recruitment & retention survey finds or nurse staffing asc
TRANSCRIPT

September 2003 Vol 19, No 9
The monthly publication for OR decision makers
In this issueJOINT COMMISSION.JCAHO adds goal on reducing infection . . . . . . . . . . . . . . . . . . . . . . . .5
JOINT COMMISSION.JCAHO National Patient SafetyGoals . . . . . . . . . . . . . . . . . . . . . . . . . .7
JOINT COMMISSION.Deadline is July 1, 2004, to comply with wrong-site surgery protocol . . . . . . . . . . . . . . . . .8
RECRUITMENT & RETENTION.Lack of anesthesia coverage closes ORs . . . . . . . . . . . . . . . . . . . . .15
RECRUITMENT & RETENTION.Bonuses not as lavish . . . . . . . . . . .16
RECRUITMENT & RETENTION.ASCs less likely to hire RNs without OR experience . . . . . . . . . .20
Hospitals to get bonuses in newMedicare demo . . . . . . . . . . . . . . . . .29
TECHNOLOGY IN SURGERY.Is it time to add a robot to your team? . . . . . . . . . . . . . . . . . . . .30
WORKPLACE . . . . . . . . . . . . . . . . .32
AMBULATORY SURGERY.Setting boundaries for vendors in OR . . . . . . . . . . . . . . . . . . . . . . . . .34
ASC STRATEGIES & TACTICS.Make clear rules on block scheduling . . . . . . . . . . . . . . . . . . . . .40
IN BUSINESS NEWS . . . . . . . . . . . .42
AT A GLANCE . . . . . . . . . . . . . . . . .44
ASC section on page 34.
Staffing in operating rooms seems tobe holding its own despite wide-spread worries about the nursing
shortage.Only 4% of ORs have closed rooms
for more than 1 week because of a short-age of OR nurses, according to a recentOR Manager survey.
Anesthesia coverage is more of aproblem. More ORs�20%�had shutdown rooms because they did not haveenough anesthesia providers.
The anesthesia shortage is likely to befelt at least through 2005, experts say.
The turnover rate for OR nursingpersonnel has improved slightly, as hasthe vacancy rate and weeks positionshave been open. Use of contract staff is
on a par with last year.Turnover and vacancy rates in the
OR continue to be lower than the nation-al averages for all RNs.
Though the staffing situation insurgery appears relatively stable, thevast majority of surgical services man-agers�87%�say recruiting experiencedOR nurses has gotten more difficult inthe past year.
To cope with staffing challenges,managers continue their strategy of hir-ing RNs without surgical experience andproviding the preparation themselves.
The results are from OR Manager�s2003 Salary/Career Survey. Findings onthe staffing portion of the survey are
Survey finds OR nurse staffingholds up in face of shortages
After years of product conver-sions and restricted choices,clinicians may be regaining
more say in supply purchasing.Group purchasing organizations
(GPOs), under scrutiny from Congressand government agencies, are movingaway from such controversial practicesas bundled contracts and sole sourceagreements.
They are also revamping their poli-cies on commitment levels, contractterms, and vendor fees, among otherissues.
The GPO changes should give nurs-es and physicians a wider choice ofproducts. It should also give them ear-lier access to innovative technology
from smaller companies. GPOs have been reforming their
contracting practices since they werecalled before Congress last year after aseries of articles in the New York Times.The articles questioned whether GPOs�
close financial ties with suppliers jeop-ardize their main mission of providinghospitals with the best products at thebest price.
In July, GPOs and some of their crit-ics came back before the Senate�santitrust subcommittee to give anupdate. Both Premier Inc andNovation, the two biggest GPOs, say t
OR nurses, physicians regain buyingclout as GPOs reform purchasing
Supply chain
Continued on page 26
Recruitment & retention
Continued on page 11
ManagingToday’s OR Suite
Conference issue
Sept 17 to 19San Diego
2
Full Page Ad
2
Please see the ad for MEDLINE INDUSTRIESin the OR Manager print version.

So you think perioperative nursingstaff are difficult to recruit? Try sur-geons and anesthesiologists.
Surgical suites are facing a demo-graphic tidal wave of patients in the next10 to 20 years that could leave themscrambling for professionals on all threecategories.
We�ve known about the nursingshortage for a while.
At the moment, despite the generalRN shortage, OR nurse staffing seemsto be relatively stable, judging byresults on staffing from the 2003 ORManager annual Salary/Career Surveyreported in this issue.
But the pinch caused by a lack ofanesthesia providers is already being felt.
Our survey found 20% of respondentshave had to close ORs for more than 1week because they did not have enoughanesthesia providers. That is far morethan the 4% who closed rooms becauseof a lack of OR nurses.
The anesthesiologist supply dipped inthe mid-90s. Though more residencyslots are being filled, the shortfall is pro-jected to continue at least through 2005.
Nurse anesthetists are affected by thesame trends as nursing generally.Though enrollments in nurse anesthesiaprograms have risen lately, it�s not clearit will be enough to offset the falloff asnurses retire in the coming years.
Surgeon shortage forecastThen, as we neared our deadline, we
learned of a new study from UCLA thatforecasts a shortage of surgeons by 2020.
The demand for some specialties willrise by nearly 50% as the over-65 popula-tion surges, according to the researchers,led by David A. Etzioni, MD, a generalsurgeon.
The greatest growth in demand, notsurprisingly, will be in cataract and car-diac surgery, which are primarily per-formed in older adults.
All of this will mean increased com-petition among facilities to attract notonly the best nurses but also the best sur-geons and anesthesia caregivers.
One big challenge will be bringingthis picture into focus for Congress, theWhite House, and state lawmakers. Howis it going to be possible to attract thebest people when physicians alreadyfind Medicare payment rates too low?
And Congress and state houses so farhave made little progress on taming thehigh malpractice premiums that are dri-ving some physicians out of state or outof practice.
On the hospital front, will we see�magnet� programs for physicians likewe�ve seen for nurses?
The magnet program from the Amer-ican Nurses Credentialing Center recog-nizes that the most effective way to attractand retain nurses is to support them asprofessionals and develop an environmentthat promotes excellence in practice.
There will be a lot of discussion in thecoming years about how to make sur-geons and anesthesia personnel the mostproductive.
You already know from experiencewhat is going to be important to them inthe surgical suite:� a well-oiled surgical scheduling sys-
tem that gives the surgeons conve-nient access to OR time without caus-ing big gaps and late-running casesthat create dissatisfaction for bothperioperative nurses and anesthesiapersonnel
� skilled, competent perioperative staffwho can give expert patient care andkeep the surgery schedule flowingsafely and efficiently
� a well-managed central sterile depart-ment that provides complete, well-maintained instrument sets and accu-rately picked supplies
� up-to-date surgical technology � a focus on customer service and team
collaboration.Nothing new here�more challenges
to come.An upside is that hospital administra-
tors will have to place recruitment andretention for all types of health care pro-fessionals at the top of their priority list. ❖
�Pat Patterson
3September 2003
September 2003 Vol 19, No 9OR Manager is a monthly publication forpersonnel in decision-making positions inthe operating room.
Elinor S. Schrader: PublisherPatricia Patterson: EditorJudith M. Mathias, RN, MA:
Clinical editorBillie Fernsebner, RN, MSN:
Consulting editorJanet K. Schultz, RN, MSN:
Consulting editorKathy Shaneberger, RN, MSN, CNOR:
Consulting editorOR Manager (USPS 743-010), (ISSN
8756-8047) is published monthly by ORManager, Inc, 1807 Second St, Suite 61,Santa Fe, NM 87505-3499. Periodicalspostage paid at Santa Fe, NM and addi-tional post offices. POSTMASTER: Sendaddress changes to OR Manager, PO Box5303, Santa Fe, NM 87502-5303.
OR Manager is indexed in the CumulativeIndex to Nursing and Allied HealthLiterature, the Hospital Literature Index, andthe National Library of Medicine�s HealthPlanning and Administration Database.
Copyright © 2003 OR Manager, Inc. All rightsreserved. No part of this publication may bereproduced without written permission.
Subscription rates: $86 per year. Canadian,$98. Foreign, $108. Single issues $10.Address subscription requests to PO Box5303, Santa Fe, NM 87502-5303. Tele:800/442-9918 or 505/982-0510. Web site:www.ormanager.com
Editorial Office: PO Box 5303, Santa Fe, NM87502-5303. Tele: 800/442-9918. Fax: 505/983-0790. E-mail: [email protected]
Advertising Manager: Anthony J. Jannetti,Inc, East Holly Ave/Box 56, Pitman, NJ08071. Telephone: 856/256-2300; Fax:856/589-7463. John R. Schmus, nationaladvertising manager. [email protected]
The monthly publication for OR decision makers
UpcomingAnnual Salary/Career Survey
Is your salary keeping pace? Whatabout your benefits? Read results ofthis year�s survey.
The coming shortage: physiciansWill your OR have enough anesthe-
sia providers and surgeons? A view ofthe trends.
Meeting staffing challengesIs your OR suffering from �gapo-
sis��surgeons want to operate late inthe day but staff want to go home?What strategies can help?
OR Manager Vol 19, No 9
Editorial
“Will we see‘magnet’ programs
for physicians?
“

4
Please see the ad for ADVANCED STERILIZATION PRODUCTSin the OR Manager print version.
One new National Patient SafetyGoal has been added for nextyear�reducing the risk of
health care-acquired infection.The six Patient Safety Goals for 2003
continue next year, for a total of seven. The Joint Commission on Accredi-
tation of Healthcare Organizationsannounced the goals July 21. The goalsare effective for accreditation surveysbeginning Jan 1.
Eliminating wrong surgery contin-ues as a goal. JCAHO has issued a new�universal protocol� for preventingwrong surgery that must be implement-ed by July 1, 2004 (page 8).
The new goal for reducing infectionrisk has two requirements:
� Comply with the current Centers forDisease Control and Prevention(CDC) hand hygiene guidelines.
� Manage as sentinel events all identi-fied cases of unanticipated death or
major permanent loss of functionassociated with a health care-acquired infection.The new goal echoes JCAHO�s sen-
tinel event alert on reducing infectionissued in January. The difference is thatorganizations are scored on compliancewith Patient Safety Goals, while sen-tinel event alerts aren�t scored unlessthey are also a safety goal.
Hand hygiene guidelinesThe CDC�s hand hygiene guidelines,
issued in 2002, recommend more wide-spread use of alcohol-based handrubsas well as gloving and washing hands.
The guidelines include recommen-dations for OR personnel on the surgi-cal scrub as well as fingernails and arti-ficial nails.
The guidelines say the surgical scrubmay be performed either with anantimicrobial soap or alcohol-based ruband spell out requirements for thescrub.
In addition, the CDC strongly rec-ommends against artificial fingernailsand nail extenders for OR personneland others involved in direct patientcare for high-risk patients. Many facili-ties have adopted policies in the pastyear banning artificial nails for directcaregivers.
Natural nails should be less than 1/4inch long. No recommendation is madeon nail polish. Nurses� long and artifi-cial nails have been linked to patientinfections, including deaths of infantsin a neonatal intensive care unit in 1997.
Infections as a patient safetyissue
The second requirement for reduc-ing risk of infection is likely to be morecontroversial. Infection control expertspoint out that health care-acquiredinfections are multifactorial, and it canbe very difficult to determine a rootcause.
There is no question, though, thatinfections are a patient safety issue.
Infections are the most common com-plication in hospital patients. An estimat-ed 2 million patients acquire an infectionin US hospitals each year. Nosocomialinfections add $4.5 billion to health care
JCAHO adds goal on reducing infection
5OR Manager Vol 19, No 9September 2003
Gail Avigne, RN, BA, CNORNurse managerShands Hospital at the University of Florida, Gainesville
Mark E. Bruley, EITVice president of accident & forensicinvestigation, ECRIPlymouth Meeting, Pa
Judith Canfield, RNC, MNA, MBAAssociate administrator of surgical servicesUniversity of Washington MedicalCenter, Seattle, Wash
Michele Chotkowski, RN, MSHADirector, perioperative servicesCentral DuPage Hospital/CentralDuPage HealthWinfield, Ill
DeNene G. Cofield, RN, BSN, CNORDirector of surgical servicesMedical Center EastBirmingham, Ala
Larry Creech, RN, MBA, CDTVice president, perioperative servicesClarian Health SystemIndianapolis, Ind
Cheryl Dendy, RNAdministrative director, AmbulatorySatellites, St John Hospital and MedicalCenter, Detroit
Franklin Dexter, MD, PhDAssociate professorDepartment of AnesthesiaUniversity of Iowa, Iowa City
Aileen Killen, RN, PhD, CNORDirector of nursing, perioperative servicesMemorial Sloan-Kettering Cancer CenterNew York City
Robert V. Rege, MDProfessor and chairmanDepartment of SurgeryUT Southwestern Medical CenterDallas, Tex
Marimargaret Reichert, RN, MAAdministrator, Surgical Care CenterSouthwest General Health CenterMiddleburg Heights, Ohio
Kathy E. Shaneberger, RN, MSN, CNORDirector, perioperative services andortho/neuro service lineMercy General Health PartnersMuskegon, Mich
Shelly Schwedhelm, RN, BSNDirector, perioperative servicesNebraska Health System, Omaha
Sallie Walker, RN, BA, CGRNBaptist Physicians Surgery CenterLexington, Ky
Allen WarrenBusiness manager, surgical servicesMission St Joseph�s HospitalAsheville, NC
Anny Yeung, RN, MPA, CNOR, CNAAAssistant vice president for perioperative services & associate hospital directorSUNY Downstate Medical CenterNew York City
Advisory Board
Joint Commission
Continued on page 7
“Reducing infectionis seen as a patient
safety issue.
“

