relation between gastric cancer and previous peptic ulcer disease
TRANSCRIPT

Gut 1997; 40: 247-252
Relation between gastric cancer and previouspeptic ulcer disease
RM Molloy, A Sonnenberg
AbstractBackground-It is presently not weliunderstood to what extent peptic ulcer andgastric cancer represent related diseases.Aims-The objective of this study was toassess past occurrence of gastric andduodenal ulcers in patients with cancer ofthe gastric cardia or other parts of thestomach.Methods-The association between pepticulcer and gastric cancer was studiedamong patients foliowed up at hospitals ofthe US Department of Veterans Affairs.Two populations of 1069 subjects withcancer ofthe cardia and 3078 subjects withcancer of other parts of the stomach werecompared with a control population of89082 subjects without gastric cancer. Inmultivariate logistic regressions, presenceor absence of cancer served as the out-come variable, while age, sex, race, pre-vious histories of gastric ulcer, duodenalulcer, peptic ulcer site unspecified, gastricresection, or vagotomy served as modifiervariables.Results-Old age, non-white ethnicity,and male sex proved strong and indepen-dent risk factors for non-cardiac gastriccancer. A previous history of gastric, butnot duodenal ulcer was associated with asignificantly raised odd ratio of 1-53 (95%confidence interval: 1-24 to 1-87). Cancerof the cardia affected predominantlywhites, and was relatively more commonin men than non-cardiac gastric cancer.Past gastric ulcers exerted no significantinfluence (1.02, 0-67 to 1-56), while duo-denal ulcers and peptic ulcer site un-specified were protective (duodenal ulcer:0-68, 0*47 to 0 95; peptic ulcer disease:0-66, 0-47 to 1.00). Partial gastrectomy wasa risk factor for non-cardiac gastriccancer (1.86, 132 to 2.63), but not forcancer ofthe cardia (1-09, 0 54 to 2.20).Conclusion-These epidemiological pat-terns might stem from underlying differ-ences in the influences of gastritis and acidsecretion on the development of the twocancer types.(Gut 1997; 40: 247-252)
Keywords: adenocarcinoma of the oesophagus,Barrett's oesophagus, duodenal ulcer, epidemiology ofpeptic ulcer, gastritis, gastric cancer, gastric ulcer,Helicobacter pyloni.
It is presently not fully understood to whatextent peptic ulcer and gastric cancer representrelated diseases.'1 Epidemiological studiesseem to suggest that while a past history of
duodenal ulcer protects against the futuredevelopment of gastric cancer, a past history ofgastric ulcer may make a subject more suscep-tible to subsequent development of gastriccancer.' Observational studies suffer fromthree common limitations.7-9 (1) Since gastriccancer has become a relatively rare disease, itis difficult to accumulate large enough numberof patients that would assure a statisticallypowerful and unequivocal result. (2) Aprospective follow up of patients with gastriculcer and controls poses tremendous logisticproblems, and in most studies the length ofobservation has been rather short. On the otherhand, spread or regression of gastritis and thedevelopment of metaplasia are disease pro-cesses that evolve slowly over prolonged timeperiods. (3) Secondary to the short observationperiods, it was difficult to discern true gastriculcers from ulcerated cancers whose benignitywas misdiagnosed initially.The issue of relatedness between peptic
ulcer and gastric cancer remains important,particularly after the discovery of Helicobacterpylori and the realisation that this bacteriumplays an important part in the development ofduodenal ulcer, gastric ulcer, as well as gastriccancer. The relation between a past history ofpeptic ulcer and gastric cancer would shed lighton the mode of action exerted by H pylori onthe gastroduodenal mucosa. A history ofgastric ulcer resulting in an increased risk forgastric cancer would suggest that both diseasesshare a partly similar pathophysiology. Differ-ences between risk factors for cancer in thecardia and other parts of the stomach wouldpoint at different mechanisms operating in thedevelopment of these two types of gastriccancer. Thus, the aim of this case control studywas to compare the past occurrence of gastricand duodenal ulcer between case subjects withand control subjects without gastric cancer.Gastric cancer was divided into cancer of thecardia and other parts of the stomach. Aspartial gastrectomy represents a risk factor forthe development of cancer in the gastricremnant, the number of gastric surgeries in thecase and control populations were taken intoaccount. The comparison of cancer cases andcontrol subjects was carried out in the largecomputerised database of all hospitalised USmilitary veterans that is maintained by theDepartment of Veterans Affairs (VA).
