p
erso
nnel
at t
he
begi
nnin
g of
201
4
Cent
er fo
r H
ealth
Sec
urity
Fi
nanc
ing
2.5.
Impr
ove
qual
ity
of s
ervi
ce
2.5.
1. Im
prov
ethe
ski
lls o
f he
alth
pro
fess
iona
ls
at b
asic
leve
l th
roug
h tr
aini
ngs,
ap
pren
tices
hips
, and
in
-hou
se tr
aini
ngs
in
Num
ber o
f he
ath
prof
essi
onal
s at
tend
ing
PON
ED tr
aini
ng:
mid
wiv
es,
All
PON
ED te
ams
(mid
wiv
es,
phys
icia
ns, n
urse
s) a
t com
mun
ity
heal
th c
ente
rs h
ave
atte
nded
PO
NED
tr
aini
ng b
y th
e en
d of
201
3
Num
ber
of h
ealth
pro
fess
iona
ls a
t
Cent
er o
f Ed
ucat
ion
and
Trai
ning
for
App
arat
us

3432
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
both
ini P
ON
ED o
r no
n-PO
NED
co
mm
unity
hea
lth
cent
ers
phys
icia
ns,
nurs
es
Num
ber o
f he
alth
pr
ofes
sion
als
who
has
take
n ap
pren
tices
hip/
atte
nded
PO
NED
in
-hou
se
trai
ning
: m
idw
ives
, ph
ysic
ians
, nu
rses
PON
ED c
omm
unity
hea
lth c
ente
rs
(oth
er th
an P
ON
ED te
am) t
akin
g ap
pren
tices
hip/
atte
ndin
g PO
NED
in-
hous
e tr
aini
ngs
incr
ease
s ev
ery
year
N
umbe
r of
hea
lth p
rofe
ssio
nals
at
non-
PON
ED c
omm
unity
hea
lth c
ente
rs
that
has
take
n ap
pren
tices
hip/
atte
ndin
g PO
NED
in-
hous
e tr
aini
ngs
incr
ease
s ev
ery
year
ac
cord
ing
to th
e ta
rget
of e
ach
regi
on
2.
5.2.
PO
NEK
hos
pita
ls
prov
ide
guid
ance
for
PON
ED c
omm
unity
he
alth
cen
ters
. It
can
be d
one
in th
e co
mm
unity
hea
lth
cent
ers
or in
PO
NEK
ho
spita
ls
Num
ber o
f PO
NED
co
mm
unity
he
alth
cen
ters
re
ceiv
ing
regu
lar
guid
ance
In 2
013
stra
tegi
es o
f gui
danc
e pr
ovid
ed b
y PO
NEK
hos
pita
ls fo
r PO
NED
com
mun
ity h
ealth
cen
ters
ha
ve b
een
deve
lope
d an
d ag
reed
up
on b
y al
l sta
keho
lder
s in
the
regi
ons.
In
201
4 al
l PO
NEK
hos
pita
ls h
ave
prov
ided
gui
danc
e fo
r PO
NED
co
mm
unity
hea
lth c
ente
rs p
erio
dica
lly
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t
2.
5.3.
Per
form
the
Mat
erna
l Per
inat
al
Num
ber o
f di
stri
cts/
citie
s N
umbe
r of d
istr
icts
/citi
es p
erfo
rmin
g M
ater
nal P
erin
atal
Aud
it an
d its
D
irec
tora
te o
f M
ater
nal H
ealth

3533
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
Aud
it an
d fo
llow
up
actio
ns w
hich
may
in
clud
e im
prov
ed
know
ledg
e an
d sk
ills
of h
ealth
per
sonn
el,
fulfi
lling
the
need
fo
r m
edic
al
equi
pmen
t and
m
edic
ines
, mod
ified
po
licie
s, e
tc.
perf
orm
ing
Mat
erna
l Pe
rina
tal A
udit
min
imum
2
times
a y
ear
follo
w-u
p ac
tion
incr
ease
eve
ry y
ear.
In
201
3 at
leas
t the
2-t
ime
Mat
erna
l Pe
rina
tal A
udit
that
is fo
llow
ed b
y th
e ne
cess
ary
actio
ns is
con
duct
ed.
In 2
015
all d
istr
icts
and
citi
es c
ondu
ct
the
Mat
erna
l Per
inat
al A
udit
that
is
follo
wed
by
the
nece
ssar
y ac
tions
4
times
2.
5.4.
Impl
emen
t bac
k re
ferr
al to
allo
w th
e re
ferr
ers
lear
n fr
om
the
resu
lts o
f the
ir
actio
ns a
nd c
ontin
ue
tope
rfor
m th
e m
onito
ring
of p
ost-
ho
spita
lized
pat
ient
s
Num
ber o
f di
stri
cts/
citie
s th
at h
ave
bac
k re
ferr
al
mec
hani
sm
Gui
delin
eon
the
refe
rral
sys
tem
(in
clud
ing
back
refe
rral
) is
com
plet
ed
by th
e M
in. o
f Hea
lth in
201
3 an
d is
ad
apte
d to
the
loca
l con
ditio
ns o
f ea
ch re
gion
. The
Gui
delin
esta
rts
to b
e us
ed b
y al
l reg
ions
at t
he b
egin
ning
of
2014
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
2.
5.5.
Con
duct
faci
litat
ive
supe
rvis
ion
on
PON
ED c
are
perf
orm
ed b
y a
coor
dina
ting
dist
rict
m
idw
ife o
r ot
her
desi
gnat
ed h
ealth
pr
ofes
sion
als
Num
ber o
f di
stri
ct a
nd c
ities
in
a p
rovi
nce
cond
uctin
g fa
cilit
ativ
e su
perv
isio
n on
PO
NED
Num
ber
of d
istr
icts
and
citi
es
cond
uctin
g fa
cilit
ativ
e su
perv
isio
n on
PO
NED
ser
vice
s re
gula
rly
incr
ease
s ev
ery
year
in a
ccor
danc
e w
ith th
e ta
rget
of e
ach
regi
on.
In 2
014
all d
istr
icts
and
citi
es h
ave
cond
ucte
d fa
cilit
ativ
e su
perv
isio
n re
gula
ry
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Dir
ecto
rate
of
nurs
ing
serv
ice
and
publ
ic
heal
th M
in. o
f H
ealth
, Pr
ovim
ce,
Dis
tric
t/Ci
ty

3634
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
3.
A
ssur
ance
of
the
func
tion
of
all P
ON
EK
hosp
itals
at
dist
rict
/city
le
vel t
o w
ork
24/7
in
acco
rdan
ce
with
the
stan
dard
3.1.
Impr
ove
the
qual
ity o
f hea
lth
pers
onne
l in
refe
rral
hos
pita
ls
in h
andl
ing
com
plic
atio
ns
case
s in
a ti
mel
y an
d ap
prop
riat
e m
anne
r,
incl
udin
g th
e av
aila
bilit
y of
gu
idel
ines
on
stan
dard
of
care
for
com
plic
atio
n ca
ses
3.1.
1. C
ondu
ct c
linic
al
man
agem
ent
trai
ning
s, in
clud
ing
trai
ning
s on
PO
NEK
, lif
e sa
ving
ski
lls a
nd
othe
r tr
aini
ngs,
for
heal
th p
rofe
ssio
nals
in
hos
pita
ls to
en
able
them
han
dle
com
plic
atio
ns c
ases
re
ferr
ed to
hos
pita
ls
Clin
ical
m
anag
emen
t tr
aini
ngs,
in
clud
ing
trai
ning
s on
PO
NEK
, life
sa
ving
ski
lls a
nd
othe
r tr
aini
ngs,
fo
r he
alth
pr
ofes
sion
als
in
hosp
itals
are
co
nduc
ted
to
enab
le th
em to
ha
ndle
the
com
plic
atio
ns
case
s re
ferr
ed to
ho
spita
ls
All
dist
rict
hos
pita
ls h
ave
a te
am o
f tr
aine
d he
alth
pro
fess
iona
ls
(obs
tetr
ics/
gyne
olog
y, p
edia
tric
s an
d an
esth
esio
logy
and
pos
t gra
duat
e st
uden
ts o
f PPD
S) w
ho is
cap
able
of
prov
idin
g PO
NEK
ser
vice
by
the
end
of
2014
.
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
Loca
l G
over
nmen
t;
Regi
onal
D
evel
opm
ent
Plan
ning
Boa
rd;
Hea
lth O
ffic
e at
Pr
ovin
cial
, D
istr
ict
and
City
Le
vel;
Hos
pita
ls;
Prof
essi
onal
O
rgan
izat
ions
3.2.
Build
co
ordi
natio
n an
d co
oper
atio
n w
ith
othe
r re
ferr
al
hosp
itals
, in
clud
ing
the
hosp
itals
of
high
er ty
pe,
priv
ate
hosp
itals
/mat
ern
3.2.
1. B
uild
coo
rdin
atio
n an
d de
velo
p a
coop
eativ
e co
nsen
sus
with
oth
er
refe
rral
hos
pita
ls,
whi
ch a
re th
e ho
spita
ls o
f hig
her
type
, pri
vate
ho
spita
ls/m
ater
nity
ho
spita
ls a
nd
MoU
or
mec
hani
sm/g
uid
elin
es fo
r co
ordi
natio
n an
d co
oper
atio
n w
ith re
ferr
al
hosp
itals
is
deve
lope
d
Ever
y di
stri
ct/c
ity a
lrea
dy h
as a
n M
oU
or c
oope
ratio
n in
201
4 D
irec
tora
te fo
r de
velo
pmen
t of
refe
rral
st
anda
rds

