relapsed multiple myeloma in the uk prior to the introduction of novel agents – a response to )
TRANSCRIPT
We read with great interest the recent study by Koleva et al.(2010), in which they documented the healthcare costsassociated with the treatment of multiple myeloma (MM)in Italy. Although the addition of bortezomib and lenalido-mide (newer agents) to MM treatment regimens has greatlyimproved response rates in relapsed and de novo disease(Weber et al. 2007; San Miguel et al. 2008), these drugs areexpensive with significant implications for healthcareresource planning. Thus, in the UK, bortezomib has onlybeen available to NHS MM patients in first relapse sinceOctober 2007, with lenalidomide being available to thosein second relapse since June 2009. Placing the cost oftreatment with newer agents in the context of the cost oftreating MM in the era before their availability is madedifficult by the lack of available data. Therefore, we carriedout a multi-centre, retrospective study to define the treat-ment pathways for MM patients from first relapse (RMM)and to describe the impact on secondary healthcareresource use associated with the treatment of RMM beforethe introduction of newer agents.
This study was conducted between February andDecember 2007 in five hospitals across a wide geographi-cal area in the UK with ethical approval from EasternMREC (ref. 06/MRE05/61). Patients with RMM wereincluded if the first episode of relapse occurred betweenFebruary 2001 and December 2007, providing data justbefore the introduction of the newer agents. Collecteddata included: chemotherapy regimen at each relapse, hos-pital attendance/admissions, blood products transfusedand supportive treatments (e.g. radiotherapy, dialysis).
Seventy-eight patients were included (46 male, 32female) with a median age of 62.8 years (range 43–89years). The most common isotypes were IgG-k (35.5%)
and IgA-k (16.5%). Co-morbidities were present in 87.2%of patients with cardiovascular disease (37%) and diabetes(24%) the most common. At the time of data collection,73 patients were deceased and seven had received treat-ment with newer agents (and were thus excluded fromfurther analysis). Data were available for second and thirdrelapse episodes from 25 and seven patients respe-ctively. The most common initial treatment regimenswere vincristine–doxorubicin–dexamethasone-type, oralkylator-based (25.6% and 26.9% respectively, Table 1).Twenty patients (25.7%) received consolidation withhigh-dose chemotherapy and autologous stem cell trans-plantation (HDT + auto-SCT), including two patients whounderwent HDT + auto-SCT on two occasions. Eightpatients failed to harvest adequate stem cell numbers andtwo further patients underwent allogeneic stem cell trans-plantation. For salvage therapy at first, second and thirdrelapses, a thalidomide-containing regimen was the mostfrequently prescribed regimen (48.7%, 52.0% and 50%respectively).
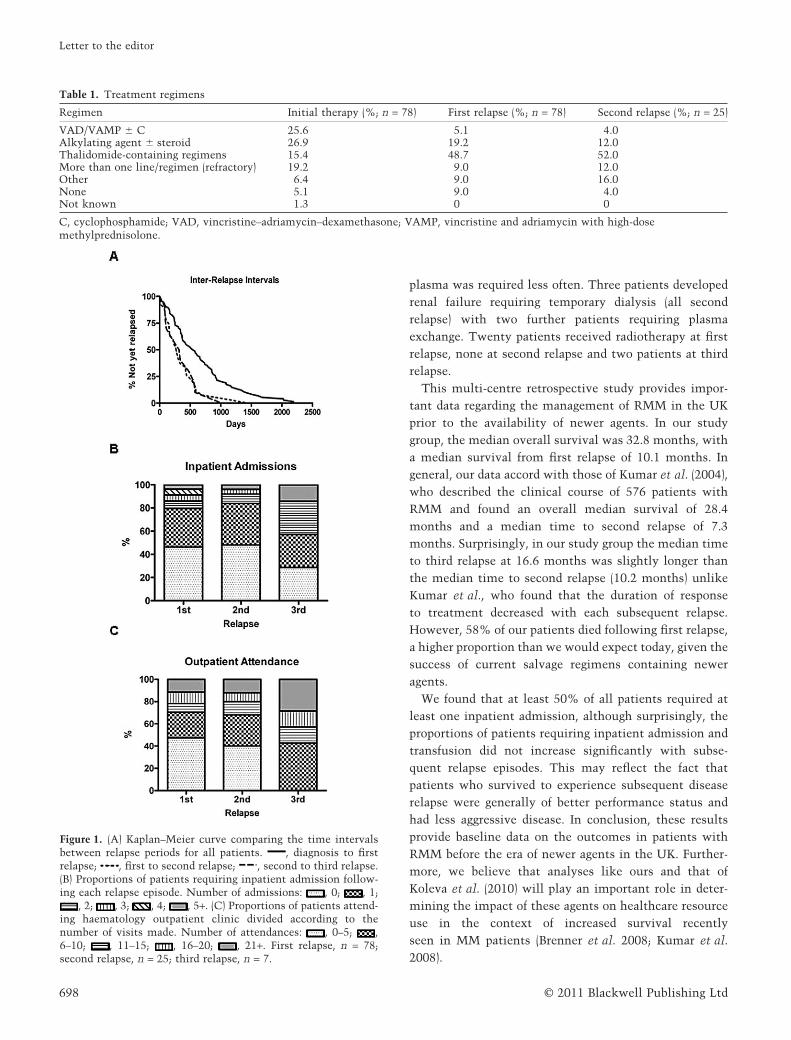
The median time from diagnosis to first relapse was19.2 months (range 65–2191 days), from first to secondrelapse 10.2 months (range 80–1085 days) and from secondto third 16.6 months (84–580 days). Figure 1A shows themedian relapse-free intervals between completion of che-motherapy and diagnosis of a further relapse. The overallmedian survival from diagnosis was 32.8 months (range105–4020 days) and from first relapse was 10.1 months(range 2–1376 days). Following all relapse episodes, at leasthalf of all patients required at least one inpatient admis-sion