a systematic review of disability awareness interventions for children and youth
TRANSCRIPT

623
Disability & Rehabilitation, 2013; 35(8): 623–646© 2013 Informa UK, Ltd.ISSN 0963-8288 print/ISSN 1464-5165 onlineDOI: 10.3109/09638288.2012.702850
Purpose: Children’s lack of knowledge about disability can adversely impact their attitudes toward people with disabilities. The purpose of this study is to review the common elements of effective disability awareness interventions. Methods: A systematic review of disability awareness interventions for children and youth was conducted to assess the effective components of these interventions. Electronic searches were conducted using OVID, CENTRAL, PsychInfo, ERIC, Social Science Citation Index, GreyNET Scopus and Google Scholar. The inclusion criteria included (i) an intervention raising awareness about disability, (ii) school-age children with the average age between 5–19 years old, (iii) at least one measurable outcome focusing on knowledge about disability or attitudes towards and/or acceptance of people with a disability and (iv) published article or grey literature. Results: Of the 1031 articles that were identified in the search, 42 met the criteria to be included in the review. We classified the disability awareness interventions into 5 broad types including (i) social contact, (ii) simulation, (iii) curriculum, (iv) multi-media curriculum and (v) multiple components. Thirty-four studies showed an improvement in attitudes towards and/or acceptance of peers with disabilities. Eight of these studies also demonstrated an improvement in knowledge of people with disabilities. Five of the interventions found no support for improving knowledge about, or acceptance of people with disabilities. Conclusion: Disability awareness interventions can successfully improve children’s knowledge about and attitudes towards peers with a disability; they should include several different components over multiple sessions. Relevance: These findings are being used to further develop disability awareness interventions to help improve the social inclusion and participation of children with disabilities within mainstream classrooms.
Keywords: Children, disability awareness, intervention, review, school-age, youth
Introduction
Improving inclusive environments within classrooms is especially critical for children with disabilities because of the increased prevalence of inclusive education (i.e. children who spend most or all of their time being schooled with their typically developing peers). Evidence consistently shows that being placed in an integrated classroom does not guarantee that children with disabilities will be accepted, valued and included [1–3]. For instance, nearly fifty percent of children with disabilities feel that they do not belong within their class, feel lonely, isolated and unsafe [4,5]. This is concerning because there are over 200,000 Canadian children and youth
Review
A systematic review of disability awareness interventions for children and youth
Sally Lindsay1 & Ashley edwards2
1Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, Toronto, Ontario, Canada and 2Inwentash Faculty of Social Work, University of Toronto, Toronto, Ontario, Canada
Correspondence: Sally Lindsay, Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, 150 Kilgour Road, Toronto, Ontario, M4G 1R8, Canada. E-mail: [email protected]
Disability & Rehabilitation
2013
35
8
623
646
© 2013 Informa UK, Ltd.
10.3109/09638288.2012.702850
0963-8288
1464-5165
Review of disability awareness interventions
11June2012
• Well-designed disability awareness interventions for children and youth can help improve knowledge about disability, attitudes towards people with a dis-ability and acceptance of peers with a disability.
• Rehabilitation health care providers and educators should be trained to recognize when children with disabilities are being socially excluded and be pre-pared to provide or recommend appropriate resources and interventions on how to address this issue.
• Clinicians, educators and children with disabilities should all be involved in the development of disability awareness programs.
• Educators should carefully choose an appropriate intervention to meet the needs of the children in their class while considering age appropriateness and diver-sity of the students. It is also important for educators to be cognizant of the broader societal influences that impact attitudes towards disability.
Implications for Rehabilitation
(Accepted June 2012)
S. Lindsay & A. Edwards
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

624 S. Lindsay & A. Edwards
Disability & Rehabilitation
living with a disability [6], the majority of whom attend integrated classrooms and are at an increased risk for social exclusion and bullying [4,7,8].
Children’s adverse attitudes toward peers with disabilities have been widely documented in preschool, elementary and secondary school settings [1,9]. Research demonstrates that children often only interact with peers who have a disability in structured settings where they are encouraged to do so [3,4]. Favazza et al. [10] found that without supportive programs children often have low acceptance of peers with disabilities. For example, a meta-analysis of 20 studies found that children aged 3–12 years old preferred being in proximity to typically developing peers compared to children with disabilities [11].
Children’s attitudes towards their peers with disabilities are often strongly influenced by their degree of knowledge about disability, which stems from their social environments [3,7,12,13]. Adverse attitudes and social exclusion are often the result of children’s lack of knowledge about disabilities [2,3]. Given that perceptions of disability often shape attitudes and behaviours, it is vital to improve children’s understand-ing of people with disabilities [13,14]. One key mechanism of improving attitudes is through disability awareness interventions.
Importance of disability awareness and social inclusion at school
The social inclusion of all children is critical. According to the UN Convention on Rights of the Child [15] all children “should enjoy a full and decent life, in conditions which ensure dignity, promote self-reliance and facilitate the child’s active participation in the community.” Thus, most integrated schools place emphasis on belonging, acceptance and sup-portive peer relationships [16]. The provision of inclusive and accepting social climates within schools is necessary to decrease the likelihood that children will be socially excluded from their peers [16]. This is particularly important because children who are victims of social exclusion often experience adverse physical, mental and social consequences such as depression, anxiety and low self-esteem [8,17,18]. It is criti-cal therefore, to help improve the social inclusion of children with disabilities because acceptance and a sense of belonging are essential to a child’s social and academic development and overall quality of life [3,4,19,20]. For integrated classrooms to be successful, children need opportunities to learn more about social inclusion and people with disabilities through ongoing learning opportunities in a co-operative environ-ment [4]. One key mechanism of improving inclusive envi-ronments is through social inclusion and disability awareness interventions, which can help children to develop respectful attitudes toward individual differences [21].
Disability awareness interventions
Interventions aimed at increasing children’s disability aware-ness within mainstream classrooms can help improve knowl-edge, attitudes and acceptance of people with disabilities [21–23]. There have been a wide variety of formats of disability
awareness interventions including providing information about disabilities [23,24], videos [25], drama [26], theatre and puppet shows [20,26–28], discussions [26], stories [29], simu-lations [30,31], structured interactions [10] and classroom activities [32,33] among others [34,35]. The outcomes of such disability awareness interventions are mixed. For example, some researchers [24,34] have found a positive change in attitudes toward people with disabilities following a disability awareness intervention, while others [23] have reported that there was no change.
Despite the growing literature on the inclusion of chil-dren with disabilities in mainstream classrooms and the subsequent increase in disability awareness interventions, the common elements of the effective components have not been synthesized and remain largely unknown. Indeed, little atten-tion has been paid to effective strategies to promote positive attitudes towards their peers with disabilities [36]. It is critical that disability awareness interventions are effective so that they can provide typically developing children with opportu-nities to learn and develop positive attitudes about differences in a respectful context [37,38]. Helping children nurture such attitudes at school can contribute to the creation of a positive social climate among children and youth [4,37]. Addressing attitudes towards people with disabilities in childhood is important because at this age their attitudes are still evolving and early interventions may be especially beneficial [27,34]. This review aims to synthesize the common characteristics of effective disability awareness interventions for children and to make recommendations for their further development.
Method
The objective of this systematic review is to critically appraise the evidence of disability awareness and social inclusion interventions for children and youth.
Research questions(1) What are the common elements of effective disability awareness interventions for children and youth? and (2) What recommendations can be made for further development of disability awareness programs?
Search strategyThe following databases were searched for relevant articles in English published from 1980–September 2011: CINAHL, MEDLINE(OVID), Healthstar (OVID) PubMed, EMBASE, Web of Science, Cochrane Databases for Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), ERIC, PsychInfo, Social Science Citation Index, Scopus, GreyNet, Conference Proceedings, and Google Scholar. The search strategy involved using the following subject headings and search terms: “disab* awareness”, and/or “social inclu-sion” were combined with “attitude” and/or “outcome.” The “similar article” function and manual cross-referencing from identified studies were used to enhance the search.
The inclusion criteria involved (i) an intervention to raise awareness about disability or to enhance social inclusion for people with disabilities; (ii) school-age children and youth
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 625
© 2013 Informa UK, Ltd.
with the majority of the sample or average age between 5–19 years old; (iii) at least one measurable outcome focusing on knowledge about disabilities, or attitudes towards people with disabilities; and (iv) published or grey literature from 1980–September 2011. These criteria were chosen because child-hood is an ideal time to help develop positive attitudes towards people with disabilities. This date range was chosen because research on this topic has dated back to the early 1980s when inclusive education policies started being implemented.
Through this search process 1031 articles were identified and two people reviewed the titles and abstracts of these arti-cles. Nine hundred and forty-seven articles were eliminated based on their title or abstract not being related to the current search. After removing duplicates and applying the inclusion criteria 42 articles remained in the final analysis. Full articles were then retrieved and evaluated for relevance.
Data abstraction and classification processData from the included studies were extracted and compiled by one author and independently verified by another investi-gator using a structured abstraction form that was based on previously completed systematic reviews [38]. Each article that met the inclusion criteria was read in its entirety by both authors before summarizing the key attributes. The first author kept a journal of decisions as part of an audit trail to ensure the study’s conformability. These journal entries were used to formulate discussion points for meetings between the authors.
Articles were summarized and coded by the second author and then checked by the first author and a research assistant. A list of all the key themes was developed and a constant com-parison method was used to facilitate the distinction of pat-terns, variations and relationships [39]. Data elements were compared and critiqued and the commonalities were sum-marized and evaluated. After the initial analysis was complete both authors reviewed the key themes identified and minor adjustments were made until consensus was reached. This review method is compatible with the use of varied data from diverse methodologies [40].
The articles were classified into a hierarchy of evidence based on the rigour of their methodology. We used the American Academy of Neurology’s classification of evidence for therapeutic intervention [41]. A summary of this classifica-tion system involves the following: (class I) randomized con-trolled trials meeting rigorous; (class II) matched prospective cohort studies or RCT in a representative population lacking on of the criteria in class one; (class III) all other controlled trials; (class IV) all other studies that did not meet the criteria for class I to III [41]. Recommendations for the effectiveness of the interventions to improve knowledge and attitudes were based on the strength of evidence of all articles [41].
Results
A total of 42 studies were included in the review. Table I pro-vides an overview of the study characteristics including sam-ple, purpose, design, components of the disability awareness interventions, results and limitations of the studies. In terms
of the focus on the intervention, 11 focused on disability in general, followed by physical disabilities (10), mental illness (7), several disabilities (6), autism (2), intellectual disability (2) and 1 article focusing on each one of the following condi-tions: schizophrenia, Tourette Syndrome, cerebral palsy and visual impairments. Sample sizes ranged from 3 to 2081. The average ages of the children involved in these studies ranged from 5 to 19 years old. Many of the studies did not contain detailed demographic information about their sample so it is difficult to make comparisons between the articles in this respect. Of the studies that gave details about the gender com-position of the sample, they were roughly equal in terms of males and females in most studies.
A wide variety of standardized measures were used to evalu-ate the effectiveness of the interventions (refer to Table I). The majority of the studies focused on measuring attitudes towards people with disabilities (e.g. Chedoke-McMaster Attitudes Toward Children with Handicaps (CATCH), Peer Acceptance Scale, Peers Attitudes Toward Handicapped (PATH), Acceptance Scales for Kindergartners (ASK), Children’s Attitudes Toward Integrated Physical Education-Revised (CAIPE-R)), accep-tance of people with disabilities (e.g. Children’s Social Distance from Handicapped) and behaviour (Personal Contact with Disabilities Scale) followed by knowledge of disability (e.g. Children’s Knowledge About Handicapped Scale). Several other non-standardized measures were also used.
The majority of the studies (32) did not have a theoretical framework to inform their intervention. Of the studies that did have a theoretical framework they included such theories as behaviour change theory [42], theory of planned behaviour [24,43,44], social learning theory [24,43], social contact the-ory [16,34], social model of disability [22], social desirability and attribution theory [23], theory of mere exposure effect [3], theory of persuasive communication and social cognitive theory [3,16], cognitive behavioural theory [7,16], models of attitude change [45], and interpersonal relations theory [45].
First, we provide an overview of the overall effectiveness of the interventions by the type of outcome measured. Next, we outline common components of the effective interventions. Finally, we highlight key lessons learned and make recom-mendations for the further development of disability aware-ness interventions.
Effectiveness of the interventionsThere were two broad outcomes that these interventions measured: (i) knowledge of people with disabilities and (ii) attitudes towards and acceptance of peers with disabilities. Overall, the majority of the studies (34) showed significant improvements in attitudes towards children with a disability as well as improvements in knowledge about people with disabilities (8 studies) (refer to Table II). Five studies did not demonstrate a significant improvement in knowledge or attitudes following the intervention.
Attitudes towards and acceptance of people with disabilitiesA key outcome among the studies we reviewed involved attitudes towards and acceptance of people with a disability.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

626 S. Lindsay & A. Edwards
Disability & Rehabilitation
Tabl
e I.
Stud
y ch
arac
teris
tics.
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dySo
cial
con
tact
Arm
stro
ng
et a
l., 1
987
(Can
ada)
(n/a
) 87
9–13
yea
rs
old
(pub
lic
scho
ol,
segr
egat
ed
clas
ses)
Phys
ical
d
isabi
litie
sRa
ndom
ized
co
ntro
l tria
l (46
bu
ddie
s, 45
co
ntro
ls)
Che
doke
-McM
aste
r At
titud
es T
owar
d C
hild
ren
with
H
andi
caps
(C
ATC
H);
Perc
eive
d
Com
pete
nce
Scal
e;
Pare
ntal
Atti
tude
s To
war
d C
hild
ren
with
Han
dica
ps
(PAT
CH
)
N/a
To e
valu
ate
the
eff
ectiv
enes
s of a
“b
uddy
” pro
gram
de
signe
d to
impr
ove
at
titud
es o
f no
n-di
sabl
ed ch
ildre
n
tow
ards
phy
sical
ly d
is-ab
led
child
ren
•Assignedabu
ddy
of
the
sam
e ge
nder
(w
ith a
disa
bilit
y)•Meetw
eeklyfor3
m
onth
s, op
port
unity
fo
r soc
ial i
nter
actio
n,
no a
cade
mic
elem
ents
•Sign
ificantly
impr
oved
attit
udes
to
war
ds
child
ren
with
di
sabi
litie
s (C
lass
II)
•Ea
chsc
hool
deve
lope
d th
eir
own
prog
ram
(not
st
anda
rdiz
ed a
cros
s sc
hool
s)•Littlekn
ownabou
tlo
ng te
rm im
pact
•Mostb
uddieswere
fem
ale
Mar
mon
et a
l.,
2007
(Isr
ael)
170
(n/a
)M
ean
age
1 0.
