radiation treatment for breast cancer - gp cme south/thurs_boardroom_0835... · radiation treatment...
TRANSCRIPT

Radiation Treatment for Breast Cancer
Melissa James
Radiation Oncologist
August 2015
OUTLINE
• External Beam Radiation treatment.
(What is Radiation, doctor?)
• Role of radiation.
(Why am I getting radiation, doctor?)
• Radiation Scheduling.
(How often will I be going in?)
• Side effects of Radiation
(Will it burn me, will I glow I the dark?)
• What is new in Radiation?

BACKGROUND
• Surgery remains the mainstay of treatment for early breast cancer.
• Mastectomy
• Lumpectomy (breast conserving surgery)
• Adjuvant treatments play an important role in preventing relapses and
therefore preventing cancer death:
• Chemotherapy
• RADIOTHERAPY
• Hormone therapy

Radiation: The Process

RADIATION TREATMENT- THE PROCESS
Planning
Planning CT
Breast
treatment

Radiation: The Role

ROLE OF RADIATION IN BREAST CANCER
• Breast conservation
• Post mastectomy
• DCIS
• Palliation

ROLE OF RADIOTHERAPY IN EARLY BREAST CANCER
• Indicated in MOST WOMEN post lumpectomy (Breast
Conservation)
• Post surgery local recurrence 20-30%
• Radiation decreases the risk of tumour recurrence in the remaining
breast tissue
• This translates into a small survival advantage.

BREAST-CONSERVING SURGERY (BCS)
Meta analysis
There were 7300 women with BCS in trials of RT
5-year local recurrence risks (mainly in the conserved breast):
• 7% vs 26% (reduction 19%)
15-year breast cancer mortality risks:
• 30.5% vs 35.9% (reduction 5.4%, SE 1.7, 2p=0.002)
15-year overall mortality risks:
• 35.2% vs 40.5% (reduction 5.3%, SE 1.8, 2p=0.005)
EBCTCG Lancet 2005; 366: 2087-2106

ROLE OF RADIOTHERAPY IN EARLY BREAST CANCER
• Indicated in SOME WOMEN post mastectomy
• Recurrence of breast cancer in chest wall may be catastrophic.
• Chest wall recurrence is frequently associated with metastatic
disease
• Thus prevention of recurrence important

MASTECTOMY AND AXILLARY CLEARANCE: N+VE
Meta analysis
There were 8500 women with mastectomy, axillary clearance,
and N+ve disease in trials of RT
5-year local recurrence risks:
• 6% vs 23% (reduction 17%)
15-year breast cancer mortality risks:
• 54.7% vs 60.1% (reduction 5.4%, SE 1.3, 2p=0.0002)
15-year overall mortality risks:
• 59.8% vs 64.2% (reduction 4.4%, SE 1.2, 2p=0.0009)
• EBCTCG Lancet 2005; 366: 2087-2106
ROLE OF RADIOTHERAPY IN EARLY BREAST CANCER
• Indications for post mastectomy radiation treatment
• 4 or more nodes involved
• T3 (5 cms or larger)
• Close or involved margins
• Other factors
• 1-3 nodes positive considered
• High risk features: lymph vascular space invasion, grade three
ROLE OF RADIOTHERAPY IN DCIS
• DCIS treated with a WLE
• Reduces recurrences by 2/3
• 50% of the recurrences will be further in situ disease
• 50% recurrences will be invasive recurrences
• No overall survival benefit
• Consider for
• High grade
• Large lesions
• Close margins

ROLE OF RADIOTHERAPY IN PALLIATION
• Painful bone metastases (80% will have pain reduction)
• Brain metastases
• Spinal cord compression
• Skin metastases
• Skin/ nodal recurrences
• Bronchial obstruction

SO radiotherapy is a very well established
treatment in breast cancer
Radiation: The
Scheduling
SCHEDULING RADIATION TREATMENT
• Daily Monday to Friday
• Each treatment 15-20 Minutes
• “Beam on time” is for only a few minutes
• Most time is “set up time”
• Treatment duration
• Most commonly 16 fractions (3+ weeks)
• May also have 25 fractions (5 weeks)
HYPOFRACTIONATED RADIATION
• Why the move to shorter treatments for early breast cancer?

META ANALYSIS
Radiation treatment
Hypofractionated treatment
(>2Gy per fraction)
Conventional fractionation
(1.8- 2 Gy per fraction).
James ML, Lehman M, Hider PN, et al. Fraction size in radiation treatment for breast conservation in early breast cancer. Cochrane Database Syst
Rev 2010;(11):CD003860.

HYPOFRACTIONATION
• The meta analysis found no difference in local recurrence rates with shorter
fractionation.
• No difference in long-term cosmesis.
• Less short-term toxicity.
• A SHORTER, MORE CONVENIENT RADIATION SCHEDULE WITH EQUIVALENT
CANCER OUTCOMES

Radiation: The Side
Effects

RADIATION THE SIDE EFFECTS
• Acute (Happen during radiation treatment and
immediately after)
• Skin reaction
• Erythema
• Dry desquamation
• Wet desquamation
• Breast/ Chest wall discomfort
• Lethargy
(No Nausea, hair loss, radioactivity)

RADIATION THE SIDE EFFECTS
Erythema Wet desquamation
RADIATION THE SIDE EFFECTS
• Late (Happen 6 months following the radiation treatment)
• Skin
• Pallor, atrophy, telangiectasia
• Soft tissue
• Fibrosis
• Pulmonary Fibrosis
• Asymptomatic
• Lymphoedema (Only if nodes are treated)
• 10-30%
• Brachial plexopathy (Only if nodes treated)
• <0.1%
• Cardiac toxicity
• Left sided patients
• <1% excess cardiac mortality with modern radiation at 15 years
• Second malignancy (Radiation induced)]
• 1-2:1000 at 10 years
Radiation: What is new in
breast treatment?

