recommendations of the canadian nurse practitioner...
TRANSCRIPT
RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE
PROGRESS REPORT
December 2009

This report has been prepared by CNA to provide information on a particular topic or topics. The views and opinions expressed in this report do not necessarily reflect the
views of the CNA board of directors.
Funding for this publication was provided by Health Canada. The opinions expressed in this publication are those of the authors and do not necessarily reflect the official views of Health Canada.
All rights reserved. No part of this document may be reproduced, stored in a retrieval system, or transcribed, in any form or by any means, electronic, mechanical, photocopying,
recording, or otherwise, without written permission of the publisher.
© Canadian Nurses Association
50 Driveway Ottawa, ON K2P 1E2
Tel.: 613-237-2133 or 1-800-361-8404
Fax: 613-237-3520
Website: www.cna-aiic.ca
December 2009
ISBN 978-1-55119-321-2
Photos: Greg Teckles Photography Inc.
CANADIAN NURSES ASSOCIATION 1
TABLE OF CONTENTS
Executive Summary 3
Introduction 4
Methods 5
Findings 7
Response Rates 7
Project Data: Responses Concerning the 84 Actions 8
Strategic Area: Legislation and Regulation 8
Strategic Area: Practice 15
Strategic Area: Health Human Resource Planning 16
Strategic Area: Education 19
Strategic Area: Strategic Communications, Change Management and Social Marketing 24
Strategic Area: Evaluation 26
Strategic Area: Governance 26
Project Data: Broad Questions 27
Discussion 29
Summary of Findings 29
Outstanding Key Issues 31
Legislation and Regulation 31
Practice 31
Health Human Resource Planning 32
Education 32
Change Management 32
Social Marketing and Strategic Communication 33
The Need for an Updated Plan of Action 33
Stakeholders 34
Provincial/Territorial Jurisdictions 34
Principal Nursing Advisers and Other Nursing Representatives from the Federal/Provincial/Territorial Governments 34
Nurse Practitioner (NP) Associations (Provincial and Territorial) or Nurse Practitioner Contacts 36
Representatives of Nurse Education Programs for NPs in Canada 37
Other Stakeholders 39
References 40


CANADIAN NURSES ASSOCIATION 3
EXECUTIVE SUMMARY
In the first three months of 2009, the Canadian Nurses Association (CNA) consulted with stakeholders and analyzed the progress made on meeting the recommendations generated from the 2006 Canadian Nurse Practitioner Initiative (CNPI). Questionnaires were developed on the basis of the action plan the CNPI proposed in its report The Way Forward Plan: Committing to Action (CNA, 2006h). Results indicate that more than half of the actions have been fully or partially completed since 2006, and that several key actions remain in progress or are not completed.1 Details of these results are presented in this report.
This report is limited in that some jurisdictions were over-represented during the consultation process, whereas others did not have adequate representation from all stakeholder groups. Information from the consultations suggests, however, that many of the issues now faced in relation to the continued implementation of the nurse practitioner role require collaboration across jurisdictions and sectors if they are to be successfully resolved.
In The Way Forward Plan, the CNPI proposes the development of a multi-stakeholder, multi-jurisdictional coordinating committee. Supporters and participants were concerned that key stakeholders would act independently rather than implement the CNPI’s recommendations from a pan-Canadian perspective, and that it would not be possible to achieve systemic change if a traditional jurisdictional implementation approach was followed.
Health Canada’s Office of Nursing Policy has taken the first step toward achieving systemic change by asking CNA to carry out this review of the status of the CNPI’s recommendations. Many outstanding key issues described in this report will need further discussion. It is recommended that the Office of Nursing Policy consider convening a multi-stakeholder, multi-jurisdictional forum to review the current CNPI list of recommendations and actions and develop an updated action plan with clear, achievable goals.
1 Four status levels concerning the recommended key actions are used in this report: (1) “completed,” all activities completed; (2) “partially completed,” activities have been implemented to some extent; (3) “action ongoing,” activities in the process of being conducted; and (4) “not completed,” no actions reported.
4 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
INTRODUCTION
As part of its commitment to provide better access to primary health services to all Canadians, the government of Canada created the Primary Health Care Transition Fund (PHCTF) (CNA, 2006g) in 2004. The fund provided $8.9 million in financial support to the Canadian Nurse Practitioner Initiative (CNPI), which had an 18-month mandate to develop a pan-Canadian framework to support the sustained integration of the nurse practitioner (NP) role into Canada’s health-care system. NPs play an important role in health care: they are “registered nurses with additional educational preparation and experience who possess and demonstrate the competencies required to autonomously diagnose, order and interpret diagnostic tests, prescribe pharmaceuticals and perform specific procedures within their legislated scope of practice” (CNA, 2006d, p. 19).
In June 2006, the CNPI published Nurse Practitioners: The Time is Now, a report containing 13 recommendations to integrate NPs into the Canadian health-care system. The CNPI then produced The Way Forward Plan: Committing to Action (CNA, 2006h) to map out the next steps required to implement the recommendations so that the CNPI vision for the NP role could become a reality. A detailed plan can be found in Appendix B, Nurse Practitioner National Implementation Plan: Suggested Roll-out (CNA, 2006a). This plan includes 84 actions for the 13 CNPI recommendations, grouped into the following seven strategic areas: legislation and regulation; practice; health human resource planning; education; strategic communications, change management and social marketing; evaluation; and governance. For each of the 84 actions, the implementation plan identifies a priority, timeline, lead or co-lead and key supporting stakeholder groups.
CNA was the sponsoring organization for the CNPI and continues to promote the implementation of the NP role in Canada. The provinces and territories have worked with the CNPI recommendations and while some progress is apparent, there has been no national coordinated effort nor information compiled recording any success in implementing the recommendations from a pan-Canadian perspective. There was some concern, however, among supporters and participants of the CNPI that the resulting recommendations would not be implemented across Canada (CNA, 2006h).
The Canadian Nurses Association (CNA)’s vision is as follows: “Registered nurses: leaders and partners working to advance health for all.” One of CNA’s strategic goals in pursuit of this vision is to promote awareness of the nursing profession so that the roles and expertise of registered nurses are understood, respected and optimized within the health-care system. From January to March 2009, CNA led a project to document the status of the 13 CNPI recommendations with the aim of providing current data for decision-makers and stakeholders such as federal/provincial/territorial (F/P/T) governments, provincial/territorial (P/T) nursing regulatory colleges and associations, nursing professional groups and nursing educational associations.
CNA consulted with representatives from governments and nursing organizations, regulators, educators and NPs across Canada. The results of this project are presented in this report. The current status of each of the actions identified by the CNPI is presented and key outstanding issues are identified from the report. Decision-makers and stakeholders will be able to use these data to redefine priorities for the support of the NP role in the Canadian health-care system.

