radioimmunolocalization and selection for surgery in recurrent colorectal cancer
TRANSCRIPT

Br. J. Surg. 1986, Vol. 73, January, 64-67
R. H. J. Begent, Patricia A. Keep, Frances Searle, A. J. Green, H. D. C. Mitchell, Barbara E. Jones, Joan Dent, J. E. H. Pendower, R. A. Parkins, K. W. Reynolds, T. G. Cooke, T. Allen Mersh and K. D. Bagshawe
Cancer Research Campaign Laboratories, Department of Medical Oncology and Departments of Surgery and Nuclear Medicine, Charing Cross Hospital and Medical School, London, UK Correspondence to: Dr R. H. J. Begent, Department of Medical Oncology, Charing Cross Hospital and Medical School, London W6, U K
Radio i m m u no loca I izat ion and selection for surgery in recurrent colorectal cancer
The value of radioimmunolocalization ( R I L ) of cancer depends on its performance in situations where the result determines the choice of management. A rise in serum carcinoembryonic antigen (CEA) values after apparently curative resection of colorectal cancer implies localized, resectable recurrence in some patients and widespread unresectable tumour in others. This study investigated the ability of RIL with radiolabelled antibody to C E A and a novel numerical method for analysis of results to determine the extent of disease in 31 patients with raised serum C E A but no physical signs of recurrence. Surgical exploration or conventional radiology later confirmed the presence of tumour in 94 per cent of sites which were positive by RIL. Negative RILpredicted the absence of disease in 53 per cent of patients. The investigation could discriminate between localized and disseminated disease and often performed better than conventional radiology. R I L appears useful in selection of patients for second look laparotomy. Keywords Radiolabelled antibodies, carcinoembryonic antigen, antitumour antibodies, radioimmunolocalization, colorectal cancer, tumour imaging, second look laparotomy
Deposits of CEA-producing tumours can be located by external scintigraphy after intravenous injection of radiolabelled antibody directed against CEA1-5. Most studies to date have attempted to validate the method (radioimmunolocalization (RIL)) by investigating patients with relatively large tumours which could be readily localized by other means.
The clinical usefulness of the investigation depends on its sensitivity and specificity by comparison with conventional imaging techniques when there is minimal tumour volume.
An opportunity to assess the usefulness of RIL in this type of situation occurs in colorectal cancer where a rise in serum CEA after apparently curative resection of the primary tumour frequently precedes clinically evident relapse by several months6*'. We have compared RIL using anti-CEA with conventional methods of assessment in such patients.
Patients and methods Thirty-one patients were studied 2 4 8 (median 14) months after apparently curative resection of adenocarcinoma of the colon (14 patients) or rectum (17 patients). During routine follow-up all were found to have at least one serum CEA value above lOpg/l by double antibody radioimmunoassay' but no palpable tumour recurrence at the time of RIL.
RI L procedure
RIL was performed as described previ~usly '*~. Briefly, hyperimmune goat antiserum to CEA absorbed with normal human colon, spleen, liver and serum* or mouse ascites rich in 11-285-14 monoclonal antibody to CEA (originating from Dr C. H. Ford and donated by Eli Lilly and Co.) were purified on columns of CEA-Sepharose or protein A-Sepharose respectively, before labelling with 13'iodine('3'I) to a specific activity of 3-10mCi/mg protein.
Patients received 60 mg potassium iodide three times daily for 10 days starting 24 h before administration of antibody and potassium
perchlorate 200 mg four times daily starting 30 min before administration of antibody. 1 pg of antibody was given intradermally 20 min before intravenous administration and one patient was excluded from further study because of an immediate type hypersensitivity reaction. 100-200pg of antibody was given by slow intravenous injection and images obtained 24h later with a Nuclear Enterprises LFOV gamma camera with a high energy collimator linked to a Nodecrest computer. Twenty-six patients were given goat polyclonal antibody and five mouse monoclonal antibody. Background distribution of antibody in non-tumour sites was simulated by obtaining images of 99mtechnetium (99mTc) and 99mT~04 as described by Goldenberg'. The total number of counts of 9 9 m T ~ and 13'1 were equalized and the 9 9 m T ~ image then subtracted from that of 13'1.
