registration requirements - edl · registration requirements ... the student will not be promoted...
TRANSCRIPT

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Registration Requirements
Kindergarten Registration Requirements for 2017-2018 school year! In order to attend kindergarten, children must be 5 years old on or before September 1, 2017.
What to Bring: 1. Student’s certified birth certificate (copies will not be accepted) 2.Student’s social security card (copies will not be accepted) 3.Student’s Mississippi Immunization Form 121 4.Proof of Residency Two current (July) utility bills 5.A completed registration packet
K-12 Admission What to bring: 1. Mortgage document, filed homestead exemption, or property deed. If leasing, original home or apartment lease 2. Two (2) current (July) utility bills (electric, water, gas, land phone). Bills addressed to a PO Box will not be accepted. Cell phone bills will not be accepted; 3. Certified birth certificate (no copies) 4. Social security card (no copies) 5. Certificate of health compliance issued by the Mississippi Department of Health or a local physician. 6. D-TAP (7th Grade Only) 7. A completed registration packet Students New to Leflore County School District in grades K-12 What to Bring: 1. Mortgage document, filed homestead exemption, or property deed. If leasing, original home or apartment lease; 2. Two (2) current (July) utility bills (electric, water, gas, land phone). Bills addressed to a PO Box will not be accepted. Cell phone bills will not be accepted; 3. Certified birth certificate (no copies); 4. Social security card (no copies); 5. Certificate of health compliance (immunization form 121) issued by the Mississippi Department of Health or a local physician; 6. Address of previous school attended; 7. Withdrawal information from the previous school attended; 8. A copy of last report card; 9. A completed registration packet from below.

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
STUDENTS LIVING WITH PARENT(S) OR GUARDIAN(S) The parent(s) or legal guardian(s) of a student seeking to enroll must provide the Leflore County School District
with at least two of the items numbered 1 through 10 below as verification of their address, except that a
document with a post office box as an address will not be accepted.
1. Filed Homestead Exemption Application form
2. Mortgage documents or property deed
3. Apartment or home lease
4. Utility bills
5. Driver's license
6. Voter precinct identification
7. Automobile registration
8. Affidavit and/or personal visit by a designated school district official and will still require two (2) of the
items numbered 1 through 10.
9. Any other documentation that will objectively and unequivocally establish that the parent or guardian
resides within the school district
10. Certified copy of filed petition for guardianship if pending and final decree when granted
HOMELESS CHILDREN When a child is determined to be homeless as defined by the Stewart B. McKinney Act 42 USC Section 11431
(1), 11432 (e) and 11302 (a), the Leflore County School District shall consider and take enrollment action that is
in the best interest of the child pursuant to 42 USC 11432 (e) (3).
STUDENTS LIVING WITH ADULTS OTHER THAN PARENTS OR LEGAL GUARDIANS: 1. The non-parent(s) claiming district residency must meet the criteria of subparagraph (a) (1) through (10)
above, required of a parent or legal guardian.
2. The district resident must provide the school with an affidavit (see last page of this policy) stating his or her
relationship to the student, and that the student will be living at his/her abode full time, and provide
documentation fully explaining the reason(s) (other than school attendance zone or district preference) for this
arrangement. The superintendent or his/her designee will make the necessary factual determinations as
required under this policy. Examples of situations where "in loco parentis" authority of an adult will be
recognized to establish residency of the minor include but are not limited to the following:
a. Death or serious illness of the child's parent(s) or guardian(s);
b. Abandonment of the child;
c. Child abuse or neglect;
d. Unstable family relationships or undesirable conditions in the home of the child's parents or
guardians having a detrimental effect on the child;
e. Students enrolled in recognized exchange programs residing with host families.
3. Whenever appropriate the person who has assumed responsibility for the care and custody of the child shall
be encouraged to obtain legal guardianship of the child.
The school district may require additional documentation and verification at any time.
At the minimum, the Leflore County School District shall maintain in a file a written instrument
identifying the types of documents used to verify each student's residency and copies of any
relevant guardianship petition or decree.
The provisions of this policy do not apply to students who reside outside the school district, but who
have legally transferred into the school district. Any court ordered procedure shall take precedent
over any procedure contained herein.