Methods
Data sourceThe patient treatment file comprises a multi-tude of individual computerised data files. The
Division ofGastroenterology,The Medical College ofWisconsin, Milwaukee,Wisconsin, USARM Molloy
Department ofVeterans AffairsMedical Center,Albuquerque,New Mexico, USAA SonnenbergCorrespondence to:Dr A Sonnenberg,Gastroenterology Section,Department of VeteransAffairs Medical Center11 1-F, 2100 RidgecrestDrive SE, Albuquerque, NewMexico 87108, USA.Accepted for publication28 August 1996
247

Modloy, Sonnenberg
data files are managed by the Department ofVeterans Affairs (VA) central AutomationCenter at Austin, Texas. Permits to use thedata and the computational facilities at Austinare granted to interested investigators by theAutomation Center. All files containing medi-cal information are available as SAS data files.The main files contain records of all inpatienttreatments from all VA hospitals distributedthroughout the United States. These files werestarted in 1970 and are available for each fiscalyear since then. From 1970 until 1980, the 8threvision of the International Classification ofDiseases (ICD-8) was used to code the medicalinformation.'" Since 1981, the 9th revision ofthe International Classification of Diseases(ICD-9) and its Clinical Modification havebeen used." In addition to five digit codes foreach disease, the ICD contains codes forindividual surgical and non-surgical pro-cedures. Prior to 1984, surgical procedureswere contained in the main files, since 1984 allprocedures performed in the operating roomare contained in separate procedural files.
Individual subjects can be identified in thedatabase by their unique social securitynumber. The main files contain the patients'demographic characteristics, such as age, race,sex, and place of residence. Besides the pri-mary, the main files from 1970 until 1983provided for the possibility to record fouradditional secondary diagnoses. Since 1984number of potential secondary diagnoses hasbeen raised to nine. Until 1983 five surgicalprocedures could be coded for each hospitalstay, since then the number has been raised tofive for each hospital day.
Extraction of case and control subjectsVeterans who were first diagnosed with gastriccancer (ICD-9-codes: 151-0-151-9) from 1990until 1994, inclusive, were extracted from thepatient treatment file, individual veterans beingidentified by their unique social securitynumber. In the subsequent analyses, patientswith ICD-9-code 151 -0 (cancer of the cardia)were kept separately from patients with ICD-9-codes 151a1-151 9 (cancer of other parts ofthe stomach). From each annual file of thepatient treatment file, each 30th patient wasselected as a control subject. Patients with anyprevious discharge diagnosis of gastric cancerbetween 1970 and 1993 were excluded from thecontrol group. Each case and control subjectwas followed up backward through the annualpatient treatment files of previous years toaccumulate all previous discharge diagnosesbetween 1970 until the diagnosis of gastriccancer. In the control subjects the date ofrecruitment served as the cut off date. Patientrecords were flagged if they carried the follow-ing primary or secondary diagnosis: gastriculcer (ICD-9: 531 00-531-92 and ICD-8:531-0-531-9), duodenal ulcer (ICD-9: 532-00-532-92 and ICD-8: 532-0-532-9), and pepticulcer site unspecified (ICD-9: 533-00-533-92and ICD-8: 533)-0533-9). The following diag-nostic codes were used as indicators for apast history of gastric surgery: gastrojejunal
ulcer (ICD-9: 534-00-534-92 and ICD-8:534-0-534 9) and postgastric surgery syn-dromes (ICD-9: 564-2 and ICD-8: 997-9). Theprocedural codes were searched for theoccurrence of gastric resection: Billroth Igastrectomy (ICD-9: 43-6 and ICD-8: 46 2),Billroth II gastrectomy (ICD-9: 43-7 and ICD-8: 46 2), and other partial gastrectomy orgastroenterostomy (ICD-9: 43-81, 43-89 or44-39 and ICD-8: 46 5). Various types surgeryinvolving vagotomy were identified by thefollowing codes: vagotomy not otherwisespecified (ICD-9: 44 00 and ICD-8: 46 8),truncal vagotomy (ICD-9: 44-01), highlyselective vagotomy (ICD-9: 44 02), otherselective vagotomy (ICD-9: 44 03). Vagotomiesare frequently performed with concomitantantrectomy or pyloroplasty (ICD-9: 44-2,44-21, 44-29 and ICD-8: 46- 1).For each of the diagnostic codes mentioned
above, its date of first and last appearance inan individual patient was recorded. Each pro-cedural code was extracted with the corres-ponding date of surgery. Unless stated other-wise, all gastric ulcers that were diagnosed forthe first time one year or less prior to the firstdiagnosis of gastric cancer (or date of recruit-ment in the controls) were excluded from theanalysis. Similarly, all gastric surgery per-formed one year prior to cancer diagnosis orrecruitment was ignored. The length of timebetween the first diagnosis of gastric cancerand the first or last mention of peptic ulcer wascalculated. We also calculated the length oftime between the first diagnosis of gastriccancer and the date of gastric surgery.
