recent investigation and enforcement trends
TRANSCRIPT

RECENT INVESTIGATION AND ENFORCEMENT TRENDS
Texas & New Mexico Hospice Organization
Annual ConferenceLas Colinas, Texas
February 23 – 25, 2019Mark S. ArmstrongHouston, Texas

2
I. Overview of the Fraud, Waste and Abuse Laws
II. Government Agencies / Contractors Involved
III. Targeted Enforcement Actions
IV. Recent Settlements and Decisions
V. Mitigating Risks
RECENT INVESTIGATION AND ENFORCEMENT TRENDS

3
I. Overview of the Fraud Waste and Abuse Laws

4
Medicare Part A beneficiaries diagnosed with a terminal illness and a life expectancyof six months or less if the illness runs its normal course, may elect to receive hospicebenefits in lieu of standard Medicare coverage for treatment of the underlyingterminal condition.
The beneficiary must agree to forego curative care in favor of palliative care tomanage pain and symptoms.
A hospice care beneficiary waives all rights to Medicare Part B payments for servicesrelated to the treatment and management of the underlying terminal illness or arelated illness for any period of time in which the hospice benefit election is in force.
A beneficiary may revoke his or her election and return to standard Medicarecoverage at any time.
Throughout the hospice election period, Medicare continues to cover servicesprovided by the patient’s attending physician, which may include a nurse practitioner.
Hospice Benefit

5
At initiation of treatment, the beneficiary’s terminal prognosis must be certified by the patient’sattending physician (if there is one), and the hospice’s medical director (or the physician member of thehospice’s IDG.
At the start of each subsequent 90 or 60 day period of hospice care, the hospice medical director orphysician member of the IDG must recertify that the beneficiary is terminally ill and has a life expectancyof 6 months or less.
A brief narrative of the clinical findings that support a life expectancy prognosis of 6 months or less mustbe provided as part of each certification and recertification.
A hospice physician or nurse practitioner must conduct a face-to-face encounter with each beneficiaryprior to the 180th day recertification of terminal illness, and each subsequent recertification, todetermine continued eligibility, and must attest that such visit occurred.
The hospice must designate one or more IDGs to meet the physical, medical, psychosocial, emotional,and spiritual needs of the patient and family. At minimum, an IDG must include: a medical doctor orosteopath employed by or under contract with the hospice, a registered nurse, a social worker, and apastoral or other counselor.
All hospice care and services furnished must follow an individualized written plan of care established bythe IDG in collaboration with the beneficiary’s attending physician (if any), the patient, and the primarycaregiver. The IDG, in collaboration with the patient’s attending physician (if any) must review, revise anddocument the plan of care as frequently as the patient’s condition requires, but no less than every 15days.
Hospice services must be reasonable and necessary for the palliation or management of the terminalillness and related conditions
Hospice Benefit

6
Medicare paid $16.7 billion for hospice care in 2016
About 1.4 million beneficiaries received hospice care in 2016
– 55% received care in the home
– 25% received care in a nursing facility or SNF
– 13% received care while residing in an assisted living facility
4,374 hospices provided care to Medicare beneficiaries in 2016
64% were for-profit hospices
– These hospices received 55% of the dollars
– Served 49% percent of the beneficiaries
Hospice Composition
– 34% were small (fewer than 90 beneficiaries per year)
– 37%were medium sized (90 to 320 beneficiaries per year)
– 29% were large (over 320 beneficiaries per year)
Hospice Facts
Vulnerabilities in the Medicare Hospice Program Affect Quality Care and Program Integrity: An OIG Portfolio, July 2018.

7
Routine Home Care– Least expensive level of care,
– Includes routine services provided to the hospice patient in the patient’s home or a facility in which thepatient resides.
Continuous Home Care– Most expensive level of care,
– Paid only during a period of crisis as necessary to maintain the beneficiary in his or her residence.
– A minimum of 8 hours of care must be provided within a 24 hour period
– Must include nursing care by a registered nurse or licensed practical nurse for more than half of the periodduring which care is provided.
Inpatient Respite Care– May be provided in a hospital, skilled nursing facility, hospice facility, or nursing facility when a caregiver
requires a temporary reprieve.
– A registered nurse must be available to provide direct patient care 24 hours a day.
– Payment may be made for a maximum of 5 days after which the patient must be converted to anotherlevel of care.
– More than 1 respite period is available per 60 or 90 day benefit period.
General Inpatient Care– Second-most expensive level of care,
– Provided for periods during which a beneficiary requires admission to an inpatient facility for pain controlor symptom management.
Levels of Care
8
The False Claims Act, 31 U.S.C. § 3729, et. seq., authorizes the United States, or private parties, known as “relators”, acting on behalf of the United States, to recover monetary damages from parties who submit, or cause others to submit, fraudulent claims for payment by the federal government.
Key Points:– Liability for submitting, or causing to be submitted, a false or fraudulent claim for
payment; making or causing to be made a false record or statement in order to secure payment of a claim; or conspiring to get a false or fraudulent claim paid.
– Materiality: The falsehood was material to the decision to pay the claim.
– Scienter: “knew or should have known”; “deliberate ignorance” of truth or falsity; “reckless disregard” of the truth or falsity of the claim.
No Specific Intent Needed
THE GOVERNMENT’S FAVORITE WEAPON
The False Claims Act