Analysis of RIL
Numerical analysis of areas of relative accumulation of I3'I antibody on the subtraction image were performed, as described by Green eta/.". In brief, regions of interest weredrawn around the suspect area and around an apparently normal area in the same organ or tissue. The ratio of countsof'311 inthetworegionswerecompared with that ~ f ~ ~ " ' T c i n the same regions. The difference between the two ratios was expressed in terms of standard deviations known as an Fx value. Previous studies had shown that positive Fx values could occur in the absence of turnour in the region of the heart, particularly the lower and right borders, the lower border of the liver, diffusely in the liver, the right mid-abdomen, the thyroid, and the kidneys and Positive Fx values in these regions were therefore excluded from analysis.
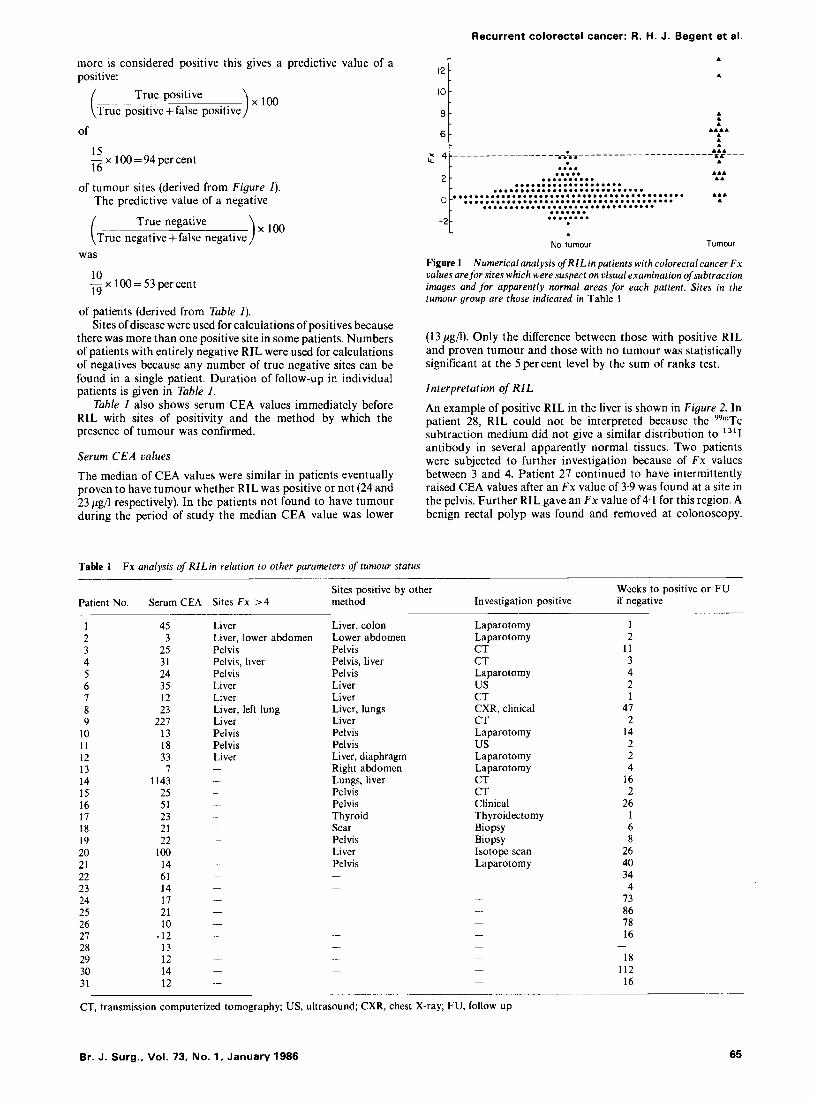
Results After RIL, patients were followed up clinically and investigations appropriate to each individual performed to confirm or refute the results of RIL. Fx values for areas at which tumour was subsequently found and for areas where n o evidence of tumour was found are shown in Figure 1. If an F x value of 4 or
64 0007-1323/86/010064-01%3.00 0 1986 Butterworth & Co (Publishers) Ltd
Recurrent colorectal cancer: R. H. J. Begent et al.