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
TRANSFER STUDENTS 1. No student is to be enrolled in this school district until any and all questions regarding residence
or immunizations have been resolved.
2. Students suspended or expelled from another school or school district may not be allowed to
enroll.
3. No pupil shall be permanently enrolled in a school in this school district who formerly was
enrolled in another school within the state or outside the state until the cumulative record of said
pupil shall have been received from the school from which he transferred. Should such record
have become lost or destroyed, then it shall be the duty of the superintendent or principal of the
school where the pupil last attended school to initiate a new record.
4. Unless a transfer student is tested in the manner provided in paragraph 5 below, the student will
be permanently enrolled and placed in a grade or class on the basis of an official transcript of
credits from the last school attended.
5. All students seeking to transfer from any school, public, private or home school, within or
outside of the boundaries of the State of Mississippi, to the Leflore County School District shall
be required to take a standardized test to determine the grade and class to which the pupil shall
be assigned at the time of pupil transfer.
The administrative head of the school shall administer the test or tests to such pupil or pupils as
shall apply for transfer to such public school. Such test or tests shall be administered within
thirty days after the filing of each such application for transfer.
Notice of the giving of such test shall be given the applicant not less than five days prior to the
date of the administration of such test.
No transfer of a pupil shall be affected until the test has been given and the pupil is assigned to
the grade and class for which the test shows he is best suited. No pupil shall be assigned to a
grade and class more than three (3) grades above or below the grade or class that the pupil
would have been assigned to had the pupil remained in the school from which the transfer is
being made. Pending the administration of the test herein provided for and its grading and an
assignment based thereon the superintendent of the Leflore County School District or the
attendance center principal to which the pupil seeks admission may assign the pupil temporarily
to a grade and class comparable to that in which the pupil would have been had the pupil
continued in the school from which the transfer was being made.
If any student is transferred or reassigned within the Leflore County School District by an order
of the board of trustees of this school district as designated by law of the State of Mississippi
and not at his own request, the requirement of that pupil's taking the standardized test shall be
waived. Likewise, if a pupil shall transfer from one school district to another school district in the
manner provided and required by the laws of the State of Mississippi, the requirement of such
pupil taking the standardized test shall be waived.
6. Any legal guardianship formed for the purpose of establishing residency for school district
attendance purposes shall not be recognized by this school board.
Note: (See also Policy JBCD Transfers and Withdrawals of Students)

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Notification of Literacy-Based Promotion
Act (for 3rd Grade Students only)
1. In compliance with the "Literacy Based Promotion Act," it is the intent of the District
to improve the reading skills of kindergarten through third grade students so that
every Student completing the third grade is able to read at or above grade level.
2. Each Student's progress shall be determined by the Student's proficiency in
reading.
3. Immediately upon the determination of a reading deficiency, and subsequently with
each quarterly progress report until the deficiency is remediated, the District shall
notify the Student's parent/legal guardian of the deficiency in accordance with
procedures outlined in this policy. If a Student's reading deficiency is not remedied
by the end of the third grade year, the Student will not be promoted to the fourth
grade.
4. Social promotion is prohibited. A Student may not be assigned a grade level based
solely on the Student's age or any other factors that constitute social promotion.
5. Beginning in the 2014-2015 school year, if a Student's reading deficiency is not
remedied by the end of the third grade, the Student shall not be promoted to fourth
grade. The District will provide written notification to the parent/legal guardian of
any third grade student who is retained that the student has not met the proficiency
level required for promotion and, if applicable, the reasons the student is not
eligible for a good cause exemption. Any third grade student who is retained shall
be provided with a high-performing teacher.
By signing below, I am aware that my child, ____________________________________
must meet the aforementioned requirements according to SB 2347 Literacy-Based Promotion
Act before he/she will be promoted.
___________________________________________ __________________________
Parent’s or Legal Guardian’s Signature Date

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Residency Registration & Documentation
Checklist
Name of Student: _____________________________________
Name of Parent/Court Appointed Guardian: _______________________________________
Address: __________________________________________________________________
Street Apartment # City State Zip Code
1. I certify that the information given above on this form is a true and correct statement of
my legal residence. Should my legal residence change while the above student is
enrolled in the above cited school district, I will promptly notify the appropriate officials
of this district. I understand that a pupil is not legally enrolled until this form is
completed and signed by the parent or court appointed guardian with whom the
student may be living. I understand that a pupil admitted under false information is not
legally enrolled and is subject to penalty.
2. I hereby certify that the student named on this registration form has not been expelled
or suspended from another school. If the student has been expelled or suspended,
please write the name of the school, date of the expulsion or suspension, and the
reason for such expulsion or suspension in the space provided below.
Date expelled/suspended:
School: ___________________________________________________________________
Reason(s):
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
Parent’s signature: _____________________________________________ Date: ________
Phone Number: _________________________________

