radiation therapy in gynecologic cancer 17-03-15
TRANSCRIPT

RADIATION THERAPY IN GYNECOLOGIC CANCER
K.S.ReddyProfessor of Radiation Oncology
MGMC & RI, Pondicherry
Radiation Therapy in Gynecologic Cancer
Radiotherapy plays a major role
in the treatment of patients with
Gynecological malignancies. Discovery of X-rays & Radioactivity
during the waning years
of 19th Century
Radium, Artificial radionuclides
Biological effects of RT
Radiation therapy was used for
treatment of Various Malignancies
Wilhelm Roentgen(1845-1923)
Marie Curie (1867-1934)

Radiotherapy Machines

Modern Linear Accelerators

Brachytherapy Machines

Radiation therapy is delivered in three ways
1.Teletherapy: X-rays are delivered from a source at distance from the body(External beam radiation therapy)2.Brachytherapy: Radiation sources are put within OR adjacent to the target to be irradiated.(Intra cavitary/interstitial)3.Radioactive Solution: solution that contains isotopes (radioactive colloidal Gold-198 or Phosphorus-32) are instilled in the peritoneal cavity to treat intra peritoneal metastatic nodules/malignant ascitis

The Goal of Radiation Therapy
Maximize tumor cell death while minimizing damage to healthy cells
This goal hasn’t changed in over 50 years!
“There is never any reason to give any dose to
uninvolved normal tissue. An increase in dose to the
tumor will, to a point, improve local control.
Achieving these objectives is self-evidently true and
does not require randomized prospective trials.”

External Beam Radiotherapy
Simple 2-dimentional Radiotherapy3-D Conformal RadiotherapyImmobilization devicesSimulators
2-D simulatorsCT- SimulatorMRI – SimulatorPET-CT- Simulator
Treatment Planning Systems

Intensity Modulated Radiotherapy
(IMRT)
Pelvic RT - treatment of large volumes of
the rectum and small bowel, exposing pts
to gastrointestinal (GI) toxicity
IMRT overcomes this problem by
reducing the dose to the small bowel and
rectum

Intensity Modulated RT (IMRT)
• Novel approach to the planning and
delivery of RT
• Unlike conventional CRT, IMRT conforms
the dose to the shape of the target
tissues in 3D, sparing normal tissues
• Normal tissue Sparing
- ⇓ toxicities ( ⇑ patient quality of life)
- ⇑ Ability to escalate dose
(⇑ tumor control)
• Rapid Arc, VMAT

Emil Grubbe (1875-1960)
Better sparing of small bowel,
bladder and rectum
IMRT
4 Field

Acute GI toxicity
IMRT vs. Conventional RT 100
90
80
70
60
50
40
30
20
10
0Grade 0 Grade 1 Grade 2 Grade 3
IMRT
CRT
Mundt et al. Int J Radiat Oncol Biol Phys 52:1330-1337, 2002

Chronic GI Toxicity
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
0 1 2 3
IMRT
CRT
Mundt AJ, Int J Radiat Oncol Biol Phys 56:1354, 2003

X-ray Mania Recently developed a "Bone Marrow Sparing" IMRT
approach
Lujan AE, Mundt AJ. Int J Radiat Oncol Biol Phys 2003;57:516-521, 2003

Public Demonstration 1902 100% 95% 90% 70% 50%
Isodose lines bend away from BM (crests)

Grade 2 WBC Toxicity
CRT versus IMRT Patients 60%
50%
40%
30%
20%
10%
0%
RT Alone
p = 0.82
RT + Chemo
p = 0.08
Brixey et al. Int J Radiat Oncol Biol Phys 52:1388-93, 2002
CRT
IMRT

LIMITATIONS
Significantly increased expenditure:
– Machine with treatment capability
– Imaging equipment: Planning and Verification
– Software and Computer hardware
Extensive physics-manpower and time required.
Conformal nature – highly susceptible to motion and setup
related errors
Target delineation remains problematic: Interpersonal,
Intrapersonal and Inter-specialists variation in PTV
delineation
Treatment and Planning time both significantly increased
Radiobiological disadvantage:
– Decreased “dose-rate” to the tumor
– Increased integral dose

with good vision today An Important Concern
While IMRT reduces the volume of normal
tissues receiving high doses, it increases the
volume of normal tissues receiving low doses
Raises concern about potential induction of 2nd
cancers
In over a decade of use, however, no
increased rate observed
But all patients need to be carefully followed up

