real world research in childhood disability: the ... · real world research in childhood...
TRANSCRIPT

Real world research in childhood disability: The challenges and
achievements
Knowledge & Innovation Department
Healthy Development Adelaide presentation 29th March 2017
Determining the rater reliability of the Novita Switch Access Solutions Assessment
(NSASA) Dr Toan Nguyen (Research Officer & Rehabilitation Engineer – Assoc Investigator)
Project team: Mrs Annabelle Tilbrook (Senior Occupational Therapist – Chief Investigator)
Mrs Myriam Sandelance (Profession Leader, Occupational Therapy – Assoc Investigator)
Dr Virginia Wright (Senior Clinician Scientist and Pediatric Physiotherapist ,
Holland Bloorview Kids Rehabilitation Hospital, Canada – Assoc Investigator)
/research
Funded by: Novita Children’s Services, 2015-2017

Why use switches?
• Switches used by children with
severe & multiple disabilities from
early age
• Successful switch use gives
opportunities for independent:
− communication
− play
− learning/education
− control of the environment
/research

Finding the appropriate switch…
Assessment is complex and requires consideration of range of factors:
• Child’s needs & abilities:
- Motor (physical)
- Visual
- Cognitive (process)
• Which body part(s) should be used?
• Which switch?– multitude of possibilities
• Where and how should the switch be positioned?
Twitch Switch Activation by small muscle movement
/research

Switching technology examples
EK1 – “Sound” switch
Disclaimer: EK is the actual initial of the client’s
name, which we have permission to use.
/research

Switching technology examples
EK2 – “Facial expression” (gesture tracking) switch
/research
Why Novita Switch Access Solutions Assessment?
• Avoid prolonged ‘trial and error’ approach used to determine
optimal solutions
• Changes in abilities in this client group happen slowly and in small
increments – small changes often missed
• Poor evaluation has potential for sub-optimal solutions and
compromise participation abilities
• No reliable and valid outcome measure for switch access
technology evaluation
• HENCE, we developed the NSASA*!!!
* We acknowledged the earlier work on the development of the NSASA by UniSA’s School of Health Sciences
Occupational Therapy Honours Students.
/research


Our current research with the NSASA?
Objective:
• To determine the reliability of the NSASA with two trained Occupational
Therapist assessors
Method:
• Review 20 videos of children interacting with their ‘prescribed’ switching
technology and completion the assessment form.
• Two assessors’ scores are then analyzed to determine their level of
agreement for overall total scores and Motor, Visual and Process sub-
scale scores
Results so far…
• We have past the half way mark and preliminary data analysis shows that
we are on the right direction
/research

Ultimate goal & future directions
• Help therapists to efficiently find the best individual solution
• Enabling children to participate to the best of their ability
• Once the validation of the NSASA has been accomplished
get this out to the world!
• Commercialise the assessment and provide accompanying
training and access to manual and assessment with Novita
& other Occupational Therapists
/research
Finally, something to think about…
“For people without disabilities, technology makes things easier. For people with disabilities, technology makes things possible!” IBM training manual 1991
/research

Kanchana Pathirana (Researcher/ Data Analyst - Chief Investigator)
Funded by: Ian Potter Foundation and Novita Children’s Services (2016-2017)
/research
‘Toys as Therapy’ project team: Kerry Evans (Profession Leader, Physiotherapy – Associate Investigator)
Ann Underwood (Occupational Therapist – Research Officer)
‘Play as Therapy’ project team: Myriam Sandelance (Profession Leader, Occupational Therapy –
Chief Investigator)
Kathryn Mahadeva (Occupational Therapist – Research Officer)
Let’s play to engage, explore, and learn about the world
Value of toys and play • Important tool for families in everyday life
• Toys and play are an essential tool in therapy
o Value of having an everyday tool in therapy
o Fun & appealing
Choosing and using toys
/research
o Real-world considerations
o Preferences & qualities
o Purpose
It’s not simply based on a child’s disability!
Take home messages!

