reference guide for pacu lumbar fusion - harvard · pdf filelumbar fusion clinical pathway all...
TRANSCRIPT

Lumbar Fusion
CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes.
This Clinical Pathway is intended to assist in clinical decision making by describing a range of generally acceptable intervention and outcomes. The guidelines attempt to define practices that meet the needs of most patients under most circumstances. However, the ultimate judgment must be made based on circumstances that are relevant to that patient and treatment may be modified according to the individual patients needs.
Reference Guide for PACU


PACU Lumbar Fusion Clinical PathwayPAIN MANAGEMENT / COMFORT – PAIN GUIDE
Preoperative Medications:
1) Acetaminophen Dose: 1000 mg PO Contraindications: severe liver dysfunction,
allergy, use within previous 6 hours
2) Pregabalin OR Gabapentin OR Home Dose if taking Mscontin or Oxycontin
Doses: Please consider contributions from other sedating agents or medical comorbidities and modify dose accordingly.
i. Pregabalin: • 150 mg if < 70 yr old and > 70 kg • 75 mg if > 70 old or < 70 kg ii. Gabapentin: • 600 mg if < 70 yr old and > 70 kg • 300 mg if > 70 yr old or < 70 kg Contraindications: renal dysfunction (GFR < 30),
allergy Chronic users should receive their scheduled dose
in preop holding if they did not take it prior to coming to the hospital.
3) Oxycontin Dose: 10 mg if not taking long-acting narcotic
chronically Patients taking MScontin, oxycontin, methadone
should receive their regularly scheduled dose instead.
4) Celecoxib Dose: 400 mg x 1 Contraindications: • Significant renal dysfunction, platelet
dysfunction • Severe CAD • Allergy (remember this drug may be
problematic in patients with sulfa allergy)
Intraoperative Analgesia Management suggestions:
1) Opioids a. Fentanyl: minimize use b. Hydromorphone/Morphine/Methadone:
Use intraoperatively as needed.
2) Ketamine: this is useful to spare opioids and to reduce risk of hyperalgesia. It is useful in highly opioid tolerant patients and in neuromonitoring cases.
Bolus dosing: 0.1-0.2 mg/kg after induction Drip: 0.1-0.2 mg/kg/hr Side effect profile is minimal using these
dosing strategies
3) Dexmedetomidine: This is very effective in highly opioid tolerant patients. Can cause significant sedation in higher doses. Can cause bradycardia and hypotension, dry mucous membranes.
Dose: 0.2-0.7 mcg/kg/hr (IBW) Bolus (use great caution) 5-10 mcg q 5 minutes
up to 1 mcg/kg IBW
4) Anti-Infectives: Antibiotics are per ID recommendations. These recommendations are posted in the OR or available on the portal.

Lumbar Fusion Pain Pathway
Epidural?
Tolerates PO?
Patient taking < 60 mg
morphine/day
Suboxone, subutex,
Naltrexone?
Patient taking> 60 mg
morphine/day
Pathway “B”Opioid tolerant
CPS/POP Consultrequired
Follow CPS plan
Pathway “A”Opioid Naive
Pathway “C”IV pathway (least preferred) Patient
should be changed to PO ASAP
Consult APS 37246
(3PAIN)
Is this aCPS patient?
Is thereadequate
analgesia?
Contact CPS
3OUCH36824
Prepare discharge plan including:1) Weaning from opioids2) PRN-(or) as needed
Excludes Dr. Glazerpatients
Lumbar Fusion Pain Pathway
Yes
Yes
Yes
Yes
No
No
No
Yes
No
No
Yes
YesNo
Yes
No
Yes
Generalized Pain Pathway Descriptions:
A Patients that are Opiate Naive: < 60 mg Morphine Equivalent/day
B Patients that are Opiate Tolerant: > 60 mg Morphine Equivalent/day
C Patients Intolerant of oral medications or strictly NPO
CPS Consult Patients on Methadone, Suboxone, Subutex, Buprenorphine, and Naltrexone IM or for any patient taking > 60 mg morphine equivalents/day for > 2 weeks

Pathway A: Opiate naïve or uses < 60 mg morphine equivalent/day (see table) “B”Drug Initial dose Frequency Adjustment options
Acetaminophen1 1000 mg Q 8 hours 500 mg Q 6-8 hours
Oxycodone 5-10 mg PO Q 4 hours 10-15 mg Q 4 hours
Hydromorphone 2-4 mg PO Q 4 hours 4-6 mg, can give Q 3hours
Morphine PO (MSIR)
15mg PO Q 4 hours None, contact APS
Anticonvulsants Start with low dose
See list below
Muscle relaxants Start with low dose
See list below
Oxycontin2 10 mg PO Q 12 hours Contact APS
MSContin2 15 mg PO Q 12 hours Q 8 hours, Contact APS
Ketamine drip (with APS consult only)
