radiosurgery beyond the brain - peacehealth beyond the brain: advances in the treatment of...
TRANSCRIPT

1
Radiosurgery Beyond the Brain:Advances in the Treatment of Extracranial Radiosurgery
Haidy Lee MD
May 12, 2009

2
Background• Extracranial radiosurgery = Stereotactic Body
Radiotherapy (SBRT)• Very large doses of extremely precise ionizing
radiation• A highly specialized form of image-guided
radiotherapy (IGRT)• Given in 1-5 fractions
3
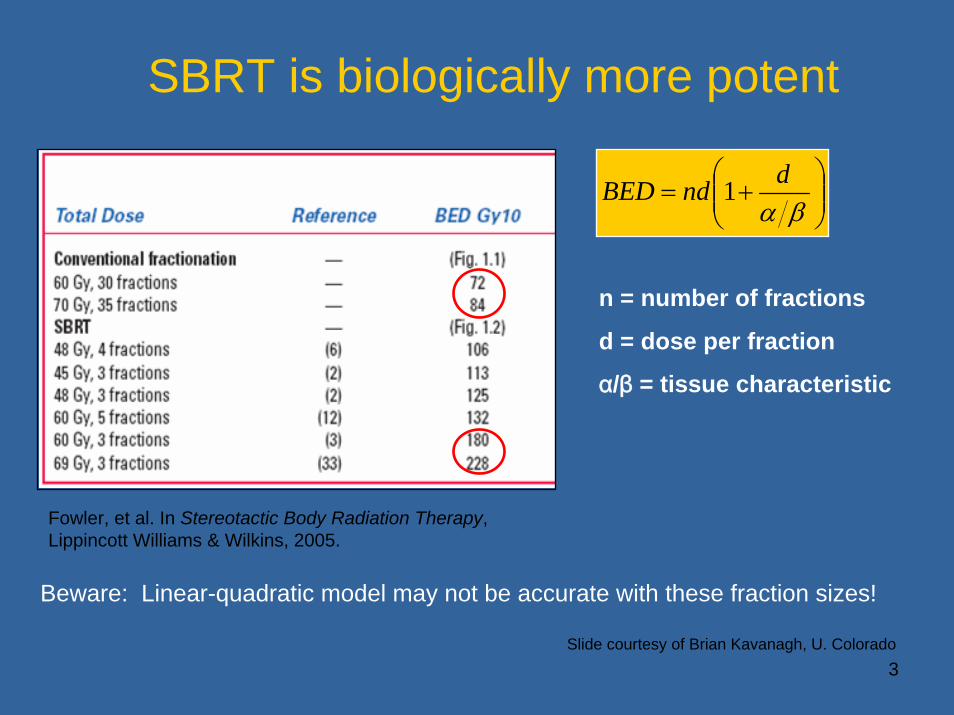
SBRT is biologically more potent
⎟⎟⎠
⎞⎜⎜⎝
⎛+=
βαdndBED 1
n = number of fractions
d = dose per fraction
α/β = tissue characteristic
Beware: Linear-quadratic model may not be accurate with these fraction sizes!
Fowler, et al. In Stereotactic Body Radiation Therapy, Lippincott Williams & Wilkins, 2005.
Slide courtesy of Brian Kavanagh, U. Colorado

4
Intracranial Stereotactic Radiosurgery versusSBRT
Slide courtesy of Brian Kavanagh, U. Colorado

5
Patient Immobilization
BodyFix dual vacuum system with abdominal compression

6
Patient Immobilization
Aquaplast mask

7
Intracranial Stereotactic Radiosurgery versusSBRT
Slide courtesy of Brian Kavanagh, U. Colorado

8
Repositioning
• Accuracy between treatment planning and treatment
• Multiple treatments• Patient comfort

9
Intracranial Stereotactic Radiosurgery versusSBRT
Slide courtesy of Brian Kavanagh, U. Colorado

10
Imaging
• CT scan or x-rays on treatment couch• Registration of anatomy• Fiducial references
Image showing both kVCT (grey) and MVCT (green)
Before Registration After Registration

