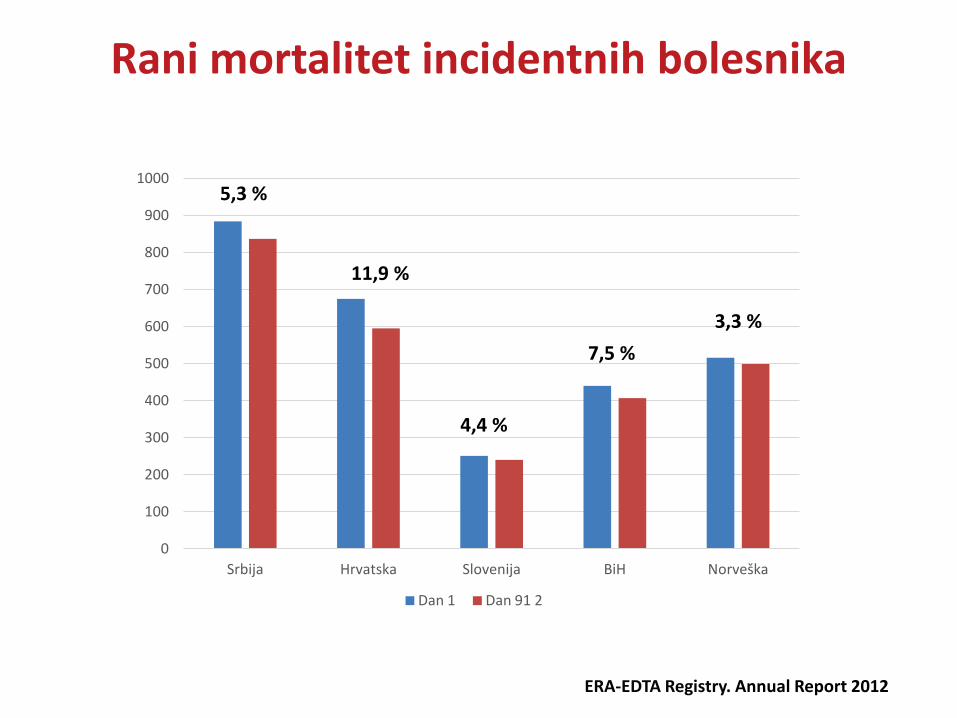
Rana smrt nakon započinjanja lečenja hemodijalizama 1 Dan 91 2 5,3 % 11,9 % 4,4 % 7,5 % 3,3 % Rani m ortalitet incidentnih bolesnika ERA-EDTA Registry. Annual Report 2012 0 20 40
22
Rana smrt nakon započinjanja lečenja hemodijalizama Radomir Naumovic Klinika za nefrologiju, KCS Medicinski fakultet u Beogradu ŠKOLA HEMODIJALIZE LESKOVAC 15-17 MAJ, 2015
HBI • Stariji bolesnici • Kasno javljanje nefrologu
HBI
• Nedostatak terapije koja prekida progresiju HBI • Nedostatak sredstava u fondovima osiguranja • Nedostatak mesta za hemodijalizu
Početak hemodijalize-Klinička neizvesnost
THBI: Povećan
morbiditet i mortalitet
Povećan rizik za
bakteriemiju
Dijalizna hipotenzija
Hipokalemija
Početak ESA Th
Gubitak rezidualne
funkcije
Rani mortalitet
• Malo podataka • Neadekvatni podaci
Rani mortalitet
• Klinička iskustva • Prve nedelje/povećana
smrtnost
Rani mortalitet
• Mere prevencije • Adekvatnije
lečenje
Foley RN, et al. Kidney International 2014; 86:392–398
Početak hemodijalize-Rani mortalitet
