re-evaluation of the condylar path as the reference for ... · original article hobo et al -...
TRANSCRIPT

Original Article Hobo et al - Re-evaluation of the Condylar Path 1
Re-evaluation of the Condylar Path as the Reference for Occlusion Sumiya Hobo, Hisao Takayama
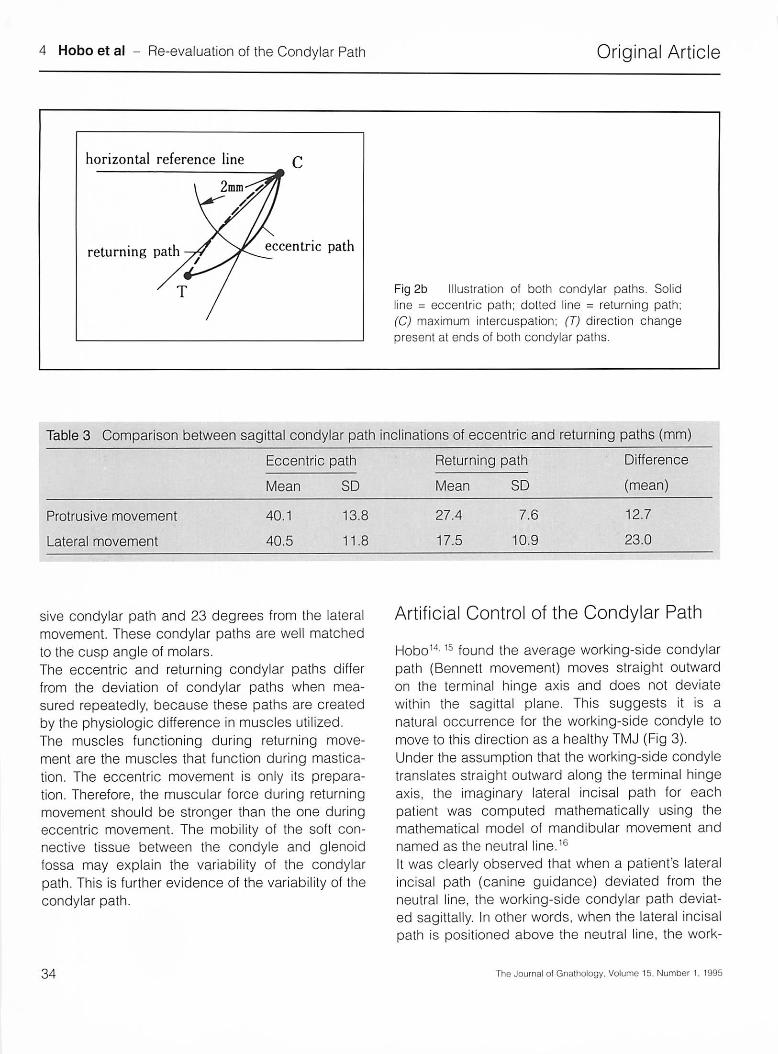
The condylar path is "the path traveled by the mandibular condyle in the temporomandibular joint during various mandibular movements." 1 It is an accepted belief that good occlusion can be created in a restoration when the condylar path is re-produced precisely on an articulator. For this purpose gnathologists have used the pantograph and the fully adjustable articulator. There are, how-ever, contrary opinions on such use of the condylar path. Craddock 2 reports that there is no correlation be-tween the sagittal condylar paths, as measured by check bite, and the configuration of the condylar tubercle obtained by radiographs. Based on the literature review, Christensen and Slabbert 3 assert that the posterior bony surface of the articular tubercle is never parallel with the more or less curvilinear or zigzag paths scribed as the sagittal condylar movements; further, they state that the sagittal condylar guidance angle is not a single and well-defined angle; rather a number of highly variable angles might exist. Experienced clinicians often find the movement of the articulator is not coincident with the facets on the cast when an articulator is adjusted using condylar path measurements. Donegan and Chris-tensen4 report there are differences between the measured value of the condylar path obtained by the check bite method (31 degrees) and by adjusting the articulator to match occlusal facets on the cast (24 degrees). The existence of a facet indicates the maxillary and mandibular teeth slide along an abraded surface. This phenomenon threw into question the value of measured condylar path. If a measured sagittal condylar path is 40 degrees, the wax-up done on an articulator with this condylar
The Journal of Gnathology. Volume 14. Number 1. 1995
path setting would produce a cusp angle of 40 de-grees. Because the average sagittal cusp angle of natural teeth is about 25 degrees, a cusp angle of 40 degrees is too sharp and may result in a cuspal interference. Thus it is questionable whether pre-cise reproduction of the condylar path on an articu-lator helps to produce good occlusion. The measurement and reproduction of the condylar path as the reference for occlusion, therefore, should be re-evaluated.
Deviation of the Condylar Path
McCollum5 recorded the condylar path of the pa-tient using a pantograph and found it did not change either when the mandible was guided by cusps of the natural teeth or when clutches with va-rious bearing pins were used. From this finding, he concluded the condylar path is a fixed factor that defies change; anterior guidance, on the other hand, can be changed freely by a dentist. This has been a basic gnathologic principle for years. Beard and Clayton6 reported that when the condy-lar path is traced repeatedly on a pantograph, the tracing line deviates and the deviations among temporomandibular disorder (TMD) patients are larger than those in healthy individuals. Clark and Lynn7 used the Sophon Visiform (U.S. Shiazai, Los Angeles, Calif) as a measuring device for mandibu-lar movement. They compared the incisal point path between "normal" patients and TMD patients. The results showed the TMD patients had larger discre-pancies in the incisal path. From this, it was theo-rized that TMD patients show discrepancies in their condylar path tracings instead of smooth tracings.
31