to hospital (Fig. 1B). Figure 1C summarises outpa-tient attendances following each relapse episode andshows that the proportion of patients making more thanfive clinic visits remained unchanged through first andsecond relapse but did increase following third relapse,52.5%, 51.6% and 100% respectively. The proportion ofpatients receiving red cell transfusions remained consis-tent through first and second relapse (41.2% and 41.3%respectively) but increased to 57.1% following thirdrelapse (Table 2). Transfusion of platelets and fresh frozen
Correspondence address: John Quinn, Clinical Research Fellow, UniversityCollege London Cancer Institute, Department of Haematology, 72 HuntleyStreet, London WC1E 6BT, UK (e-mail: [email protected]).
Accepted 17 October 2010DOI: 10.1111/j.1365-2354.2011.01248.x
European Journal of Cancer Care, 2011, 20, 697–699
Letter to the editor
Relapsed multiple myeloma in the UK prior to theintroduction of novel agents – a response toKoleva et al. (2010)ecc_1248 697..699
© 2011 Blackwell Publishing Ltd
plasma was required less often. Three patients developedrenal failure requiring temporary dialysis (all secondrelapse) with two further patients requiring plasmaexchange. Twenty patients received radiotherapy at firstrelapse, none at second relapse and two patients at thirdrelapse.
This multi-centre retrospective study provides impor-tant data regarding the management of RMM in the UKprior to the availability of newer agents. In our studygroup, the median overall survival was 32.8 months, witha median survival from first relapse of 10.1 months. Ingeneral, our data accord with those of Kumar et al. (2004),who described the clinical course of 576 patients withRMM and found an overall median survival of 28.4months and a median time to second relapse of 7.3months. Surprisingly, in our study group the median timeto third relapse at 16.6 months was slightly longer thanthe median time to second relapse (10.2 months) unlikeKumar et al., who found that the duration of responseto treatment decreased with each subsequent relapse.However, 58% of our patients died following first relapse,a higher proportion than we would expect today, given thesuccess of current salvage regimens containing neweragents.
We found that at least 50% of all patients required atleast one inpatient admission, although surprisingly, theproportions of patients requiring inpatient admission andtransfusion did not increase significantly with subse-quent relapse episodes. This may reflect the fact thatpatients who survived to experience subsequent diseaserelapse were generally of better performance status andhad less aggressive disease. In conclusion, these resultsprovide baseline data on the outcomes in patients withRMM before the era of newer agents in the UK. Further-more, we believe that analyses like ours and that ofKoleva et al. (2010) will play an important role in deter-mining the impact of these agents on healthcare resourceuse in the context of increased survival recentlyseen in MM patients (Brenner et al. 2008; Kumar et al.2008).
Table 1. Treatment regimens
Regimen Initial therapy (%; n = 78) First relapse (%; n = 78) Second relapse (%; n = 25)
VAD/VAMP � C 25.6 5.1 4.0Alkylating agent � steroid 26.9 19.2 12.0Thalidomide-containing regimens 15.4 48.7 52.0More than one line/regimen (refractory) 19.2 9.0 12.0Other 6.4 9.0 16.0None 5.1 9.0 4.0Not known 1.3 0 0
C, cyclophosphamide; VAD, vincristine–adriamycin–dexamethasone; VAMP, vincristine and adriamycin with high-dosemethylprednisolone.