r A more is considered positive this gives a predictive value of a positive:
True positive ),la0 ( True positive +false positive
of
15 -xla0=94percent 16
of tumour sites (derived from Figure I). The predictive value of a negative
True negative i True negative +false negative was
10 - x 100 = 53 per cent 19
of patients (derived from Table I). Sites of disease were used for calculations of positives because
there was more than one positive site in some patients. Numbers of patients with entirely negative RIL were used for calculations of negatives because any number of true negative sites can be found in a single patient. Duration of follow-up in individual patients is given in Table I.
Table 1 also shows serum CEA values immediately before RIL with sites of positivity and the method by which the presence of tumour was confirmed.
Serum C E A values
The median of CEA values were similar in patients eventually proven to have tumour whether RIL was positive or not (24 and 23 pg/l respectively). In the patients not found to have tumour during the period of study the median CEA value was lower
Table 1 Fx analysis of RlLin relution to other parameters of tumour status
10 '*I 6
A
A A A
A A A A A A A
A A A
A
A A A A A
.... I=---
A A A A
.... ..... .......... .................... ............................ ........................................... ....................................... ................................ ....... ........ . No tumour Tumour
Figure 1 Numerical analysis of RILin patients with colorectal cancer Fx values are for sites which were suspect on visual examination of subtraction images and for apparently normal areas for each patient. Sites in the tumour group are those indicated in Table 1
(13 pg/l). Only the difference between those with positive RIL and proven tumour and those with no tumour was statistically significant at the 5 percent level by the sum of ranks test.
Interpretation of RIL
An example of positive RIL in the liver is shown in Figure 2. In patient 28, RIL could not be interpreted because the 9 9 m T ~ subtraction medium did not give a similar distribution to 13 '1
antibody in several apparently normal tissues. Two patients were subjected to further investigation because of F x values between 3 and 4. Patient 27 continued to have intermittently raised CEA values after an F x value of 3.9 was found at a site in the pelvis. Further RIL gave an F x value of 4.1 for this region. A benign rectal polyp was found and removed at colonoscopy.
Sites positive by other Weeks to positive or FU Patient No. Serum CEA Sites Fx > 4 method Investigation positive if negative
~
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31
45 3
25 31 24 35 12 23
227 13 18 33 7
1143 25 51 23 21 22
100 14 61 14 17 21 10
* 12 13 12 14 12
Liver Liver, lower abdomen Pelvis Pelvis, liver Pelvis Liver Liver Liver, left lung Liver Pelvis Pelvis Liver -
-
Liver, colon Lower abdomen Pelvis Pelvis, liver Pelvis Liver Liver Liver, lungs Liver Pelvis Pelvis Liver, diaphragm Right abdomen Lungs, liver Pelvis Pelvis Thyroid Scar Pelvis Liver Pelvis -
Laparotomy Laparotomy CT CT Laparotomy us CT CXR, clinical CT Laparotomy us Laparotomy Laparotomy CT CT Clinical Thyroidectomy Biopsy Biopsy Isotope scan Laparotomy
~
~
-
-
- - - - -
-
~
1 2
11 3 4 2 I
47 2
14 2 2 4
16 2
26 1 6 8
26 40 34 4
73 86 78 16
18 112
16
-
CT, transmission computerized tomography; US, ultrasound; CXR, chest X-ray; FU, follow up
Br. J. Surg., Vol. 73, No. 1, January 1986 65

Recurrent colorectal cancer: I?. H. J. Begent et al.
