rehab registrars presentation june 2016
TRANSCRIPT

1
Upper Limb Retraining A1er Stroke
Karl Schurr Physiotherapist
Bankstown-‐Lidcombe Hospital 2016
Plan • Review essenFal components and analysis of:
– Reaching and Grasping • Review Evidence:
– Overview of effecFve intervenFons – Examples of intervenFons for stroke survivors who are:
• Weak • Stronger
• PracFce intensity • Outcomes:
– Measurement is essenFal • Discussion/QuesFons
Take-‐Home Messages • EssenFal to analyse causes of movement problems carefully
• Know, seek and train essenFal muscle acFons for grasp and reaching (essenFal components)
• The hand drives the shoulder • High doses of pracFce are required • PracFce doesn’t have to be perfect • Discuss pracFce and achievements with stroke survivors
• Expect people to improve: measurement!
EssenFal
Components 1

2
Essen%al Components
“Those elements upon which the ac1vity depends ” [Carr, 1987]
• Common features across individuals • KinemaFc features (what you see) • KineFc requirements (forces that produce what you see) • Environmental/physical constraints will modify task performance
Essential Components of Reaching for a Glass Transport:
Shoulder Forward Flexion External Rotation Protraction Elbow Flexion Elbow Extension
Pre-shaping: – Wrist extension – Ulnar/Radial deviation & Supination – Thumb Abduction – Thumb Conjunct Rotation – MCP and IP Extension – Finger abduction
Compensa%ons
• Strategies adopted by paFents to achieve desired goals when essenFal components are missing or impaired
• Become subsFtutes for efficient and flexible task performance
• Become learned behaviours if these strategies are successful in achieving the immediate goal and are pracFsed
Analysis of Reach to Grasp 2
3
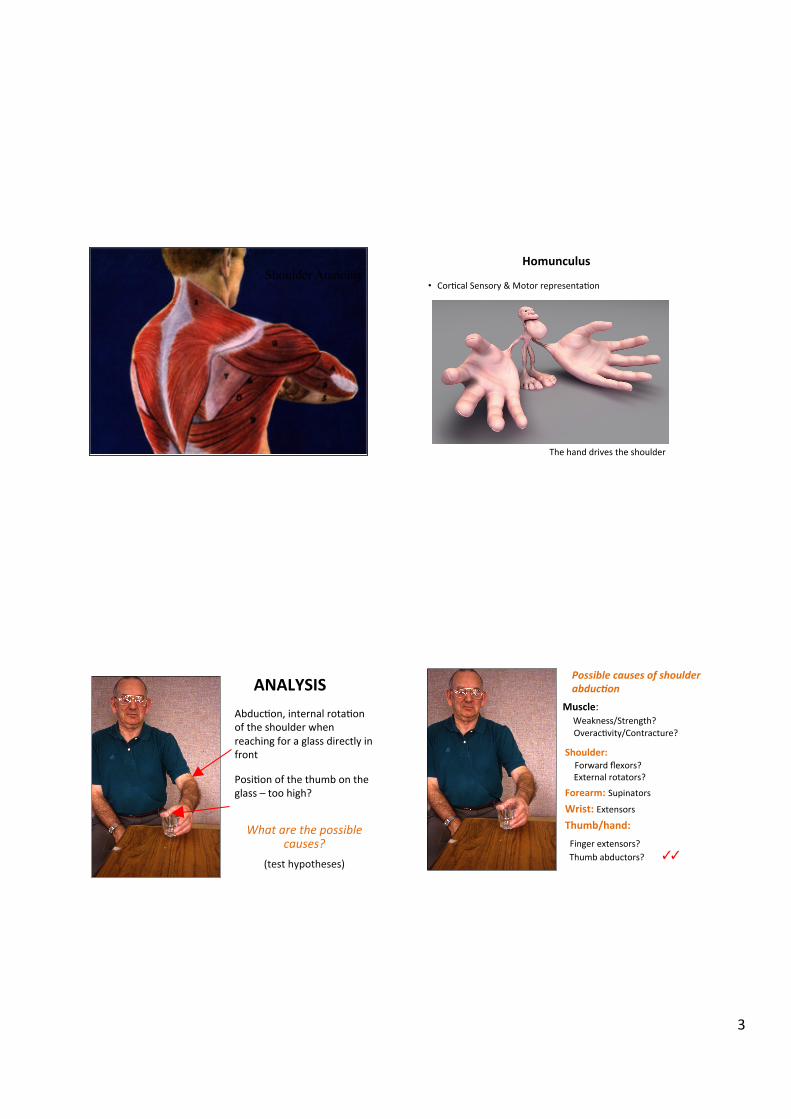
Shoulder Anatomy
The hand drives the shoulder
Homunculus
• CorFcal Sensory & Motor representaFon
ANALYSIS AbducFon, internal rotaFon of the shoulder when reaching for a glass directly in front
PosiFon of the thumb on the glass – too high?