CANADIAN NURSES ASSOCIATION 5
METHODS
The Nurse Practitioner National Implementation Plan: Suggested Roll-out was used by CNA as the basis for the questions used in the consultations (CNA, 2006a). To ascertain the current status, questions were developed relating to each of the 84 action items. The status of each of the following eight actions, identified by strategic area and key action number, was not investigated because they were deemed to be too broad for this project.
• Develop and implement a framework to facilitate the practice of extended/expanded role of registered nurses. (Legislation and regulation, 19)
• Reflect the guiding philosophy, assumptions and values found in the Education Framework for Nurse Practitioners in Canada. (Education, 38)
• Develop philosophy, mission and goal statements that are aligned with pan-Canadian frameworks governing NP education and periodically assess and review them. (Education, 43)
• Be responsive to broadly defined, evidence-based stakeholder needs. (Education, 46)
• Develop preceptor preparation programs. (Education, 57)
• Implement evidence-based student evaluation and testing methodologies. (Education, 62)
• Establish a pan-Canadian resource bank, including approaches and tools. (Education, 63)
• Implement cross-jurisdictional collaboration among schools and regulatory bodies to ensure that the licensure-to-practice process for NP students is supported by NP educational program content and teaching and learning processes. (Education, 64)
CNA identified the stakeholders (leads, co-leads or key supporting stakeholder groups) for each of the actions, then prepared an individualized questionnaire relating to the actions for each group as identified in the implementation plan. A number of actions were designated to be undertaken by more than one stakeholder group, and thus there was some overlap among the questionnaires. Questionnaires were tailored for representatives of each of the following stakeholder groups:
• principal nursing advisers and other nursing representatives from F/P/T governments in Canada;
• educational programs for NPs in Canada;
• Canadian Association of Schools of Nursing (CASN);
• nursing regulatory bodies and CNA jurisdictional members representing each province and territory;
• Canadian Health Services Research Foundation/Canadian Institute of Health Research (CHSRF/CIHR) Chair Program in Advanced Practice Nursing;
• Canadian Nurses Protective Society (CNPS);
• Canadian Federation of Nurses Unions (CFNU);
• CNA;
6 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
• Health Canada’s Office of Nursing Policy;
• the Canadian Association of Advanced Practice Nurses (CAAPN), provincial NP associations and interest groups; and
• NPs across Canada.
Five questionnaires were developed using the SurveyMonkey software. The questionnaires were piloted with NPs and representatives from CASN, CNA and others. The questionnaires were translated, except for the ones prepared for unilingual respondents. Data collection with all stakeholders occurred between January 26 and February 20, 2009, and in June 2009. The majority of data were collected through an electronic survey program. Some of the data were collected by e-mail or during semi-structured interviews as a number of questionnaires had fewer than five stakeholders. Additional data from an unpublished discussion document on the regulation of NPs in Canada, Regulation of Nurse Practitioners in Canada: A Discussion Document, were used to document findings related to the CNPI’s strategic area of legislation and regulation.
Additional summary questions were asked of five groups of respondents: (1) principal nursing advisers and other nursing representatives from F/P/T governments in Canada; (2) representatives of nursing regulatory bodies and CNA jurisdictional members; (3) representatives of the Canadian Association of Advanced Practice Nurses, provincial NP associations and interest groups; (4) NPs; and (5) representatives of educational programs for NPs in Canada. The questions were meant to identify changes that had occurred since 2006 on meeting the CNPI’s recommendations and to identify the current priorities of these respondents. Customized to each group, the questions were to encourage respondents to answer from the perspective of their own organization and role. They were:
• Since the CNPI project made its recommendations in 2006, what have been the major changes?
• What do you see as the key priorities?
In addition, NPs were asked:
• What supports are important in establishing your NP practice?
• Describe any barriers that you are experiencing in your current role as an NP.
Employers of NPs were identified in the implementation plan as the leads or co-leads for a number of actions, and were not consulted for the present project because of time constraints. Instead, NPs were asked questions concerning their employer, where appropriate. The Mutual Recognition Agreement (MRA) working group was formed early in 2006 by the P/T regulatory bodies and CNA to plan and facilitate the development of a new MRA for RN and NP regulation in Canada. The second phase of the project began in 2008. The P/T regulatory bodies met to facilitate the movement of NPs from one jurisdiction to another within Canada. The MRA working group gave CNA permission to use the data that were collected as part of the MRA discussions in the development of this report. Where possible, these data were used so that CNA could avoid collecting duplicate data from regulators. Except for information that is publicly available, data in this report were validated by stakeholders.
CANADIAN NURSES ASSOCIATION 7
2 This is to minimize bias in the data collection process as CNA was the project leader.
FINDINGS
Response Rates
All 12 P/T principal nursing advisers were sent a questionnaire, as were the following federal agencies: First Nations and Inuit Health Branch and Office of Nursing Policy at Health Canada, Veterans Affairs Canada, Department of National Defence and Correctional Service of Canada. Nineteen responses were received from this group, including responses from all of the P/T principal nursing advisers, except Quebec. This sample provides a pan-Canadian perspective of P/T opinions from governments and federal agencies.
A questionnaire was sent to all nursing regulatory bodies and CNA jurisdictional members. The regulatory bodies in all of the provinces and territories responded, except Quebec, resulting in a total of 11 responses.
A questionnaire was sent to CAAPN and to NP associations and interest groups in nine of the provinces (Prince Edward Island does not have an association or interest group of NPs). Some associations and interest groups provided multiple responses, some associations provided a single response and some did not respond, so the sample does not provide a pan-Canadian perspective. A total of 23 responses were received in this category.
NP associations were asked to send the NP questionnaire to NPs in their province. In areas where there is no formal NP interest group (territories and Prince Edward Island), key contacts in these jurisdictions were asked to forward the questionnaire to NPs in their territory or province. Yukon has recently enacted legislation to implement the NP role; however Yukon was not represented in this sample. According to a 2009 report from nursing regulatory bodies, there are approximately 2,000 NPs in Canada; 44 responses were received, for a response rate of approximately 2%. The number of responses was insufficient to permit analysis of the data by jurisdiction, but the responses provide common areas and some differences between the provinces and territories.
A questionnaire was sent to all directors of educational programs for NPs. The list of programs used in this project was validated by CASN. Responses were received from at least one educational program for NPs in almost every province. (There are currently no educational programs for NPs offered in Prince Edward Island, Nunavut and Yukon.) Responses were received from 15 of the 28 schools, for a response rate of 54%. One jurisdiction is not represented in the findings.
Responses were also received from the CHSRF/CIHR Chair Program in Advanced Practice Nursing, CNPS, CASN, CFNU, and CNA. The people consulted from CNA were not involved in the data collection processes.2
8 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
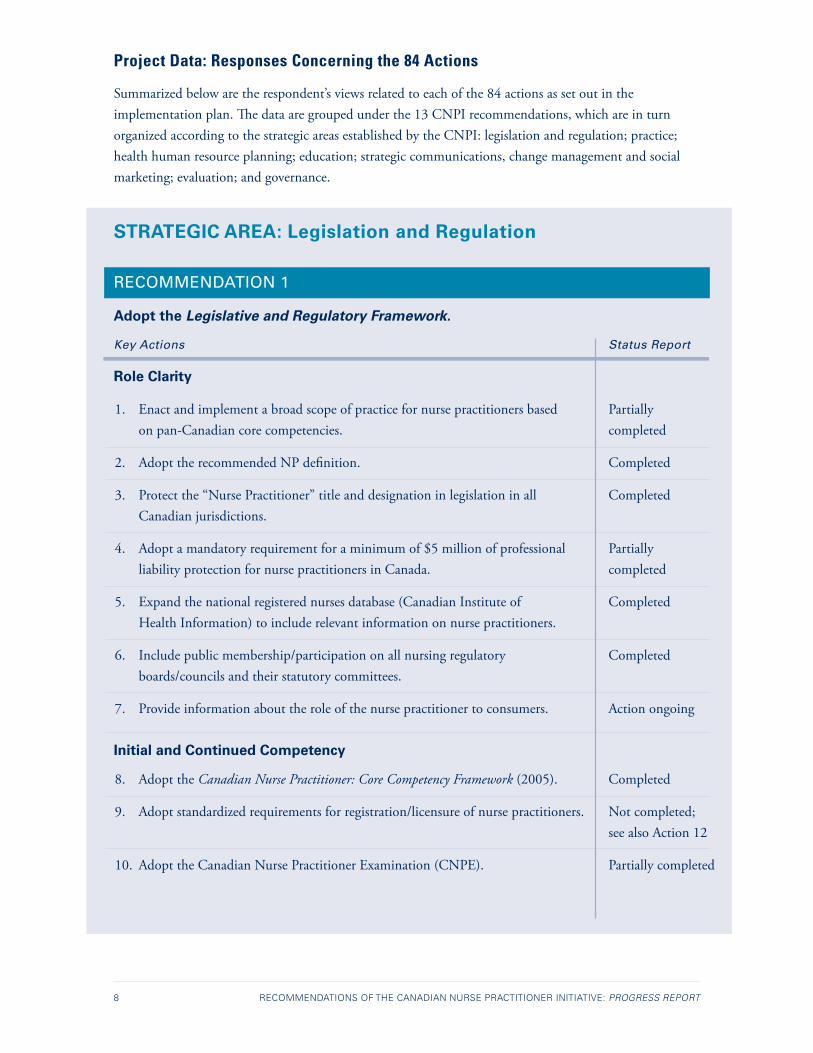
Project Data: Responses Concerning the 84 Actions
Summarized below are the respondent’s views related to each of the 84 actions as set out in the implementation plan. The data are grouped under the 13 CNPI recommendations, which are in turn organized according to the strategic areas established by the CNPI: legislation and regulation; practice; health human resource planning; education; strategic communications, change management and social marketing; evaluation; and governance.
STRATEGIC AREA: Legislation and Regulation
RECOMMENDATION 1
Adopt the Legislative and Regulatory Framework.
Key Actions Status Report
Role Clarity
1. Enact and implement a broad scope of practice for nurse practitioners based Partially on pan-Canadian core competencies. completed
2. Adopt the recommended NP definition. Completed
3. Protect the “Nurse Practitioner” title and designation in legislation in all Completed Canadian jurisdictions.
4. Adopt a mandatory requirement for a minimum of $5 million of professional Partially liability protection for nurse practitioners in Canada. completed
5. Expand the national registered nurses database (Canadian Institute of Completed Health Information) to include relevant information on nurse practitioners.
6. Include public membership/participation on all nursing regulatory Completed boards/councils and their statutory committees.
7. Provide information about the role of the nurse practitioner to consumers. Action ongoing
Initial and Continued Competency
8. Adopt the Canadian Nurse Practitioner: Core Competency Framework (2005). Completed
9. Adopt standardized requirements for registration/licensure of nurse practitioners. Not completed; see also Action 12
10. Adopt the Canadian Nurse Practitioner Examination (CNPE). Partially completed
CANADIAN NURSES ASSOCIATION 9
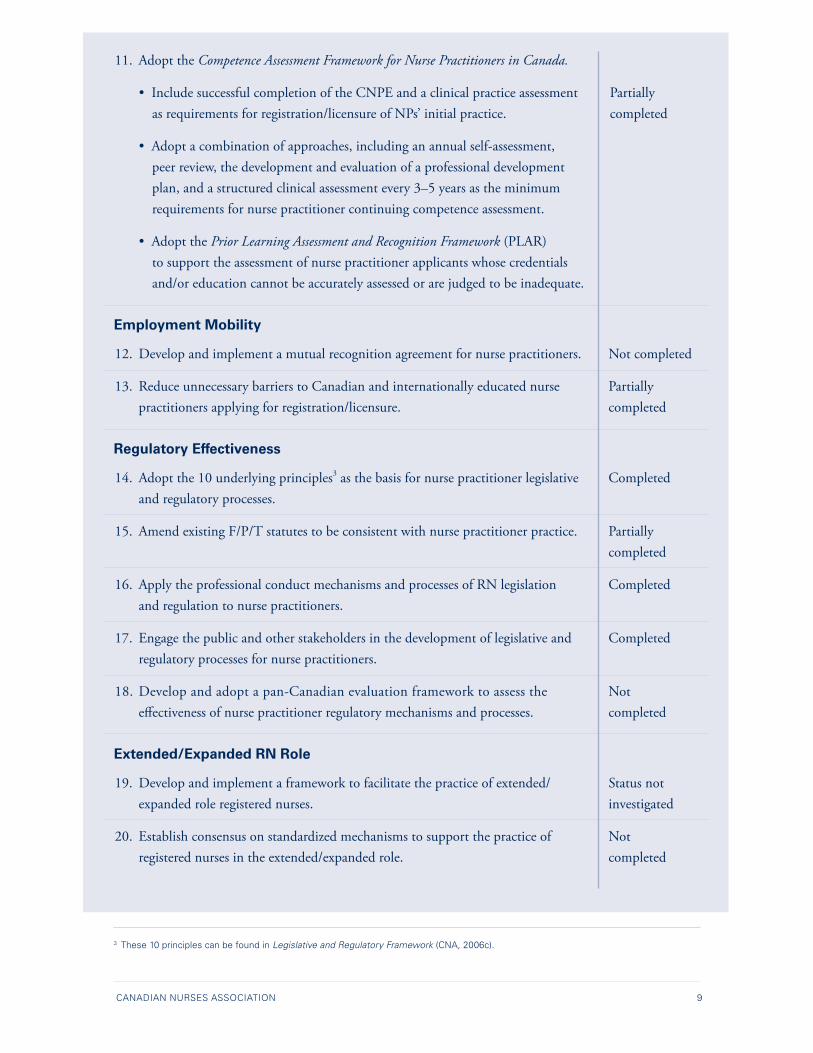
11. Adopt the Competence Assessment Framework for Nurse Practitioners in Canada.
• Include successful completion of the CNPE and a clinical practice assessment Partially as requirements for registration/licensure of NPs’ initial practice. completed
• Adopt a combination of approaches, including an annual self-assessment, peer review, the development and evaluation of a professional development plan, and a structured clinical assessment every 3–5 years as the minimum requirements for nurse practitioner continuing competence assessment.
• Adopt the Prior Learning Assessment and Recognition Framework (PLAR) to support the assessment of nurse practitioner applicants whose credentials and/or education cannot be accurately assessed or are judged to be inadequate.
Employment Mobility
12. Develop and implement a mutual recognition agreement for nurse practitioners. Not completed
13. Reduce unnecessary barriers to Canadian and internationally educated nurse Partially practitioners applying for registration/licensure. completed
Regulatory Effectiveness
14. Adopt the 10 underlying principles3 as the basis for nurse practitioner legislative Completedand regulatory processes.
15. Amend existing F/P/T statutes to be consistent with nurse practitioner practice. Partially completed
16. Apply the professional conduct mechanisms and processes of RN legislation Completed and regulation to nurse practitioners.
17. Engage the public and other stakeholders in the development of legislative and Completed regulatory processes for nurse practitioners.
18. Develop and adopt a pan-Canadian evaluation framework to assess the Not effectiveness of nurse practitioner regulatory mechanisms and processes. completed
Extended/Expanded RN Role
19. Develop and implement a framework to facilitate the practice of extended/ Status not expanded role registered nurses. investigated
20. Establish consensus on standardized mechanisms to support the practice of Not registered nurses in the extended/expanded role. completed
3 These 10 principles can be found in Legislative and Regulatory Framework (CNA, 2006c).
10 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
This strategic area included actions 1 to 20 from the implementation plan, and the questionnaires sent to representatives of regulatory bodies and CNA jurisdictional members included questions on these 20 actions. Other groups (i.e., CNA, CNPS, principal nursing advisers and other nursing representatives from F/P/T governments, CAAPN, NP associations) were identified as stakeholders for some of these actions related to legislation and regulation in the implementation plan and, thus, their questionnaires included questions concerning the relevant actions. Eight of the 20 actions have been completed, six have been partially completed, one was classified as ongoing, four have not been completed and one was not included in the questionnaires.
The CNPI technical report Legislative and Regulatory Framework (CNA, 2006d) promotes a consistent approach to the legislation and regulation of NPs in all Canadian jurisdictions. The following is a summary of the findings for each of the 20 actions in the legislation and regulation strategic area.
Role Clarity
All respondents agreed that a broad scope of practice for NPs based on pan-Canadian core competencies should be enacted and implemented. One jurisdiction has further elaborated the core competencies and specified how the competencies are applied in practice within the three NP registration categories: NP family/all ages, NP (adult) and NP (pediatric). Implementation of broad core competencies has been partially completed: half of the respondents reported that this action has not been achieved within their jurisdictions. Some respondents commented that legislative changes were currently underway in their jurisdictions. Implementation of the NP scope of practice hinges on governmental support for putting in place legislative changes to enable a broad scope of practice. The respondents indicated that further work is needed before NPs can be given a broad scope of practice within the prescribing authority. There are restrictions that limit the ability to prescribe controlled substances and to initiate prescribing in in-patient tertiary care settings. Allowing NPs to prescribe controlled substances and changing some of the jurisdictional legislation would enable NPs to practise within their scope of practice in in-patient tertiary care settings.
The CNPI’s definition of “nurse practitioner” is integrated into the policy documents of CNA and its jurisdictional associations. Respondents from some representatives of regulatory bodies and CNA jurisdictional members noted that elements of the definition have been used in publications produced by their own organization, standards of practice and framework documents. The title “Nurse Practitioner” is now protected in all Canadian jurisdictions in which NP legislation exists.
Most NP registrants have liability protection of $5 million, as recommended by the CNPI, through their registration as an NP. However, this is not the case in Ontario and Quebec. Liability coverage in Quebec is offered through a private insurer. In Ontario, NPs obtain liability coverage with CNPS through the Registered Nurses’ Association of Ontario or their employer.
The Canadian Institute for Health Information (CIHI) collects data on NPs, although respondents made suggestions to improve and expand these data, such as adding an NP registration category. The NP registration category is different in some jurisdictions and includes specialty streams. Other suggestions were to add questions on workload benchmarks for NPs, and to add a report on NPs whose registration has lapsed and who would like to practise again.
CANADIAN NURSES ASSOCIATION 11
The public is involved in NP legislation and regulation through membership on regulatory boards and councils in all jurisdictions.
Respondents from six representatives of regulatory bodies and CNA jurisdictional members reported that they provide information about the NP role to consumers. The CNA website includes a number of documents related to NPs, such as fact sheets, position statements and CNPI documents, and several organizations are working to develop information targeted to the public. CNA reported research results indicating that the public’s awareness of NPs has not changed significantly since 2006 (Decima, 2006 & Ekos, 2008).
Initial and Continued Competency
The CNPI’s Canadian Nurse Practitioner: Core Competency Framework (CNA, 2005b) has been adopted by the majority of regulators. A respondent from one regulatory body questioned whether the framework can stand alone as the standard for the educational preparation of NPs and the assessment of applicants for registration.
There is agreement in principle among regulators that standardized requirements for registration/licensure should be adopted, but this will require significant work. Consistency of educational preparation, scope of practice, assessment processes and streams or registration categories of NPs has not yet been achieved.
Some of the actions in this section refer to another CNPI technical report: Competence Assessment Framework for Nurse Practitioners in Canada (CNA, 2006b). The recommendations from this framework have been only partially met. There is variation in the initial assessment processes for NPs, including prior learning assessment and recognition (PLAR) processes and the types and kinds of examinations. Most jurisdictions have a continuing competence program, but only two require a clinical assessment every three to five years. A number of jurisdictions are in the process of planning such a requirement.
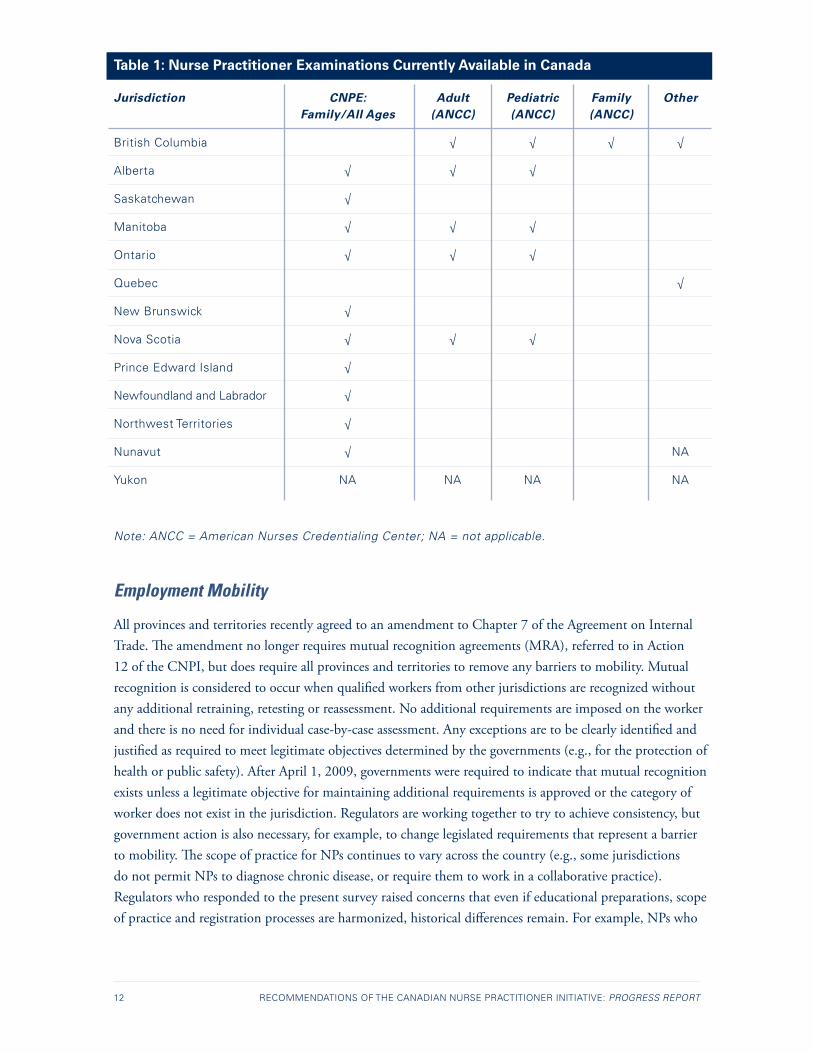
There was general agreement among the respondents that an examination is required to practise as an NP, but some respondents from two jurisdictions questioned whether the current Canadian Nurse Practitioner Examination: Family/All Ages (CNPE: F/AA) is adequate, or whether a clinical examination should also be required. Progress has been made in reaching some consensus on the streams or registration categories of NPs, although there are still some differences across the country (see Table 1). Written examinations are now available for three categories: NP family/all ages, NP (adult) and NP (pediatric). The CNPE: F/AA is used in 8 of 10 provinces. (The territories register NPs after they have been registered elsewhere in Canada.) One jurisdiction uses the American Nurses Credentialing Center (ANCC) Family exam, while five jurisdictions use the ANCC adult and pediatric NP exams (J. Barry, personal communication, 2009), and another jurisdiction has developed its own exams for its registration categories. Two jurisdictions require all NP applicants to successfully complete the Objective Structured Clinical Examination (OSCE) for their registration categories.
A pan-Canadian assessment centre has not yet been established. Respondents from six representatives of regulatory bodies and CNA jurisdictional members supported this initiative; they believed that such a centre would be helpful for international applicants and for the development of common standards for assessment in Canada under the Agreement on Internal Trade.
12 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
Table 1: Nurse Practitioner Examinations Currently Available in Canada
Jurisdiction CNPE: Adult Pediatric Family Other Family/All Ages (ANCC) (ANCC) (ANCC)
British Columbia √ √ √ √
Alberta √ √ √
Saskatchewan √
Manitoba √ √ √
Ontario √ √ √
Quebec √
New Brunswick √
Nova Scotia √ √ √
Prince Edward Island √
Newfoundland and Labrador √
Northwest Territories √
Nunavut √ NA
Yukon NA NA NA NA
Note: ANCC = American Nurses Credentialing Center; NA = not applicable.
Employment Mobility
All provinces and territories recently agreed to an amendment to Chapter 7 of the Agreement on Internal Trade. The amendment no longer requires mutual recognition agreements (MRA), referred to in Action 12 of the CNPI, but does require all provinces and territories to remove any barriers to mobility. Mutual recognition is considered to occur when qualified workers from other jurisdictions are recognized without any additional retraining, retesting or reassessment. No additional requirements are imposed on the worker and there is no need for individual case-by-case assessment. Any exceptions are to be clearly identified and justified as required to meet legitimate objectives determined by the governments (e.g., for the protection of health or public safety). After April 1, 2009, governments were required to indicate that mutual recognition exists unless a legitimate objective for maintaining additional requirements is approved or the category of worker does not exist in the jurisdiction. Regulators are working together to try to achieve consistency, but government action is also necessary, for example, to change legislated requirements that represent a barrier to mobility. The scope of practice for NPs continues to vary across the country (e.g., some jurisdictions do not permit NPs to diagnose chronic disease, or require them to work in a collaborative practice). Regulators who responded to the present survey raised concerns that even if educational preparations, scope of practice and registration processes are harmonized, historical differences remain. For example, NPs who
CANADIAN NURSES ASSOCIATION 13
were assessed and registered before the harmonization had to meet different registration requirements, with some jurisdictions not requiring an examination, or where the scope of practice was expanded and additional regulatory oversight was not implemented.
Regulatory Effectiveness
The CNPI legislative and regulatory framework recommends 10 principles for NP legislative and regulatory processes. The respondents from P/T regulatory bodies agreed with the 10 principles but noted that their implementation required support from government. For example, Principle 6 states, “The framework promotes sufficient rigor to ensure safe practice by autonomous nurse practitioners with a broad scope of practice” (CNA, 2006c, p. 19). Some of the respondents reported regulatory changes that support a broad scope of practice in their jurisdiction. Others reported that further changes in legislation and regulation are needed to achieve this goal. One regulatory body raised the same issue of concern for public safety when the scope is expanded and a commensurate increase in regulatory oversight is not implemented.
There has been little change in most jurisdictions regarding the inclusion of NPs in legislation for hospitals, workers’ compensation and motor vehicles. The federal government has not yet implemented the regulation that allows NPs to prescribe controlled substances. There are also barriers to NP practice within federal policies, such as the unemployment insurance and disability forms. Examples of federal legislation that omits nurse practitioners include:
• Narcotic Control Regulations under the Controlled Drugs and Substances Act;
• Canada Pension Plan Disability policies to complete the medical report section of the benefits application form;
• Employment Insurance disability benefits medical report section of the benefits application form; and
• Food and Drugs Act regulations that do not allow NPs to distribute drug samples to their clients.
These federal laws have created significant barriers to nursing practice. NPs are not able to provide full range of care to their clients. The majority of respondents from F/P/T governments reported changes related to the Registered Nurses Act and the Pharmacy Act that directly relate to NP prescribing authority. Others are concerned with the inability of NPs to prescribed narcotics.
All regulators apply professional conduct mechanisms and processes of registered nurse legislation and regulation to NPs. In addition, there is consensus on the engagement of the public and other stakeholders in the development of legislative and regulatory processes for NPs.
The development of a pan-Canadian evaluation framework to assess the effectiveness of NP regulatory mechanisms and processes has not been completed, but there is ongoing dialogue on this issue.
14 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
Extended/Expanded RN Role
During the CNPI’s consultations, a number of concerns were raised about the work of RNs who were practising in expanded roles that included skills common to the nurse practitioner role but did not meet the requirements for registration as an NP (CNA, 2005a). This concern was mainly related to RN practice in northern and remote communities where this role is evolving. In fact, one jurisdiction offers NP services for on-call support for RNs in these practice areas. It was recommended that standardized mechanisms to support such practice be developed. This has not occurred; however, many jurisdictions continue to authorize these activities through some form of delegation from physicians.
Two jurisdictions include this expanded role in the scope of practice for RNs. One indicated that their jurisdiction’s Health Professions Act enables the regulatory body to register an RN in a separate class of practice called “certified practice.” RNs in this class must have successfully completed a certified practice course and exit evaluation approved by the regulatory body and must apply to the regulatory body for certified practice designation. Rural remote practice is one of the designations.
The results of this project indicate that the following five actions from the legislation and regulation strategic area have not been completed:
1. Identify barriers to employment mobility and look for ways to remove these barriers or to apply for exemptions under legitimate objectives. Develop and implement an MRA for NPs.
2. Adopt standardized requirements for registration/licensure of NPs.
3. Amend existing F/P/T statutes to be consistent with NP practice.
4. Develop and adopt a pan-Canadian evaluation framework to assess the effectiveness of NP regulatory mechanisms and processes.
5. Establish consensus on standardized mechanisms to support the practice of RNs in the extended/expanded role.
CANADIAN NURSES ASSOCIATION 15
STRATEGIC AREA: Practice
RECOMMENDATION 2
Adopt the Practice Framework for Nurse Practitioners in Canada in order to facilitate consistency in F/P/T approaches to practice.
Key Actions Status Report
Role Clarity
21. Adopt the CNPI NP role description. Partially completed
Interprofessional Collaborative Practice
22. Develop and implement clear policy direction for models of interprofessional Partially primary health-care (PHC) service delivery and a supportive change completed management strategy.
Liability for All Health-Care Professionals Including Nurse Practitioners
23. Ensure all health professionals have liability insurance protection. Partially • Explore interprofessional team liability coverage. completed
24. P/T governments cover the costs of professional practice and liability protection Partially as is done for other professionals in the province. completed
25. Establish a national voluntary database to track claims and payments made Not against health providers, including NPs. completed
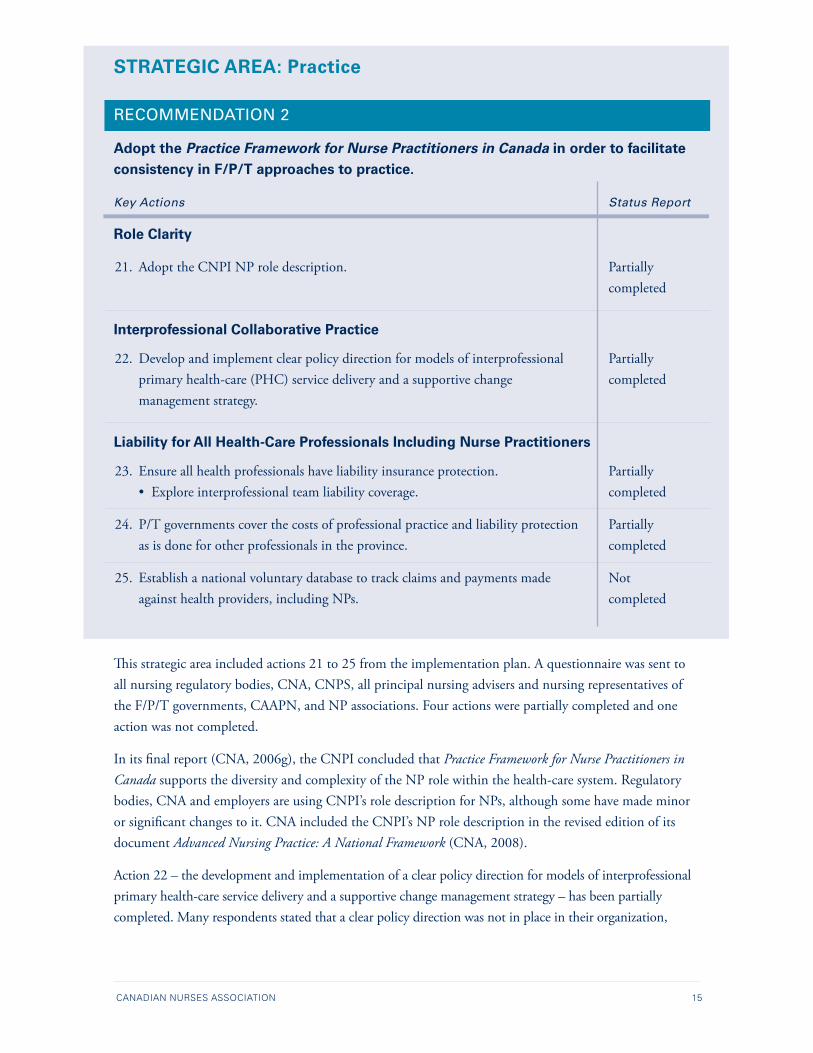
This strategic area included actions 21 to 25 from the implementation plan. A questionnaire was sent to all nursing regulatory bodies, CNA, CNPS, all principal nursing advisers and nursing representatives of the F/P/T governments, CAAPN, and NP associations. Four actions were partially completed and one action was not completed.
In its final report (CNA, 2006g), the CNPI concluded that Practice Framework for Nurse Practitioners in Canada supports the diversity and complexity of the NP role within the health-care system. Regulatory bodies, CNA and employers are using CNPI’s role description for NPs, although some have made minor or significant changes to it. CNA included the CNPI’s NP role description in the revised edition of its document Advanced Nursing Practice: A National Framework (CNA, 2008).
Action 22 – the development and implementation of a clear policy direction for models of interprofessional primary health-care service delivery and a supportive change management strategy – has been partially completed. Many respondents stated that a clear policy direction was not in place in their organization,