Figure 2 RILshowing hepatic metastases. Anterior views of the abdomen in patient 1 showing distribution oJ I , '"I antibody to CEA: E, 99mTc subtraction medium; S , residual radioactivity in the liver after subtraction. Fx was 11.4. L, liver; B, bladder; T, tumour deposits
Laparotomy was then performed and no tumour found. Patient 18 had an F x value of 3.8 in the region of the abdominal scar. This led to ultrasound examination being performed which showed evidence of recurrence in the scar. This was confirmed surgically. In four patients (2, 8, 10 and 12) C T of the abdomen failed to show definite evidence of tumour at sites positive by RIL and later confirmed by other means. Of the five patients with positive RIL confirmed at laparotomy (Table I), three had negative CT in the appropriate area, one had positive CT and one a positive ultrasound. In one, barium enema was equivocal. Positive RIL in an area known to produce artefacts (the right mid abdomen) led to one patient (13) having C T of this area at which a mass of tumour was found on the posterior abdominal wall.
Resectability of recurrence
Eight patients were considered for resection of tumour. Two had malignant tumour resected. One of these was a metachronous carcinoma of the sigmoid colon (Figure 3), and one recurrence of carcinoma in the laparotomy scar (patient 18). The latter patient had progressively rising CEA after the second operation and was later shown to have residual carcinoma in the posterior abdomen lying directly behind the positive area in the scar. A benign polyp of the sigmoid colon was resected in another patient. Four patients (3, 5, 12 and 13) were found to have unresectable tumour at laparotomy but one (13) achieved a complete response on CT after chemotherapy with 5- fluorouracil and CCNU, followed by radiotherapy. She remains apparently free from tumour 29 months after RIL. One patient with a solitary liver metastatis was considered unfit for surgery because of chronic obstructive airways disease.
Discussion The value of an investigation in clinical practice depends on its ability to provide information not available by other means or to d o so with less disturbance to the patient or at significantly lower cost. In the context of localization of early recurrence of colorectal cancer RIL was sometimes able to provide unique information. It is capable of locating tumours in the lumen of the bowel, on peritoneal surfaces and in the liver and other viscera. This repertoire is beyond the scope of any other single
investigation but the number of false negative results is a limitation. In several of these instances, however, it was some months after RIL before the site of tumour was identified by other means. The number of misleading negative results can effectively be reduced by investigating a particular area further by other means when an F x value between 3 and 4 is found or when a positive region is located in an area known to produce artefacts. Fortunately the majority of recurrences of colorectal cancer are in areas not normally producing artefacts and even though a diffuse liver image and positive areas along the lower hepatic margin have to be discounted, discrete liver metastases can be visualized.
The quantitative assessment of positivity provided by the F x value" is not available with conventional tumour imaging methods and makes objective assessments of sensitivity and specificity possible. Previous studies of sensitivity based on more subjective judgements of the subtracted image2v4 reported positive localization of colorectal carcinoma in 41-92 per cent of patients, most of whom had advanced disease. It is to be expected that the proportion of positive images will fall as patients are studied at an earlier stage of the disease. Indeed, sensitivity has little meaning unless related to a particular disease situation. The data presented here relate to recurrence of colorectal cancer before abnormal physical signs occurred. It can be seen from Figure 1 that sensitivity can be increased by reducing the threshold for a positive F x value. This carries a penalty in terms of specificity which was considered unacceptable when the data were used to determine whether a patient should have a laparotomy.
Laparotomy and resection of recurrence have been widely studied in patients whose serum CEA rises progressively after apparently curative resection' - I 4 . Whilst some individuals have undoubtedly benefited from resection of recurrent or metachronous tumours found in this way, several groups have found the disease to be unresectable in most patient^".'^. Results of randomized studies of the effect of second look laparotomy on survival are awaited with interest.
Performing RIL when a rise in serum CEA occurs and only operating on those patients with disease which appears sufficiently localized for there to be a chance of resectability seems a more satisfactory alternative. RIL can be performed when one raised CEA value has occurred without waiting for a sustained rise. It is interesting that 4 of the patients in whom tumour was confirmed did not have a sustained rise in CEA.
Figure 3 RIL showing a metachronous tumour in the sigmoid colon. Views with patient I0 sitting above the gamma camera showing distribution oJ I , 13'1 antibody; E, 99mTC subtraction medium; S , residual activity behind the bladder after subtraction. Fx was 6 4 . B, bladder; 7;. turnour deposit
66 Br. J. Surg., Vol. 73, No. 1, January 1986

Recurrent colorectal cancer: R. H. J. Begent at al.