3735
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
ity h
ospi
tals
and
m
ilita
ry
hosp
itals
, to
expa
nd th
e ac
cess
for
com
plic
atio
ns
case
s in
hos
pita
ls
mili
tary
hos
pita
ls, t
o ex
pand
the
acce
ss
for
com
plic
atio
ns
case
s in
hos
pita
ls
3.3.
Ensu
re th
e ac
cess
to s
afe
bloo
d
3.3.
1. Im
prov
e an
d st
reng
then
the
coop
erat
ion
with
th
e In
done
sian
Red
Cr
oss
Coop
erat
ion
betw
een
the
Indo
nesi
an R
ed
Cros
s an
d ho
spita
ls’ b
lood
tr
ansf
usio
n un
it on
blo
od
prov
isio
n is
es
tabl
ishe
d
Coop
erat
ion
betw
een
the
Indo
nesi
an
Red
Cros
s an
d ho
spita
ls’ b
lood
tr
ansf
usio
n un
it in
all
dist
rict
s/ci
ties
on b
lood
pro
visi
on is
agr
eed
upon
by
the
end
of 2
013
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t
3.
3.2.
Impr
ove
the
func
tion
of b
lood
tr
ansf
usio
n un
it
A b
lood
tr
ansf
usio
n un
it is
ava
ilabl
e in
ho
spita
ls a
nd
func
tioni
ng in
ac
cord
ance
with
th
e st
anda
rd
All
publ
ic h
ospi
tals
’ blo
od tr
ansf
usio
n un
it ar
e fu
nctio
ning
by
the
end
of
2013
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t
3.
3.3.
Impr
ove
the
coop
erat
ion
betw
een
hosp
itals
,
MoU
/coo
pera
tion
betw
een
MoU
/coo
pera
tion
betw
een
hosp
itals
, in
the
sam
e re
gion
or
ousi
de th
e D
irec
tora
te o
f Ba
sic
Hea
lth

3836
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
both
in th
e sa
me
regi
on a
nd o
utsi
de
the
regi
on,o
n bl
ood
prov
isio
n
hosp
itals
, in
the
sam
e re
gion
or
ousi
de th
e re
gion
, on
bloo
d pr
ovis
ion
regi
on, o
n bl
ood
prov
isio
n is
es
tabl
ishe
d by
the
end
of 2
013
Ca
re
Dev
elop
men
t
3.4.
Impr
ove
post
pa
rtum
fam
ily
plan
ning
ac
cept
ors
N
umbe
r of
post
part
um
fam
ily p
lann
ing
acce
ptor
s in
ho
spita
ls
incr
ease
s ev
ery
year
Num
ber o
f pos
tpar
tum
fam
ily
plan
ning
acc
epto
rs in
hos
pita
ls
incr
ease
s ev
ery
year
in a
ccor
danc
e w
ith th
e ta
rget
of e
ach
regi
on
In 2
015
the
num
ber
of p
ostp
artu
m
mot
hers
who
bec
ome
fam
ily p
lann
ing
acce
ptor
s in
crea
se b
y 50
% c
ompa
red
to th
e pr
evio
us y
ear
Dir
ecto
rate
of
Mat
erna
l Hea
lth
3.5.
Ensu
re th
e av
aila
bilit
y of
ob
stet
ric
and
neon
atal
car
e at
an
y tim
e (2
4 ho
urs
7 da
ys)
3.5.
1. C
ompl
emen
t/ad
d pe
rson
nel t
o en
sure
th
e se
rvic
e de
liver
y 24
/7. P
rovi
de a
PO
NEK
team
ca
pabl
e of
pro
vidi
ng
emer
genc
y ca
re,
incl
udin
g a
caes
aria
n se
ctio
n op
erat
ors
(obs
tetr
icia
n/gy
neco
logi
st, p
ost-
grad
uate
st
uden
t of
obst
etri
cs),
Num
ber o
f PO
NEK
hos
pita
ls
capa
ble
of
prov
idin
g se
rvic
es 2
4/7
In 2
014
all d
istr
ict p
ublic
hos
pita
ls c
an
serv
e as
a P
ON
EK h
ospi
tal 2
4/7
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s

3937
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
pedi
atri
cian
, A
nest
hesi
olog
ist a
nd
para
med
ics,
mid
wife
an
d nu
rse
3.
5.2.
Com
plem
ent
/add
the
infr
astr
uctu
re:
oper
atin
g ro
om a
nd
its p
rior
ity u
se
arra
ngem
ent,
C-
sect
ion
kits
, m
edic
ines
, blo
od,
etc
Dis
tric
t pub
lic
hosp
itals
hav
e fa
cilit
ies
and
infr
astr
uctu
res
acco
rdin
g to
the
serv
ice
stan
dard
All
dist
rict
hos
pita
ls h
ave
com
plet
e fa
cilit
ies
and
infr
astr
uctu
res
in 2
014
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
3.
5.3.
Con
duct
inno
vativ
e ap
proa
ches
ac
cord
ing
to th
e lo
cal c
ondi
tions
for
the
hosp
itals
un
derg
oing
hum
an
reso
urce
s sh
orta
ge,
part
icul
arly
in
rem
ote
bord
er a
reas
an
d is
land
s. F
or
exam
ple
is th
e si
ster
ho
spita
l pro
gram
im
plem
ente
d in
Eas
t N
usa
Teng
gara
Inno
vativ
e ac
tions
to
redu
ce h
uman
re
sour
ces
gap,
in
clud
ing
med
ical
sp
ecia
lists
, are
ta
ken
In 2
013s
tudy
on
the
inno
vativ
e ac
tions
is
ava
ilabl
e
In 2
014
the
impl
emen
tatio
n be
gins
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
Nat
iona
l, Pr
ovin
cial
, D
istr
ict/
City
Le
vel
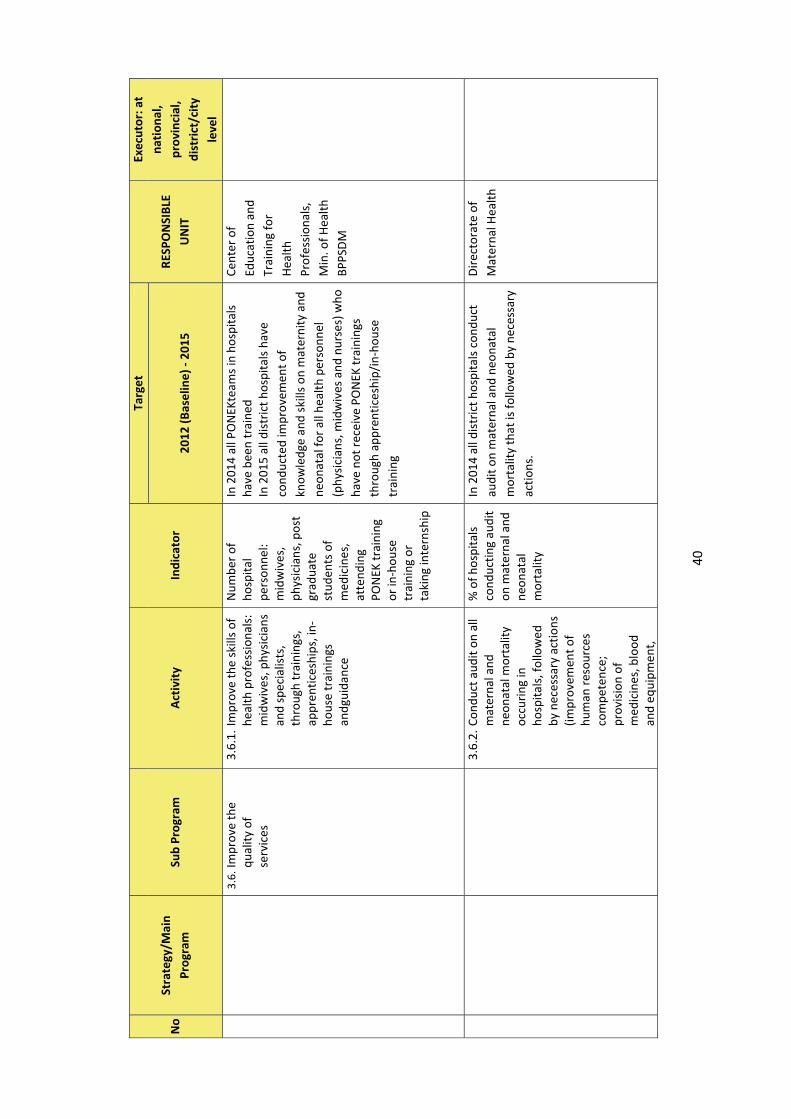
4038
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
3.6.
Impr
ove
the
qual
ity o
f se
rvic
es
3.6.
1. Im
prov
e th
e sk
ills
of
heal
th p
rofe
ssio
nals
: m
idw
ives
, phy
sici
ans
and
spec
ialis
ts,
thro
ugh
trai
ning
s,
appr
entic
eshi
ps, i
n-ho
use
trai
ning
s an
dgui
danc
e
Num
ber o
f ho
spita
l pe
rson
nel:
mid
wiv
es,
phys
icia
ns, p
ost
grad
uate
st
uden
ts o
f m
edic
ines
, at
tend
ing
PON
EK tr
aini
ng
or in
-hou
se
trai
ning
or
taki
ng in
tern
ship
In 2
014
all P
ON
EKte
ams
in h
ospi
tals
ha
ve b
een
trai
ned
In 2
015
all d
istr
ict h
ospi
tals
hav
e co
nduc
ted
impr
ovem
ent o
f kn
owle
dge
and
skill
s on
mat
erni
ty a
nd
neon
atal
for
all h
ealth
per
sonn
el
(phy
sici
ans,
mid
wiv
es a
nd n
urse
s) w
ho
have
not
rec
eive
PO
NEK
trai
ning
s th
roug
h ap
pren
tices
hip/
in-h
ouse
tr
aini
ng
Cent
er o
f Ed
ucat
ion
and
Trai
ning
for
Hea
lth
Prof
essi
onal
s,
Min
. of H
ealt
h BP
PSD
M
3.
6.2.
Con
duct
aud
it on
all
mat
erna
l and
ne
onat
al m
orta
lity
occu
ring
in
hosp
itals
, fol
low
ed
by n
eces
sary
act
ions
(im
prov
emen
t of
hum
an re
sour
ces
com
pete
nce;
pr
ovis
ion
of
med
icin
es, b
lood
an
d eq
uipm
ent,
% o
f hos
pita
ls
cond
uctin
g au
dit
on m
ater
nal a
nd
neon
atal
m
orta
lity
In 2
014
all d
istr
ict h
ospi
tals
con
duct
au
dit o
n m
ater
nal a
nd n
eona
tal
mor
talit
y th
at is
follo
wed
by
nece
ssar
y ac
tions
.
Dir
ecto
rate
of
Mat
erna
l Hea
lth