0.1-0.3 mg/kg/hr Infusion Contact APS
Celecoxib3 400 mg PO Once/day 200 mg BID3 x 24 hr
1. Acetaminophen: decrease dose or avoid in patients with liver dysfunction.
2. Consider omitting in opioid naïve patients who are not taking any opioids at baseline.
3. Single preoperative celecoxib dose OK. If celecoxib or ketorolac are needed postop, attending surgeon approval is required.
PO Pain Medication Pathways:Patients should remain on all preoperative medications during
the hospitalization unless contraindicated for the surgery.
Use fewest number of medications required at lowest doses necessary.
Limit long-acting opioids to 5 days following discharge unless patients are stabilized on them prior to surgery.
Use caution with combining narcotics and sedatives in patients with:
o Obstructive sleep apnea
o Cognitive dysfunction
o Over 70 years old
Restrict use
Preferred

IV breakthrough Pain Medications:Drug Dose Frequency Adjustments
Hydromorphone 0.5-1 mg Q 4 hours 0.25 mg patients > 70 years old
Morphine 1-2 mg Q 4 hours 0.5 – 4 mg
Meperidine 25-100 mg PO/IV/IM Q 6 hours APS/CPS only
Anticonvulsant Medications for Pain Management (all PO only):Drug Dose Frequency Adjustments 1) Decrease the dose in renal
insufficiency
2) Decrease the dose in patients > 70 years old.
3) Use caution (avoid) in patients with cognitive dysfunction.
Gabapentin 100-300 mg (naïve) Q 8 hours 300 mg-900 mg Q 8 hr
Pregabalin 75-150 mg Q 12 hours 75-300 mg Q 12 hr
Topiramate 25-50 mg (APS/CPS only unless stabilized on drug)
Q 12 hours 25-200 mg/day
Muscle Relaxants for Pain Management:Drug Dose Frequency Adjustments 1. Increased risk of serotonin syndrome
when used in patients on SSRIs.
2. Initiate with recommendation by APS or CPS only. Continue drug if patient has been stabilized on one of these drugs preoperatively.
With all of these drugs use great cau-tion in patients > 70 years old. They may increase the risk of delirium especially in combination with other medications.
If patient is stabilized on regimen, please consider modifying dose rather than add-ing another drug in the same class.
Diazepam 5 mg PO BID-QID prn 10 mg BID-QID
Lorazepam 0.5-1 mg PO BID-TID prn 2 mg BID-TID
Flexeril1 (cyclo-benzaprine)
5 mg PO Q 8 hours 10 mg Q 8 hours
Skelaxin (metaxalone)
800 mg PO(APS/CPS only2)
Q 8 hours 800 mg Q 6 hours
Robaxin (methocarba-mol)
500 mg PO(APS/CPS only2)
Q 4 hours 1000 mg Q 6 hours, 1500 mg Q 8 hours x 48 hours
Baclofen PO 5 mg PO(APS/CPS only2)
Q 8 hours 10-15 mg Q 8 hours
Baclofen pump Consult CPS for interrogation preop and postop
α-2 adrenergic agonists: Drug Dose Frequency Adjustments These drugs should be initiated by APS
or CPS only.
If patients are taking these preoperatively, do NOT discontinue abruptly.
Avoid in patients > 70 years old unless stabilized on regimen.
Clonidine 0.1 mg PO Q 12 hr 0.2 mg Q 12 hrs over several days
Clonidine transdermal 0.1 mg patch Q 7 days none
Tizanidine 2-4 mg PO Q 8 hours 4 mg Q 8 hrs after several days
Morphine Equivalents (in mg/day):Drug IV PO Methadone and buprenorphine equivalents are controversial.
Do not make adjustments without consulting CPS or APS.
Consult CPS for patients on Methadone, Suboxone, Subutex, buprenorphine, Naltrexone IM or for any patient taking greater than 60 mg morphine equivalents per day for greater than 2 weeks.