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Acceptable Use of Internet Policy
Leflore County School District Acceptable Use Policy Please read the following information carefully:
Internet access is available to students and staff in the Leflore County School District (LCSD). Our
goal in providing this service is to further the mission of the LCSD: to provide a quality formal
education to enable its students to achieve academic success and become productive, contributing
members of society. Internet access is to be used for educational purposes.
Pupil guidelines for Internet use:
Pupils are responsible for good behavior on the Internet, just as they are in a classroom or a school
corridor. General school rules apply. Access is a privilege, not a right, and that access requires
responsibility.
Individual users of the Internet are responsible for their behavior and communications over the
network. Users will comply with school standards and honor the agreements they have signed.
Computer storage areas will be treated in a similar manner as school lockers. Staff may review files
and communications to insure that users are using the system responsibly. Users should not expect
that stored files would be private.
During school, teachers will guide pupils toward appropriate materials. Families bear responsibility for
providing such guidance as they must exercise with other information sources, such as television,
telephones, movies, radio, and other potentially offensive media.
The following are not permitted:
1. Sending or displaying offensive or inappropriate messages or pictures
2. Using obscene or inappropriate language
3. Harassing, insulting or attacking others
4. Damaging computers, computer systems or computer networks or changing computer settings
5. Violating copyright laws
6. Using others' passwords or teacher’s logins
7. Trespassing in others' folders, work or files
8. Intentionally wasting resources
9. Using network for commercial purposes
10. Installing ANY software on LCSD computers
11. Downloading ANY files without a teacher’s permission
12. Revealing personal addresses, phone numbers or student names
13. Participating in chat sessions not supervised by a teacher
Students are to notify an adult immediately if they encounter materials which violate the rules of
appropriate use.
Students are to be prepared to be held accountable for their actions and for disciplinary
consequences if the Acceptable Use Policy is violated

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Parent Internet Network Access Agreement
IMPORTANT NOTICE TO PARENTS
Due to the nature of the Internet, it is neither practical nor possible for the school district to enforce
compliance with user rules at all times. Accordingly, parents and students must recognize that
students will be required to make independent decisions and use good judgment in their use of the
Internet. Therefore, parents must participate in the decision whether to allow their children access to
the Internet and must communicate their own expectations to their children regarding its appropriate
educational use.
As a parent/guardian of this student, I have read the board-adopted policies on Internet Use by
Students, the administrative procedures, and the Internet Network Access Agreement.
I understand that Internet access is designed for educational purposes and that the
school/district will attempt to discourage access to objectionable material and
communications that are intended to exploit, harass or abuse students. However, I
recognize it is impossible for the Leflore County School District to restrict access to all
objectionable material, and I will not hold the school or school district responsible for
materials acquired or contacts made on the Internet.
I understand that a variety of inappropriate and offensive materials are available over
the Internet and that it may be possible for my child to access these materials if he/she
chooses to behave irresponsibly. I also understand that it is possible for undesirable or
ill-intended individuals to communicate with my child over the Internet, that there is no
practical means for the school/district to prevent this from happening, and that my child
must take responsibility to avoid such communications if they are initiated. While I
authorize the staff to monitor any communications to or from my child on the Internet, I
recognize that it is not possible for the school to monitor all such communications. I
have determined that the benefits of my child having access to the Internet outweigh
potential risks.
I understand that any conduct by the herein named student that is in conflict with these
responsibilities is inappropriate, and such behavior may result in termination of access
and possible disciplinary action.
I have reviewed these responsibilities with my child, and I hereby grant permission to
the school/district to provide Internet network access.
I agree to compensate the school/district for any expenses or costs it incurs as a result
of my child’s violation of Internet policies or administrative procedures
Parent/Guardian Name(s) _________________________________________________________
(Please Print)
Parent/Guardian Signature(s) ______________________________________________________