4139
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
mod
ifica
tion
of
polic
y)
3.
6.3.
Opt
imiz
e su
perv
isio
n an
d qu
ality
ass
uran
ce in
ho
spita
ls
Supe
rvis
ion
and
qual
ity
assu
ranc
e in
ho
spita
ls a
re
cond
ucte
d re
gula
rly
In 2
014
all d
istr
ict h
ospi
tals
hav
e gu
idel
ines
and
con
duct
sup
ervi
sion
an
d qu
ality
ass
uran
ce in
hos
pita
ls
regu
larl
y
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
Dis
tric
t/Ci
ty
Leve
l
3.
6.4.
Use
a se
rvic
e ed
ict t
o in
crea
se th
e ro
le o
f th
e so
ciet
y in
im
prov
ing
the
serv
ice
qual
ity
% o
f hos
pita
ls a
t di
stri
ct/c
ity le
vel
that
hav
e a
serv
ice
edic
t
In 2
014
all d
istr
ict h
ospi
tals
hav
e se
rvic
e ed
it
Cent
er fo
r he
alth
pr
omot
ion
3.7.
Stre
ngth
en
mat
erni
ty a
nd
neon
atal
ser
vice
sy
stem
in
hosp
itals
3.7.
1. D
evel
op/m
odify
po
licie
s in
hea
lth
care
faci
litie
s:
adm
issi
on fl
ow a
nd
hand
ling
of o
bste
tric
an
d ne
onat
al
emer
genc
y ca
ses,
av
aila
bilit
y an
d pr
oper
func
tioni
ng
of th
e em
erge
ncy
room
, etc
Polic
ies
on
hosp
ital s
ervi
ces
are
avai
labl
e,
incl
udin
g ad
mis
sion
flow
an
d ha
ndlin
g of
ob
stet
ric
and
neon
atal
em
erge
ncy
case
s,
avai
labi
lity
and
prop
er
func
tioni
ng o
f
By th
e en
d of
201
3 al
l dis
tric
t hos
pita
ls
have
and
impl
emen
t cle
ar a
nd
adeq
uate
pol
icie
s on
hos
pita
l ser
vice
s
Dir
ecto
rate
of
Mat
erna
l Hea
lth

