recurring immune response - rx study guidesphar 504 exam iv lecture review (11/10) orjala lecture:...
TRANSCRIPT
PHAR 504 EXAM IV Lecture Review (11/10) Orjala Lecture: Medicinal Chemistry of Inflammatory Bowel Disease- Medications and Antihistamines Inflammatory Bowel Disease (IBD): Chronic inflammatory condition of the GI tract resulting from a recurring immune response that produces inflammation ± ulceration. The most common forms are Crohn’s Disease and Ulcerative Colitis. General symptoms of an IBD patient include D, Rectal blood loss, abdominal pain, and weight loss.
- Treatment Goals: (1) Induce Remission (2) Prevent flare-ups - Disease States: Crohn’s Disease, Ulcerative Colitis - Treatment options include: Aminosalicylates, Glucocorticoids, Immunomodulators, Antibiotics, Biologics
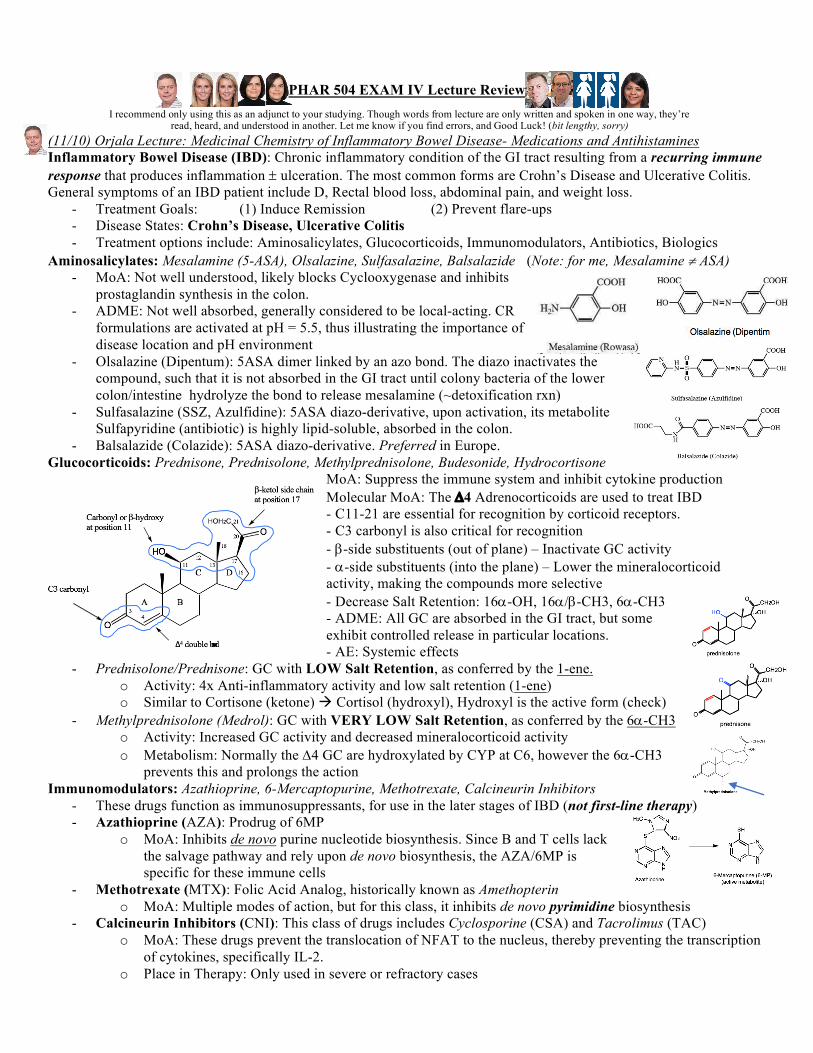
Aminosalicylates: Mesalamine (5-ASA), Olsalazine, Sulfasalazine, Balsalazide (Note: for me, Mesalamine ¹ ASA) - MoA: Not well understood, likely blocks Cyclooxygenase and inhibits
prostaglandin synthesis in the colon. - ADME: Not well absorbed, generally considered to be local-acting. CR
formulations are activated at pH = 5.5, thus illustrating the importance of disease location and pH environment
- Olsalazine (Dipentum): 5ASA dimer linked by an azo bond. The diazo inactivates the compound, such that it is not absorbed in the GI tract until colony bacteria of the lower colon/intestine hydrolyze the bond to release mesalamine (~detoxification rxn)
- Sulfasalazine (SSZ, Azulfidine): 5ASA diazo-derivative, upon activation, its metabolite Sulfapyridine (antibiotic) is highly lipid-soluble, absorbed in the colon.