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Student Internet Access Agreement
I accept the responsibility to abide by the Leflore County School District’s board-approved policy on
Internet Network Access and by procedures as stated below in this Agreement. I understand that the
use of the Internet and access to it is a privilege and not a right. I agree:
To use the Internet network for appropriate educational purposes and research;
To use the Internet network only with permission of designated school staff;
To be considerate of other users on the network and to use appropriate language for
the school environment;
To not intentionally degrade or disrupt Internet network services or equipment. This
includes but is not limited to tampering with computer hardware or software,
vandalizing data, invoking computer viruses, attempting to gain access to restricted or
unauthorized network services, or violating copyright laws;
To report immediately any security problems or breeches of these responsibilities to
appropriate staff;
To comply with all rules and expectations included in the policies included under
Internet Use by Students (Policy IJ-R) and with administrative procedures and
guidelines; and,
To not divulge personal information such as addresses and telephone numbers over
the Internet.
I understand that I have no right to privacy when I use the school/district Internet network(s), and I
consent to the monitoring of my communications over the Internet by school/district staff.
I also understand that any conduct that is in conflict with these responsibilities is inappropriate and
may result in termination of Internet access and possible disciplinary action.
Name: _______________________________ School: __________________________________
(Please Print)
Home Address: ________________________________________________________________
Student Signature: ____________________________________ Date: __________________
NOTE: This form is to be used in conjunction with the following policies: (EI) Computer Software
Usage, (IJ) Technology and Instruction / Electronic Information Resources, IJ-E (1) Internet Network
Access Agreement, IJ-E (2) Internet Parental Consent Agreement, (IJA-E) Internet Etiquette, (IJA-P)
Internet Administrative Procedures
LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
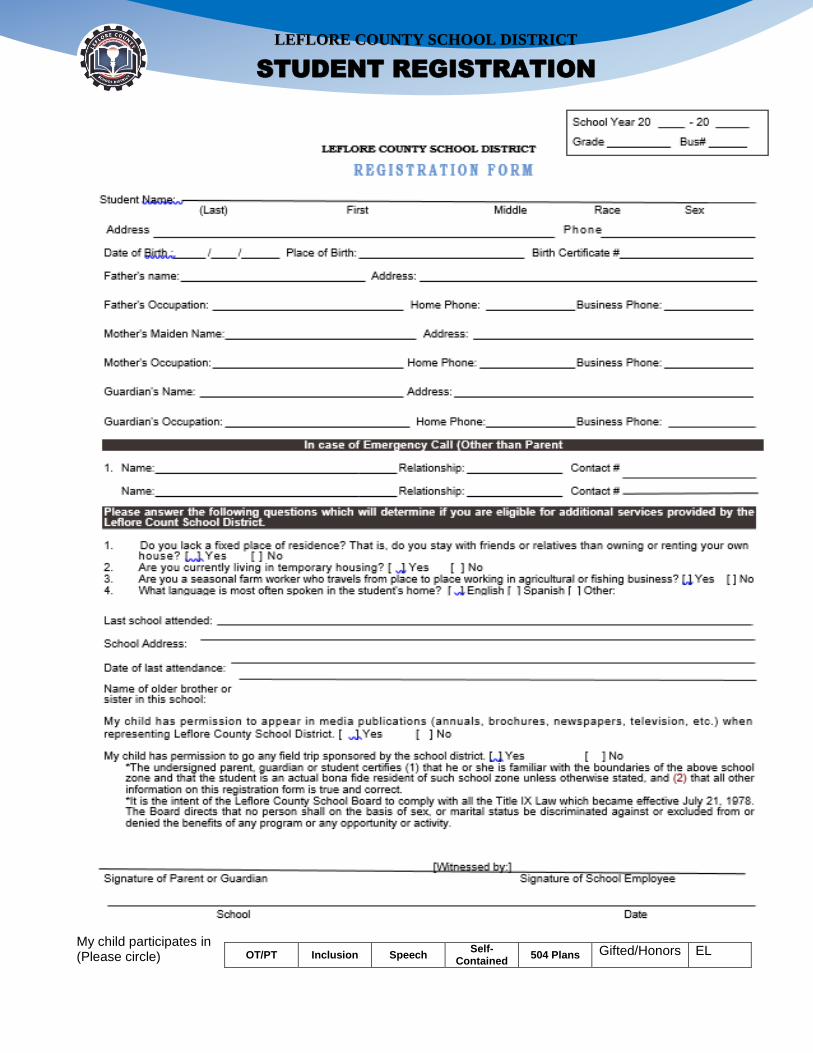
My child participates in (Please circle)
OT/PT Inclusion Speech Self-
Contained 504 Plans Gifted/Honors EL