Modern Computer-Controlled But the revolution continues…IGRT

What is IGRT?
Image Guided RT (IGRT) is the use of
real-time imaging to guide RT
Imaging of the patient on the treatment table in
the treatment position
IGRT can be used to:
- Improve setup accuracy of patients
- Manage internal organ motion
- Adapt treatment to changes in patient
anatomy and/or tumor response

multiple electron energies) Why IGRT? Reason 1
Fields are large and
difficult to set up
Accurate setup is
essential due to
proximity of normal
tissues
Cone Beam CT could
improve daily setup
Schefter T et al.
Cervical Cancer: Case Study
IMRT: A Clinical Perspective 2005

1990s Why IGRT?
Reason 2
Organ motion issues
exist, particularly in pts
with an intact uterus
Large CTV-PTV margins
are thus used
IGRT could reduce these
margins, improving
sparing of normal
tissues
Huh et al. (Korea)
Radiother Oncol 2004;71:73

Why IGRT?
Reason 3
Changes occur during
treatment
Treatment plan needs to be adapted to these changes
Dynamic Adaptive RT (DART)

Radiation Oncology
46% ⇓GTV, 18% ⇓ CTV, 9% ⇓ PTV
Re-planning improved rectal sparing
If >30cc GTV reduction, re-planning
improved sparing of the small bowel
Supports for DART concept
GTV
Pre-RT 30 Gy

• Most exciting use of IGRT is the ability to
adapt treatment to changes in the patient
and/or tumor
• Although many tumors shrink over the
course of treatment, it is common to largely
ignore these changes and use a single
treatment plan
• At best, patients are re-planned once
midway through treatment if large changes
occur
Dynamic Adaptive RT (DART)