9
“REVERSE” FALSE CLAIMS
Overpayments
Penalties can be imposed on anyone who “knows of an overpayment” and fails to report and return it.
Under this law, the retention of an overpayment beyond 60 days constitutes an “obligation” within the meaning of the FCA.

10
The federal False Claims Act is a qui tam statute, meaning that privatecitizens (“relators”) may file complaints alleging violations of the FCAunder seal on behalf of the U.S. Government and may receive at least15%, but not more than 30%, of any amount recovered, depending onwhether the government intervenes.
Once a whistleblower files a suit, the Department of Justicemust decide whether to “intervene” (i.e., take over and prosecute thesuit).
If the government does not intervene, the case is unsealedand the whistleblower may proceed on his/her own.
Qui Tam Relators

11
Inadequate documentation of
services performed
Billing for services that are of such poor quality
they are deemed “worthless.”
False CertificationsBilling for Goods or
Services not Provided
Improper or Complete Absence of Qualified Personnel Rendering
Service
Upcoding to inflate Medicare reimbursement
Admitting patients to hospice care that are not
terminally ill
Falsifying documents and patient records indicating patients were eligible for or had elected hospice
benefits
Knowingly bill Medicare for services not in
compliance with patients’ Plan of Care
Instructing staff to enroll patients for hospice care without proper physician authorization or clinical
information.
Medical Necessity –Eligibility for the Billed
ServiceLength of Stay/Service
EXAMPLES AND TYPES OF FALSE CLAIMS ACT ALLEGATIONS
The False Claims Act

Specifically, the AKS prohibits individuals and entities fromknowingly and willfully:
– Offering, paying, soliciting, or receiving anything of value toinduce or reward the referral of Federal health care programbusiness; or
– Offering, paying, soliciting, or receiving anything of value toinduce or reward purchasing, leasing, ordering, or arranging foror recommending purchasing, leasing or ordering any good,facility, service, or item for which payment may be made under aFederal health care program.
(THE “AKS”)
The Federal Anti-Kickback Statute

“One purpose test”
– Anti-Kickback Statute applies if one purpose of theremuneration is to induce referrals even if there areother legitimate purposes. (U.S. v. Greber, 760 F.2d 68(3d Cir. 1985)).
– Difficult to disprove.
Ignorance of the law is no excuse.
Anti-Kickback Statute

Violating the AKS is a felony.
– Conviction can result in fines up to $25,000 per violation, upto a 5-year prison term, or both.
False Claims Act Liability
– Kickback violations can also lead to False Claims Act liability,previously under the “implied certification” theory, and nowexpressly by statute.
– While the AKS itself does not provide a private right ofaction, the False Claims Act allows private individuals tobring qui tam actions alleging AKS violations.
Anti-Kickback Statute

Exclusion from federal health care programs
– OIG can exclude individuals and entities that violate the AKSfrom participating in Federal health care programs andsubject them to a $50,000 civil monetary penalty perviolation and an assessment of up to 3 times the totalamount of the kickback payment.
The AKS applies to everyone (not just providers or physicians).
– Vendors, manufactures, marketers, directors, etc. may beliable.
– Statute often used in criminal cases against patientrecruiters, and marketers.
Anti-Kickback Statute

Applies to any form of remuneration to induce or reward referrals for federal program business.
– Money.
– Free or discounted items or services (e.g., perks, gifts, space, equipment, meals, insurance, trips, CME, etc.).
– Overpayments or underpayments (e.g., not fair market value).
– Payments for items or services that are not provided.
– Payments for items or services that are not necessary.
– Professional courtesies.
– Waivers of copays or deductibles.
– Low interest loans or subsidies.
– Business opportunities that are not commercially reasonable.
Anti-Kickback Statute