Morphine Sulfate 20 mg 60 mg
Oxycodone n/a 40 mg
Hydromorphone 4 mg 20 mg
Oxycontin n/a 40mg
MSContin n/a 60 mg
Fentanyl patch 25 mcg/hr n/a
Oxymorphone n/a 40-50 mg

Pathway B: Opiate tolerant patients (> 60 mg morphine equivalents/day) “C”.
a) These patients should have a preoperative POP consult with CPS.
b) If patients do not have a CPS or POP consult, please use the suggested doses listed below. Consider APS consult.
c) Please use IV breakthrough narcotics as listed for opiate-naïve patients
Drug Initial dose Frequency Adjustment options
Oxycodone 10-15 mg PO Q 4 hours 20 mg Q 4 hours
Hydromorphone 4-6 mg PO Q 4 hours 4-8 mg, may give Q 3hours
Morphine PO (MSIR) 15-30mg PO Q 4 hours 30 mg Q 4 hours
Acetaminophen 1000 mg PO Q 8 hours 500 mg Q 6-8 hours1
Anticonvulsants4 Start with low dose. (see note 4 below)
See list below
Muscle relaxant Start with low dose.
See list below
Oxycontin 10 mg (or preoperative dose)
Q 12 hours Use APS/CPS recommended dose
MSContin 15 mg (or preoperative dose)
Q 8-12 hours Use APS/CPS recommended dose
Clonidine(APS consult unless patient taking preoperatively)
0.1 mg patch +/- tablet
Q 7 days Contact APS for any dosing adjustments
Ketamine drip(APS consult required)
0.1-0.3 mg/kg/hr Infusion Contact APS2
Celecoxib3 400 mg PO Once/day After initial dose: 200 mg BID3
1. Acetaminophen: decrease dose or avoid in patients with liver dysfunction.
2. APS will manage ketamine infusions in conjunction with CPS.
3. Single preoperative dose Celecoxib permitted. If celecoxib or ketorolac are needed postop, attending surgeon approval is required.
4. Patients who have been stabilized on anticonvulsants should continue on preoperative dose. Consider increasing dose for inadequate analgesia if patients are having pain and are not overly sedated.
PO Pain Medication Pathways:Patients should remain on all preoperative medications during the
hospitalization unless contraindicated for the surgery.Use fewest number of medications required at lowest doses necessary.
Limit long-acting opioids to 5 days following discharge unless patients are stabilized on them prior to surgery.
Use caution with combining narcotics and sedatives in patients with:
o Obstructive sleep apnea,
o Cognitive dysfunction
o Over 70 years old.
Restrict use
Preferred

IV breakthrough Pain Medications:Drug Dose Frequency Adjustments
Hydromorphone 0.5-1 mg Q 4 hours 0.25 mg patients > 70 years old
Morphine 1-2 mg Q 4 hours 0.5 – 4 mg
Meperidine 25-100 mg PO/IV/IM Q 6 hours APS/CPS only
Anticonvulsant Medications for Pain Management (all PO only):Drug Dose Frequency Adjustments 1) Decrease the dose in renal
insufficiency
2) Decrease the dose in patients > 70 years old.
3) Use caution (avoid) in patients with cognitive dysfunction.
Gabapentin 100-300 mg (naïve) Q 8 hours 300 mg-900 mg Q 8 hr
Pregabalin 75-150 mg Q 12 hours 75-300 mg Q 12 hr
Topiramate 25-50 mg (APS/CPS only unless stabilized on drug)
Q 12 hours 25-200 mg/day
Muscle Relaxants for Pain Management:Drug Dose Frequency Adjustments 1. Increased risk of serotonin syndrome
when used in patients on SSRIs.
2. Initiate with recommendation by APS or CPS only. Continue drug if patient has been stabilized on one of these drugs preoperatively.
With all of these drugs use great cau-tion in patients > 70 years old. They may increase the risk of delirium especially in combination with other medications.
If patient is stabilized on regimen, please consider modifying dose rather than add-ing another drug in the same class.
Diazepam 5 mg PO BID-QID prn 10 mg BID-QID
Lorazepam 0.5-1 mg PO BID-TID prn 2 mg BID-TID
Flexeril1 (cyclo-benzaprine)
5 mg PO Q 8 hours 10 mg Q 8 hours
Skelaxin (metaxalone)
800 mg PO(APS/CPS only2)
Q 8 hours 800 mg Q 6 hours
Robaxin (methocarba-mol)
500 mg PO(APS/CPS only2)
Q 4 hours 1000 mg Q 6 hours, 1500 mg Q 8 hours x 48 hours
Baclofen PO 5 mg PO(APS/CPS only2)
Q 8 hours 10-15 mg Q 8 hours
Baclofen pump Consult CPS for interrogation preop and postop
α-2 adrenergic agonists: Drug Dose Frequency Adjustments These drugs should be initiated by APS
or CPS only.