5 ye
ars
Disa
bilit
y (g
ener
al)
Qua
si
expe
rimen
tal
desig
n
(non
-equ
ival
ent
cont
rol g
roup
)
Attit
udes
tow
ards
ch
ildre
n w
ith d
is-ab
ilitie
s (ba
sed
on
Sille
r et a
l.’s (1
967)
m
easu
re; C
hild
ren’s
Se
lf-Effi
cacy
Sca
le
(Ban
dura
198
9)
Con
tact
th
eory
(A
llpor
t 19
54)
To a
sses
s to
wha
t ext
ent
a di
rect
cont
act p
rogr
am
(Par
tner
s to
Incl
usio
n)
chan
ged
the
gene
ral
educ
atio
n st
uden
ts’
attit
udes
tow
ards
ch
ildre
n w
ith
disa
bilit
ies
•1-yearprogram
pr
ovid
ed d
irect
co
ntac
t with
stud
ents
w
ith d
isabi
litie
s th
roug
h w
eekl
y or
bi
-wee
kly
join
t ac
tiviti
es la
stin
g 30
–90 m
in•
mean#ofdire
ct
cont
act m
eetin
gs w
as
16.7
5
•Sign
ificantly
impr
oved
di
sabi
lity-
rela
ted
attit
udes
and
spec
ific
self-
effica
cy im
prov
ed
over
tim
e (C
lass
III)
•Participantsweren’t
rand
omly
ass
igne
d•Con
troland
ex
perim
enta
l gro
ups
wer
e no
t sy
stem
atic
ally
m
atch
ed
New
berr
y an
d Pa
rish,
198
7 (U
S)45
6 (4
9%
fem
ale)
8–11
yea
rs
old
Men
tal,
phys
ical
an
d in
telle
ctua
l di
sabi
litie
s, he
arin
g
Pre-
and
post
-tes
ts;
rand
omly
ass
igne
d en
viro
nmen
tal a
nd
cont
rol g
roup
s
Pers
onal
Attr
ibut
e
Inve
ntor
y fo
r C
hild
ren
N/a
To e
xplo
re so
cial
in
tera
ctio
n ou
tsid
e th
e cl
assr
oom
; to
asse
ss if
th
ere
wer
e at
titud
inal
be
nefit
s for
child
ren
with
an
d w
ithou
t di
sabi
litie
s to
inte
ract
at
a w
eekl
y sc
out
mee
ting
•6weeks×1hper
wee
k•10group
s,5includ
ed
1 m
embe
r with
a
disa
bilit
y
•Dire
ctso
cialco
ntact
can
fost
er in
crea
sed
acce
ptan
ce a
nd m
ore
posit
ive
attit
udes
(C
lass
III)
•Labelling
ofthe
disa
bled
child
•Onlyon
echild
in
each
scou
t tro
op h
ad
a di
sabi
lity
Pier
cy e
t al.,
200
2 (N
ew Z
eala
nd)
51 (4
3%
fem
ale)
5–7
year
s old
(6
boys
from
seg-
rega
ted
clas
s;
rem
aind
er fr
om
mai
nstr
eam
cl
ass)
Inte
llect
ual
disa
bilit
ies
Rand
omly
ass
igne
d to
one
of 3
gro
ups
(co-
oper
ativ
e
lear
ning
gro
up,
soci
al co
ntac
t gr
oup,
cont
rol);
pr
e-po
st te
st
Peer
-Acc
epta
nce
Scal
e, Po
pula
rity
In
dex,
Soc
ial-D
is-ta
nce
Scal
e,
Beha
viou
r O
bser
vatio
ns
N/a
To u
nder
stan
d th
e
impa
ct o
f a
coop
erat
ive-
lear
ning
pr
ogra
m o
n th
e so
cial
ac
cept
ance
of c
hild
ren
with
mod
erat
e to
seve
re
lear
ning
disa
bilit
ies
•10weekprogram
•Coo
perativ
elearning
gr
oup,
soci
al-c
onta
ct
grou
p
•Sign
ificantly
incr
ease
d po
sitiv
e in
tera
ctio
ns b
etw
een
child
ren
with
and
w
ithou
t int
elle
ctua
l di
sabi
litie
s (C
lass
III)
•Unk
nownwhether
coop
erat
ive-
lear
ning
is
bette
r em
brac
ed b
y yo
unge
r chi
ldre
n
(Con
tinue
d)
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 627
© 2013 Informa UK, Ltd.
Soci
al c
onta
ct
Fred
eric
kson
and
Tu
rner
, 200
3 (U
K)20
(5%
fe
mal
e)6–
12 y
ears
ol
d (in
tegr
ated
cl
asse
s)
Emot
iona
l and
be
havi
oura
l di
fficu
lties
Com
paris
on/
cont
rol g
roup
; ra
ndom
ized
(b
etw
een
grou
p de
igns
)
Soci
omet
ric R
atin
g Sc
ale;
Sel
f-Pe
rcep
tion
Profi
le fo
r Chi
ldre
n;
Teac
her’s
Rat
ings
Sc
ale
of C
hild
’s
Act
ual B
ehav
iour
; M
y C
lass
In
vent
ory
N/a
To e
valu
ate
two
smal
l in
terv
entio
ns, a
nd
obse
rve
the
impa
ct o
f C
ircle
of F
riend
s on
va
rious
asp
ects
of a
ch
ild’s
soci
al
com
pete
nce
•Ph
ase1:Circ
leof
Frie
nds f
or 6
wee
ks•Ph
ase2:ju
ststud
ents
who
had
not
par
-tic
ipat
ed in
Circ
le
of F
riend
s; 6
wee
kly
mee
tings
(firs
t by
ed. p
sych
olog
ist, r
est
by sc
hool
), w
ithin
-su
bjec
ts d
esig
n
•Sign
ificantlyim
proved
perc
eptio
ns a
bout
di
sabl
ed ch
ild•Interventio
nhad
posit
ive
effec
ts o
n so
cial
acc
epta
nce
by
clas
smat
es (C
lass
III)
•Po
tentialfornega-
tive
labe
lling
for t
he
disa
bled
child
•Sm
allsizeofstud
ygr
oup
Barr
ett a
nd R
an-
dall,
200
4 (U
K)
6 (3
3%
fem
ale)
Gra
des 3
/4
(incl
usiv
e sc
hool
)
Disa
bilit
ies
(gen
eral
)Pr
e-te
st, p
ost-
test
qu
estio
nnai
reSo
ciom
etric
qu
estio
nnai
reN
/aTo
inve
stig
ate
an
adap
ted
vers
ion
of th
e C
ircle
of F
riend
s pr
ogra
m
•6weeks(1
×weekfor
30 m
in) c
o-le
d by
an
Educ
atio
nal P
sych
olo-
gist
and
teac
her
•Structure:warmup
activ
ity, m
ain
activ
ity,
rela
xatio
n ex
erci
se•Mod
el1:circ
leof
frie
nds a
roun
d th
e ch
ild (c
hild
not
pr
esen
t in
clas
s di
scus
sion)
; Mod
el 2
: ch
ild w
ith d
isabi
lity
is in
clude
d in
clas
s di
scus
sion
whe
n
circ
le o
f frie
nds i
s in
trodu
ced;
Mod
el 3
: ci
rcle
of f
riend
s is s
et
up ar
ound
mor
e tha
n on
e chi
ld in
the c
lass
.
•Im
provedch
ildren’s
perc
eptio
ns (i
n th
e w
hole
clas
s con
tact
gr
oup)
(Cla
ss IV
)
•Shorttermin
terven
-tio
n •Who
leclassc
ontext
not a
ddre
ssed
Whi
take
r et a
l.,
1998
(UK
)(n
/a)
5210
–14
year
s ol
d
(mai
nstr
eam
sc
hool
)
Autis
mIn
terv
iew
s and
qu
estio
nnai
reno
t giv
enN
/aTo
faci
litat
e in
tera
ctio
ns
for t
he id
entifi
ed ch
ild
with
oth
er ch
ildre
n; to
re
duce
the
perc
eive
d im
pairm
ent f
or th
e
iden
tified
child
; re
cogn
ize
the
im
pairm
ent o
f soc
ial
skill
s for
child
ren
with
di
sabi
litie
s; an
d to
ad
dres
s spe
cific
in
divi
dual
pro
blem
s
•circleoffrie
nds
appr
oach
•4mainsteps:
es
tabl
ishin
g
prer
equi
sites
, di
scus
sion
with
the
clas
s, es
tabl
ish a
ci
rcle
, wee
kly
m
eetin
gs o
f the
circ
le•Meetin
g1:ledby
Autis
m O
utre
ach
Team
, tea
cher
sele
cts
6–8
circ
le m
embe
rs
•Sign
ificant
impr
ovem
ents
in
inte
ract
ions
with
ch
ildre
n w
ith
disa
bilit
ies
(Cla
ss IV
)
•Somechild
ren
beca
me
upse
t or
dist
ress
ed w
hen
the
iden
tified
child
re
acte
d un
expe
cted
ly
or in
tens
ely
•Nocontrolgroup
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

628 S. Lindsay & A. Edwards
Disability & Rehabilitation
Sim
ulat
ion
Pivi
k et
al.,
200
2 (C
anad
a)(n
/a)
609–
11 y
ears
ol
dPh
ysic
al
disa
bilit
yC
ontr
olle
d
pre-
test
, pos
t-te
st
desig
n; ra
ndom
The
Kno
wle
dge
Que
stio
nnai
re;
Chi
ldre
n’s S
ocia
l D
istan
ce fr
om
Han
dica
pped
Pe
rson
s Sca
le
N/a
To a
sses
s the
eff
ectiv
enes
s of a
vi
rtua
l rea
lity
co
mpu
ter g
ame
to
educ
ate
child
ren
abou
t ac
cess
ibili
ty a
nd
attit
udin
al b
arrie
rs
•30min,desktop
vir-
tual
real
ity p
rogr
am;
child
ren
view
ed g
ame
as if
they
wer
e sit
ting
in a
whe
elch
air
(exp
erie
nced
ob
stac
les,
stai
rs,
narr
ow d
oors
, ob
ject
s too
hig
h to
re
ach,
etc
)
•Programwas
effec
tive
for
incr
easin
g
child
ren’s
kno
wle
dge
of a
cces
sible
bar
riers
•Grades5
–6sh
owed
grea
test
chan
ge; n
o ge
nder
diff
eren
ces i
n kn
owle
dge
of
barr
iers
but
mal
es
had
high
er p
ost t
est
attit
ude
scor
e
(Cla
ss II
)
•Accessib
lesc
hooland
m
ay h
ave
alre
ady
had
posit
ive
attit
udes
Hut
zler
et a
l.,
2007
a (I
srae
l)75
(41%
fe
mal
e)7–
10 y
ears
ol
dPh
ysic
al
disa
bilit
yQ
uest
ionn
aire
Attit
udes
Tow
ards
Pe
ers w
ith
Disa
bilit
y;
Chi
ldre
n’s
Attit
udes
Tow
ards
Pe
ers w
ith
Disa
bilit
y Sc
ales
Theo
ry
of
plan
ned
beha
v-io
ur;
soci
al
lear
ning
th
eory
To d
eter
min
e th
e eff
ect
of th
e C
hild
ren’s
A
ttitu
des T
owar
ds P
eers
w
ith D
isab
ility
Sca
les
and
an e
lite
whe
elch
air
bask
etba
ll ga
me
on
alte
ring
chi
ldre
n’s
attit
udes
tow
ard
thei
r pe
ers w
ith d
isab
ilitie
s
•1h
simulatedm
ove-
men
t act
iviti
es
follo
wed
by
a
disc
ussio
n•Childrenwere
as
signe
d a
sim
ulat
ed d
isabi
lity
•Im
provedattitud
es
tow
ards
incl
udin
g ch
ildre
n w
ith d
isabi
li-tie
s (C
lass
IV)
•Nocontrolgroup
Hut
zler
et a
l.,
2007
b (I
srae
l)(n
/a)
121
Gra
des
10–1
1Ph
ysic
al
disa
bilit
yQ
uest
ionn
aire
Attit
udes
Tow
ards
Pe
ers w
ith
Disa
bilit
y
Theo
ry o
f pl
anne
d be
hav-
iour
; so
cial
le
arni
ng
theo
ry
To d
eter
min
e th
e eff
ect
of th
e C
hild
ren’s
At
titud
es T
owar
ds P
eers
w
ith D
isabi
lity
Scal
es
and
an el
ite w
heel
chai
r ba
sket
ball
gam
e on
al
terin
g ch
ildre
n’s
attit
udes
tow
ard
thei
r pe
ers w
ith d
isabi
litie
s
•3×
3demon
stratio
nfr
om e
lite
w
heel
chai
r ba
sket
ball
play
ers
vers
us th
e sc
hool
te
am w
ho
sat o
n ex
tra
w
heel
chai
rs•Athletesthen
in
trod
uced
th
emse
lves
and
to
ld th
e cr
owd
ab
out t
hem
selv
es
as w
ell a
s th
eir
te
am
•Im
provedattitud
es
for b
oth
gend
ers,
an
d on
ly g
irls
beha
viou
rally
(C
lass
IV)
•Nocontrolgroup
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 629
© 2013 Informa UK, Ltd.
Sim
ulat
ion
Loov
is an
d
Loov
is, 1
997
(US)
430
(51%
fe
mal
es)G
rade
s 2–6
Disa
bilit
y
(gen
eral
)Pr
e-po
st d
esig
n
(no
cont
rol
grou
p)
CAT
CH
N/a
To m
easu
re th
e effi
cacy
of
sim
ulat
ed
expe
rienc
es w
ith a
va
riety
of d
isabi
litie
s on
the
attit
udes
of
elem
enta
ry sc
hool
st
uden
ts
•Inphysic
al
educ
atio
n, sm
all
grou
ps o
f stu
dent
s sp
ent 5
min
each
in
: fing
er sp
ellin
g an
d sig
n la
ngua
ge
exer
cise
s, or
ient
atio
n an
d fil
ling
a kna
psac
k w
hile
usin
g ki
tche
n to
ngs,
man
oeuv
rabi
lity
thro
ugh
an o
bsta
cle
cour
se in
a w
heelc
hair,
w
ord
scra
bble
and
sent
ence
reco
gniti
on
and
writ
ing
with
a pe
ncil
and
pick
ing
up
coin
s wea
ring
glov
es
with
tiss
ue st
uffed
in
the fi
nger
s.