Statistical analysisQuantitative parameters, such as age andlengths of time, were expressed as mean valueswith their standard errors. For univariate com-parisons of quantitative parameters betweencases and controls, the t test was used. Forunivariate comparisons of qualitative para-meters, such as sex and race, the x2 test wasused. In the multivariate analysis, case andcontrol subjects were compared by multi-variate logistic regression using theLOGISTIC procedure of SAS.'2 Presence orabsence of gastric cancer served as the outcomevariable. Age, sex, race, and a previous historyof gastric ulcer, duodenal ulcer, peptic ulcersite unspecified, gastric resection, or vagotomyserved as modifier variables. The length of timebetween the last occurrence of various ulcertypes and ulcer surgery were also considered inthe model. The results of the analyses wereexpressed as odds ratios and their 95 per centconfidence intervals. An odds ratio was con-sidered significant if its 95% confidenceinterval did not include unity.
ResultsOf all patients discharged from VA hospitalsbetween 1990 and 1994, 4147 patients werediagnosed for first time to have gastric cancer.A population of 89082 patients dischargedduring the same period as the cancer cases
248
Gastric cancer and peptic ulcer
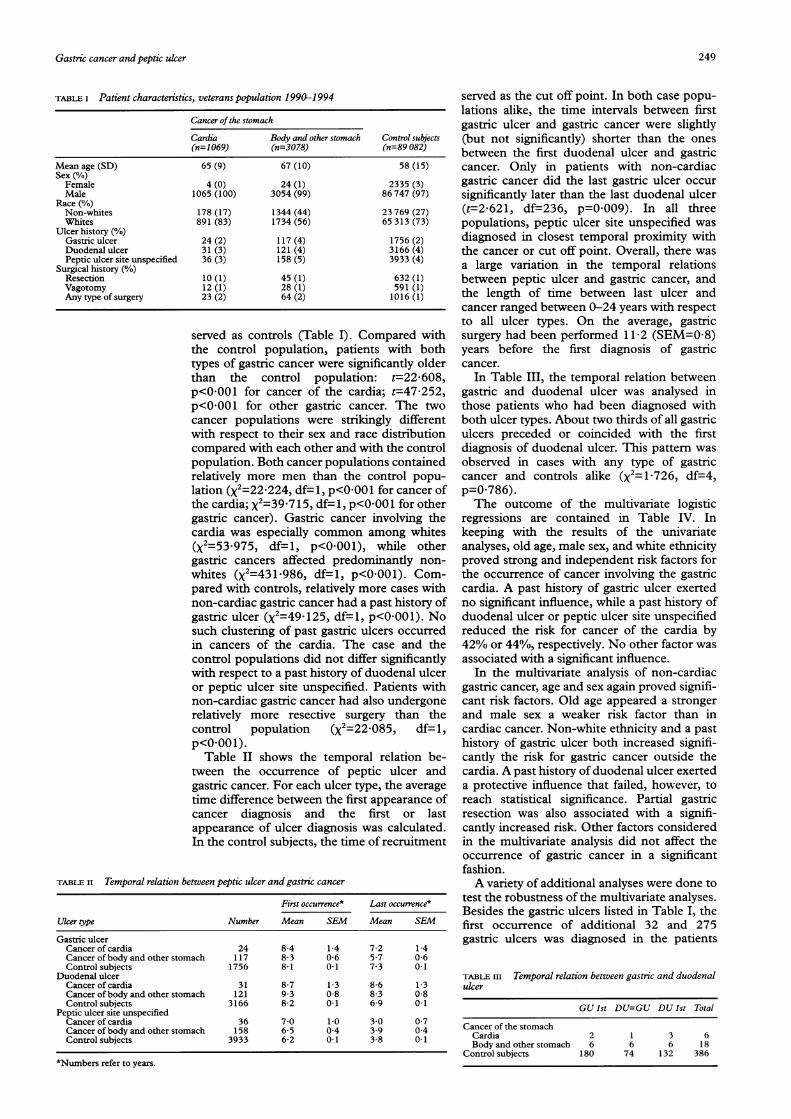
TABLE I Patient characteristics, veterans population 1990-1994
Cancer of the stomach
Cardia Body and other stomach Control subjects(n=1069) (n=3078) (n=89 082)
Mean age (SD) 65 (9) 67 (10) 58 (15)Sex (%/o)Female 4 (0) 24 (1) 2335 (3)Male 1065 (100) 3054 (99) 86 747 (97)
Race (%)Non-whites 178 (17) 1344 (44) 23 769 (27)Whites 891 (83) 1734 (56) 65 313 (73)
Ulcer history (%)Gastric ulcer 24 (2) 117 (4) 1756 (2)Duodenal ulcer 31 (3) 121 (4) 3166 (4)Peptic ulcer site unspecified 36 (3) 158 (5) 3933 (4)
Surgical history (%)Resection 10 (1) 45 (1) 632 (1)Vagotomy 12 (1) 28 (1) 591 (1)Any type of surgery 23 (2) 64 (2) 1016 (1)
served as controls (Table I). Compared withthe control population, patients with bothtypes of gastric cancer were significantly olderthan the control population: t=22-608,p<OOOl for cancer of the cardia; t=47-252,p<0001 for other gastric cancer. The twocancer populations were strikingly differentwith respect to their sex and race distributioncompared with each other and with the controlpopulation. Both cancer populations containedrelatively more men than the control popu-lation (X2=22 224, df=1, p<0001 for cancer ofthe cardia; X2=39 715, df=1, p<0-001 for othergastric cancer). Gastric cancer involving thecardia was especially common among whites(x2=53 975, df=l, p<0-001), while othergastric cancers affected predominantly non-whites (X2=43l1986, df=l, p<0001). Com-pared with controls, relatively more cases withnon-cardiac gastric cancer had a past history ofgastric ulcer (x2=49 125, df=l, p<0-001). Nosuch clustering of past gastric ulcers occurredin cancers of the cardia. The case and thecontrol populations did not differ significantlywith respect to a past history of duodenal ulceror peptic ulcer site unspecified. Patients withnon-cardiac gastric cancer had also undergonerelatively more resective surgery than thecontrol population (X2=22-O85, df= 1,p<OOOl).Table II shows the temporal relation be-
