radiation therapy for prostate cancer - denver, colorado · radiation therapy for prostate cancer...
TRANSCRIPT
Radiation Therapy for Radiation Therapy for Prostate CancerProstate Cancer
Amy Amy HouHou, MD, MDResident Resident –– Dept of UrologyDept of Urology
General Surgery Grand RoundGeneral Surgery Grand RoundNovember 24, 2008November 24, 2008
External Beam RadiationExternal Beam Radiation

Advances Improving TherapyAdvances Improving Therapy
•• Generation of linear accelerators and Generation of linear accelerators and conformational techniques allowing conformational techniques allowing delivery of high doses of radiation deep delivery of high doses of radiation deep into pelvis while respecting normal tissue into pelvis while respecting normal tissue surrounding targetsurrounding target
•• Image guided techniques allowing for Image guided techniques allowing for placement of radioactive sources directly placement of radioactive sources directly into prostate, versus freeinto prostate, versus free--handhand
TechniqueTechnique
•• CT scan of pelvis in treatment positionCT scan of pelvis in treatment position•• Planning target volume (PTV)Planning target volume (PTV)
–– Prostate +/Prostate +/-- seminal vesicleseminal vesicle–– Margin of 0 to 4Margin of 0 to 4--6mm or more around the 6mm or more around the
prostateprostate•• Smaller margin on rectal side, due to fear of rectal Smaller margin on rectal side, due to fear of rectal
toxicitytoxicity
–– Definition of rectal length/ volume variesDefinition of rectal length/ volume varies

Conventional radiation therapy treatment portal (A). Prostate location inferred from the foley balloon, bladder and wire anal marker.
Conformal radiation therapy treatment portal (B). 3D prostate reconstructed from planning CT scan.
IMRTIMRT
•• Conformal dosing to the prostateConformal dosing to the prostate•• During each beam angle, a part of the During each beam angle, a part of the
radiation field is blocked at a specified radiation field is blocked at a specified time to optimize treatment to prostate but time to optimize treatment to prostate but limit dose to surrounding structureslimit dose to surrounding structures
•• At any given time, multiple beams At any given time, multiple beams consecutively fired and converging on consecutively fired and converging on target organtarget organ