What are the possible causes?
(test hypotheses)
Shoulder: Forward flexors? External rotators? Forearm: Supinators? Wrist: Extensors?
Thumb/hand:
Finger extensors? Thumb abductors?
Possible causes of shoulder abduc0on
✓✓
Muscle: Weakness/Strength? OveracFvity/Contracture?
4
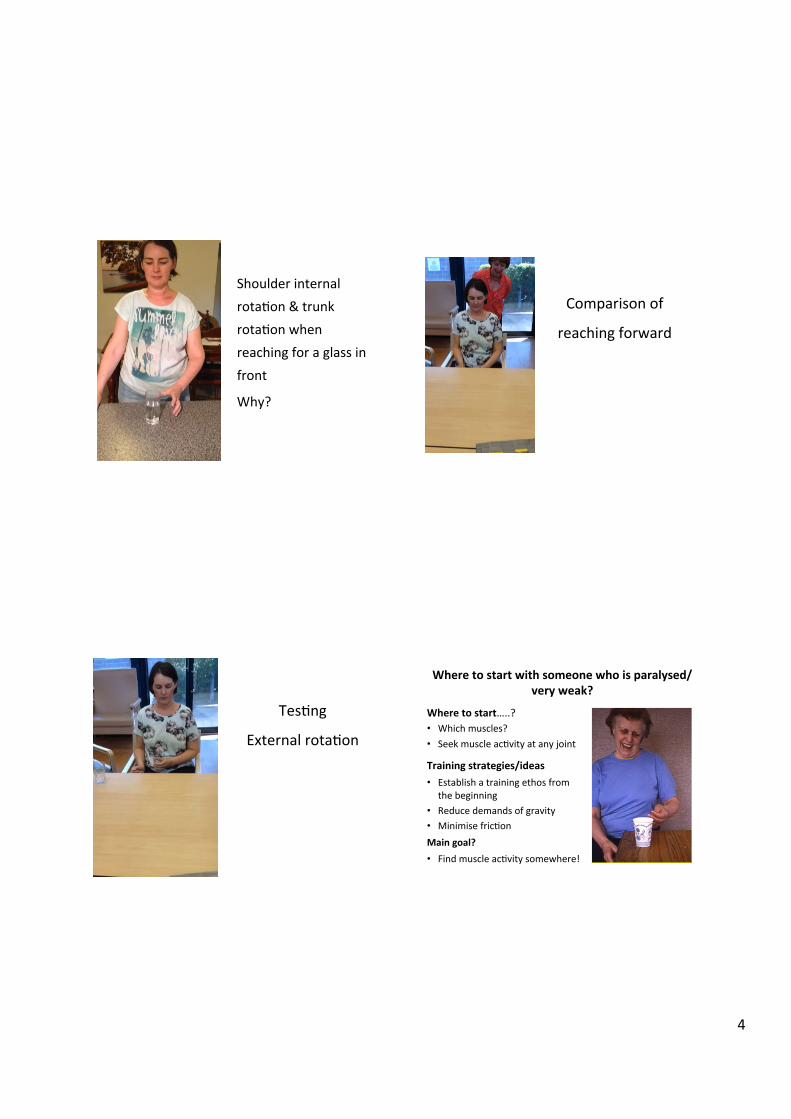
Shoulder internal rotaFon & trunk rotaFon when reaching for a glass in front
Why?
ANALYSIS
Comparison of
reaching forward
TesFng
External rotaFon
Where to start with someone who is paralysed/very weak?
Where to start…..? • Which muscles? • Seek muscle acFvity at any joint
Training strategies/ideas • Establish a training ethos from the beginning
• Reduce demands of gravity • Minimise fricFon Main goal? • Find muscle acFvity somewhere!