No liability if all the requirements of a safe harbor are satisfied.
Not required to fit within safe harbor because ultimate question is whether “one purpose” of remuneration is to induce or reward referrals.
The closer you come to satisfying regulatory requirements, the safer you will be.
Anti-Kickback Statute

Exceptions and safe harbors– Bona fide employment
– Personal services contracts
– Leases for space or equipment
– Investments in group practice
– Investments in ASCs
– Sale of practice
– Recruitment
– Certain investment interests
– Waiver of beneficiary coinsurance and deductible amounts.
(42 C.F.R. §1001.952)
EXCEPTIONS AND SAFE HARBORS
Anti-Kickback Statute

Exceptions and safe harbors (cont.)– OB malpractice insurance subsidies
– Referral services
– Referral arrangements for specialty services
– Warranties
– Discounts
– Group purchasing organizations
– Price reductions offered to health plans and MCOs
– Ambulance replenishing
– Health centers
– Electronic health record items or services
(42 C.F.R. §1001.952)
EXCEPTIONS AND SAFE HARBORS
Anti-Kickback Statute
20
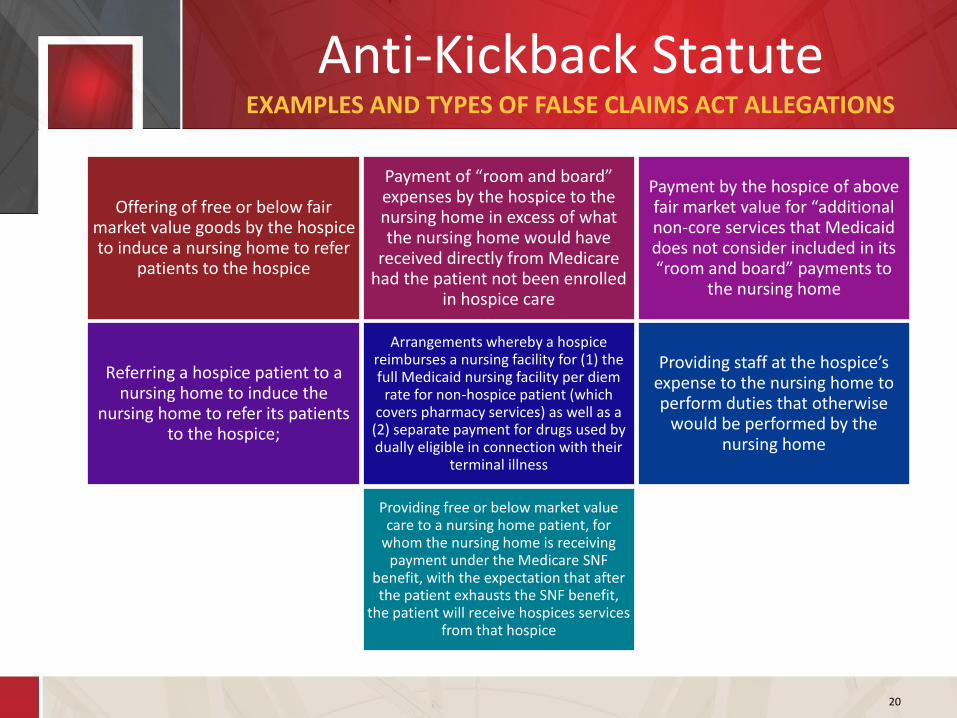
Offering of free or below fair market value goods by the hospice to induce a nursing home to refer
patients to the hospice
Payment of “room and board” expenses by the hospice to the nursing home in excess of what the nursing home would have
received directly from Medicare had the patient not been enrolled
in hospice care
Payment by the hospice of above fair market value for “additional non-core services that Medicaid does not consider included in its “room and board” payments to
the nursing home
Referring a hospice patient to a nursing home to induce the
nursing home to refer its patients to the hospice;
Arrangements whereby a hospice reimburses a nursing facility for (1) the full Medicaid nursing facility per diem
rate for non-hospice patient (which covers pharmacy services) as well as a
(2) separate payment for drugs used by dually eligible in connection with their
terminal illness
Providing staff at the hospice’s expense to the nursing home to perform duties that otherwise
would be performed by the nursing home
Providing free or below market value care to a nursing home patient, for
whom the nursing home is receiving payment under the Medicare SNF
benefit, with the expectation that after the patient exhausts the SNF benefit,
the patient will receive hospices services from that hospice
EXAMPLES AND TYPES OF FALSE CLAIMS ACT ALLEGATIONS
Anti-Kickback Statute
21
II. Government Agencies /Contractors Involved