Brachytherapy
Radioactive isotopes placed close to or with
in the tumor volume
Intra cavitary
Interstitial
Internal : Instillation
Brachytherapy is an integral part of
Radiotherapy in Gynecologic cancer
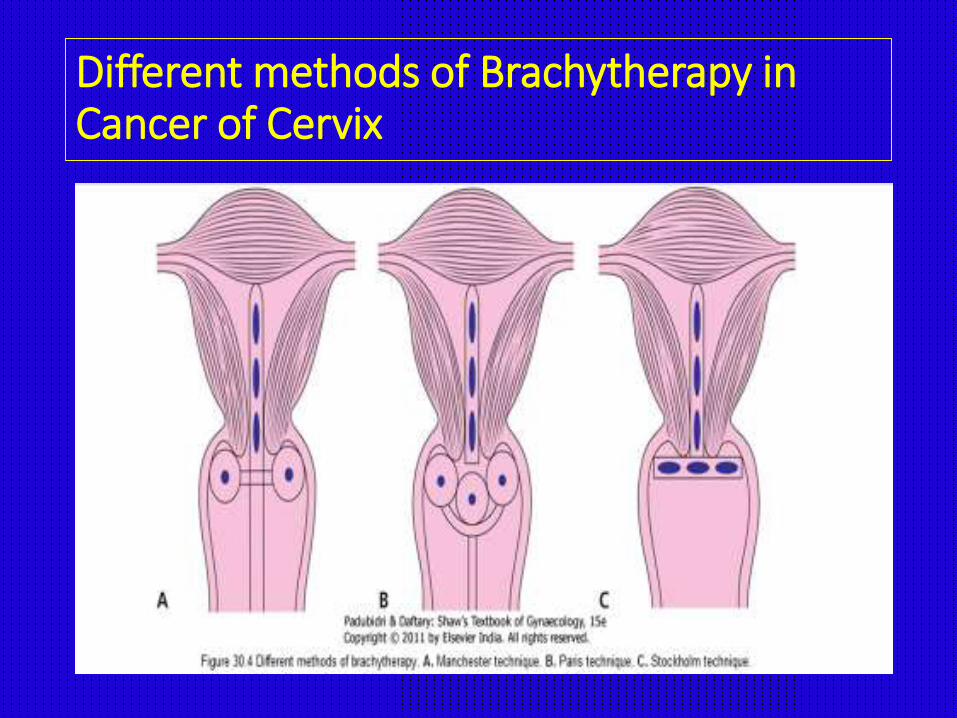
Different methods of Brachytherapy in Cancer of Cervix
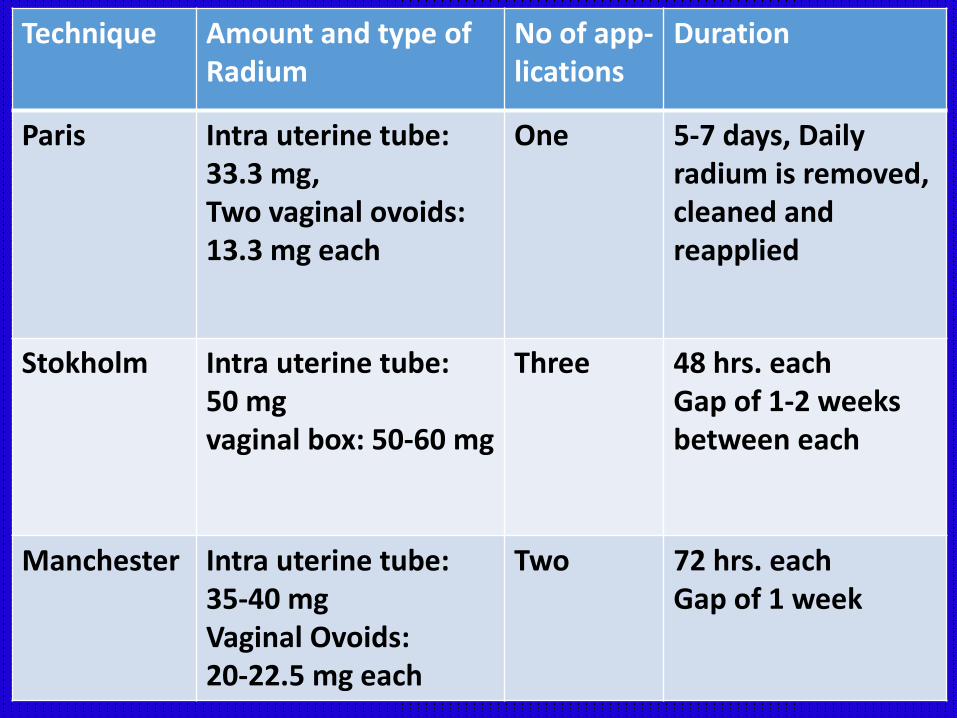
Technique Amount and type of Radium
No of app-lications
Duration
Paris Intra uterine tube: 33.3 mg, Two vaginal ovoids: 13.3 mg each
One 5-7 days, Daily radium is removed,cleaned and reapplied
Stokholm Intra uterine tube: 50 mgvaginal box: 50-60 mg
Three 48 hrs. eachGap of 1-2 weeks between each
Manchester Intra uterine tube: 35-40 mgVaginal Ovoids: 20-22.5 mg each
Two 72 hrs. eachGap of 1 week

Pre-loadedAfter loaded
ManualRemote
-Low dose rate40-200 cGy/hr
-High dose rate>1200 cGy/hr


Intracavitary applicationIsodose distribution

Interstitial implantation
Cervix Vagina

Carcinoma of the Uterine Cervix
•For stage IA1, simple type 1 extrafascialhysterectomy is potentially curative.
•For stage IB1, the procedure of choice is a radical hysterectomy with resection of the parametria and dissection of the pelvic lymph nodes. Para-aortic lymph nodes should be examined and sampled if findings are suggestive of metastatic disease.
•If parametrial extension or regional nodal metastasis is identified intraoperatively, many gynecologic oncologists abort hysterectomy and proceed to pelvic radiotherapy.