16 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
and even more noted that a change management strategy had not been implemented. Some respondents described significant progress in this area, such as the development of models, and some indicated a need for more action. This area is critical to the integration of NPs and should be the focus of further investigation.
Action 23, which concerns liability protection and interprofessional team liability coverage, has been partially completed. Issues of liability protection have been clarified (refer to Role Clarity, under the legislation and regulation strategic area). As indicated, most NPs now have a minimum of $5 million in liability protection as part of their registration. However, as new team models develop, more consideration needs to be given to ensuring adequate liability coverage for all members of the health-care team – especially in the case of small employers in which a physician is the employer, and where NPs act as independent contractors. In response to the questionnaire, CNPS reported that there is no mechanism in Canada to track claims and payments made against health-care providers; it also indicated that each insurance company has its own database and information from these databases is not shared or disclosed for corporate security and competition issues. Progress on this action is unlikely to occur.
Action 24, which concerns P/T government coverage of the cost of professional practice and liability protection, has been partially completed. The liability protection for NPs is covered by the employer and the NP registration application fees.
STRATEGIC AREA: Health Human Resource (HHR) Planning
Recommendations 3 to 7 are included in this strategic area, along with 12 actions.
RECOMMENDATION 3
Conduct needs-based HHR planning for NPs using a pan-Canadian, interprofessional approach that is based on a conceptual framework. To support this planning, use the Health Human Resources Planning Simulation Model for NPs in Primary Health Care.TM
Key Actions Status Report
26. Secure long-term sustainable investment for the development of comprehensive Partially valid and reliable data to support HHR planning. completed
27. Develop a minimum data set to use the model. Not completed
Representatives of provincial nursing associations and governments were questioned about Action 26. Respondents reported that this action has not been completed except in one jurisdiction. However, there are many strategies established to recruit and retain NPs in some of the jurisdictions. CNA has not developed a minimum data set to use the model owing to a lack of resources.
CANADIAN NURSES ASSOCIATION 17
RECOMMENDATION 4
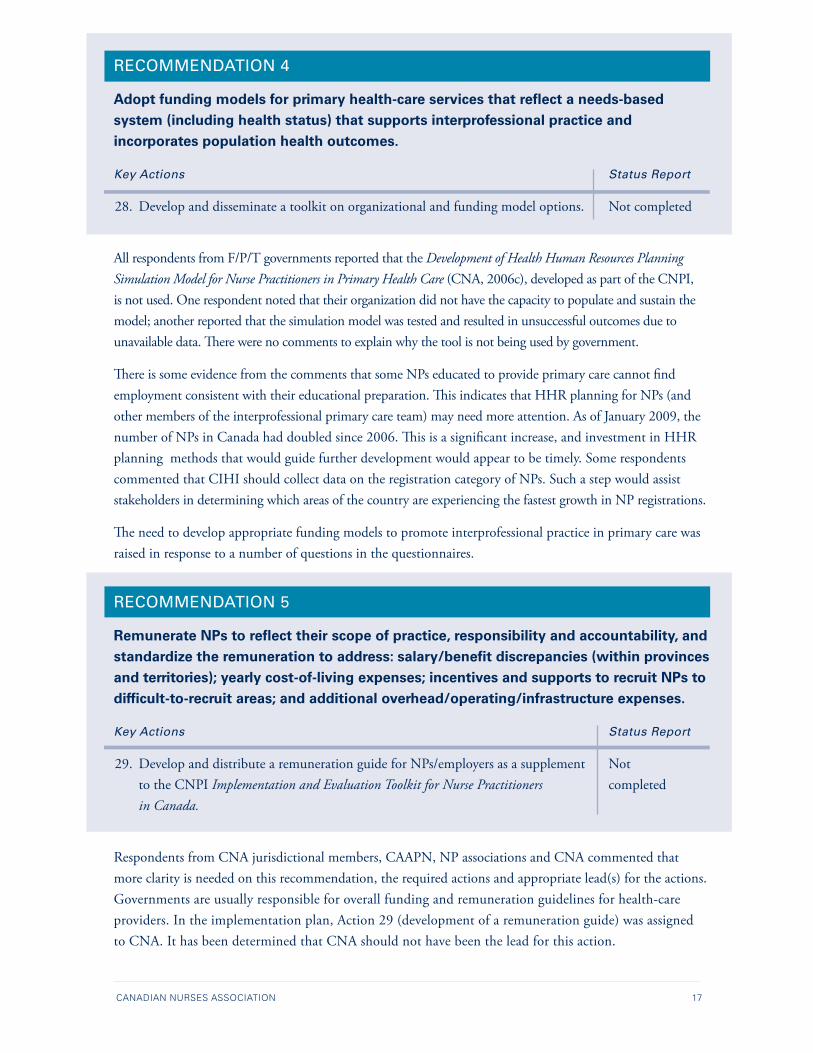
Adopt funding models for primary health-care services that reflect a needs-based system (including health status) that supports interprofessional practice and incorporates population health outcomes.
Key Actions Status Report
28. Develop and disseminate a toolkit on organizational and funding model options. Not completed
All respondents from F/P/T governments reported that the Development of Health Human Resources Planning Simulation Model for Nurse Practitioners in Primary Health Care (CNA, 2006c), developed as part of the CNPI, is not used. One respondent noted that their organization did not have the capacity to populate and sustain the model; another reported that the simulation model was tested and resulted in unsuccessful outcomes due to unavailable data. There were no comments to explain why the tool is not being used by government.
There is some evidence from the comments that some NPs educated to provide primary care cannot find employment consistent with their educational preparation. This indicates that HHR planning for NPs (and other members of the interprofessional primary care team) may need more attention. As of January 2009, the number of NPs in Canada had doubled since 2006. This is a significant increase, and investment in HHR planning methods that would guide further development would appear to be timely. Some respondents commented that CIHI should collect data on the registration category of NPs. Such a step would assist stakeholders in determining which areas of the country are experiencing the fastest growth in NP registrations.
The need to develop appropriate funding models to promote interprofessional practice in primary care was raised in response to a number of questions in the questionnaires.
RECOMMENDATION 5
Remunerate NPs to reflect their scope of practice, responsibility and accountability, and standardize the remuneration to address: salary/benefit discrepancies (within provinces and territories); yearly cost-of-living expenses; incentives and supports to recruit NPs to difficult-to-recruit areas; and additional overhead/operating/infrastructure expenses.
Key Actions Status Report
29. Develop and distribute a remuneration guide for NPs/employers as a supplement Not to the CNPI Implementation and Evaluation Toolkit for Nurse Practitioners completedin Canada.
Respondents from CNA jurisdictional members, CAAPN, NP associations and CNA commented that more clarity is needed on this recommendation, the required actions and appropriate lead(s) for the actions. Governments are usually responsible for overall funding and remuneration guidelines for health-care providers. In the implementation plan, Action 29 (development of a remuneration guide) was assigned to CNA. It has been determined that CNA should not have been the lead for this action.
18 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
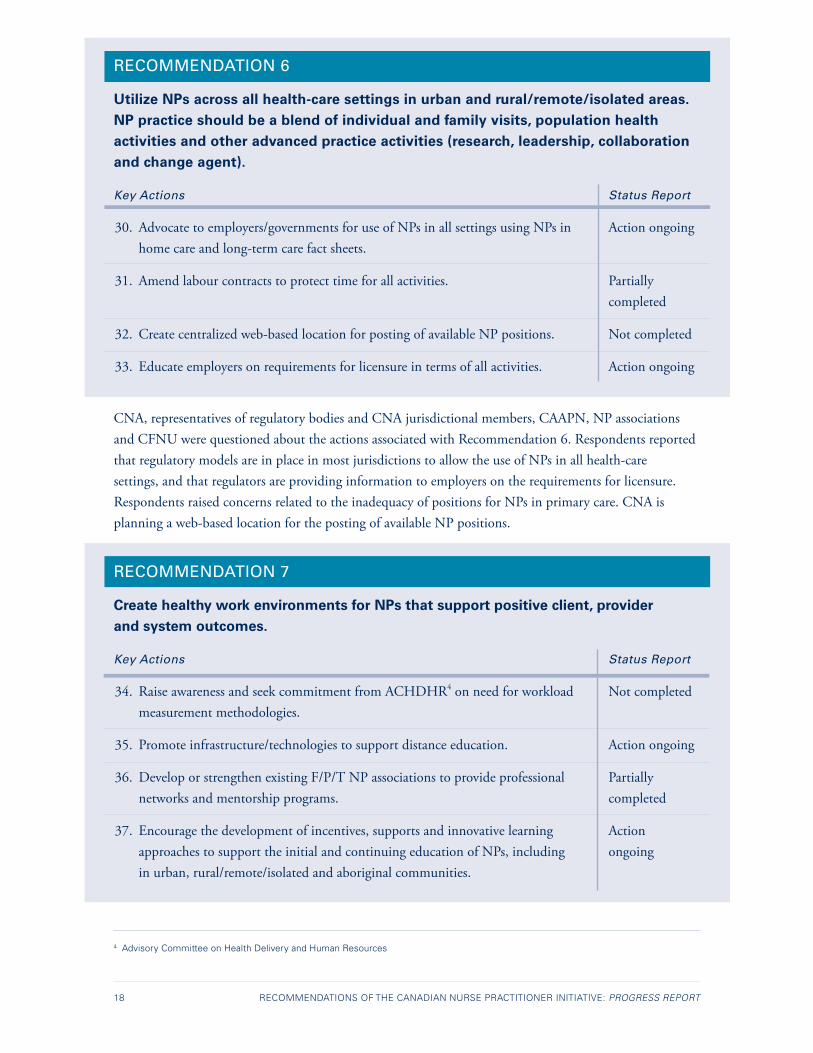
RECOMMENDATION 6
Utilize NPs across all health-care settings in urban and rural/remote/isolated areas. NP practice should be a blend of individual and family visits, population health activities and other advanced practice activities (research, leadership, collaboration and change agent).
Key Actions Status Report
30. Advocate to employers/governments for use of NPs in all settings using NPs in Action ongoing home care and long-term care fact sheets.
31. Amend labour contracts to protect time for all activities. Partially completed
32. Create centralized web-based location for posting of available NP positions. Not completed
33. Educate employers on requirements for licensure in terms of all activities. Action ongoing
CNA, representatives of regulatory bodies and CNA jurisdictional members, CAAPN, NP associations and CFNU were questioned about the actions associated with Recommendation 6. Respondents reported that regulatory models are in place in most jurisdictions to allow the use of NPs in all health-care settings, and that regulators are providing information to employers on the requirements for licensure. Respondents raised concerns related to the inadequacy of positions for NPs in primary care. CNA is planning a web-based location for the posting of available NP positions.
RECOMMENDATION 7
Create healthy work environments for NPs that support positive client, provider and system outcomes.
Key Actions Status Report
34. Raise awareness and seek commitment from ACHDHR4 on need for workload Not completedmeasurement methodologies.
35. Promote infrastructure/technologies to support distance education. Action ongoing
36. Develop or strengthen existing F/P/T NP associations to provide professional Partially networks and mentorship programs. completed
37. Encourage the development of incentives, supports and innovative learning Action approaches to support the initial and continuing education of NPs, including ongoing in urban, rural/remote/isolated and aboriginal communities.
4 Advisory Committee on Health Delivery and Human Resources
CANADIAN NURSES ASSOCIATION 19
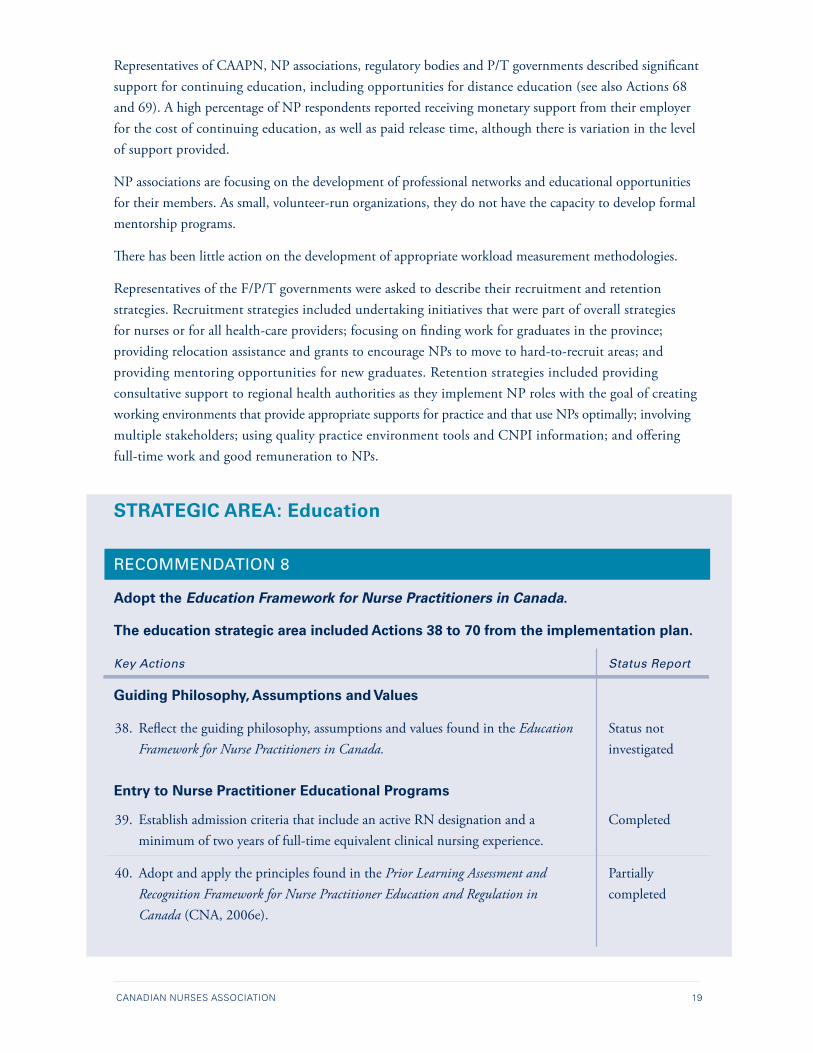
Representatives of CAAPN, NP associations, regulatory bodies and P/T governments described significant support for continuing education, including opportunities for distance education (see also Actions 68 and 69). A high percentage of NP respondents reported receiving monetary support from their employer for the cost of continuing education, as well as paid release time, although there is variation in the level of support provided.
NP associations are focusing on the development of professional networks and educational opportunities for their members. As small, volunteer-run organizations, they do not have the capacity to develop formal mentorship programs.
There has been little action on the development of appropriate workload measurement methodologies.
Representatives of the F/P/T governments were asked to describe their recruitment and retention strategies. Recruitment strategies included undertaking initiatives that were part of overall strategies for nurses or for all health-care providers; focusing on finding work for graduates in the province; providing relocation assistance and grants to encourage NPs to move to hard-to-recruit areas; and providing mentoring opportunities for new graduates. Retention strategies included providing consultative support to regional health authorities as they implement NP roles with the goal of creating working environments that provide appropriate supports for practice and that use NPs optimally; involving multiple stakeholders; using quality practice environment tools and CNPI information; and offering full-time work and good remuneration to NPs.
STRATEGIC AREA: Education
RECOMMENDATION 8
Adopt the Education Framework for Nurse Practitioners in Canada.
The education strategic area included Actions 38 to 70 from the implementation plan.
Key Actions Status Report
Guiding Philosophy, Assumptions and Values
38. Reflect the guiding philosophy, assumptions and values found in the Education Status notFramework for Nurse Practitioners in Canada. investigated
Entry to Nurse Practitioner Educational Programs
39. Establish admission criteria that include an active RN designation and a Completed minimum of two years of full-time equivalent clinical nursing experience.
40. Adopt and apply the principles found in the Prior Learning Assessment and PartiallyRecognition Framework for Nurse Practitioner Education and Regulation in completedCanada (CNA, 2006e).