22
$2.8 Billion in recoveries– $2.5 Billion involving health care industry
– $2.1 Billion from Whistleblower cases
764 Criminal actions
813 Civil actions
2,712 Exclusions
FY2018
OIG Report by the Numbers

23
Federal Departments:
Department of Justice (DOJ)
– Offices of the United States Attorneys (USAO)
Federal Bureau of Investigation (FBI)
Department of Health and Human Services (HHS)
– Office of Inspector General (OIG)
– Office of Audit Services (OAS)
– Office for Civil Rights (OCR)
– Office of Evaluations and Inspections (OEI)
– Center for Medicare and Medicaid Services (CMS)
• Center for Program Integrity (CPI): “Serves as CMS' focal point for all national and state-wide Medicare and Medicaid programs and CHIP integrity fraud and abuse issues.” (CMS/CPI Functional Statement)
CONCERTED EFFORTS TO COMBINE AND POOL RESOURCES
Federal Government Agencies

24
State Departments:
Texas Office of Attorney General
– Medicaid Fraud Control Unit
• investigating criminal and civil fraud by Medicaid providers;
• investigating physical abuse and criminal neglect of patients in health care facilities licensed by the Medicaid program, including nursing homes and Texas Department of Aging and Disability Services homes;
• prosecuting criminal fraud by Medicaid providers or assisting local and federal authorities with such prosecution;
• investigating fraud within the administration of the Medicaid program.
https://www.texasattorneygeneral.gov/cj/criminal-medicaid-fraud /
Texas Office of Inspector General
– The mission of the Texas Inspector General is the "prevention, detection, audit, inspection, review, and investigation of fraud, waste, and abuse in the provision and delivery of all health and human services in the state, including services through any state-administered health or human services program that is wholly or partly federally funded, and the enforcement of state law relating to the provision of these services.“
https://oig.hhsc.texas.gov/about
CONCERTED EFFORTS TO COMBINE AND POOL RESOURCES
State Government Agencies

25
State-of-the-Art Technologies
• CMS Fraud Prevention System• Accounted for 20% of CMS’ fraud investigations
• Uses automated controls that identify payments associated with potential fraud and deny claims that violate Medicare rules or policies before the claims are paid
• $11.5 to $1 return on investment
Increased Collaboration
• Health Care Fraud Prevention and Enforcement Action Team (HEAT)
• Medicare Fraud Strike Force
• Healthcare Fraud Prevention Partnership (HFPP)
GOVERNMENT INVESTMENTS IN FRAUD ENFORCEMENT ACTIVITIES
Enforcement Environment

26
Medicare Medicaid
Medicare Administrative Contractors (MACs)
Recovery Auditors (RACs) Medicaid RACs
Zone Program Integrity Contractors (ZPICs)
Review-of-Provider, Audit and Education Medicaid Integrity Contractors (MICs)
Unified Program Integrity Contractors (UPICs)
Comprehensive Error Rate Testing (CERT)State Medicaid Fraud Control Units (MFCU)
The Contractors

27
Permanent program created by Tax Relief and Health Care Act of 2006
Detect and correct past improper payments (over/under payments)
Apply statutes, regulations, CMS coverage and billing policies and LCDs to make determinations
Look-back period not to exceed 3 years
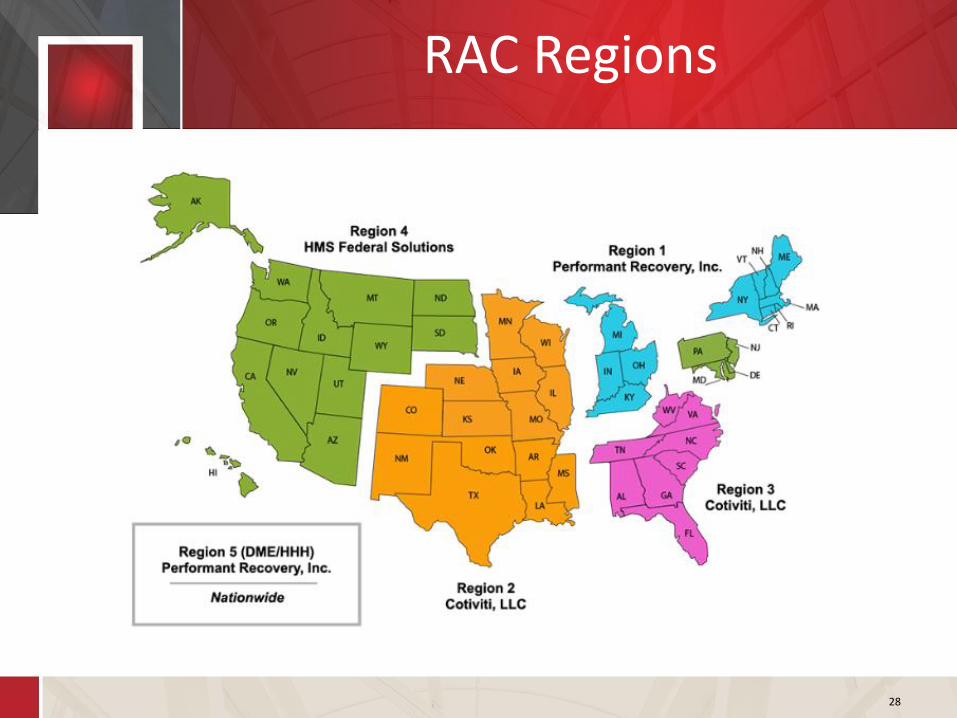
5 Regions each with a different contractor
– Region 2 (Texas and New Mexico) RAC Contractor: Cotiviti, LLC
– Region 5 (Nationwide for DMEPOS/HHA/Hospice): Performant Recovery, Inc.
Section 6411(b) of Affordable Care Act (“ACA”) expands use of RACs to all of Medicare and not just Part A and B
RACs: What do they do?
28
RAC Regions