PSA BouncePSA Bounce
•• 964 men treated with full dose EBRT 964 men treated with full dose EBRT alone for localized prostate cancer at MD alone for localized prostate cancer at MD AndersonAnderson
•• PSA bounce defined as initial increase in PSA bounce defined as initial increase in serum [PSA] >= 0.5ng/ml, with return to serum [PSA] >= 0.5ng/ml, with return to prepre--bounce baseline serum PSA no more bounce baseline serum PSA no more than 60mo after EBRTthan 60mo after EBRT
PSA Bounce PSA Bounce -- ResultsResults
•• 12% (119 pts) with PSA bounce, mean 12% (119 pts) with PSA bounce, mean time 18months after treatmenttime 18months after treatment–– No pretreatment factors or radiation dose No pretreatment factors or radiation dose
could predict PSA bouncecould predict PSA bounce–– Had significantly higher biochemical diseaseHad significantly higher biochemical disease--
free survival than those without bounce free survival than those without bounce (p=0.0001)(p=0.0001)
•• 34.3% (334pts) with biochemical 34.3% (334pts) with biochemical recurrence at median of 21 months after recurrence at median of 21 months after treatmenttreatment
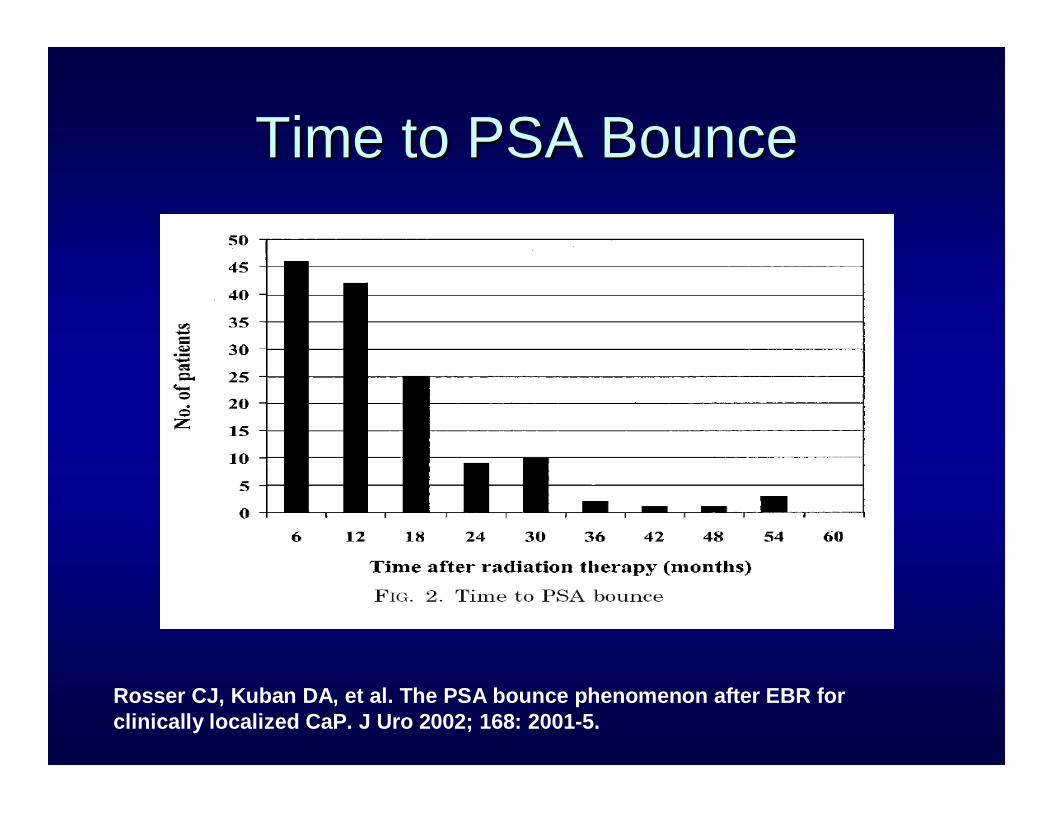
Time to PSA BounceTime to PSA Bounce
Rosser CJ, Kuban DA, et al. The PSA bounce phenomenon after EBR for clinically localized CaP. J Uro 2002; 168: 2001-5.

Dutch Multicenter Dose Dutch Multicenter Dose Escalation TrialEscalation Trial
•• Randomized, multicenter trial looking at Randomized, multicenter trial looking at dose escalation of EBRT for localized dose escalation of EBRT for localized prostate cancerprostate cancer
•• 669 patients between 1997669 patients between 1997--20032003•• Median 70month Median 70month followupfollowup in 68Gy in 68Gy vsvs
78Gy radiotherapy78Gy radiotherapy•• Neo/adjuvant hormone therapy allowedNeo/adjuvant hormone therapy allowed
–– Balanced between both treatment armsBalanced between both treatment arms

78Gy 78Gy vsvs 68Gy68Gy•• Primary endpoint: Freedom from failure, Primary endpoint: Freedom from failure,
clinical and biochemicalclinical and biochemical–– ASTRO BF definitionASTRO BF definition –– 3 consecutive 3 consecutive –– rises in PSArises in PSA–– Phoenix BF definition Phoenix BF definition –– nadir PSA + 2mg/Lnadir PSA + 2mg/L
•• Better 7year freedom from failure rates with Better 7year freedom from failure rates with 78 78 GyGy by both definitionsby both definitions–– ASTRO: 54% ASTRO: 54% vsvs 47%, p = 0.0447%, p = 0.04–– Phoenix: 56% Phoenix: 56% vsvs 45%, p = 0.0345%, p = 0.03
•• No statistically significant difference in FFCF No statistically significant difference in FFCF and overall survivaland overall survival