5
Current Evidence: • Task-‐Specific Training • Goals • Strength Training • Mirror Therapy • Electrical SFmulaFon • Constraint Induced Movement Therapy (CIMT)
3 2014
Pollock et al (2014)
Moderate quality evidence suggests that the following intervenFons may be effecFve: constraint-‐induced movement therapy (CIMT), mental prac%ce, mirror therapy, task specific interven%ons for sensory impairment, virtual reality and rela%vely high dose or repe%%ve task prac%ce. Moderate quality evidence also evidence also indicates that unilateral arm training (exercise for the affected arm) may be more effecFve than bilateral arm training.
Pollock et al (2014)
6
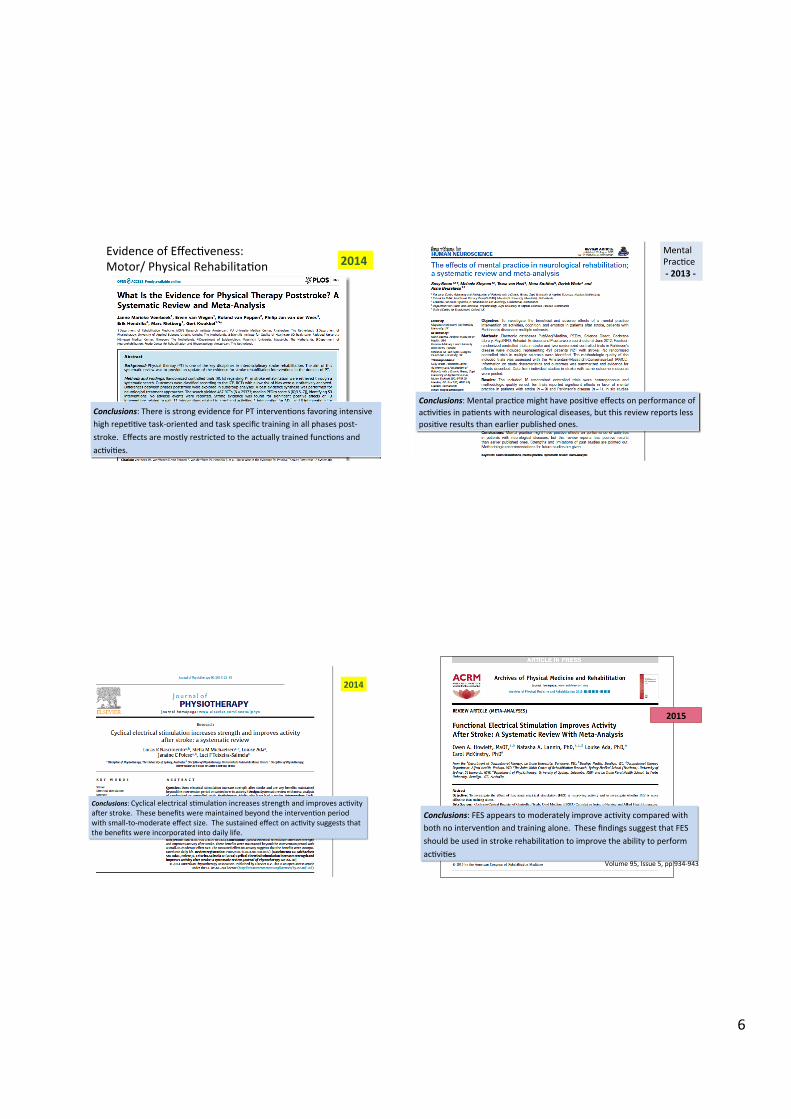
Evidence of EffecFveness: Motor/ Physical RehabilitaFon 2014
Conclusions: There is strong evidence for PT intervenFons favoring intensive high repeFFve task-‐oriented and task specific training in all phases post-‐stroke. Effects are mostly restricted to the actually trained funcFons and acFviFes.
Mental PracFce -‐ 2013 -‐
Conclusions: Mental pracFce might have posiFve effects on performance of acFviFes in paFents with neurological diseases, but this review reports less posiFve results than earlier published ones.