29
Created by Medicare Prescription Drug, Improvement and Modernization Act of 2003– Move away from Program Safeguard Contractor concept which divided contracts by
service line (e.g., Part A, B, Home Health, etc…)
– Part A, B, DME, Home Health and Hospice
Investigate leads generated by the Fraud Prevention System (FPS) and other sources
Perform data analysis to identify and investigate cases of suspected fraud, waste, and abuse
Make referrals to OIG/DOJ for investigation/prosecution
Provide support for ongoing law enforcement investigations
Initiate payment suspensions
Recommend administrative action against providers (e.g., exclusion, revocation of provider number, collection of overpayment)
Zone 4 (Texas and New Mexico): Health Integrity, LLC
ZPICs: What do they do?

30
ZPIC Zones

31
Investigate instances of suspected fraud, waste, and abuse
Perform medical review, as appropriate
Perform data analysis
Identify the need for administrative actions – Payment suspensions
– Prepayment or auto-denial edits
– Revocations
– Overpayment determination
Share information with other UPICs
Refer cases to OIG/DOJ for civil or criminal prosecution
UPICs may: – Request medical records and documentation
– Conduct interviews with beneficiaries, complainants, or providers
– Conduct site verification
– Conduct an onsite visit
UPICs: What do they do?

32
SafeGuard Services LLC
SafeGuard Services LLC
AdvanceMed
Qlarant
Qlarant
UPIC Regions

33
Billing for services not furnished
Pattern of overutilization
Vacant supplier/provider location
Medically unnecessary services
Stolen provider / beneficiary info
Schemes of collusion (e.g., kickbacks)
OIG November 2011 Report: Zone Program Integrity Contractors’ Data Issues Hinder Effective Oversight
Top ZIPC/UPIC Issues

34
Coordinate audits with other auditing entities
Report fraud to Medicaid Fraud Control Units
Set limits on number and frequency of medical records for review
Adhere to 3 year look-back period
Maintain 1 FTE Medical Director who is a M.D. or D.O.
Hire certified coders unless state determines not needed
Develop education and outreach programs
Incentivize RACs to detect underpayments
STATES / RACs MUST:
Medicaid RACs

35
Oversight / Risk Analysis

36
III. Target Enforcement Actions

37
https://oig.hhs.gov/reports-and-publications/workplan/active-item-table.asp
Health Care Enforcement

38
Protecting Medicare Hospice Beneficiaries From Harm
The Medicare hospice program is an important benefit for beneficiaries and their families and caregivers at the end of a beneficiary's life.– We will use the survey reports to provide more detail about poor-quality
care that resulted in harm to beneficiaries. We will describe specific instances of harm to Medicare hospice beneficiaries and identify the vulnerabilities in Medicare's process for preventing and addressing harm.
OIG Work Items

39
Medicare Payments Made Outside of the Hospice Benefit
In general, a hospice beneficiary waives all rights to Medicare payments for any services that are related to the treatment of the terminal condition for which hospice care was elected. Medicare continues to pay for covered medical services that are not related to the terminal illness.– We will produce summary data on all Medicare payments made outside
the hospice benefit, without determining the appropriateness of such payments, for beneficiaries who are under hospice care. In addition, we will conduct separate reviews of selected individual categories of services (e.g., durable medical equipment, prosthetics, orthotics and supplies, physician services, outpatient) to determine whether payments made outside of the hospice benefit complied with Federal requirements.
OIG Work Items