20 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
41. Establish a pan-Canadian approach to transfer of credits. (Note: Educational Not completed institutions were asked about their transfer of credit policy in a question (see Action 42) relating to Action 42.)
42. Allow for the transfer of credits between educational institutions subject to Completed maximums established by the institutions.
Curriculum Alignment and Linkages
43. Develop philosophy, mission and goal statements that are aligned with Status not pan-Canadian frameworks governing NP education, and periodically assess investigated and review them.
44. Establish and promote participation in a pan-Canadian accreditation process Not completed for NP educational programs.
45. Develop linkages between accreditation and approval processes. Not completed
46. Be responsive to broadly defined, evidence-based stakeholder needs. Status not investigated
47. Be consistent with the Canadian Nurse Practitioner: Core Competency Framework Completed(CNA, 2005b) and the standards inherent in the NP program approval process.
48. Adopt the master’s degree (MN/MScN) as the required exit credential, ideally Partially by 2010, but no later than 2015. completed
49. Develop and institute bridging mechanisms to support program transition to Not completed a graduate degree (MN/MScN) as the standardized exit credential.
50. Develop and institute bridging mechanisms to support an individual’s Partially transition to a graduate degree. completed
Nurse Practitioner Education Delivery
51. Where practical, designate PhD-prepared practising NPs to teach NP-specific Completed courses. Where limited, facilitate access to PhD preparation, engage qualified masters-prepared NPs or non-NPs, and/or use team teaching or shared resource models.
52. Recognize NP faculty clinical hours as teaching hours. Partially completed
53. Establish and monitor guidelines governing NP educational program Completed faculty-student ratios.
54. Establish 700 hours as the standard minimum number of clinical practice hours. Completed