11
Intracranial Stereotactic Radiosurgery versusSBRT
Slide courtesy of Brian Kavanagh, U. Colorado

12
Respiratory Control
• Abdominal compression• Respiratory gating• Tumor tracking

13
Abdominal Compression
• Paddle used to induce shallow breathing
Elekta Stereotactic Body Frame

14
Beam ON Beam ONBeam OFF
tumortumor
tumor
Respiratory Gating
Slide courtesy of P. Keall, VCU

15
Tumor Tracking

16
Treatment Delivery
• Ablative doses• Conformal delivery• Rapid dose fall off

17
Treatment Delivery
ManufacturerSBRT
Radiation Unit
Image Guidance
RespiratoryManagement
FieldCollimation
Unit restrictedto SRS
Accuray CyberKnifeDual Fixed X-ray;
Simultaneous Imaging
Frameless real time fiducial based tracking Circular cones only Yes
BrainLab NovalisDual Fixed X-ray;
Sequential Imaging
Respiratory gating with IR markers
Micro-MLC with minimum of 3 mm
at isocenter or circular cone attachments
No: Field size limited to 10x10 cm at
isocenter
Elekta Synergy S
Rotating kV x-ray for fixed planar
views and kVCBCT
Active breathing control (ABC): Breath hold technique and frame/abdominal
compression
Micro-MLC with minimum of 4 mm
at isocenter or circular cone attachments
No, Field size limit
16 x 21 cm atisocenter
Siemens Primatom
In-room CT scanner with
couch coupled to linac
Frame/ abdominal compression
MLC with 1 cm leaf or circular cone
attachmentsNo
Tomotherapy HiArtTomotherapy Fan beam MVCT Frame/ abdominal
compression
Minimum MLC leaf configuration of 6 mm and 6 mm jaw
width
No
Varian Trilogy
Rotating kV x-ray for fixed planar
views and kVCBCT
Respiratory gating with IR marker system
Micro-MLC with minimum of 5 mm
at isocenter or circular cone attachments
No

18
Treatment Delivery

19
Indications• Organs
– Parallel vs Serial Organs• Definitive treatment
– Early stage NSCLC– Hepatoma– Prostate– Pancreas
• Palliative treatment– Oligometastatic disease
• Lung, Liver, Spine– Recurrence
• Prior radiation therapy

20
Indications• Organs
– Parallel vs Serial Organs• Definitive treatment
– Early stage NSCLC– Hepatoma– Prostate– Pancreas
• Palliative treatment– Oligometastatic disease
• Lung, Liver, Spine– Recurrence
• Prior radiation therapy

21
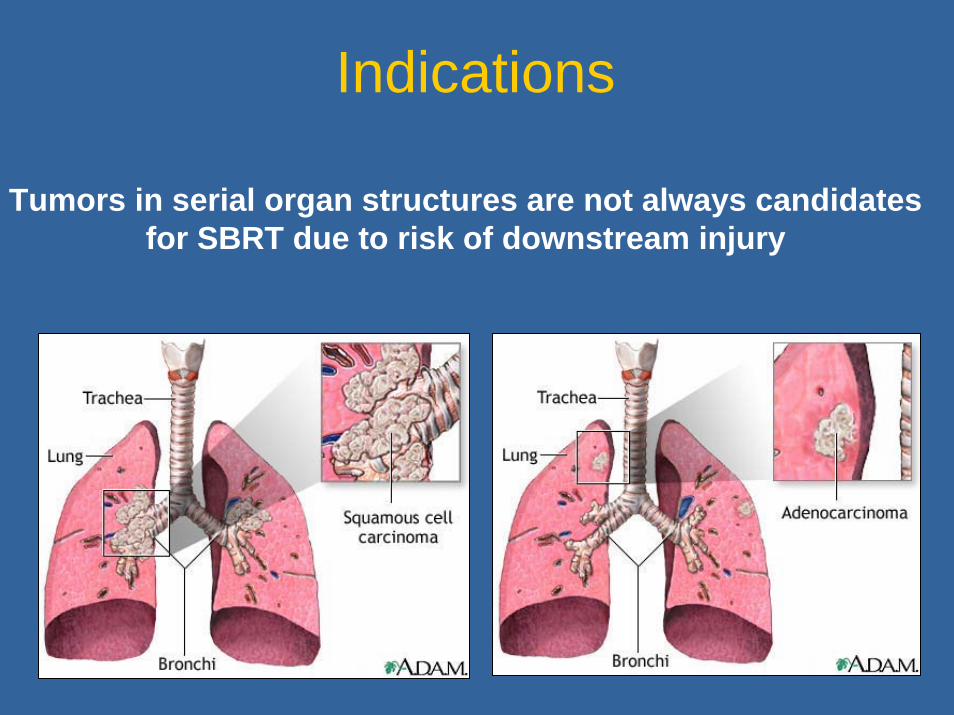
Indications• Parallel Organs• Serial Organs
Lung: Serial organ structure proximally becominga parallel organ structure distally
22
Tumors in serial organ structures are not always candidates for SBRT due to risk of downstream injury
Indications

23
Early stage NSCLC

24
Early stage NSCLC56 year old woman with a 1.2 cm biopsy proven right lung lesion as her only site of disease

25
Early stage NSCLCIsodose distribution
37.5Gy in 3 fractions
Axial
Sagittal
c Coronal

26
Early stage NSCLCThe planning scan is co-registered with the MVCT scan prior to
treatment to ensure accuracy of delivery
Planning CT in grey
MVCT in yellow