40
Duplicate Drug Claims for Hospice Beneficiaries
Medicare may have paid twice for prescription drugs for hospice beneficiaries, once under the Part A per diem rate and again under Part D. – We review the appropriateness of Part D drug claims for individuals who are
receiving hospice benefits under Part A.
– We will also review whether Part D continues to pay for prescription drugs that should have been covered under the per diem payments made to hospice organizations.
OIG Work Items

41
Trends in Hospice Deficiencies and Complaints
The Medicare hospice program is an important benefit for beneficiaries and their families at the end of life. Surveys and complaint investigations are critical oversight mechanisms that address the care provided to beneficiaries by hospices. These surveys assess the extent to which hospices meet Federal health and safety standards and require that surveyors cite hospices with deficiencies if they fail to meet the standards. – As part of OIG's ongoing commitment to address quality of care, we will
determine the extent and nature of hospice deficiencies and complaints and identify trends.
OIG Work Items

42
Hospice Home Care — Frequency of Nurse On-Site Visits to Assess Quality of Care and Services
Medicare requires that a registered nurse make an on-site visit to the patient's home at least once every 14 days to assess the quality of care and services provided by the hospice aide and to ensure that services ordered by the hospice interdisciplinary group meet the patient’s needs
– We will review registered nurses made required on-site visits to the homes of Medicare beneficiaries who were in hospice care.
OIG Work Items

43
Review of Hospices’ Compliance with Medicare Requirements
When a beneficiary elects hospice care, the hospice agency assumes the responsibility for medical care related to the beneficiary’s terminal illness and related conditions.
– We will review hospice medical records and billing documentation to determine whether Medicare payments for hospice services were made in accordance with Medicare requirements.
OIG Work Items

44
Medicare Payments for Chronic Care Management
Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare beneficiaries who have multiple (two or more), significant chronic conditions (Alzheimer’s disease, arthritis, cancer, diabetes, etc.) that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline. These significant chronic conditions are expected to last at least 12 months or until the death of the patient. CCM cannot be billed during the same service period as transitional care management, home health care supervision/hospice care, or certain end-stage renal disease services.
– We will determine whether payments for CCM services were in accordance with Medicare requirements.
OIG Work Items

45
OIG Conclusion and Recommendations
• Seek statutory authority to establish
additional remedies for hospices with poor
performance
• Strengthen the survey process
• Develop and disseminate additional
information on hospices to help beneficiaries
and their families and caregivers make
informed choices about their care
• Educate beneficiaries and their families and
caregivers about the hospice benefit
• Promote physician involvement and
accountability to ensure that beneficiaries
get appropriate care
• Strengthen oversight of hospices to reduce
inappropriate billing
• Tie payment to beneficiary care needs and
quality of care to ensure that services
rendered

46
IV. Recent Settlements and Decisions

47
December 13, 2018 – SouthernCare, Inc. pays $5.8 Million to settle FCA allegations
SouthernCare agreed to pay $5,863,426 to the federal government to resolve allegationsthat the company violated the False Claims Act by submitting claims to Medicare forhospice care that was medically unnecessary or lacked documentation.
The whistleblowers alleged that SouthernCare provided hospice care to patients whowere not eligible under the Medicare program. To be eligible, hospice care must bereasonable and necessary, a physician must certify that the patient’s life expectancy is sixmonths or less, and the provider must satisfy other documentation requirements. Thewhistleblowers alleged that SouthernCare admitted patients into hospice who were notterminally ill and lacked appropriate medical documentation showing such anillness. The company allegedly treated some patients for many years.
Recent Settlements and Decisions

48
October 11, 2018 - Hospice Owner Pleads Guilty to $15 Million in Fraudulent Claims
Charline Brandon, a former owner of Haven Hospice, North Haven Hospice, Lion Hospiceand North Lion Hospice in Mississippi pleaded guilty to making fraudulent hospice claimsto federal insurers. Brandon acknowledged submitting nearly $12 million in fraudulentclaims to Medicare and nearly $3 million to Medicaid while she was running the hospices.
Brandon admitted that she fraudulently submitted claims to Medicare and Medicaid forhospice services that were not medically necessary or that were not provided to thehospice patients as claimed. Brandon further admitted that she illegally recruitedpatients who were not hospice eligible.
Recent Settlements and Decisions