6
Please see the ad for ENCISION, INCin the OR Manager print version.
7OR Manager Vol 19, No 9September 2003
Joint Commission
costs a year, the CDC estimates. Surgical site infection was the sec-
ond largest category of adverse eventsin the well-known Harvard study pub-lished in 1991. That study is one sourcefor the Institute of Medicine�s 1999 esti-mate that 44,000 to 98,000 patients die ayear in hospitals from medical errors.
Looking for root causesThe CDC�s director, Julie Gerber-
ding, MD, MPH, writing in the Annalsof Internal Medicine (2002;137:665-670),advocates taking a quality improve-ment approach to infection, much likethat for medication errors. She suggest-ed that infection control teams considerconducting a root cause analysis if theysuspect an infection was preventable,even if the patient�s condition was com-plex. They might ask, for example:� Was aseptic technique used in insert-
ing the urinary catheter?
� What was the staffing level? Lowstaffing has been associated withhigher urinary tract infection rates.
� Was the patient a candidate for ananti-infective-coated catheter? Re-search suggests that such catheters,while more costly, can be cost-effec-tive in high-risk patients.If a surgical-site infection was
involved, the surgical team would like-ly participate in the root cause analysis,and questions would be asked aboutOR practices. The team would look forevidence that a prophylactic antibioticwas ordered, if appropriate, and whenthe antibiotic was given. There mightalso be questions about use of cathetersand drains, instrument reprocessing,sterilization parameters, aseptic prac-tice, and OR attire.
Though infection control profession-als, with their training in epidemiology,are skilled in analysis, taking a safetyapproach to infection will require achange in attitude on everyone�s part,notes Patrice Spath, BA, RHIT, whocommented on the subject for an articlein the April OR Manager.
If a patient dies from a nosocomialinfection, the organization will have tobe willing to ask, �Might the patienthave recovered if it hadn�t been for theinfection?�
�If the answer is �yes,� that means
admitting the patient-care process wasflawed in some way,� Spath observed.
As with other patient safety issues,that means overcoming fear and shame.It means being open to looking at infec-tion as the result of larger system prob-lems.
�That will take leadership andcourage,� Spath noted. ❖
The CDC guidelines are at www.cdc.gov/handhygiene. The CDC also has afact sheet, slides, posters, and buttons avail-able.
Continued from page 5
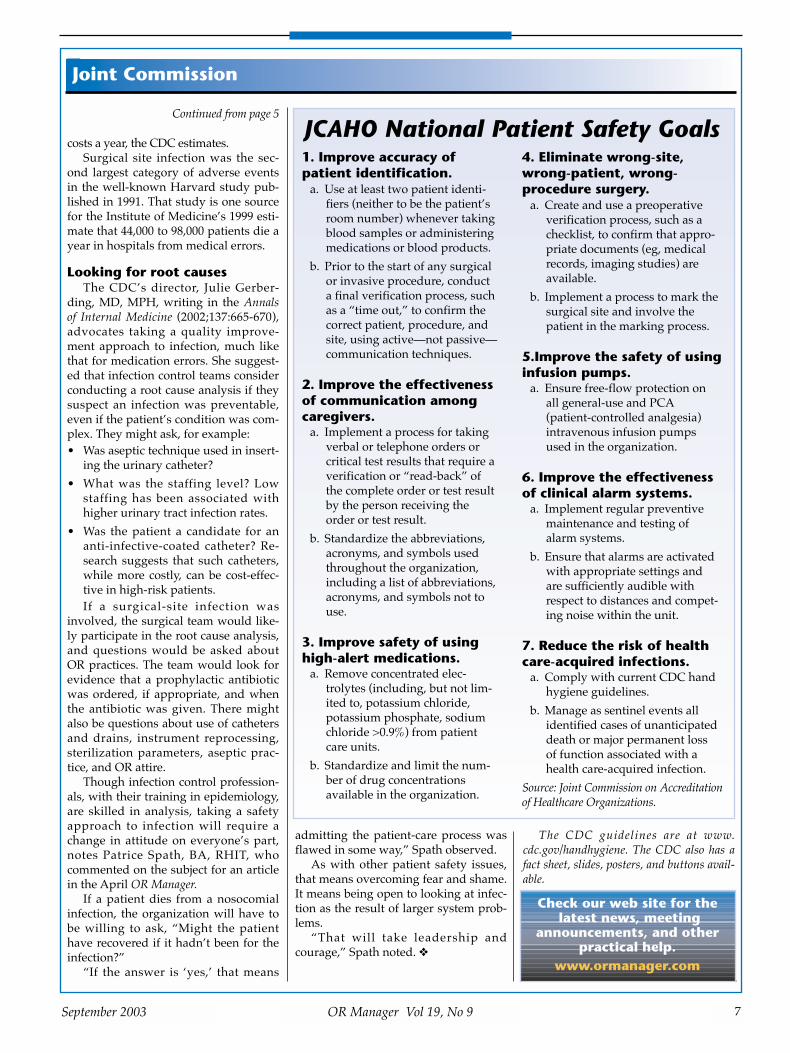
JCAHO National Patient Safety Goals1. Improve accuracy ofpatient identification.
a. Use at least two patient identi-fiers (neither to be the patient�sroom number) whenever takingblood samples or administeringmedications or blood products.
b. Prior to the start of any surgicalor invasive procedure, conducta final verification process, suchas a �time out,� to confirm thecorrect patient, procedure, andsite, using active�not passive�communication techniques.
2. Improve the effectivenessof communication amongcaregivers.
a. Implement a process for takingverbal or telephone orders orcritical test results that require averification or �read-back� ofthe complete order or test resultby the person receiving theorder or test result.
b. Standardize the abbreviations,acronyms, and symbols usedthroughout the organization,including a list of abbreviations,acronyms, and symbols not touse.
3. Improve safety of usinghigh-alert medications.
a. Remove concentrated elec-trolytes (including, but not lim-ited to, potassium chloride,potassium phosphate, sodiumchloride >0.9%) from patientcare units.
b. Standardize and limit the num-ber of drug concentrationsavailable in the organization.
4. Eliminate wrong-site,wrong-patient, wrong-procedure surgery.
a. Create and use a preoperativeverification process, such as achecklist, to confirm that appro-priate documents (eg, medicalrecords, imaging studies) areavailable.
b. Implement a process to mark thesurgical site and involve thepatient in the marking process.
5.Improve the safety of usinginfusion pumps.
a. Ensure free-flow protection onall general-use and PCA(patient-controlled analgesia)intravenous infusion pumpsused in the organization.
6. Improve the effectivenessof clinical alarm systems.
a. Implement regular preventivemaintenance and testing ofalarm systems.
b. Ensure that alarms are activatedwith appropriate settings andare sufficiently audible withrespect to distances and compet-ing noise within the unit.
7. Reduce the risk of healthcare-acquired infections.
a. Comply with current CDC handhygiene guidelines.
b. Manage as sentinel events allidentified cases of unanticipateddeath or major permanent lossof function associated with ahealth care-acquired infection.
Source: Joint Commission on Accreditationof Healthcare Organizations.
Check our web site for thelatest news, meeting
announcements, and otherpractical help.
www.ormanager.com
Beginning July 1, 2004, organiza-tions will have to comply with anew �universal protocol� for pre-
venting wrong surgery. The protocol,approved in July by the Joint Commis-sion on Accreditation of HealthcareOrganizations, is based on consensusreached at a national summit in May.
The protocol is expanded from the2003 National Patient Safety Goal onwrong surgery, which generated ques-tions and controversy on surgical sitemarking. Preventing wrong surgery con-tinues to be a Patient Safety Goal for2004.
The final protocol has only minorchanges from the draft released for com-ment in June. More than 3,000 commentswere submitted, which JCAHO saidwere �overwhelmingly in support� ofthe protocol.
The protocol includes eight principlesand three steps. The three steps are:
1. Preoperative verificationprocess.
Purpose: �To ensure that all of the rel-evant documents and studies are avail-able prior to the start of the procedureand that they have been reviewed andare consistent with each other and withthe patient�s expectations and with theteam�s understanding of the intendedpatient, procedure, and site, and asapplicable, any implants. Missing infor-mation or discrepancies must beaddressed before starting the proce-dure.� [This last sentence was addedafter the draft was issued.]
Process: �An ongoing process ofinformation gathering and verification,beginning with the determination to dothe procedure, continuing through allsettings and interventions involved inthe preoperative preparation of thepatient, up to and including the �timeout� just before the start of the proce-dure.�
2. Marking the operative site.Purpose: �To identify unambiguously
the intended site of incision or insertion.�Process: �For procedures involving
right/left distinction, multiple structures(such as fingers and toes), or multiplelevels (as in spinal procedures), the
intended site should be marked such thatthe mark will be visible after the patienthas been prepped and draped.�
3. “Time out” immediatelybefore starting the procedure.
Purpose: �To conduct a final verifica-tion of the correct patient, procedure,site, and as applicable, implants.�
Process: �Active communicationamong all members of the surgical/pro-cedure team, consistently initiated by adesignated member of the team, con-ducted in a �fail-safe� mode, ie, the proce-dure is not started until any questions orconcerns are resolved.�
Guidelines spell out detailsThe protocol is accompanied by
guidelines with details for implementingthe steps. JCAHO says it expects compli-ance with the guidelines as well as theprotocol.
The guidelines, in addition to outlin-ing specifically what is expected for sitemarking, list exemptions that respond toa flurry of questions from physicians andnurses around the country. Exemptionsfrom site marking include:� single-organ cases (eg, cesarean sec-
tion, cardiac surgery)
� interventional cases for which thecatheter/instrument insertion site isnot predetermined (eg, cardiaccatheterization)
� teeth�but indicate operative toothname(s) on documentation or markthe operative tooth (teeth) on the den-tal radiograph or dental diagram.
� premature infants, for whom themark may cause a permanent tattoo.Clarifying another issue that has
raised questions, the guidelines say:�The person performing the procedureshould do the site marking.� TheNational Patient Safety Goal was silenton who should mark the site.
Despite all the attention focused onpreventing this type of error, JCAHOsays it continues to receive five to eightnew reports of wrong-site surgery amonth. ❖
Information on the protocol is atwww.jcaho.org
8 OR Manager Vol 19, No 9 September 2003
Joint Commission
Deadline is July 1, 2004, to complywith wrong-site surgery protocol
Call for abstracts:Share yoursuccesses
Have you developed new pro-grams to retain perioperativestaff or led a successful cost-
management effort? Perhaps you have found creative
ways to foster leadership in your staff ordevelop a culture of patient safety.
Or perhaps you�ve heard a dynamicspeaker you think your colleagues wouldbenefit from hearing.
Share your ideas and successes withthe planning committee for the 2004Managing Today�s OR Suite conference.The committee is inviting proposals forthe conference, which will be held Oct 6to 8, 2004, at the Hyatt Regency Chicago.
Send a proposal of about 500 wordsdescribing the session you wish to present.
Provide enough information to givethe committee a good understanding ofthe content.
Sessions are 1 1/2 hours long andfocus on practical topics related to man-agement of surgical services, such asachieving greater efficiency, managementof information, leading and developingstaff, and keeping costs under control.
The keynote address and general ses-sions feature nationally known speakerswho have important messages for surgicalservices directors. If you wish to suggest ageneral session speaker, please obtain asmuch information about the person as youcan, such as the speaker�s title, organiza-tion, address, and phone number.
The deadline for proposals and sug-gestions is Nov 1.
OR Business ManagementConference
Proposals are also invited for the fifthannual OR Business ManagementConference to be held May 12 to 14, 2004,at the Hyatt Regency Downtown inAlbuquerque, NM.
Covered are topics such as financialmanagement, materials and technologymanagement, automation, and ORdesign and construction. ❖
Please fax or e-mail proposals by Nov 1 toBillie Fernsebner, RN, MSN, education spe-cialist, OR Manager, Inc, at 303/442-5960 [email protected]
If you have questions, call her at 303/442-1661.