It can be simple but it’s still a
multifaceted process – it’s not just
the child’s disability, there’s many
things to take into consideration (e.g.
having a few ideas whilst being
flexible and responsive).
How to use play as a means to
achieve kids’ everyday goals?
Need for formally upskilling therapist
to better support our families with
above point.
Need for more visual, practical, and
accessible information!
/research
So what next?

Where are we up to?
Video Series
Recorded 5 live therapy sessions
Begun long journey of editing and
launching the videos
Edited two videos
Piloting
• Finalizing videos
• Launch
• Evaluation
Staff Training Webinar
Set up objectives
• Drafting content and format
• Piloting
• Evaluation
• Launch within Novita
? Make available externally

Activity Boost Challenge trial: Impact of a foot muscle stimulator on physical activity participation of kids
with Cerebral Palsy
Funded by: Thyne Reid Foundation, Channel 7 Children’s Research Foundation, and Novita
/research
Dr Annemarie Wright (Research Officer – Associate Investigator)
Project team: Kerry Evans (Profession Leader, Physiotherapy – Chief Investigator)
Lisa Dodds (Senior Orthotist – Associate Investigator)
Dr Virginia Wright (Senior Scientist and Pediatric Physiotherapist,
Holland Bloorview Kids Rehabilitation Hospital, Canada – Associate Investigator)

We couldn’t do it without our junior scientists
• Children & young people aged 6-17 years and their families
• Hemiplegic cerebral palsy (GMFCS Level I or II – able to
walk/run without aids)
• Meet eligibility criteria (e.g. sufficient ankle movement and
enough time since surgery or Botox injections)
/research

Fast facts about Cerebral Palsy (CP)
• Most common physical disability in childhood
• Life-long disorder of posture and movement
• Many children with CP have weakness or spasticity in
their lower leg muscles
• Can cause trips/falls
• Often prescribed leg or foot braces
• BUT… often restricts ankle movements, impacting on speed or
agility, and necessitates larger footwear to accommodate the
extra width.
/research

Activity Boost Challenge
Aim:
To investigate the impact of an 8 week physio+WalkAide® intervention
Primary outcomes:
Child & family goals and a measure of advanced gross motor skills
(the ‘Challenge’)
Research questions:
1. Can our intervention improve advanced motor skills and physical activity?
2. Is the physio+WalkAide intervention better than physio alone?
3. What do children and their family what they think about using the
WalkAide?
/research

What is a WalkAide?
• Worn around the calf while walking and running
• Uses functional electrical stimulation to restore nerve to muscle signals in the leg and foot
• Can be programmed to lift toes at the right time – smoother walking
• Some evidence that use can increase muscle size and strength
• Most research in adults
/research

Motor learning based physiotherapy
Motor learning strategies are the approaches we take to structure
the motor learning variables within the given intervention to optimize
motor learning possibilities and fit the goals of the child/family
(Levac et al., 2011)
Motor
Learning Strategies
A) What the Therapist
SAYS
B) What the Therapist
DOES
C) How the Session is Organized
/research
J Ryan, unpublished figure, Bloorview Research Institute, Toronto, December 2016

/research

What are we doing?
• Stage 1: Feasibility study • 3 girls and 3 boys
• 6-17 years old
• Completed (2015-2016; funded by Thyne Reid Foundation & Novita)
• Stage 2: Randomised controlled trial • 30+ children & young people
• Mixed methods
• 2016-18; funded by Channel 7 CRF& Novita
• Stage 3: In the pipeline… • Come and talk to us over a glass of wine!
/research

What do we know so far?
• Kids love the physio sessions and a chance to work on
‘fun’ goals
• Substantial improvements from physio sessions
• Some kids love the WalkAide and others are not so
keen
• It makes a big difference to have the Challenge test as
a meaningful outcome measure that kids enjoy!
/research