WHAT’S NEW IN RADIOTHERAPY?
• Excellent local control and survival rates for early breast
cancer
• Focus of Research is in decreasing the potential toxicity
IMPROVING ACUTE SIDE EFFECTS
• A dressing has been shown to improve rates of wet desquamation in breast cancer
patients receiving radiation treatment1.
• The dressing is called mepitel
• This is being introduced for post mastectomy
patients in Christchurch hospital
1. Radiother Oncol. 2014 Jan;110(1):137-43. doi:
10.1016/j.radonc.2014.01.005. Epub 2014 Jan 30.
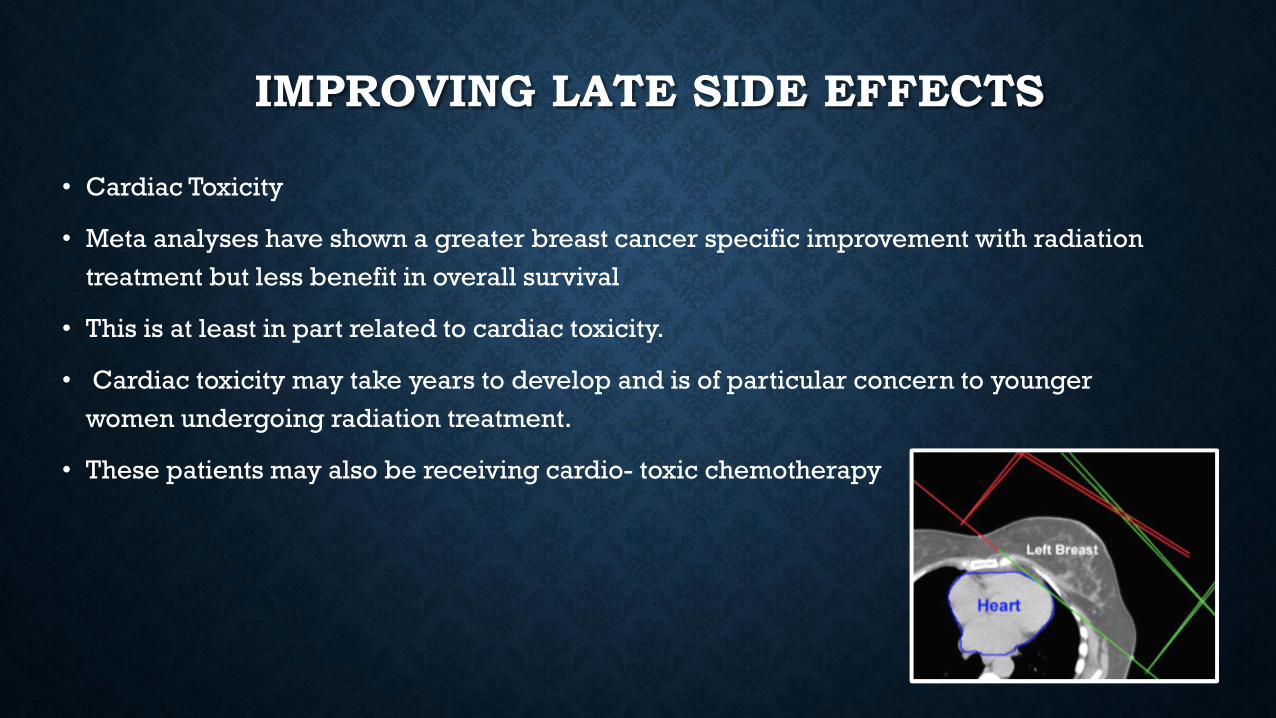
IMPROVING LATE SIDE EFFECTS
• Cardiac Toxicity
• Meta analyses have shown a greater breast cancer specific improvement with radiation
treatment but less benefit in overall survival
• This is at least in part related to cardiac toxicity.
• Cardiac toxicity may take years to develop and is of particular concern to younger
women undergoing radiation treatment.
• These patients may also be receiving cardio- toxic chemotherapy

IMPROVING CARDIAC OUTCOMES IN PATIENTS
• We now are better than ever able to see the heart position and model the dose to the
heart with planning software
• This allows us to shield the heart
• Move the radiation beams to shield the heart
• Set the patient up differently (prone technique)

IMPROVING LATE SIDE EFFECTS
• Deep inspiratory breath hold
• is a method of helping patients to
maintain a good lung expansion,
• which keeps the amount of heart in the
radiation field to a minimum.

MODERN RADIATION TREATMENT FOR BREAST CANCER
•Safe
•Effective

MORE INFORMATION
http://www.targetingcancer.co.nz/