Opšta stopa smrtnosti i u zavisnosti od modaliteta lečenja
USRDS. Annual data report 2014
Opšta stopa smrtnosti kod prevalentnih bolesnika na hemodijalizi
USRDS. Annual data report 2014
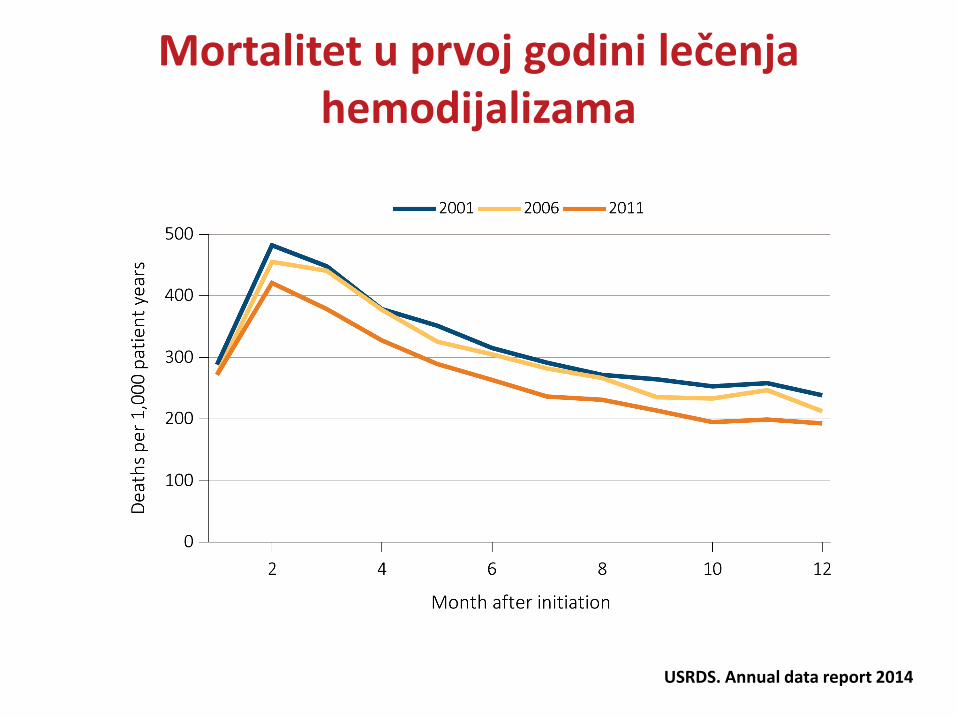
Mortalitet u prvoj godini lečenja hemodijalizama
USRDS. Annual data report 2014
USRDS. Annual data report 2014
Kardiovaskularni mortalitet u prvoj godini lečenja hemodijalizama
ERA-EDTA Registry. Annual Report 2012
0
100
200
300
400
500
600
700
800
900
1000
Srbija Hrvatska Slovenija BiH Norveška
Dan 1 Dan 91 2
5,3 %
11,9 %
4,4 %
7,5 % 3,3 %
Rani mortalitet incidentnih bolesnika
ERA-EDTA Registry. Annual Report 2012
0
20
40
60
80
100
120
140
160
180
Srbija Hrvatska Slovenija BiH Norveška
Series 1 Series 2
5,3 %
11,9 %
4,4 % 7,5 %
3,3 %
Mortalitet u prva 3 meseca lečenja dijalizama (pmp)
Stopa incidence bolesnika lečenih metodama ZFB prvog i 91. dana
Godišnji izveštaj o lečenju dijalizama i transplantacijom bubrega u Srbiji, 2010 .
29,2%
Godišnji izveštaj o lečenju dijalizama i transplantacijom bubrega u Srbiji, 2012 .