Tumour localisation of radiolabelled antibodies against carcinoembryonic antigen in patients with carcinoma. N Engl J Med 1980; 303 5-10. Begent RHJ, Bagshawe KD. Radioimmunolocalization ofcancer. Chapter 9 in: Oncodevelopmental Markers. New York: Academic Press, 1983: 167-88. N.I.H. Consensus Statement. Carcinoembryonic antigen: its role as a marker in the management of cancer. Br Med J 1981; 282 373-5. Tate H. Plasma CEA in the post-surgical monitoring ofcolorectal carcinoma. Br J Cancer 1982; 46: 323-30. Lewis JCM, Keep PA. Relationship of serum CEA levels to tumour size and CEA content in nude mice bearing colonic tumour xenografts. Br J Cancer 1981; 44 381-7. Searle F, Bagshawe KD, Begent RHJ, el al. Radioimmuno- localisation of turnours by external scintigraphy after administration of I 3 l I antibody to carcinoembryonic antigen. Nuclear Med Commun 1980; 1: 131-9. Green AJ, Begent RHJ, Keep PA, Bagshawe KD. Analysis of radioimmunodetection of tumours by the subtraction technique. J Nucl Med 1984; 25: 96-100. Mach J-P, Vienny H, Jaeger P, Haldemann B, Egely R, Pettavel J. Long-term follow-up of colorectal carcinoma patients by repeated CEA radioimmunoassay. Cancer 1978; 42: 143947. Moertel CG, Schutt AJ, Go VLW. Carcinoembryonic antigen test for recurrent colorectal carcinoma. Inadequacy for early detection. J Am Med Assoc 1978; 239 1065-6. Attiyeh FF, Stearns MW. Second-look laparotomy based on CEA elevations in colorectal cancer. Cancer 1981; 4 7 2119-25. Wood CB, Ratcliffe JG, Burt RW, Malcolm AJH, Blumgart LH. The clinical significance of the pattern of elevated serum carcinoembryonic antigen (CEA) levels in recurrent colorectal cancer. Br J Surg 1980; 67: 468 . Martin EW, Cooperman M, King G, Rinker L, Carey LC, Minton JP. A retrospective and prospective study of serial CEA determinations in the early detection of recurrent colon cancer. Am J Surg 1979; 137: 167-9.
This is in keeping with the previous finding that a raised serum CEA value is not necessary for positive RILZ and may permit resection of recurrence at an earlier stage.
The proportion of patients likely to benefit from surgery for recurrent colorectal cancer is small but RIL appears to have a part to play in their selection. Patients at high risk of recurrence with no rise in serum CEA concentration may also be investigated by RIL. We have already located and resected recurrent tumour in two such patients. The earlier recurrence is detected the higher the proportion resectable is likely to be”. Perhaps more important in the long term is the possibility that earlier detection by RIL will give favourable circumstances for new systemic therapies as they are developed.
Acknowledgements We are grateful for the assistance ofour colleagues in the Departments of Medical Oncology, Surgery and Radiology at Charing Cross Hospital. We are indebted to the late Mr Louis de Jode for his support.
This work was supported by the Cancer Research Campaign and the Medical Research Council.
References 1. Goldenberg DM, DeLand F, Kim E et al. Use of radiolabelled
antibodies to carcinoembryonic antigen for the detection and localization of diverse cancers by external photoscanning. New Engl J Med 1978; 298: 1384-8. Goldenberg DM, Kim EE, Bennett SJ, Nelson MO, DeLand FH. Carcinoembryonic antigen radioimmunodetection in the evaluation of colorectal cancer and in the detection of occult neoplasms. Gastroenterology 1983; 84: 524-32. Dykes PW, Hine KR, Bradwell AR et al. Localisation of tumour deposits by external scanning after injection of radiolabelled anti- carcinoembryonic antigen. Br Med J 1980; 280 22G22. Mach J-P, Carrel S, Forni M, Ritschard J, Donath A, Albert0 P.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Paper accepted 26 June 1985
Br. J. Surg., Vol. 73, No. 1, January 1986 67