•Girlsa
ttitudes
tow
ards
pee
rs w
ith
disa
bilit
ies c
hang
ed
signi
fican
tly
(Cla
ss IV
)
•Nocontrolgroup
Cur
ricu
lum
God
eau
et a
l.,
2010
(Fra
nce)
784
(58%
fe
mal
e)
12–1
3 ye
ars
old
(mos
tly
high
so
cio-
econ
omic
st
atus
)
Disa
bilit
y
(gen
eral
)Ra
ndom
ized
, con
-tr
ol g
roup
CAT
CH
Que
stio
n-na
ire; H
BSC
Fa
mily
Affl
uenc
e Sc
ale;
KID
-SC
REEN
-52;
M
ultin
atio
nal
Stud
y of
Atti
tude
s To
war
d In
divi
dual
s w
ith In
telle
ctua
l D
isabi
litie
s
N/a
To a
sses
s the
eff
ectiv
enes
s of a
n
inte
rven
tion
on th
e at
titud
e of
7th
gra
de
stud
ents
tow
ard
thei
r pe
ers w
ith a
disa
bilit
y an
d id
entif
y pe
rson
al o
r en
viro
nmen
tal f
acto
rs
asso
ciat
ed w
ith at
titud
es
held
by
stud
ents
and
m
etho
d to
impr
ovin
g at
titud
es
•Teachersand
staff
atte
nded
a fi
lm o
n in
clus
ive
educ
atio
n an
d th
en p
artic
ipat
ed
in a
deb
ate
med
iate
d by
the
rese
arch
team
•Teacherswerethen
aske
d to
org
anize
se
vera
l les
sons
that
in
clude
d th
e edu
ca-
tiona
l mat
eria
l pro
-vi
ded
by th
e res
earc
h-er
s (fil
m, e
xerc
ises,
inclu
sive e
duca
tion
polic
y, ro
le pl
ays a
nd a
bibl
iogr
aphy
)
•Afte
redu
catio
nal
prog
ram
no
sig
nific
ant c
hang
e in
at
titud
es to
war
d
disa
bilit
y (C
lass
I)
•Childrenwho
re
spon
ded
in p
re a
nd
post
test
wer
e m
ore
com
mon
ly a
ssoc
iate
d w
ith sp
ecifi
c so
cio-
econ
omic
fa
ctor
s
Rahm
an e
t al.,
19
98 (P
akist
an)
100
(50%
fe
mal
e)
12–1
6 ye
ars
old
Men
tal
heal
thC
ontr
olle
d de
sign;
pr
e-te
st, p
ost t
est
ques
tionn
aire
19 q
uest
ion
qu
estio
nnai
re
writ
ten
in U
rdu;
ba
sed
on
unst
ruct
ured
in
terv
iew
s with
lo
cals
N/a
To a
sses
s a sc
hool
bas
ed
inte
rven
tion
to d
evel
op
men
tal-h
ealth
aw
aren
ess f
or sc
hool
ch
ildre
n, th
eir p
aren
ts,
frie
nds a
nd n
eigh
bour
s
•Participatory
educ
atio
nal m
etho
ds;
awar
enes
s act
iviti
es
inco
rpor
ated
to d
aily
ac
tiviti
es in
clud
ing
essa
ys, p
lays
, ann
ual
spee
ch co
ntes
ts
•Sign
ificantch
ange
for s
tude
nts
awar
enes
s of m
enta
l he
alth
issu
es
(Cla
ss II
)
•Fewergirlsthenbo
ys
atte
nd sc
hool (C
ontin
ued)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

630 S. Lindsay & A. Edwards
Disability & Rehabilitation
Cur
ricu
lum
Batta
glia
et a
l.,
1990
(US)
1380
(6
0%
fem
ale)
Gra
des 6
–12
(inte
grat
ed
clas
ses)
Men
tal
illne
ssPo
st-t
est
ques
tionn
aire
an
d co
ntro
l gr
oup
Nor
thum
berla
nd
Cou
ntry
Cou
ncil
Pupi
l Que
stio
nnai
re
N/a
To e
valu
ate
the
use
of a
m
enta
l illn
ess a
war
enes
s w
eek
prog
ram
•45minpresentation
give
n by
20
resid
ents
fr
om a
uni
vers
ity
psyc
hiat
ry p
rogr
am
•Attitud
esto
ward
ps
ychi
atris
ts w
ere
mor
e po
sitiv
e fo
r yo
uth
who
had
at
tend
ed th
e
pres
enta
tion
and
m
ore
likel
y to
seek
he
lp fr
om p
sych
iatr
ist
(Cla
ss II
I)
•Unsureifpresentatio
nch
ange
d he
lp se
ekin
g be
havi
our
•Nofollo
w-up
Hol
tz, 2
007
(US)
179
(49%
fe
mal
e)
Age
d 7–
15
year
s old
(m
ean
age
9.5
year
s); (
4 pu
blic
, 2
priv
ate
scho
ols)
–
65%
Cau
ca-
sian,
8%
A
fric
an
Am
eric
an,
5% A
sian,
9%
H
ispan
ic, 1
3%
Oth
er
ethn
icity
Tour
ette
’s
Synd
rom
ePr
e- a
nd
post
-tes
t;
rand
omiz
ed
cont
rolle
d tr
ial
Kno
wle
dge
Q
uest
ionn
aire
; C
hedo
ke-M
cMas
ter
Attit
udes
Tow
ard
Chi
ldre
n w
ith
Han
dica
ps
ques
tionn
aire
Beha
v-io
ur
chan
ge
theo
ry
(Ajz
en)
To d
eter
min
e th
e im
pact
of
an
educ
atio
nal v
ideo
on
Tou
rette
’s Sy
ndro
me
on th
e at
titud
es a
nd
know
ledg
e of
child
ren
•Video“Y
ou’ve
Gota
Frie
nd”
•Stud
entsin
the
co
ntro
l gro
up
wat
ched
a v
ideo
ca
lled
“Bra
inst
orm
: Th
e Tr
uth
Abo
ut
YourBrainon
D
rugs
” an
unre
late
d in
form
ativ
e vi
deo
•Sign
ificantch
angein
kn
owle
dge,
attit
udes
, be
havi
oura
l in
tent
ions
and
soci
al
acce
ptan
ce (C
lass
III)
•Didnotm
easurebe-
havi
our s
peci
fical
ly•Unsureifthechanges
rem
aine
d ov
ertim
e;
Mar
tinez
, 200
7 (U
S)(n
/a)
78G
rade
s 3–4
(L
atin
o; u
rban
; lo
w S
ES)
Disa
bilit
y
(var
iety
)Ra
ndom
as
signm
ent;
ex
perim
enta
l and
co
ntro
l co
nditi
ons;
pr
e-an
d
post
-tes
t
Acc
epta
nce
Scal
e:
Elem
enta
ry L
evel
; A
bout
Me
D
emog
raph
ic;
Wha
t I Th
ough
t A
bout
the
Book
Q
uest
ionn
aire
N/a
To a
ddre
ss th
e at
titud
es
of ch
ild b
efor
e an
d aft
er
they
had
par
ticip
ated
in
a di
sabi
lity
awar
enes
s pr
ogra
m
•6sessions(5
week
peri
od);
led
by a
sc
hool
psy
chol
ogis
t•boo
kdiscussing
ba
sic
fact
s abo
ut th
e di
sabi
lity
(Cla
ss I)
•Disc
ussio
ninclu
ded:
plot
/con
tent
, ex
plan
atio
n of
dis-
abili
ty, s
imila
ritie
s be
twee
n ch
ildre
n w
ith
and
with
out d
isabi
litie
s (5
boo
ks: b
lindn
ess,
autis
m, p
hysic
al
disa
bilit
y, in
telle
ctua
l di
sabi
lity
and
AD
HD
; 2
book
s gen
eral
di
sabi
lity)
•Sign
ificanceinflu
ence
on ch
ildre
n’s at
titud
es
tow
ard
peer
s with
sp
ecia
l nee
ds•Girlsw
eremore
ac
cept
ing
of p
eers
w
ith sp
ecia
l nee
ds
(Cla
ss II
I)
•6weeksm
aynothave
been
a lo
ng e
noug
h pe
riod
for
inte
rven
tion
•Diffi
culttom
easure
whe
ther
attit
ude
chan
ge tr
ansla
ted
to b
ehav
iour
al a
nd
inte
ntio
nal c
hang
e
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 631
© 2013 Informa UK, Ltd.
Cur
ricu
lum
Pitr
e et
al.,
200
7 (C
anad
a)14
4 (5
5%
fem
ale)
Gra
des 3
–6M
enta
l hea
lthPr
e-an
d po
st- t
est;
expe
rimen
tal a
nd
cont
rol g
roup
s (r
ando
miz
ed)
Mod
ified
O
pini
ons A
bout
M
enta
l Illn
ess S
cale
(O
MI)
N/a
To a
lter t
he at
titud
es o
f ch
ildre
n in
rega
rd to
m
enta
l hea
lth st
igm
ati-
zatio
n
•3×
45-m
inplays
whe
re p
uppe
ts p
or-
tray
ed p
ople
with
a
men
tal i
llnes
s (sc
hizo
-ph
reni
a, d
emen
tia
and
depr
essio
n/an
xiet
y)
•Sign
ificantlyim
proved
attit
udes
tow
ards
men
-ta
l illn
ess (
Cla
ss II
I)
•Sm
allerthanintend
ed
stud
y•Oneed
ucationalsem
i-na
r unl
ikely
to h
ave
long
lasti
ng im
pact
•Teachertraining
reco
mm
ende
d•Im
portantthatcom
-m
unity
is co
mm
itted
Trili
va e
t al.,
20
09 (G
reec
e)22
0 (4
8%
fem
ales
)Gra
des 1
–6D
isabi
lity
(g
ener
al)
Pre-
post
des
ign
w
ith a
com
paris
on
grou
p
Mod
ified
ver
sion
of
Haz
zard
’s (1
983)
sc
ales
to a
sses
s ch
ildre
n’s k
now
ledg
e ab
out p
eopl
e w
ith
disa
bilit
ies
Soci
al
mod
el o
f di
sabi
lity/
psyc
ho
educ
a-tio
nal
To a
sses
s the
eff
ectiv
enes
s of a
pr
ogra
m to
sens
itize
el
emen
tary
scho
ol
stud
ents
to is
sues
re
late
d to
disa
bilit
y
•10weeks×1h/w
eek
(act
iviti
es in
clud
ed:
lear
ning
abo
ut
disa
bilit
y, ba
rrie
rs
expe
rienc
ed, b
reak
ing
dow
n st
ereo
type
s)
•Stud
entsweresen-
sitiz
ed to
disa
bilit
y iss
ues a
nd re
port
ed
mor
e po
sitiv
e at
titud
es
tow
ard
thei
r disa
bled
pe
ers a
nd h
ighe
r lev
els
of e
xpos
ure/
cont
act
•Childrenhadmore
corr
ect i
nfor
mat
ion
abou
t disa
bled
peo
ple
and
thei
r cap
abili
ties
(Cla
ss II
I)
•Notra
ndom
ized
Bink
ard
1985
(U
S)(n
/a)
1989
Gra
des 4
–6D
isabi
lity
(var
iety
)Pr
e-po
st
ques
tionn
aire
Non
-sta
ndar
dize
d m
easu
res a
bout
vie
ws
of ch
ildre
n’s v
iew
s of
disa
bilit
y
N/a
To e
xplo
re th
e
effec
tiven
ess o
f a
disa
bilit
y aw
aren
ess
prog
ram
•60-m
inpup
pet
show
pre
sent
atio
n (~
10 m
in sc
ripts
for
each
pup
pet t
hat h
as a
di
sabi
lity)
•88%ofchildrensaid
they
lear
ned
so
met
hing
new
ab
out d
isabi
litie
s;
94%
like
d th
e pup
pet
show
; 92%
felt
bette
r ab
out c
hild
ren
with
di
sabi
litie
s (C
lass
IV)
•Nocontrolgroup
;no
sign
ifica
nce
test
s; un
stan
dard
ized
m
easu
res
Essle
r et a
l.,
2006
(UK
)(n
/a)
104
13–1
4 ye
ars
old
(inte
grat
ed
clas
ses)
Men
tal h
ealth
Non
-con
trol
led
inte
rven
tion;
qu
estio
nnai
re
quiz
(pre
and
pos
t te
st)
Min
dout
for
Men
tal H
ealth
Qui
zN
/aTo
ass
ess t
he
effec
tiven
ess o
f a
scho
ol-b
ased
in
terv
entio
n in
volv
ing
a pr
ofes
siona
l the
atre
co
mpa
ny to
incr
ease
kn
owle
dge
and
posit
ive
attit
udes
of t
eena
gers
to
war
ds m
enta
l hea
lth
•Fi
rst p
hase
: qui
z, dr
ama,
gam
es w
hich
fo
cuse
d on
men
tal
heal
th (C
lass
IV)
•Se
cond
pha
se: b
uild
se
lf es
teem
and
aw
aren
ess o
f one
’s ow
n at
titud
es, s
igns
an
d sy
mpt
oms o
f m
enta
l hea
lth
(util
ized
gam
es an
d sti
cker
s)•Trainedfacilitator,
rese
arch
er a
nd
thea
tre
com
pany
led
•Im
provedkno
wledge
and
attit
udes
tow
ards
m
enta
l hea
lth (C
lass
IV
)
•Canno
texamine
indi
vidu
al ch
ange
s be
caus
e th
e qu
izze
s re
turn
ed w
ere
an
onym
ous
•Onlyaproxymeasure
for a
ttitu
de a
nd
know
ledg
e•Nocontrolgroup
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

632 S. Lindsay & A. Edwards
Disability & Rehabilitation
Cur
ricu
lum
Kim
, 200
9
(Kor
ea)
(n/a
) 20
81G
rade
s 5–6
(in
clus
ive
cl
assr
oom
s)
Disa
bilit
y
(gen
eral
)Q
uest
ionn
aire
, in
terv
iew
sN
on-s
tand
ardi
zed
mea
sure
s ass
essin
g at
titud
es to
war
ds
child
ren
with
di
sabi
litie
s;
perc
eptio
ns o
f the
in
terv
entio
n
N/a
To a
sses
s whe
ther
a
thea
tre-
in-e
duca
tion
pres
enta
tion
wou
ld
enha
nce
the
awar
enes
s, pe
rcep
tion
and
attit
udes
to
war
d in
divi
dual
s with
di
sabi
litie
s
•40minplay,follo
wed
by a
pos
t-th
eatr
e w
orks
hop
to d
iscus
s di
sabi
lity
•71%attitud
es
impr
oved
•85%fo
undthe
pl
ay in
tere
stin
g
•Com
mon
reactio
ns
incl
uded
real
ism,
auth
entic
ity, p
ower
of
exp
erie
nce
of
disa
bilit
y (C
lass
IV)
•Lackofstand
ardized
mea
sure
•Unsurelong
term
im
plic
atio
n
Mic
ou, 2
003
(U
S)16
2 (4
8%
fem
ale)
Gra
des 2
& 5
(7
5% C
auca
sian,
10
% H
ispan
ic,
7% A
sian,
4%
A
frica
n A
mer
ican,
3%
M
iddl
e Eas
tern
, 2%
Oth
er 2
%;
mid
dle-
low
in
com
e ne
ighb
ourh
oods
)Atte
ntio
n
defic
it, h
yper
ac-
tivity
di
sord
er
(AD
HD
)
Ana
log
stud
yQ
uest
ionn
aire
(B
ased
on
Whi
te,
Rubi
n &
Gra
czyk
; lik
abili
ty sc
ale
in
the
Pupi
l Ev
alua
tion
Inve
ntor
y, tr
ait
infe
renc
es fr
om
Revi
sed
Cla
ss P
lay
and
attr
ibut
iona
l di
men
sions
)
N/a
To in
vest
igat
e ch
ildre
n’s
perc
eptio
ns o
f AD
HD
•Participantswere
read
1 o
f 3 sc
enar
ios
and
show
ed th
e ch
ild
illus
trat
ions
•Childrenwerethen
aske
d qu
estio
ns
asse
ssin
g th
e
likab
ility
of t
he
targ
et in
divi
dual
•Interventio
n
prov
ides
supp
ort o
f eff
ectiv
enes
s of a
pee
r pa
iring
pro
gram
for
alte
ring
attit
udes
of
child
ren
tow
ards
th
eir p
eers
tow
ards
ch
ildre
n w
ith A
DH
D
(Cla
ss IV
)
•Morethanju
st
asso
ciat
ion
is
need
ed to
impr
ove
a
child
’s so
cial
st
atus
Nab
ors a
nd
Lehm
kuhl
, 20
05 (U
S)
180
(50%
fe
mal
e)
16–3
1 ye
ars
old
(mea
n ag
e =
19);
(Cau
casia
n (1
53),
Afr
ican
A
mer
ican
(14)
, H
ispan
ic (3
), A
sian
(9),
did
not s
peci
fy (1
)
Cer
ebra
l pa
lsyG
ende
r blo
cked
, th
en ra
ndom
ly
assig
ned
to
vign
ette
s
Ana
logu
e de
sign;
D
emog
raph
ic
Que
stio
nnai
re;
ROC
Q S
cale
;
N/a
To e
xam
ine
fact
ors
influ
enci
ng y
oung
ad
ults’
per
cept
ions
of
child
ren
with
cere
bral
pa
lsy
•20–30m
invignette
•Lesspositivepercep-
tion
of ch
ildre
n w
ith ce
rebr
al p
alsy
co
mpa
red
to h
ealth
y ch
ildre
n•Femaleshadm
ore
posit
ive
perc
eptio
ns
of a
ll ch
ildre
n th
an
mal
es (C
lass
IV)
•Analoguedesig
nlim
its th
e “r
eal w
orld
” pr
esen
tatio
n of
the
mat
eria
l•Morerealisticto
use
pict
ures
or v
ideo
•Shortvignette
sonly
focu
sed
on p
hysic
al
limita
tions
Stua
rt, 2
006
(Can
ada)
(n/a
) 57
113
–18
year
s ol
dM
enta
l he
alth
Pre-
and
pos
t-te
st
desig
n;Su
rvey
s ada
pted
fr
om se
vera
l pr
ogra
m si
tes i
n th
e W
orld
Psy
chia
tric
A
ssoc
iatio
ns’s
glob
al
anti
stig
ma
prog
ram
N/a
To e
valu
ate
the
eff
ectiv
enes
s of u
sing
a vi
deo-
base
d pr
ogra
m to
ad
dres
s the
kno
wle
dge
and
attit
udes
of h
igh
scho
ol st
uden
ts in
re
gard
s to
sc
hizo
phre
nia
•Le
sson
#1: s
tude
nts s
hare
th
eir cu
rrent
know
ledge
ab
out s
chizo
phre
nia
befo
re w
atchi
ng a
20
min
vide
o•Le
sson
#2:
role
pl
ayin
g, th
e le
sson
m
ater
ial i
s acc
ompa
-ni
ed b
y di
scus
sion
•Stud
entswere
signi
fican
tly m
ore
know
ledg
eabl
e an
d le
ss so
cial
dist
anci
ng
tow
ards
disa
bled
pe
ers (
Cla
ss IV
)
•Unsureabou
tlon
gte
rm im
pact (C
ontin
ued)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.
