radiotherapy and radionuclides - royal surrey county hospital · the christie nhs foundation trust...
TRANSCRIPT
The Christie NHS Foundation Trust
Radiotherapy and radionuclides
Kate Garcez
Consultant Clinical Oncology
Christie NHS Foundation Trust
Manchester
9th Nov 2016

The Christie NHS Foundation Trust
Where does radiation fit in?

The Christie NHS Foundation Trust
How does radiotherapy work? • High energy photons produced by linear
accelerators cause ejection of electrons
from molecules
• Direct or indirect interaction with DNA
damages it
• Preferentially kills dividing cells
• No discrimination between cancerous or
normal……toxicity
• Aim is to exploit differences between normal
cells and cancer cells – normal cells better
able to repair damage

The Christie NHS Foundation Trust
The Challenge
Dose to cancer = cure rates
Dose to normal tissues = side effects

The Christie NHS Foundation Trust
• Relevance of acute vs late toxicity depends on prognosis
• All toxicity increases with total dose
• Fraction size affects late toxicity more than acute toxicity

The Christie NHS Foundation Trust
Aim of palliative EBRT for bone mets
• Treat bone pain
• Preserve function (eg MSCC)
• Consolidate surgical intervention
• 60-80% response rates
• Some (approx 25%) have complete pain response
• Can take 4-6 weeks to achieve result
The Christie NHS Foundation Trust
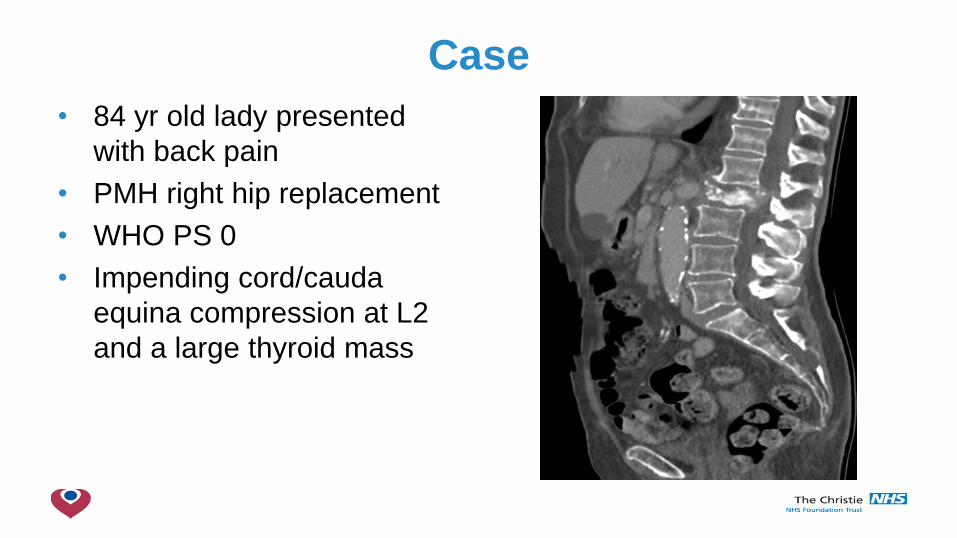
Case
• 84 yr old lady presented
with back pain
• PMH right hip replacement
• WHO PS 0
• Impending cord/cauda
equina compression at L2
and a large thyroid mass

The Christie NHS Foundation Trust
• Underwent spinal
decompression and
stabilisation
• Histology confirmed
follicular thyroid cancer
• Excellent post op recovery,
independently mobile, PS 1
• Referred for post-op RT
• 20Gy in 5# T12-L4
• Single post field

The Christie NHS Foundation Trust
Surgery/RT for MSCC
• Surgery + RT better than RT alone
• Scoring systems to evaluate prognosis/guide selection of patients • General condition, number of bone mets other than spinal mets, number of spinal mets, type
of primary lesion, presence of mets in other organs, state of paralysis
• Aim is to debulk and stabilise
• Does not obviate need for post op RT
• Little evidence re doses in post-op setting – aim is to eradicate
microscopic residual disease, often use longer fractionated
schedules
Patchell et al Lancet 2005; 26;366(9486):643-648
Tokuhashi et al Spine 2005;30:2186-2191