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Student’s Checklist
Registration Form
Book Card
Residency Documentation (2 proofs)
Administration of Medicine at School Form
Asthma Action Plan (AAP) if applicable
Birth Certificate
Social Security Card
Immunization Record
Home Language Survey
Photo-In District Travel Consent Form
Parent-Student-Teacher-Principal Compact
Parent-Student- Handbook Agreement
Acceptable Use Policy-Signed Agreements
SB 2347 Literacy Based Promotion Act Agreement (3rd Grade Students Only)
Athletic Participation Form (if applicable)
7th Graders- Updated Immunization (T-dap)
Student’s Name: ___________________________________________ Grade Level: _____________________
Parent’s Name: ____________________________________________ Contact Number: _________________
School’s Name: ____________________________________________________________________________
District Personnel’s Signature: _____________________________________ Date: _____________________

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
DEPARTMENT OF ATHLETICS
STUDENT PARTICIPATION CLEARANCE FORM
I hereby give consent for my child, _________________________________________to participate in
the __________________________________ School District’s athletic and activities programs during
the_____________________ school year. I agree to abide by the rules and regulations of my school
district and its governing body, the Mississippi High School Activities Association.
I hereby authorize and give permission for emergency medical treatment to be rendered for and on
behalf of my child, ____________________________________, for any injury received while
participating in any supervised school activity. This authorization includes, but is not limited to, any
treatment deemed necessary by certified personnel, physicians, hospital emergency room physicians
and hospitals.
I hereby release the _____________________________ School District and all school personnel for
any and all liability associated with such necessary treatment.
I hereby acknowledge that health and accident insurance is recommended for participation in all
organized sports and activities and further certify that my child is covered under the health and accident
program listed below.
School day insurance: ________________________ Other insurance: _______________________
Policy # _______________________________ Policy # _______________________________
In addition, I assume any expenses for liability not covered by the insurance policy above for injury
received by the above named student while participating in sports and school activities. I accept full
responsibility for medical and hospital expenses and any other related expenses and do hereby hold
harmless the ______________________________ School District and the Board of Trustees, their
agents or assignees, of responsibility for any such injury or expenses and waive any and all claims
which may arise against them. I realize that participation in organized sports and activities involves the
potential for injury, sometimes severe enough to result in total disability, paralysis, or death.
I give the Mississippi High School Activities Association and its assigns, licensees and legal
representatives the irrevocable right to use any picture or image or sound recording of the student in
all forms and media and in all manners, for any lawful purposes. In addition, I consent to the disclosure,
by my child’s/ward’s school, to the MHSAA, upon its request, of all records relevant to his/her eligibility
and participation including, but not limited to, his/her records relating to enrollment and attendance,
academic standing, age, discipline, residence and physical fitness.
The Student Participation Clearance Form is required for all students to participate in MHSAA
athletic and activity programs.
Parent/Legal Guardian ___________________________ Phone # _______________________
Cell #________________________________ Date _________________ (valid 365 from this date)

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Home Language Survey
Student’s Name: _________________________________________ Date of Birth: _____________ Sex: ______
Parent/Guardian’s Name: _____________________________________________________________________
Address: ___________________________________________________________________________________
Home Telephone: ________________________________________ Work Telephone: ____________________
School: ______________________________________________ Grade: _____________ Date: _____________
Federal and state laws require the following information be collected about the primary and home language of
every student upon enrollment in the school district. Please completer a survey for each child you are enrolling
in the school district.
1. What language did your child learn when he/she first began to talk? ___________________________
2. What language does your child most frequently speak at home? _______________________________
3. What language is spoken by you and your family most of the time at home? ______________________
If language other than English is indicated for any of the above questions, the school district will test
your child’s English language proficiency to determine eligibility for initial and contributing placement
in an English language development program. You will be notified about the results of this testing.
4. If available, in what language would you prefer to receive information from the school? ____________
5. Has this student attended any U.S. school in any three years of his/her lifetime? __________________
____________________________________________________________________ _____________________
Parent or Guardian’s Name Date
Office Use Only
Student ID # Date Distributed Date Received