49
June 25, 2018 - Caris Agrees To Pay $8.5 Million Court Settle False Claims Act Lawsuit Alleging That it Billed for Ineligible Hospice Patients
Caris Healthcare, L.P. and its wholly-owned subsidiary, Caris Healthcare, LLC (“Caris Healthcare”),agreed to resolve allegations that they violated the False Claims Act by knowingly submitting falseclaims, and knowingly retaining overpayments, for the care of patients who were ineligible for theMedicare hospice benefit because they were not terminally ill. Under the settlement agreement,Caris Healthcare, agreed to pay $8.5 million.
The settlement resolves allegations that Caris Healthcare admitted and recertified patients forhospice care that were ineligible for the hospice benefit. The government’s complaint alleged that,in an effort to meet the aggressive admissions and census targets set by the company, Carisadmitted patients whose medical records did not support a terminal prognosis. The government’scomplaint further alleged that when Caris was alerted to the ineligibility of these patients — viainternal audits, concerns raised by its Chief Medical Officer, and recommendations of its nurseemployees who actually examined the patients — Caris not only continued to submit hospiceclaims to Medicare for the patients, but also took no meaningful action to determine whether ithad previously received improper payments for these and other patients that should have beenreturned to Medicare.
Recent Settlements and Decisions

50
May 18, 2018 - Health and Palliative Services of the Treasure Coast, Inc., The Hospice of Martin and St. Lucie, Inc., and Hospice of the Treasure Coast, Inc. Paid $2.5 Million to Settle FCA Allegations
Health and Palliative Services of the Treasure Coast, Inc., The Hospice of Martin and St. Lucie, Inc., and Hospice of the Treasure Coast, Inc. have paid $2.5 million to settle allegations that they violated the False Claims Act by submitting false claims to Medicare for hospice patients.
The settlement resolved allegations that between 2005 and 2011, the defendants knowinglysubmitted or caused to be submitted false claims to Medicare, for services to hospice patients whowere not eligible for all or part of their hospice care under Medicare requirements. Medicare’shospice benefit is available for patients who elect palliative treatment (medical care focused on thepatient’s relief from pain and stress) for a terminal illness and have a life expectancy of six months orless if their disease runs its normal course. Patients who elect the hospice benefit forgo the right tocurative care (medical care focused on treating the patient’s illness).
The allegations arose from a lawsuit filed by whistleblowers, John Simons, M.D. and Lewis Cook,M.D., under the qui tam provisions of the False Claims Act. The doctors received $476,373.73 fromthe announced recovery.
Recent Settlements and Decisions

51
V. Mitigating Risks

52
Ensuring Effectiveness
– An effective compliance program is dynamic and evolves
– One size does not fit all – an effective program is tailored to a provider’s structure and operation
– Track guidance for government views as to what is necessary
• HHS-OIG Compliance Program Guidance
• Federal Sentencing Guidelines
• Recent CIAs
– Know your fraud and abuse risk areas – they change
Develop and implement an effectivecorporate compliance program
Compliance Program Activites

53
Audit and Monitor High Risk Areas
– Develop and adhere to a work plan that sets forth a schedule and scope of internal reviews
– Consider periodic external reviews by independent third parties
– Identify and refund overpayments within 60 days
Evaluate Your Data to Identify Trends and Investigate Outliers
AUDITING AND MONITORING
Compliance Program Activities

54
https://www.cgsmedicare.com/hhh/medreview/hos_denial_reasons.html
Hospice Medical ReviewTOP DENIAL REASON CODES
Rank Denial Code Denial Description# of Claims
Denied
% of Claims
Denied
1 5PM01
According to Medicare hospice requirements, the information
provided does not support a terminal prognosis of six months or
less.
42 53%
2 5PX06The notice of election is invalid because it doesn’t meet
statutory/regulatory requirements.13 16%
3 5PC01The physician narrative statement was not present or was not
valid.7 9%
4 5PC08 Face-to-Face Encounter requirements not met. 4 5%
5 5MP02
According to Medicare hospice requirements, the documentation
indicates the general inpatient level of care was not reasonable
and necessary. Therefore, payment will be adjusted to the routing
home care rate.
4 4%
Updated: 01.25.19

55
Consider Engaging Legal Counsel to Conduct or Direct Auditing Activities You Want Protected By Privilege
– Compliance effectiveness review
– Targeted internal investigations
Utilize Legal Counsel to Monitor and Manage Financial Relationships
Ensure Background and Exclusion/Debarment Checks Are Regularly Conducted
– Not only employees, but also independent contractors and vendors
– Check both HHS-OIG LEIE database and GSA’s SAM database
– Also state Medicaid excluded provider lists
AUDITING AND MONITORING
Compliance Program Activities