Review of disability awareness interventions 633
© 2013 Informa UK, Ltd.
Cur
ricu
lum
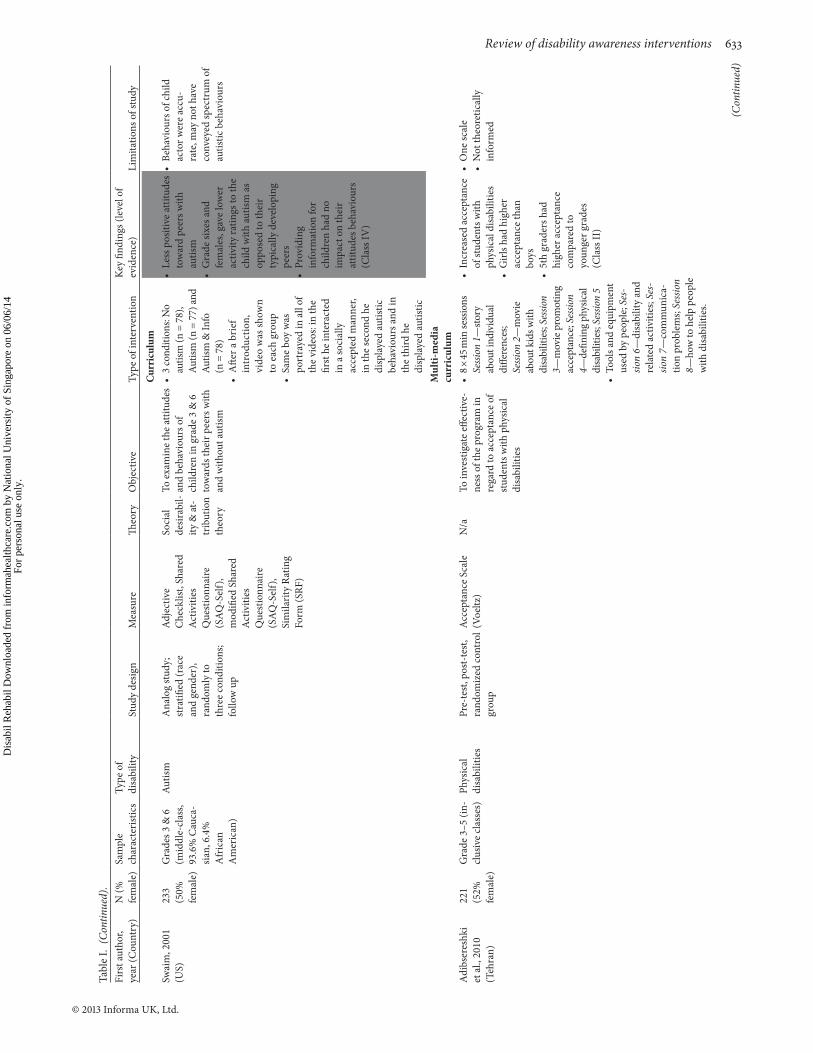
Swai
m, 2
001
(U
S)23
3 (5
0%
fem
ale)
Gra
des 3
& 6
(m
iddl
e-cl
ass,
93.6
% C
auca
-sia
n, 6
.4%
A
fric
an
Am
eric
an)
Autis
mA
nalo
g st
udy;
st
ratifi
ed (r
ace
an
d ge
nder
),
rand
omly
to
thre
e co
nditi
ons;
follo
w u
p
Adj
ectiv
e
Che
cklis
t, Sh
ared
A
ctiv
ities
Q
uest
ionn
aire
(S
AQ
-Sel
f),
mod
ified
Sha
red
Act
iviti
es
Que
stio
nnai
re
(SA
Q-S
elf)
, Si
mila
rity
Ratin
g Fo
rm (S
RF)
Soci
al
desir
abil-
ity &
at-
trib
utio
n th
eory
To e
xam
ine
the
attit
udes
an
d be
havi
ours
of
child
ren
in g
rade
3 &
6
tow
ards
thei
r pee
rs w
ith
and
with
out a
utism
•3cond
ition
s:No
au
tism
(n =
78)
, Au
tism
(n =
77)
and
Autis
m &
Info
(n
= 7
8)•Afte
rabrief
intr
oduc
tion,
vi
deo
was
show
n
to e
ach
grou
p•Samebo
ywas
port
raye
d in
all
of
the
vide
os: i
n th
e
first
he
inte
ract
ed
in a
soci
ally
ac
cept
ed m
anne
r, in
the
seco
nd h
e di
spla
yed
autis
tic
beha
viou
rs a
nd in
th
e th
ird h
e
disp
laye
d au
tistic
•Lesspositiveattitud
es
tow
ard
peer
s with
au
tism
•Gradesixesa
nd
fem
ales
, gav
e lo
wer
ac
tivity
ratin
gs to
the
child
with
autis
m a
s op
pose
d to
thei
r ty
pica
lly d
evel
opin
g pe
ers
•Providing
in
form
atio
n fo
r ch
ildre
n ha
d no
im
pact
on
thei
r at
titud
es b
ehav
iour
s (C
lass
IV)
•Be
haviou
rsofchild
acto
r wer
e ac
cu-
rate
, may
not
hav
e co
nvey
ed sp
ectr
um o
f au
tistic
beh
avio
urs
Mul
ti-m
edia
cu
rric
ulum
Adi
bser
eshk
i et
al.,
201
0
(Teh
ran)
221
(52%
fe
mal
e)
Gra
de 3
–5 (i
n-cl
usiv
e cl
asse
s)Ph
ysic
al
disa
bilit
ies
Pre-
test
, pos
t-te
st,
rand
omiz
ed co
ntro
l gr
oup
Acc
epta
nce
Scal
e (V
oeltz
)N
/aTo
inve
stig
ate
effec
tive-
ness
of t
he p
rogr
am in
re
gard
to a
ccep
tanc
e of
st
uden
ts w
ith p
hysic
al
disa
bilit
ies
•8×
45minsessions
Sessi
on 1
—sto
ry
abou
t ind
ivid
ual
diffe
renc
es;
Sessi
on 2
—m
ovie
ab
out k
ids w
ith
disa
bilit
ies;
Sessi
on
3—m
ovie
pro
mot
ing
acce
ptan
ce; S
essio
n 4—
defin
ing
phys
ical
di
sabi
litie
s; Se
ssion
5•To
olsa
ndequ
ipment
used
by
peop
le; S
es-
sion
6—di
sabi
lity
and
rela
ted
activ
ities
; Ses
-sio
n 7—
com
mun
ica-
tion
prob
lem
s; Se
ssio
n 8—
how
to h
elp
peop
le
with
disa
bilit
ies.
•Increasedacceptance
of st
uden
ts w
ith
phys
ical
disa
bilit
ies
•Girlsh
adhigher
acce
ptan
ce th
an
boys
•5thgradersh
ad
high
er a
ccep
tanc
e co
mpa
red
to
youn
ger g
rade
s (C
lass
II)
•Onesc
ale
•Notth
eoretic
ally
info
rmed
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

634 S. Lindsay & A. Edwards
Disability & Rehabilitation
Mul
ti-m
edia
cu
rric
ulum
Wat
son,
200
4 (U
S)15
66
(52%
fe
mal
e)
Gra
des 6
–8
(1.9
% A
sian
Am
eric
an, 2
.6%
A
fric
an-A
mer
-ic
an, 1
6.3%
H
ispan
ic, 1
.2%
N
ativ
e A
mer
i-ca
n,.4
Pac
ific
Isla
nder
, 69.
8%
Cau
casia
n, 7
.8%
m
ixed
eth
nici
ty)M
enta
l illn
ess
Pre-
and
post
st
udy
desig
nTh
e K
now
ledg
e
Test
(cur
ricul
um
eval
uatio
n) a
nd
r-A
Q (s
hort
-form
At
trib
utio
n
Que
stio
nnai
re)
N/a
To e
valu
ate
the
impa
ct
part
icip
atin
g in
a
curr
icul
um b
ased
in
terv
entio
n ab
out t
he
scie
nce
of m
enta
l on
at
titud
es to
war
ds
indi
vidu
als w
ith
men
tal i
llnes
s
• U
ses p
rint a
nd w
eb
base
d ac
tiviti
es to
fa
cilit
ate
lear
ning
, th
roug
h sim
ulat
ions
, an
imat
ions
and
vi
deos
•Sm
allbutsign
ificant
impr
ovem
ents
in
attit
udes
(Cla
ss II
)
•Nocontrolgroup
or
follo
w u
p to
see
if th
e ch
ange
was
m
aint
aine
d•Hardtodetermine
whe
ther
inte
rven
tion
had
an im
pact
on
thei
r act
ual b
ehav
iour
Haz
zard
and
Ba
ker,
1982
(US)
(n/a
) 32
5G
rade
s 3–6
(6
0%
Cau
casia
n,
40%
min
ority
)
Disa
bilit
y
(gen
eral
)Ra
ndom
ly
assig
ned;
pre
an
d po
st te
sts
Chi
ldre
n’s
Kno
wle
dge
Abo
ut
Han
dica
pped
Pe
rson
’s Sc
ale;
C
hild
ren’s
Soc
ial
Dist
ance
from
H
andi
capp
ed P
eers
Sc
ale;
The
Pe
rcep
tion
of a
H
andi
capp
ed
Pers
on M
easu
re
N/a
To e
valu
ate
the
impa
ct
of th
e m
ulti-
med
ia
prog
ram
in
chan
ging
/impr
ovin
g
the
attit
udes
of
child
ren
tow
ards
th
eir p
eers
with
di
sabi
litie
s; to
faci
litat
e m
ains
trea
min
g in
sc
hool
s
•6×
45-m
in
sess
ions
(m
ultim
edia
pr
ogra
m)
•Ea
chse
ssion
in
clud
ed 1
5 min
film
, di
scus
sion,
cl
assr
oom
ac
tivity
, boo
k le
ft in
th
e cl
assr
oom
to b
e re
ad in
free
tim
e•2trainersledthe
se
ssio
ns, b
ut
clas
sroo
m te
ache
rs
wer
e en
cour
aged
to
part
icip
ate
•Sign
ificantin
crease
in d
isabi
lity
kn
owle
dge
•greatera
warenesso
fap
prop
riate
beh
av-
iour
al re
spon
ses t
o di
sabl
ed p
eers
•girlsm
orepo
sitive
then
boy
s in
term
s of
soci
al d
istan
ce,
beha
viou
r and
inte
nt
to in
tera
ct (C
lass
III)
•Goo
dfirststep,sug
-ge
sted
to u
se in
con-
junc
tion
with
ano
ther
in
terv
entio
n•Onlyfemaletrainers
(sug
gest
one
mal
e, on
e fe
mal
e)
Pinf
old
et a
l.,
2003
(UK
)(n
/a)
472
Gra
des 9
–12
Men
tal h
ealth
Pre-
and
post
st
udy
desig
n (6
m
onth
pos
t tes
t)
Pret
est P
ilot
Que
stio
nnai
reN
/aTo
ass
ess t
he
effec
tiven
ess o
f an
in
terv
entio
n w
ith
youn
g pe
ople
aim
ed at
in
crea
sing
men
tal
heal
th li
tera
cy a
nd
chal
leng
ing
nega
tive
st
ereo
type
s ass
ocia
ted
with
seve
re m
enta
l ill
ness
•Worksho
psdelivered
by a
trai
ned
faci
lita-
tor;
Sess
ion
1:
1-h
men
tal h
ealth
(v
ideo
); Se
ssio
n 2:
pr
omot
ing
w
ell-b
eing
and
chal
-le
ngin
g us
e of
de
roga
tory
term
s an
d la
bels;
em
phas
is pl
aced
on
rem
ovin
g di
stan
ce b
etw
een
us
and
them
; gro
up
exer
cise
s and
in
form
atio
n le
aflet
s
•Greatestchanges
occu
rred
for f
emal
es
attr
ibut
ed to
cont
act
with
peo
ple
who
hav
e m
enta
l illn
ess
•Mentalh
ealth
ed
ucat
iona
l ses
-sio
ns a
re a
succ
essf
ul
man
ner t
o ch
alle
nge
ster
eoty
pica
l atti
tude
s to
war
d pe
ople
with
m
enta
l hea
lth is
sues
(C
lass
III)
•Nocontrolgroup
for
pre
and
post
stud
y•So
cialdesira
bilitybias
in at
titud
e as
sess
-m
ents
•Writtenview
sand
ex
pres
sed
attit
udes
m
ay n
ot re
flect
any
be
havi
oura
l cha
nge
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 635
© 2013 Informa UK, Ltd.