4240
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
the
emer
genc
y ro
om, e
tc
3.
7.2.
Im
plem
ent b
ack
refe
rral
mad
e by
the
hosp
itals
for
the
refe
rrer
s, s
o th
e m
onito
ring
of t
he
post
-hos
pita
lized
pa
tient
s ca
n be
pr
ovid
ed b
y th
e re
ferr
ers
% o
f dis
tric
t ho
spita
ls m
akin
g ba
ck r
efer
ral
and
reco
rd a
nd
cond
uctin
g a
regu
lar
repo
rtin
g
By th
e en
d of
201
3 al
l dis
tric
t hos
pita
ls
mak
e ba
ck re
ferr
als
and
mak
e a
reco
rd a
nd c
ondu
ct a
regu
lar
repo
rtin
g
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
4.
A
ssur
ance
of
the
impl
emen
tatio
n of
eff
ectiv
e re
ferr
al fo
r co
mpl
icat
ions
ca
ses
4.1.
Ens
ure
the
avai
labl
ity o
f re
ferr
al
guid
elin
es
4.1.
1. D
evel
op/e
stab
lish
clea
r ref
erra
l gu
idel
ines
at
natio
nal l
evel
Num
ber o
f pr
ovin
ces
and
dist
rict
s an
d ci
ties
that
has
gu
idel
ines
on
mat
erna
l and
ne
onat
al r
efer
ral
syst
em
Gui
delin
eon
the
refe
rral
sys
tem
(in
clud
ing
back
refe
rral
) is
com
plet
ed
by th
e M
inis
try
of H
ealth
in 2
013.
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s;
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Hea
lth O
ffic
e at
Pr
ovin
cial
, D
istr
ict a
nd C
ity
Leve
l, Lo
cal
Gov
ernm
ent,
Re
gion
al
Dev
elop
men
t Pl
anni
ng B
oard
; ho
spita
ls;
prof
essi
onal
or
gani
zatio
n
4.
1.2.
Dev
elop
/est
ablis
h cl
ear r
efer
ral
guid
elin
es a
nd
Num
ber o
f di
stri
ct/c
ities
th
at h
ave
The
guid
elin
es a
re a
dapt
ed to
the
cond
ition
s in
eac
h re
gion
. The
gu
idel
ines
are
alr
eady
ava
ilabl
e an
d
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
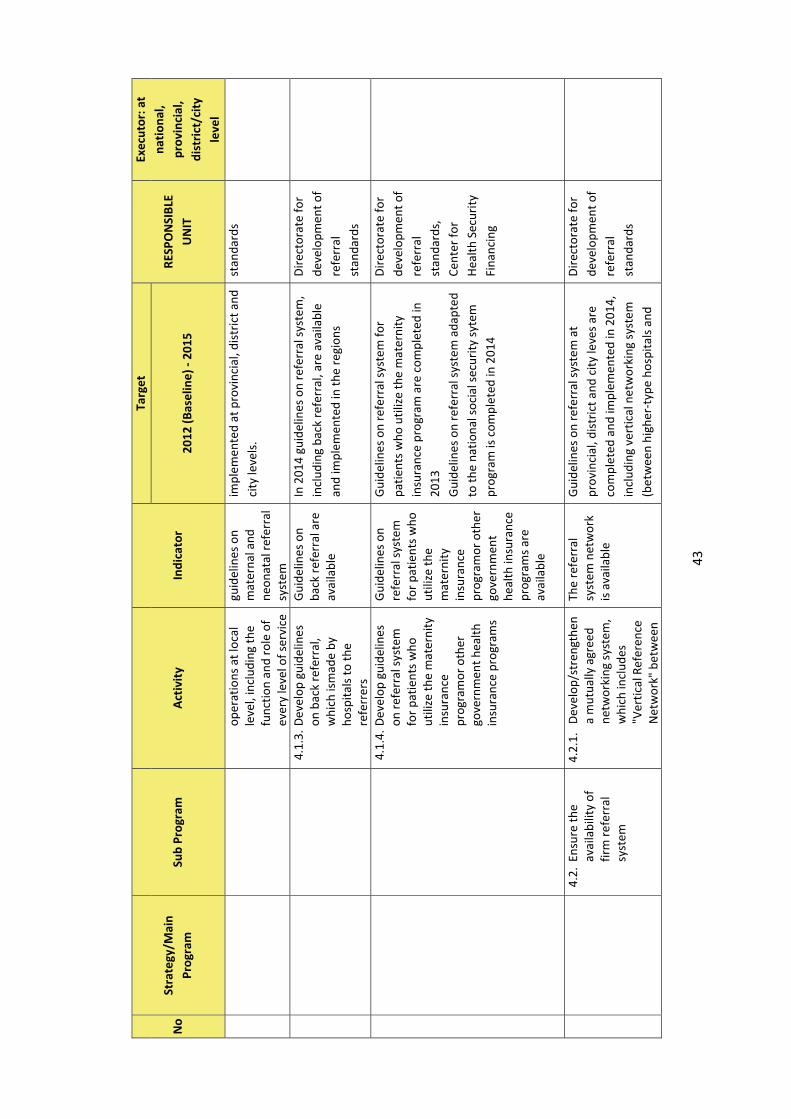
4341
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
oper
atio
ns a
t loc
al
leve
l, in
clud
ing
the
func
tion
and
role
of
ever
y le
vel o
f ser
vice
guid
elin
es o
n m
ater
nal a
nd
neon
atal
ref
erra
l sy
stem
impl
emen
ted
at p
rovi
ncia
l, di
stri
ct a
nd
city
leve
ls.
stan
dard
s
4.
1.3.
Dev
elop
gui
delin
es
on b
ack
refe
rral
, w
hich
ism
ade
by
hosp
itals
to th
e re
ferr
ers
Gui
delin
es o
n ba
ck r
efer
ral a
re
avai
labl
e
In 2
014
guid
elin
es o
n re
ferr
al s
yste
m,
incl
udin
g ba
ck r
efer
ral,
are
avai
labl
e an
d im
plem
ente
d in
the
regi
ons
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
4.
1.4.
Dev
elop
gui
delin
es
on re
ferr
al s
yste
m
for
patie
nts
who
ut
ilize
the
mat
erni
ty
insu
ranc
e pr
ogra
mor
oth
er
gove
rnm
ent h
ealth
in
sura
nce
prog
ram
s
Gui
delin
es o
n re
ferr
al s
yste
m
for
patie
nts
who
ut
ilize
the
mat
erni
ty
insu
ranc
e pr
ogra
mor
oth
er
gove
rnm
ent
heal
th in
sura
nce
prog
ram
s ar
e av
aila
ble
Gui
delin
es o
n re
ferr
al s
yste
m fo
r pa
tient
s w
ho u
tiliz
e th
e m
ater
nity
in
sura
nce
prog
ram
are
com
plet
ed in
20
13
Gui
delin
es o
n re
ferr
al s
yste
m a
dapt
ed
to th
e na
tiona
l soc
ial s
ecur
ity s
ytem
pr
ogra
m is
com
plet
ed in
201
4
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s,
Cent
er fo
r H
ealth
Sec
urity
Fi
nanc
ing
4.2.
Ens
ure
the
avai
labi
lity
of
firm
refe
rral
sy
stem
4.2.
1. D
evel
op/s
tren
gthe
n a
mut
ually
agr
eed
netw
orki
ng s
yste
m,
whi
ch in
clud
es
"Ver
tical
Ref
eren
ce
Net
wor
k" b
etw
een
The
refe
rral
sy
stem
net
wor
k is
ava
ilabl
e
Gui
delin
es o
n re
ferr
al s
yste
m a
t pr
ovin
cial
, dis
tric
t and
city
leve
s ar
e co
mpl
eted
and
impl
emen
ted
in 2
014,
in
clud
ing
vert
ical
net
wor
king
sys
tem
(b
etw
een
high
er-t
ype
hosp
itals
and
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s

4442
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
basi
c se
rvic
es a
nd
serv
ices
at a
hig
her
leve
l (ho
spita
l se
rvic
es),
and
"Hor
izon
tal R
efer
ral
Net
wor
k"
low
-typ
e ho
spita
ls),
hori
zont
al
netw
orki
ng s
yste
m (b
etw
een
publ
ic
and
priv
ate
hosp
itals
) and
cro
ss-
regi
onal
net
wor
king
sys
tem
4.
2.2.
Dev
elop
/str
engt
hen
a m
utua
lly-a
gree
d re
gion
al n
etw
orki
ng
syst
em, e
spec
ially
to
han
dle
rem
ote
and
bord
er a
reas
Regi
onal
ne
twor
king
of
refe
rral
sys
tem
is
ava
ilabl
e
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
4.
2.3.
Dev
elop
a r
efer
ral
com
mun
icat
ion
syst
em th
at h
as tw
o ob
ject
ives
: to
prov
ide
guid
ance
an
d se
rvic
es fo
r ob
tain
ing
the
conf
irm
atio
n ab
out
the
avai
labi
lity
of
the
refe
rral
hos
pita
l se
rvic
es (t
he
avai
labi
lity
of
doct
or, b
ed, b
lood
, m
edic
ines
, etc
.)
The
refe
rral
co
mm
unic
atio
n sy
stem
is
esta
blis
hed
In 2
015
all d
istr
icts
/citi
es th
at h
ave
a go
od te
leco
mm
unic
atio
n ne
twor
k ha
ve d
evel
oped
and
impl
emen
ted
the
refe
rral
com
mun
icat
ion
syst
em
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s,
Cent
er o
f Dat
a an
d In
form
atio
n
4.
2.4.
Str
engt
hen
the
Adm
issi
on a
nd
By th
e en
d of
201
3 al
l dis
tric
t hos
pita
ls
Dir
ecto
rate
for

4543
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
adm
issi
on a
nd
hand
ling
syst
em fo
r ca
ses
in th
e ho
spita
ls, i
nclu
ding
ha
ndlin
g flo
w,
coor
dina
tion
with
ob
stet
rici
an o
r po
st-
grad
uate
stu
dent
s of
obs
tetr
ics,
and
co
ordi
natio
n w
ith
othe
r sp
ecia
lists
as
soci
ated
with
m
ater
nal d
eath
s du
e to
indi
rect
ca
uses
hand
ling
syst
em
for
emer
genc
y ca
ses
in
hosp
itals
are
im
plem
ente
d in
ac
cord
ance
with
th
e ho
spita
ls
accr
edita
tion
stan
dard
s.
have
and
impl
emen
ted
the
polic
y on
em
ergn
ecy
care
for
emer
genc
y ca
ses
in h
ospi
tals
acc
ordi
ng to
the
hosp
ital
accr
edita
ton
stan
dard
s
deve
lopm
ent o
f re
ferr
al
stan
dard
s
4.
2.5.
Dev
elop
/str
engt
hen
a m
utua
lly-a
gree
d ne
twor
king
sys
tem
fo
r re
mot
e ar
eas
and
isla
nds
Net
wor
king
sy
stem
in
rem
ote
area
s an
d is
land
s is
av
aila
ble
Net
wor
king
sys
tem
in re
mot
e ar
eas
and
isla
nds
is e
stab
lishe
d by
the
end
of 2
013
5.
A
dole
scen
t re
prod
uctiv
e he
alth
ser
vice
s as
ear
ly
inte
rven
tion
effo
rt to
pr
even
t
5.1.
Ens
ure
avai
labi
lity
of
yout
h-fr
iend
ly
heal
th s
ervi
ces
that
focu
s on
pr
omot
ion
and
prev
entio
n
5.1.
1. In
crea
se n
umbe
r of
yo
uth-
frie
ndly
pu
skes
mas
(PKP
R)
thro
ugh
trai
ning
of
heal
th w
orke
rs a
nd
tech
nica
l as
sist
ance
s
Cove
rage
of
dist
rict
s th
at
have
min
imal
4
PKPR
pus
kesm
as
95%
of t
otal
dis
tric
ts th
at h
ave
min
imal
4 P
KPR
pusk
esm
as b
y 20
14
Dir
ecto
rate
of
Child
Hea
lth
Hea
lth O
ffic
e an
d Pu
blic
H
ospi
tal a
t Pr
ovin
cial
, D
istr
ict a
nd C
ity
Leve
l;