tween the occurrence of peptic ulcer andgastric cancer. For each ulcer type, the averagetime difference between the first appearance ofcancer diagnosis and the first or lastappearance of ulcer diagnosis was calculated.In the control subjects, the time of recruitment
TABLE II Temporal relation between peptic ulcer and gastric cancer
First occurrence* Last occurrence*
Uker type Number Mean SEM Mean SEM
Gastric ulcerCancer of cardia 24 8-4 1-4 7-2 1-4Cancer ofbody and other stomach 117 83 06 57 0-6Control subjects 1756 8-1 0 1 7-3 0 1
Duodenal ulcerCancerofcardia 31 8-7 1-3 8-6 1-3Cancer ofbody and other stomach 121 9 3 0-8 8-3 0-8Control subjects 3166 8-2 0 1 6-9 0 1
Peptic ulcer site unspecifiedCancer of cardia 36 7-0 1 0 3 0 0 7Cancer ofbody and other stomach 158 6-5 0-4 3 9 0-4Control subjects 3933 6-2 0 1 3-8 0 1
*Numbers refer to years.
served as the cut off point. In both case popu-lations alike, the time intervals between firstgastric ulcer and gastric cancer were slightly(but not significantly) shorter than the onesbetween the first duodenal ulcer and gastriccancer. Only in patients with non-cardiacgastric cancer did the last gastric ulcer occursignificantly later than the last duodenal ulcer(t=2-621, df=236, p=0009). In all threepopulations, peptic ulcer site unspecified wasdiagnosed in closest temporal proximity withthe cancer or cut off point. Overall, there wasa large variation in the temporal relationsbetween peptic ulcer and gastric cancer, andthe length of time between last ulcer andcancer ranged between 0-24 years with respectto all ulcer types. On the average, gastricsurgery had been performed 11 2 (SEM=0-8)years before the first diagnosis of gastriccancer.
In Table III, the temporal relation betweengastric and duodenal ulcer was analysed inthose patients who had been diagnosed withboth ulcer types. About two thirds of all gastriculcers preceded or coincided with the firstdiagnosis of duodenal ulcer. This pattern wasobserved in cases with any type of gastriccancer and controls alike (x2=11726, df=4,p=0786).The outcome of the multivariate logistic
regressions are contained in Table IV. Inkeeping with the results of the univariateanalyses, old age, male sex, and white ethnicityproved strong and independent risk factors forthe occurrence of cancer involving the gastriccardia. A past history of gastric ulcer exertedno significant influence, while a past history ofduodenal ulcer or peptic ulcer site unspecifiedreduced the risk for cancer of the cardia by42% or 44%, respectively. No other factor wasassociated with a significant influence.