Mul
ti-m
edia
cu
rric
ulum
Tava
res,
2011
(C
anad
a)(n
/a)
5112
–13
year
s ol
dPh
ysic
al
disa
bilit
yQ
uasi-
expe
rimen
tal
grou
p; p
re- a
nd
post
- tes
t; fo
llow
up
1 m
onth
afte
r po
st-t
est
Che
doke
-McM
aste
r At
titud
es T
owar
d C
hild
ren
with
H
andi
caps
Sca
le
(CAT
CH
); So
cial
In
tera
ctio
n
Que
stio
nnai
res
N/a
To e
valu
ate
the
influ
ence
of
a p
rese
ntat
ion
on th
e at
titud
es o
f chi
ldre
n to
war
ds th
eir p
eers
with
ph
ysic
al d
isabi
litie
s
•45minpresentation
•Kno
wledgeis
co
rrec
ted
or a
dded
to
•Disc
usssim
ilarities
betw
een
the
able
bo
died
and
disa
bled
; vi
deo
“Kid
s Jus
t W
ant t
o H
ave
Fun”
•Presentersask
spec
ific q
uest
ions
ab
out t
he ch
ild’s
disa
bilit
y an
d th
e ch
ildre
n an
swer
th
e qu
estio
ns•Ro
leplaying
•Morepo
sitive
at
titud
es a
nd g
reat
er
unde
rsta
ndin
g of
di
sabi
lity
•Shorttermpositive
impa
ct o
n at
titud
es
and
pote
ntia
l on
the
soci
al in
clus
ion
of th
e no
n-in
clud
ed ch
ild
(Cla
ss II
I)
•Re
sultsnotcon
sistent
acro
ss a
ll sc
hool
s•To
osm
allofsam
ple
size
to g
ener
aliz
e•Interventio
nmayhave
nega
tivel
y im
pact
ed
targ
et ch
ild (f
elt o
ver-
whe
lmed
or i
sola
ted)
•Identifi
catio
nofch
ild
with
di
sabi
lity
– ta
ken
ou
t of t
he cl
assr
oom
•Un
sureab
outlo
ngterm
im
pact
Mul
tiple
com
pone
nts
Clu
nie-
Ross
and
O
’Mea
ra, 1
989
(Aus
tral
ia)
(n/a
) 60
Gra
de 4
(in
tegr
ated
an
d
non-
inte
grat
ed
scho
ols)
Inte
llect
ual
disa
bilit
ies
and
disa
bilit
y in
ge
nera
l
Pre-
test
, pos
t tes
t (e
xper
imen
tal
grou
p (3
0) a
nd
cont
rol g
roup
(3
0)
Peer
Atti
tude
s To
war
d th
e H
andi
capp
ed S
cale
(P
ATH
S): 3
su
b-sc
ales
(p
hysic
al,
lear
ning
, be
havi
oura
l)
and
a to
tal s
core
N/a
To e
valu
ate
the
effec
tive-
ness
of a
pro
gram
to
chan
ge th
e at
titud
es o
f pr
imar
y sc
hool
stud
ents
to
war
ds ch
ildre
n w
ith
disa
bilit
ies i
n bo
th in
clu-
sive
and
non-
incl
usiv
e cl
assr
oom
s
Mul
ti-m
edia
cu
rric
ulum
, sim
ulat
ion
and
soci
al co
ntac
t•4×
90minse
ssions
(ove
r 2 w
eeks
)•Se
ssion
1: m
ovie,
str
uctu
red
abou
t ba
rrie
rs•Se
ssio
n 2:
exp
erie
nces
in
whe
el ch
air
•Sign
ificantlym
ore
posit
ive
attit
ude
tow
ard
peer
s with
di
sabi
litie
s by
ch
ildre
n in
the
ex
perim
enta
l gro
up
•Eff
ectiv
einattitud
eto
war
d di
sabl
ed
•Se
ssio
n 3:
stor
y an
d vi
deo
abou
t di
ffer
ence
s an
d si
mila
ritie
s•Se
ssio
n 4:
soci
al
cont
act –
10
stud
ents
w
ith in
telle
ctua
l di
sabi
litie
s wen
t ro
ller s
katin
g w
ith
the
grad
e 4
clas
ses
•Th
roug
houtall
ph
ases
the
in
tegr
ated
had
mor
e po
sitiv
e at
titud
es
(Cla
ss II
)
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

636 S. Lindsay & A. Edwards
Disability & Rehabilitation
Mul
tiple
com
pone
nts
Flor
ian
and
Ke
hat,
1987
(I
srae
l)
(n/a
) 11
4G
rade
s 10–
11
(het
erog
eneo
us
cultu
ral a
nd
soci
oeco
nom
ic
back
grou
nds;
urba
n ce
ntre
)
Phys
ical
di
sabi
lity
Rand
om
assig
nmen
t; 3
ex
perim
enta
l gr
oups
, 1 co
ntro
l gr
oup
Jord
an a
nd
Ces
sna’s
qu
estio
nnai
re
(sho
rten
ed
vers
ion)
N/a
To e
xam
ine
the
impa
cts
of d
iffer
ently
stru
ctur
ed
educ
atio
nal p
rogr
ams
on h
igh
scho
ol st
uden
ts’
attit
udes
tow
ard
in
divi
dual
s with
ph
ysic
al d
isabi
litie
s;
addr
essin
g ho
w to
ch
ange
spec
ific
com
pone
nts o
f at
titud
es
Curr
icul
um, s
imul
atio
n an
d so
cial
cont
act
•G
roup
1: (
n =
28),
one m
eetin
g pe
r wee
k (le
ctur
e and
disc
us-
sion,
role
sim
ulat
ion;
fie
ld tr
ip)
•G
roup
2: (
n =
26),
(lect
ure,
disc
ussio
n,
role
sim
ulat
ion
in th
e co
mm
unity
)•G
roup
3: (
n =
31),
(lect
ure,
disc
ussio
n,
role
sim
ulat
ion
with
in
the c
lass
room
, soc
ial
cont
act)
•G
roup
4: (
n =
29)
cont
rol g
roup
•Group
2sign
ificant
chan
ge in
attit
udes
•Group
3:change
oc
curr
ed b
ut n
ot st
a-tis
tical
ly si
gnifi
cant
•Meetin
gwith
in
divi
dual
s with
di
sabi
litie
s did
not
im
pact
attit
ude
•Im
portanttorely
on v
ario
us m
etho
ds
and
met
hodo
logi
cal
com
bina
tions
•Differencebetween6
and
9 w
eek
prog
ram
ha
d no
effe
ct
(Cla
ss II
)
•Psycho
metric
m
easu
re w
as n
ot
sens
itive
eno
ugh
to
eval
uate
val
id
impa
cts o
f the
pr
ogra
m’s
impl
emen
tatio
n•Technicald
ifficul-
ties w
ith o
ne g
roup
le
avin
g th
e sc
hool
to
com
plet
e th
eir t
asks
Rein
a et
al.
2011
(S
pain
)34
4 (4
7%
fem
ale)
10–1
5 ye
ars
old
(mea
n ag
e 13
.3)
Visu
al
impa
irmen
tQ
uasi
ex
perim
enta
l de
sign
Attit
udes
Tow
ard
Disa
bilit
y
Que
stio
nnai
re
(ATD
Q)
N/a
To e
xplo
re th
e eff
ect o
f tw
o aw
aren
ess p
rogr
ams
(6-d
ay v
ersu
s 1-d
ay
prog
ram
s) o
n ch
ildre
n’s
attit
udes
tow
ard
peer
s w
ith a
visu
al im
pairm
entM
ulti-
med
ia c
urric
ulum
an
d sim
ulat
ion
•6-dayprogram
incl
uded
: lec
ture
an
d vi
deo
on v
isual
im
pairm
ents
, a g
ame,
simul
ated
act
iviti
es,
trai
ning
and
com
peti-
tive
socc
er u
sing
blin
d fo
lded
gog
gles
and
a
spor
t sho
w•1-dayprogram
incl
uded
onl
y th
e le
ctur
e an
d vi
deo
•Sign
ificanteffectsin
the
cogn
itive
, em
otio
nal a
nd
beha
viou
ral s
cale
s•Sign
ificantlym
ore
fem
ales
show
ed
favo
urab
le re
sults
th
an m
ales
•Th
e6-daydyadic
inte
rven
tion
was
m
ore
effec
tive
than
th
e 1-
day
awar
enes
s un
it (C
lass
II)
•Th
isstud
ydidno
tta
ke in
to a
ccou
nt th
e im
pact
of p
revi
ous
cont
act o
n kn
owle
dge
of p
eopl
e w
ith a
dis-
abili
ty
Rose
nbau
m e
t al.,
19
86 (C
anad
a)66
(45%
fe
mal
e)G
rade
s 4–7
(9
–13
year
s ol
d)
Disa
bilit
y
(gen
eral
)Q
uasi
ex
perim
enta
l (p
re-t
est,
post
test
w
ith a
cont
rol
grou
p)
Ched
oke-
McM
aste
r At
titud
es to
war
d
Child
ren
with
H
andi
caps
(CAT
CH):
Perc
eived
Co
mpe
tenc
e Sca
le,
Pare
ntal
Attit
udes
to
war
d Ch
ildre
n w
ith
Han
dica
ps (P
ATCH
), Kn
owled
ge o
f D
isabl
ed P
eopl
e
N/a
To e
xplo
re th
e
effec
tiven
ess o
f tw
o
inte
rven
tions
for
impr
ovin
g at
titud
es
tow
ard
disa
bilit
y an
d m
ore
spec
ifica
lly
child
ren
with
di
sabi
litie
s - lo
ok at
eff
ectiv
enes
s of
prog
ram
s ind
ivid
ually
an
d co
llabo
rativ
ely
Curr
icul
um a
nd so
cial
co
ntac
t•Bu
ddyprogram:3
mon
ths
•KidsO
ntheBlock:
10weeks×45m
in,
4 pu
ppet
show
s and
di
scus
sions
•Com
binedKidsO
nth
e Bl
ock
& B
uddy
Pr
ogra
m: b
oth
pro-
gram
s con
curr
ently
•KO
Bandbu
ddy
gr
oup
attit
udes
wer
e sig
nific
antly
low
er
than
the
budd
y on
ly
grou
p•KO
B-Bu
ddyg
roupwas
poor
er th
en th
e con
trol
and
KOB
alone
•Bu
ddyon
lygroup
kn
ew m
ore
child
ren
with
disa
bilit
ies
(Cla
ss II
I)
•Natureofbud
dy
prog
ram
diff
ered
f ro
m sc
hool
to sc
hool
•Needtodefine
rela
tions
hip
betw
een
attit
ude
and
be
havi
oura
l (Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 637
© 2013 Informa UK, Ltd.
Mul
tiple
com
pone
nts
Rillo
tta a
nd
Net
telb
eck,
20
07 (A
ustr
alia
)
259
(55%
fe
mal
e)
Gra
de 9
–12
(priv
ate
scho
ol)
Inte
llect
ual
disa
bilit
yQ
uasi
expe
rimen
tal;
age
mat
ched
co
ntro
l gro
ups
Attit
udes
Tow
ard
Pers
ons w
ith a
n
Inte
llect
ual
Disa
bilit
y
Que
stio
nnai
re;
Theo
ry
of m
ere
expo
sure
eff
ect;
theo
ry o
f pe
r-su
asiv
e co
mm
u-ni
catio
n
To u
nder
stan
d th
e
impa
ct o
f lon
g-la
stin
g po
sitiv
e at
titud
es
rega
rdin
g ed
ucat
iona
l an
d so
cial
incl
usio
n fo
r pe
ople
with
an
in
telle
ctua
l disa
bilit
y, th
roug
h a
soci
al a
nd
educ
atio
nal i
nteg
rate
d se
tting
alo
ng w
ith a
pr
ogra
m th
at p
rovi
ded
trai
ning
in d
isabi
lity
awar
enes
s
Mul
ti-m
edia
cur
ricul
um
and
soci
al co
ntac
t•Grade6
Stu
dent
s: 3×
45minsessionsof
disa
bilit
y aw
aren
ess
prog
ram
s (in
clude
d:
getti
ng to
kno
w
stude
nts w
ith an
inte
l-le
ctua
l disa
bilit
y, to
ur-
ing
thei
r cla
ssro
om,
play
ing
spor
ts/co
okin
g to
geth
er, g
uest
spea
ker
disc
ussin
g in
clusio
n)•G
rade
8 st
uden
ts:
8×45
minaw
areness
of d
isabi
lity
prog
ram
ra
n by
teac
hers
(pre
-se
ntat
ions
, disc
ussio
n,
vide
o, g
uest
spea
kers
, ke
y ele
men
t was
non
-di
sabl
ed an
d di
sabl
ed
stude
nt in
tera
ctin
g by
pl
anni
ng an
d un
der
taki
ng an
activ
ity)
•G
rade
8 st
uden
ts:
com
plet
ed a
10 se
ssio
n pr
ogra
m (s
imila
r to
othe
r gro
up b
ut 2
ad-
ditio
nal s
essio
ns w
ith
mor
e dire
ct co
ntac
t an
d tw
o vi
deos
)
•Stud
entswho
com
-pl
eted
an
8-se
ssio
n aw
aren
ess p
rogr
am
repo
rted
mor
e po
si-tiv
e at
titud
es to
war
d pe
ople
with
disa
bilit
ies
than
thos
e w
ho at
-te
nded
onl
y 3
sess
ions
•Similarp
ositivityin
at
titud
es in
child
ren
who
had
just
com
-pl
eted
the
sess
ions
and
th
ose
who
had
8 y
ears
pr
evio
usly
•Mostp
romising
for
fem
ales
(Cla
ss II
I)
•Scho
olsd
ifferedin
pr
esen
tatio
n,
com
mitm
ent a
nd
unde
rsta
ndin
g
Schu
lze
et a
l.,
2003
(Ger
man
y)(n
/a)
150
14–1
8 ye
ars
old
Schi
zoph
reni
aPr
e-te
st, p
ost t
est
with
a co
ntro
l gr
oup
Que
stio
nnai
re
(des
igne
d fo
r thi
s st
udy:
ster
eoty
pic
view
s of
schi
zoph
reni
a an
d so
cial
dist
ance
N/a
To re
duce
stig
ma
and
disc
rimin
atio
n to
war
ds
indi
vidu
als w
ith
schi
zoph
reni
a w
ithin
a
scho
ol e
nviro
nmen
t
Mul
ti-m
edia
curr
icul
um
and
soci
al co
ntac
t•Usedartworkand
gam
es to
pro
mot
e em
otio
nal w
ellbe
ing
and
men
tal h
ealth
•Followe
dbydiscussio
nwa
ys to
cope
with
ill
ness
or w
hen
they
fee
l “do
wn”
; a yo
ung
pers
on w
ith
schi
zoph
reni
a disc
usse
d th
eir ow
n sto
ries
•Re
sultedinsig-
nific
ant r
educ
tion
of
ster
eoty
pes (
impr
oved
at
titud
es) (
Cla
ss II
I)
•Attitud
esarenot
the
only
fact
or to
be
havi
our (C
ontin
ued)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(C
ount
ry)
N (%
fe
mal
e)Sa
mpl
e
char
acte
ristic
sTy
pe o
f disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.
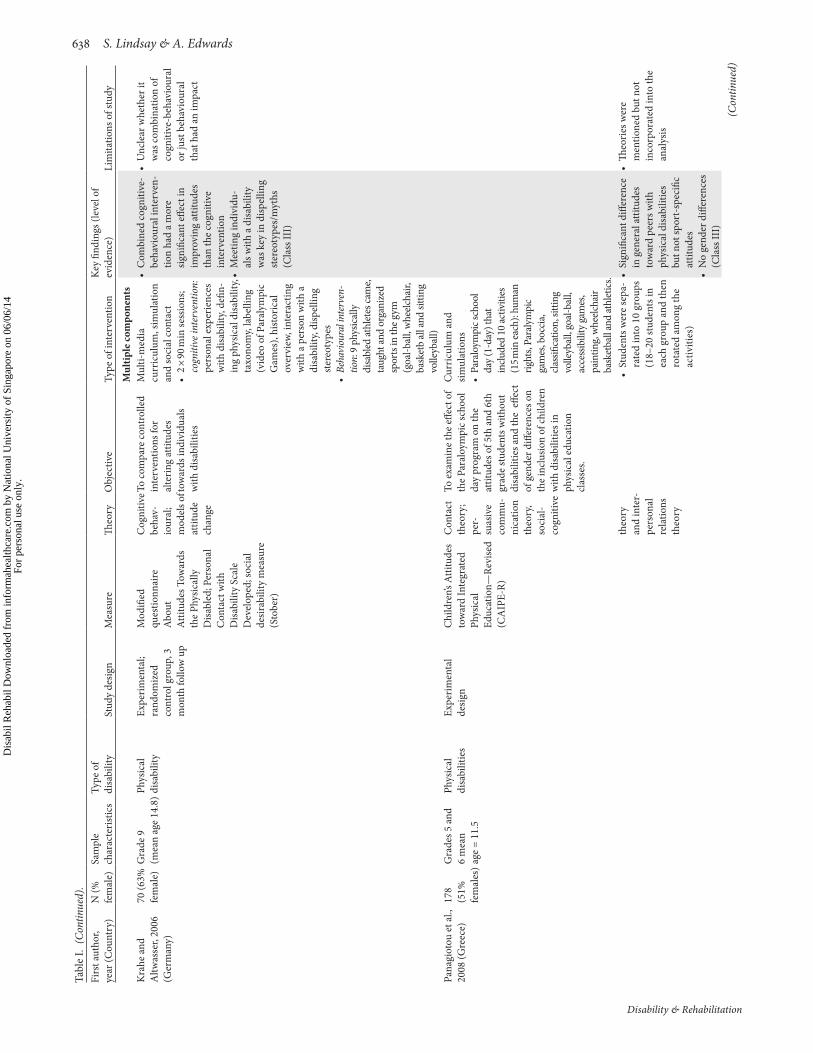
638 S. Lindsay & A. Edwards
Disability & Rehabilitation
Mul
tiple
com
pone
nts
Kra
he a
nd
Altw
asse
r, 20
06
(Ger
man
y)
70 (6
3%
fem
ale)
Gra
de 9
(m
ean
age
14.8
)Phys
ical
di
sabi
lity
Expe
rimen
tal;
rand
omiz
ed
cont
rol g
roup
, 3
mon
th fo
llow
up
Mod
ified
qu
estio
nnai
re
Abo
ut
Attit
udes
Tow
ards
th
e Ph
ysic
ally
D
isabl
ed; P
erso
nal
Con
tact
with
D
isabi
lity
Scal
e D
evel
oped
; soc
ial
desir
abili
ty m
easu
re
(Sto
ber)
Cog
nitiv
e be
hav-
iour
al;
mod
els o
f at
titud
e ch
ange
To co
mpa
re co
ntro
lled
inte
rven
tions
for
alte
ring
attit
udes
to
war
ds in
divi
dual
s w
ith d
isabi
litie
s
Mul
ti-m
edia
cu
rric
ulum
, sim
ulat
ion
and
soci
al co
ntac
t•2×
90minse
ssions;
cogn
itive
inte
rven
tion:
pe
rson
al e
xper
ienc
es
with
disa
bilit
y, de
fin-
ing
phys
ical
disa
bilit
y, ta
xono
my,
labe
lling
(v
ideo
of P
aral
ympi
c G
ames
), hi
stor
ical
ov
ervi
ew, i
nter
actin
g w
ith a
per
son
with
a
disa
bilit
y, di
spel
ling
ster
eoty
pes
•Be
havi
oura
l int
erve
n-tio
n: 9
phy
sical
ly
disa
bled
athl
etes
cam
e, ta
ught
and
orga
nize
d sp
orts
in th
e gym
(g
oal-b
all,
whe
elcha
ir,
bask
etb
all a
nd si
tting
vo
lleyb
all)
•Com
binedcogn
itive-
beha
viou
ral i
nter
ven-
tion
had
a m
ore
signi
fican
t effe
ct in
im
prov
ing
attit
udes
th
an th
e co
gniti
ve
inte
rven
tion
•Meetin
gindividu
-al
s with
a d
isabi
lity
was
key
in d
ispel
ling
ster
eoty
pes/
myt
hs
(Cla
ss II
I)
•Unclearwhetherit
was
com
bina
tion
of
cogn
itive
-beh
avio
ural
or
just
beh
avio
ural
th
at h
ad a
n im
pact
Pana
giot
ou e
t al.,
20
08 (G
reec
e)17
8 (5
1%
fem
ales
)Gra
des 5
and
6
mea
n
age
= 11
.5
Phys
ical
di
sabi
litie
sEx
perim
enta
l de
sign
Chi
ldre
n’s A
ttitu
des
tow
ard
Inte
grat
ed
Phys
ical
Ed
ucat
ion—
Revi
sed
(CA
IPE-
R)
Con
tact
th
eory
; pe
r-su
asiv
e co
mm
u-ni
catio
n th
eory
, so
cial
-co
gniti
ve
To e
xam
ine
the
effec
t of
the
Para
loym
pic s
choo
l da
y pr
ogra
m o
n th
e
attit
udes
of 5
th a
nd 6
th
grad
e st
uden
ts w
ithou
t di
sabi
litie
s and
the
effe
ct
of g
ende
r diff
eren
ces o
n th
e in
clus
ion
of ch
ildre
n
with
disa
bilit
ies i
n
phys
ical
edu
catio
n cl
asse
s.