Electrical sFmulaFon
2014
Conclusions: Cyclical electrical sFmulaFon increases strength and improves acFvity a1er stroke. These benefits were maintained beyond the intervenFon period with small-‐to-‐moderate effect size. The sustained effect on acFvity suggests that the benefits were incorporated into daily life.
2015
Volume 95, Issue 5, pp 934-‐943
Conclusions: FES appears to moderately improve acFvity compared with both no intervenFon and training alone. These findings suggest that FES should be used in stroke rehabilitaFon to improve the ability to perform acFviFes

7
Lancet Neurology 2015
CIMT
2015 42 RCTs
51 RCTs
Conclusions: The original and modified types of CIMT have beneficial effects on motor funcFon, arm–hand acFviFes, and self-‐reported arm–hand funcFoning in daily life, immediately a1er treatment and at long-‐term follow-‐up, whereas there is no evidence for the efficacy of constraint alone (as used in forced use therapy).
Features of effec%ve UL motor interven%ons
Ø Task specificity
Ø Intensity of training
Ø Enable high repeFFons
Strength Training
Mirror Therapy
Electrical SFmulaFon
[Mental pracFce]
CIMT
Training Reaching Examples of ideas for people with profoundly weak muscles
• ProtracFon • External rotaFon • Elbow extension
4
Protrac%on
Goal: ‘Can you touch the table with the straw?’
Cylinder to reduce fricFon on the table
Cardboard cylinder to hold elbow in extension
Straw atached to side of cylinder – to touch goal marked on table
Counter to record repeFFons

8
Electrical s%mula%on: External RotaFon
Infraspinatus
Teres Minor
EMG triggered ES to elicit elbow extension
3 electrodes: EMG signal Muscle sFmulaFon
Go to botom of page ……
Training Pre-‐Shaping of the Forearm & Hand
• Wrist extension • SupinaFon • Thumb AbducFon & RotaFon • Finger MCP Extension
5
Mirror therapy to train wrist extension via Skype

9
Electrical SFmulaFon – Thumb AbducFon
Goal
Goal: To move thumb between the lines [with ES]
Lines drawn on top of index finger
ES for thumb abductors with muscles in a lengthened posiFon around a container
Mirror therapy: Finger /Wrist Extension Visual feedback for a stroke survivor
Example 1: Short-‐Medium Term Goals, Part-‐Whole PracFce
Goal
Goal: Slide the cup forward 5 cm -‐ stay within the lines
Goal
Goal
A B C
Advanced hand skills • Analysis of fork use 6

10
Analysis: ManipulaFon of a fork Analysis: ManipulaFon of a fork
Analysis: Manipulation of a fork Essential Components
Rotation at Thumb CMC joint
(vs thumb flexion)
Hint: look for posiFon of thumb nail
11
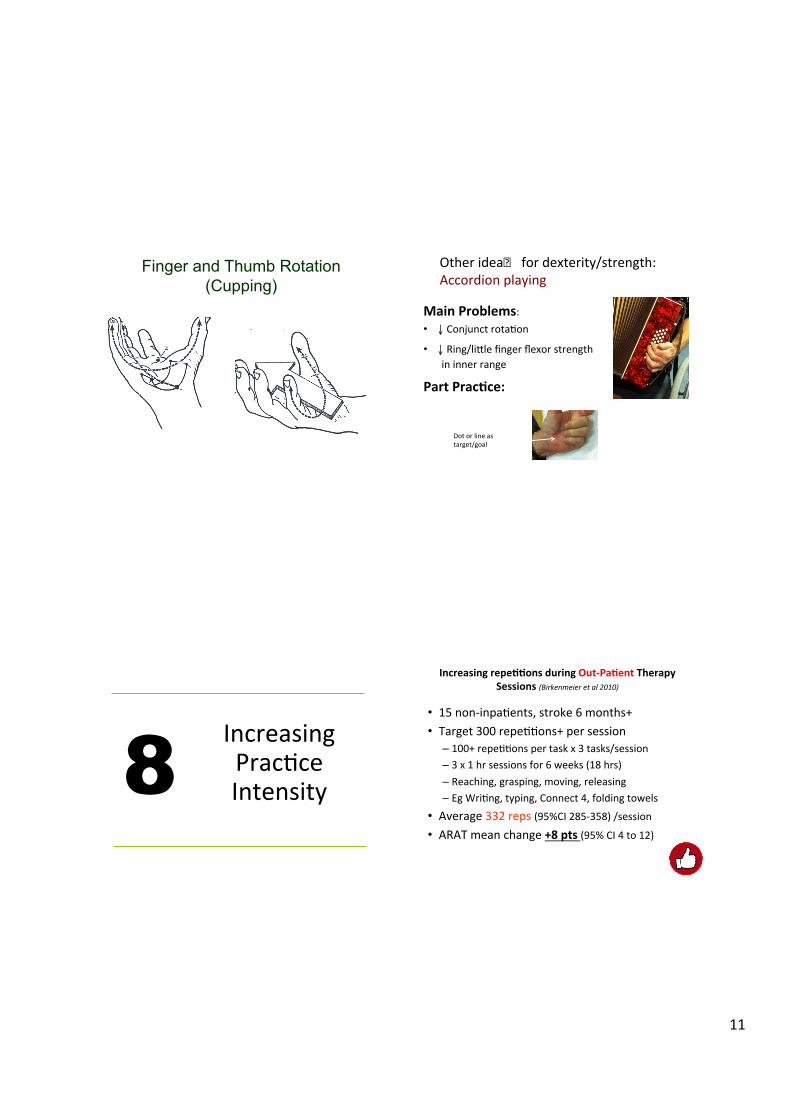
Finger and Thumb Rotation (Cupping)
Other ideas for dexterity/strength: Accordion playing
Main Problems: • ↓ Conjunct rotaFon • ↓ Ring/litle finger flexor strength in inner range
Part Prac%ce:
