relationship between chewing ability and high-level functional capacity in an 80-year-old population...
TRANSCRIPT

Or ig ina l a r t i c l e
Relationship between chewing ability and high-level functionalcapacity in an 80-year-old population in Japan
Yutaka Takata1, Toshihiro Ansai2, Inho Soh2, Sumio Akifusa2, Kazuo Sonoki1, KiyoshiFujisawa1, Akihiro Yoshida2, Shuntaro Kagiyama1, Tomoko Hamasaki2, Ikuo Nakamichi1,
Shuji Awano2, Takehiro Torisu1 and Tadamichi Takehara2
Divisions of 1General Internal Medicine; and 2Community Oral Health Science, Department of Health Promotion, Kyushu Dental College,
Kitakyushu, Japan
doi:10.1111/j.1741-2358.2007.00203.x
Relationship between chewing ability and high-level functional capacity in an 80-year-old populationin Japan
Objectives: To evaluate the association between high-level functional capacity and chewing in a middle-
old community-based population.
Background: Although basic and instrumental activities of daily living are known to be associated with
chewing ability in the elderly, an association between higher levels of competence and chewing ability has
not been evaluated in the elderly.
Materials and methods: The association between chewing ability using a number of different foods and
high-level functional capacity by the Tokyo Metropolitan Institute of Gerontology was evaluated in 694,
80-year-old people residing in Fukuoka Prefecture, Japan.
Results: A significant correlation was found, using multiple regression or logistic regression analyses
adjusted for various confounding factors, between the number of total chewable foods, hard foods or
moderately hard foods, and total functional capacity, instrumental activity, intellectual activity or social
role ability. In contrast, the number of slightly hard foods, easily chewable foods and remaining teeth were
only partly related to total functional capacity and intellectual activity.
Conclusion: High-level functional capacity including intellectual activity and social role in middle-old
elderly was associated with the ability to chew hard foods than to chew easily chewable foods. Mainte-
nance of chewing ability in elderly might result in better intellectual activity and social role.
Keywords: chewing, ADL, elderly, dental.
Accepted 13 September 2007
Introduction
It is well known that there is an association
between impaired chewing ability and malnutri-
tion. Impaired chewing ability may affect nutrient
intake1,2 and exacerbate nutritional status3,4. It is
also reported to be associated with general health
status among the elderly5–7. On the other hand,
masticatory ability for gummy jelly was reported to
be influenced by cognitive function in the elderly,
suggesting limitation using a test food8. Miura
et al.5 conducted a study on 79 elderly individuals
ranging in age between 65 and 74 years and found
that chewing ability was related to activities of daily
living (ADL) as determined by the Ministry of
Health and Welfare of Japan or the Tokyo Metro-
politan Institute of Gerontology (TMIG)9,10. Locker
et al.11 followed up community-dwelling old indi-
viduals aged 50 years and older for over 7 years,
and concluded that poor general health at baseline
increased the onset of a chewing problem. In a very
elderly Japanese population it was found that
chewing ability may contribute to independence in
ADL12. Physical fitness13 and quality of life (QOL)14
were also associated with chewing ability in the
very elderly and recently was found to be associ-
ated with mortality in community residents and a
possible predictor for their survival rate15.
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154 147

Although basic ADL, which includes feeding,
bathing, toileting and dressing, and instrumental
ADL, which includes shopping, preparing meals
and using transportation are known to be associ-
ated with chewing ability in the elderly, an asso-
ciation between higher levels of competence
(intellectual activity or social role activity) and
chewing ability has not been evaluated in a very
elderly population. Therefore, this study evaluated
the association between high-level ADL and
chewing in a middle-old community-based
population.
Materials and methods
In 1998, 1282 80-year-old individuals residing in
one of three cities (Buzen, Yukuhashi or Munak-
ata), four towns (Katsuyama, Tikujo, Toyotsu or
Kanda), one village (Shinyoshitomi), or one ward
(Tobata of Kikakyushu City) in Fukuoka Prefecture
of Japan were invited to participate in the present
study. Of these, 694 (54.1%) (276 male and 418
female) were included. The distribution of partici-
pants was 132 of 192 (68.8%) 80-year-old residents
in Buzen, 81 of 159 (50.9%) in Yukuhashi, 146 of
283 (51.6%) in Munakata, 24 of 42 (57.1%) in
Katsuyama, 42 of 67 (62.7%) in Tsuiki, 17 of 40
(42.5%) in Toyotsu, 58 of 116 (50.0%) in Kanda,
23 of 28 (82.1%) in Shinyoshitomi and 174 of 355
(49.0%) in Tobata. The authors performed a dental
examination on each subject in the manner rec-
ommended by the World Health Organization16.