27
Pretreatment scan 2 months post treatment
3 months post treatment 6 months post treatment
- early fibrosis
12 months after treatment
12 months post treatment
- fibrosis
Early stage NSCLC

28
Metastatic sarcoma 20 Gy in one fraction
Pretreatment CT scan 2 months post treatment
Palliation Lung

29
Prospective Liver Metastasis SBRT Clinical Trials
• Hoyer phase II colorectal metastases (n = 44); 45 Gy/ 3 fxs 2-year actuarial lesion control rate of 86%
• Kavanagh phase I/II trial (n = 36)36-60 Gy/ 3 fxs without reaching DLT (I); 93% local control at 18mo with no grade 4 toxicity (II)
Hoyer M, Roed H, Traberg Hansen A, et al. Phase II study on stereotactic body radiotherapy of colorectal metastases. Acta Oncol 2006;45:823-830.Kavanagh BD, Schefter TE, et al. Interim analysis of a prospective phase I/II trial of SBRT for liver metastases. Acta Oncol 2006;45:848-855.
PalliationLiver

30
Palliation Liver

31
First Spinal RS• University of Arizona
– 45 Gy external radiation previous XRT
– 8-10 Gy for recurrent tumor in single fraction
• Setup aided by surgically implanted device that docked into external frame (FIGURE)
• 5 patients followed median 6 months– Good local control and palliation
described
Hamilton et al, Neurosurgery. 36(2):311-319, February 1995
Palliation Spine

32
• Continuous 20-sec MRI during normal breathing • Spinal cord motion is generally small (< 0.5 mm)
Palliation Spine

33
Study n Dose (Gy) Pain Improvement
Jin (2007) 196 10-18 85%
Gibbs (2007) 74 16-25 84%
Gerszten (2007) 500 12.5-25 84%
Gerszten (2005) 26 16-20 92%
Degen (2005) 51 10-37.5 97.3%
Gerszten (2004) 115 12-20 94%
DeSalles (2004) 14 8-21 50%
Benzil (2004) 31 0.5-50 94%
Ryu (2004) 49 10-16 85%
Sheehan 34 18-24 90%
Pain Relief
PalliationSpine

34
Study n Control
Gerszten (2007) 500 90%
Gwak (2006) 3 33%
Ryu (2004) 49 95%
Sheehan 34 90%
Tumor Control
PalliationSpine

35
Palliation Spine
Isodose Distribution24 Gy in 3 fractions
Axial Coronal Sagittal

36
MSKCC Spinal SBRT Experience
• 93 patients, 103 lesions– No spinal cord compression
• Single fraction 18-24 Gy– CTV usually vertebral body– PTV = CTV +2mm– Spinal cord max 12-14 Gy
• Better control at higher dose (24 Gy) than lower (above)
Yamada et al, Int J Rad Oncol Biol Phys, 2008
Metastatic Colorectal CA

37
Spinal Target volumes, from “Partial Volume Tolerance of the Spinal Cord and Complications of Single-Dose Radiosurgery”
Ryu et al, Cancer, 2007
• Cord drawn 6mm above and below target• Major constraint: no more than 10% of cord receives
dose above 10 Gy• Only 1 observed cord complication among 177 pts

38
Note: Patient was heavily pre-and post-treated with chemotherapy.Symptoms included RLE weakness, resolved with steroids
Toxicity“Partial Volume Tolerance of the Spinal Cord and Complications of Single-Dose Radiosurgery” Ryu et al, Cancer, 2007
Pretreatment Isodose Plan
Post treatment

39
Toxicity
Freedom from grade 3-5 toxicity

40
Toxicity
• 40 patients treated at UVA
• T1-2 non-small cell lung cancer
• 45-60Gy in 3 fractions
Number (%) n=40
Chest Wall pain 9 (23%)
Rib Fracture 2 (5%)
Pneumonitis
Grade 1 5 (12%)
Grade 2 1 (2%)
Grade 3 1 (2%)
Median (range)
Onset of Pain (months) 7.1 (0.6 - 32.3)
Time to rib fracture (months) 20.6 (8.9 – 33.3)

41
Future Directions
• Radiobiology• Interaction with chemotherapy,
targeted agents, radioprotectors• Improved Treatment Delivery• Long-term outcome data• Economics

42
Disclosures
• None

43
Credits
University of Virginia Department of Radiation Oncology– Paul Read MD, PhD– Stan Benedict PhD– Ke Sheng PhD– Jing Cai PhD– Neal Dunlap MD– Jason Sheehan MD (Dept of Neurosurgery)