Cur
ricu
lum
and
sim
ulat
ions
•Paraloym
picschool
day (
1-da
y) th
at
inclu
ded
10 ac
tiviti
es
(15 m
in ea
ch):
hum
an
right
s, Pa
raly
mpi
c ga
mes
, boc
cia,
cla
ssifi
catio
n, si
tting
vo
lleyb
all, g
oal-b
all,
acce
ssib
ility
gam
es,
pain
ting,
whe
elcha
ir ba
sket
ball
and
athl
etics
.th
eory
an
d in
ter-
pers
onal
re
latio
ns
theo
ry
•Studentsw
eresepa
-ra
ted
into
10
grou
ps
(18–
20 st
uden
ts in
ea
ch g
roup
and
then
ro
tate
d am
ong
the
activ
ities
)
•Sign
ificantdifference
in g
ener
al at
titud
es
tow
ard
peer
s with
ph
ysic
al d
isabi
litie
s bu
t not
spor
t-sp
ecifi
c at
titud
es•Nogend
erdifferences
(Cla
ss II
I)
•Th
eorie
swere
men
tione
d bu
t not
in
corp
orat
ed in
to th
e an
alys
is
(Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 639
© 2013 Informa UK, Ltd.
Xaf
opou
lous
et
al.,
200
9
(Cze
ch R
epub
lic)
71 (4
0%
fem
ale)
Aver
age
age
= 11
.3Ph
ysic
al
disa
bilit
yPr
e-po
st d
esig
nC
hild
ren’s
Atti
tude
To
war
d In
tegr
ated
Ph
ysic
al
Educ
atio
n-Re
vise
d (C
AIP
E-R)
Theo
ry
of
plan
ned
beha
vi-
our
To in
vest
igat
e th
e eff
ect
of P
arao
lym
pic d
ay
on ch
ildre
n’s at
titud
es
tow
ards
pee
rs w
ith a
di
sabi
lity
in g
ener
al
phys
ical
edu
catio
n cl
ass
Mul
tiple
com
pone
nts
Soci
al co
ntac
t and
sim
ulat
ions
•6grou
ps(1
2stud
ents
each
) rot
ated
into
6
activ
ities
(40 m
in
each
): (1
) Par
alym
pic
spor
ts (v
ideo
and
di
scus
sion)
, (2
) sle
dge
hock
ey
(ada
pted
equ
ip-
men
t and
pra
ctic
al
exer
cise
),
(3) w
heel
chai
r m
obili
ty
(exp
erie
nced
bei
ng
diffe
rent
and
mov
ing
in a
diff
eren
t way
) (4
) whe
elch
air b
as-
ketb
all,
(5
) mee
t an
athl
ete
with
a d
isabi
lity,
(6
) boc
cia
(the
pro
-gr
am e
mph
asiz
ed
resp
ect a
nd a
ccep
-ta
nce
of in
divi
dual
di
ffere
nces
, ath
letic
ac
hiev
emen
ts a
nd
right
s of d
isabl
ed
peop
le to
take
par
t in
spor
ts
•Th
eon
e-day
inte
rven
tion
po
sitiv
ely
influ
ence
d th
e ge
nera
l atti
tude
s of
girl
s but
not
thei
r sp
ort s
peci
fic
attit
udes
(Cla
ss IV
)
•Nocontrolgroup
Fava
zza
and
Odo
m, 1
997
(U
S)
46 (5
0%
fem
ale)
5–6
year
s old
(8
5% C
auca
sian,
15
% A
fric
an
Am
eric
an;
low
SES
) –
inte
grat
ed
clas
ses
Disa
bilit
y
(gen
eral
)Ra
ndom
ized
co
ntro
l gro
up
(pre
test
and
pos
t te
st)
Acc
epta
nce
Scal
e fo
r Kin
derg
arte
ners
(A
SK),
Inve
ntor
y of
D
isabi
lity
Re
pres
enta
tion
(ID
R), O
pini
ons
Rela
tive
to M
ain-
stre
amin
g (O
RM)
N/a
To e
xam
ine
the
effec
ts
of le
vel o
f con
tact
, bo
oks a
nd d
iscus
sions
on
the
attit
udes
of
kind
erga
rten
-age
ch
ildre
n to
war
d pe
ople
w
ith d
isabi
litie
s
Curr
icul
um a
nd so
cial
co
ntac
t•9weekprogramdivid
-ed
into
3 g
roup
s (no
, lo
w an
d hi
g co
ntac
t)•Eq
uipm
entavailable
for c
hild
ren
to e
xplo
re•3storiesreadeach
wee
k in
the
high
co
ntac
t•15minofstructured
play
with
child
ren
with
disabilities3
×/week
•So
cialco
ntactand
us
e of
child
ren’s
bo
oks a
re e
ffect
ive
mea
ns to
alte
r the
at
titud
es o
f chi
ldre
n (C
lass
IV)
•Differencesincontact
grou
ps co
uld
be
rela
ted
to sc
hool
se
tting
s•Infoabo
utch
ild’s
unde
rsta
ndin
g or
pe
rcep
tion
of a
per
son
with
a d
isabi
lity
was
no
t ass
esse
d•Cou
ldhavebeen
stre
ngth
ened
by
usin
g be
havi
oura
l ob
serv
atio
n (Con
tinue
d)
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

640 S. Lindsay & A. Edwards
Disability & Rehabilitation
Mul
tiple
com
pone
nts
Curr
icul
um a
nd so
cial
co
ntac
tFa
vazz
a et
al.,
20
00 (U
S)(n
/a)
575–
6 ye
ars o
ld
(2%
Cau
casia
n;
98%
Afr
ican
A
mer
ican
; lo
w S
ES)
Disa
bilit
y
(gen
eral
)Ra
ndom
ized
co
ntro
l gro
up
(pre
test
and
pos
t te
st)
Teac
her I
mpr
essio
n Sc
ale;
Acc
epta
nce
Scal
e fo
r K
inde
rgar
tene
rs
(ASK
);
Inve
ntor
y of
D
isabi
lity
Re
pres
enta
tion
(I
DR)
N/a
To e
xam
ine
the
eff
ectiv
enes
s of a
n
inte
rven
tion
to
prom
ote
acce
ptan
ce o
f yo
ung
child
ren
with
di
sabi
litie
s
•W
hole
Inte
rven
tion:
st
ory
time,
disc
us-
sions
in cl
assr
oom
, st
ruct
ured
pla
y w
ith
child
ren
with
di
sabi
litie
s, st
ory
time
and
disc
ussio
ns at
ho
me
•St
ory
Gro
up:
part
icip
ated
in st
ory
tim
e pa
rt o
f in
terv
entio
n at
hom
e an
d sc
hool
•Pl
ay G
roup
: pa
rtic
ipat
ed o
nly
in th
e str
uctu
red
play
aspe
ct
of th
e int
erve
ntio
n;
story
tim
e and
disc
us-
sions
cent
red
arou
nd
disa
bilit
y
•Childrenexpo
sedto
indi
vidu
al
com
pone
nts o
f the
in
terv
entio
n ha
d sh
ort-
term
gai
ns in
ac
cept
ance
of
indi
vidu
als w
ith
disa
bilit
y w
hile
ch
ildre
n ex
pose
d to
th
e w
hole
inte
rven
-tio
n ha
d sh
ort a
nd
long
-ter
m g
ains
in
acce
ptan
ce•sig
nificantgainsin
le
vels
of ac
cept
ance
fo
und
only
in th
e “hi
gh
leve
l of c
onta
ct” g
roup
s (le
ss ex
posu
re to
peo
ple
with
disa
bilit
ies w
as
linke
d w
ith lo
wer
ac
cept
ance
(Cla
ss IV
)
•Childreninth
eco
ntro
l gro
up w
ere
at
a di
ffere
nt sc
hool
than
th
e ot
her 3
gro
ups
•Lo
wre
liabilityofASK
(d
ue to
self-
repo
rts)
•Classwasra
ndom
ly
assig
ned,
not
the
indi
vidu
al st
uden
ts
Ison
et a
l., 2
010
(Aus
tral
ia)
147
(32%
fe
mal
e)
9–11
yea
rs o
ld
(priv
ate
scho
ols;
2 A
nglic
an, 1
C
atho
lic
scho
ol; 1
Boy
s sc
hool
, 2
Co-
ed)
Disa
bilit
y (g
ener
al)
Pre-
post
test
an
d fo
cus g
roup
Base
line
qu
estio
nnai
re fo
r th
is st
udy
(Lik
ert
Scal
e, Tr
ue/F
alse
, O
pen
Ende
d
rela
ting
to
pres
enta
tion)
Cog
nitiv
e be
hav-
iour
al
To e
valu
ate
the
eff
ectiv
enes
s of a
shor
t di
sabi
lity
awar
enes
s pa
ckag
e fo
r stu
dent
s in
5th
grad
e, to
add
ress
ga
ps in
kno
wle
dge,
ac
cept
ance
and
at
titud
es to
war
d
peop
le w
ith d
isabi
litie
s
Curr
icul
um, s
imul
atio
n an
d so
cial
cont
act
•2×
90minse
ssionsheld
1–2
wee
ks ap
art
•Atleastonepresenter
had
cere
bral
pal
sy
•in
form
atio
n/co
gniti
ve
activ
ities
: (di
scus
sion,
la
ngua
ge u
se, B
raill
e &
ASL
(fing
er sp
ellin
g) an
d co
mpr
ehen
sion
activ
ity
abou
t Par
aoly
mpi
cs)
•Pa
rtici
patio
n ac
tiviti
es
(sim
ulat
ion
of d
aily
ac-
tiviti
es w
ith a
disa
bilit
y, qu
estio
n an
d an
swer
se
ssio
n w
ith so
meo
ne
who
had
a di
sabi
lity
and
dem
onstr
atio
n of
com
-m
on eq
uipm
ent)
•Im
provem
entsin
kn
owle
dge
and
ac
cept
ance
and
at
titud
es to
war
ds
indi
vidu
als w
ith
disa
bilit
ies
•Fo
cusg
roup
in
dica
ted
that
usin
g in
tera
ctiv
e ac
tiviti
es
alon
g w
ith h
avin
g a
pres
ente
r with
a
disa
bilit
y w
ere
key
to
the
posit
ive
ou
tcom
es (C
lass
IV)
•Notara
ndom
ized
cont
rolle
d tr
ial
(sch
ools
requ
este
d to
pa
rtic
ipat
e)•Unabletom
atchdata
•Onlyinclud
edin
de-
pend
ent a
nd C
atho
lic
scho
ols
Uns
hade
d: C
lass
I an
d II
; Lig
ht sh
aded
: Cla
ss II
I; D
ark
shad
ed: C
lass
IV.
Tabl
e I.
(Con
tinue
d).
Firs
t aut
hor,
year
(Cou
ntry
)N
(%
fem
ale)
Sam
ple
ch
arac
teris
tics
Type
of
disa
bilit
ySt
udy
desig
nM
easu
reTh
eory
Obj
ectiv
eTy
pe o
f int
erve
ntio
nKe
y fin
ding
s (le
vel o
f ev
iden
ce)
Lim
itatio
ns o
f stu
dy
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.
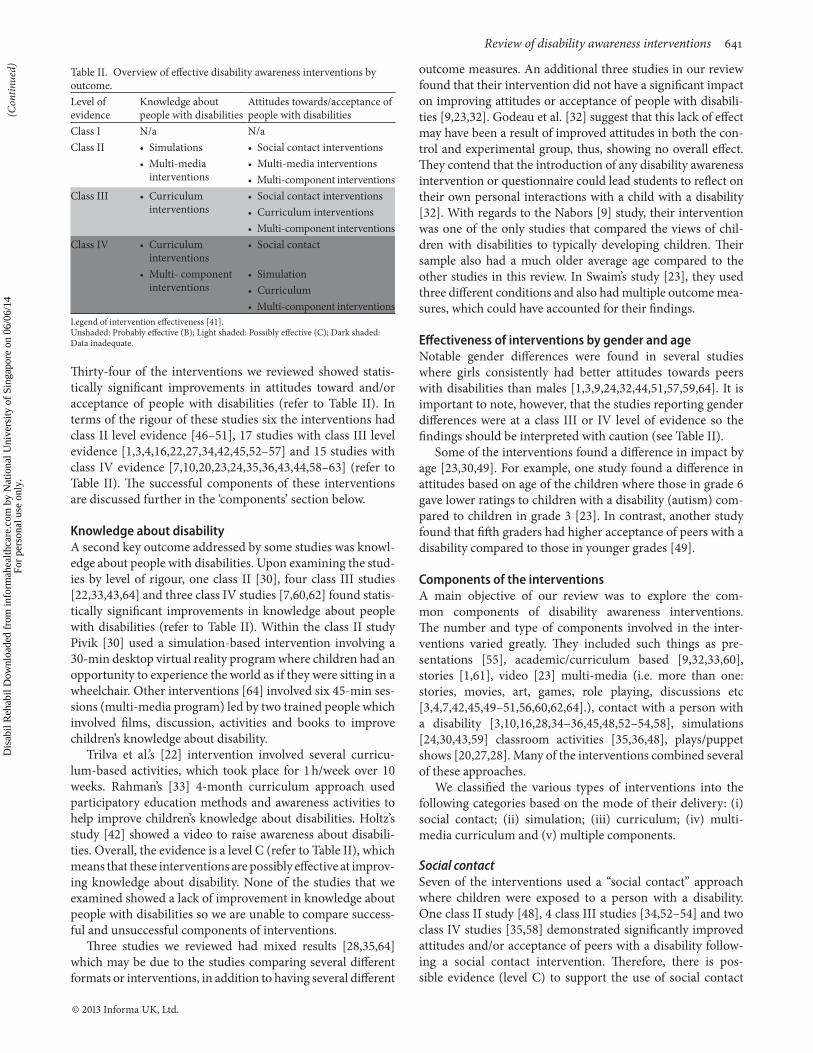
Review of disability awareness interventions 641
© 2013 Informa UK, Ltd.