Dot or line as target/goal
Increasing PracFce Intensity 8
Increasing repe%%ons during Out-‐Pa%ent Therapy Sessions (Birkenmeier et al 2010)
• 15 non-‐inpaFents, stroke 6 months+ • Target 300 repeFFons+ per session
– 100+ repeFFons per task x 3 tasks/session – 3 x 1 hr sessions for 6 weeks (18 hrs) – Reaching, grasping, moving, releasing – Eg WriFng, typing, Connect 4, folding towels
• Average 332 reps (95%CI 285-‐358) /session • ARAT mean change +8 pts (95% CI 4 to 12)

12
CIMT Task-‐specific prac%ce: High intensity; mulFple repeFFons
From: Kwakkel et al [2015] p 225
Example of Task-‐Specific PracFce: Electric drill use
Day 2/3 Day 6 Day 8
ID Day 1 2 3 4 5 6 7 8 9 10 Av/hr Av/hr Total reps
S (JW) 1278 940 1230 1597 1469 1419 1114 948 1261 991 325 286 12,247
S (RB) 1293 1494 1720 1513 1141 1709 2029 1939 1507 -‐ 358 449 14,345
S(AG) 766 1511 1168 2041 1835 1983 1916 2056 1090 1509 366 427 15,875 S(BH) 463 878 1539 1482 1013 895 1125 1153 1227 1432 359 291 11,207 S (EP) 782 197* -‐ -‐ -‐ 200* 151* 120* -‐ 129* 200 150 1,579** S (CM) 491 603 628 -‐ 1186 758 771 1057 -‐ 1058 242 304 6,552 L (JF) 1894 1838 2201 1741 2168 1699 2258 2144 -‐ 2262 492 523 18,205 L (CM) 952 1341 1131 1452 1680 1304 1462 1652 1545 1482 328 372 14,001 L (CD) 1724 3045 3083 3771 3439 3375 3853 3697 -‐ 3576 753 906 29,563 L (CG) 2054 2489 1380 3206 1997 1921 2366 2647 1454 2615 556 419 19,514 L (BM)
2477 2433 3274 3512 2692 3211 1373 -‐ -‐ -‐ 719 1146 18,972
T (LW)
560 646 885 -‐ -‐ 846 962 -‐ 857 894 174 222 5650
T (SM)
722 852 1170 965 1002 799 1002 1183 900 910 236 240 9505
T (SS)
410 719 619 841 793 812 772 656 843 682 169 188 7147
T (JT)
765 1017 1095 1097 958 1004 1058 919 1135 919 245 252 9937
T (GC)
420 660 904 673 1019 816 736 1080 1032 972 184 232 8315
-‐ = Absent * = One hour CIMT/day due to illness ** = 8 hour total CIMT program
Repe%%ons/day /hour over 2-‐week CIMT programs (n=16)
Lowest
Highest
Increasing Repe%%ons during Out-‐Pa%ent Therapy Sessions (Birkenmeier et al 2010)
• 15 non-‐inpaFents, stroke 6 months+ • Target 300 repeFFons+ per session
– 100+ repeFFons per task x 3 tasks/session – 3 x 1 hr sessions for 6 weeks (18 hrs) – Reaching, grasping, moving, releasing – Eg WriFng, typing, Connect 4, folding towels
• Average 332 reps (95%CI 285-‐358) /session • ARAT mean change +8 pts (95% CI 4 to 12)

13
Measuring Change 9
EssenFal to measure
• Accuracy of analysis • Dosage of pracFce • Establish measureable goals:
– Person’s knowledge of achievements
– Feedback about progress within sessions as well as long term
• Determine effecFveness of intervenFons
Measuring Change
• Tasks of provide in-‐built measurements: – Time / speed (eg 1me to perform 2 reps)
– Accuracy of performance – Limb trajectory – Size of object grasped (mm) – Distance moved (mm) – % of correct atempts