“[My physio] set me some really fun tasks so I found that pretty cool”.
“I did a balance [goal] and I think I didn’t fall over in a month or two. It was all worth it! I find stuff like that really fun, doing exercise.”
/research

Real (NDIA) world research
• Supporting the need for physio for high functioning kids
• Hoping to provide evidence for the cost effectiveness of
the physio+WalkAide intervention
• Negotiating rigorous research methodology in a
community-based service
/research

• “I didn’t think I could run one lap [of the oval]….and I did
– and it felt good!”
Why we do it…
/research

Project contacts:
• Novita Switch Access Solutions Assessment – [email protected]
• Let’s Play – [email protected]
• Activity Boost Challenge – [email protected]
• Quality of Life – [email protected]
Knowledge & Innovation – [email protected]
/research
For more information
General contact:

Thank You!

Three year trajectories of
global perceived quality of life for youth with chronic health conditions
Presented by : Virginia Wright, PT, PhD – Senior Scientist and Holland
Bloorview Chair in Pediatric Rehabilitation, Bloorview Research Institute,
Toronto, Ontario, Canada
Co-Principal investigator on this CIHR funded project: Janette McDougall,
PhD - Researcher, Thames Valley Children’s Centre, London, Ontario,
Canada

For more information on our research and downloadable copies of our papers
please visit:
Please visit our webpage: http://www.tvcc.on.ca/qol
You can also reach us directly at: [email protected] and


Our Key Questions: What patterns of change occur
in the QOL of youth over a 3 year period?
What are the key factors affecting QOL?
Three year follow-up of youth with chronic conditions to learn
about trajectories of change in QOL and the key factors that
affect QOL . Mixed methods design
Quantitative component: Youth (11 to 17 years) and their
parents completed our study surveys four times over a
3-year follow-up interval. This timing would let us capture
QOL through key transition stages.
Funded by: Canadian Institutes of Health Research
2009-2017 ($742,340)

Our Research Team
• Co-Principal Investigators
– Janette McDougall, Thames Valley Children’s Centre, London, Canada
– Virginia Wright, Bloorview Research Institute, Toronto, Canada
• Co-investigator
– Linda Miller, Western University, London, Canada
• 8 OACRS Centres (London, Toronto, Ottawa, Sudbury, Chatham-Kent, Windsor, Kingston, Simcoe York)
– 2 Clinician/Researchers
– 2 Project Coordinators
– 7 Research Assistants
– 18 Study Interviewers 8 Collaborators

Introduction
• Optimizing quality of life (QOL) for children and youth is a primary goal of children’s rehabilitation services
• Many supports and interventions directed toward this goal

Introduction
• Optimizing quality of life (QOL) for children and youth is a primary goal of children’s rehabilitation services
• Many supports and interventions directed toward this goal
• It is important to understand the key factors that influence QOL and changes in QOL for children and youth with chronic conditions

How would you define quality of life?
Think about what affects your QOL …

How would you define quality of life?
Think about what affects your QOL …
‘ Quality of life is subjective and multidimensional,
encompassing positive and negative features of life.
It is a dynamic condition that responds to life
events: A job loss, illness or other upheavals can
change one's definition of "quality of life" rather
quickly and dramatically.’
Accessed at
http://www.ieseinsight.com/doc.aspx?id=1478

How would you define quality of life?
Think about what affects your QOL …
"Quality of life" is subjective and multidimensional,
encompassing positive and negative features of life.
It is a dynamic condition that responds to life
events: A job loss, illness or other upheavals can
change one's definition of "quality of life" rather
quickly and dramatically.
“Quality Of Life: Everyone Wants It, But What Is It?”
• Life satisfaction, which is subjective and may fluctuate.
• Multidimensional factors that include everything from physical health, psychological state, level of independence, family, education, wealth, religious beliefs, a sense of optimism, local services and transport, employment, social relationships, housing and the environment.
• Not just the absence of disease but the presence of physical, mental and social well-being.
• Our interpretation of facts and events, which helps to explain why some people with disabilities report an excellent "quality of life" while others don't.
• Our level of acceptance of our current condition, and our ability to regulate negative thoughts and emotions about that condition.
Accessed at - http://www.ieseinsight.com/doc.aspx?id=1478&%3Bar=17