Thirty-four of the interventions we reviewed showed statis-tically significant improvements in attitudes toward and/or acceptance of people with disabilities (refer to Table II). In terms of the rigour of these studies six the interventions had class II level evidence [46–51], 17 studies with class III level evidence [1,3,4,16,22,27,34,42,45,52–57] and 15 studies with class IV evidence [7,10,20,23,24,35,36,43,44,58–63] (refer to Table II). The successful components of these interventions are discussed further in the ‘components’ section below.
Knowledge about disabilityA second key outcome addressed by some studies was knowl-edge about people with disabilities. Upon examining the stud-ies by level of rigour, one class II [30], four class III studies [22,33,43,64] and three class IV studies [7,60,62] found statis-tically significant improvements in knowledge about people with disabilities (refer to Table II). Within the class II study Pivik [30] used a simulation-based intervention involving a 30-min desktop virtual reality program where children had an opportunity to experience the world as if they were sitting in a wheelchair. Other interventions [64] involved six 45-min ses-sions (multi-media program) led by two trained people which involved films, discussion, activities and books to improve children’s knowledge about disability.
Trilva et al.’s [22] intervention involved several curricu-lum-based activities, which took place for 1 h/week over 10 weeks. Rahman’s [33] 4-month curriculum approach used participatory education methods and awareness activities to help improve children’s knowledge about disabilities. Holtz’s study [42] showed a video to raise awareness about disabili-ties. Overall, the evidence is a level C (refer to Table II), which means that these interventions are possibly effective at improv-ing knowledge about disability. None of the studies that we examined showed a lack of improvement in knowledge about people with disabilities so we are unable to compare success-ful and unsuccessful components of interventions.
Three studies we reviewed had mixed results [28,35,64] which may be due to the studies comparing several different formats or interventions, in addition to having several different
outcome measures. An additional three studies in our review found that their intervention did not have a significant impact on improving attitudes or acceptance of people with disabili-ties [9,23,32]. Godeau et al. [32] suggest that this lack of effect may have been a result of improved attitudes in both the con-trol and experimental group, thus, showing no overall effect. They contend that the introduction of any disability awareness intervention or questionnaire could lead students to reflect on their own personal interactions with a child with a disability [32]. With regards to the Nabors [9] study, their intervention was one of the only studies that compared the views of chil-dren with disabilities to typically developing children. Their sample also had a much older average age compared to the other studies in this review. In Swaim’s study [23], they used three different conditions and also had multiple outcome mea-sures, which could have accounted for their findings.
Effectiveness of interventions by gender and ageNotable gender differences were found in several studies where girls consistently had better attitudes towards peers with disabilities than males [1,3,9,24,32,44,51,57,59,64]. It is important to note, however, that the studies reporting gender differences were at a class III or IV level of evidence so the findings should be interpreted with caution (see Table II).
Some of the interventions found a difference in impact by age [23,30,49]. For example, one study found a difference in attitudes based on age of the children where those in grade 6 gave lower ratings to children with a disability (autism) com-pared to children in grade 3 [23]. In contrast, another study found that fifth graders had higher acceptance of peers with a disability compared to those in younger grades [49].
Components of the interventionsA main objective of our review was to explore the com-mon components of disability awareness interventions. The number and type of components involved in the inter-ventions varied greatly. They included such things as pre-sentations [55], academic/curriculum based [9,32,33,60], stories [1,61], video [23] multi-media (i.e. more than one: stories, movies, art, games, role playing, discussions etc [3,4,7,42,45,49–51,56,60,62,64].), contact with a person with a disability [3,10,16,28,34–36,45,48,52–54,58], simulations [24,30,43,59] classroom activities [35,36,48], plays/puppet shows [20,27,28]. Many of the interventions combined several of these approaches.
We classified the various types of interventions into the following categories based on the mode of their delivery: (i) social contact; (ii) simulation; (iii) curriculum; (iv) multi-media curriculum and (v) multiple components.
Social contactSeven of the interventions used a “social contact” approach where children were exposed to a person with a disability. One class II study [48], 4 class III studies [34,52–54] and two class IV studies [35,58] demonstrated significantly improved attitudes and/or acceptance of peers with a disability follow-ing a social contact intervention. Therefore, there is pos-sible evidence (level C) to support the use of social contact
Table II. Overview of effective disability awareness interventions by outcome.Level of evidence
Knowledge about people with disabilities
Attitudes towards/acceptance of people with disabilities
Class I N/a N/aClass II • Simulations • Social contact interventions
• Multi-media interventions
• Multi-media interventions• Multi-component interventions
Class III • Curriculum interventions
• Social contact interventions• Curriculum interventions• Multi-component interventions
Class IV • Curriculum interventions
• Social contact
• Multi- component interventions
• Simulation• Curriculum• Multi-component interventions
Legend of intervention effectiveness [41].Unshaded: Probably effective (B); Light shaded: Possibly effective (C); Dark shaded: Data inadequate.
(Con
tinue
d)D
isab
il R
ehab
il D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
atio
nal U
nive
rsity
of
Sing
apor
e on
06/
06/1
4Fo
r pe
rson
al u
se o
nly.

642 S. Lindsay & A. Edwards
Disability & Rehabilitation
interventions to improve children’s attitudes towards peers with a disability (see Table II). Social contact interventions were often based on social contact theory, which suggests that interaction between groups may change attitudes toward out-groups and may reduce stereotyping and prejudice. Interventions in this category varied in length from 6 weeks to 1 year. Three of the studies used a “Circle of Friends” approach [35,54,58] to enhance social inclusion in a mainstream set-ting. This works by mobilizing peers to provide support to a child with a disability. Others, such as Armstrong [48], used a “buddy system” where children with disabilities were paired up with a typically developing peer of the same gender and met regularly at school to engage in social activities. Newberry and Parish [52] had a similar principle behind their interven-tion; however, they focused on social interaction outside of the classroom. Further, Piercy’s [53] study brought children with disabilities and typically developing children together through co-operative learning groups, which were more aca-demic based than the other interventions. We were unable to compare the successful and unsuccessful components of social contact disability awareness interventions because all of these studies showed positive outcomes.
Simulation-based interventionsFour of the interventions included in our analysis used simu-lations to raise awareness about disabilities among children [24,30,43,59]. One class II study [30] and three class IV stud-ies [24,43,59] showed improvements in children’s knowledge about disability (refer to Table II). For example, Pivik’s [30] simulation-based study engaged students in a 30-min virtual reality program to gain a better understanding of what it is like to move around in a wheelchair and the obstacles that are experienced. There is possible evidence (level C) to sup-port the use of simulation interventions to improve children’s knowledge about people with disabilities. Three class IV studies [24,43,59] showed improvements in attitudes towards children with disabilities; however, the data are inadequate to make a recommendation on the effectiveness of this type of intervention.
Curriculum-based interventionsFourteen of the interventions included in our search were curriculum-based and focused on a wide range of disabilities including disability in general (6), mental illness (5), Tourette Syndrome, autism, cerebral palsy, and attention deficit hyperactivity disorder. There was a great range in the type of curriculum-based intervention including presentations [45], games [41], classroom exercises [4,32,33], videos [23,42,62], plays and puppet shows [20,27,63] and stories [1,9,61].
In regards to using curriculum-based interventions to improve knowledge about disabilities, one class II study [33], two class III studies [22,42] and three class IV studies [60,62,63] reported a significant change in knowledge about disability. This evidence is at a level C indicating that these interventions are possibly effective at improving knowledge about disabilities. Among the studies with a higher level of evidence, Rahman [33] used participatory educational
methods and awareness activities in the classroom to improve knowledge about mental health. Holtz’s [42] intervention involved a video about children with a disability. Meanwhile, Trilvia’s [22] intervention involved classroom-based activities that occurred 1 h/week over 10 weeks.
The findings from curriculum-based interventions regard-ing improving attitudes towards children with disabilities are mixed. For example, one class I study [32] found no significant change in attitudes towards disability following their intervention (refer to Table II). As we mentioned earlier this may have been due to both the intervention and control group having improved attitudes. Meanwhile, four class III [1,22,27,42,55] and three IV studies [20,61,62] also showed significant improvements in attitudes using curriculum-based interventions. These interventions included one-off presenta-tions or class activities [20,42,55,61] to multiple sessions over a longer period of time [1,22,27]. As a result of the interven-tions showing conflicting results we are unable to make a recommendation of best practices using a curriculum-based intervention to influence attitudes towards children with disabilities.
Multi-media based curriculum interventionsFive of the interventions used multi-media curriculum based interventions to improve attitudes towards children with disabilities. This included two class II studies [49,50] and three class III studies [4,57,64]. The interventions ranged in length from one 45-min session (i.e. simulations and class activities) to eight 45-min sessions involving presentations, movies and class activities. The type of disability that inter-ventions focused on also varied from disability in general for the younger grades to more specific conditions (i.e. mental health, visual impairments) for high school students. This evidence (level C) from these multi-media interventions indi-cates that these interventions are possibly effective at improv-ing attitudes towards children with disabilities.
Only one multi-media based curriculum intervention [64] examined improvements in knowledge about disability, thus, the evidence is insufficient to make a recommendation about best practices.
Multi-component interventionsTwelve of the interventions included in our analysis used multiple components (i.e. several of the approaches men-tioned above). Two class II studies [46,47], five class III studies [3,16,45,51,56] and four class IV studies [7,10,36,44] dem-onstrated an improved attitude towards peers following the intervention. Thus, these interventions (level C evidence) are possibly effective at improving attitudes towards children with disability. For example, three interventions used a combined approach involving curriculum activities and social contact with a person with a disability [10,28,36]. Two other studies similarly used multi-media curriculum activities combined with social contact [3,56]. Four interventions included a vari-ety of curriculum activities, simulation exercises and social contact with a person with a disability [7,45–47]. Ison et al.’s [7] participants reported that using interactive activities along
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 643
© 2013 Informa UK, Ltd.
with social contact (i.e. having a presenter with a disability) was the key to the success of their intervention. Children reported that social contact/exposure to someone with a dis-ability is critical to improving behaviours [7,52,57]. Meanwhile Panagantiou [16] and Xafpoulous [44] used curriculum activi-ties and simulation exercises to influence children’s attitudes through a range of Paralympics activities. The programs varied in length from a one-day session of Paralympic activities [16] to four 90-min sessions over 2 weeks [46] to a 6-day program involving multi-media curriculum activities and simulation exercises [51].
One of the advantages of a multiple components interven-tion was that several authors compared the effectiveness of different components within their intervention. For example, Krahe [45] found that social contact was essential to improv-ing attitudes towards people with disabilities. They also reported that a combined cognitive-behavioural intervention had a statistically significant effect in improving attitudes towards people with disabilities than cognitive intervention. Meanwhile, Favazza [10] found that those exposed to the whole intervention as opposed to individual components had both short and long-term gains in terms of social acceptance of peers with disabilities. They found that statistically signifi-cant gains in acceptance were made in the group that had a high level of contact with peers with a disability. In contrast, Florian and Kehat [47] found that social contact did not influ-ence attitudes.
Rosenbaum’s [28] study had mixed findings where they compared different interventions for improving attitudes. One involved a buddy program lasting 3 months, one involved a series of 4 (45 min puppet shows) over 10 weeks and the final intervention combined the puppet show and the buddy pro-gram concurrently. They found that the children in the inter-vention that combined the puppet show and buddy program did not have improved attitudes compared to the children in the buddy-only group. They suggest that this may have been a result of the dissonance between what children experienced and what they were led to expect in the educational puppet program [28].
In sum, there were five key types of interventions based on their mode of delivery (i.e. social contact; simulation; cur-riculum; multi-media curriculum, and multiple components) which influenced knowledge of disability, attitudes and accep-tance of peers with disabilities.
Length of the interventionsThe length of the disability awareness interventions varied greatly from a one-off 20-min session to a 1-year program with bi-weekly activities lasting 30–90 min each session. With a few exceptions, most studies that had positive outcomes involved more than one session and had multiple components such as books, videos, discussions, simulations, practical exer-cises, and/or interaction with people with disabilities. Some researchers also recommended that several approaches and methods be used for disability awareness interventions [47].
Only two studies examined the impact of different lengths/types of programs on the attitudes toward children with
disabilities. Reina et al. [51] found that their 6-day interven-tion was more effective than the 1-day awareness unit. In Rillota and Nettlebeck’s [3] study, students who completed an 8-session awareness program reported more positive atti-tudes toward children with a disability compared to those who attended the 3-session awareness program. Meanwhile, Florian [47] found no difference between a 6-week and 9-week program in altering attitudes in a multi-component interven-tion. Pitre [27] argued that a one-off session is unlikely to have a long-lasting impact on attitudes and behaviour. This suggests that there may be a threshold when the program can maintain its impact. The first two studies compared shorter duration (6-day versus 1-day; and 8 weeks versus 3 weeks) while the study that found no difference in outcomes was 6 versus 9 weeks (considerably longer than the comparisons in the first two studies). The discrepancy in findings by length of programs could also have been due to the heterogeneous culturally and socio-economically diverse sample.
Discussion
This review provides evidence for how to achieve optimal outcomes for improving attitudes towards and acceptance of people with a disability. Uncovering the effective components of disability awareness interventions is especially important as schools, educators and health professionals increasingly invest in the development of disability awareness interven-tions to further enhance social inclusion [38]. Although some interventions in this review have more recently implemented inclusive education policies compared to others, the authors of these interventions consistently argue that there are diffi-culties with achieving social inclusion of children with dis-abilities and that this cannot be achieved through inclusive polices alone [20].
Our review shows that several different types of disability awareness interventions can be used to positively influence knowledge about people with disability. Common elements of successful interventions included breaking down stereotypes and creating awareness of the barriers that with people with disabilities encounter. Such interventions were done in a vari-ety of different formats including simulations, multi-media and curriculum-based interventions which varied greatly in length and target audience.
Our findings also highlight that several successful strate-gies can be used to influence attitudes towards children with disabilities. Common components of successful interven-tions included social contact with a person with a disability over a period of time, multi-media and multi-component approaches involving stories, class activities and discus-sions. The social contact approach was used more often with younger children over longer periods of time from 6 weeks to 1-year programs to allow time to develop understanding of disability and possible friendships. A few of the other types of interventions were one-off sessions while many others ran over a longer period of time.
Improving knowledge about disability is important because children’s attitudes are often strongly influenced by their degree
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

644 S. Lindsay & A. Edwards
Disability & Rehabilitation
of knowledge [7,65]. A lack of understanding can perpetuate stigma and social exclusion [2,60]. Indeed, unfavourable peer attitudes are a major barrier to the full social inclusion of chil-dren with disabilities in integrated schools [32].
Many of the disability awareness interventions we reviewed reported a consistent gender and age-based pattern influencing attitudes whereby females often had more posi-tive attitudes towards peers with disabilities than males. Past evidence also shows that girls often have more favourable attitudes towards children with a disability compared to boys [1] and that some interventions may appeal differently to boys and girls [38]. Similarly, an age based pattern emerged where children from older grades were more accepting than younger children. This is consistent with similar research on bullying interventions suggesting that younger children may benefit less than older children [8]. Our review also highlighted that interventions used most often with younger children focused on disability in general while some successful interventions with older students were more disability specific.
Our recommendations for the further development of disability awareness programs include having multiple com-ponents, interactive activities, social contact with people who have a disability, several sessions over a longer period of time rather than a brief one-off session and having standardized measures and a rigorous methodological design. Interventions should also be context specific taking educational policies and societal customs into account.