The study was approved by the Human Investiga-
tions Committee of Kyushu Dental College, and
informed consent was obtained from all partici-
pants. The protocol was in accordance with the
Helsinki Declaration of 1975, as revised in 2000.
Questionnaires concerning food intake have
proved valuable in epidemiological surveys of
masticatory function in the elderly17–19. Accord-
ingly, each subject was asked about their ability to
chew the following 15 foods: peanuts, yellow
pickled radish, hard rice crackers, French bread,
beefsteak, octopus in vinegar, pickled shallots,
dried scallops, dried cuttlefish, squid sashimi,
konnyaku, a tubular roll of boiled fish paste, boiled
rice, tuna sashimi and grilled eel. These were se-
lected to represent four main groups: three foods
that are very hard to chew (hard rice crackers,
peanuts and yellow pickled radish), six foods that
are moderately hard to chew (French bread, beef-
steak, octopus in vinegar, pickled shallots, dried
scallops and dried cuttlefish), three foods that are
slightly hard to chew (konnyaku, a tubular roll of
boiled fish paste and squid sashimi) and three foods
that are easy to chew (boiled rice, tuna sashimi and
grilled eel)20. Japanese investigators21 compared
two methods, a chewing gum method and ques-
tionnaire, for examining masticatory ability, and
concluded that both tests were useful for evaluat-
ing chewing ability in epidemiological studies.
A questionnaire from 100 different food substances
was compared with the questionnaire in this study
for 15 in 110 full denture wearers, concluding that
the larger questionnaire is superior22. Nevertheless,
the shorter version has been widely used for sur-
veying the Japanese elderly population23. The
number of foods that a subject could chew was
used as an index of chewing ability. This was as-
sessed as a possible independent influence on the
high-level functional capacity as assessed by the
TMIG Index of Competence9,10, using multivariate
and logistic regression analyses.
The TMIG Index of Competence, a standardised
multidimensional 13-item instrument developed
by the TMIG group, was used to measure func-
tional capacity and in turn to measure the level of
competence corresponding to the fifth, sixth and
seventh sublevels of Lawton’s model24. The
13 items are shown in Table 1: items 1–5 were
Table 1 Tokyo Metropolitan Institute of Gerontology
Index of Competence.
Items
Instrumental
self-maintenance
1. Can you use public
transportation (the bus or
train) by yourself unaided?
2. Are you able to shop for
daily necessities?
3. Are you able to prepare meals
by yourself?
4. Are you able to arrange to
pay bills?
5. Can you handle your own
banking?
Intellectual
activity
6. Are you able to fill in forms
for your pension?
7. Do you read the newspaper?
8. Do you read books or
magazines?
9. Are you interested in news
stories or programmes dealing
with health?
Social roles 10. Do you visit friends’ homes?
11. Are you sometimes asked for
advice?
12. Are you able to visit sick
friends?
13. Do you sometimes initiate
conversations with young people?
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154
148 Y. Takata et al.

classified as instrumental self-maintenance, items
6–9 as intellectual activity, items 10–13 as social
roles and items 1–13 as total functional capacity.
The response to each item was simply ‘yes’ or ‘no’,
and was scored 1 for ‘yes’ or 0 for ‘no’. The total
score was the sum total of the number of items
answered ‘yes’, and a high score indicated high-
level functional capacity. A score for each subscale
of this index was also used to measure the capacity
levels of instrumental self-maintenance, intellec-
tual activity or social roles.
All data are reported as mean ± SD. Differences
in mean values between groups were assessed by
analysis of variance. When comparing between
groups, the chewable number of foods and number
of teeth were classified into four groups as shown
in Table 2. Categorical variables were compared
using the chi-squared test. Multiple regression
analysis was carried out to evaluate which factors
were related to high-level functional capacity after
adjustment for confounding variables. Logistic
regression was also used to determine which cate-
gorical factors were independent predictors of
functional capacity. All statistical analyses were
performed using StatView 5.0 (SAS Institute, Cary,
NC, USA). Results were considered statistically
significant when p < 0.05.