Many measures of QOL for children and youth
• Many focus on physical, emotional, social functioning/well-being
and measure health as a part of quality of life
• But how do we then separate QOL from health factors?
• A few avoid a focus on health and try to capture ‘satisfaction’ with broad aspects of life
• Regardless of which one uses, need to be aware of what is being measured and interpret the findings accordingly
• Many measures have both child and parent report options
• Might want to compare child and parent report
• Evidence that children with disabilities tend to rate their QOL higher than their parents do as proxies, while children with acute/new conditions are more inclined to rate QOL lower than parents do

QOL as a driving force in policy development
• “There is now a rising worldwide demand that policy be
more closely aligned with what really matters to
people as they themselves characterize their well-being.
More and more world leaders are talking about the
importance of well-being as a guide for their nations and
the world.”
Professor Jeffrey D. Sachs, Director of the Earth Institute at
Columbia University and Special Advisor to the UN Secretary
General

The qualitative part of our research

What our youth had to say …
• Qualitative descriptive research design with emphasis on youths’ lived experience
• 18 clients, Ages 11 - 20 years
– Youth had: cerebral palsy (10), autism spectrum disorder (4), other central nervous disorder or developmental delay (4)
– Had not been involved in our quantitative study so did not have exposure to any QOL measures or our QOL lingo!
• Each did a semi-structured individual interviews and attended a focus group a few weeks after
• This was first published study to specifically ask youth
with chronic conditions what QOL means to them

What our youth had to say …
• Qualitative descriptive research design with emphasis on youths’ lived experience
• 18 clients, Ages 11 - 20 years
– Youth had: cerebral palsy (10), autism spectrum disorder (4), other central nervous disorder or developmental delay (4)
– Had not been involved in our quantitative study so did not have exposure to any QOL measures or our QOL lingo!
• Each did a semi-structured individual interviews and attended a focus group a few weeks after
• This was first published study to specifically ask youth
with chronic conditions what QOL means to them
• Interviews and focus group conducted by
two clinicians with ++ interview experience
• Audio-taped, transcribed
• Coding process - NVivo10, line-by-line
coding of transcripts, codes collapsed into
categories, and themes identified

We asked each youth …
• What does quality of life mean to you?
• What do you think makes a difference to your quality of life?
• Note – we also asked questions about the meaning and experiences of self-determination and spirituality

To these youth, quality of life meant….
• “How enriched and fulfilling your life is.”
• “How you enjoy life and get the best out of life.”
• “That you live life to the fullest and you never give up.”
• “How satisfied you are with living.”
• “Being a useful person and being happy.”
• “Making sure everyone has a good life.”
• “The value of your life and how much you think you are enjoying your life.”
• “Having a sense of purpose.”
• “Having fun.”
• “Doing the best you can with your circumstances and abilities.”
• “To be alive.” (see McDougall et al., 2015)

Key Themes Related to QOL …
1. Relationships are essential
“If you don’t have your family to raise you, then how do you survive in this world? I mean, generally my Mom and Dad, but I can throw siblings in there too because they teach you how to love too.” “Friends give you acceptance, encouragement, someone to talk to, and someone to learn from.”
“Just knowing that my teachers and Education Assistants are there when you need them”

Key Themes Related to QOL …
2. Supportive environments
“Parents always making sure food is on the table.”
“Career planning and those supports at school”
“Having access to things that help me when I can’t write very well, so like having access to a computer”
“Having more wheelchair accessible places”

Key Themes Related to QOL …
3. Doing things
“I can do most things I want to do, like the wheelchair basketball. I’m actually better at it than regular basketball.”
“It’s always fun to laugh with my friends and sometimes we all just get together and play a game.”
“…going to the mall, shopping, getting out of the house so Mom can have her quality time”

Key Themes Related to QOL …
4. Personal growth and moving forward
“For me, if I’m doing well in school, then I sort of know that in a sense I’m doing something right, it’s sort of proof on paper that I’m doing well in life.”
“I was really excited when my Mom woke me up at 8 o’clock in the morning and said, very calmly, ‘by the way you’ve been accepted into college’. Yeah that was all she had to say and I jumped out of bed and I started hooting and hollering and showed my Dad, I was happy.”