4644
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
adol
esce
nt
preg
nanc
y th
roug
h IE
C an
d co
unse
ling
Stra
tegy
2: E
ncha
ncin
g th
e lo
cal g
over
nmen
ts’ a
nd p
riva
te s
ecto
r’s
role
in im
prov
ingm
ater
nal h
ealth
6.
A
ssur
ance
of
the
loca
l go
vern
men
ts’e
ndor
se fo
r th
e re
gula
tions
th
an c
an
effe
ctiv
ely
supp
ort t
he
prog
ram
im
plem
enta
tion
6.1.
Regu
latio
n on
th
e pr
ocur
emen
t an
d as
sign
men
t of
hea
lth
prof
essi
onal
s
6.1.
1. S
ubm
it a
prop
osal
to
the
cent
ral a
nd lo
cal
gove
rnm
ents
to
mee
t the
man
pow
er
need
s in
hea
lth c
are
faci
litie
s at
var
ious
le
vels
, so
peop
le
have
acc
ess
24/7
to
mat
erni
ty a
nd
neon
atal
ser
vice
s w
hich
are
req
uire
d.
The
prop
osal
in
clud
es
Co
mpl
etin
g th
e m
anpo
wer
at
PON
ED a
nd P
ON
EK
faci
litie
s th
at d
o no
t ha
ve tr
aine
d pe
rson
nel
A
ssig
ning
a P
ON
ED
team
at P
ON
ED
faci
litie
s gr
adua
lly
A
ssig
ning
a P
ON
EK
team
at P
ON
EK
N
umbe
r of
PON
ED
com
mun
ity
heal
th c
ente
rs
in a
dis
tric
t an
d ci
ty th
at
has
the
requ
ired
sp
ecia
lists
Num
ber o
f PO
NEK
ho
spita
ls in
a
prov
ince
that
ha
s th
e re
quir
ed
spec
ialis
ts
By
the
end
of 2
013
all P
ON
EK
hosp
itals
hav
e be
en c
ompl
eted
w
ith th
e re
quir
ed s
peci
alis
ts, s
o th
ey c
an fu
nctio
n 24
/7
In
201
3 al
l PO
NED
com
mun
ity
heal
th c
ente
rs a
re c
ompl
eted
with
th
e re
quir
ed s
peci
alis
ts s
o th
ey c
an
func
tion
24/7
In
201
5 al
l com
mun
ity h
ealth
ce
nter
s th
at p
rovi
de e
mer
genc
y ca
re h
ave
heal
th p
erso
nnel
who
ar
e ca
pabl
e of
pro
vidi
ng P
ON
ED
24/7
BPPS
DM
(Pusreng
unakes
) H
ealth
Off
ice
at
Prov
inci
al,
Dis
tric
t and
City
Le
vel,
Loca
l G
over
nmen
t,
Regi
onal
D
evel
opm
ent
Plan
ning
Boa
rd;
hosp
itals
; pr
ofes
sion
al
orga
niza
tion

4745
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
hosp
itals
gra
dual
ly
En
suri
ngth
e av
aila
bilit
y of
sp
ecia
lists
atP
ON
EK
hosp
itals
or
publ
ic
hosp
itals
that
hav
e no
t obt
aine
d PO
NEK
st
atus
6.1.
2. S
ubm
it a
prop
osal
to
the
loca
l go
vern
men
ts to
se
cure
the
assi
gnm
ent o
f pe
rson
nel w
ho h
ave
rece
ived
PO
NED
/PO
NEK
tr
aini
ng, s
o th
ey w
ill
not b
e tr
ansf
erre
d or
repl
ace
them
with
ot
her p
erso
nnel
who
ha
ve e
qual
cap
acity
an
d ha
ve b
een
prep
ared
% o
f dis
tric
ts
and
citie
s in
a
prov
ince
that
ha
ve o
ffic
ially
ob
tain
ed P
ON
ED
stat
us th
roug
h a
decr
ee
(incl
udin
g de
cree
for
pers
onne
l) %
of d
istr
icts
an
d ci
ties
in a
pr
ovic
e th
at
have
off
icia
lly
obta
ined
PO
NEK
st
atus
thro
ugh
a de
cree
(in
clud
ing
In 2
014
all P
ON
ED c
omm
unity
hea
lth
cent
er h
ave
offic
ially
obt
aine
d PO
NED
st
atus
thro
ugh
a dc
ree
In 2
014
all P
ON
EK h
ospi
tals
hav
e of
ficia
lly o
btai
ned
PON
EK s
tatu
s th
roug
h a
decr
ee
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t D
irec
tora
te fo
r de
velo
pmen
t of
refe
rral
st
anda
rds

4846
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
decr
ee fo
r pe
rson
nel)
6.
2. Re
gula
tion
on
the
assu
ranc
e of
th
e av
aila
bilit
y of
ne
cess
ary
med
icin
es in
ba
sic
heal
th c
are
faci
litie
s
6.2.
1. I
mpr
ove
and
stre
ngth
en
coor
dina
tion
with
na
tiona
l and
loca
l go
vern
men
t, s
o th
e av
aila
bilit
y of
the
med
icin
es re
quir
ed
is a
ssur
ed a
t all
times
, inc
ludi
ng th
e pl
anni
ng p
roce
ss,
man
agem
ent a
nd
mon
itori
ng-
eval
uatio
n
Perc
enta
ge o
f th
e av
aila
bilit
y of
ess
entia
l m
edic
ines
for
mot
hers
and
ne
wbo
rns.
In 2
014,
100
% o
f ess
entia
l med
icin
es
for
mot
hers
and
new
born
s ar
e av
aila
ble
acco
rdin
g to
the
type
and
am
ount
of t
he m
edic
ies.
Dir
ecto
rate
of
Publ
ic
Med
icin
esan
d H
ealth
Supp
lies
Nat
iona
l, H
ealth
O
ffic
e at
pr
ovin
cial
, di
stri
ct/c
ity
leve
l
6.
2.2.
Im
prov
e an
d st
reng
then
co
ordi
natio
n w
ith
the
Indo
nesi
an R
ed
Cros
s re
gard
ing
the
bloo
d pr
ovis
ion,
if
nece
ssar
y th
roug
h a
Mem
oran
dum
of
Und
erst
andi
ng a
t lo
cal l
evel
MO
U o
n bl
ood
prov
isio
n be
twee
n he
alth
of
fice
and
the
Indo
nesi
an R
ed
Cros
s is
es
tabl
ishe
d
In 2
014,
MO
U b
etw
een
all h
ealth
of
fices
at p
rovi
ncia
l, di
stri
ct/c
ity le
vels
an
d th
e In
done
sian
Red
Cro
ss is
es
tabl
ishe
d
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
6.
2.3.
Im
prov
e an
d M
OU
on
bloo
d In
201
4, M
OU
bet
wee
n al
l hos
pita
ls
Dir
ecto
rate
of
Prov
inci
al,

4947
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
stre
ngth
en
coor
dina
tion
betw
een
hosp
itals
, pu
blic
and
and
pr
ivat
e, b
oth
with
in
the
regi
on a
nd
outs
ide
the
regi
on
(pro
vinc
ial h
ospi
tals
or
the
near
est
hosp
ital),
in th
e pr
ovis
ion
of
equi
pmen
t,
med
icin
es a
nd
bloo
d, if
nec
essa
ry
thro
ugh
a M
emor
andu
m o
f U
nder
stan
ding
at
loca
l lev
el
prov
isio
n be
twee
n ho
spita
ls a
nd
the
Indo
nesi
an
Red
Cros
s is
es
tabl
ishe
d
and
the
Indo
nesi
an R
ed C
ross
is
esta
blis
hed
Basi
c H
ealth
Ca
re
Dev
elop
men
t,
Dir
ecto
rate
for
deve
lopm
ent o
f re
ferr
al
stan
dard
s
Dis
tric
t/Ci
ty
Leve
l
6.3.
Regu
latio
n on
ad
min
istr
ativ
e an
d fin
anci
al
gove
rnan
ce
6.3.
1. S
ubm
it a
prop
osal
to
the
loca
l go
vern
men
ts to
in
crea
se th
e re
gion
al
budg
et a
lloca
tion
to
supp
ort h
ealth
ac
tiviti
es th
at h
ave
a hi
gh le
vera
ge to
ac
hiev
e th
e M
DG
5:
Loca
l bud
get
allo
catio
n fo
r th
e ac
tiviti
es
that
hav
e hi
gh
leve
rage
to
achi
eve
MD
G 5
in
crea
ses
as
need
ed
Serv
ices
pro
vide
d by
PO
NEK
hos
pita
ls
for
24/7
and
by
at le
ast 4
PO
NED
co
mm
unity
hea
lth c
ente
rs fo
r 24
/7
per d
istr
ict a
nd b
y tr
aine
d m
idw
ives
ar
e pe
rfor
med
eve
ry y
ear
The
num
ber
of c
omm
unity
hea
lth
cent
ers
prov
idin
g em
erge
ncy
care
that
Loca
l G
over
nmen
t,
Loca
l Par
liam
ent