If patients are taking these preoperatively, do NOT discontinue abruptly.
Avoid in patients > 70 years old unless stabilized on regimen.
Clonidine 0.1 mg PO Q 12 hr 0.2 mg Q 12 hrs over several days
Clonidine transdermal 0.1 mg patch Q 7 days none
Tizanidine 2-4 mg PO Q 8 hours 4 mg Q 8 hrs after several days
Morphine Equivalents (in mg/day):Drug IV PO Methadone and buprenorphine equivalents are controversial.
Do not make adjustments without consulting CPS or APS.
Consult CPS for patients on Methadone, Suboxone, Subutex, buprenorphine, Naltrexone IM or for any patient taking greater than 60 mg morphine equivalents per day for greater than 2 weeks.
Morphine Sulfate 20 mg 60 mg
Oxycodone n/a 40 mg
Hydromorphone 4 mg 20 mg
Oxycontin n/a 40mg
MSContin n/a 60 mg
Fentanyl patch 25 mcg/hr n/a
Oxymorphone n/a 40-50 mg
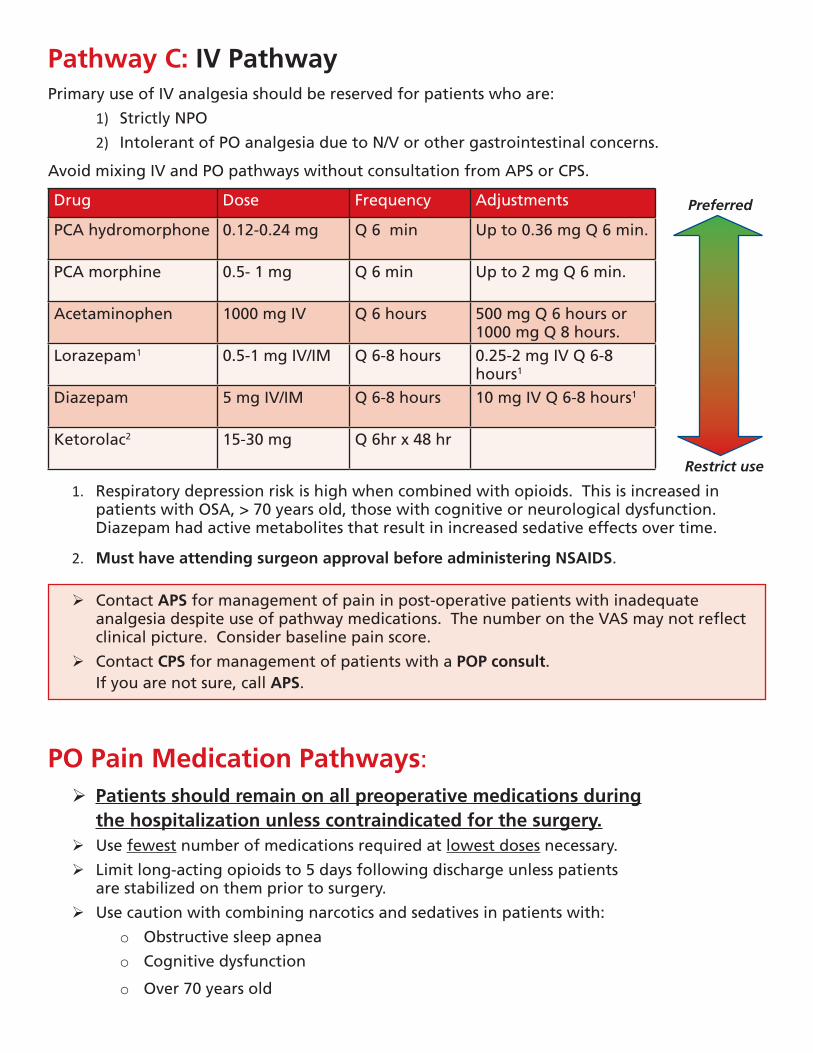
Pathway C: IV PathwayPrimary use of IV analgesia should be reserved for patients who are:
1) Strictly NPO
2) Intolerant of PO analgesia due to N/V or other gastrointestinal concerns.