Key Themes Related to QOL …
“ “There’s people that give you a label, but ultimately it’s not their fault…they’re not educated about that. Or they just think they should treat everybody in a wheelchair like that. But…you can’t get mad at them…it’s not a big deal…I’m just happy.”
“Asperger’s is a good disorder, did you know that? It makes you very smart.”
5. Self-understanding/acceptance of disability

The quantitative arm
• 439 youth across 8 centres in Ontario, Canada (rural to large city)
• Ages 11 to 17 years (mean = 13 years, 10 months) when they entered
the study – each followed for 3 years
• 56% male
• 35%) had cerebral palsy, 13% acquired brain injury,
9% communication disorders, 8% autism spectrum disorders,
8% spina bifida, and 26% another condition (e.g., developmental
delay, Down syndrome, amputee, etc.)
• Parent participants were mainly birth mothers (83%)
Study methods
• Questionnaires were administered to youth and their primary
caregiver shortly after admission to the study and then again
every 12 months for 3 years (4 time points – the anticipated
challenge would be to get as many back as possible!)
• Each youth took part in a face-to-face guided completion of
forms with study interviewer (30-60 minutes)
• The parent questionnaire (30-60 minutes) was self-completed
at the same time and place as the youth interview
• 302 (70%) youth/parent dyads completed all four data collection
time points

Primary measure
• Perceived QOL: Life Satisfaction
– Student Life Satisfaction Scale (SLSS) (Huebner, 1991)
– Youth self-report and parent report - domain-free overall life
assessment – no health questions!
– 7 items using 6-point rating scale from 1 = strongly disagree to 6 =
strongly agree
– My life is going well (My child feels his/her life is going well)
– My life is just right
– I would like to change things in my life
– I would like to have a different kind of life
– I have a good life
– I have what I want in life
– My life is better than most kids

Measures amalgamated into our study survey
• Youth Functioning/Personal Factors
– Pain/Physical Symptoms - The Child and Adolescent Factors Inventory (Bedell, 2004)
– Emotional Functioning - Strengths and Difficulties Questionnaire (Goodman, 1997)
– Spirituality (defined as deep feelings/beliefs) - Spiritual Transcendence Index (Seidlitz
et al., 2002)
– School Productivity/Engagement - School Productivity Measure (McDougall, 2008)
– Self-Determination (i.e., having the power and will to make choices) - ARC-Brief Version (ARC’s Self-Determination Scale - adapted) (Wehmeyer & Kelcher, 1995)
• Interpersonal/Environmental Factors
– Social Support from Parents - Social Support Appraisals Scales (Dubow & Ullman, 1989)
– Overall Family Functioning - Family Functioning Scale (NLSCY, 1998)
– School Belongingness/Safety - (HBSCS, 2005)
– Home and Community Environment (Physical, Attitudinal, Social, and
Policy Barriers) - Child/Adolescent Scale of Environment (Bedell, 2004)

Baseline Findings
Life Satisfaction Scale Total Scores
Respondent Mean (/30) SD
Youth
25.43 5.1/6
Moderately agree
4.32
Parent
23.28 4.6/6, Mildly to
moderately agree
4.68
Youth scores higher than parent scores t = 09.06, p<0.001
Longitudinal Data Analysis
• Latent Class Growth Analysis
– Latent Class Growth Analyses (LCGA) were conducted to identify groups of youth with unique trajectories of perceived QOL from both youth and parent perspectives
• Multinomial Regression Analyses
– Multinomial logistic regression analyses were then conducted to determine the influence of a given variable predicting the likelihood of belonging to one group in relation to being in the largest group
– Basic health and socio-economic variables were included to control for their effect (i.e., age at diagnosis, youth and parent age, youth and parent gender, family income, parent education, parent marital status)