Stopa incidence bolesnika lečenih metodama ZFB prvog i 91. dana
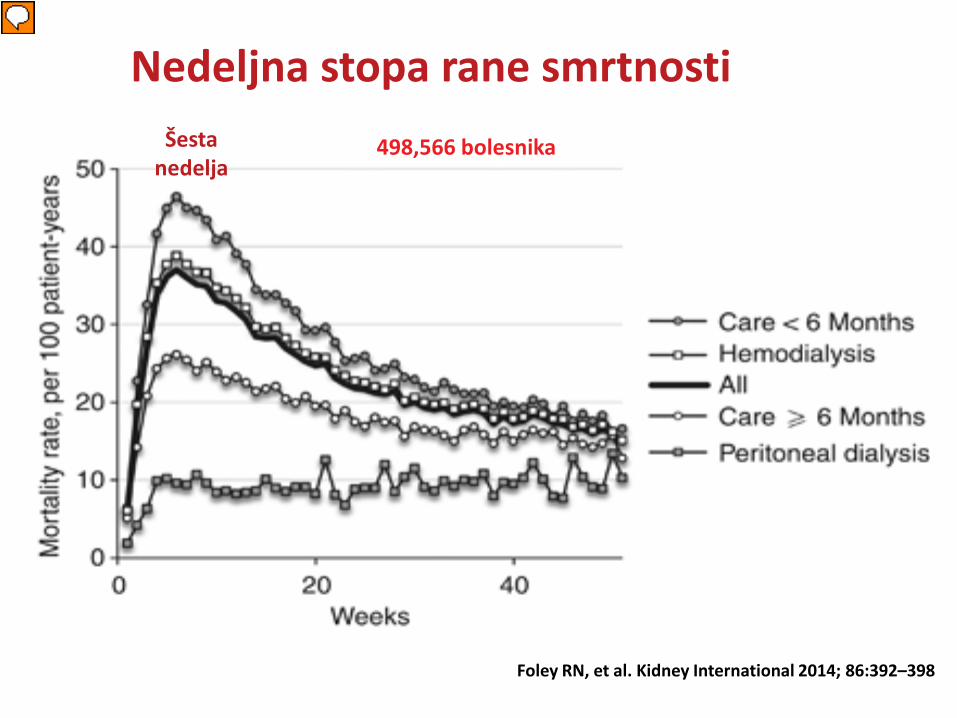
Nedeljna stopa rane smrtnosti
Foley RN, et al. Kidney International 2014; 86:392–398
Šesta nedelja
498,566 bolesnika
Presenter
Presentation Notes
Stopa mortaliteta HD bolesnika je 5.9/100 bolesničkih godina prve nedelje, dostiže maksimum od 37 / 100 bolesničkih godina u šestoj nedelji i postepeno opada do kraja prve godine kada je d declined steadily to intermediate levels by week 51 (14.8 per 100 person-years). Figure 1 also shows weekly mortality rates in subgroups defined by duration of nephrologist care and initial mode of dialysis. At all time points, rates were highest with nephrologist care o6 months followed by hemodialysis, nephrologist careX6 months, and peritoneal dialysis. Mortality rates peaked after 4 weeks in all subgroups and gradually declined in all subgroups except in peritoneal dialysis patients, for whom rates remained stable. Figure 1 shows weekly mortality rate intervals following hemodialysis initiation. Mortality rates in the dialysis population were 5.9 per 100 person-years in week 1, peaked at 37.0 per 100 person-years in week 6, and declined steadily to intermediate levels by week 51 (14.8 per 100 person-years). Figure 1 also shows weekly mortality rates in subgroups defined by duration of nephrologist care and initial mode of dialysis. At all time points, rates were highest with nephrologist care o6 months followed by hemodialysis, nephrologist careX6 months, and peritoneal dialysis. Mortality rates peaked after 4 weeks in all subgroups and gradually declined in all subgroups except in peritoneal dialysis patients, for whom rates remained stable.
Relativni rizik za rani mortalitet i hospitalzacije
Chan KE, et al. CJASN 2011; 6:2642-2649
303 289 bolesnika
Druga nedelja (RR 2.86)
Prva nedelja (RR 1.98)
Presenter
Presentation Notes
(A) Among patients starting chronic dialysis (n = 303,289), the relative risk of death at each 1-week interval was compared with a reference group of patients who survived the first year of dialysis. The period of highest death risk occurred in the second week (relative risk [RR] = 2.86; l [CI] 2.63 to 3.12; referenced to patients who survived the first year of dialysis). Patients were followed over 35,067,157 dialysis treatments for mortality outcomes. (B) Among patients starting chronic dialysis (n = 303,289), the RR of hospitalization at each 1-week interval was compared with a reference group of patients who survived the first year of dialysis. The period of highest hospitalization risk occurred in the first week (RR = 1.98; 95% CI 1.92 to 2.03; referenced to patients who survived the first year of dialysis).