Post-op RadiotherapyIn a study by the Gynecology Oncology Group (GOG)
•277 patients had 2 or more of the following riskfactors identified after surgery:
Greater than one third cervical stromal invasion,
Capillary/lymphatic space invasion, and
Large clinical tumor diameter.
•Patients were randomized to receive 46-50Gy of whole-pelvic radiotherapy postoperativelyversus no further treatment.

• Statistically significant (47%) reduction in local recurrence of cervical cancer
• Prolongation in recurrence-free survival.
• However, this occurred at the cost of a 4% increase in grade
3/4 (6% vs 2.1%) toxicity, including 1 patient death.
• Statistically significant improvement in overall survival was
not observed.
• Interestingly, much of the benefit of postoperative radiation
seemed to be confined to non-squamous histologies.
Rotman,Sedlis et al IJROBP, 2006. 65(1):169

Treatment combining chemotherapy with radiotherapy•Traditionally, whole-pelvic radiotherapy alone was offered in this setting, but a randomized trial by GOG, reported by Peters et al. demonstrated a survival advantage for patients who received chemoradiation as compared with radiation therapy alone.
•Post-operative pelvic chemoradiation is recommended for patients with cancers of stage IB1 or higher that are incidentally found after simple hysterectomy for presumed benign disease.

•The addition of concurrent chemotherapy to radiation in the treatment of cervical cancer, both in the postoperative adjuvant setting for early stage disease and as definitive primary therapy for advanced disease, emerged as one of the major breakthroughs in the treatment of gynecologic cancer in the last decade.
•The results of a number of randomized trials showed dramatic survival advantages for chemoradiotherapy versus radiotherapy alone. Meta-analysis would indicate a survival advantage of approximately 30% when chemotherapy is incorporated into treatment.

5 Trials Demonstrating Improved Survival with Chemo-Radiation compared to Radiation Alone
Adapted from: Thomas. NEJM,1999. 340: 1198-1200

•Given these findings, in 1999 the (NCI) National Cancer Institute issued a rare clinical announcement that
“Strong consideration should be given to the incorporation of concurrent cisplatin-based chemotherapy with radiation therapy in women who require radiation therapy for treatment of cervical cancer."

•Treatment of bulky stage I (stage IB2, clinical tumor diameter >4 cm) cervical cancer remains controversial.
•Common treatment strategies consist of primary radical hysterectomy, with postoperative adjuvant chemoirradiation administration tailored to histopathologic findings, or definitive primary chemoradiotherapy. Proponents of definitive primary chemoradiation point to the fact that many (or in some series, most) patients undergoing radical surgery demonstrate surgical-pathologic risk factors that may ultimately require them to receive adjunctive postoperative chemoradiation, with an attendant increase in morbidity.

•Neoadjuvant chemotherapy administration (to reduce tumor volume preoperatively) followed by radical hysterectomy and
•Chemoradiotherapy followed by type I extrafascialhysterectomy are additional treatment strategies that are less-commonly used (endocervical –adeno carcinoma).
•Randomized trials defining the optimal treatment strategy of bulky cervical cancer are not available.
• Regardless of treatment, patients with bulky stage I cervical cancers have significantly higher rates of regional lymph node metastases, locoregional and distant-site relapse, and poor outcome.

Primary chemo-radiotherapy is generally indicated for the management of stage IIB-IVA locally advanced cervical cancer.
Surgical treatment is usually reserved for patients with isolated central pelvic disease that persists or recurs after definitive chemo-radiotherapy.

Treatment combining XRT and brachytherapy
• Comprehensive radiotherapy for stage IB-IVA cervical cancer involves both XRT and brachytherapy. Initial external-beam fields encompass a clinical target volume including the primary tumor and the adjacent areas at risk for direct occult invasion or regional lymph-node metastases.
• For patients with gross disease in the para-aortic nodal region, some believe retroperitoneal lymphadenectomy before XRT can improve the likelihood of disease control.