In the multivariate analysis of non-cardiacgastric cancer, age and sex again proved signifi-cant risk factors. Old age appeared a strongerand male sex a weaker risk factor than incardiac cancer. Non-white ethnicity and a pasthistory of gastric ulcer both increased signifi-cantly the risk for gastric cancer outside thecardia. A past history of duodenal ulcer exerteda protective influence that failed, however, toreach statistical significance. Partial gastricresection was also associated with a signifi-cantly increased risk. Other factors consideredin the multivariate analysis did not affect theoccurrence of gastric cancer in a significantfashion.A variety of additional analyses were done to
test the robustness of the multivariate analyses.Besides the gastric ulcers listed in Table I, thefirst occurrence of additional 32 and 275gastric ulcers was diagnosed in the patients
TABLE III Temporal relation between gastnc and duodenalulcer
GU Ist DU=GU DU Ist Total
Cancer of the stomachCardia 2 1 3 6Body and other stomach 6 6 6 18
Control subjects 180 74 132 386
249

Molloy, Sonnenberg
TABLE iv Risk factors for gastric cancer
95% ConfidenceVanrable Odds ratio intervals Wald (x2) p Value
Cancer of the cardia (ICD-Code 151 0)Age* 1-38 1-32to 1 45 184-3816 0 0001Male sex 6 51 2-44 to 17-41 13-9534 0-0002White etmicity 1-60 1-36 to 1-89 32-3799 0 0001Gastric ulcer 1-02 0-67 to 1-56 0-0088 0-9254Duodenal ulcer 0-68 0-47 to 1-00 3 9017 0-0482Peptic ulcer site unspecified 0-66 0-47 to 0-94 5 3967 0-0202Gastric resection 1-09 0 54 to 2-20 0 0536 0 8170Vagotomy 1-89 0-97 to 3-69 3-4555 0-0630Cancer of the stomach (ICD-Codes 151 1-151 9)Age* 1-69 1-64to 1-74 1222-7250 0 0001Male sex 2-58 1-72 to 3-87 20-8977 0 0001White etnicity 0 39 0-36 to 0-42 632-8373 0 0001Gastric ulcer 1-53 1-24 to 1-87 16 2356 0 0001Duodenal ulcer 0-89 0 73 to 1-08 1-3687 0-2420Peptic ulcer site unspecified 0 94 0-79 to 1-12 0-5128 0-4739Gastric resection 1-86 1-32 to 2-63 12 5484 0 0004Vagotomy 0 80 0-52 to 1-24 0-9720 0-3242
*Increase in risk ratio per 10 years.
with cardiac and non-cardiac gastric cancer,respectively, during the year preceding the firstdiagnosis of gastric cancer. The correspondingnumber of first diagnosed gastric ulcers in thecontrol population was 733. If these ulcerswere included in the regression analysis ofnon-cardiac gastric cancer, the odds ratio associatedwith gastric ulcer rose to 2-97 (95% confidenceinterval: 2-58 to 3 40). On the other hand,extending the exclusion period for gastriculcers preceding non-cardiac cancer from oneyear up to five years left the outcomes of themultivariate analysis largely unchanged. Theodds ratio of gastric ulcer with three yearexclusion period was 1-48 (1-17 to 1P86) andwith five year exclusion 1-50 (1P15 to 1-94).Gastric surgery represents a known risk factorfor the development of gastric cancer. Themultivariate analysis adjusts for the contri-bution of individual factors. Nevertheless, torule out completely any possible interactionbeween peptic ulcer and subsequent ulcersurgery, the regression analysis was repeatedwith only those ulcers that had not been treatedsubsequently by gastric surgery. In case ofnon-cardiac gastric cancer, this measure failed toalter the odds ratio associated with gastric ulcer(OR=1-50, 1-15 to 1-94) or duodenal ulcer(OR=0-90, 0 74 to 1.09) in any substantiveway. In cardiac cancer, the odds ratios changedto (OR=0-98, 0.61 to 1-58) for gastric ulcerand (OR=0-72, 0-48 to 1P07) for duodenalulcer.