9
Please see the ad for KARL STORZ ENDOSCOPY-AMERICA
in the OR Manager print version.

10
Please see the ad for INTEGRATED MEDICAL SYSTEMSin the OR Manager print version.
reported in this issue. This is the thirdyear the staffing questions have beenasked. The rest of the survey results willbe in the October issue.
The survey was mailed in May to1,197 OR Manager subscribers with man-agement titles in hospitals, with a returnrate of 37%. The survey has a 95% confi-dence level with a margin of error of4.75%. A separate survey was conductedfor ambulatory surgery centers.
Closing ORs, canceling surgeryClosing ORs because of a lack of anes-
thesia coverage is more of an issue forteaching institutions than communityhospitals. In all, 28% of teaching hospi-tals closed ORs for more than 1 weekcompared with 19% of community facili-ties. The larger ORs are more likely tohave had an anesthesia shortage thanmedium-sized or small ORs. This is thefirst year the survey asked about anes-thesia coverage.
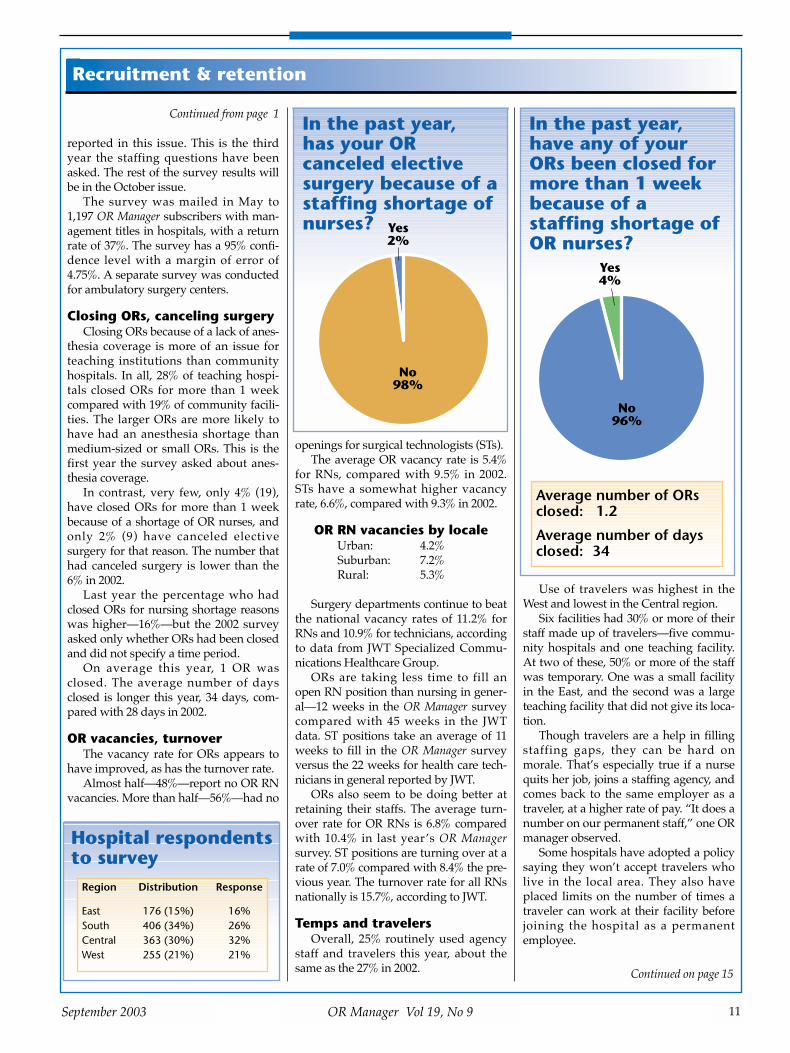
In contrast, very few, only 4% (19),have closed ORs for more than 1 weekbecause of a shortage of OR nurses, andonly 2% (9) have canceled electivesurgery for that reason. The number thathad canceled surgery is lower than the6% in 2002.
Last year the percentage who hadclosed ORs for nursing shortage reasonswas higher�16%�but the 2002 surveyasked only whether ORs had been closedand did not specify a time period.
On average this year, 1 OR wasclosed. The average number of daysclosed is longer this year, 34 days, com-pared with 28 days in 2002.
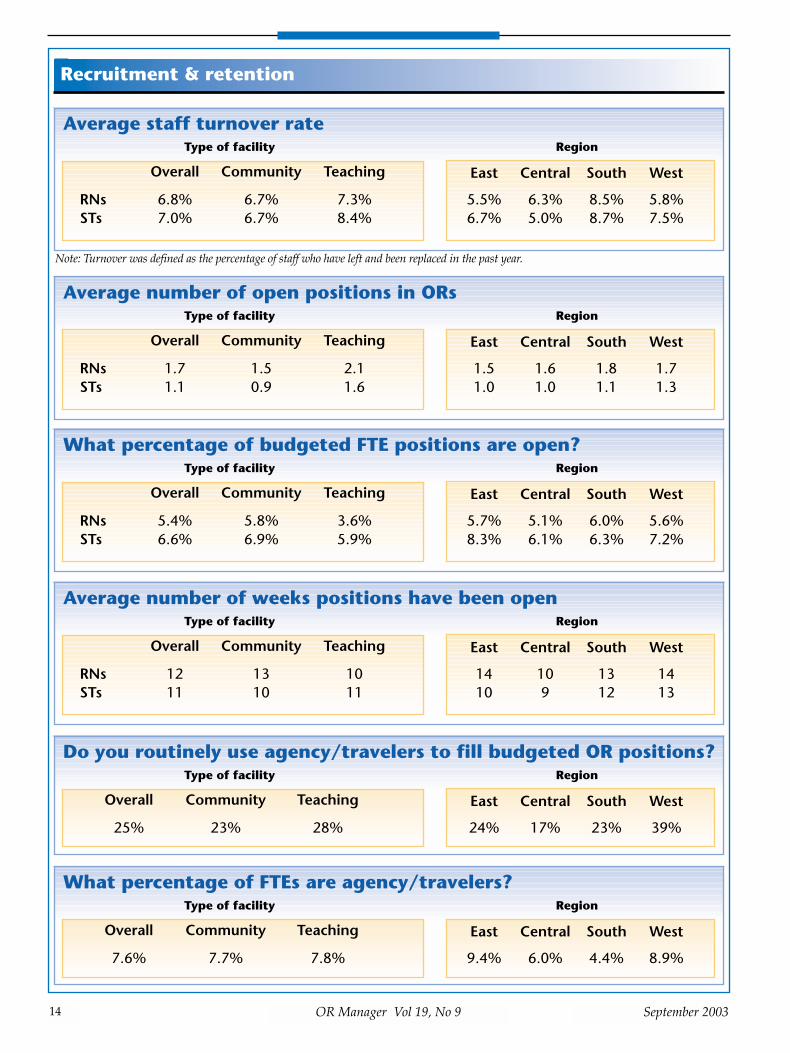
OR vacancies, turnoverThe vacancy rate for ORs appears to
have improved, as has the turnover rate. Almost half�48%�report no OR RN
vacancies. More than half�56%�had no
openings for surgical technologists (STs).The average OR vacancy rate is 5.4%
for RNs, compared with 9.5% in 2002.STs have a somewhat higher vacancyrate, 6.6%, compared with 9.3% in 2002.
OR RN vacancies by localeUrban: 4.2%Suburban: 7.2% Rural: 5.3%
Surgery departments continue to beatthe national vacancy rates of 11.2% forRNs and 10.9% for technicians, accordingto data from JWT Specialized Commu-nications Healthcare Group.
ORs are taking less time to fill anopen RN position than nursing in gener-al�12 weeks in the OR Manager surveycompared with 45 weeks in the JWTdata. ST positions take an average of 11weeks to fill in the OR Manager surveyversus the 22 weeks for health care tech-nicians in general reported by JWT.
ORs also seem to be doing better atretaining their staffs. The average turn-over rate for OR RNs is 6.8% comparedwith 10.4% in last year�s OR Managersurvey. ST positions are turning over at arate of 7.0% compared with 8.4% the pre-vious year. The turnover rate for all RNsnationally is 15.7%, according to JWT.
Temps and travelers Overall, 25% routinely used agency
staff and travelers this year, about thesame as the 27% in 2002.
Use of travelers was highest in theWest and lowest in the Central region.
Six facilities had 30% or more of theirstaff made up of travelers�five commu-nity hospitals and one teaching facility.At two of these, 50% or more of the staffwas temporary. One was a small facilityin the East, and the second was a largeteaching facility that did not give its loca-tion.
Though travelers are a help in fillingstaffing gaps, they can be hard onmorale. That�s especially true if a nursequits her job, joins a staffing agency, andcomes back to the same employer as atraveler, at a higher rate of pay. �It does anumber on our permanent staff,� one ORmanager observed.
Some hospitals have adopted a policysaying they won�t accept travelers wholive in the local area. They also haveplaced limits on the number of times atraveler can work at their facility beforejoining the hospital as a permanentemployee.
11OR Manager Vol 19, No 9September 2003
Recruitment & retention
Continued from page 1
Continued on page 15
Hospital respondentsto survey
Region Distribution Response
East 176 (15%) 16%South 406 (34%) 26%Central 363 (30%) 32%West 255 (21%) 21%
In the past year, has your ORcanceled electivesurgery because of astaffing shortage ofnurses? Yes
2%
No 98%
In the past year,have any of yourORs been closed formore than 1 weekbecause of astaffing shortage ofOR nurses?
Yes 4%
No 96%
Average number of ORsclosed: 1.2
Average number of daysclosed: 34