CANADIAN NURSES ASSOCIATION 21
55. Require clinical preceptors to be an NP or an advanced practice nurse or Completed equivalent subject matter expert in a relevant professional discipline with a sound understanding of the NP role.
56. Initiate a coordinated effort to sustain and increase the supply of available Partially preceptors. completed
57. Develop preceptor preparation programs. Status not investigated
58. Develop pan-Canadian standards for NP distance education. Not completed
59. Develop and deliver distance education courses for NPs. Completed
60. Develop innovative approaches to support collaborative programming and Partially pursue and implement funding for collaborative programming approaches. completed
61. Develop and offer interprofessional courses. Partially completed
62. Implement evidence-based student evaluation and testing methodologies. Status not investigated
63. Establish a pan-Canadian resource bank, including approaches and tools. Status not investigated
Licensure to Practice
64. Implement cross-jurisdictional collaboration among schools and regulatory bodies Status not to ensure that the licensure-to-practice process for NP students is supported by investigated NP educational program content and teaching and learning processes.
Transition to the Workplace
65. Develop and implement processes and structures to facilitate the transition of Partially NPs from their educational program to the workplace and from novice to expert. completed
66. Establish mentorship and a mentorship culture as standard features of the NP Completed learning experience.
67. Develop pan-Canadian mentorship tools and promote their use across all NP Not completed educational programs and in the workplace.
68. Create and support a culture of continuous learning among students and Action ongoing practising NPs.
69. Remove potential barriers to continuing education, including funding, time off, Partially and access to learning opportunities. completed
70. Develop refresher training programs, as required, for re-entry to practice. Not completed
22 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
The four main stakeholder groups consulted for this recommendation were the lead faculty members or directors of NP educational programs, representatives of CASN, representatives of the P/T regulatory bodies and NPs. In addition, other stakeholder groups, such as the principal nursing advisers and other nursing representatives from the F/P/T governments, CNA, CAAPN and NP provincial associations were questioned about some of the specific actions in this strategic area.
Of the 33 actions in this strategic area, nine were completed, nine were partially completed and seven were not completed. Seven of the actions were not investigated in the present project. One action is ongoing.
Education was identified by stakeholders during CNPI consultations as one of the key areas in the sustained integration of NPs. In its report, the CNPI identified variations amongst the NP educational programs (CNA, 2006g). These variations were responsible for the perception of inconsistencies in the education and competencies of graduating NPs. A consistent approach to education is needed to ensure that Canadians are confident that an NP is consistently prepared for the role throughout Canada.
The Education Framework for Nurse Practitioners in Canada (CNA, 2006f ) recommends six elements that must be considered in developing a pan-Canadian perspective on NP education. The CNPI-recommended actions relate to each of these six elements; relevant findings from the present study are presented below.
1. Guiding philosophy, assumptions and values
CNPI recommended that the guiding philosophy, assumptions and values of NP educational programs reflect those in the education framework (Action 38 from the implementation plan). This action was not measured in the present project because an in-depth analysis of the curriculum in NP educational programs would be required. CNA recommends that each institution assess its curriculum on the basis of the guiding philosophy, assumptions and values as recommended in the CNPI.
2. Entry to nurse practitioner educational programs
A harmonized entry requirement to NP educational programs is important for NP credibility and mobility. Results from this project demonstrate consistency in the amount of full-time equivalent clinical nursing experience required to enter NP educational programs: applicants must have an active RN registration and at least two years of experience as an RN. All NP educational programs stipulated that the completion of a BScN program was the minimum educational requirement – except for one, which is moving toward a master’s requirements by 2010.
The prior learning assessment and recognition (PLAR) process is important for RNs who were working in the NP role before changes were introduced to the educational requirements for NPs and the regulation of NPs. The CNPI defines PLAR as a “systematic process used to assess whether individuals possess the competencies necessary for obtaining educational credit or licensure ∕registration” (CNA, 2006e, p. 12). Only three educational programs reported using a PLAR process, and there has not been significant progress in expanding its availability since 2006.
CANADIAN NURSES ASSOCIATION 23
Results of this project indicate that there is still variability in the transfer-of-credit policies across institutions. Transfer-of-credit policies are determined at the institutional level, and faculties or schools of nursing do not have the authority to independently set policies in this area. Respondents provided examples of transfer-of-credit guidelines that varied from one to six credits. CASN noted another aspect of the transfer-of-credit issue: NP educational programs are not consistently delivered at a master’s level of education across the country. There is a need for a pan-Canadian approach to facilitate mobility of students between NP programs.
3. Curriculum alignment and linkages
There is currently no accreditation process for NP programs. CASN indicated that it does not see accreditation as a priority. One respondent from a regulatory body commented on the importance of a consistent program approval process across the country.
The Canadian Nurse Practitioner: Core Competency Framework (CNA, 2005b) is used by 93% of the respondents from NP educational programs within their curriculum. Respondents from institutions not using this framework reported that instead, they are using documents developed by the regulatory body in their jurisdiction.
Respondents from institutions offering NP educational programs not currently at the master’s level indicated that government action is required in their jurisdiction to support such a change. The CNPI recommends the master’s degree be adopted as the exit credential for NPs by 2010, but no later than 2015.
4. Nurse practitioner education delivery
The CNPI reports that the effectiveness of educational programs is directly related to the quality of the faculty delivering the courses (CNA, 2006g). Institutions reported that they are increasing the number of PhD-prepared NP faculty members and supplementing these with qualified master’s-prepared NPs and non-NPs, such as physicians. Results from this investigation indicate that guidelines are in place for faculty-student ratios. The minimum number of clinical practice hours is now 700 in all programs that provided responses to the questionnaires.
Only 25% of the educational institutions that responded recognize faculty clinical hours as teaching hours, and clinical practice may be required to maintain registration as an NP. Many distance courses do currently exist for initial NP education. Unlike the United States, Canada does not have any national standards for NP distance education. Work is in progress related to collaborative programming and interprofessional courses, but such action requires agreement from other faculties.
There is a need for more attention to be paid to sustaining and increasing the supply of appropriate preceptors. A total of 52% of individual NPs responded that they had been a preceptor for NP students. Respondents reported that there were no formal incentives for NP preceptors, with the exception of one respondent who described incentives for NPs during clinical placements.