Results
The mean number of teeth was 8.0 ± 8.9 (n = 694),
and the number of foods that subjects could chew
was 11.6 ± 3.6 (n = 686). Of these individuals, 656
filled in questionnaires for the TMIG Index of
Competence. The mean scores of the TMIG index
were 10.9 ± 2.7 for total functional capacity
(maximum 13 points), 4.1 ± 1.3 for instrumental
self-maintenance (maximum 5 points), 3.1 ± 1.1
for intellectual activity (maximum 4 points) and
2.8 ± 1.2 for social roles (maximum points 4
points). A gender difference was present in the total
number of foods that were chewed, in the number
of foods very hard to chew and in those moderately
hard to chew, while no gender difference was
found in those slightly hard to chew and in those
easy to chew (Table 3). The number of teeth was
also different between men and women. However,
there was no gender difference in total functional
capacity, instrumental self-maintenance and social
roles, whilst a slight gender difference was found in
intellectual activity.
Associations of chewing ability or number of
teeth with high-level functional capacity were as-
sessed by simple regression analyses (Table 4).
Significant correlations were found in the total
Table 2 Groups according to
number of chewable foods and
number of teeth.
Group 1 Group 2 Group 3 Group 4
Total number of chewable foods 0–4 5–9 10–14 15
Number of foods very hard to chew 0 1 2 3
Number of foods moderately hard
to chew
0–1 2–3 4–5 6
Number of foods slightly hard
to chew
0 1 2 3
Number of foods easy to chew 0 1 2 3
Number of teeth 0 1–9 10–19 20‡
Table 3 Number of chewable foods,
number of teeth and Tokyo Metro-
politan Institute of Gerontology
Index of Competence in men and
women.
Men Women
Total number of chewable foods 12.1 ± 3.4 11.2 ± 3.6�
Number of foods very hard to chew 2.4 ± 0.9 2.1 ± 1.1�
Number of foods moderately hard to chew 4.1 ± 1.9 3.6 ± 2.1�
Number of foods slightly hard to chew 2.7 ± 0.7 2.6 ± 0.7
Number of foods easy to chew 2.9 ± 0.5 2.8 ± 0.5
Number of teeth 9.5 ± 9.6 7.0 ± 8.2�
Total functional capacity 9.9 ± 2.7 10.0 ± 2.5
Instrumental self-maintenance 4.1 ± 1.3 4.2 ± 1.3
Intellectual activity 3.2 ± 1.0 3.0 ± 1.1*
Social roles 2.7 ± 1.2 2.8 ± 1.1
*p < 0.05, �p < 0.01, �p < 0.001.
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154
Chewing and high-level ADL in the elderly 149

number of foods chewed, the number of foods hard
to chew or those moderately hard to chew with
total functional activity, instrumental activity,
intellectual activity or social role activity. It was
also found that the number of teeth or number of
foods easy to chew was only slightly associated
with intellectual activity, but was not associated
with total functional activity, instrumental activity
or social role activity. In the number of foods
slightly hard to chew, a slight but significant asso-
ciation was found both with total functional
capacity and intellectual activity.
Total functional capacity and intellectual activity
were improved significantly in groups with an in-
creased number of total chewable foods, hardly
chewable foods or moderately hardly chewable
foods (Table 5). Instrumental activity also was im-
proved with increases in moderately hardly chew-
able foods, and intellectual activity improved with
increases in easily chewable foods. Intellectual
activity was increased with more remaining teeth
(v2=12.4, p < 0.01), but total functional capacity,
instrumental activity or social role was not different
among the four groups relating to number of teeth
(0, 1–9, 10–19, 20‡).
Multiple regression analysis adjusted for gender,
smoking, marital status and regular dental or
medical care showed that the total number of foods
to chew, number of foods hardly chewable or
number of foods moderately hardly chewable was
positively related to total functional capacity,
instrumental activity, intellectual activity or social
role activity (Table 6). The number of slightly hard
chewable foods, however, was only associated with
total functional capacity, and that of teeth or easy
chewable foods was only associated with intellec-
tual activity. Explanatory factors such as gender,
smoking, marital status and regular dental or
medical care on high-level ADL in regression
analysis was selected because there was gender
difference in the number of chewable foods and
ADL level. In addition, it is likely that marital status
and regular dental or medical care could be related
to dental care.