Cancer of Uterine cervix
Early stage cancer• Stage I-A1: Two intracavitary treatments 65-75 Gy to Point A
Stage I-A2: EBRT 40-45 Gy + ICRT 30-35 GY to Pt ASurvivals are similar to surgery (95-100%)
• Stage I-B1, Non bulky stage II A: EBRT 40-45 Gy + ICRT 40-45 GySurvivals are similar to surgery (85-90%)
(Alternative to surgery in early stage lesions)Adjuvant RT: Post op- High risk group(Ly nodes, Parametria, margins are +ve)EBRT 46-50 Gy + Brachytherapy to proximal 3rd vagina 15 Gy at 0.5 cmSignificant reduction risk of recurrence/progressionSignificant improvement in overall survival
Rotman et al. IJROBP. 2006, 65:169-176

Cancer Cervix-Bulky and advanced cancersStage IB2 to IV A
Concurrent Chemo Radiation• EBRT 45-50 Gy + ICRT 40-45 Gy to Pt.A(total dose
85-90 Gy to PtA)
• Weekly Cisplatin 40 mg/m2 X 6 or
3 weekly Cisplatin+5-FU X 2
• 5 yr survivals reported are
80-85% - Stage I B2/II A
70-80% - Stage II B
50 % - Stage III B
15-20% - Stage IV A
Peters et al.JCO,2000,18:1606-1613; Randal et al. IN Principles & Practice of Gynecologic Oncology 4th ed, 2005

Carcinoma of the Uterine Corpus
•When hysterectomy is medically contraindicated, primary radiotherapy can offer 5-year disease-specific survival rates of 80-90%, approaching those achieved with surgery.
•Indications for adjuvant radiation after surgery for endometrial cancer are somewhat controversial.
•Whole-pelvis external-beam radiotherapy (EBRT) and intravaginal brachytherapy are potential adjuvant postoperative therapies for patients with stage I disease.
•Recommendations are based on the stage and grade of disease.
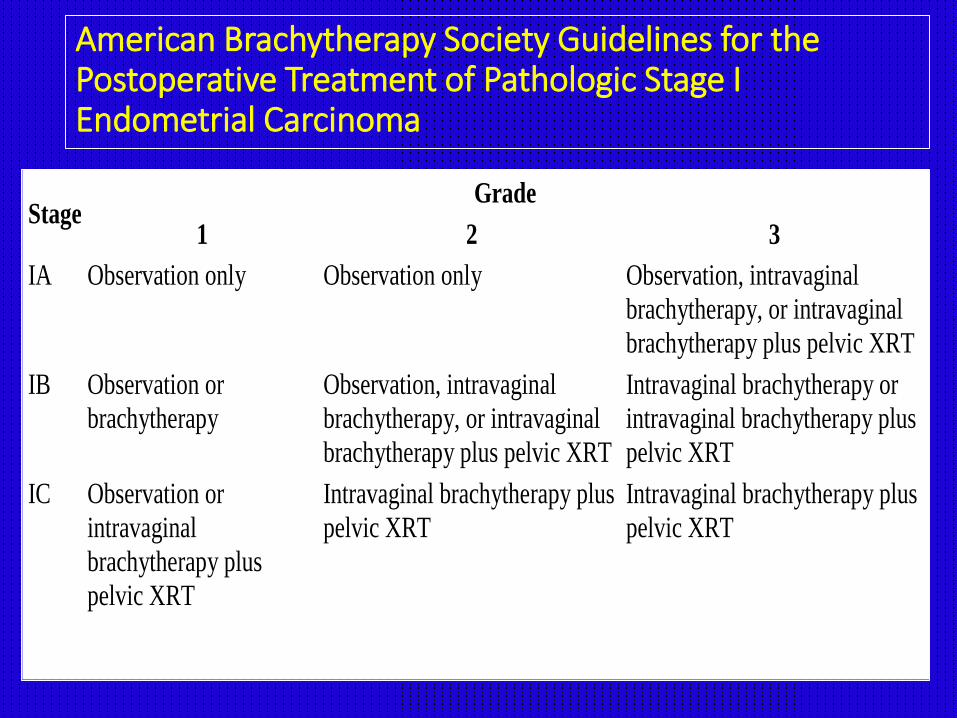
American Brachytherapy Society Guidelines for the Postoperative Treatment of Pathologic Stage I Endometrial Carcinoma
Stage Grade
1 2 3
IA Observation only Observation only Observation, intravaginal
brachytherapy, or intravaginal
brachytherapy plus pelvic XRT
IB Observation or
brachytherapy
Observation, intravaginal
brachytherapy, or intravaginal
brachytherapy plus pelvic XRT
Intravaginal brachytherapy or
intravaginal brachytherapy plus
pelvic XRT
IC Observation or
intravaginal
brachytherapy plus
pelvic XRT
Intravaginal brachytherapy plus
pelvic XRT
Intravaginal brachytherapy plus
pelvic XRT