Rani mortalitet
Faktori pre početka HD
Komorbiditet
Lečenje anemije
Faktori Uzrokovani
HD
Faktori rizika ranog mortaliteta
Kevin E. Chan et al. CJASN 2011;6:2642-2649
Rani mortalitet na HD: Faktori rizika
Rani mortalitet na HD
Početak HD preko katetera Ishemijska bolest srca
Rani mortalitet na HD eJGF≥15ml/min, Kraće predijalizno
nefrološko lečenje Hipertenzivna bolest bubrega
Rani mortalitet na HD
Stariji bolesnici, Ženski pol, Bela rasa ATN
Rosansky S, et al. Clin J Am Soc Nephrol 2011; 6:1222–1228.
Presenter
Presentation Notes
Table 2 shows hazard ratios for mortality in two time frames, 7–12 weeks (inclusive) and 13–51 weeks (inclusive). In each of these time frames, multivariate analysis showed that mortality was associated with older age, female sex, white race, non-Hispanic ethnicity, ESRD from hypertension and acute tubular necrosis, ischemic heart disease, estimated glomerular filtration rate X15 ml/min per 1.73m2, shorter duration of nephrologist care, and hemodialysis, especially with a catheter. For early mortality risk, adjusted hazard ratios (AHRs) X2 were seen with age 465 years (AHR 5.80 vs.o40 years), hemodialysis with a catheter (AHR 2.73 vs. hemodialysis with a fistula), and age 40–64 years (AHR 2.33); for later mortality, AHRs X2 were seen with age 465 years (AHR 4.32), hemodialysis with a catheter (AHR 2.10), and age 40–64 years (AHR 2.00).
Od 01. januara 2005.g. do 03.05.2015.g., 134 bolesnika je zapocelo lecenje hemodijalizama u nasem centru. Od tog broja je bilo 50 zena i 84 muskaraca. Prosecna starost bolesnika u trenutku zapocinjanja HD, Od 01. januara 2005.g., u nasem centru je 52 godine. 32 bolesnika koji su zapoceli HD u nasem centru je bilo u starosnoj dobi od 60-70 god. 22 bolesnika koji su zapoceli HD u nasemcentru je bilo u starosnoj dobi od 70-90 god. Kod 12 bolesnika koji su zapoceli HD u nasem centru od 01.01.2005.g. do danasnjeg dana je u toku prve godine nastupio smrtni ishod. 3 bolesnika u roku od 3 meseca umrlo. Kod 3 bolesnika je smrtni ishod nastupio u cetvrtom mesecu
Desetogodišnje iskustvo NFK KCS
0
2
4
6
8
10
12
14
1-3 mesec Četvrti mesec 5-12 mesec Ukupno
Broj
um
rlih
bole
snik
a
Vreme (meseci)
2,2% 2,2%
4,5%
8,9%
Presenter
Presentation Notes
Kod 12 bolesnika koji su zapoceli HD u nasem centru od 01.01.2005.g. do danasnjeg dana je u toku prve godine nastupio smrtni ishod. 3 bolesnika u roku od 3 meseca umrlo. Kod 3 bolesnika je smrtni ishod nastupio u cetvrtom mesecu
Kako poboljšati ishod?
Prevencija i lečenje KV
morbiditeta
Prevencija i lečenje SHP.
Pravovremeno lečenje anemije
Pravovremeno kreiranje AVF
Individualizacija
modaliteta lečenja
Presenter
Presentation Notes
The most common form of acute allograft rejection is initiated when donor alloantigens are presented to the T lymphocytes of the recipient by antigen-presenting cells (APCs). Immature dendritic cells within the graft carry donor antigens from the transplanted organ to the recipient’s draining lymph nodes and spleen; during their journey, these antigens mature into APCs.29 The recipient’s antigen-presenting dendritic cells also participate and circulate through the graft. The APCs then home to lymphoid organs, where they activate the recipient’s T cells. These T cells differentiate into various subgroups and return to the graft, where they take part in destroying the transplanted organ.