Figure 1. (A) Kaplan–Meier curve comparing the time intervalsbetween relapse periods for all patients. , diagnosis to firstrelapse; , first to second relapse; , second to third relapse.(B) Proportions of patients requiring inpatient admission follow-ing each relapse episode. Number of admissions: , 0; , 1;
, 2; , 3; , 4; , 5+. (C) Proportions of patients attend-ing haematology outpatient clinic divided according to thenumber of visits made. Number of attendances: , 0–5; ,6–10; , 11–15; , 16–20; , 21+. First relapse, n = 78;second relapse, n = 25; third relapse, n = 7.
Letter to the editor
© 2011 Blackwell Publishing Ltd698

ACKNOWLEDGEMENTS
Funding: Janssen-Cilag Ltd, and statistical analysis: pHAssociates.
JOHN QUINNCRUK Clinical Research Fellow,
Department of Haematology,University College London Cancer Institute,
London, UK
FRAN PERCIVALScientific Consultant,
pH Associates,Marlow, UK
MARTIN AUGERConsultant,
Department of Haematology,Norfolk and Norwich University Hospital,
Norwich, UK
SUPRATIK BASUConsultant,
Department of Haematology,New Cross Hospital,Wolverhampton, UK
PATRICK CHUConsultant
Department of Haematology,Royal Liverpool and Broadgreen University Hospitals
NHS Trust,Liverpool, UK
MAADH ALDOURIConsultant,
Department of Haematology,Medway NHS Trust,
Gillinghamr, UK
ADRIAN LAMBOURNEStatistician,
pH Associates,Marlow, UK
SABINE GAUGRISSenior Outcomes Research Manager,
Department of Outcomes Research, Jansen-Cilag Ltd,High Wycombe, UK
KWEE YONGReader in Haematology,
Department of Haematology,University College London Cancer Institute,
London, UK
REFERENCES
Brenner H., Gondos A. & Pulte D.(2008) Recent major improvement inlong-term survival of younger patientswith multiple myeloma. Blood 111,2521–2526.
Koleva D., Cortelazzo S., Toldo C. & Garat-tini L. (2010) Healthcare costs ofmyeloma: an Italian study. EuropeanJournal of Cancer Care 20, 330–336.
Kumar S.K., Therneau T.M., Gertz M.A.,Lacy M.Q., Dispenzieri A., RajkumarS.V., Fonseca R., Witzig T.E., Lust J.A.,Larson D.R., Kyle R.A. & Greipp P.R.(2004) Clinical course of patients with
relapsed multiple myeloma. Mayo ClinicProceedings 79, 867–874.
Kumar S.K., Rajkumar S.V., Dispenzieri A.,Lacy M., Hayman S., Buadi F., ZeldenrustS.R., Dingli D., Russell S.J., Lust J.A.,Greipp P.R., Kyle R.A. & Gertz M.A.(2008) Improved survival in multiplemyeloma and the impact of novel thera-pies. Blood 111, 2516–2520.
San Miguel J.F., Schlag R., Khuageva N.K.,Dimopoulos M.A., Shpilberg O., KropffM., Spicka I., Petrucci M.T., PalumboA., Samoilova O.S., Dmoszynska A.,Abdulkadyrov K.M., Schots R., Jiang B.,Mateos M.V., Anderson K.C., EsseltineD.L., Liu K., Cakana A., van de Velde
H., Richardson P.G. & VISTA TrialInvestigators (2008) Bortezomib plusmelphalan and prednisone for initialtreatment of multiple myeloma. TheNew England Journal of Medicine 359,906–917.
Weber D.M., Chen C., Niesvizky R., WangM., Belch A., Stadtmauer E.A., Siegel D.,Borrello I., Rajkumar S.V., Chanan-KhanA.A., Lonial S., Yu Z., Patin J., Olesny-ckyj M., Zeldis J.B., Knight R.D. & Mul-tiple Myeloma (009) Study Investigators(2007) Lenalidomide plus dexamethasonefor relapsed multiple myeloma in NorthAmerica. The New England Journal ofMedicine 357, 2133–2142.
Table 2. Transfusion products given at each relapse
Relapse First Second Third
Blood product
Patients requiringtransfusion(%; n = 78)
No. oftransfusionevents
Patients requiringtransfusion(%; n = 25)
No. oftransfusionevents
Patients requiringtransfusion(%; n = 7)
No. oftransfusionevents
Red cells 41.2 137 48.0 62 57.1 37Platelets 6.4 42 4.0 4 28.6 6FFP 1.3 2 0 0 0 0Total 48.7 181 44.8 66 85.7 43
FFP, fresh frozen plasma.
Letter to the editor
© 2011 Blackwell Publishing Ltd 699