DiscussionThis study showed an increased risk for non-cardiac cancer associated with rising age, non-white ethnicity, and male sex. These findingsare in agreement with previously reported epi-demiological patterns of gastric cancer in theUnited States.'3 Moreover, the study showedthat a past history of gastric, but not duodenalulcer was associated with an increased risk forgastric cancer outside the cardia. Our resultsleave little doubt that gastric ulcer was trulyassociated with an increased risk for gastriccancer, because even after the exclusion of allgastric ulcers up to five years prior to the firstcancer diagnosis the odds ratio remainedsignificantly increased. Although the majority
of gastric ulcers first diagnosed in closetemporal proximity to the subsequent diag-nosis of gastric cancer may be suspicious formisdiagnosed malignant ulcers, this explan-ation becomes less probable the further back intime one moves from the initial diagnosis ofgastric cancer. Gastric resection resulted in anincreased risk for non-cardiac gastric cancer.This finding is consistent with many previousreports that have shown an increased risk forgastric stump cancer after gastric resection, therisk rising with the length of the time sincesurgery.'1'6 In striking contrast with cancerinvolving the body and the antrum of thestomach, cancer of the cardia affected pre-dominately whites. Cancer of the cardia wasalso relatively more common in men than theother types of gastric cancer. A history ofgastric ulcer exerted no significant influenceand duodenal ulcer or peptic ulcer site un-specified were both protective. Gastric surgeryexerted no significant influence on itsoccurrence.
Part of the epidemiological correlation be-tween gastric and duodenal ulcer relates to anunderlying infectious gastritis in bothdiseases.'7 Over time, the gastritis may spreadfrom the antrum to the rest of the stomach. Asthe area ofthe acid secreting mucosa decreases,the duodenal ulcer tends to burn out and thepatient becomes more susceptible to gastriculceration.'8 Further progression of the gas-tritis and development of extensive intestinalmetaplasia may then lead to gastric cancer.However, this hypothetical sequence is some-what at odds with the results of this study, aswell as those of previous studies. Firstly, allpublished series of peptic ulcer contained afraction of patients who presented with bothulcer types at the same time or even with aduodenal ulcer diagnosed subsequently to agastric ulcer.7 19-20 Secondly, although the lastgastric and duodenal ulcers occurred onaverage 5-7 and 8-3 years, respectively, beforethe diagnosis of non-cardiac gastric cancer, thetime difference between the two diagnosesranged anywhere between 0 and 24 years.Large series of patients have been accumu-lated, in whom gastric and duodenal ulcers orat least scars thereofwere found concomitantlywith the cancer.2' 22 These findings wouldsuggest that the hypothesis regarding thetemporal sequence of the three diseases is toosimplistic or that it applies only to a fraction ofthe patient population.
Gastric cancer of the body and the antrumon one hand and gastric cancer of the cardiaon the other hand seem to constitute twodifferent disease entities. Cancer of the cardiais frequently associated with Barrett's epi-thelium, which represents a severe form gastro-oesophageal reflux disease. Reflux diseasecharacterised by ulcerations, strictures, orBarrett's epithelium is more common amongmen than women and whites than non-whites.23 In the present analysis, a similar dis-tribution by sex and ethnicity was also revealedby cancer of the cardia. Gastro-oesophagealreflux disease results from the corrosive actionof the acidic refluate on the oesophageal
250
Gastric cancer and peptic ulcer
mucosa. Long term infection with H pylonileads to multifocal atrophic gastritis and loss ofgastric acidity, which could protect the patientagainst reflux disease and possibly also againstadenocarcinoma originating from Barrett'sepithelium. Such mechanisms could underliethe missing influence of gastric ulcer or eventhe protective influence of duodenal ulcer andpeptic ulcer site unspecified on cardiac cancer.On the other hand, the multifocal atrophicgastritis related to H pyloni predisposes thepatient to gastric ulcer, as well as gastric cancerin the body or antrum.2"25 No such clear cutrelation exists between this type of gastritis andduodenal ulcer.26
Cancers of the cardia and other parts of thestomach show opposing time trends. While theincidence rates of cancer in the gastric body orantrum have notably decreased, those ofcardiac cancer have increased during the sameperiod.13 17 27-31 In the United States, the mostpronounced rise and fall of cardiac and non-cardiac cancers, respectively, affected whitemen; the rise and fall were less noticeableamong non-whites.32 Again, these time trendsare consistent with the contention that in-fection with H pyloni determines the epidemio-logical pattern of both types of gastric cancer.The recent improvements in hygiene andsocioeconomic status decreased the infectionrates ofH pyloni in the general population. Asthe improvements benefited whites more thannon-whites, gastric cancer rates have decreasedprimarily in whites. During the same time, thepopulation wide decrease in H pylon inducedatrophic gastritis and its associated hypoch-lorhydria increased the general susceptibilityfor reflux disease, Barrett's oesophagus, andadenocarcinoma of the cardia. Other factors,such as changes in dietary habits, may havealso contributed to these temporal changes.33
In relying on the patient treatment file forconducting the present research project, it isimportant to consider several shortcomings ofthis large database. Like all large databases, thepatient treatment file is limited in capturing allpertinent health care activity in individualpatients. For instance, no records exist torecord diagnoses made outside of the VeteransAffairs system, and our analysis may under-estimate the true frequency of previous pepticulcers. Oesophagogastroduodenoscopy andupper gastrointestinal x rays are frequentlyperformed as outpatient procedures. Our in-ability to record outpatient activity could haveintroduced a systematic error to both groups ofcase and control subjects. As individualveterans received part of their medical care asoutpatients or outside VA facilities altogether,the time sequence of diagnoses, as they appearin the computerised database, may not neces-sarily reflect their true temporal relation. Onthe other hand, the different influences ofgastric and duodenal ulcer on various types ofgastric cancer rules out a simple selection ordetection bias as an explanation for theobserved findings.