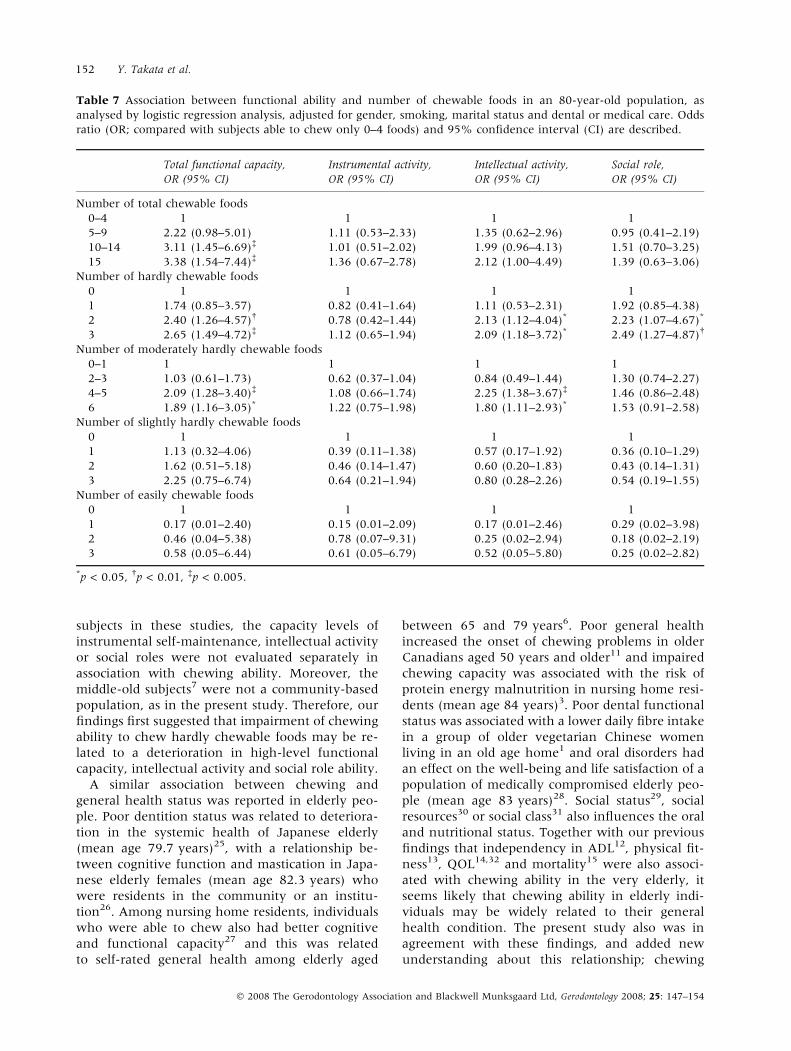
For logistic regression analysis, the subjects were
grouped according to the number of foods they
could chew (Table 7). Similar to the multiple
regression analysis, gender, smoking, marital status
and regular dental or medical care were adjusted as
confounding factors. Increases in total functional
capacity were 3.1 times or 3.4 times more prevalent
in individuals who were able to chew 10–14 or 15
foods than in those who were able to chew only 0–
4 foods. Similarly, total functional capacity was
improved in individuals who were able to chew a
higher number of hardly chewable foods or mod-
erately hardly chewable foods than in those who
were able to chew only few foods. Intellectual
activity was also improved in individuals who were
able to chew hard-to-chew foods or moderately
hard-to-chew foods, while social role activity was
only related to the number of hard-to-chew foods.
Improved total functional capacity was more pre-
valent in individuals with 1–9 remaining teeth than
in edentulous individuals (OR, 1.54; 95% CI, 1.02–
2.30; p £ 0.05), and the prevalence of improved
intellectual activity was higher in individuals with
20 and more teeth (OR, 1.91; 95% CI, 1.16–3.15;
p < 0.05) or 10–19 teeth (OR, 2.01, 95% CI, 1.28–
3.17; p < 0.01) than in edentate individuals.
Discussion
In the present study, a relationship was found be-
tween high-level functional capacity and chewing
ability in a community-based middle-old Japanese
population. The number of very hard and moder-
ately hard chewable foods was more closely asso-
ciated with high-level functional capacity rather
than that of slightly hardly and easily chewable
Table 4 Correlations between func-
tional ability and number of chew-
able foods or teeth, using simple
regression analysis in an 80-year-old
population. Coefficient of correlation
(r) is described.