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Administration of Medicine at School
Procedure for parent to follow if it is essential that a student received medication during time of attendance at
school.
1. Your physician must complete and sign the "Permission for Medication Administration at School" form.
Instructions must be specific and not dependent on school staff judgement.
2. You must sign the "Permission for Medication Administration at School" form and return the form to your
child's school.
3. Provide medicine in container with the original label from the doctor or pharmacist. This label must have
your child's name, the name of the medication, dosage and time of administration, and correct date.
4. To prevent unsupervised access of your child or other students to the medication, you must deliver the
medicine to the school. The quantity acceptable to keep at school may be restricted.
5. Maintain a record of the date and quantity of medicine you provided the school so you will know when to
replenish the medication.
6. Provide the school with new permission if there is a change in medication or change of your child's health
care provider. Permission must be renewed each school year.
7. If your child has asthma, please complete an Asthma Action Plan that can be found at your school.
8. If a parent or guardian cannot be reached, the school staff reserves the right to notify the physician for any
questions regarding medicine or condition of the student.
9. The complete Leflore County School District policy on medicine in school on medicine in school is in the
student's handbook.
Thank you for your cooperation.
__Beverly Quinn___________________ __Tammie Coleman________________________
District School Nurse District School Nurse
___Dr. Ilean Richards______________
Interim Superintendent I have read and understand the policy on medicine administration, I also understand that if my child has
asthma, an Asthma Action Plan must be completed.
________________________________________________________________________________
Parent/Guardian Signature Date

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Leflore County School District
PARENT AUTHORIZATION AND IDEMNITY AGREEMENT
The undersigned parent/s of _____________________________________________ , Child's Name
a minor child, has requested personnel of this school district to administer prescription medicine to
this student. This request has been made for my/our convenience as a substitute for parental
administration of this medicine.
Medications:
1. _____________________________________________________________________
2. _____________________________________________________________________
3. _____________________________________________________________________
4. _____________________________________________________________________
5. _____________________________________________________________________
6. _____________________________________________________________________
7. _____________________________________________________________________
8. ______________________________________________________________________
Reactions to Medication (how it affects the child, etc.) ________________________________ It is understood that the school personnel administering the medicine will not have to have medical or nursing training.
I/We forever release, discharge and covenant to hold harmless the School District, its personnel and Board of Trustees from any and all claims, demands, damages, expenses, loss of services and causes of action belonging to the minor child or to the undersigned arising out of or on account of any injury, sickness, disability, loss or damages of any kind resulting from the administration of the prescription medicine. I understand that I as parent/guardian am responsible, to personally inform the building principal of any changes in dosage(s), medication(s), or prescriptive discontinuations.
The undersigned agree to repay the school district, its personnel or Trustees any sum of money, expenses, or attorney's fees that any of them may be compelled to pay in defense of any action or on account of any such injury to the minor child as a result of the administration of medicine. I have read the foregoing release and indemnity agreement and fully understand it.
Executed the ________________ day of _________________________, 20 ___________ .
Parent or Guardian:_______________________________________________________________
Witness:__________________________________________________________________________