Original Article
lnte.rcondylar axis
Hobo et al - Re-evaluation of the Condylar Path 5
s
Fig 3 Bird's-eye view of the motion of intercondylar axis. During lateral movements. the mandible rotates around a center of rotation and advances straight outward along the terminal hinge axis, together with the body of the mandible as a whole. (From Hobo S: An electronic mandibular movement measuring system: its principle and clinical applications. In: Restoration of the Partially Dentate Mouth. Bates et al (eds). Chicago: Quintessence 1984; 55-78. Used with permission.)
ing-side condylar path deviates superiorly. When the lateral incisal path is positioned under the neutral line, the working-side condylar path deviates inferiorly. A similar tendency was observed in the anteroposterior direction (Fig 4). In this way, the sagittal deviation of the working-side condylar path shows a strong correlation with the deviation from the neutral line of the lateral incisal path. The correlation coefficient between the two deviations was 0.99 in the superoinferior direction and 0.97 in an anteroposterior direction (P = .001 ). This suggests the possibility that the working-side condylar path may deviate sagittally, as influenced by anterior guidance.
The Journal of Gnathology. Volume 14, Number 1, 1995
To verify this clinically, it was necessary to determine whether the working-side condylar path can be controlled by changing the anterior guidance. The subjects of this experiment were patients whose working-side condylar paths deviated more than 1 mm within the sagittal plane. The condylar paths of an arcon-type semiadjustable articulator on which the working-side condyle moves on the terminal hinge axis were adjusted using a patient's mea-sured condylar path. The neutral line was convert-ed mathematically to a computed value for the an-terior guide table of an articulator. Study casts mounted on the articulator were used to fabricate a resin guide table (Figs Sa to Sc). The
35


Original Article Hobo et al - Re-evaluation of the Condylar Path 7
RIGHT CONDYLE LEIT CONpYLE
SAGITTAL E--r.n 0 a..
"ti HORIZONTAL "ti 0 (/)
L
~ /
INF-
o R
\ ' '
~t .. 11 .......
-· L t ' i
-LEFT RIGHT-
RIGHT-
(
~L '\,
\ I R • .
---!
t
-INF
SCALE: MM
FRONTAL
CONOYLAR PATH
Fig 6 Results of the artificial control test of the working-side condylar path obtained by measuring the lateral movement of the subject using electronic measuring system. Dotted line= measured data obtained when the maxillary and mandibular teeth slide in contact. Solid line = measured data obtained by placing resin guide table and guide pin in the subject's mouth and allowing the guide table and tip of the guide pin to slide in contact. (R) right lateral movement; (L) left lateral movement.
anterior guide table was then placed in the mouth, and the patient was instructed to make an eccentric movement. When the guide table was used, the sagittal deviation of the working-side condylar path decreased to one fourth the original amount. More-over, in one patient the immediate sideshift and working-side condylar path disappeared simul-taneously (Fig 6).17
In dentistry, the condylar path has been considered the standard reference for occlusion. However, the above results show the condylar path is not fixed
The Journal of Gnathology, Volume 14. Number 1, 1995
but changeable. Furthermore, the fact than a change in the anterior guidance causes the immediate sideshift and working condylar path to disappear instantaneously proves that the condylar paths are influenced by anterior guidance. Poor anterior guidance, therefore, will adversely affect the condylar path, and if such a condylar path is measured precisely, reproduced on an articulator, and used as a reference for the fabrication of a restoration, the occlusion of the restorations can be similarly affected. Thus, the concept of applying
37