Total
functional
capacity
Instrumental
activity
Intellectual
activity
Social
role
Total chewable foods 0.157§ 0.100* 0.159§ 0.099*
Hardly chewable foods 0.162§ 0.107� 0.133� 0.126�
Moderately hardly
chewable foods
0.153§ 0.096* 0.162§ 0.091*
Slightly hardly chewable
foods
0.086* 0.060 0.079* 0.055
Easily chewable foods 0.048 0.021 0.095* 0.002
Teeth 0.070 0.032 0.100* 0.032
*p < 0.05, �p < 0.01, �p < 0.001, §p < 0.0001.
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154
150 Y. Takata et al.

foods. Intellectual activity and social role ability
were also more closely associated with the number
of chewable foods than instrumental activity.
A high level of competence using TMIG was
similarly reported to be associated with chewing
activity in 79 young-old (mean age 69.3 years)
subjects who were living in a Japanese Prefecture5,
and in 92 middle-old (mean age 80.5 years) sub-
jects who were residents in a nursing home for frail
elderly7. However, because of the small number of
Table 5 Prevalence of improved
high-level functional capacity among
four chewing groups in an 80-year-
old population, with the difference
being compared by chi-squared test.
Number of subjects who had im-
proved functional capacity/number
of all subjects, corresponding to the
number of chewable foods.
Total functional
capacity
Instrumental
activity
Intellectual
activity Social role
Number of total chewable foods
0–4 10/38 (26.3) 20/38 (52.6) 12/38 (31.6) 10/38 (26.3)
5–9 58/125 (46.4) 71/125 (56.8) 47/125 (37.6) 34/125 (27.2)
10–14 152/294 (51.7) 154/294 (52.4) 140/294 (47.6) 102/294 (34.7)
15 107/192 (55.7) 115/192 (59.9) 96/192 (50.0) 65/192 (33.9)
v2 12.0� 2.9 8.2 * 3.1
Number of hardly chewable foods
0 21/66 (31.8) 37/66 (56.1) 21/66 (31.8) 13/66 (19.7)
1 32/70 (45.7) 37/70 (52.9) 24/70 (34.3) 21/70 (30.0)
2 64/126 (50.8) 62/126 (49.2) 60/126 (47.6) 41/126 (32.5)
3 210/386 (54.4) 224/386 (58.0) 190/386 (49.2) 136/386 (35.2)
v2 12.2� 3.2 10.9* 6.4
Number of moderately hardly chewable foods
0–1 48/116 (41.4) 66/116 (56.9) 41/116 (35.3) 32/116 (27.6)
2–3 57/141 (40.4) 62/141 (44.0) 47/141 (33.3) 42/141 (29.8)
4–5 109/190 (57.4) 110/190 (57.9) 105/190 (55.3) 66/190 (34.7)
6 113/201 (56.2) 122/201 (60.7) 102/201 (50.7) 71/201 (35.3)
v2 15.8� 10.3* 22.8� 2.9
Number of slightly hardly chewable foods
0 5/15 (33.3) 10/15 (66.7) 8/15 (53.3) 7/15 (46.7)
1 14/38 (36.8) 17/38 (44.7) 14/38 (36.8) 10/38 (26.3)
2 45/99 (45.5) 51/99 (51.5) 38/99 (38.4) 28/99 (28.3)
3 263/496 (53.0) 282/496 (56.9) 235/496 (47.4) 166/496 (33.5)
v2 6.9 3.5 4.2 3.0
Number of easily chewable foods
0 2/3 (66.7) 2/3 (66.7) 2/3 (66.7) 2/3 (66.7)
1 5/19 (26.3) 5/19 (26.3) 5/19 (26.3) 7/19 (36.8)
2 23/52 (44.2) 32/52 (61.5) 15/52 (28.8) 13/52 (25.0)
3 297/574 (51.7) 321/574 (55.9) 273/574 (47.6) 189/574 (32.9)
v2 5.9 7.5 10.2* 3.1
Values in parenthesis are expressed in percentage.*p < 0.05, �p < 0.01, �p < 0.005.