Several randomized trials have now examined the role of postoperative adjuvant radiation in endometrial cancer.
• The first, a randomized study conducted at the Norwegian
Radium Hospital,
• In the study, 540 patients with stage I endometrial cancer
were treated between 1968 and 1974 with 6000 cGy of
vaginal radium. These patients were then randomized to
receive no further treatment versus an additional 4000 cGy
of XRT.
• demonstrated a statistically significant reduction in the risk
of vaginal and pelvic recurrence in patients external radiation
treatment compared with those who did not (1.9% vs 6.9%,
respectively)
• No difference in overall 5-year survival.
Alders et al. Obstet Gynecol 56:419-427,1980

Postoperative Radiotherapy in Endometrial Cancer [PORTEC]
•conducted in the Netherlands at numerous radiation oncology centers between 1990 and 1997
• In the study, 715 patients who had undergone hysterectomy for intermediate-risk endometrial cancer were randomized to receive 46 Gy of XRT versus no further treatment. No vaginal brachytherapy was used and routine surgical staging was not performed.
•Radiation reduced locoregional recurrence (4% vs 14%),
•5-year overall survival and cancer-specific death rates were not statistically different in the 2 treatment groups.
Creutzberg et al.:Lancet 355:1404-1411, 2000

Gynecologic Oncology Group, GOG 99
conducted between 1987 and 1995, in which 448 patients with intermediate-risk endometrial cancer were randomized to receive postoperative XRT (50.4Gy) versus no further therapy, the cancer recurrence rate was lower (3% vs 12%)in the radiation group.
•Unlike the PORTEC trial, in which patients with deeply invasive grade 3 tumors were excluded, the definition of intermediate risk for enrollment into the GOG trial included any degree of myometrial invasion of any grade in the absence of lymph node metastases. Patients in the GOG trial underwent routine surgical staging with lymphadenectomy.
Keys et al.:Gynecol Oncol 92:744-751,2004

Brachytherapy
•Although neither GOG 99 nor the PORTEC study incorporated intravaginal brachytherapy, the vaginal cuff is well recognized to be a common site of recurrence in many patients with early stage disease. Therefore, one can extrapolate from these trials when considering adjuvant intravaginal brachytherapy in lieu of whole-pelvis irradiation. Intravaginal brachytherapy may be administered with an after loading device (LDR) or (HDR).

•The HDR technique has become popular because of its convenience as a well-tolerated outpatient regimen.
•When intravaginal brachytherapy is given after pelvic XRT, a typical dosage schedule for intravaginal brachytherapy is 15 Gyprescribed to a depth of 0.5 cm over 3-4 cm of the upper vagina, given in 3 weekly fractions of 5 Gy each.
•When intravaginal brachytherapy is administered without pelvic XRT, a dose of 21 Gy to a depth of 0.5cm given in 3 fractions is commonly prescribed.

Additional considerations• Two important pathologic findings not specifically addressed in
the FIGO/AJCC staging system are extensive invasion of the lymphovascular space and a close (less than a few millimeters) margin of resection. When either feature is found, consideration of postoperative radiotherapy is warranted. Also, adjuvant treatment should be considered in certain patients with pathologic stage I disease in whom surgical staging was incomplete.
• For stage II endometrial carcinoma, preoperative or postoperative radiotherapy may be administered. The goals of preoperative treatment are to facilitate hysterectomy by reducing tumor bulk, by clearing microscopic infiltration from the upper vaginal mucosa, or by rendering cells incapable of local implantation. Pelvic XRT may be combined with brachytherapy in this setting.
• For stage II disease recognized during postoperative histopathologic analysis, pelvic XRT and intravaginal brachytherapy may be indicated.