12
Please see the ad for MOLNLYCKE HEALTH CARE INCin the OR Manager print version.

13
Please see the ad for MOLNLYCKE HEALTH CARE INC
in the OR Manager print version.
14 OR Manager Vol 19, No 9 September 2003
Recruitment & retention
Average staff turnover rateType of facility Region
Overall Community Teaching
RNs 6.8% 6.7% 7.3%STs 7.0% 6.7% 8.4%
East Central South West
5.5% 6.3% 8.5% 5.8%6.7% 5.0% 8.7% 7.5%
Average number of open positions in ORsType of facility Region
Overall Community Teaching
RNs 1.7 1.5 2.1STs 1.1 0.9 1.6
East Central South West
1.5 1.6 1.8 1.71.0 1.0 1.1 1.3
What percentage of budgeted FTE positions are open?Type of facility Region
Overall Community Teaching
RNs 5.4% 5.8% 3.6%STs 6.6% 6.9% 5.9%
East Central South West
5.7% 5.1% 6.0% 5.6%8.3% 6.1% 6.3% 7.2%
Average number of weeks positions have been openType of facility Region
Overall Community Teaching
RNs 12 13 10STs 11 10 11
East Central South West
14 10 13 1410 9 12 13
Do you routinely use agency/travelers to fill budgeted OR positions?Type of facility Region
Overall Community Teaching
25% 23% 28%
East Central South West
24% 17% 23% 39%
Note: Turnover was defined as the percentage of staff who have left and been replaced in the past year.
What percentage of FTEs are agency/travelers?Type of facility Region
Overall Community Teaching
7.6% 7.7% 7.8%
East Central South West
9.4% 6.0% 4.4% 8.9%
15OR Manager Vol 19, No 9September 2003
Recruiting still toughThough vacancy and turnover rates
may have stabilized, recruiting experi-enced OR nurses isn�t getting any easier.
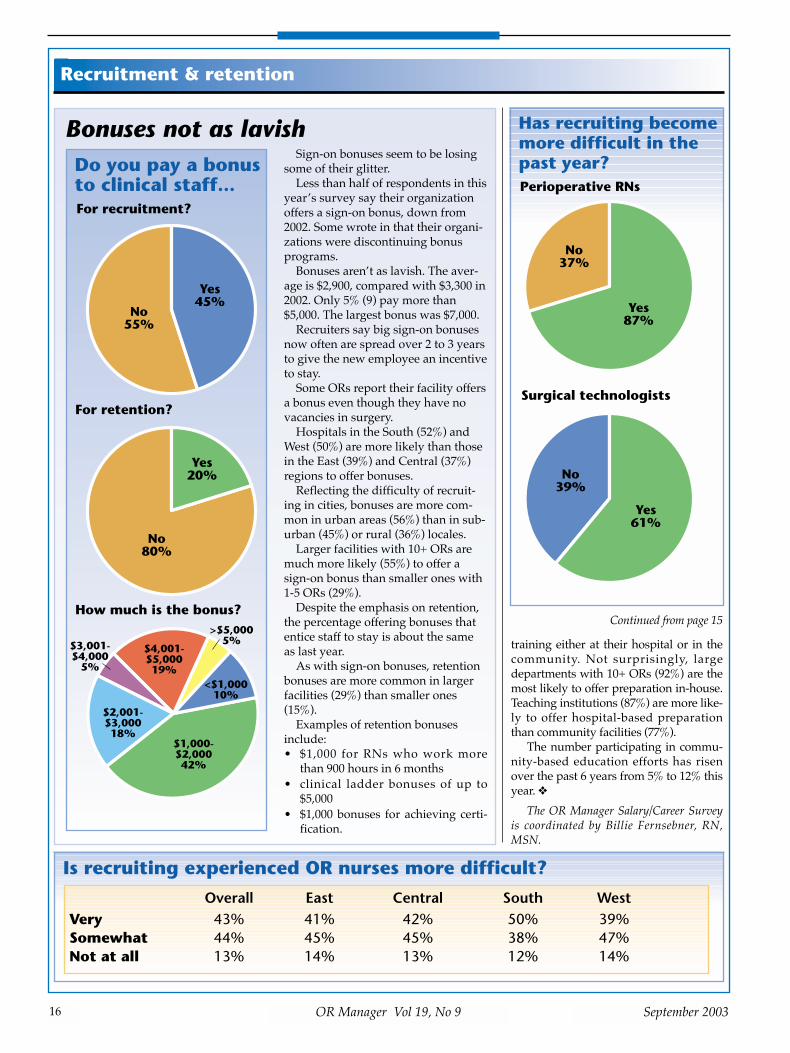
The 87% who say recruiting RNs hasbecome more difficult in the past year isup from 71% in 2002. For STs, 61% sayrecruiting is more difficult, about thesame as last year.
Small ORs (1-5 rooms) and those inrural areas are more likely to say recruit-ing is very difficult. Attracting staffseems to be more difficult for communityhospitals than teaching institutions.
Hiring without experienceMost surgical services managers
accept the fact that experienced OR RNsare scarce. Most nursing schools haven�tprepared RNs for the operating room ina generation.
The overwhelming majority of respon-dents�89%�say they hire RNs withoutexperience in the OR, a number littlechanged since 2000. Still, a minority con-tinues to require experience in surgery:
Never hire RNs without ORexperience
East: 10%Central: 6%South: 13%West: 18%
10+ ORs: 7%6-9 ORs: 12%1-5 ORs: 16%
To compensate for the lack of OR-experienced RNs, managers typicallyhire nurses from other clinical areas andprovide their own OR preparation.Similar to last year, 88% provide OR
Recruitment & retention
Nursing shortage:The national picture
RNs TechniciansVacancy rates 11.2% 10.9%Turnover rates 15.7% 28.4%Days to fillpositions 45 days 22 days
Lack of anesthesia coverage closes ORs
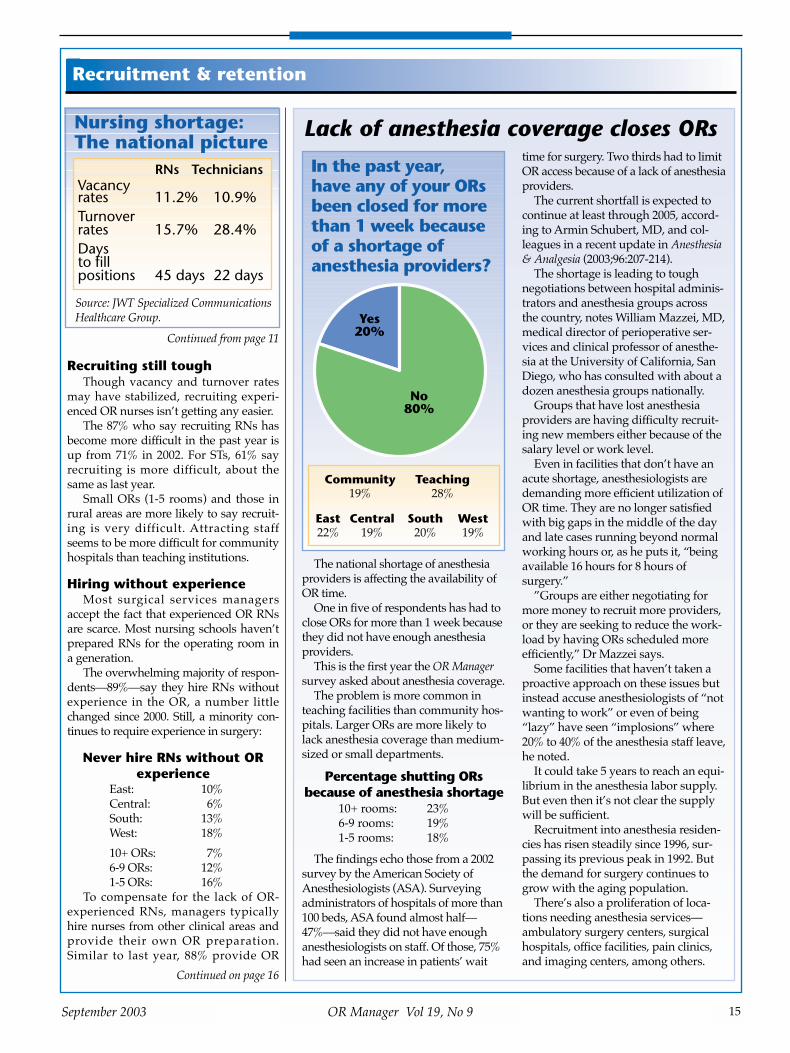
The national shortage of anesthesiaproviders is affecting the availability ofOR time.
One in five of respondents has had toclose ORs for more than 1 week becausethey did not have enough anesthesiaproviders.
This is the first year the OR Managersurvey asked about anesthesia coverage.
The problem is more common inteaching facilities than community hos-pitals. Larger ORs are more likely tolack anesthesia coverage than medium-sized or small departments.
Percentage shutting ORsbecause of anesthesia shortage
10+ rooms: 23%6-9 rooms: 19%1-5 rooms: 18%
The findings echo those from a 2002survey by the American Society ofAnesthesiologists (ASA). Surveyingadministrators of hospitals of more than100 beds, ASA found almost half�47%�said they did not have enoughanesthesiologists on staff. Of those, 75%had seen an increase in patients� wait
time for surgery. Two thirds had to limitOR access because of a lack of anesthesiaproviders.
The current shortfall is expected tocontinue at least through 2005, accord-ing to Armin Schubert, MD, and col-leagues in a recent update in Anesthesia& Analgesia (2003;96:207-214).
The shortage is leading to toughnegotiations between hospital adminis-trators and anesthesia groups acrossthe country, notes William Mazzei, MD,medical director of perioperative ser-vices and clinical professor of anesthe-sia at the University of California, SanDiego, who has consulted with about adozen anesthesia groups nationally.
Groups that have lost anesthesiaproviders are having difficulty recruit-ing new members either because of thesalary level or work level.
Even in facilities that don�t have anacute shortage, anesthesiologists aredemanding more efficient utilization ofOR time. They are no longer satisfiedwith big gaps in the middle of the dayand late cases running beyond normalworking hours or, as he puts it, �beingavailable 16 hours for 8 hours ofsurgery.�
�Groups are either negotiating formore money to recruit more providers,or they are seeking to reduce the work-load by having ORs scheduled moreefficiently,� Dr Mazzei says.
Some facilities that haven�t taken aproactive approach on these issues butinstead accuse anesthesiologists of �notwanting to work� or even of being�lazy� have seen �implosions� where20% to 40% of the anesthesia staff leave,he noted.
It could take 5 years to reach an equi-librium in the anesthesia labor supply.But even then it�s not clear the supplywill be sufficient.
Recruitment into anesthesia residen-cies has risen steadily since 1996, sur-passing its previous peak in 1992. Butthe demand for surgery continues togrow with the aging population.
There�s also a proliferation of loca-tions needing anesthesia services�ambulatory surgery centers, surgicalhospitals, office facilities, pain clinics,and imaging centers, among others.
In the past year, have any of your ORsbeen closed for morethan 1 week becauseof a shortage ofanesthesia providers?
Yes 20%
No 80%
Continued on page 16
Source: JWT Specialized CommunicationsHealthcare Group.
Continued from page 11
Community Teaching19% 28%
East Central South West22% 19% 20% 19%
training either at their hospital or in thecommunity. Not surprisingly, largedepartments with 10+ ORs (92%) are themost likely to offer preparation in-house.Teaching institutions (87%) are more like-ly to offer hospital-based preparationthan community facilities (77%).
The number participating in commu-nity-based education efforts has risenover the past 6 years from 5% to 12% thisyear. ❖
The OR Manager Salary/Career Surveyis coordinated by Billie Fernsebner, RN,MSN.
16 OR Manager Vol 19, No 9 September 2003
Recruitment & retention
Is recruiting experienced OR nurses more difficult?
Overall East Central South WestVery 43% 41% 42% 50% 39%Somewhat 44% 45% 45% 38% 47%Not at all 13% 14% 13% 12% 14%
Has recruiting becomemore difficult in thepast year?
No 37%
Yes 87%
No 39%
Yes 61%
Perioperative RNs
Surgical technologists
Bonuses not as lavishSign-on bonuses seem to be losing
some of their glitter.Less than half of respondents in this
year�s survey say their organizationoffers a sign-on bonus, down from2002. Some wrote in that their organi-zations were discontinuing bonusprograms.
Bonuses aren�t as lavish. The aver-age is $2,900, compared with $3,300 in2002. Only 5% (9) pay more than$5,000. The largest bonus was $7,000.
Recruiters say big sign-on bonusesnow often are spread over 2 to 3 yearsto give the new employee an incentiveto stay.
Some ORs report their facility offersa bonus even though they have novacancies in surgery.
Hospitals in the South (52%) andWest (50%) are more likely than thosein the East (39%) and Central (37%)regions to offer bonuses.
Reflecting the difficulty of recruit-ing in cities, bonuses are more com-mon in urban areas (56%) than in sub-urban (45%) or rural (36%) locales.
Larger facilities with 10+ ORs aremuch more likely (55%) to offer asign-on bonus than smaller ones with1-5 ORs (29%).
Despite the emphasis on retention,the percentage offering bonuses thatentice staff to stay is about the sameas last year.
As with sign-on bonuses, retentionbonuses are more common in largerfacilities (29%) than smaller ones(15%).
Examples of retention bonusesinclude:� $1,000 for RNs who work more
than 900 hours in 6 months� clinical ladder bonuses of up to
$5,000� $1,000 bonuses for achieving certi-
fication.
Do you pay a bonusto clinical staff...
No 55%
Yes 45%
No 80%
Yes 20%
>$5,000 5%
$4,001- $5,000 19%
$3,001- $4,000
5%
$2,001- $3,000 18%
$1,000- $2,000 42%
<$1,000 10%
For retention?
For recruitment?
How much is the bonus?Continued from page 15

17
Please see the ad for BOVIE MEDICAL
in the OR Manager print version.
18 OR Manager Vol 19, No 9 September 2003
New GI scope guidelineshave wide endorsement
New guidelines from the AmericanSociety for Gastrointestinal Endoscopy(ASGE), endorsed by ASGE and ten othergroups, provide recommendations onpreventing infection from flexible GIendoscopes.
The guidelines repeat the well-knownmessage�that all published episodes ofpathogen transmission related to GIendoscopy have been associated withfailure to follow establish cleaning anddisinfection guidelines or with use ofdefective equipment.
Among those endorsing the guide-lines are the Joint Commission on Accre-ditation of Healthcare Organizations,Association of periOperative RegisteredNurses, Association for Professionals inInfection Control and Epidemiology, andSociety for Gastroenterology Nurses andAssociates.
The guidelines, authored by D. B.Nelson et al, are in Infection Control andHospital Epidemiology, July 2003, 24:362-386. http://www.ichejournal. com/
They can be downloaded for free atwww.asge.org. Registration is required. ❖
Recruitment & retention
Does your OR hire RNs without OR experience?
No 11%
Often 35% Occasionally
54%
No 12%
Often 34% Occasionally
53%
2003 2000
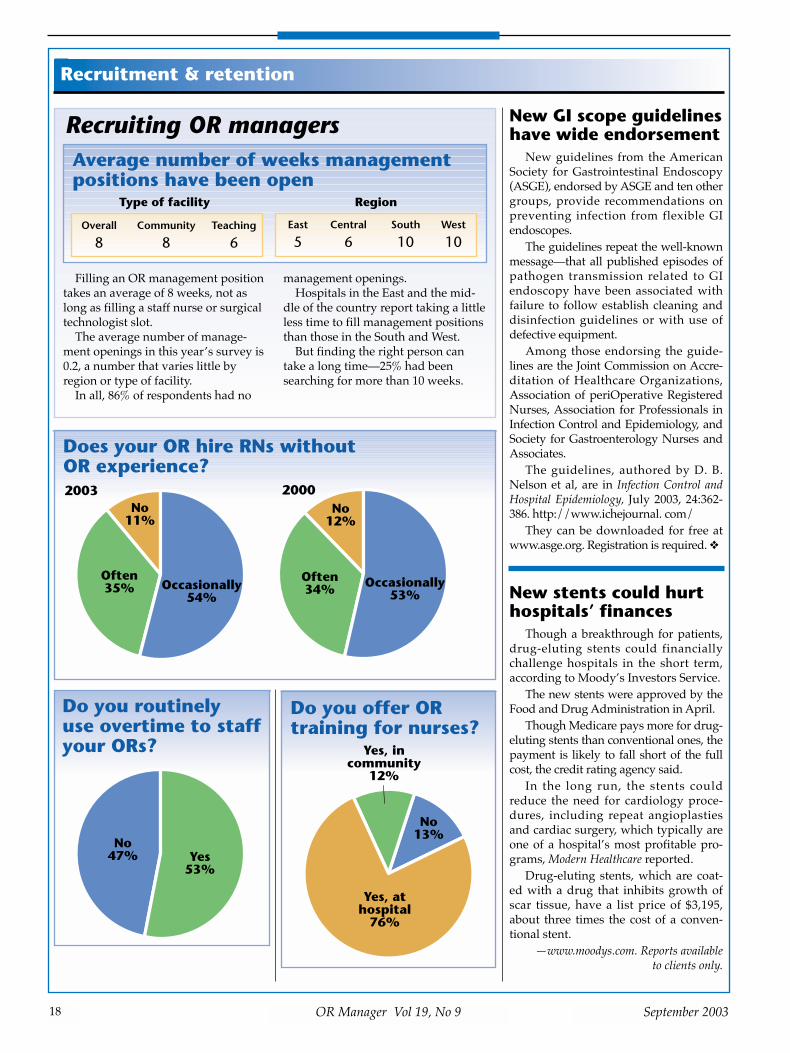
Recruiting OR managers
Filling an OR management positiontakes an average of 8 weeks, not aslong as filling a staff nurse or surgicaltechnologist slot.
The average number of manage-ment openings in this year�s survey is0.2, a number that varies little byregion or type of facility.
In all, 86% of respondents had no
management openings. Hospitals in the East and the mid-
dle of the country report taking a littleless time to fill management positionsthan those in the South and West.
But finding the right person cantake a long time�25% had beensearching for more than 10 weeks.
Average number of weeks managementpositions have been open
Type of facility
Overall Community Teaching
8 8 6East Central South West
5 6 10 10
Region
Do you routinely use overtime to staffyour ORs?
No 47% Yes
53%
New stents could hurthospitals’ finances
Though a breakthrough for patients,drug-eluting stents could financiallychallenge hospitals in the short term,according to Moody�s Investors Service.
The new stents were approved by theFood and Drug Administration in April.
Though Medicare pays more for drug-eluting stents than conventional ones, thepayment is likely to fall short of the fullcost, the credit rating agency said.
In the long run, the stents couldreduce the need for cardiology proce-dures, including repeat angioplastiesand cardiac surgery, which typically areone of a hospital�s most profitable pro-grams, Modern Healthcare reported.
Drug-eluting stents, which are coat-ed with a drug that inhibits growth ofscar tissue, have a list price of $3,195,about three times the cost of a conven-tional stent.
�www.moodys.com. Reports availableto clients only.
Do you offer ORtraining for nurses?
No 13%
Yes, in community
12%
Yes, at hospital
76%