Example of trajectories: GMFCS Motor Growth Curves
Functional groupings
of kids with cerebral
palsy – used to be
classified as mild,
moderate , severe
Used Gross Motor
Function Measure
scores from 300+
kids ages 1 to 15

Model of distinct trajectories for youth report over 3 years
Class 2
85.7% of sample
Class 1
14% of sample
Overall group mean on
the Life Satisfaction
Measure = 25.4 / 30

Model of Distinct Trajectories for Parent Report
Overall group mean on
the LIfe Satisfaction
Measure = 23.2 / 30
Class 3
36% of sample
Class 2
46% of sample
Class 1
18% of sample
Interpreting Longitudinal Findings
• Based on youth and parent reports, most youth are faring well
in terms of their perceived QOL (life satisfaction)
• However, a significant percentage of youth in both the youth
(14%) and parent (18%) reports had moderate/low QOL scores.
A number of the high QOL youth were viewed by parents as
having moderate QOL (47%)
• Surprisingly, all trajectories were stable in nature

How might we explain this stability?
• Cummins (2010) demonstrated a theory of homeostasis:
Humans have a subjective wellbeing ‘set-point’, with
individual set-points ranging from 70 to 90 out of 100, and
a mean of 80
• If groups within a population drop below this set-point, it
represents homeostatic failure: when groups of
individuals experience excessive demands and lack of
resources, homeostasis can be overwhelmed
• When demands are ongoing, this homeostatic drop can
become a stable and ongoing phenomenon!

How does Homeostasis Theory
play out in real life?
• Tomyn et al. (2015) tested predictions based on Homeostasis
Theory about intervention outcome for youth with various
physical and psychological conditions
• They hypothesized youth functioning within a normal set-point
range would achieve just a small increase from an
intervention. Alternatively, those experiencing homeostatic
failure would raise their subjective well-being substantially
• Their study results confirmed these hypotheses