- Balsalazide (Colazide): 5ASA diazo-derivative. Preferred in Europe. Glucocorticoids: Prednisone, Prednisolone, Methylprednisolone, Budesonide, Hydrocortisone
MoA: Suppress the immune system and inhibit cytokine production Molecular MoA: The D4 Adrenocorticoids are used to treat IBD - C11-21 are essential for recognition by corticoid receptors. - C3 carbonyl is also critical for recognition - b-side substituents (out of plane) – Inactivate GC activity - a-side substituents (into the plane) – Lower the mineralocorticoid activity, making the compounds more selective - Decrease Salt Retention: 16a-OH, 16a/b-CH3, 6a-CH3 - ADME: All GC are absorbed in the GI tract, but some exhibit controlled release in particular locations. - AE: Systemic effects
- Prednisolone/Prednisone: GC with LOW Salt Retention, as conferred by the 1-ene. o Activity: 4x Anti-inflammatory activity and low salt retention (1-ene) o Similar to Cortisone (ketone) à Cortisol (hydroxyl), Hydroxyl is the active form (check)
- Methylprednisolone (Medrol): GC with VERY LOW Salt Retention, as conferred by the 6a-CH3 o Activity: Increased GC activity and decreased mineralocorticoid activity o Metabolism: Normally the D4 GC are hydroxylated by CYP at C6, however the 6a-CH3
prevents this and prolongs the action Immunomodulators: Azathioprine, 6-Mercaptopurine, Methotrexate, Calcineurin Inhibitors
- These drugs function as immunosuppressants, for use in the later stages of IBD (not first-line therapy) - Azathioprine (AZA): Prodrug of 6MP
o MoA: Inhibits de novo purine nucleotide biosynthesis. Since B and T cells lack the salvage pathway and rely upon de novo biosynthesis, the AZA/6MP is specific for these immune cells
- Methotrexate (MTX): Folic Acid Analog, historically known as Amethopterin o MoA: Multiple modes of action, but for this class, it inhibits de novo pyrimidine biosynthesis
- Calcineurin Inhibitors (CNI): This class of drugs includes Cyclosporine (CSA) and Tacrolimus (TAC) o MoA: These drugs prevent the translocation of NFAT to the nucleus, thereby preventing the transcription
of cytokines, specifically IL-2. o Place in Therapy: Only used in severe or refractory cases
I recommend only using this as an adjunct to your studying. Though words from lecture are only written and spoken in one way, they’re read, heard, and understood in another. Let me know if you find errors, and Good Luck! (bit lengthy, sorry)

Biological Agents: Monoclonal antibodies targeting components of the immune system (discussed later by Federle) - TNFa: Critical multifunctional pro-inflammatory cytokine. Anti-TNF mAb target TNFa in the bloodstream
o mAb: Infliximab (Remicade), Adalimumab (Humira), Certolizumab (Cimzia), Golimumab (Simponi) - Integrin a4: Cell-adhesion protein essential for the egress of Leukocytes out of the bloodstream and into the gut.
o mAb: Natalizumab (Tysabri), Vedolizumab (Entyvio). Slow leukocyte migration, lower inflammation Investigational Agents
- TNFa is a major drug target for the treatment of patients with IBD. Currently, xanthine-related compounds are being investigated, and some others – reinvestigated. Thalidomide, Pentoxifylline.