19
Please see the ad for KIMBERLY-CLARK CORPORATION
in the OR Manager print version.
20 OR Manager Vol 19, No 9 September 2003
Recruitment & retention
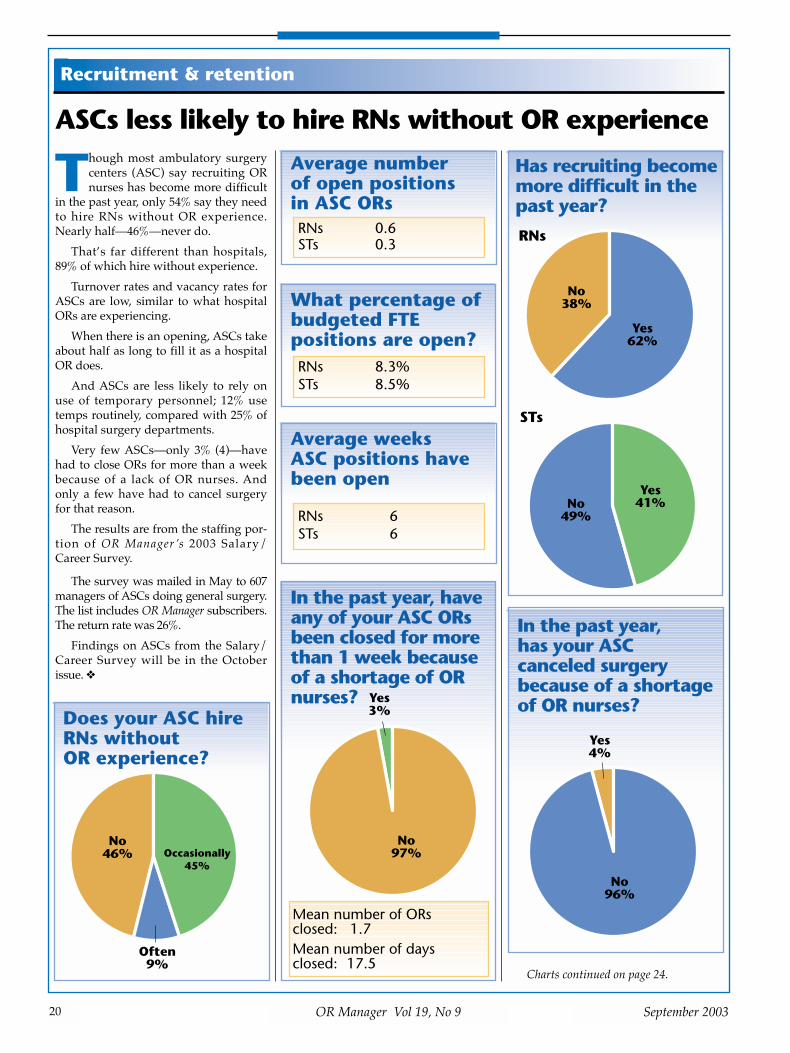
ASCs less likely to hire RNs without OR experience
Though most ambulatory surgerycenters (ASC) say recruiting ORnurses has become more difficult
in the past year, only 54% say they needto hire RNs without OR experience.Nearly half�46%�never do.
That�s far different than hospitals,89% of which hire without experience.
Turnover rates and vacancy rates forASCs are low, similar to what hospitalORs are experiencing.
When there is an opening, ASCs takeabout half as long to fill it as a hospitalOR does.
And ASCs are less likely to rely onuse of temporary personnel; 12% usetemps routinely, compared with 25% ofhospital surgery departments.
Very few ASCs�only 3% (4)�havehad to close ORs for more than a weekbecause of a lack of OR nurses. Andonly a few have had to cancel surgeryfor that reason.
The results are from the staffing por-tion of OR Manager �s 2003 Salary/Career Survey.
The survey was mailed in May to 607managers of ASCs doing general surgery.The list includes OR Manager subscribers.The return rate was 26%.
Findings on ASCs from the Salary/Career Survey will be in the Octoberissue. ❖
Charts continued on page 24.
In the past year, has your ASCcanceled surgerybecause of a shortageof OR nurses?
Yes 4%
No 96%
In the past year, haveany of your ASC ORsbeen closed for morethan 1 week becauseof a shortage of ORnurses? Yes
3%
No 97%
Average number of open positions in ASC ORsRNs 0.6STs 0.3
Mean number of ORs closed: 1.7Mean number of days closed: 17.5
What percentage ofbudgeted FTEpositions are open?RNs 8.3%STs 8.5%
Has recruiting becomemore difficult in thepast year?
No 38%
Yes 62%
RNs
STs
No 49%
Yes 41%
Does your ASC hireRNs without OR experience?
No 46%
Often 9%
Occasionally 45%
Average weeks ASC positions havebeen open
RNs 6STs 6

21
Please see the ad for OLYMPUS ENDOSCOPY
in the OR Manager print version.

22
Please see the ad for DUPONTin the OR Manager print version.

23
Please see the ad for DUPONT
in the OR Manager print version.
24 OR Manager Vol 19, No 9 September 2003
Recruitment & retention
Listen to your most important customers.Your surgeons.
An excellent way to listen to your surgeons is throughOR Benchmarks’s SurgeonSatisfaction Survey.
Physicians feel more com-fortable with an independent,external source that asks abouttheir satisfaction through aconfidential survey.
In a user-friendly question-naire, OR Benchmarks asksabout how easy and efficientyour surgeons find yourscheduling. We ask howsatisfied they are with yourpreoperative testing protocols.They tell us whether they findthe nursing and managementstaff clinically skilled andresponsive to their needs.Open-ended questions allowfor additional comments.
The Surgeon Satisfaction Survey is to be conducted inSeptember/October 2003
For a sample of the surveyquestionnaire, registrationmaterials, or additionalinformation, call 800/442-9918 or fax 505/982-7766.
Visit our website atwww.orbenchmarks.com
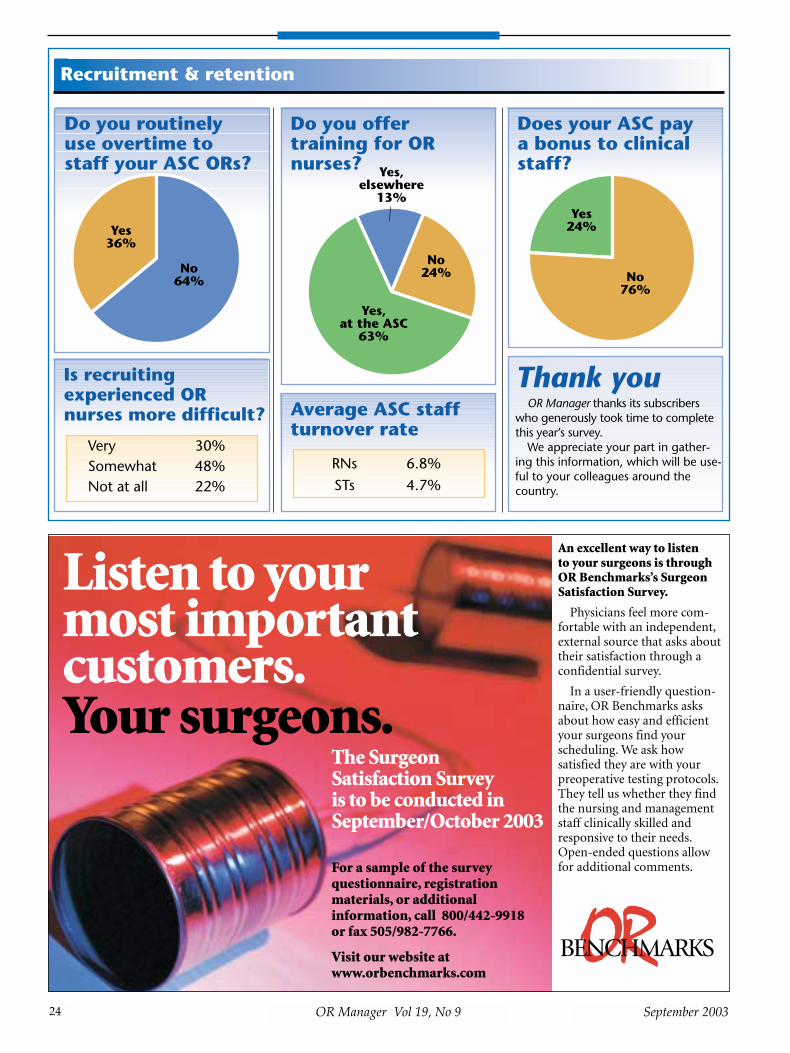
Is recruitingexperienced ORnurses more difficult?
Very 30%Somewhat 48%Not at all 22%
Do you routinely use overtime tostaff your ASC ORs?
Yes 36%
No 64%
Does your ASC pay a bonus to clinicalstaff?
Yes 24%
No 76%
Thank youOR Manager thanks its subscribers
who generously took time to completethis year’s survey.
We appreciate your part in gather-ing this information, which will be use-ful to your colleagues around thecountry.
Average ASC staffturnover rate
RNs 6.8%STs 4.7%
Do you offertraining for ORnurses?
No 24%
Yes, elsewhere
13%
Yes, at the ASC
63%