Original Article
1 : 2
2 3
Fig 7a Illustration of the influences of protrusive condylar path and incisal path on the amount of dis-occlusion at the second molar. (Op) amount of dis-occlusion during protrusive movement. (From Hobo et al: Clinical Atlas of Occlusion. Tokyo: Quintessen-ce. 1995.)
Conclusion
The quality of measuring systems for mandibular movement has been drastically improved since the days of McCollum. For example, a mechanical pantograph cannot measure Bennett movement graphically and digitally, as is possible today. The accuracy of the mechanical pantograph was about 1.0 mm but electronic systems are capable of mea-suring to about 0.1 mm. Scientific data obtained through these systems are changing old concepts. Therefore, gnathology must progress accordingly. Because the emphasis in gnathologic treatment has shifted from balanced occlusion to mutually protect-ed occlusion, anterior guidance has gained import-ance. In order to reproduce mutually protected oc-clusion, it is necessary to give equal consideration to the three apices of the mandibular triangle. Reli-ance solely on the condylar path must change. Because the condylar path deviates greatly and the
The Journal of Gnathology. Volume 14, Number 1, 1995
Hobo et al - Re-evaluation of the Condylar Path 9
Fig 7b Illustration of the influences of lateral condy-lar path and incisal path on the amount of dis-occlusion at the second molar. (ON) amount of dis-occlusion on nonworking side; (Ow) amount of dis-occlusion on working side. (From Hobo et al: Clini-cal Atlas of Occlusion. Tokyo: Quintessence1995.)
influence of the condylar path on occlusion is much smaller than that of anterior guidance, use of the condylar path as the reference for occlusion is questionable. However, this does not mean panto-graphic measurement of the condylar path is obsolete. The pantograph is an effective tool in the diagnosis and assessment of TMD and is consid-ered essential for educational purposes. During mandibular movement each apex of the mandibular triangle has two degrees of freedom for movement, for a total of six degrees of freedom. In order to obtain precise measurement, process the output data, and analyze the results, a computer-ization of the pantograph is indispensable. Since the mechanical pantograph lacks one apex, the anterior position, it is capable of measurement in only four degrees of freedom. The mechanical pantograph, therefore, is inadequate. The next-generation pantographic system must be a total system capable of measuring eccentric
39

10 Hobo et al - Re-evaluation of the Condylar Path
and masticatory movements with six degrees of freedom under tooth-contact condition, measuring opening and closing movements in reference to a horizontal plane, centric relation, and vertical dimen-sion, and at the same time, measuring muscle activity. The addition of computer graphics would be especially helpful in patient education.
References 1 The Academy of Prosthodontics : Glossary of prosthodontics terms. J Pros-
thet Dent 1994; 71: 43-112. 2 Craddock FW: The accuracy and practical value of records of condyle path
inclinations . J Am Dent Assoc 1949; 38: 697-710 . 3 Christensen LV. Slabbert CG: The concept of the sagittal condylar guid -
ance: biological fact of fallacy? J Oral Rehabil 1978; 5: 1-7 . 4 Donegan SJ, Christensen LV: Sagittal condylar guidance as determined by
protrusion records and wear facets of teeth. Int J Prosthodont 1991: 4: 469-472.
5 McCollum BB: Fundamentals involved in prescribing restorative dental remedies. A Research Report . In: McCollum BB. Stuart CE (eds). Scientific Press, South Pasadena. Calif 1955; 34-86.
6 Beard CC, Clayton JA: Electronic PAI consistency in diagnos ing temporo-mandibular joint dysfunction . J Prosthet Dent 1975; 55: 255-259 .
7 Clark GT. Lynn P: Horizontal plane jaw movements in controls and clinic patients with temporomandibular dysfunction. J Prosthet Dent 1986; 55: 730-735.
8 Oliva RA, Takayama H, Hobo S: Three-dimens ional study of mandibular movement using an automatic electronic measuring system. J Gnathol 1986; 5: 115-182 .
9 Hobo S. Mochizuki S: A kinematic investigation of mandibular border move-ment by means of an electronic measuring system. Part I. Development of the measuring system. J Prosthet Dent 1983; 50: 368-373.
10 Hobo S: A kinematic investigation of mandibular border movement by means of an electronic measuring system. Part II. A study of the Bennett movement. J Prosthet Dent 1984; 51: 642-646.
40
Original Article
11 Hobo S, lchida E. Garc ia LT: Osseointegration and Oral Rehabilitation . Quintessence . Tokyo 1990.
12 Hansson T. Oberg T. Carlsson GE. Kopp S: Thickness of the soft tissue layers and the articular disk in the temporomandibular joint. Acta Odontol Scand 1977: 35: 77-83 .
13 Hobo S. Takayama H: Analysis of differences between the eccentric and re-turning sagitta l condylar paths (In progress)
14 Hobo S: A kinematic investigation of mandibular border movement by an electronic measuring system. Part II. A study of the Bennett movement. J Prosthet Dent 1984; 51: 642-646 .
15 Hobo S: A kinematic investigation of mandibular border movement by means of an electron ic measuring system . Part Ill. Rotational center of lateral movement. J Prosthet Dent 1984; 52: 66-72 .
16 Hobo S, Takayama H: Effect of canine guidance on working condylar path. Int J Prosthodont 1989; 2: 73-79 .
17 Hobo S, Takayama H: Analysis of cuspid guidance effect on the working side condyle path (In progress)
18 Haramoto N. Takayama H, Hobo S: Measurement of disocclusion during protrusive movement. Part I. Normal dentition with anterior teeth. J Jpn Gnathol 1993: 14: 41-44 .
Address:
Sumiya Hobo Director Hisao Takayama Senior Researcher Lecturer Kanagawa Institute of Technology
International Dental Academy, 25-18, 1-chome, Shotoh, Shibuya-ku, Tokyo, 150 Japan
The Journal of Gnathology, Volume 15, Number 1, 1995