5048
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
PON
EK h
ospi
tals
, re
ferr
ed h
ospi
tals
, PO
NED
com
mun
ity
heal
th c
ente
rs a
nd
com
pete
nt
mid
wiv
es
are
conv
erte
d in
to c
omm
unity
hea
lth
cent
ers
prov
idin
g PO
NED
24/
7 in
crea
se to
4 p
er d
istr
ict i
n 20
14
6.
3.2.
Sub
mit
a pr
opos
al to
th
e lo
cal
gove
rnm
ents
abo
ut
the
need
for
brea
kthr
ough
eff
orts
re
late
d to
mat
erna
l an
d ne
onat
al c
are,
in
clud
ing
cons
ider
ing
the
emer
genc
y as
pect
s in
ser
vice
del
iver
y (a
fter
wor
king
ho
urs)
Regi
onal
re
gula
tion
on
brea
kthr
ough
ef
fort
s fo
r m
ater
nal a
nd
neon
atal
car
e,
incl
udin
g pr
ovis
ion
of
serv
ices
by
spec
ialis
ts, i
s de
velo
ped
In 2
013
the
regi
onal
reg
ulat
ion
rega
rdin
g m
ater
nal a
nd n
eona
tal c
are
is m
odifi
ed
Dir
ecto
rate
of
Mat
erna
l H
ealth
, D
irec
tora
te o
f Ch
ild H
ealth
6.
3.3.
Sub
mit
a pr
opos
al to
th
e lo
cal
gove
rnm
ents
to
mak
e cl
ear
regu
latio
ns fo
r bo
rder
and
rem
ote
area
s, in
clud
ing
the
regu
latio
n go
vern
ing
Polic
ies/
loca
l re
gula
tions
on
refe
rral
sys
tem
fo
r bo
rder
and
re
mot
e ar
eas
In 2
014
polic
ies/
loca
l reg
ulat
ions
on
refe
rral
sys
tem
for b
orde
r an
d re
mot
e ar
eas
are
effe
ctiv
e
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t

5149
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
the
refe
rral
sys
tem
of
obs
tetr
ic a
nd
neon
atal
cas
es to
fa
cilit
ate
the
peop
le
in th
ese
area
s to
ac
cess
the
heal
th
care
ser
vice
s ne
arby
6.
4. Re
gula
tion
on
impr
oved
qu
ality
/ski
lls o
f he
alth
pr
ofes
sion
als
6.4.
1. S
ubm
it a
prop
osal
to
the
loca
l go
vern
men
ts to
im
prov
e th
e qu
ality
an
d cl
inic
al s
kills
of
heal
th p
rofe
ssio
nals
th
roug
h tr
aini
ng,
appr
entic
eshi
p or
ot
her
trai
ning
pr
ogra
ms
Ann
ual p
lan
on
clin
ical
trai
ning
fo
r he
alth
pe
rson
nel i
s av
aila
ble
In 2
013
a cl
inic
al tr
aini
ng p
lann
ing
is
deve
lope
d fo
r 20
14 a
nd 2
015
Cent
er o
f Ed
ucat
ion
and
Trai
ning
for
Hea
lth
Prof
essi
onal
s
6.
4.2.
Reg
ulat
e th
e pe
rmit
for e
stab
lishi
ng
scho
ols
or a
cade
my
in th
e re
gion
s to
re
fer
to th
e cu
rren
t pr
ofes
sion
al
stan
dard
of
com
pete
nce
Pust
anse
rdik
BP
PSD
M
6.
4.3.
Con
duct
so
cial
izat
ion
of th
e
BP
PSD
M
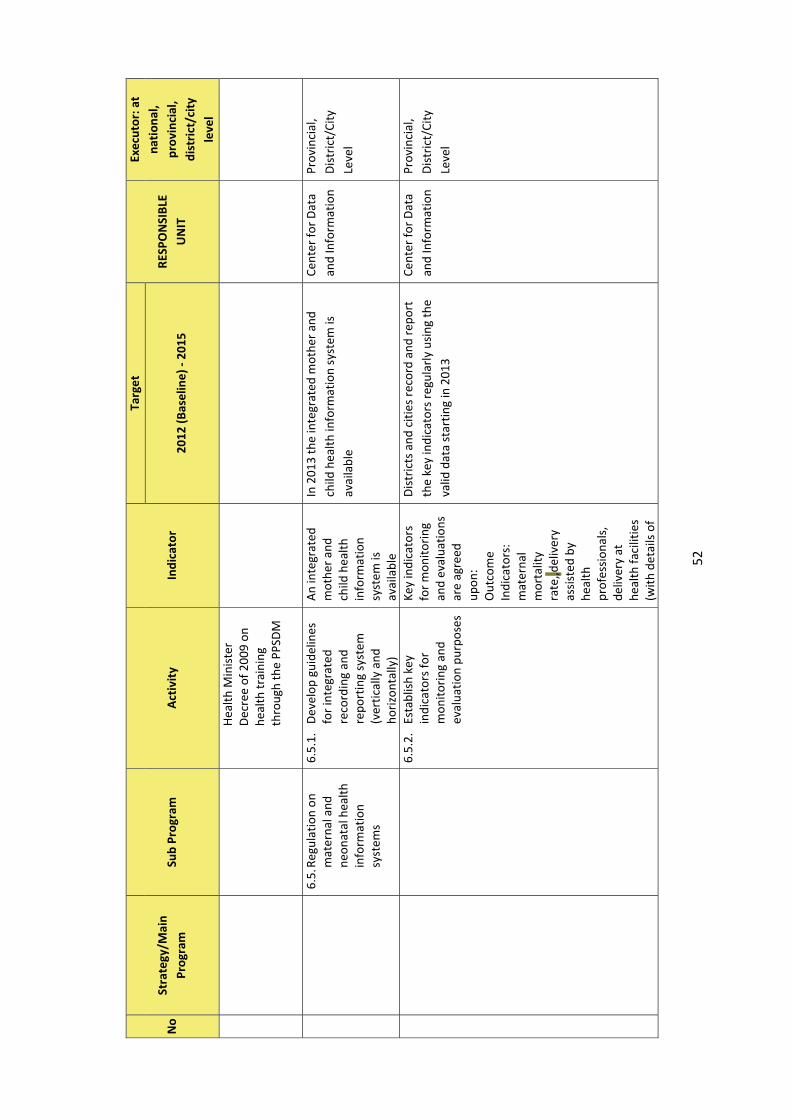
5250
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
Hea
lth M
inis
ter
Dec
ree
of 2
009
on
heal
th tr
aini
ng
thro
ugh
the
PPSD
M
6.5.
Regu
latio
n on
m
ater
nal a
nd
neon
atal
hea
lth
info
rmat
ion
syst
ems
6.5.
1.
Dev
elop
gui
delin
es
for
inte
grat
ed
reco
rdin
g an
d re
port
ing
syst
em
(ver
tical
ly a
nd
hori
zont
ally
)
An
inte
grat
ed
mot
her a
nd
child
hea
lth
info
rmat
ion
syst
em is
av
aila
ble
In 2
013
the
inte
grat
ed m
othe
r an
d ch
ild h
ealth
info
rmat
ion
syst
em is
av
aila
ble
Cent
er fo
r D
ata
and
Info
rmat
ion
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
6.
5.2.
Es
tabl
ish
key
indi
cato
rs fo
r m
onito
ring
and
ev
alua
tion
purp
oses
Key
indi
cato
rs
for
mon
itori
ng
and
eval
uatio
ns
are
agre
ed
upon
: O
utco
me
Indi
cato
rs:
mat
erna
l m
orta
lity
rate
,,del
iver
y as
sist
ed b
y he
alth
pr
ofes
sion
als,
de
liver
y at
he
alth
faci
litie
s (w
ith d
etai
ls o
f
Dis
tric
ts a
nd c
ities
rec
ord
and
repo
rt
the
key
indi
cato
rs re
gula
rly
usin
g th
e va
lid d
ata
star
ting
in 2
013
Cent
er fo
r D
ata
and
Info
rmat
ion
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l