Stage III-IV endometrial cancer
• For stage III-IV disease, numerous institutions have reported outcomes for patients treated with combinations of pelvic XRT, whole-abdomen radiotherapy (WAR), intravaginal brachytherapy, and chemotherapy; however, no clear consensus has emerged.
• A study (GOG 122) comparing WAR with combination chemotherapy involving doxorubicin and cisplatin to treat advanced endometrial carcinoma found that chemotherapy was apparently the more effective treatment.
• Of 396 assessable patients, 202 were randomized to receive WAR and 194 to receive chemotherapy. At 60 months, 50% of patients who received chemotherapy were predicted to be alive and disease-free as compared with 38% of patients who received radiotherapy, a survival advantage that reached statistical significance.
• Treatment was thought to have contributed to the death of 8 patients (4%) treated with chemotherapy and 5 patients (2%) treated with radiation.
Randall et al.: J Clin Oncol 24: 36-44, 2006

Histological variants of Endometrial carcinoma
•Uterine papillary serous cancer (UPSC) is characterized by a propensity for local and distant recurrence.
•Carcinosarcoma, formerly called Malignant Mixed Müllerian Tumor (MMMT), is associated with a particularly high rate of pelvic failure after hysterectomy.
•Patients may benefit from postoperative pelvic XRT in all stages of disease.

Vaginal Cancer
• Primary nonsurgical treatment is usually preferable for stage I or II vaginal lesions, partial or total vaginectomyfollowed by postoperative radiotherapy is sometimes feasible for these.
• Combined treatment with RT+Cisplatin is likely to be more beneficial than RT alone because the biologic behavior of vaginal cancer is expected to be similar to that of cervical cancer.
• After EBRT is administered to fields in doses of 45-50 Gy
• Tailored interstitial brachytherapy is generally necessary to deliver potentially curative doses of radiation to the primary site.

Vulvar cancer• The aim of integrated multimodality therapy including
surgery, chemo-radiotherapy is to reduce the risk of local, regional failure in patients with advanced primary or distant nodal involvement.
• To obviate the need of exenteration in women having urethra , anal extension of cancer.
• The dose of radiation given is 45-50Gy with microscopic and 60-64Gy with macroscopic disease.
• Pre operative Interstitial implant(60 Gy in 6 days) shrinks the tumor and facilitates extirpation of tumor at later date .
• Post operative radiotherapy is preferred in women with +ve inguinal nodes.

Ovarian Cancer
• Whole-abdomen radiation (WAR) was used, but its popularity has waned because of the favorable toxicity profiles of current chemotherapeutic regimens.
• Techniques for WAR have included AP-PA field treatment to the entire peritoneal cavity at doses of 25-30Gy given in fractions of 1-1.5 Gy.
• Renal doses of less than 20Gy and whole-liver doses of less than 30Gy were advisable using shielding techniques.
• Boost treatment to the pelvis and para-aortic lymph nodes may be combined with WAR for total doses of 45-50 Gy to these regions. Unfortunately, small bowel obstruction several years following WAR was a common complication.
Palliative radiotherapy
• Palliative radiotherapy is frequently offered to patients who have focally symptomatic recurrences of ovarian cancer.
• For patients with painful or hemorrhagic pelvic masses refractory to chemotherapy, a hypofractionated schedule of 14.8Gy given in 4 fractions within 2 days may be administered by using AP-PA fields and then repeated once or twice at 2- to 4-week intervals.
• Three monthly fractions of 10Gy are also reasonable, especially in patients with poor performance and a limited life expectancy in whom convenience and expediency are paramount.

Radiotherapy in choriocarcinoma
Though the tumor is radiosensitive, RT is usually not used in the management as
Chemotherapy is highly effective
Radiation is reserved for
Metastases to CNS, Spinal Cord or Liver

Radiotherapy in hormonal ablation
• Tamoxifen is widely given to premenopausal women with estrogen receptor–positive breast cancer.
• However, low-dose radiotherapy is sometimes administered.
• Radiotherapy can be highly effective and cost-effective.
• A dose of 10-20Gy in 5-10 fractions is usually sufficient to eliminate ovarian hormone production.
• To limit the size of the radiotherapeutic field, the location of the ovaries is ideally verified by performing Ultrasound/CT scanning.