What is lacking in the disability awareness interventions we reviewed is that they tended to target one class at a time. It would be worthwhile to explore a whole-school based inter-vention, which has been shown to be effective in the bully-ing literature [8]. An intervention that is only based on one level (e.g. classroom) may not have a lasting impact. Failing to address the systemic issues and the social environment related to social exclusion can undermine the success of the interven-tion [8]. Thus, a multi-level and multi-component approach is needed involving school boards, community, teachers, par-ents and children to improve attitudes towards people with disabilities.
An important element for future programs to consider is the influence of the socio-contextual environment of how children with disabilities are perceived and treated [2]. This is particularly critical when choosing an intervention that it is not only age appropriate but also that it is culturally sensitive as well in recognizing different views of disability. Consistent evidence shows that attitudes towards people with disability vary by cultural context [66]. The studies examined in our review were from a wide range of countries where views of disability may vary considerably.
Conclusion
Our review focused on disability awareness interventions for school aged children. This study addressed several gaps in the literature by synthesizing the common components of effec-tive disability awareness interventions. Developing a better understanding of the effective components is critical to help
improve the social inclusion of children with disabilities [38]. A focus on children is important because their attitudes are still evolving and early interventions can be especially ben-eficial. Successful interventions can provide children with opportunities to develop positive attitudes about differences in respectful contexts [38].
Overall, the studies reviewed suggest that there is possible evidence that disability awareness interventions are effective at influencing knowledge about and attitudes toward people with disabilities. Commonalities of successful interventions included having multiple components over a period of time and often included social contact with a person who has a disability.
Several limitations to this review need to be considered. First, some studies had heterogeneous samples and relatively small sample sizes. Second, the use of variable outcome mea-sures may limit the ability to accurately measure the effects of the interventions. Finally, the studies were conducted over a broad range spanning over 30 years and across different cultures. Thus, attitudes towards people with disabilities may differ across time and context [66].
There are several directions for future research. First, more rigorous designs are needed (e.g. RCTs) to evaluate the effectiveness of interventions on attitudes towards children with disabilities and over longer periods of time to assess any changes. Second, more research is needed to explore compari-sons of different lengths, formats and types of schools (e.g. public, private), setting (e.g. class versus whole-school based) and geographic locations. Specifically, comparisons of effec-tive components within interventions should be evaluated individually to examine what works best for whom and in what context. Third, further work should explore who ben-efits most from the interventions by paying close attention to the socio-demographic characteristics of the sample (i.e. gen-der, social class, ethno-cultural status, geographic location). Fourth, more exploration is needed around simulation and curriculum-based interventions which showed mixed results in our review. Further, despite the wide variety of approaches used to enhance disability awareness, we did not find any studies meeting our inclusion criteria that used a computer game. Further research could explore this as a mechanism of influencing attitudes towards people with disabilities. Finally, very little is known about the impact of these interventions on children with disabilities (e.g. their perceptions of how peers are treating them) and how interventions make them feel. It would also be worthwhile to seek their involvement in the future development of disability awareness interventions.
Implications for Rehabilitation
This review can help rehabilitation professionals, educators and policy makers to better understand what types of inter-ventions work best for school age children to enable more youth with disabilities to feel socially included at school. First, rehabilitation health care providers should help children with disabilities to be knowledgeable about their condition and how and when it is best to disclose to their peers. This can help
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

Review of disability awareness interventions 645
© 2013 Informa UK, Ltd.
to facilitate knowledge about their specific needs at school. Clinicians and educators should be aware of the challenges that children with disabilities face such as social exclusion at school and be prepared to provide children with resources and interventions on how to cope. Second, clinicians, educa-tors and children with disabilities should both contribute to the development of age appropriate disability awareness interventions. Very few of the interventions were developed or implemented by clinicians knowledgeable about pediatric dis-ability. Involving such professionals at the outset of developing a program may enhance disability awareness interventions. Researchers, clinicians and educators need to work together to further develop and test interventions that can facilitate dis-ability awareness among school-age children to reduce some of the negative consequences children such as social exclusion. Third, educators should choose an appropriate intervention to meet the needs of the children in their classroom (i.e. age, disability type, cultural background) while also considering the broader societal influences on attitudes towards disability. Finally, at a community level, disability advocacy should target schools, teachers and increased government funding for dis-ability awareness programs for school-age children.
Declaration of Interest: The authors report no conflicts of interest. This study was funded by Bloorview Research Institute Institutional start-up grant and a Ward Family summer student program.
References 1. Martinez R, Carspecken P. Effectiveness of a brief intervention on
Latino children’s social acceptance of peers with special needs. J Appl Sch Psycho 2006;23:97–115.
2. Lindsay S, McPherson AC. Experiences of social exclusion and bullying at school among children and youth with cerebral palsy. Disabil Rehabil 2012;34:101–109.
3. Rillotta F, Nettelbeck T. Effects of an awareness program on attitudes of students without an intellectual disability towards persons with an intel-lectual disability. J Intellect Dev Disabil 2007;32:19–27.
4. Tavares W. An evaluation of the Kids are Kids disability awareness pro-gram: increasing social inclusion among children with physical disabili-ties. J Soc Work Disabil Rehabil 2011;10:25–35.
5. McDougall J, King G, de Wit DJ, Miller LT, Hong S, Offord DR, LaPorta J, Meyer K. Chronic physical health conditions and disability among Canadian school-aged children: a national profile. Disabil Rehabil 2004;26:35–45.
6. Statistics Canada. Participation and activity limitation survey. Ottawa: Statistics Canada; 2008.
7. Ison N, McIntyre S, Rothery S, Smithers-Sheedy H, Goldsmith S, Parsonage S, Foy L. ‘Just like you’: a disability awareness programme for children that enhanced knowledge, attitudes and acceptance: pilot study findings. Dev Neurorehabil 2010;13:360–368.
8. Vreeman RC, Carroll AE. A systematic review of school-based interven-tions to prevent bullying. Arch Pediatr Adolesc Med 2007;161:78–88.
9. Nabors LA, Keyes LA. Brief report: preschoolers’ social preferences for interacting with peers with physical differences. J Pediatr Psychol 1997;22:113–122.
10. Favazza P, Phillipsen L, Kumar P. Measuring and promoting accep-tance of young children with disabilities. Exceptional Children 2000;4:491–508.
11. Nowicki E, Sandieson R. A meta-analysis of children’s attitudes toward individuals with intellectual and physical disabilities. Int J Disabil Dev Educ 2002;49:243–266.
12. Roberts C, Smith P. Attitudes and behaviour of children toward peers with disabilities. Int J Disabil Dev Educ 1999;46:35–50.
13. Nowicki EA. A cross-sectional multivariate analysis of children’s atti-tudes towards disabilities. J Intellect Disabil Res 2006;50:335–348.
14. Hunt C, Hunt B. Changing attitudes toward people with disabili-ties: experimenting with an educational intervention. J Manag Issues 2004;16:266–280.
15. United Nations. Convention on the rights of the child, in UN Document, A/Res/44/23. 1989.
16. Panagitou A, Evaggelinou C, Doulkeridou A, Mouratidou K, Koidou E. Attitudes of 5th and 6th grade Greek students toward the inclusion of children with disabilities in physical education classes after a Paralympic education program. Eur J Adap Phys Activ 2008;1:31–43.
17. Gini G, Pozzoli T. Association between bullying and psychosomatic problems: a meta-analysis. Pediatrics 2009;123:1059–1065.
18. Pittet I, Berchtold A, Akré C, Michaud PA, Surís JC. Are adolescents with chronic conditions particularly at risk for bullying? Arch Dis Child 2010;95:711–716.
19. Cutts S, Sigafoos J. Social competence and peer interactions of students with intellectual disability in an inclusive high school. J Intellect Dev Disabil 2001;26:127–141.
20. Kim B. A journey of change with a blue whale: a theatre-in-education programme on disability and dilemmas in the inclusive classroom in Korea. Res Drama Educ 2009;14:115–131.
21. ColumnaL,LiebermanL,ArndtK,YangS.Usingonlinevideosfordis-ability awareness. J Phys Educ Recreat Dance 2009;80:1–60
22. Triliva S, Anagnostopoulou T, Hatzinikolaou S, Chimienti G, Mastorakou A. The development and evaluation of a program to sensi-tize Greek grammar school students to issues relating to disability. Eur J Counsel Psychol 2009;1:3–17.
23. Swaim K. Children’s attitudes and behavioral intentions toward a peer presented as having autism: does a brief educational intervention have an effect? Dissertation Abstracts International: Section B: The Sciences and Engineering 1999;59(9-B).
24. HutzlerY,Fliess-DouerO,AvrahamA,ReiterS,TalmorR.Effectsofshort-term awareness interventions on children’s attitudes toward peers with a disability. Int J Rehabil Res 2007;30:159–161.
25. Siperstein GN, Bak JJ, O’Keefe P. Relationship between children’s atti-tudes toward and their social acceptance of mentally retarded peers. Am J Ment Retard 1988;93:24–27.
26. Gash H, Coffey D. Influences on attitudes towards children with mental handicap. Eur J Spec Needs Educ 1995;10:1–16.
27. Pitre N, Stewart S, Adams S, Bedard T, Landry S. The use of puppets with elementary school children in reducing stigmatizing attitudes towards mental illness. J Ment Health 2007;16:415–429.
28. Rosenbaum PL, Armstrong RW, King SM. Improving attitudes toward the disabled: a randomized controlled trial of direct contact versus Kids-on-the-Block. J Dev Behav Pediatr 1986;7:302–307.
29. Pivik J, McComas J, Macfarlane I, Laflamme M. Using virtual reality to teach disability awareness. J Educ Comput Res 2002;26:203–218.
30. Flower A, Burns M, Bottsford-Miller N. Meta-analysis of disability sim-ulation research. Remed Spec Educ 2007;28:72–79.
31. Godeau E, Vignes C, Sentenac M, Ehlinger V, Navarro F, Grandjean H, Arnaud C. Improving attitudes towards children with disabilities in a school context: a cluster randomized intervention study. Dev Med Child Neurol 2010;52:e236–e242.
32. Rahman A, Mubbashar MH, Gater R, Goldberg D. Randomised trial of impact of school mental-health programme in rural Rawalpindi, Pakistan. Lancet 1998;352:1022–1025.
33. Marmon M, Cohen D, Naon D. Changing disability-related attitudes and self-efficacy of Israeli children via the partners to inclusion pro-gram. Int J Disabil Dev Educ 2007;54:113–127.
34. Barrett W, Randall L. Investigating the circle of friends approach: adapta-tions and implications for practice. Educ Psychol Pract 2004;4:353–368.
35. Favazza P, Odom S. Promoting positive attitudes of kindergarten-age children toward people with disabilities. Excep Child 1997;63:405–418.
36. Cummings J, Pepler D, Mishna F, Craig W. Bullying and victim-ization among students with exceptionalities. Excep Educ Canada 2006;16:193–222.
37. Lindsay S, McPherson A, Aslam H, McKeever P, Wright V. Exploring children’s perceptions of two school-based social inclusion programs: a pilotstudy.Child&YouthCareForum(InPress).
38. Grbich C. Qualitative data analysis. London: Sage; 2007. 39. Whittemore R, Knafl K. The integrative review: updated methodology. J
Adv Nurs 2005;52:546–553.40. EdlundW,GronsethG,SoY,FranklinG.Clinicalpracticeguidelines
process manual. St. Paul: American Academy of Neurology; 2004.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.

646 S. Lindsay & A. Edwards
Disability & Rehabilitation
41. Holtz K, Tessman G. Evaluation of a peer- focused intervention to increase knowledge and foster positive attitudes toward children with tourette syndrome. J Dev Phys Disabil 2007;19:531–542.
42. HutzlerY,Fliess-DouerO,AvrahamA,ReiterS,TalmorR.Effectsofshort-term awareness interventions on children’s attitudes toward peers with a disability. Int J Rehabil Res 2007;30:159–160.
43. Xafopoulos G, Kudlacek M, Evaggelinou C. Effect of the intervention program “paralympic school day” on attitudes of children attending international school towards inclusion of students with disabilities. Act Univ Palacki Olomuc Gymn 2009;39:63–71.
44. Krahe B, Altwasser C. Changing negative attitudes towards persons with physical disabilities: an experimental intervention. J Community Appl Soc Psychol 2006;16:59–69.
45. Cline-Ross G, O’Meara K. Changing the attitudes of students towards peers with disabilities. Aust Psychol 1989;24:273–284.
46. Florian V, Kehat D. Changing high school students’ attitudes toward dis-abled people. Health Soc Work 1987;12:57–63.
47. Armstrong RW, Rosenbaum PL, King SM. A randomized controlled trial of a ‘buddy’ programme to improve children’s attitudes toward the disabled. Dev Med Child Neurol 1987;29:327–336.
48. Adibereshki N, Tajrishi M, Mirzamani M. The effectiveness of a prepa-ratory students programme on promoting peer acceptance of students with physical disabilities in inclusive schools of Tehran. Educ Stud 2010;36:447–459.
49. Watson AC, Otey E, Westbrook AL, Gardner AL, Lamb TA, Corrigan PW, Fenton WS. Changing middle schoolers’ attitudes about mental ill-ness through education. Schizophr Bull 2004;30:563–572.
50. Reina R, López V, JiménezM, García-Calvo T, Hutzler Y. Effects ofawareness interventions on children’s attitudes toward peers with a visual impairment. Int J Rehabil Res 2011;34:243–248.
51. Newberry MK, Parish TS. Enhancement of attitudes toward handicapped children through social interactions. J Soc Psychol 1987;127:59–62.
52. Piercy M, Wilton K, Townsend M. Promoting the social accep-tance of young children with moderate-severe intellectual dis-abilities using cooperative-learning techniques. Am J Ment Retard 2002;107:352–360.
53. Frederickson N, Turner J. Utilizing the classroom peer group to address children’s social needs: an evaluation of the circle of friends intervention approach. J Spec Educ 2003;36:234–245.
54. Battaglia J, Coverdale JH, Bushong CP. Evaluation of a Mental Illness Awareness Week program in public schools. Am J Psychiatry 1990;147:324–329.
55. Schulze B, Richter-Werling M, Matschinger H, Angermeyer MC. Crazy? So what! Effects of a school project on students’ attitudes towards people with schizophrenia. Acta Psychiatr Scand 2003;107:142–150.
56. Pinfold V, Toulmin H, Thornicroft G, Huxley P, Farmer P, Graham T. Reducing psychiatric stigma and discrimination: evaluation of educational interventions in UK secondary schools. Br J Psychiatry 2003;182:342–346.
57. Whitaker P, Barratt P, Joy H, Potter M, Thomas G. Children with autism and peer group support: using ‘circles of friends’. Br J Specl Educ 1998;25:60–64.
58. Loovis EM, Loovis CL. A disability awareness unit in physical educa-tion and attitudes of elementary school students. Percept Mot Skills 1997;84:768–770.
59. Essler V, Arthur A, Stickley T. Using a school-based intervention to chal-lenge stigmatizing attitudes and promote mental health in teenagers. J Ment Health 2006;15:243–250.
60. Micou L. Social evaluations of children with ADHD participating in peer pairing interventions: disconfirming behavior versus peer associa-tion. Unpublished PhD Thesis, Illinois, 2003.
61. Stuart H. Reaching out to high school youth: the effectiveness of a video-based antistigma program. Can J Psychiatry 2006;51:647–653.
62. Binkard B. A successful handicap awareness program. Coun Excep Child 1985;12–16.
63. Hazzard A, Baker B. Enhancing children’s attitudes toward disabled peers using a multi-media intervention. J Appl Dev Psychol 1982;3:247–262.
64. Vignes C, Coley N, Grandjean H, Godeau E, Arnaud C. Measuring chil-dren’s attitudes towards peers with disabilities: a review of instruments. Dev Med Child Neurol 2008;50:182–189.
65. Ali Z, Fazil Q, Bywaters P, Wallace L, Singh G. Disability, ethnicity and childhood: a critical review of research. Disabil Soc 2001;16:949–968.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Nat
iona
l Uni
vers
ity o
f Si
ngap
ore
on 0
6/06
/14
For
pers
onal
use
onl
y.