5351
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
faci
litie
s ty
pe),
obst
etri
c co
mpl
icat
ions
re
ceiv
ing
trea
tmen
t at
PON
EK
hosp
itals
, tee
n bi
rth
rate
, 4-
time
visi
t
6.5.
3.
Cond
uct a
n an
alys
is
and
utili
zatio
n of
in
form
atio
n as
a
basi
s fo
r de
term
inin
g po
licie
s an
d pr
ogra
ms
Polic
ies
on
prog
ram
im
plem
enta
tion
base
d on
in
form
atio
n/da
ta
anal
ysis
are
av
aila
ble
In 2
013
polic
ies
on p
rogr
am
impl
emen
tatio
n ba
sed
on th
e an
nual
in
form
atio
n/da
ta a
naly
sis
are
avai
labl
e.
Balit
bang
kes
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
6.6.
Ass
uran
ce o
f su
ppor
t for
oth
er
requ
ired
re
gula
tion
6.6.
1. D
evel
op m
acro
and
fu
ndam
enta
l po
licie
s re
late
d to
co
mm
unity
hea
lth
cent
er. T
hese
po
licie
s in
clud
e th
e co
ncep
t of
com
mun
ity h
ealth
ce
nter
, spe
cific
w
orkf
orce
and
fin
anci
al
Polic
ies
on
com
mun
ity
heal
th c
ente
rs
whi
ch in
clud
es
the
conc
ept o
f co
mm
unity
he
alth
cen
ter,
sp
ecifi
c w
orkf
orce
and
fin
anci
al
gove
rnan
ce a
re
Star
ting
in 2
014
com
mun
ity h
ealth
ce
nter
s ha
ve m
acro
and
fund
amen
tal
polic
ies
whi
ch in
clud
e th
e co
ncep
t of
com
mun
ity h
ealth
cen
ter,
spe
cific
w
orkf
orce
and
fina
ncia
l gov
erna
nce
Dir
ecto
rate
of
Basi
c H
ealth
Ca
re
Dev
elop
men
t,
Fina
ncia
l Off
ice
and
BMN
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l

5452
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
gove
rnan
ce
avai
labl
e
6.6.
2. D
evel
op re
gula
tions
to
det
erm
ine
prio
rity
hea
lth c
are
area
s
Regu
latio
ns to
de
term
ine
prio
rity
are
as fo
r m
ater
nal a
nd
neon
atal
car
e ar
e av
aila
ble
In 2
013
the
regu
latio
ns o
n th
e de
term
inat
ion
of p
rior
ity h
ealth
car
e ar
eas
are
avai
labl
e
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
6.
6.3.
Con
duct
so
cial
izat
ion
of th
e na
tiona
l ref
erra
l gu
idel
ines
(Hea
lth
Min
iste
r Re
gula
tion
No.
1/2
012)
Soci
aliz
atio
n of
th
e re
gula
tions
on
the
dete
rmin
atio
n of
hea
lth c
are
prio
rity
are
as is
co
nduc
ted
In 2
013
the
regu
latio
n is
dis
sem
inat
ed
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
6.
6.4.
Dev
elop
regu
latio
ns
on th
e re
ferr
al
syst
em fo
r m
ater
nal
and
neon
atal
hea
lth
at d
istr
ict/
city
leve
l
Gui
delin
es fo
r m
ater
nal a
nd
neon
atal
hea
lth
refe
rral
are
av
aila
ble
In 2
013
guid
elin
es fo
r m
ater
nal a
nd
neon
atal
hea
lth r
efer
ral a
re a
vaila
ble
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
6.
6.5.
Con
duct
adv
ocac
y on
del
ayed
mar
riag
e ba
sed
on h
ealth
co
nsid
erat
ions
th
roug
h va
riou
s ap
proa
ches
, in
clud
ing
diss
emin
atio
n of
Adv
ocac
y m
ater
ials
/mes
sage
s ab
out
biol
ogic
al a
nd
psyc
holo
gica
l re
adin
es o
f te
ens
for
preg
nanc
y ar
e
In 2
013c
omm
unic
atio
n, in
form
atio
n an
d ed
ucat
ion
mat
eria
ls a
bout
te
enag
e m
arri
age
are
avai
labl
e an
d re
ady
for
dist
ribu
tion
Dir
ecto
rate
of
Child
Hea
lth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l

5553
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
com
mun
icat
ion,
in
form
atio
n an
d ed
ucat
ion
mat
eria
ls
abou
t bio
logi
cal a
nd
psyc
holo
gica
l re
adin
ess
of te
ens
for
preg
nanc
y
avai
labl
e
7.
Im
prov
ed
Cros
s-Se
ctor
al
and
Priv
ate
Part
ners
hip
W
ork
with
oth
er s
ecto
rs
othe
r tha
n lo
cal
gove
rnm
ent:
1.
Med
ical
edu
catio
n in
stitu
tions
to w
ork
in
loca
l hos
pita
ls to
en
sure
the
avai
labi
lity
of a
dequ
ate
serv
ice
24
hour
s/7
days
, suc
h as
th
roug
h th
e as
sign
men
t of
pos
t-gr
adua
te
stud
ents
of o
bste
tric
s pr
ogra
m
2.
Pri
vate
sec
tor
whi
ch
dire
ctly
pro
vide
s ob
stet
ric
care
(m
ater
nity
hos
pita
ls,
clin
ics,
gen
eral
MoU
on
any
form
of
coop
erat
ion
is
esta
blis
hed
In 2
013,
201
4 an
d 20
15 th
e nu
mbe
r of
M
oU o
n co
oper
atio
n at
pro
vinc
ial,
dist
rict
and
city
leve
l, bo
th w
ith
gove
rnm
ent a
nd p
riva
te s
ecto
r in
crea
ses
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Hea
lth O
ffic
e at
Pr
ovin
cial
, D
istr
ict a
nd C
ity
Leve
l, Lo
cal
Gov
ernm
ent,
Re
gion
al
Dev
elop
men
t Pl
anni
ng B
oard
; ho
spita
ls;
prof
essi
onal
or
gani
zatio
n,
Educ
atio
nal
Inst
itutio
n,
Relig
ious
In
situ
tion,
Pr
ivat
e Se
ctor

5654
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
hosp
itals
) is
expe
cted
to
bui
ld c
oord
inat
ion
for p
rovi
ding
mid
wife
ry
serv
ices
to th
e co
mm
unity
, inc
ludi
ng
the
refe
rral
sys
tem
, th
roug
h a
Mem
oran
dum
of
Und
erst
andi
ng (M
oU)
on C
oope
ratio
n 3.
The
Nat
iona
l Fam
ily
Plan
ning
Coo
rdin
atin
g Bo
ard,
to im
prov
e ac
cess
for
all w
omen
of
child
bear
ing
age
to
info
rmat
ion
on
repr
oduc
tive
heal
th a
nd
acce
ss to
fam
ily
plan
ning
met
hods
4.
Rel
igio
us s
ecto
r, to
im
prov
e ac
cess
for
all
girl
s in
relig
ion-
base
d sc
hool
s,
mad
rasah(
scho
ol
heal
th u
nit)
and
all

5755
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
brid
es-t
o-be
who
re
gist
er th
eir
mar
riag
e at
the
offic
e of
relig
ious
af
fair
s, to
info
rmat
ion
on r
epro
duct
ive
heal
th,
incl
udin
g bo
dy
read
ines
s fo
r fir
st
preg
nanc
y 5.
Pri
mar
y an
d se
cond
ary
educ
atio
n se
ctor
s, to
in
crea
se a
cces
s fo
r all
adol
esce
nts,
esp
ecia
lly
girl
s, in
sch
ools
(sch
ool
heal
th u
nit)
to
info
rmat
ion
on
repr
oduc
tive
heal
th.
The
impl
emen
tatio
n of
12
-yea
r co
mpu
lsor
y ed
ucat
ion
is e
xpec
ted
to b
e ut
ilize
d by
the
heal
th s
ecto
r to
con
vey
the
info
rmat
ion
rela
ted
to re
prod
uctiv
e he
alth
an
d ot
her h
ealth
-re
late
d in
form
atio
n
% o
f pri
vate
co
mpa
nies
that
ha
ve C
SR
prog
ram
on
mat
erna
l hea
lth

5856
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
6. P
riva
te s
ecto
r w
hich
ha
s in
dire
ct
role
s(ed
ucat
iona
l in
stitu
tions
for h
ealth
pe
rson
nel,
com
pani
es’
CSR)
is e
xpec
ted
to
wor
k to
geth
er to
im
prov
e m
idw
ifery
co
vera
ge a
nd s
ervi
ces,
ei
ther
thro
ugh
the
impr
oved
qua
lity
of
stud
ents
of h
ealth
-re
late
d pr
ogra
m b
ased
on
the
natio
nal
stan
dard
s, o
r th
roug
h th
e ut
iliza
tion
of C
SR
fund
s 7.
Pro
fess
iona
l or
gani
zatio
n, to
in
crea
se it
s ro
le in
im
prov
ing
the
qual
ity o
f se
rvic
es o
f its
mem
bers
, su
ch a
s th
roug
h tr
aini
ng,
appr
entic
eshi
p,
coac
hing
and