The Christie NHS Foundation Trust
Treatment delivery

The Christie NHS Foundation Trust
Toxicity of EBRT
• Pain flare
• Lasts 1-2 days
• Treat with steroids
• Skin reaction
• Fatigue
• Location specific: nausea, diarrhoea, cystitis, hair loss

The Christie NHS Foundation Trust
Case cont’d
• Staging bone scan showed
known disease at L2,
patchy uptake elsewhere in
spine, and left upper femur
• X-ray
• Referred to orthopaedic
surgeons

The Christie NHS Foundation Trust
• Underwent prophylactic
nailing of left femur
• Well post-op
• Post-op RT
• 8Gy 1#
• Single ant/post field
• Cover metalwork

The Christie NHS Foundation Trust
Dose/fractionation
• Single vs fractionated treatment
• Equivalent rates of pain relief, time to pain relief (ASTRO guidelines)
• Convenience of single #
• Retreatment rates higher with single # (20% vs 8%)
• Acute toxicity greater/more prolonged with fractionated treatment
(except pain flare)
• Typical schedules - 8Gy/1#, 20Gy/5#, 30Gy/10#
• SCORAD III – single vs multifraction RT in MSCC
• Always important to consider prognosis/intended benefit
Lutz et al Int J Radiat Onc Biol Phys 2011; 15; 79(4):965-76

The Christie NHS Foundation Trust
Other examples
• 57 yr old man, locally advanced H&N cancer
• PS 3, severe lower back pain
• Wire to localise on planning scan, 8Gy 1#

The Christie NHS Foundation Trust
• 60 yr old lady
• Metastatic thyroid cancer
• 30Gy 10#
• Planned conformally (4
beams)
• Higher doses to disease,
less dose to surrounding
tissue

The Christie NHS Foundation Trust
• 69 yr old man incidental
finding of bone mets
• Biopsy confirmed metastatic
thyroid cancer
• Embolisation and
stabilisation of L1
• Post-op RT, 40Gy in 20#
• 6 beams
• OARs (organs at risk)

The Christie NHS Foundation Trust
SBRT (stereotactic body radiotherapy)
• Emerging for oligometastatic
disease (≤ 3 sites)
• Extremely conformal with steep
dose gradient
• Tight margins 2-3mm
• High total dose, few fractions
• 30-40Gy in 3# alt days
• 24-27Gy in 3# alt days spine
• Local control rates 90%
• May delay the need for systemic
therapy, possible improve PFS
Owen et al Pract Rad Oncol 2014; 4(2) e143-4149

The Christie NHS Foundation Trust
SBRT
• Immobilisation crucial – minimise intra-fraction motion
• Increased planning (dosimetry/verification/monitoring) time
• Increased treatment delivery time (ie time on the bed)
• Available in UK through Commissioning through Evaluation
programme for spine and bone mets
• CORE trial (Conventional care Or Radioablation in the treatment of
Extracranial metastases)
• Collect data (acute/late toxicity may be different)

The Christie NHS Foundation Trust
Radionuclides
Iodine 131
Radium 223

The Christie NHS Foundation Trust
I131 – thyroid cancer • Differentiated thyroid cancer (papillary,
follicular)
• Iodine selectively taken up by thyroid
cells via sodium-iodide symporter
(NIS)
• β particles (path length 1-2mm)
• Excretion via urine 75%
• Half life 8 days
• Thyroid remnant ablation, first line
therapy for metastatic disease