Lastly, our database deals exclusively withUS military veterans. This population consistsprimarily of male subjects with low family
income and increased exposure to environ-mental risk factors, for instance, H pyloninfection or smoking. Their health behaviourand medical care are different from those ofother Americans. In general, their healthawareness and concern about prevention maybe less developed than in the whole US popu-lation. On the other hand, very similar oddsratios were reported in a recent study fromSweden.34 A history of duodenal ulcer reducedthe cancer risk by 40%, while that of gastriculcer increased the cancer risk twofold. Incontradistinction with the case control designof the present study, Hansson and coworkersfollowed a cohort of ulcer patients over a timeperiod of 9 1 years. The minor differencesbetween the results of the study by Hanssonand ours could be explained by the fact that hedid not consider a breakdown of cancers bydifferent gastric sites. The similar findingsobserved by two independent groups suggestthat the relation between peptic ulcer andgastric cancer apply to different populationsalike and that these associations would beshown also by future studies, irrespective of theparticular study design chosen by theinvestigators.
In summary, the results of this study clearlyshow cancers involving the gastric cardia orother parts of the stomach to represent twoopposites of a spectrum of gastric cancer.Cardiac cancer affects mostly white men. Aprevious ulcer history does not influence itsoccurrence, if anything, it might protectagainst its development. On the other hand,cancer in other parts of the stomach affectsmostly non-whites, male predominance is lessstriking than in cardiac cancer, and a pasthistory of gastric ulcer confers an increasedrisk. These patterns might stem from under-lying differences in the influences of gastritisand acid secretion on the development of thetwo cancer types.
1 Graham DY. Helicobacterpylori: Its epidemiology and its rolein duodenal ulcer disease. J Gastroenterol Hepatol 199 1; 6:105-13.
2 Graham DY. Helicobacter pylori: epidemiology, relationshipto gastric cancer and the role of infants in transmission.EurJ7 Gastroenterol Hepatol 1992; 4 (suppl 1): S 1-6.
3 Hu PJ, Li YY, Zhou MH, Chen MH, Du GG, Huang BJ,et al. Helicobacter pylori associated with a high prevalenceof duodenal ulcer disease and a low prevalence of gastriccancer in a developing nation. Gut 1993; 36: 198-202.
4 Sonnenberg A. Concordant occurrence of gastric andhypertensive diseases. Gastroenterology 1988; 95: 42-8.
5 Wanebo HJ, KennedyBJ, ChmielJ, Steele GJr, WmchesterD,Osteen R. Cancer of the stomach. A patient care studyby the American College of Surgeons. Ann Surg 1993;218: 583-92.
6 Graham DY, Go MF, Genta RM. Helicobacter pylori, duo-denal ulcer, gastric cancer: tunnel vision or blinders. AnnMed 1995; 27: 331-6.
7 Mowat NAG, Needham CD, Brunt PW. The naturalhistory of gastric ulcer in a community: a four-year study.QjMed 1975; 44: 45-56.
8 Maaroos HI, Salupere V, Uibo R. Gastric cancer, gastritisand gastric carcinoma. Ann Clin Res 1981; 13: 151-3.
9 Rollag A, Jacobsen CD. Gastric ulcer risk of cancer. A five-year follow-up study. Acta Med Scand 1984; 216: 105-9.
10 World Health Organization. Eighth revision internationalclassification of diseases, adaptedfor use in the United States.PHS publication no 1693. Washington, DC: Departmentof Health, Education and Welfare and Public HealthService, US Government Printing Office, 1970.
11 World Health Organization. The international classification ofdiseases, 9th revision. Clinical modification. 3rd ed. DHHSpublication no (PHS) 89-1260. Washington, DC: PublicHealth Service, US Government Printing Office, March1989.