24 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
5. Transition to the workplace
Almost 80% of NPs reported that their educational program adequately prepared them for the workplace. Respondents from NP educational programs reported on initiatives to assist with this transition. Supports such as mentorships are also required in the workplace to assist with the NP’s transition to the workforce, as they are with other novice practitioners; further action is required in this area. There are currently no refresher programs for NPs.
Many examples of continuing educational activities (Actions 68 and 69) were cited by NPs. Areas of concern are the lack of continuing educational opportunities for casual and self-employed NPs, and an overall lack of NP-focused educational opportunities.
STRATEGIC AREA: Strategic Communications, Change Management and Social Marketing
RECOMMENDATION 9
Change management – Disseminate and promote understanding, acceptance and utilization of the Implementation and Evaluation Toolkit for Nurse Practitioners in Canada and Health Human Resources Planning Simulation Model for NPs in Primary Health Care.TM
Key Actions Status Report
71. Develop and implement a communications/marketing plan to generate Partially understanding and utilization of the Implementation and Evaluation Toolkit completedfor Nurse Practitioners in Canada.
72. Adapt the Implementation and Evaluation Toolkit for Nurse Practitioners Partiallyin Canada to reflect appropriate culture and language of the First Nations, completedInuit and Métis communities.
73. Develop and implement a communications/marketing plan to generate Not completed understanding, acceptance and utilization of the Health Human Resources Planning Simulation Model for NPs in Primary Health Care.TM
Respondents from CNA jurisdictional members, CAAPN, NP associations and CNA indicated that they are promoting existing tools (Implementation and Evaluation Toolkit for Nurse Practitioners in Canada and Health Human Resources Planning Simulation Model for NPs in Primary Health CareTM) where appropriate, but an overall communications/marketing plan does not yet exist. Existing tools have not yet been adopted. Current communication and marketing efforts probably result in duplication and are less effective than efforts guided by an overall plan would be.

CANADIAN NURSES ASSOCIATION 25
RECOMMENDATION 10
Social marketing – Continue and further develop and implement a five-year pan-Canadian social marketing campaign to promote interprofessional collaborative care and practice and the NP role as part of the solution to access and wait times.
Key Actions Status Report
74. Build a consortium/coalition to seek funding for a sustained social marketing Not completed campaign.
75. Implement a five-year social marketing campaign. Not completed
A social marketing plan has not yet been developed.
RECOMMENDATION 11
Strategic communications – Develop and implement a pan-Canadian coordinating mechanism to facilitate the ongoing dissemination of existing and new NP information.
Key Actions Status Report
76. Maintain the existing database of stakeholders. Not completed
77. Maintain and populate the existing CNPI website Partially • Toolkit completed • Centralized location for posting of available NP positions
78. Provide information link to salaries for unionized NPs on CNPI website or Completed CNA portal.
79. Encourage stakeholders and partners to use existing promotion tools/materials Action ongoing developed during the CNPI.
80. Seek partnership with stakeholders to disseminate information to their Action ongoing members/stakeholder groups.
81. Develop and disseminate new and relevant information and tools Partially (e.g., NP profiles, fact sheets). completed
Organizations are working together to share and disseminate information. There has not been much action on the development of new materials, especially materials relevant on a national level. There is no pan-Canadian coordination mechanism to facilitate the ongoing dissemination of existing and new NP information, with the exception of CNA’s maintenance of the CNPI site.
More clarity is needed on this recommendation and the required actions and appropriate lead(s) for the actions.

26 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
STRATEGIC AREA: Evaluation
RECOMMENDATION 12
Adopt the Implementation and Evaluation Toolkit for Nurse Practitioners in Canada as a national guide to support the ongoing implementation of NP roles in different settings.
Key Actions Status Report
82. Develop linkages to universities, government, practitioners and health-care Partially networks to continually update the tools and resources section of the toolkit. completed
83. Promote the use of the toolkit to researchers to encourage standardized approach Not completed and comparison of results over time.
It is difficult to determine how widely the toolkit is being used. There is no mechanism in place to update the toolkit and promote appropriate use. Some jurisdictions have contacted CNA for information on the toolkit. The CHSRF/CIHR Chair Program in Advanced Practice Nursing reported that the tool was developed to support the integration of NPs and to help with internal evaluation. This tool would therefore be of most use to employers, but this project did not include employers.
More clarity is needed on this recommendation and the required actions and appropriate lead(s) for the actions.
STRATEGIC AREA: Governance
RECOMMENDATION 13
Establish a national coordinating committee to work with provincial and territorial representatives and federal partners to implement system-wide change.
Key Actions Status Report
84. Establish a steering committee to begin work on the terms of reference, Not completed membership and a workplan for the coordinating committee.
Health Canada’s Office of Nursing Policy reported that the possibility of a national coordinating committee was discussed with principal nursing advisers from P/T governments. At that time, the group was not convinced of the need for such a committee, given that many of the jurisdictions were moving forward on many of the recommendations. They decided to wait for the results of this report before determining if a coordinating committee was needed.
CANADIAN NURSES ASSOCIATION 27
Project Data: Broad Questions
Representatives of regulatory bodies, CNA jurisdictional members, principal nursing advisers and other nursing representatives from F/P/T governments in Canada, representatives of CAAPN, provincial NP associations and interest groups, NPs, and representatives of educational programs for NPs in Canada were asked broad questions in addition to the specific questions on the actions relevant to their stakeholder group. Their responses to these broad questions are summarized below.
NPs were asked two general questions:
1. What supports are important to you in establishing your NP practice?
For this question, NPs were given four options and could select more than one. They responded as follows:
• employer support for networking and education: 90%;
• peer support groups: 85%;
• mentor: 70%; and
• policy documents from professional nursing organizations: 65%.
Comments included:
• all of these are important;
• administrative understanding and support is critical, including position descriptions, infrastructure and communication concerning the role; and
• MD partnerships are important.
2. Describe any barriers that you are experiencing in your current role as a nurse practitioner.
In response to this question, respondents identified the following key themes, listed in order of decreasing frequency:
• limitations on scope of practice (e.g., drug lists, lists of tests, cannot refer to specialists);
• lack of funding for positions, particularly in primary care;
• lack of models that support genuine collaborative practice (e.g., funding model requires that a physician see the patient and patients cannot be assigned to the NP);
• lack of understanding of, and readiness for, the NP role by physicians, managers, laboratories, etc.;
• lack of supports (e.g., continuing education, performance evaluation, physician backup when needed, support from other NPs, help with patient scheduling, computer support);
• legislative restrictions (e.g., NPs cannot fill out workers’ compensation board forms, NPs cannot prescribe narcotics); and
• regulatory issues (e.g., inconsistency between provinces, registration requirements, the challenge of maintaining clinical hours when there are no jobs for NPs).
28 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
Five groups of respondents were asked two broad questions from the perspective of their own organization or role:
1. Since the CNPI project made its recommendations in 2006, what have been the major changes?
2. What do you see as the key priorities?
Key themes identified by more than one respondent group are outlined below.
Stakeholders have differing views on changes that have occurred since the CNPI project made its recommenda-tions in 2006, due partly to the differences between jurisdictions that were evident during the consultations. Some differences now appear to be resolving, whereas others remain. More than one stakeholder group reported regulatory changes (e.g., the introduction of new regulated categories of NPs, regulations with broader scope, title protection and examination); however, some participants (regulators, government representatives, association representatives and NPs) reported no regulatory changes since 2006. More than one group of respondents (government and association respondents and NPs) noted the growth in awareness and acceptance of the NP role.
In response to the second question on key priorities, four key issues were identified by several groups of respondents, despite being asked to answer the broad questions from the perspective of their own organization/role. The number of times each issue was mentioned varied, as did the way in which respondents approached each issue. They were as follows:
1. scope-of-practice changes and other legislative changes, such as acts related to controlled drugs and hospitals (identified by regulators, and respondents from governments, associations and NPs);
2. practice models and sufficient funding for change management, particularly in primary care (identified by regulators and educators, and respondents from governments, associations and NPs);
3. communication and marketing of the NP role (identified by educators, and respondents from governments, associations and NPs); and
4. harmonization of educational standards (e.g., master’s level education) and regulatory processes (identified by regulators and educators, and respondents from associations and NPs).
Other common themes included:
• the need for supports for NPs (mentorship and peer support; support of administrators and colleagues; compensation, including space and continuing education);
• the need to integrate other forms of NPs;
• the need to graduate more NPs;
• the need to integrate more NPs in emergency and long-term care areas; and
• the need for research on the impact of the role.
CANADIAN NURSES ASSOCIATION 29
DISCUSSION
Summary of Findings
The following findings resulted from a review of the project data and the information previously obtained from the regulators’ work on and MRA:
• There is title protection in all jurisdictions, and changes are planned to enact a broad scope of practice for NPs. Most jurisdictions require NP applicants to pass the CNPE: F/AA, and some require additional exams for other categories of NPs. Some jurisdictions require all NP applicants to successfully complete the Objective Structured Clinical Examination (OSCE) for their registration category. Most NPs have a minimum of $5 million liability insurance as part of their registration.
• The number of NPs has doubled since the CNPI completed its work in 2006. NP associations and interest groups exist in all jurisdictions except for Prince Edward Island and the Yukon, providing support, networking opportunities, conferences and continuing education initiatives. There is good employer support for continuing education in terms of funding and release time.
• The master’s degree has not yet become established as the required credential for entry into NP practice, although most of the recommended changes to entry requirements and curricula have been made by educators. These include a minimum requirement of 700 clinical practice hours plus two years experience as an RN, as well as requirements for faculty preparation and student-faculty ratios. Distance education, both initial and continuing, is widely available. Most NPs report being prepared for practice. The NP role is more visible and accepted than it was in 2006, despite the relative newness of the role.
• Concerns associated with the NP role related to achieving a broad scope of practice for NPs, and the fact that a standardized mechanism to support the work of RNs in expanded roles has not been completed. Although a broad scope of practice has been achieved in half of the jurisdictions, changes to legislation that currently impedes effective practice are required. Consistency has not been achieved in the assessment process for registration, requirements for continuing competence and quality assurance, and registration categories for NPs.
• Key priorities identified during the project include (1) ensuring that the legislated scope of practice of NPs meets the needs of the population and includes the prescription of controlled substances, and (2) giving more attention to HHR planning for NPs and other members of the interprofessional primary care team.
• NP associations are small and volunteer-run, so they have limited resources. More attention to supports (such as mentorship programs), particularly for novice NPs, and to sustaining and increasing the supply of preceptors, is needed. There is a still a lack of readiness for, and understanding of, the NP role in some areas, and there is no organized social marketing strategy.
• There is a need to develop effective models of interprofessional primary health-care service delivery and effective change strategies. There is also a need for changes in scope of practice and other legislation to support effective use of the NP role.