Table 6 Relationship between func-
tional ability and number of chew-
able foods or teeth in an 80-year-old
population, as analysed by multiple
regression analysis, adjusted for gen-
der, smoking, marital status and
dental or medical care. Standardized
regression coefficient (b-value) is
described.
Total
functional
capacity
Instrumental
activity
Intellectual
activity
Social
role
Total chewable foods 0.162§ 0.106� 0.152§ 0.110�
Hardly chewable foods 0.171§ 0.116� 0.132� 0.137§
Moderately hardly
chewable foods
0.156§ 0.100* 0.155§ 0.100*
Slightly hardly chewable
foods
0.088* 0.064 0.068 0.065
Easily chewable foods 0.053 0.023 0.097* 0.006
Teeth 0073 0.036 0.091* 0.043
*p < 0.05, �p < 0.01, �p < 0.005, §p < 0.001.
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154
Chewing and high-level ADL in the elderly 151
subjects in these studies, the capacity levels of
instrumental self-maintenance, intellectual activity
or social roles were not evaluated separately in
association with chewing ability. Moreover, the
middle-old subjects7 were not a community-based
population, as in the present study. Therefore, our
findings first suggested that impairment of chewing
ability to chew hardly chewable foods may be re-
lated to a deterioration in high-level functional
capacity, intellectual activity and social role ability.
A similar association between chewing and
general health status was reported in elderly peo-
ple. Poor dentition status was related to deteriora-
tion in the systemic health of Japanese elderly
(mean age 79.7 years)25, with a relationship be-
tween cognitive function and mastication in Japa-
nese elderly females (mean age 82.3 years) who
were residents in the community or an institu-
tion26. Among nursing home residents, individuals
who were able to chew also had better cognitive
and functional capacity27 and this was related
to self-rated general health among elderly aged
between 65 and 79 years6. Poor general health
increased the onset of chewing problems in older
Canadians aged 50 years and older11 and impaired
chewing capacity was associated with the risk of
protein energy malnutrition in nursing home resi-
dents (mean age 84 years)3. Poor dental functional
status was associated with a lower daily fibre intake
in a group of older vegetarian Chinese women
living in an old age home1 and oral disorders had
an effect on the well-being and life satisfaction of a
population of medically compromised elderly peo-
ple (mean age 83 years)28. Social status29, social
resources30 or social class31 also influences the oral
and nutritional status. Together with our previous
findings that independency in ADL12, physical fit-
ness13, QOL14,32 and mortality15 were also associ-
ated with chewing ability in the very elderly, it
seems likely that chewing ability in elderly indi-
viduals may be widely related to their general
health condition. The present study also was in
agreement with these findings, and added new
understanding about this relationship; chewing
Table 7 Association between functional ability and number of chewable foods in an 80-year-old population, as
analysed by logistic regression analysis, adjusted for gender, smoking, marital status and dental or medical care. Odds
ratio (OR; compared with subjects able to chew only 0–4 foods) and 95% confidence interval (CI) are described.
Total functional capacity,
OR (95% CI)
Instrumental activity,
OR (95% CI)
Intellectual activity,
OR (95% CI)
Social role,
OR (95% CI)
Number of total chewable foods
0–4 1 1 1 1
5–9 2.22 (0.98–5.01) 1.11 (0.53–2.33) 1.35 (0.62–2.96) 0.95 (0.41–2.19)
10–14 3.11 (1.45–6.69)� 1.01 (0.51–2.02) 1.99 (0.96–4.13) 1.51 (0.70–3.25)
15 3.38 (1.54–7.44)� 1.36 (0.67–2.78) 2.12 (1.00–4.49) 1.39 (0.63–3.06)
Number of hardly chewable foods
0 1 1 1 1
1 1.74 (0.85–3.57) 0.82 (0.41–1.64) 1.11 (0.53–2.31) 1.92 (0.85–4.38)