25
Please see the ad for CBPN
in the OR Manager print version.

have made significant progress.But the Senate�s chief GPO critic, Sen
Herb Kohl (D-Wis), said he thinks �notenough is happening� quickly enough.
Right after the hearing, he asked theSecretary of Health and Human Ser-vices to appoint a watchdog to overseegroup purchasing in health care.
In a new report issued July 16, theGeneral Accounting Office (GAO)found that although GPOs had adoptedcodes of conduct, the codes weren�tuniform, and some had clauses thatcould limit their effectiveness.
GPOs tout progressExecutices for Premier Inc and Nova-
tion told the senators about steps theyhave taken.
On physician preference items,Premier Inc�s chairman and CEO,Richard Norling, said the alliance nowhas multisource contracts with no com-mitment levels or bundling. Neuro-surgery products, which were previouslygrouped, have been separated into 11categories, for instance.
Norling said Premier has brought inoutside organizations, including therespected nonprofit ECRI to help assessnew technology.
A Premier spokesman told OR Man-ager that the GPO will be looking atunbundling a number of contracts,including those in the surgical area.
Mark Mckenna, head of Novation,said that among changes his organiza-tion has made is not to have sole-sourcecontracts unless there is no alternativeand the contract is approved by a clinicalcouncil. For example, for safety needlesand syringes, Novation has expandedfrom one vendor to four.
But a small-company executive, SalidHilal of Applied Medical ResourcesCorp, which makes trocars and otherminimally invasive surgery products,charged GPOs essentially act like �com-missioned sales representatives� fordominant companies, and �freeze out�small companies like his.
Halil noted, however, that Novationhad recently agreed to entertain a bid fromhis company after previously refusing.
Periop council aids in reviewNovation�s perioperative council has
taken several steps since the GPO
adopted new operating principles lastyear, said Zee Robertson, Novation�ssenior director for the surgical serviceline, in an interview with OR Manager.The 19-member council is made up pri-marily of perioperative nurses repre-senting member hospitals.
The council has reviewed the entiresurgical services contract portfolio toidentify �clinical preference� items,Robertson says. Clinical preferenceitems are those that meet a specific defi-nition, including being used in directpatient care.
�For clinical preference items, mostoften, we want a dual or multi-sourceagreement to give clinicians more selec-tion,� she says.
As part of opening up the process tonew technology, the periop council hasadded ten products from seven compa-nies, including four from AppliedMedical Resources.
Novation has also set up an onlinetechnology forum where vendors canpost information about new products.
In October, the periop council plans totake a look at Novation�s only majorbundled contract for surgical products,which is for sutures and endomechani-cals, to see if it should be taken apart.
Bundling is rappedSome question whether unbundling
contracts for sutures and endomechani-cals makes sense. There are only twomajor vendors, and dual sourcingwould be unlikely to provide as good aprice.
But bundled contracts have raisedeyebrows among GPO critics. Such con-tracts combine an array of products in asingle package.
Customers who agree to buy thebundle get a discount on all of theproducts in the package. Bundled con-tracts are the most controversial when
they involve a variety of unrelateditems from a single manufacturer.
Critics say bundling stifles competi-tion because it can give one manufac-turer a major share of the market andclose out others, particularly smallervendors.
The government is extending itsscrutiny of bundling to some compa-nies that do business with GPOs.
Connecticut�s attorney general,Richard Blumenthal, told the July 17New York Times his office had subpoe-naed Johnson & Johnson for informa-tion on the way it markets sutures andendomechanical devices. He also saidseveral other companies are beingexamined but declined to name them.The intent is to see if bundling violatesantitrust statutes and fraud and abuseregulations.
Johnson & Johnson has said it doesnot consider the contracts anticompeti-tive.
The GAO�s new report saysbundling may be declining. The reportexamined practices of seven nationalGPOs, including Premier Inc andNovation. For one of the two (not iden-tified), single-manufacturer bundledcontracts made up about 40% of itsmed-surg purchasing under contracts
26 OR Manager Vol 19, No 9 September 2003
Supply chain
Continued from page 1 Why are GPOsunder scrutiny?
Concerns raised by the GPOs� chiefcritic, Sen Herbert Kohl. GPOs saytheir codes of conduct address eachof these:
� Conflicts of interest, such aswhen GPOs or their executivesinvest in medical supplierswith which they do business
� Sole source contracts, whereone supplier has an exclusivedeal for a product with a GPO
� High commitment levels hospi-tals must meet (eg, 95%) toqualify for the best price from aGPO-approved vendor
� Bundling practices, which givea hospital an extra discount forbuying a bundle of products inone contract
� High GPO fees in excess of 3%charged to suppliers.
“Bundled contractshave raised eyebrowsamong GPO critics.
“
27OR Manager Vol 19, No 9September 2003
in effect Jan 1. But the GAO foundinterest in bundling was on the wane.
Why is bundling an issue?�The problem is, it�s a good deal for
a big company, but it�s bad for smallmanufacturers,� Lynn Everard, a healthcare supply chain consultant, told ORManager. Everard testified at the hear-ing as a critic of GPOs.
�When these deals get made, thedominant manufacturer wants to lockup business by bundling its products ina contract. The smaller manufacturerthat doesn�t have a broad product linebut has a better price won�t get used inthose hospitals.
�If the GPO believes everything isequal,� he added, �it will award the con-tract on the basis of the bundle that pro-duces the most fee revenue for the GPO.A small company doesn�t have thewherewithal to pay that much in fees.�
If smaller companies have troublecompeting, that could stifle innovation.
�More competition is what we needto get prices down,� he argues.
Everard would like to see Congresstake one of two actions:� Eliminate the safe harbor for health
care GPOs. The safe harbor was setup by Congress under the federalantikickback statute to protect GPOsreceiving fees from contracted ven-dors. GPOs also operate in anantitrust �safety zone� granted bythe government in 1996.
� Set up oversight of GPOs with rulesfor their business practices andpenalties for violations.Everard also would like to see more
hospitals declare their independencefrom GPOs. He contends hospitalsactually can save more by contractingindependently than they can withGPOs. Everard and his associate, PattiKing, have set up the nonprofitFoundation for Healthcare Integrity(www.healthcareintegrity.org) to workfor group-purchasing reform. ❖
The GAO report is at www.gao.gov
NewThe ORManagement SeriesA collection of articles from recent OR Managers
All modules now available• Patient Safety
• OR Design and Construction
• Recruitment and Retention
• Scheduling Surgery, Staffing, and Efficiency
• Infection Control and Sterilization
The OR Management
Series
A compilation of articles
from OR Manager
Patient Safety The
OR Management Series
A compilation of articles from OR Manager
OR Design & Construction
Order all five modules now $195Shipping and handling $7.95
Individual modules $45Shipping and handling $7.95
Order by calling 800/442-9918 or order online at www.ormanager.com
Supply chain
OR Manager “super subscription”
OR Manager is offering a newoption—the “super subscription.”You can continue to receive theprint version of OR Manager everymonth, plus an early electronicversion, which will be available onthe OR Manager web site, www.ormanager.com 2 to 3 weeksbefore your print copy.
You will also have access to ORReports, our monthly review of thelatest studies on the OR environ-ment, and regular e-mail bulletinswith news you need. The price:$129 a year.
If you wish, you can continueto subscribe to the print copyonly for $86 annually.

28
Please see the ad for SKYTRON, INC.in the OR Manager print version.

September 2003
Hospitals to get bonusesin new Medicare demo
Hospitals belonging to Premier Inc will beable to get higher Medicare payments ifthey meet quality measures for five condi-
tions�acute myocardial infarction, heart failure,hip and knee replacement, pneumonia, and coro-nary artery bypass graft (CABG).
The voluntary 3-year pilot project announced inJuly is a partnership between Premier, a grouppurchasing alliance, and the Centers for Medicareand Medicaid Services (CMS).
Premier expects about 300 hospitals will partici-pate.
Hospitals will be scored on quality measuresfor each condition. Premier will track performancethrough its online database called Perspective.
Hospitals in the top 10% for a given conditionwill receive a 2% bonus from Medicare. Hospitalsin the second 10% will receive a 1% bonus.
There would also be penalties in the third yearfor poor performers. A baseline will be set at the bot-tom two percentiles after the first year. Hospitalsthat fall below that in the third year would haveMedicare payments cut. CMS does not expect that tohappen because it expects hospitals at the bottom toimprove at least above the baseline level.
Data from the participating hospitals will bepublished on the CMS web site.
If the pilot is successful, CMS could proposeexpanding it to all hospitals, but that wouldrequire action by Congress.
The quality indicators for surgical conditions inthe demo are:
Coronary artery bypass graft� Aspirin prescribed at discharge� CABG using internal mammary artery� Prophylactic antibiotic received within 1 hour
prior to surgical incision� Prophylactic antibiotic selection for surgical
patients� Prophylactic antibiotics discontinued within 24
hours after surgery end time� Inpatient mortality rate� Postoperative hemorrhage or hematoma� Postoperative physiologic and metabolic
derangement
Hip and knee replacement� Prophylactic antibiotic received within 1 hour
prior to surgical incision� Prophylactic antibiotic selection for surgical
patients� Prophylactic antibiotics discontinued within 24
hours after surgery end time� Postoperative hemorrhage or hematoma� Postoperative physiologic and metabolic
derangement� Readmissions 30 days postdischarge� Discharge to home/home health ❖
Please see the ad for ECRI
in the OR Manager print version.

A regular column on technology trendsfor surgical services.
Robotic surgery has moved fromfiction to fact, and surgeons�interest is growing.
Is it time to invest? Though the technology shows sig-
nificant potential, surgical robotics is inits infancy, and widespread use of truerobotic surgery is probably years away.Even hospitals with sufficient capitalcan�t yet justify the $1 million or sorequired to purchase a telemanipula-tion surgical robot, such as the daVincior Zeus.
For most facilities that are interestedin getting into robotics now, the firststep is likely to be the less sophisticated�surgical-assist� robots. Surgical-assistrobots are sufficiently developed andaffordable for a typical hospital to con-sider. The most common type of surgi-cal-assist robot is the robotic endoscopeholder, which holds and positions anendoscope during minimally invasivesurgery (MIS). An example is the Aesop3000 from Computer Motion, whichECRI evaluated recently. Robotic endo-scope holders typically cost less than$125,000 compared with more than $1million for telemanipulation surgicalrobots.
Because telemanipulation systemsare expensive, have limited application,and so far have shown little if any bene-fit over manual surgery, these systemsprobably are more suited to large teach-ing hospitals that want to train sur-geons who will eventually have accessto improved technology.
For most hospitals at present, inECRI�s view, the success of surgical-assist robots is mainly in helping tobuild a safety record for robotics in gen-eral and in allaying concerns aboutrobotics. For now, it is unrealistic inmost cases to expect more tangible out-comes, such as eliminating a staff posi-tion or significantly boosting revenue.More likely, a robotic endoscope holderwill allow occasional reassignment of asurgical assistant to other duties.Whether a robotic endoscope holdercould help increase revenue dependson whether the facility could expand itspatient base. This might be possible if
the facility could increase its volume ofendoscopic procedures, especially car-diac procedures. This offers somepotential for offsetting the cost. Butwhether the robot can actually pay foritself depends on how successful a facil-ity is in marketing its use. ECRI hasheard of situations where robotic endo-scope holders were purchased butquickly relegated to the supply closet,either because the surgeons were notinterested in the technology or did notfeel it offered sufficient clinical advan-tages.
These are some questions to ask ifyour facility is considering a surgical-assist robot, such as the robotic endo-scope holder.
Are the facility’s surgeonsinterested in exploring thesurgical application of robots?
Many surgeons believe robots willshape the future of surgery, and interesthas increased tremendously. Becausemost hospitals can�t afford to invest inan advanced robotic system, a roboticendoscope holder may be a good firststep. Using a robotic endoscope holderallows surgeons to overcome the novel-ty and challenge of operating withrobotics.
Will the robot help the facilityperform new types of MISprocedures, or will it signifi-cantly improve procedures thefacility already performs?
Though robotic endoscopic holdersoffer performance that is in many wayssuperior to that of a human scope hold-er�they hold the scope steady, respondprecisely to the surgeon�s commands,and don�t get tired or bored�mostendoscopic procedures can be per-
formed without these devices. A robotic endoscopic holder may,
however, allow facilities to performprocedures that are extremely difficultif not impossible to perform with ahuman scope holder. Examples are:� endoscopic coronary artery bypass
graft (e-CABG)
� laparoscopic radical prostatectomy.The e-CABG requires the scope to be
very close to the surgical site and theimage to be greatly magnified. Thisrequires an image stability a humanassistant cannot achieve. The e-CABGcurrently is the �holy grail� for surgicalrobotics because of the high reimburse-ment margins for cardiac surgery. Butendoscopic surgery still is limited tosingle vessels. And despite the goodreimbursement, there is no additionalpayment for a robot. So a facility wouldneed to be sure the extra cost of therobot would not consume the margin.
There also is a learning curve for e-CABG, though the learning curve is notas great for using a robotic endoscopeholder as it is for learning to operate atelemanipulation system, particularly ifthe surgeon is already accustomed toendoscopic surgery. During the learn-ing phase, it is not unusual for any typeof robotic surgery to take twice as longas the same operation performed usingstandard open or endoscopic tech-niques.
Further complicating the picture isthe Food and Drug Administration�srecent approval of drug-eluting cardiacstents, which may reduce the overallvolume of CABG surgery. Thoughrobotics could really shine in cardiacsurgery as well as in other types ofsurgery, it�s too early to know whetherthe potential will pan out.
For laparoscopic radical prostatecto-my, the advantage of the Aesop roboticendoscope holder that ECRI evaluatedis to provide extra room for the surgicalteam. The robot�s small footprint givesthe surgical team more space to maneu-ver. Though that many be true for thetelemanipulation systems as well, ECRIhas not examined those systems.
Facilities performing e-CABG orlaparoscopic radical prostatectomy
30 OR Manager Vol 19, No 9 September 2003
Is it time to add a robot to your team?Technology in Surgery
“Surgeons’ interesthas increasedtremendously.
“
Continued on page 32