• Keep measures simple and immediate
Standardised measures that capture change in people who are very weak :
n Motor Assessment Scale
n Box and block test
Concentrate on intensifying pracFce ….NOT assessing….
Measuring Change

14
Roles 10
How rehab specialists can assist with implementaFon of evidence for stroke survivors
• Contribute to development of team environments where ongoing examinaFon of evidence is established
• Team decisions/agreement regarding implementaFon of evidence: (eg Botulinum injecFons)
• Regular review of success of implementaFon • Expect measurement of change and clear goal se|ng at all stroke survivor progress reviews
• Don’t destroy stroke survivors’ hopes • Don’t refer to “my paFents” or “my staff”
Reference List Barclay-‐Goddard E et al (2011). Mental pracFce for treaFng upper extremity deficits in individuals with
hemiparesis a1er stroke. Cochrane Database of SystemaFc Reviews, Issue 1, Art No CD005950. Birkenmeier RL, Prager EM & Lang CE (2010). TranslaFng animal doses of task-‐specific training to people with
chronic stroke in 1-‐hour therapy sessions: A proof-‐of-‐concept study. NeurorehabilitaFon and Neural Repair, 24(7), 620-‐635.
Braun S, et al (2013) The effects of mental pracFce in neurological rehabilitaFon; a systemaFc review and meta-‐analysis. Front. Hum. Neurosci., 02 August
Howlet A et al (2015) FuncFonal electrical sFmulaFon improves acFvity a1er stroke: A systemaFc review with meta-‐analysis. Archives of Physical Medicine and Rehabilita1on. 96 (5), 934-‐943.
Katalinic OM, Harvey LA, Herbert RD, Moseley AM, Lannin NA, Schurr K (2010). Stretch for the treatment and prevenFon of contractures. Cochrane Database of SystemaFc Reviews, Issue 9, Art no. CD007455.
Kwakkel G Veerbeek J, van Wegen E & Wolf S (2015) Constraint-‐induced movement therapy a1er stroke. The Lancet Neurology. Volume 14, Pp 224–234
Lannin N.A., & Ada, L. (2011). Neurorehabilitaton splinFng: Theory and principles of clinical use. NeuroRehabilita1on. 28, 21-‐28.
Lohse, K.R., Lang, C.R., & Boyd, L.A. (2014 -‐ online early). Is more beter? Using metadata to explore dose-‐response relaFonships in stroke rehabilitaFon. Stroke, 45, 00-‐00.
Nascimento R et al (2014). Cyclical electrical sFmulaFon increases strength and improves acFvity a1er stroke: A systemaFc review. Journal of Physiotherapy, 60, 22-‐30.
Ross, L.F., Harvey, L.A., & Lannin, N.A. (online early, 2016). Strategies for increasing the intensity of upper-‐limb task-‐specific pracFce a1er acquire brain impairment: A secondary analysis from a randomised controlled trial. Bri1sh Journal of Occupa1onal Therapy.
Veerbeek M, et al (2014). What is the evidence for physical therapy post-‐stroke? A systemaFc review and meta-‐analysis. PLOS One, 9 (2, Feb), e87987.