2 2.40 (1.26–4.57)� 0.78 (0.42–1.44) 2.13 (1.12–4.04)* 2.23 (1.07–4.67)*
3 2.65 (1.49–4.72)� 1.12 (0.65–1.94) 2.09 (1.18–3.72)* 2.49 (1.27–4.87)�
Number of moderately hardly chewable foods
0–1 1 1 1 1
2–3 1.03 (0.61–1.73) 0.62 (0.37–1.04) 0.84 (0.49–1.44) 1.30 (0.74–2.27)
4–5 2.09 (1.28–3.40)� 1.08 (0.66–1.74) 2.25 (1.38–3.67)� 1.46 (0.86–2.48)
6 1.89 (1.16–3.05)* 1.22 (0.75–1.98) 1.80 (1.11–2.93)* 1.53 (0.91–2.58)
Number of slightly hardly chewable foods
0 1 1 1 1
1 1.13 (0.32–4.06) 0.39 (0.11–1.38) 0.57 (0.17–1.92) 0.36 (0.10–1.29)
2 1.62 (0.51–5.18) 0.46 (0.14–1.47) 0.60 (0.20–1.83) 0.43 (0.14–1.31)
3 2.25 (0.75–6.74) 0.64 (0.21–1.94) 0.80 (0.28–2.26) 0.54 (0.19–1.55)
Number of easily chewable foods
0 1 1 1 1
1 0.17 (0.01–2.40) 0.15 (0.01–2.09) 0.17 (0.01–2.46) 0.29 (0.02–3.98)
2 0.46 (0.04–5.38) 0.78 (0.07–9.31) 0.25 (0.02–2.94) 0.18 (0.02–2.19)
3 0.58 (0.05–6.44) 0.61 (0.05–6.79) 0.52 (0.05–5.80) 0.25 (0.02–2.82)
*p < 0.05, �p < 0.01, �p < 0.005.
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154
152 Y. Takata et al.

ability to chew hardly chewable foods was more
closely associated with high-level functional
capacity, especially intellectual activity and social
role, than the ability to chew easily chewable foods.
Although the time span between the collection of
the data and our publication was considerably long,
the present findings could be considered worth-
while. Maintenance of chewing ability in the
elderly might contribute to better intellectual
activity and social roles.
In conclusion, high-level functional capacity,
including intellectual activity and social role in
middle-old elderly, had a greater association with
the ability to chew a larger number of hard chew-
able foods than with the ability to chew easily
chewable foods.
Acknowledgements
This work was supported in part by Grants-in-Aid
for Scientific Research (B) 18390570, 15390655
and by a Grant-in-Aid for Exploratory Research (C)
17659663 from the Japan Society for the Promo-
tion of Science.
References
1. Kwok T, Yu CN, Hui HW et al. Association be-
tween functional dental state and dietary intake of
Chinese vegetarian old age home residents. Gerodon-
tology 2004; 21: 161–166.
2. Kwon J, Suzuki T, Kumagai S et al. Risk factors
for dietary variety decline among Japanese elderly
in a rural community: an 8-year follow-up study
from TMIG-LISA. Eur J Clin Nutr 2006; 60: 305–
311.
3. Nordenram G, Ljunggren G, Cederholm T.
Nutritional status and chewing capacity in nursing
home residents. Aging (Milano) 2001; 13: 370–377.
4. Ritchie CS, Burgio KL, Locher JL et al. Nutritional
status of urban homebound older adults. Am J Clin
Nutr 1997; 66: 815–818.
5. Miura H, Araki Y, Umenai T. Chewing activity and
activities of daily living in the elderly. J Oral Rehabil
1997; 24: 457–460.
6. Miura H, Arai Y, Sakano S et al. Subjective eval-
uation of chewing ability and self-rated general
health status in elderly residents of Japan. Asia Pac J
Public Health 1998; 10: 43–45.
7. Miura H, Kariyasu M, Yamasaki K et al. Rela-
tionship between general health status and change in
chewing ability: a longitudinal study of the frail el-
derly in Japan over a 3-year period. Gerodontology
2005; 22: 200–205.
8. Ono T, Hori K, Ikebe K et al. Factors influencing
eating ability of old in-patients in a rehabilitation
hospital in Japan. Gerodontology 2003; 20: 24–31.
9. Shibata H, Sugisawa H, Watanabe S. Functional
capacity in elderly Japanese living in the community.
Geriatr Gerontol Int 2001; 1: 8–13.
10. Koyano W, Shibata H, Nakazato K et al. Mea-
surement of competence: reliability and validity of
the TMIG index of competence. Arch Gerontol Geriatr
1991; 13: 103–116.
11. Locker D, Matear D, Lawrence H. General health
status and changes in chewing ability in older Cana-
dians over seven years. J Public Health Dent 2002; 62:
70–77.