30 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
• There is a need to develop truly collaborative practice models with appropriate and sufficient funding and change management strategies to ensure effective implementation of the NP role (particularly in primary care), as well as research to determine the best approaches, and communications and marketing strategies to improve visibility and understanding of the role.
• Finally, harmonization of key areas such as scope of practice and educational preparation is essential. A consensus on the level of rigour required to assess the initial and ongoing competence of NPs is important. Given the current level of demand for NP refresher programs, it is likely that such programs will not be needed in each jurisdiction; therefore, interjurisdictional discussion and planning is needed for this action.
CANADIAN NURSES ASSOCIATION 31
OUTSTANDING KEY ISSUES
Legislation and Regulation
• Regulators are meeting to discuss the development of consistent registration processes and standards for NPs and to ensure that the requirements of Canada’s Agreement on Internal Trade (AIT) are met. However, current legislation does not describe a consistent level of educational preparation or scope of practice across Canada; rather, registration standards set by regulatory bodies reflect current requirements for educational preparation and competencies and scope of practice.
• As mentioned earlier, Principle 6 of the CNPI Legislative and Regulatory Framework states, “The framework promotes sufficient rigor to ensure safe practice by autonomous nurse practitioners with a broad scope of practice” (CNA, 2006c, p. 19). It appears that significant work is still needed to amend F/P/T statutes to support the most effective use of NPs. While a number of jurisdictions indicate a broad scope of NP practice through high-level jurisdictional documents and legislation, there is a large degree of variation and restrictions in actual practice.
• There continue to be some differences in the processes used by regulators to assess initial and continuing competence. Further discussion is needed between governments and regulators, as well as other stakeholders, to resolve the outstanding issues. This is particularly important so as to ensure that the public is protected as governments move to facilitate mobility of NPs through the implementation of the AIT.
• There has been progress in harmonizing the types of registration categories across the jurisdictions, but differences remain. Currently, five jurisdictions have additional categories for NPs who have completed adult and pediatric examinations, and nine jurisdictions have categories for NPs who have completed the CNPE: F/AA. One jurisdiction uses the ANCC Family exam and requires NP applicants to successfully complete a clinical exam for their registration category. Two jurisdictions use other registration categories and exams (written and clinical).
Practice
• The development and implementation of practice models in primary care require discussion and collaboration by a wide range of stakeholders. Some respondents described effective practice models. However, there appears to be a number of issues needing resolution, including clarity on the meaning of interprofessional practice and the development of funding mechanisms that promote true collaborative practice and ensure the best use of the competencies of all health-care providers. There are barriers to the implementation of the scope of practice of NPs in the current practice models.
32 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
Health Human Resource Planning
• HHR is a challenge for all governments. Health human resource models that follow a needs-based approach (such as the Health Human Resources Planning Simulation Model for NPs in Primary Health CareTM) are recent innovations. Governments more commonly look at historical numbers of health-care providers to determine future needs, but because nurse practitioners are a new category of practitioner, governments cannot rely on historical numbers in their planning processes. The data from this project suggest that, at least in some jurisdictions, there are not sufficient positions available in primary care for the numbers of NPs being prepared for practice in that area. HHR planning is needed to determine the number and type (e.g., family/all ages, pediatric, adult) of NPs that will be required.
Education
• Progress has been made in achieving greater consistency in educational preparation. There is significant concern from the stakeholders consulted that master’s level preparation is not yet the standard across Canada. NPs are increasingly being expected to practise within a broad scope of practice and to bring competencies to their roles in areas such as research, leadership and change management. This requires education at a master’s level, which is the standard in the United States and in many other western countries educating NPs. Finalizing the pan-Canadian transition to master’s level education for NPs will ensure consistency in the exit credential across the country.
• There are educational programs available in Canada for NPs who wish to specialize in caring for pediatric or adult populations. Canada is moving away from a model in which NPs were often considered either “specialist/acute care” or “primary care” practitioners to preparing NPs to practise across the age continuum. The specialist provider was often prepared for practice in a specialty area such neurology or cardiology. In some jurisdictions, the education of pediatric or adult NPs has moved toward broader preparation for NPs to practise across the age continuum in a range of practice areas. This is a recent change, and no data were collected that allowed the comparison of the preparation of adult or pediatric NPs with that of more specialized NPs.
Change Management
• The implementation of the NP role is a recent initiative and much progress has already been made in integrating NPs in primary care and other practice settings. The two tools developed through the CNPI process (Implementation and Evaluation Toolkit for Nurse Practitioners in Canada and Health Human Resources Planning Simulation Model for NPs in Primary Health CareTM) have not been updated and it is not clear from the results of this project how effective these instruments have been. Clearly, the introduction of NPs is a complex innovation, and sophisticated change management strategies for targeted audiences are needed to ensure effective implementation of the NP role. A mechanism that would allow sharing of effective strategies across employer groups and provinces or territories would probably be helpful in supporting more effective change management strategies.

CANADIAN NURSES ASSOCIATION 33
Social Marketing and Strategic Communication
• Respondents described efforts made by their individual organizations, as well as informal cooperation among stakeholders, related to increasing the visibility of NPs and the understanding of the NP role, both within the health-care system and in the general population. The need for improved visibility and understanding in relation to the NP role was cited by many respondents. Such an initiative would need commitment and cooperation from a broad group of stakeholders.
The Need for an Updated Plan of Action
In The Way Forward Plan, the CNPI proposes the development of a multi-stakeholder, multi-jurisdictional coordinating committee. The committee was proposed because supporters and participants were concerned that the CNPI recommendations would not be implemented from a pan-Canadian perspective. The fear was that key stakeholders would act independently when approaching the implementation process. “If a traditional jurisdictional approach is followed in implementing the CNPI recommendations, systemic change will never be achieved and the progress on NP integration into the health-care system will be limited. Long-term change will require a pan-Canadian approach that is based on inter-jurisdictional and interprofessional collaboration and commitment between educators, legislators, employers, practitioners and health human resources planners across jurisdictions” (CNA, 2006h, p.2).
This review on the progress of the CNPI recommendations indicates that more than half of the actions have been fully or partially completed since 2006, and that several key actions remain in progress or are incomplete. Some of the stakeholders acknowledged the importance of a central committee to oversee the completion of the outstanding recommendations from the CNPI.
It may be an appropriate time to consider convening a multi-stakeholder, multi-jurisdictional forum to review the current CNPI list of recommendations and actions. An updated action plan with clear, achievable goals is needed, and participants in the group should agree on which body or bodies will be accountable for achieving each goal. The forum should consider whether further progress can be most effectively achieved by establishing a coordinating committee, such as the one proposed in The Way Forward Plan.
34 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
STAKEHOLDERS
The CNPI stakeholders comprised representatives of regulatory bodies and CNA jurisdictional members representing each province and territory.
Provincial/Territorial Jurisdictions
Jurisdiction Name
RNANT/NU Steven Leck, Executive Director
YRNA Patricia McGarr, Executive Director
CRNBC Laurel Brunke, Executive Director
CARNA Mary-Anne Robinson, Executive Director
SRNA Donna Brunskill, Executive Director
CRNM Sue Neilson, Executive Director
RNAO Doris Grinspun, Executive Director
CNO Heather Campbell, Director, Practice & Policy
OIIQ Carole Mercier, Acting Executive Director
NANB Roxanne Tarjan, Executive Director
CRNNS Linda Hamilton, Executive Director
ARNPEI Becky Gosbee, Executive Director
ARNNL Pegi Earle, Executive Director
Principal Nursing Advisers and Other Nursing Representatives from the Federal/Provincial/Territorial Governments
Province Name
Newfoundland Anita Ludlow Chief Nurse, Policy & Planning Division Department of Health and Community Services
Prince Edward Island Patrice Drake Nursing Policy Analyst PEI Department of Health
Nova Scotia Donna Denney Nursing Policy Adviser, Nursing Advisory Services Nova Scotia Department of Health

CANADIAN NURSES ASSOCIATION 35
New Brunswick Alice Thériault Chief Nursing Officer & Nursing Resources Adviser HHR Planning & Medicare Services Division New Brunswick Health
Quebec Sylvie Hains Directrice conseil en soins infirmiers Ministère de la santé et des services sociaux du Québec
Ontario Vanessa Burkoski Chief Nursing Officer, The Nursing Secretariat Ministry of Health & Long-Term Care
Manitoba Liz Ambrose Senior Policy Analyst, Workforce Policy and Planning Manitoba Health
Saskatchewan Lynn Digney Davis Chief Nursing Officer Saskatchewan Ministry of Health
Alberta Anita Paras Senior Workforce Planner, Health Workforce Planning Alberta Health and Wellness
British Columbia Wendy Hill Assistant Deputy Minister and Chief Nurse Executive Health Authorities Division Ministry of Health
Yukon Jan Horton Health Human Resources Coordinator Yukon Department of Health & Social Services
Northwest Territories Donna Allen Manager, Primary Community Services Department of Health & Social Services
Nunavut Frederick Montpetit Chief Nursing Officer, Department of Health and Social Services Nunavut Territory
Office of Nursing Policy, Health Canada Sandra MacDonald-Rencz Executive Director
Office of Nursing Service, Health Canada Joyce Desjarlais Executive Director, First Nations Health Inuit Branch
Veterans Affairs Canada Donna Davis National Nursing Officer, Client Service and Quality Management Directorate
Correctional Services Canada Joanne Barton Senior Nursing Adviser, Health Services