56
Allows hospices to compare their billing statistics with national, jurisdiction andstate percentile values for each target area:
– Live Discharges - No Longer Terminally Ill
– Live Discharges Revocations
– Live Discharges Length of Stay 61-179 days
– Long Length of Stay (greater than 180 days)
– Continuous Home Care Provided in an Assisted Living Facility
– Routine Home Care Provided in an Assisted Living Facility
– Routine Home Care Provided in a Nursing Facility
– Routine Home Care Provided in a Skilled Nursing Facility
– Claims with Single Diagnosis Coded
– No General Inpatient Care or Continuous Home Care
– Long General Inpatient Care Stays
https://www.pepperresources.org/
Auditing ToolsPEPPER REPORT

57
If outliers are revealed by PEPPER data, review claims anddocumentation in medical record, consider patient populationand external factors
Develop best practices regardless of whether there is an outlier
PEPPER data is not publically available; TMF Health QualityInstitute does not provide PEPPER data to MACs or RACs, but theMACs provide access to database with PEPPER statistics for theirregions, so it is available to the MACs
Auditing ToolsPEPPER REPORT

58
Designate a specific individual to be responsible for tracking and understanding regulatory changes and disseminating information to appropriate staff
Importance of documentation training hospice staff
• Certification of plans of care
• Certification of terminal illness
• Face-to-face visits
Focused training for marketing staff on interactions with referral sources and beneficiaries
HHS-OIG HEAT Provider
Compliance Training Initiative
resources
TRAINING AND EDUCATION
Compliance Program Activities
59
Track and log compliance questions, complaints and issues raised through the compliance program, steps taken to follow up, how issues were resolved, including corrective and preventative actions
Implement systems to ensure timely certifications, F2F visits, therapy reassessment visits
• EHRs can have features built-in to flag patients with upcoming requirements
• Schedule IDGs sufficiently in advance to help monitor key timing requirements
Have means to identify disgruntled employee or contractor
• Publicize compliance hotline to contractors, vendors
• Conduct and document exit interviews, reviewed by compliance officer
Monitor payor and contractor audits for patterns for signs of systemic issues
• Multiple audits of same/similar issues, multiple RAC or ZPICaudits
Other Risk Mitigation Actions

60
Vary in type and intensity
– Contractor audits and additional documentation requests
– Administrative subpoenas– OIG subpoenas– Civil Investigative Demands– Grand Jury subpoenas– Search warrant
What to expect:
– Unannounced requests– Medical record demands– Rigorous data analysis– Potential for conflicting interpretation
of Medicare guidelines
Government Overtures

61
CMS Informationhttp://www.cms.gov/Research-Statistics-Data-and-Systems/Research-Statistics-Data-and-Systems.html
CMS Regulation and Guidancehttp://www.cms.gov/Regulations-and-Guidance/Regulations-and-Guidance.html
CMS List Servehttps://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads//MailingLists_FactSheet.pdf
Medicare Claims Processing Manual (Chapter 11 – Hospice Claims)http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS018912.html
OIG Compliance 101 Education Materialshttp://oig.hhs.gov/compliance/101/index.asp
OIG Active Work Planhttps://oig.hhs.gov/reports-and-publications/workplan/active-item-table.asp
Useful Resources

62
OIG Report to Congresshttps://oig.hhs.gov/reports-and-publications/semiannual/index.asp
OIG Exclusion Listhttp://exclusions.oig.hhs.gov/
OIG LEIE Downloadable Databasehttps://oig.hhs.gov/exclusions/exclusions_list.asp
GSA Excluded Party Listhttps://www.epls.gov
Texas Medicaid Exclusion Listhttps://oig.hhsc.state.tx.us/Exclusions/Search.aspx
HIPAA Breach Notification Rulehttp://www.hhs.gov/ocr/privacy/hipaa/administrative/breachnotificationrule/index.html
Useful Resources

63
Medicare Fee-For-Service Appeals http://www.cms.hhs.gov/OrgMedFFSAppeals/
Medicare Learning Networkhttp://www.cms.hhs.gov/MLNGenInfo/
National Government Services (NGS)http://www.ngsmedicare.com
PEPPER Reporthttps://www.pepperresources.org/
Palmetto GBA – Jurisdiction M Home Health and Hospice MAChttps://www.palmettogba.com/palmetto/providers.nsf/DocsCatHome/JM%20Home%20Health%20and%20Hospice
Useful Resources