The Christie NHS Foundation Trust
I 131 therapy
• Low iodine diet
• TSH stimulation
• Isolation
The Christie NHS Foundation Trust
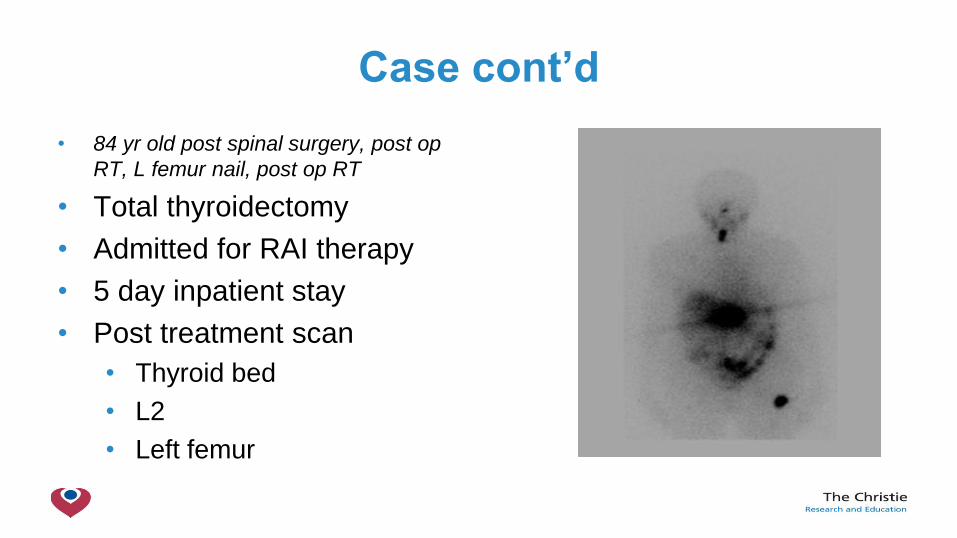
Case cont’d
• 84 yr old post spinal surgery, post op
RT, L femur nail, post op RT
• Total thyroidectomy
• Admitted for RAI therapy
• 5 day inpatient stay
• Post treatment scan
• Thyroid bed
• L2
• Left femur

The Christie NHS Foundation Trust
Case cont’d
• 1 year later
• Tg rising, more left hip pain
• Further admission for RAI
• Post treatment scan
• 3 months later pain
improved

The Christie NHS Foundation Trust
Toxicity and restrictions
• Acute: parotiditis, altered taste, nausea, possible tumour
‘flare’ – pain, swelling (caution with vertebral mets, consider
steroid cover)
• Late: xerostomia, sialadenitis, second malignancy
• Length of stay variable (5 days)
• Uptake scan before discharge
• Radiation protection precautions on discharge

The Christie NHS Foundation Trust
Radium 223 – prostate cancer
• Metastatic castration resistant
prostate cancer (bone)
• Bone seeking calcium mimetic,
accumulates in bone with increased
turnover eg osteoblastic or sclerotic
mets
• α emitter, very short path (< 100µm,
2-10 cell diameters) therefore highly
localised effect
• Half life 11.4 days
The Christie NHS Foundation Trust
Radium 223 therapy
• 6 treatments at monthly intervals
• IV administration
• Outpatient treatment
• Stop calcium supplements, check FBC
• Excretion via faeces – 75% in first week
• 5% in urine
• Minimal restrictions

The Christie NHS Foundation Trust
• 921 patients, phase 3, randomised, double blind
• 2:1 radium x 6 vs placebo x 6
• Primary: OS
• Secondary: time to first symptomatic skeletal event, various
biochemical endpoints

The Christie NHS Foundation Trust
Results • Eligibility:
• Progressive castration
resistant prostate cancer
• ≥ 2 symptomatic bone
mets, no visceral disease
• +/- previous docetaxel
• Baseline PSA ≥ 5ng/ml
• Median overall survival
extended by 3.6 months

The Christie NHS Foundation Trust
• 6 month delay to first
symptomatic skeletal event
• Well tolerated
• No clinically meaningful
differences in G3-4 adverse
events
• Improved QOL scores
• In practice:
• Consent for pain flare,
myelosuppression, nausea,
diarrhoea
• Most patients receive the planned
6 cycles

The Christie NHS Foundation Trust
Summary
• Radiation therapy remains an important treatment modality in
management of bone metastases
• Reduces symptoms and can improve overall survival
• Should be tailored to suit individual patients
The Christie NHS Foundation Trust
Thank you