36 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
Nurse Practitioner (NP) Associations (Provincial and Territorial) or Nurse Practitioner Contacts
Province Name Affiliated Agency
British Columbia Natasha Prodan-Bhalla BC Nurse Practitioner Association President
Alberta Rajamalar Seyon Nurse Practitioners Association of Alberta (NPAA) President
Barb Waters Nurse Practitioner Council of Canada (NPCC) Chair
Saskatchewan Maureen Klenk Nurse Practitioners Association of Saskatchewan President
Manitoba Katie de Leon-Demare Nurse Practitioner Association of Manitoba
Ontario Jane Sanders Nurse Practitioners’ Association of Ontario (NPAO) Executive Director
Quebec Suzanne Watt McGill University Health Centre – Royal Victoria CNS Pain Management Hospital, Montreal, Quebec
New Brunswick Barbara Hennessy Advanced Practice Nurses New Brunswick President (APNNB)
Nova Scotia Rosalind Benoit Nurse Practitioners’ Association of Nova Scotia Chair (NPANS) (Official Provincial Partner)
Prince Edward Island Janet Loo Prince Edward Island nurse practitioner
Newfoundland and Sueann Kean Newfoundland and Labrador NP special Labrador President interest group (NLNPSIG)
Joanne Simms (Official Provincial Partner)
Past president, CAAPN
Yukon Lee Holliday Yukon Territories Currently no established Yukon APN group
Northwest Territories Pat Nymark Northwest Territories and Nunavut NP special Instructor, Health Programs interest group Aurora College, Yellowknife, NT
Nunavut and NWT Kristy Feltham Canadian Nurses Association board member and nurse practitioner
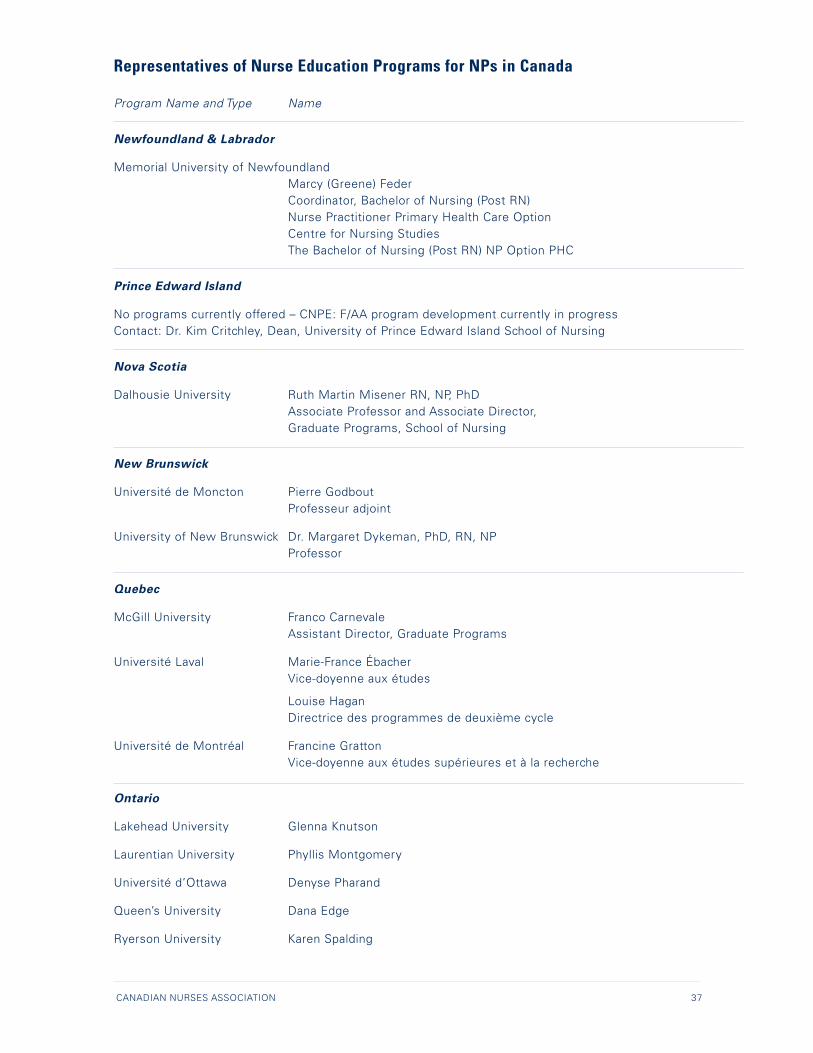
CANADIAN NURSES ASSOCIATION 37
Representatives of Nurse Education Programs for NPs in Canada
Program Name and Type Name
Newfoundland & Labrador
Memorial University of Newfoundland Marcy (Greene) Feder Coordinator, Bachelor of Nursing (Post RN) Nurse Practitioner Primary Health Care Option Centre for Nursing Studies The Bachelor of Nursing (Post RN) NP Option PHC
Prince Edward Island
No programs currently offered – CNPE: F/AA program development currently in progress Contact: Dr. Kim Critchley, Dean, University of Prince Edward Island School of Nursing
Nova Scotia
Dalhousie University Ruth Martin Misener RN, NP, PhD Associate Professor and Associate Director, Graduate Programs, School of Nursing
New Brunswick
Université de Moncton Pierre Godbout Professeur adjoint
University of New Brunswick Dr. Margaret Dykeman, PhD, RN, NP Professor
Quebec
McGill University Franco Carnevale Assistant Director, Graduate Programs
Université Laval Marie-France Ébacher Vice-doyenne aux études
Louise Hagan Directrice des programmes de deuxième cycle
Université de Montréal Francine Gratton Vice-doyenne aux études supérieures et à la recherche
Ontario
Lakehead University Glenna Knutson
Laurentian University Phyllis Montgomery
Université d’Ottawa Denyse Pharand
Queen’s University Dana Edge
Ryerson University Karen Spalding

38 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
University of Western Ontario Marilyn Ford-Gilboe
University of Western Ontario Susan Ray
University of Windsor Debbie Kane
York University Mina Singh
University of Toronto Krista Keilty, MN, NP-Paeds Assistant Professor Coordinator, Master of Nursing, Nurse Practitioner Field, Director, Post Masters Nurse Practitioner Diploma
Manitoba
University of Manitoba Judith Scanlan, BN, RN, MEd, PhD Associate Professor & Associate Dean, Graduate Programs Faculty of Nursing
Saskatchewan
University of Saskatchewan Tammy Morrison Graduate Program Secretary
Lynnette Leeseberg Stamler, RN, PhD College of Nursing
Saskatchewan Institute of Applied Sciences and Technology Joyce Bruce, RN(NP), MSA, MN-ANP Program Head, Primary Care Nurse Practitioner Program
Alberta
Athabasca University Dr. Kimberley Lamarche Program Manager, Faculty of Nursing
University of Calgary Dianne M. Tapp, RN PhD Interim Dean, Faculty of Nursing
British Columbia
British Columbia Institute of Technology Stephanie Wood Program Assistant
University of British Columbia Gloria Joachim, MSN, RN, NP (Family), MSN, FNP(USA), APRN, BC(USA) Associate Professor, School of Nursing
University of Northern British Columbia Dr. Vince Salyers Chair, School of Nursing
University of Victoria Marjorie McIntyre Associate Director
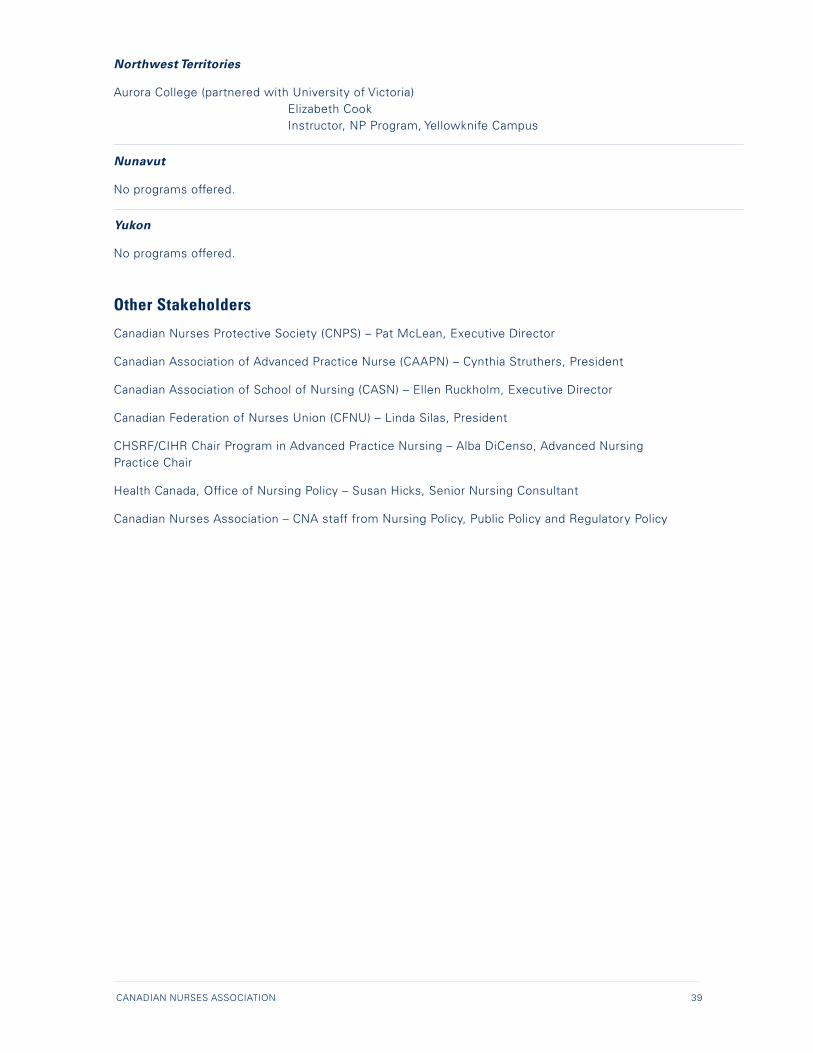
CANADIAN NURSES ASSOCIATION 39
Northwest Territories
Aurora College (partnered with University of Victoria) Elizabeth Cook Instructor, NP Program, Yellowknife Campus
Nunavut
No programs offered.
Yukon
No programs offered.
Other Stakeholders
Canadian Nurses Protective Society (CNPS) – Pat McLean, Executive Director
Canadian Association of Advanced Practice Nurse (CAAPN) – Cynthia Struthers, President
Canadian Association of School of Nursing (CASN) – Ellen Ruckholm, Executive Director
Canadian Federation of Nurses Union (CFNU) – Linda Silas, President
CHSRF/CIHR Chair Program in Advanced Practice Nursing – Alba DiCenso, Advanced Nursing Practice Chair
Health Canada, Office of Nursing Policy – Susan Hicks, Senior Nursing Consultant
Canadian Nurses Association – CNA staff from Nursing Policy, Public Policy and Regulatory Policy
40 RECOMMENDATIONS OF THE CANADIAN NURSE PRACTITIONER INITIATIVE: PROGRESS REPORT
REFERENCES
Canadian Nurses Association. (2005a). Legislation and regulation component: Initial consultation report. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2005b). Canadian nurse practitioner: Core competency framework. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2006a). Nurse practitioner national implementation plan: Suggested roll-out. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2006b). Competence assessment framework for nurse practitioners in Canada. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx.
Canadian Nurses Association. (2006c). Legislative and regulatory framework. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2006d). Practice framework for nurse practitioners in Canada. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2006e). Prior learning assessment and recognition framework for nurse practitioner education and regulation in Canada. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2006f ). Education framework for nurse practitioners in Canada. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2006g). Nurse practitioners: The time is now, A solution to improving access and reducing wait times in Canada. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2006h). The way forward plan: Committing to action. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Canadian Nurses Association. (2008). Advanced nursing practice: A national framework (Revised). Ottawa: Author.
Decima Research (2006). Public opinion research for the Canadian nurse practitioner initiative: Wave 2. Ottawa: Author. Retrieved June 24, 2009, from http://www.cna-aiic.ca/CNA/practice/advanced/initiative/evaluation/default_e.aspx
Ekos (2008). Opinion poll commissioned by CNA [unpublished report].



cna-aiic ca