31
Please see the ad for CENSIS TECHNOLOGIES INC.in the OR Manager print version.

32 OR Manager Vol 19, No 9 September 2003
Please see the ad for OLYMPUS ENDOSCOPY
in the OR Manager print version.
could benefit from purchase of a roboticendoscope holder, though ECRI stillencourages facilities to do their home-work before making a purchase.Facilities may also benefit if they fre-quently perform long endoscopic pro-cedures where fatigue is a factor.
But unless a facility can answer �yes�to both of these questions, the purchaseof a robotic endoscope holder probablywill not be justified at this time. ❖
�Dan AltHealth Devices Group
ECRI, Plymouth Meeting, Pa
Dan Alt can be reached at [email protected]
ECRI, a nonprofit organization some-times called the Consumer Reports ofhealth care, is known for its objectiveapproach to medical device evaluation. Visitwww.ecri. org or phone 610/825-6000.
Continued from page 30
OR Manager’s ToolboxCheck our web site for practical help
on personnel evaluation, codes of con-duct, and patient assessment.
Go to www.ormanager.com. Lookunder The OR Manager’s Toolbox.
WorkplaceAwards given for quality care
Three hospitals and a health systemhave been honored for leadership andinnovation in quality, safety, and com-mitment to care.
Abington Memorial Hospital in Abing-ton, Pa, won the top prize of $75,000 in theAmerican Hospital Association�s Amer-ican Hospital Quest for Quality.
Two other finalists, Beaumont Hos-pitals in Royal Oak, Mich, and the Uni-versity of Wisconsin Hospital and Clinicsin Madison, each received $12,500.
The common focus of the winningfacilities was a culture of safety and ablame-free environment where reportingof errors is encouraged and facilitatedamong staff, patients, and families.
The awards are supported by grantsfrom the McKesson Corporation andFoundation.
�www.aha.org/questforquality
Shorter work hours forresidents costing millions
New rules by the AccreditationCouncil for Graduate Medical Educa-
tion that limit work hours for residentswill cost teaching hospitals millions ofdollars a year. The increased costs comefrom hiring additional personnel tocover hours residents are no longerallowed to work, according to the July10 Chicago Tribune.
Effective July 1, residents workhours fell from 130 or more hours toabout 80 hours a week. The rules alsorequire residents to have 10 hours ofrest between daily work hours andbeing on call.
Chicago�s Northwestern MemorialHospital is expected to spend morethan $5 million a year in additional staffand hospitalists, who care for patientswhile in the hospital.
The University of Chicago Hospitalsexpect an additional $3 million in costseach year to make up for lost residenttime. The biggest single cost comes frompersonnel such as nurse practitionersand operating room nurses who serve assurgical assistants, according to the hos-pital�s vice president for planning.
�www.chicagotribune.com

33
Please see the ad for PERIOPTIMUM
in the OR Manager print version.
34 OR Manager Vol 19, No 9 September 2003
Almost every month, a surgicalspecialty meeting is held some-where in the US. Surgeons come
back, and soon you find a request fornew equipment on your desk. Or youmay find the equipment has alreadybeen ordered, and the surgeon has plansto use it as soon as it arrives. And, by theway, the surgeon needs a company rep-resentative in the OR to provide adviceas he begins using the equipment.
Ambulatory surgery centers (ASCs)have close relationships with industryrepresentatives, and they depend oneach other. Surgeons and nurses rely onreps for their expertise in the equipmentthey sell. Reps obviously depend onphysicians and ORs for their sales.
For the most part, these relationshipsare positive and supportive. But therealso need to be clear boundaries.
With the technology explosion andconcerns about patient privacy and safe-ty, surgery facilities are taking a moreproactive approach to their relationswith vendor reps. They are developingpolicies and procedures to clearly definesales reps� roles in the facility and specifyhow their presence will be authorizedand their activities governed.
�It�s important to point out to physi-cians that they need good policies to
protect themselves and the facility.Policies are important to minimize thecenter �s liability and protect theinvestors,� points out Nancy Jo Vinson,RN, BA, CASC, director of clinical oper-ations for Acumen Healthcare, Dallas.Vinson spoke on the topic at the 5thInternational Congress on AmbulatorySurgery in May in Boston.
High-profile casesSome notorious incidents have
pointed out the need for good policies. In one high-profile case in 1997, a
young woman died at Beth IsraelMedical Center in New York City afterwhat should have been a routine hys-teroscopy. The procedure was per-formed with a new device investigatorssaid hadn�t been properly introduced
into the facility. There were initialreports that a sales rep might haveoperated the device�s controls, but astate panel later found no evidence thathe operated the equipment and said hispresence did not affect the care thepatient received.
More recently, the Guidant Cor-poration pled guilty in June to 10felonies and agreed to a $92 million fineto settle charges over thousands of inci-dents in which its abdominal aorticaneurysm graft�s delivery system mal-functioned. In some cases, when thedelivery device became stuck, to avoidan open procedure, sales reps instruct-ed the surgeons how to free the deviceby breaking the handle and removing itin pieces, even though this techniquehad not been tested, and neither thedoctors nor the reps had been trainedon its use. In some cases, patients died.Patients have filed lawsuits.
Strike a balanceThe ASC�s administrator and med-
ical director should be involved indrafting the policies, getting buy-infrom the physicians, and educating thephysicians and nurses about the expec-tations. Policies should strike a balancebetween the legitimate role a sales repcan play in technical support and edu-cation and the ASC�s concerns forpatient safety, privacy, and risk man-agement.
Two good resources for developingpolicies are statements from the Amer-ican College of Surgeons (ACS) andAssociation of periOperative RegisteredNurses (AORN) approved in 2000. Aself-learning module for sales reps isavailable from ECRI, a nonprofit orga-nization that assesses health care tech-nology (sidebar).
Accrediting bodies consider obser-vers in the OR to be primarily an issueof patient privacy and confidentiality.
The Joint Commission on Accredi-tation of Healthcare Organizations says
Setting boundaries for vendors in OR
Gwendolyn Grothouse, RNAdministrative directorApple Hill Surgical CenterYork, Pa
Barbara Harmer, RN, BSN, MHASenior consultantHealthCare Consultants, IncCelebration, Fla
Jerry Henderson, RN, BS, CNOR, CASCExecutive directorThe SurgiCenter of BaltimoreOwings Mills, Md
Diana Procuniar, RN, BA, CNORNursing administratorWinter Haven Ambulatory Surgical
CenterWinter Haven, Fla
Donna Gelardi-Slosburg, RN, BSN, CASCNational surgery specialistHealthSouthSt Petersburg, Fla
Rhonda Tubbe, RN, CASC, CNORAdministratorThe Surgery Center of NacogdochesNacogdoches, Tex
Ambulatory Surgery Advisory Board
Continued on page 36
“Carefully definewhy sales reps need
to be present.
“

35
Please see the ad for SURGICAL INFORMATION SYSTEMS
in the OR Manager print version.

patients have a right to privacy andshould be asked to give their consent ifobservers will be present during theirprocedures.
The Accreditation Association forAmbulatory Health Care (AAAHC)does not address vendor relationsdirectly, but its standards say patients�privacy and confidentiality will be pro-tected. AAAHC�s surgical services stan-dards say that only authorized personsare allowed in the surgical area.
HIPAA and sales repsSales reps� presence is a gray area
under the privacy rule of the HealthInsurance Portability and Accountabil-ity Act (HIPAA). The issue has yet to beaddressed by the government in any ofits HIPAA guidances.
Amy Fehn, an attorney with Wachler& Associates, Royal Oak, Mich, whichconsults on HIPAA, advises ASCs thatthe best approach is to:� carefully define the reasons why
sales personnel need to be presentduring patient care
� have patients sign an authorizationif a sales rep will be present duringtheir care.A patient authorization is a specific
document required under HIPAA whena person�s protected health informationwill be disclosed for purposes otherthan treatment, payment, or health careoperations. At the very least, ASCsshould require sales reps to sign a con-fidentiality agreement, Fehn says. Inher opinion, a business associate agree-ment doesn�t fit the situation becausesales reps who observe surgery aren�tproviding a service to the center. UnderHIPAA, business associates are partieswho are exposed to patient informationwhile providing a service on behalf of acovered entity; examples are lawyers,accountants, and billing firms.
Another HIPAA expert, RobertTennant of the Medical Group Man-agement Association, says the issuehinges on whether sales personnel willhave access to patients� protectedhealth information. For example, the
surgeon says to the rep before a proce-dure, �We are performing a hysterecto-my on Mrs Jones today.
�That clearly is disclosing protectedinformation,� says Tennant. �Prudencewould dictate that you should eitherhave the rep sign a business associateagreement if they are performing a ser-vice with the patient�s information forthe ASC or a confidentiality agree-ment.�
On the other hand, if the rep onlyprovides in-service education and is notexposed to patient information,Tennant advises that a business associ-ate agreement probably isn�t necessarybut a confidentiality agreement wouldbe wise. �That would put the rep onnotice that any incidental exposure topatient information must be protected,�he says.
Review state lawYour state may have specific regula-
tions pertaining to patient privacy andobservers in the OR. You need to knowwhat the state law is because a state lawmay take precedence over HIPAA orother federal regulations.
What areas should the policyaddress?
These are specific areas that should beaddressed in a vendor relations policy.
Define vendors’ roles The policy should spell out compa-
ny representatives� role in the ASC,such as to provide in-service educationand technical assistance. AORN�s state-ment advises that reps should not scrubin on cases. Regarding equipment,AORN says reps �with specialized
training may perform remote calibra-tion to adjust devices to the surgeon�sspecification,� such as pacemakers or alaser.
�But it should be not the other wayaround�they don�t tell the surgeonwhat he needs for specifications,�Vinson cautions. �The surgeon shouldhave enough knowledge about theequipment to give the sales rep direc-tions, not vice versa.�
Sales reps should attend only toequipment of the company they repre-sent and should not operate or trou-bleshoot equipment made by other ven-dors.
Define in the policy the appropriatebehavior for sales reps while in thefacility.
�There used to be a lot of kiddingaround. But that�s not appropriate anymore with so many patients awake dur-ing their procedures,� Vinson com-ments. Proper demeanor should beexpected everywhere in the facilitybecause patients can easily overhearconversations while waiting for surgeryand recovering afterward.
Define the approval process The policy should spell out the
process for authorizing sales personnelto be in the facility and in the OR.Among issues to consider:� How far in advance approval should
be sought. AORN recommends boththe reps� presence and purpose forbeing there should be determined inadvance.
� A requirement for an identificationbadge with the rep�s name and com-pany
� The person in the ASC who is autho-rized to approve sales reps� presenceand ensure compliance with policies
� Sanctions if the policy is violated.For example, if there are repeatedviolations, the policy might say thatthe company will be contacted, andthe rep will no longer be allowed atthe facility. If a physician continuallyviolates the policy by bringing reps
36 OR Manager Vol 19, No 9 September 2003
AmbulatorySurgery
Continued from page 34
Continued on page 38
“It’s not good enoughto have a casual
statement on yourconsent form.
“

37
Please see the ad for TRUMPF MEDICAL INC.
in the OR Manager print version.
38 OR Manager Vol 19, No 9 September 2003
into his or her cases, the policymight state that the matter will bereported to the medical staff execu-tive committee.
Determine qualificationsThe policy should define the qualifi-
cations and competencies sales reps
will be expected to demonstrate beforebeing an observer. AORN recommendsdeveloping a system to document thatsales personnel have completed instruc-tion in:� principles of asepsis
� fire and safety protocols
� infection control practices
� bloodborne pathogens
� patients� rights.Additional areas might include
HIPAA and knowledge of the ASC�spertinent policies.
There are a variety of ways ofaccomplishing this, ranging from docu-menting instruction provided by thesales rep�s company through providingtraining in your own facility or organi-zation.
�All of these areas should bereviewed with the rep,� says Vinson. Ata minimum, reps need to know wherethe exits are in case of a fire, what asterile field is and how to avoid conta-minating it, how to protect themselvesfrom contact with blood and other bodyfluids, and how to conduct themselvesin accord with patients� rights.
At facilities Vinson�s company man-ages, the reps receive a review sheetcovering each of these areas. They alsoare asked if they have completedhepatitis B immunization and had arecent TB test. She finds that for many,this is a company requirement.
Patient consentThe policy should include a require-
ment that surgeons notify patients andobtain their consent for observers. Or, ifyour center determines it is necessaryto comply with HIPAA, patients couldbe asked to sign an authorization formacknowledging a sales rep will be pre-sent. The consent or authorization formshould be included in the patient�smedical record.
Says Vinson, �It is not good enoughto have a casual statement on your con-sent form that says any observer can bein the OR,� which might have been thepractice in the past.
Donna Slosburg, RN, BSN, CASC,national surgery specialist for Health-
South, says its ASCs typically have aconsent form signed by the patient,physician, and vendor before a salesrep is present in the OR.
�This way, all parties involved areaware of the vendor�s presence and rea-son for being in the OR,� she says.
Physicians generally call in advanceto let the center know a sales rep iscoming because they are aware of theconsent protocol.
DocumentationThe policy should provide that the
sales rep�s presence during a procedurewill be documented in the OR recordby the circulating nurse. The informa-tion also should be documented in thephysician�s operative note. ❖
AmbulatorySurgery
Resources onvendors in ORAmerican College ofSurgeons
312/202-5000www.facs.orgStatement on issues to be considered
before new surgical technology isapplied to the care of patients. ST-23.
�www.facs.org/fellows_info/statements/st-23.html
Statement on health care industryrepresentatives in the operating room.ST-33.
�www.facs.org/fellows_info/statements/st-33.html
Association of periOperativeRegistered Nurses
800/755-2676www.aorn.orgEvaluation and selection of products
and medical devices used in ambulato-ry practice settings. In AmbulatorySurgery Principles and Practices, 3rd ed.Denver: AORN, 2003.
AORN statement on the role of thehealth care industry representative inthe operating room. In 2003 Standards,Recommended Practices, and Guidelines.Denver: AORN, 2003.
ECRI610/825-6000 ext 5888www.ecri.orgSelf-directed learning module for
sales representatives in the operatingroom. Health Care Risk Control. Vol 1.January 1998.
Can be ordered as a separate articlefor $75. Can be photocopied within thesame facility.
Continued from page 36
Joint Commissionadds core measurerequirements
Hospitals accredited by the JointCommission on Accreditation of Health-care Organizations will be required togather and use data on an additional setof core performance measures beginningin January.
The new requirement will increasethe scope of data collection and report-ing from two to three core measure sets.
Hospitals currently can choose fromfour core measure sets that addressacute myocardial infarction, heart fail-ure, community-acquired pneumonia,and pregnancy-related conditions.
New measure sets are expected tobecome available over the next 6 to 24months. These will address surgicalinfection prevention, ICU care, painmanagement, and inpatient pediatricasthma.
Core measures are part of the JointCommission�s ORYX initiative aimed atintegrating outcomes and other perfor-mance measurement data into theaccreditation process. The goal is a con-tinuous, data-driven accreditationprocess focused on results of care. ❖
�www.jcaho.org