5957
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
arra
ngem
ent o
f pr
ofes
sion
al
licen
cere
gist
ratio
n. T
he
loca
l gov
ernm
ents
and
th
e lo
cal h
ealth
off
ices
ar
e ex
pect
ed to
wor
k w
ith th
e pr
ofes
sion
al
orga
niza
tions
in
acco
rdan
ce w
ith th
eir
resp
ectiv
e ro
les
as
agre
ed u
pon
8. R
elig
ious
org
aniz
atio
ns
can
play
a ro
le in
at
leas
t tw
o as
pect
s
Del
iver
y of
hea
lth
info
rmat
ion,
suc
h as
info
rmat
ion
on
repr
oduc
tive
heal
th
and
heal
th in
sura
nce
(mat
erni
ty
insu
ranc
e, n
atio
nal
soci
al s
ecur
ity
syst
em),
thro
ugh
the
exis
ting
orga
niza
tion
netw
orks
, and

6058
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
A
s pa
rt o
f the
Loc
al
Hea
lth S
ervi
ce
Net
wor
k 9.
Dev
elop
/im
prov
e ot
her
part
ners
hips
acc
ordi
ng
to th
e ci
rcum
stan
ces
and
cond
ition
s of
the
regi
ons
Stra
tegy
3: E
mpo
wer
ing
fam
ily a
nd c
omm
unity
8.
Im
prov
ed
Und
erst
andi
ng
and
Impl
emen
tatio
n of
Del
iver
y Pl
anni
ng a
nd
Com
plic
atio
ns
Prev
entio
n in
the
Com
mun
ity
8.1.
Reo
rien
tatio
n fo
r al
l rel
evan
t he
alth
per
sonn
el
rega
rdin
g th
e de
liver
y pl
anni
ng
and
com
plic
atio
ns
prev
entio
n pr
ogra
m to
cr
eate
the
sam
e ap
prop
riat
e un
ders
tand
ing
abou
t the
pr
ogra
m
conc
ept,
in
clud
ing
the
8.1.
1. R
eori
enta
tion
for a
ll re
leva
nt h
ealth
pe
rson
nel r
egar
ding
th
e de
liver
y pl
anni
ng a
nd
com
plic
atio
ns
prev
entio
n pr
ogra
m
to c
reat
e th
e sa
me
appr
opri
ate
unde
rsta
ndin
g ab
out t
he p
rogr
am
conc
ept,
incl
udin
g th
e pu
rpos
e an
d be
nefit
s of
the
prog
ram
, and
the
mea
sure
s th
at m
ust
Num
ber o
f co
mm
unity
he
alth
cen
ters
co
nduc
ting
reor
ient
atio
n ab
out t
he
deliv
ery
plan
ning
and
co
mpi
licat
ions
pr
even
tion
for
heal
th p
erso
nnel
In 2
014,
90%
of c
omm
unity
hea
lth
cent
ers
have
con
duct
ed o
rien
tatio
n ab
out t
he d
eliv
ery
plan
ning
and
co
mpl
icat
ions
pre
vent
ion
prog
ram
for
heal
th p
erso
nnel
.
Cent
er fo
r H
ealth
Pr
omot
ion,
D
irec
tora
te o
f M
ater
nal H
ealth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l

6159
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
purp
ose
and
bene
fits
of th
e pr
ogra
m, a
nd
the
mea
sure
s th
at m
ust b
e ta
ken
be ta
ken
8.
1.2.
Con
duct
ori
enta
tion
for h
ealth
cad
res
and
soci
ety
abou
t th
e da
nger
sig
ns o
f pr
egna
ncy
and
child
birt
h as
wel
l as
thei
r ro
le in
the
deliv
ery
plan
ning
an
d co
mpl
icat
ions
pr
even
tion
prog
ram
Num
ber o
f co
mm
unity
he
alth
cen
ters
co
nduc
ting
orie
ntat
ion
for
heal
th c
adre
s ab
out t
he
bene
fits
and
step
s of
the
deliv
ery
plan
ning
and
co
mpl
icat
ions
pr
even
tion
prog
ram
In 2
014,
90%
of c
omm
unity
hea
lth
cent
ers
cond
uct o
rien
tatio
n ab
out t
he
deliv
ery
plan
ning
and
com
plic
atio
ns
prev
entio
n pr
ogra
m t
o he
alth
cad
res
Cent
er fo
r H
ealth
Pr
omot
ion,
D
irec
tora
te o
f M
ater
nal H
ealth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l and
cro
ss-
sect
or (P
KK,
PMD
)
8.2.
Reo
rien
tatio
n ab
out t
he
impo
rtan
ce o
f ne
cess
ary
mea
sure
s du
ring
8.2.
1. C
ondu
ct m
ater
nal
clas
s us
ing
mot
her
and
child
hea
lth
guid
e bo
ok
Num
ber o
f co
mm
unity
he
alth
cen
ters
co
nduc
ting
mat
erna
l cla
ss
usin
g m
othe
r
Num
ber o
f com
mun
ity h
ealth
cen
ters
co
nduc
ting
mat
erna
l cla
ss in
crea
ses
ever
y ye
ar a
nd b
y th
e en
d of
201
3 50
% o
f pub
lich
heal
th c
ente
rs h
ave
cond
ucte
d m
ater
nal c
lass
usi
ng
Dir
ecto
rate
of
Mat
erna
l Hea
lth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l

6260
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
preg
nanc
y an
d ch
ildbi
rth
and
child
hea
lth
Gui
delin
e m
othe
r and
chi
ld h
ealth
Gui
delin
e
8.
2.2.
Soc
ializ
e th
e da
nger
si
gns
of p
regn
ancy
an
d ch
ildbi
rth
thro
ugh
appr
opri
ate
med
ia to
eve
ry
segm
ent o
f soc
iety
in
acc
orda
nce
with
th
e ac
cept
able
cu
lture
and
nor
ms
% o
f pre
gnan
t m
othe
rs w
ho
unde
rsta
nd th
e da
nger
sig
ns o
f pr
egna
ncy
In 2
015
, 70
% o
f pre
gnan
t mot
hers
un
ders
tand
the
dang
er s
igns
of
preg
nanc
y, c
hild
birt
h an
d pu
erpe
rium
Cent
er fo
r H
ealth
Pr
omot
ion,
D
irec
tora
te o
f M
ater
nal H
ealth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l
8.
2.3.
Con
duct
so
cial
izat
ion
abou
t th
e im
port
ance
of
anem
ia p
reve
ntio
n th
roug
h he
alth
y lif
esty
le, c
onsu
min
g bl
ood
supp
lem
ent
pills
, and
con
sum
ing
nutr
itiou
s ba
lanc
ed
food
dur
ing
preg
nanc
y
Soci
aliz
atio
n ab
out t
he
impo
rtan
ce o
f an
emia
pr
even
tion
for
preg
nant
m
othe
rs is
co
nduc
ted
thro
ugh
suita
ble
med
ia fo
r al
l pu
blic
seg
men
ts:
preg
nant
m
othe
rs w
ho
com
e to
hea
lth
care
faci
litie
s,
By th
e en
d of
201
3 co
mm
unic
atio
n,
info
rmat
ion
and
educ
atio
n m
ater
ials
ab
out a
nem
ia o
n pr
egna
nt m
othe
rs
are
avai
labl
e fo
r va
riou
s se
gmen
ts o
f so
ciet
y at
nat
iona
l lev
el
At t
he b
egin
ning
of 2
014
com
mun
icat
ion,
info
rmat
ion
and
educ
atio
n m
ater
ials
abo
ut a
nem
ia o
n pr
egna
nt m
othe
rs a
re a
vaila
ble
for
vari
ous
segm
ents
of s
ocie
ty a
t dis
tric
t an
d ci
ty le
vel a
nd in
com
mun
ity h
ealth
ce
nter
s
Cent
er fo
r H
ealth
Pr
omot
ion,
D
irec
tora
te o
f M
ater
nal H
ealth
Prov
inci
al,
Dis
tric
t/Ci
ty
Leve
l

6361
No
Stra
tegy
/Mai
n Pr
ogra
m
Sub
Prog
ram
A
ctiv
ity
In
dica
tor
Targ
et
RESP
ON
SIBL
E U
NIT
Exec
utor
: at
nati
onal
, pr
ovin
cial
, di
stri
ct/c
ity
leve
l
2012
(Bas
elin
e) -
2015
brid
es-t
o-be
, te
enag
e st
uden
ts a
t pu
blic
sc
hool
s/m
adra
s ah
In 2
015
100%
of c
omm
unity
hea
lth
cent
ers
cond
uct s
ocia
lizat
ion
abou
t an
emia
, eith
er d
irec
tly o
r th
roug
h co
oper
atio
n w
ith o
ther
sec
tors
.