- Thalidomide: Originally an antiemetic agent used in treating morning sickness of pregnant women, this drug was previously discontinued due to teratogenic effects. However, it is now being used for its potent effects in inhibiting the biosynthesis of TNFa as well as increasing the rate of TNFa mRNA degradation
- Pentoxifylline: Prodrug, its keto is reduced to the active hydroxyl (Lisofylline). It downregulates TNFa production at the protein AND mRNA levels, though its TNFa inhibition is lower than thalidomide’s.
Antihistamines: 4 Histamine receptors have been identified, each with unique binding affinities to the histamine analogues. Antihistamines are drugs that antagonize the action of histamine at the H1 receptor. There are two general classes of antihistamines: First generation (sedating), and second generation (non-sedating)
- H1 Antagonists: C2 specific, Used to treat allergies, allergic rhinitis
- H2 Antagonists: C4 specific, Used to inhibit gastric acid secretion
- H3 Antagonists: aC-Amine, receptors located in the CNS, generally not targeted.
- H4 Antagonists: Receptors localize on cells of hematopoietic origin
- H1 Receptor Antagonists: Classically known as the Antihistamines o Structure: Tertiary Amine, 2 Aromatic Rings (AR) o Molecular MoA:
§ Amine binds in the Anionic Binding site § The 2 Aromatics bind in different hydrophobic pockets
o S-A-R: The structure-activity relationships of our AR and subs § AR1 Ortho-meta subs: Decrease H1 antagonistic activity § AR1 Para subs: Increase H1 antagonistic activity, AND
decreases the anticholinergic AE! NICE! § Para subs on both AR1+2 decrease H1 antagonistic
activity § AR2: Should not have subs. But, the entire AR2 can be substituted for a Heteroaromatic ring
• Heteroaromatic rings have higher affinity for H1 receptor § 4 Carbons between Amine N and the 2 Aromatics. Significance – (need to update)
o First Generation: Lipophilic (penetrate the BBB – CNS sedation), + some anticholinergic AE § Alkylamines: Brompheniramine, Dexbrompheniramine, Chlorpheniramine § Ethanolamines: Diphenhydramine (DPH), Clemastine
o Second Generation: These drugs do not penetrate the BBB, and have little to no anticholinergic AE § First Products: Terfenadine and Astemizole. Rapidly metabolized by CYP3A4
• 3A4 substrates (Ketoconazole/Clarithromycin) increase their plasma concentration, and may give rise to cardiac toxicity/arrhythmias via (hERG inhibition).
• hERG: Potassium channel in the heart. At high concentrations, some drugs will interact with hERG, blocking potassium influx à Arrhythmias. As a result, hERG counterscreens are part of EVERY NDA during drug development. Frequently found in peristaltic drugs
§ Fexofenadine (Allegra): Potent, Non-sedating. It is the active metabolite of Terfenadine • Terfenadine --3A4à Fexofenadine. Bypassing CYP carboxylation of terfenadine tert-
butyl greatly lowers hERG affinity avoids CYP elimination (avoid drug-drug interaX) • Big Amine Nitrogen group (“big N head”) à No anticholinergic effects
§ Cetirizine (Zyrtec): Potent, Very low Sedation. Oxidized active metabolite of Hydroxyzine • Metabolism: Mostly eliminated unchanged, less drug-drug interaX
§ Levocetirizine (Xyzal): Levorotary enantiomer of cetirizine, patent $cam § Loratadine (Claritin): Tricyclic ring system. Metabolized by 3A4 to
Desloratadine. No hERG § Desloratadine (Clarinex): Mostly excreted unchanged, some
hydroxylation on heteroaromatic