12 SAS Institute Inc. SAS/STAT user's guide, version 6, 4thed, vol 2, chapter 27. The logistic procedure. Cary, NC: SASInstitute Inc, 1989: 1071-126.
251

Molloy, Sonnenberg
13 Sandler RS. Gastric cancer. In: JE Everhart, ed. Digestivediseases in the United States: epidemwlogy and impact. USDepartnent of Health and Human Services. Washington,DC: US Government Printing Office 1994; NIH publi-cation no 94-1447: 181-204.
14 Stalsberg H, Taksdal S. Stomach cancer following previousgastric surgery for benign conditions. Lancet 1971; ii:1175-7.
15 Tersmette AC, Goodman SN, Offerhaus GJ, Tersmette KW,Giardiello FM, Vandenbroucke JP, et al. Multivariateanalysis of the risk of stomach cancer after ulcer surgeryin an Amsterdam cohort of postgastectomy patients. AmJEpidemiol 1991; 134: 14-21.
16 Lundegardh G, Adami HO, Helmick C, Zack M, Meirik 0.Stomach cancer after partial gastrectomy for benign ulcerdisease. NEnglJMed 1988; 319: 195-200.
17 Sonnenberg A. The US temporal and geographic variationsof diseases related to Helicobacterpylori. AmJPuAblic Health1993; 83: 1006-10.
18 FryJ. Peptic ulcer: a profile. BMJ 1964; 2: 809-12.19 Krause U. Long term results of medical and surgical treat-
ment of peptic ulcer. A follow-up investigation of patientsinitially treated conservatively between 1925-34. ActaChir Scand 1963; suppl 310: 1-111.
20 Ihre BJE, Barr H, Havermark G. Ulcer-cancer of thestomach. A follow-up study of 473 cases of gastric ulcer.Gastroenterologia 1964; 102: 78-91.
21 Lewis JH, Woods M m. Gastric carcinoma in patients withunoperated duodenal ulcer disease. Am Jf Gastroenterol1982; 77: 368-73.
22 Hole DJ, Quigley EMM, Gillis CR, Watkinson G. Pepticulcer and cancer: an examination of the relationshipbetween chronic peptic ulcer and gastric carcinoma.ScandJ Gastroenterol 1987; 22: 17-23.
23 Sonnenberg A. Esophageal diseases. In: JE Everhart, ed.Digestive diseases in the United States: epidemiology andimpact. US Department of Health and Human Services.
Washington, DC: US Government Printing Office 1994;NIH publication no 94-1447: 299-356.
24 Kekki M, Sipponen P, Siurala M, Laszewicz W. Peptic ulcerand chronic gastritis: their relation to age and sex, and tolocation ofulcer and gastritis. Gastroenterol Clin Biol 1990;14: 217-23.
25 Lechago J, Correa P. Prolonged achlorhydria and gastricneoplasia: is there a causal relationship? Gastroenterology1993; 104:1551-7.
26 Sipponen P. Long-term consequences of gatroduodenalinflammation. EurJ Gastroenterol Hepatol 1992; 4 (suppl2): S25-9.
27 Howson CP, Hiyama Y, Wynder EL. The decline in gastriccancer: epidemiology of an unplanned triumph. EpidemiolRev 1986; 8: 1-27.
28 Hesketh PJ, Clapp RW, Doos WG, Spechler SJ. Theincreasing frequency of adenocarcinoma of theesophagus. Cancer 1989; 64: 526-30.
29 Powell J, McConkey CC. Increasing incidence of adeno-carcinoma of the gastric cardia and adjacent sites. Br JCancer 1990; 62: 440-3.
30 Blot J, Devesa SS, Kneller RW, Fraumeni JF. Rising inci-dence of adenocarcinoma of the esophagus and gastriccardia.JAAL4 1991; 265: 1287-9.
31 Locke HI GR, Talley NJ, Carpenter HA, HarmsenWS, Zinsmeister AR, Melton HI y. Changes in thesite- and histology-specific incidence of gastric cancerduring a 50-year period. Gastroenterology 1995; 109:1750-6.
32 Sonnenberg A, El-Serag HB. Epidemiology of gastro-esophageal reflux disease. Dig Surg (in press).
33 Sonnenberg A. Dietary salt and gastric ulcer. Gut 1986; 27:1138-42.
34 Hansson LE, Nyren 0, HsingAW, Bergstrom R, Josefsson S,Chow WH, et al. The risk of stomach cancer in patientswith gastric or duodenal ulcer. N EnglJ Med 1996; 335:242-9.
252