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
Asthma Information Sheet
Asthma is a serious condition in which there are symptoms of shortness of breath, wheezing, coughing, or
rattling sounds with breathing. Episodes can be caused by various triggers, such as a sudden change in
weather, pollen, dust, smoke, strong perfumes, or air fresheners. These symptoms are due to a sensitivity of
the airways in the respiratory system that causes a difficulty with getting air in and out of the lungs. Severe,
uncontrolled attacks can cause a child to stop breathing.
Ways to better manage your child’s asthma:
1. Always make sure your child has his/her inhaler available, whether he carries it with him or keeps it in
the classroom. Make sure medication has not expired and that it is not empty. Ask doctor to make a
prescription for 2 inhalers-one for school and one for home.
2. There is a medication teacher assigned to each school who can administer a breathing treatment with
proper orders from the doctor. The school nurse oversees the teaching of these procedures and keeps
constant contact with the teacher.
3. Be mindful about your child’s asthma and what triggers cause attacks. Fall, spring, and flu season are
the most prevalent times for asthma attacks. Be aware of weather changes.
4. Keep regular doctor appointments at least twice a year.
5. Take prescription medications only as the doctor orders them.
6. Be aware of when asthma is beginning to get worse. Pay attention to how student feels and how
his/her breathing is. Do not wait until asthma gets too bad to take to the doctor!
7. Have all medical forms completed at school so the teachers and school nurse will be aware of your
child’s condition. In order for us to take the best care of your child, we need to know all about his/her
condition.
LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION
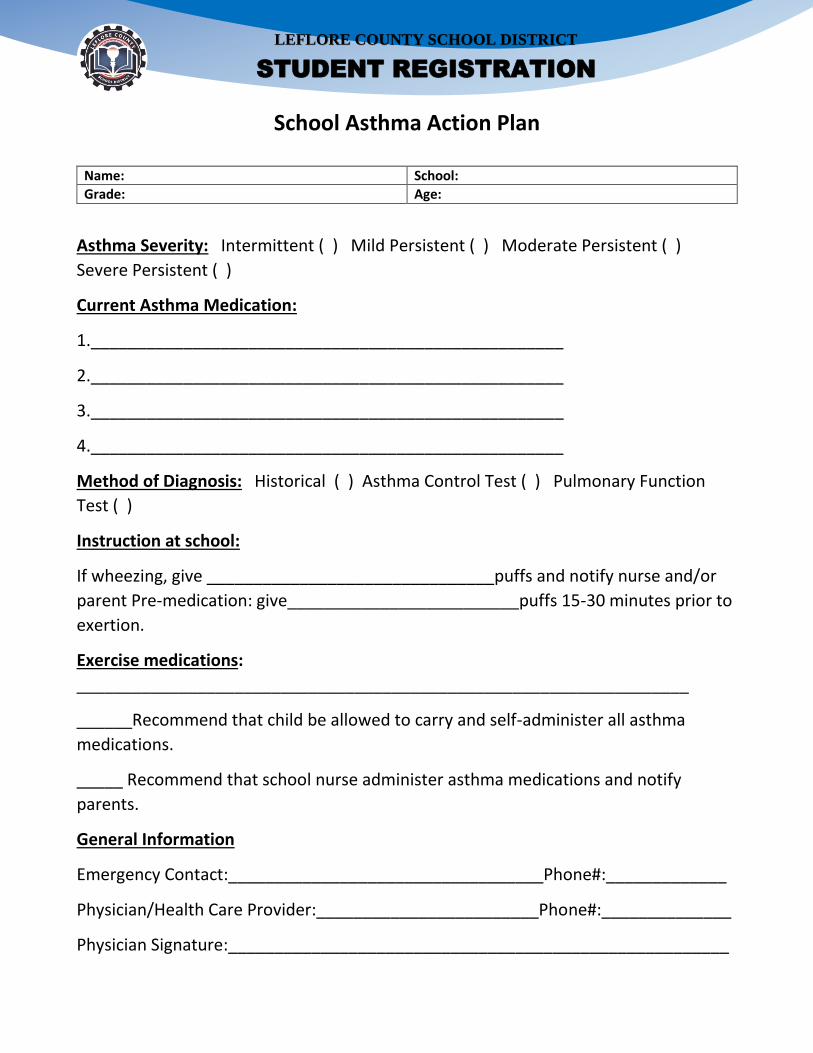
School Asthma Action Plan
Name: School:
Grade: Age:
Asthma Severity: Intermittent ( ) Mild Persistent ( ) Moderate Persistent ( )
Severe Persistent ( )
Current Asthma Medication:
1.___________________________________________________
2.___________________________________________________
3.___________________________________________________
4.___________________________________________________
Method of Diagnosis: Historical ( ) Asthma Control Test ( ) Pulmonary Function
Test ( )
Instruction at school:
If wheezing, give _______________________________puffs and notify nurse and/or
parent Pre-medication: give_________________________puffs 15-30 minutes prior to
exertion.
Exercise medications:
__________________________________________________________________
______Recommend that child be allowed to carry and self-administer all asthma
medications.
_____ Recommend that school nurse administer asthma medications and notify
parents.
General Information
Emergency Contact:__________________________________Phone#:_____________
Physician/Health Care Provider:________________________Phone#:______________
Physician Signature:______________________________________________________

LEFLORE COUNTY SCHOOL DISTRICT
STUDENT REGISTRATION