Predictors of Group Membership
for Youth QOL (Youth Report)
Estimated Odds Ratios
C1 (vs C2) Correlates
Youth functioning/personal factors
Emotional symptoms (YR) 1.32**
Pain/other physical symptoms (PR) 1.38
Self-determination (YR) 0.88***
Spirituality (YR) 0.86***
School productivity/engagement (PR) 0.80*
Interpersonal/Environmental factors
Youth social support from family (YR) 0.84***
Overall family functioning (PR) 1.04
School belongingness/safety (YR) 0.88*
Home and community barriers (PR) 1.03
YR = Youth Report; PR = Parent Report
C2 = high and stable quality of life (reference group) (84.3 % n = 367 )
C1 = moderate/low and stable quality of life (15.7% n = 68)
* p < .05; ** p < .01; *** p < .001
n = 435 youth; 8 youth treatment centres
. . .
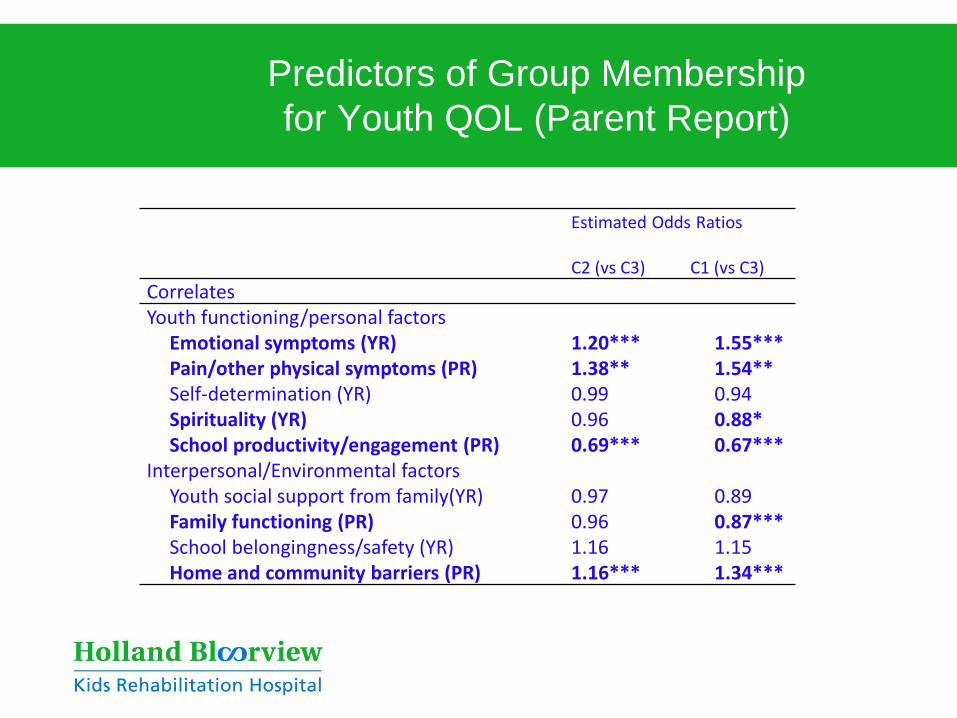
Predictors of Group Membership
for Youth QOL (Parent Report)
Estimated Odds Ratios
C2 (vs C3)
C1 (vs C3)
Correlates Youth functioning/personal factors
Emotional symptoms (YR) 1.20*** 1.55*** Pain/other physical symptoms (PR) 1.38** 1.54** Self-determination (YR) 0.99 0.94 Spirituality (YR) 0.96 0.88* School productivity/engagement (PR) 0.69*** 0.67***
Interpersonal/Environmental factors Youth social support from family(YR) 0.97 0.89 Family functioning (PR) 0.96 0.87*** School belongingness/safety (YR) 1.16 1.15 Home and community barriers (PR) 1.16*** 1.34***

Factors Related to Perceived QOL: Comparing Method Findings
Quantitative
• Physical and Emotional Well-being (pain/physical symptoms, emotional well-being)
• Purpose and Passion (spirituality, school productivity/engagement, self-determination)
• People (family support, family functioning, school safety/ belongingness, home, school, and community environments)
Qualitative
• Physical and Emotional Well-being (mobility, accessibility, self understanding, acceptance of disability)
• Purpose and Passion (spirituality, personal growth/moving forward, self-determination)
• People (relationships with family, friends + others, doings things, supportive home, school, community environments)

Points of reflection…
• In what ways do our services currently recognize and
support the personal vision, motivation and relational
needs of individual youth?
• What changes in services related to youth purpose,
passion, and connections with others could enhance their
QOL?
• How can environments (home, school, community) be
modified to enhance youth QOL?

Novita’s projects demonstrate that it is all about optimizing children’s QOL
from early years on …

But what are the challenges for our QOL team? How do we get knowledge from our
QOL study with youth into practice?
• Quantitative AND qualitative findings both suggest a holistic, positive approach is important
Encourage more thinking about emotional well-being, self-determination, school productivity, social support, and community participation.
Provide additional supports like spiritual care and self-advocacy support, and advocate for optimal school and community environments where youth can thrive and develop to their full potential

Knowledge into Practice
• Service providers should consider our key themes/factors when doing initial and ongoing assessments to ensure ‘at-risk’ youth are identified for the services, supports, and resources they may need
• Policy makers could consider these themes/factors when developing universal prevention initiatives to safeguard resilience for all youth - the goal is to prevent shift to adverse developmental trajectories of QOL for youth with unmet needs as they progress through adolescence

The new title!
Quality of Life for Youth
As They Move Through Adolescence: People, Purpose, and Passion Matter