Avoid mixing IV and PO pathways without consultation from APS or CPS.
Drug Dose Frequency Adjustments
PCA hydromorphone 0.12-0.24 mg Q 6 min Up to 0.36 mg Q 6 min.
PCA morphine 0.5- 1 mg Q 6 min Up to 2 mg Q 6 min.
Acetaminophen 1000 mg IV Q 6 hours 500 mg Q 6 hours or 1000 mg Q 8 hours.
Lorazepam1 0.5-1 mg IV/IM Q 6-8 hours 0.25-2 mg IV Q 6-8 hours1
Diazepam 5 mg IV/IM Q 6-8 hours 10 mg IV Q 6-8 hours1
Ketorolac2 15-30 mg Q 6hr x 48 hr
1. Respiratory depression risk is high when combined with opioids. This is increased in patients with OSA, > 70 years old, those with cognitive or neurological dysfunction. Diazepam had active metabolites that result in increased sedative effects over time.
2. Must have attending surgeon approval before administering NSAIDS.
Contact APS for management of pain in post-operative patients with inadequate analgesia despite use of pathway medications. The number on the VAS may not reflect clinical picture. Consider baseline pain score.
Contact CPS for management of patients with a POP consult. If you are not sure, call APS.
PO Pain Medication Pathways:Patients should remain on all preoperative medications during
the hospitalization unless contraindicated for the surgery.Use fewest number of medications required at lowest doses necessary.
Limit long-acting opioids to 5 days following discharge unless patients are stabilized on them prior to surgery.
Use caution with combining narcotics and sedatives in patients with:
o Obstructive sleep apnea
o Cognitive dysfunction
o Over 70 years old
Restrict use
Preferred

IV breakthrough Pain Medications:Drug Dose Frequency Adjustments
Hydromorphone 0.5-1 mg Q 4 hours 0.25 mg patients > 70 years old
Morphine 1-2 mg Q 4 hours 0.5 – 4 mg
Meperidine 25-100 mg PO/IV/IM Q 6 hours APS/CPS only
Anticonvulsant Medications for Pain Management (all PO only):Drug Dose Frequency Adjustments 1) Decrease the dose in renal
insufficiency
2) Decrease the dose in patients > 70 years old.
3) Use caution (avoid) in patients with cognitive dysfunction.
Gabapentin 100-300 mg (naïve) Q 8 hours 300 mg-900 mg Q 8 hr
Pregabalin 75-150 mg Q 12 hours 75-300 mg Q 12 hr
Topiramate 25-50 mg (APS/CPS only unless stabilized on drug)
Q 12 hours 25-200 mg/day
Muscle Relaxants for Pain Management:Drug Dose Frequency Adjustments 1. Increased risk of serotonin syndrome
when used in patients on SSRIs.
2. Initiate with recommendation by APS or CPS only. Continue drug if patient has been stabilized on one of these drugs preoperatively.
With all of these drugs use great cau-tion in patients > 70 years old. They may increase the risk of delirium especially in combination with other medications.
If patient is stabilized on regimen, please consider modifying dose rather than add-ing another drug in the same class.
Diazepam 5 mg PO BID-QID prn 10 mg BID-QID
Lorazepam 0.5-1 mg PO BID-TID prn 2 mg BID-TID
Flexeril1 (cyclo-benzaprine)
5 mg PO Q 8 hours 10 mg Q 8 hours
Skelaxin (metaxalone)
800 mg PO(APS/CPS only2)
Q 8 hours 800 mg Q 6 hours
Robaxin (methocarba-mol)
500 mg PO(APS/CPS only2)
Q 4 hours 1000 mg Q 6 hours, 1500 mg Q 8 hours x 48 hours
Baclofen PO 5 mg PO(APS/CPS only2)
Q 8 hours 10-15 mg Q 8 hours
Baclofen pump Consult CPS for interrogation preop and postop
α-2 adrenergic agonists: Drug Dose Frequency Adjustments These drugs should be initiated by APS
or CPS only.
If patients are taking these preoperatively, do NOT discontinue abruptly.
Avoid in patients > 70 years old unless stabilized on regimen.
Clonidine 0.1 mg PO Q 12 hr 0.2 mg Q 12 hrs over several days
Clonidine transdermal 0.1 mg patch Q 7 days none
Tizanidine 2-4 mg PO Q 8 hours 4 mg Q 8 hrs after several days
Morphine Equivalents (in mg/day):Drug IV PO Methadone and buprenorphine equivalents are controversial.