39
Please see the ad for ADVANCED STERILIZATION PRODUCTS
in the OR Manager print version.
Q. Block time raises a lot of questionsat our facility. We�d like your advice onthese issues: What should we require forblock time utilization by our surgeons?How often should block time be adjusted?What should our release time be for blocktime that is not scheduled? Also, what areyour suggestions for adjusting block time ofsurgeon owners who may not be utilizingtheir block time at the expected level?
A. As a company, we deal withmany surgeons on a day-to-day basis,and we ask them questions. Theresponses, more often than not, lead toopportunities. We currently have about4,500 surgeons in our databank whomwe have formally interviewed. Eachinterview is held one on one and in pri-vate, so we are pretty confident we aregetting accurate feedback. This data hasproven to be very helpful in designingprograms around what surgeons arelooking for in surgery, both inpatientand outpatient.
For this column, we tapped into ourdatabank for information on blockbooking. Of the 4,456 surgeons in ourdatabank, 38% like it, want it, and saythey cannot survive without it. Another35% percent hate it, never want to dealwith it, and would draw blood to avoidit. An additional 15% want some sort ofcombination of block booking and first-come, first-served; 10% could care lesseither way; and 2% admirably evadedanswering the question.
Booking a tableWith that in mind, let�s look at the
block-booking dilemma. I like analogiesto life situations.
Block booking is essentially a reser-vation. Let�s say you are going to din-ner on Saturday night, and you don�twant to wait for a table. You call aheadand reserve�block book�a table. Yourevening is pretty well planned now.You don�t have to worry about rushingaround or getting to the restaurantearly�you are taken care of.
Conversely, so is the establishment.Their goal is to make money. They can
only make money if their tables are fullof happy, eating people.
Let�s take it a step further. After din-ner, you want to celebrate, and youknow you just might celebrate a bitmuch. So you wisely call Holiday InnExpress and make a similar reservationfor that night. It is right across the streetfrom the restaurant so you can walkright over there. But unlike the restau-rant that so graciously accepted yourreservation, the wise people in the hotelbusiness would like you to back upyour reservation with a credit card.
�Not a problem,� you tell them asyou roll out the numbers of your card.
�Just be sure you cancel this before 6pm, or we will charge you for theroom,� the voice from the hotel says.
�As if that will happen!� you quipback.
The day unfolds, and you spendtime working in the yard, dealing withkid issues, and about 6 pm you look atyour spouse and you both come to thesame conclusion: �I�m too tired to goout. Why don�t we order a pizza andstay in?�
�Great idea!�And so it goes.�Should I call the restaurant and
cancel our reservation, honey?��Naw, they deal with that all the
time. They know people won�t showup. Not a problem.�
�Exactly. What can they do any-way?� you say, chuckling.
�What about the hotel room?��Oh, yes,� you say, jumping off the
couch. �Get them on the phone rightnow�tell them we had an emergency,and we have to cancel the room fortonight. Hurry, it�s almost 6 o�clock,
and they will charge my credit card ifwe don�t cancel right now.�
Run it like a businessSo is your surgery center a restau-
rant or a hotel? If you book an airlineflight and don�t show up, you still paidfor the ticket. Most car rental compa-nies now charge for �no shows� as well.
Please tell me the difference betweena surgery department and these exam-ples. If you are going to use block book-ing for elective, nonemergency sched-uled cases, you need to run it like abusiness�because that is what it is.
If you are a surgeon, and you tell meyou are going to fill an operating roomfor 5 hours every other week, then youhad better do it because your �reserva-tion� prevents me from letting someoneelse use that time to pay my staff whoare hanging around waiting for theirpaychecks.
�But,� you say, �I filled 3 hours ofmy slot!�
�Great, you say. Then I only have topay three fifths of my expenses? I don�tthink so!�
Set clear rulesIf you are going to block book, you
need rules. Make them exceedinglyclear. Remember, your surgeon is yourclient. But also remember you need rev-enue to survive.
I personally like the first-come, first-served way of booking cases, but I canobjectively see both sides of the issue.
Set a limit on the blocks. For exam-ple, during any one quarter (or monthor week; you choose the time frame),the surgeons� block will be for only thenumber of hours the block was usedduring the previous period. Say the sur-geon used only 75% of the time allocat-ed; therefore, his or her time has beenreduced by 25% for the next period.
Always keep at least one operatingroom �off book,� so when surgeonsactually do go over their time, they canbook their other cases on a first-come,
40 OR Manager Vol 19, No 9 September 2003
AmbulatorySurgery
Make clear rules on block scheduling
ASC Strategy & Tactics
ASC Strategy & Tactics
Continued on page 42

41
Please see the ad for B E SMITH
in the OR Manager print version.
42 OR Manager Vol 19, No 8 August 2003
first-served basis in the nonblockedroom.
As a facility that wants to be success-ful, you need to make sure your operat-ing rooms stay full. Have a cut-off pointfor booking every block. You knowyour center or department better thananyone else, but a common practice isto say that if a block is not full 3 busi-ness days before the day of surgery, youhave the option to reduce the blocktime or eliminate it completely. Yes,people will get mad at you over this�but they get mad at you anyway sowhy not do it over something that isgood?
The surgeon ownerIf the surgeon is a partner in the
facility, he or she has a vested interestin the utilization of the facility. Thus,the surgeon should be willing to adjust
the block so it is more in line with actu-al usage. If the individual isn�tamenable to self-adjust the time, Iwould add an item to the agenda forthe next meeting of the partnershipentitled �Block time utilization byphysician.� If that doesn�t do it, or if theother partners don�t seem to care aboutit, then let it go and find other issues tofocus on. ❖
�Stephen W. Earnhart
Stephen W. Earnhart is president andCEO of Earnhart & Associates, Inc, Dallas.He can be reached at [email protected]
Earnhart & Associates has benchmarksfrom hundreds of facilities across the coun-try. To find out how to receive free bench-marks, visit www.earnhart.com
If you�d like to submit a question for thecolumn, please e-mail it to [email protected].
AmbulatorySurgery
Continuedfrom page 40 On-line continuingeducation in OR and anesthesiamanagement
Franklin Dexter, MD, PhD, is offeringeducational modules on using OR andanesthesia information system data toenhance managerial decision making for:� OR staffing and block time allocation
� OR financial assessment for strategicdecision making
� anesthesia staffing to increase pro-ductivity and reduce costs
� economics of anesthetic drugs andsupplies.The course web site is at www.
FranklinDexter.net. Slides and synchro-nized audio are also available on CD.Credit is available from the Universityof Iowa Carver College of Medicine. Forinformation, e-mail [email protected] ❖
Please see the ad for CAP GEMINI ERNST & YOUNGin the OR Manager print version.
In Business NewsZimmer poised to acquire Centerpulse
Orthopedic device manufacturer Zimmer, Warsaw, Ind,was set to buy Centerpulse, based in Zurich, Switzerland,after rival Smith & Nephew decided not to raise its bid.
The acquisition would make Zimmer the largest orthope-dic implant company in the world, according to the FinancialTimes of London.
Centerpulse also is a maker of implants and biologicals fororthopedics.
Device reprocessor agrees to stop, correctprocesses
The Food and Drug Administration (FDA) announcedAug 8 that Adven Medical, Lubbock, Tex, had agreed tostop reprocessing and distributing medical devices until itcorrects manufacturing problems. The FDA said it foundnumerous violations of federal requirements during inspec-tions of the firm. Adven reprocesses both used and open-but-unused devices such as catheters and biopsy forceps.
SEC fines former head of SRI/Surgical ExpressThe Securities and Exchange Commission fined the for-
mer president of the surgical supply company SRI/SurgicalExpress, Tampa, Fla, $50,000 in August to settle a complaintthat the company misstated revenue in its 2001 quarterlyreports, according to the Associated Press. ❖

43
Please see the ad for SPECTRUM SURGICAL INSTRUMENTS
in the OR Manager print version.
44 OR Manager Vol 19, No 9 September 2003
P O Box 5303Santa Fe, NM 87502-5303
The monthly publication for OR decision makers
At a Glance
The monthly publication for OR decision makers
Periodicals
What leads to surgeons’ errors?Inexperience and lack of competence,
communication breakdowns, and fatigueor excessive workload are the most com-mons system factors leading to errors bysurgeons, according to confidential inter-views with 38 surgeons from threeMassachusetts teaching hospitals whoreported on 146 incidents.
More than 30% of the incidents result-ed in permanent disability and 13% inpatient death. A total of 77% of the errorsinvolved injuries related to a surgical orother invasive procedure, 13% involvedunnecessary or inappropriate procedures,and 10% involved unnecessary advance-ment of disease. Two-thirds of the errorsoccurred intraoperatively, 27% preopera-tively, and 22% postoperatively.
�Gawande A et al. Surgery. June2003;133:614-621.
Rings increase risk of handcontamination
Ring wearing was associated with a10-fold higher median count in skinorganisms in surgical intensive care unitnurses. Risk of contamination increasedwith the number of rings worn in astudy from the Centers for DiseaseControl and Prevention in Atlanta andCook County Hospital and RushMedical College in Chicago.
Researchers also compared handhygiene agents used by the nurses andfound that hand contamination with anytransient organism was significantly lesslikely after use of an alcohol-based handrub compared with plain soap and
water, but not after use of a medicatedhand wipe.
�Trick W E et al. Clin Infect Dis. June2003;36:1383-1390.
Device harvests patient’s ownstem cells for spinal fusion
A new minimally invasive surgicaldevice allows surgeons to harvest anduse a patient�s own stem cells for spinalfusion surgery.
The new technique (Cellect, DePuyAcroMed, a Johnson & Johnson Com-pany) uses a needle to collect bone mar-row cells from the hip area and thenprocesses the cells so they can be graftedonto the spine.
Bone harvesting for spinal fusion is tra-ditionally performed through a 3- to 5-inch incision. More than a fourth ofpatients continue to feel pain in the hiparea up to 2 years after harvesting surgery.
The new technology, developed incollaboration with the Cleveland ClinicFoundation, allows surgeons to selective-ly control or increase the population ofbone-forming cells in a region wherenew bone tissue is needed.
�www.jnj.com
Hospital web sites feature livesurgery
Taking reality programming to a newlevel, hospitals are beaming surgeries�from tummy tucks to open-heart repairs�live to the public on their web sites.
Live web casts of surgeries are usedto educate doctors promote the hospital�s
name, and generate business, accordingto the July 16 Boston Globe .
For Brigham and Women�s first liveweb cast, the chief of surgery narratedthe action from the next room so the sur-geon could focus on the surgery.Questions e-mailed to the hospital by theviewers were answered out loud by thenarrator.
�www.boston.com
Patients adding pounds toqualify for surgery
Patients who fall short of the poundsneeded to qualify for weight-loss surgeryare eating more to gain pounds.
Desperate patients turned down forthe surgery are returning to their doc-tors weeks or months later after inten-tionally gaining 10, 15, or even 25pounds to qualify.
This new phenomenon is one reasonthat the American Society for BariatricSurgery (ASBS) decided to hold a majorconference next spring to re-evaluateguidelines for who qualifies for thesurgery, according to the July 8 WallStreet Journal.
Presently to qualify, a patient must beat least 100 pounds overweight or have abody mass index of at least 40.
Surgeons say the guidelines forbariatric surgery need to be re-evaluatedbecause severely overweight patientsinevitably will develop serious problemseven if they aren�t yet 100 pounds over-weight. ❖�www.wsj.com. A subscription is required.