12. Takata Y, Ansai T, Awano S et al. Activities of
daily living and chewing ability in an 80-year-old
population. Oral Dis 2004; 10: 365–368.
13. Takata Y, Ansai T, Awano S et al. Relationship of
physical fitness to chewing in an 80-year-old popu-
lation. Oral Dis 2004; 10: 44–49.
14. Takata Y, Ansai T, Awano S et al. Chewing ability
and quality of life in an 80-year-old population. J Oral
Rehabil 2006; 33: 330–334.
15. Ansai T, Takata Y, Soh I et al. Relationship be-
tween chewing ability and 4-year mortality in a co-
hort of 80-year-old Japanese people. Oral Dis 2007;
13: 214–219.
16. World Health Organization. Oral Health Surveys,
Basic Methods, 4th edn. Geneva: WHO, 1997.
17. Slade GD, Spencer AJ, Roberts-Thomson K.
Tooth loss and chewing capacity among older adults
in Adelaide. Aust NZ J Public Health 1996; 20: 76–82.
18. Nagai H, Shibata H, Haga H et al. Chewing ability
in relation to physical health status. Nippon Ronen
Igakkai Zasshi 1990; 27: 63–68.
19. Leake JL. An index of chewing ability. J Public Health
Dent 1990; 50: 262–267.
20. Yamamoto T. Arrangement of complete denture
molar part artificial tooth – anterior cross-bite in
particular. Pract Prosthodont 1972; 5: 395–400 (in
Japanese).
21. Yano M, Ando Y, Kobayashi H et al. Epidemio-
logical survey on adult dental health (2) Masticatory
ability. J Niigata Dent Soc 1989; 19: 25–38.
22. Sato Y, Ishida E, Minagi S et al. The aspect of
dietary intake of full denture wearer. J Jpn Prosthodont
Soc 1988; 32: 774–779.
23. Kanmori H, Yoshihara A, Ando Y et al. The effect
of chewing ability on the dietary intake of healthy
elderly people. J Dent Hlth 2003; 53: 13–22.
24. Lawton MP. Assessing the competence of older
people. In: Kent DP, Kastenbaum R, Sherwood S eds.
Research Planning and Action for the Elderly: The Power
and Potential of Social Science. New York: Human Sci-
ence Press, 1972: 122–143.
25. Shimazaki Y, Soh I, Saito T et al. Influence of
dentition status on physical disability, mental
impairment, and mortality in institutionalized elderly
people. J Dent Res 2001; 80: 340–345.
26. Miura H, Yamasaki K, Kariyasu M et al. Rela-
tionship between cognitive function and mastication
in elderly females. J Oral Rehabil 2003; 30: 808–811.
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154
Chewing and high-level ADL in the elderly 153

27. Nordenram G, Ljunggren G. Oral status, cognitive
and functional capacity versus oral treatment need in
nursing home residents: a comparison between
assessments by dental and ward staff. Oral Dis 2002; 8:
296–302.
28. Locker D, Matear D, Stephens M et al. Oral
health-related quality of life of a population of med-
ically compromised elderly people. Community Dent
Health 2002; 19: 90–97.
29. Chen CC, Chang CK, Chyun DA et al. Dynamics of
nutritional health in a community sample of Ameri-
can elders: a multidimensional approach using roy
adaptation model. ANS Adv Nurs Sci 2005; 28: 376–
389.
30. Allen PF. Association between diet, social resources
and oral health related quality of life in edentulous
patients. J Oral Rehabil 2005; 32: 623–628.
31. Singh RB, Beegom R, Mehta AS et al. Social class,
coronary risk factors and undernutrition, a double
burden of diseases, in women during transition, in
five Indian cities. Int J Cardiol 1999; 69: 139–147.
32. Akifusa S, Soh I, Ansai T et al. Relationship of
number of remaining teeth to health-related quality
of life in community-dwelling elderly. Gerodontology
2005; 22: 91–97.
Correspondence to:
Yutaka Takata, Division of General Internal Medi-
cine, Kyushu Dental College, Manazuru 2-6-1,
Kokurakita-ku, Kitakyushu City 803-8580, Japan.
Tel.: +81 93 582 1131 (ext. 2011)
Fax: +81 93 582 0592
E-mail: [email protected]
� 2008 The Gerodontology Association and Blackwell Munksgaard Ltd, Gerodontology 2008; 25: 147–154
154 Y. Takata et al.