Do not make adjustments without consulting CPS or APS.
Consult CPS for patients on Methadone, Suboxone, Subutex, buprenorphine, Naltrexone IM or for any patient taking greater than 60 mg morphine equivalents per day for greater than 2 weeks.
Morphine Sulfate 20 mg 60 mg
Oxycodone n/a 40 mg
Hydromorphone 4 mg 20 mg
Oxycontin n/a 40mg
MSContin n/a 60 mg
Fentanyl patch 25 mcg/hr n/a
Oxymorphone n/a 40-50 mg

Lumbar Fusion Clinical Pathway 2015
What: Clinical Pathway Practice Changes
Who: Lumbar Fusion Patients
Why: Clinical Pathway Education related to Pain Management, Mobility, Patient Education, and Discharge Planning
Goals:
1. Improved Pain Management with Early Utilization of Oral Pain Medications
2. Increase Early Mobilization to Prevent or Decrease Post-Operative Risk Factors. (ie. Ileus, Blood Clots, and Infections)
3. Improve Documentation of Patient Progress related to pain and mobility.
4. Enhanced Continuous Patient Education and Discharge Planning
5. Decrease the Length of Stay in the Patients S/P Lumbar Fusion Generalized Pain Pathway Descriptions:
A Patients that are Opiate Naive: < 60 mg Morphine Equivalent/day
B Patients that are Opiate Tolerant: > 60 mg Morphine Equivalent/day
C Patients Intolerant of oral medications or strictly NPO
CPS Consult Patients on Methadone, Suboxone, Subutex, Buprenorphine, and Naltrexone IM or for any patient taking > 60 mg morphine equivalents/day for > 2 weeks
Important Practice Changes for the Lumbar Fusion Pathway
Documentation Clinical Pathway in Patient’s Chart
Actual designation of a Pain Pathway A, B, C, or CPS Consult
Use of pre-op oral pain medications: Gabapentin, Tylenol, Oxycontin/MS Contin
No use of PCA’s post-op: Utilizing oral pain medications immediately post op, along with IV pain medications for breakthrough pain instead of PCA:
• Overview of doses
• “OK” to use full dose
• Explain adjustment options
Strict Q4H pain check-ins
• Important to stay ahead of the pain
• Set appropriate expectations with the patient (language?)
• Wake patients at night
If a brace is indicated, use of prefabricated braces are issued to patients by POD 0/POD 1. (Exception of Dr. Glazer’s patients)
Early Mobilization by Nursing. PT Eval and Treatment: POD#2 and POD#4.
Use of standing PO Bowel Medications and addition of SC Methylnaltrexone POD 1
Use of PO Flomax POD #1 in men ages 55 years of age or older
Starting SC Heparin POD #1, unless patient is ambulating
Pai
n M
anag
emen
t
Bracing
Activity
Other
STANDARDIZED PATHWAY VALUE Better Pain Management Increased Mobility, Decreased Risk Factors

Lumbar Fusion Pain Pathway
Epidural?
Tolerates PO?
Patient taking < 60 mg
morphine/day
Suboxone, subutex,
Naltrexone?
Patient taking> 60 mg
morphine/day
Pathway “B”Opioid tolerant
CPS/POP Consultrequired
Follow CPS plan
Pathway “A”Opioid Naive
Pathway “C”IV pathway (least preferred) Patient
should be changed to PO ASAP
Consult APS 37246
(3PAIN)
Is this aCPS patient?
Is thereadequate
analgesia?
Contact CPS
3OUCH36824
Prepare discharge plan including:1) Weaning from opioids2) PRN-(or) as needed
Excludes Dr. Glazerpatients
Lumbar Fusion Pain Pathway
Yes
Yes
Yes
Yes
No
No
No
Yes
No
No
Yes
YesNo
Yes
No
Yes
Generalized Pain Pathway Descriptions:
A Patients that are Opiate Naive: < 60 mg Morphine Equivalent/day
B Patients that are Opiate Tolerant: > 60 mg Morphine Equivalent/day
C Patients Intolerant of oral medications or strictly NPO
CPS Consult Patients on Methadone, Suboxone, Subutex, Buprenorphine, and Naltrexone IM or for any patient taking > 60 mg morphine equivalents/day for > 2 weeks