Complications Complications --78 78 GyGy vsvs 68 68 GyGy
•• Grade 2 or greater GU toxicityGrade 2 or greater GU toxicity–– Incidence similar in the two armsIncidence similar in the two arms
•• 40% 40% vsvs 41%, p = 0.0641%, p = 0.06
–– Gardner et al demonstrated a 59% GU toxicity Gardner et al demonstrated a 59% GU toxicity rate in a 15year rate in a 15year followupfollowup
•• Grade 2 or greater GI toxicityGrade 2 or greater GI toxicity–– Cumulative incidence greater in 78 Cumulative incidence greater in 78 GyGy armarm
•• 35% 35% vsvs 35%, p = 0.0435%, p = 0.04
–– Rectal bleeding and fecal incontinence 2x Rectal bleeding and fecal incontinence 2x more commonmore common

Al-Mamgani A, et al. Update of Dutch multicenter dose-escalation trial of radiotherapy for localized CaP. Int J Rad Onc Biol Phys 2008; 72(4): 980-88.

Complications of Radiation Therapy
• GU (56% (MGH))– Urethral stricture– Total incontinence– Bladder cancer
(5.6%)*– Continues over time– 13% of patients with
acute urinary toxicity eventually developed chronic urinary toxicity vs 5% who did not
• GI– Proctitis– Fecal incontinence– GI bleed– Secondary GI cancer

Nieder AN, et al. Radiation therapy increases risk of bladder and rectal cancer. J Uro2008; 180: 2005-10.


BrachytherapyBrachytherapy
•• Insertion of radioactive implantsInsertion of radioactive implants•• Via TRUS (Holm 1983), CT (Via TRUS (Holm 1983), CT (KoutrevelisKoutrevelis
1998) or MRI (D1998) or MRI (D’’Amico 1998)Amico 1998)•• Under US visualization, 17 or 18Under US visualization, 17 or 18--gauge gauge
needles inserted through template into needles inserted through template into prostateprostate–– Metallic seeds containing radioactive isotope Metallic seeds containing radioactive isotope
deployed as needles withdrawndeployed as needles withdrawn
Walsh, Retic,Vaughan, Wein, eds. Campbell’s Urology, 8th ed. 2002

Prostatic Template:Prostatic Template:TransperinealTransperineal
•• As described by As described by PuthawalaPuthawala::–– 2 concentric rings with radii of 12 concentric rings with radii of 1--2cm2cm–– 66--12 guide holes12 guide holes–– Up to 18 metallic source guides, 17gauge, Up to 18 metallic source guides, 17gauge,
20cm long20cm long–– Tips of guides usually 1cm above bladder Tips of guides usually 1cm above bladder
neckneck–– Template fixed to perineum by 0Template fixed to perineum by 0--0 silk suture0 silk suture
Gunderson LL, Tepper JE, eds. Clinical Radiation Oncology, 2nd ed. Elsevier 2007.

Prostatic ImplantsProstatic Implants
•• Permanent Iodine 125Permanent Iodine 125•• Palladium 103 implantsPalladium 103 implants
–– Shorter t1/2 Shorter t1/2 vsvs II--125 125 –– 17days 17days vsvs 60days60days–– Lower energy Lower energy –– 21KeV 21KeV vsvs 27KeV27KeV
•• Means slightly lower tissue Means slightly lower tissue penetrancepenetrance, made , made insignificant if seed to seed distances are 1.7cm or insignificant if seed to seed distances are 1.7cm or lessless

Patient placed in high lithotomy position with transrectal ultrasound probe fixed to the stepper device. Needle containing radioactive seeds inserted transperineallyvia a grid.
Walsh et al. Campbell’s Urology, 9th ed.
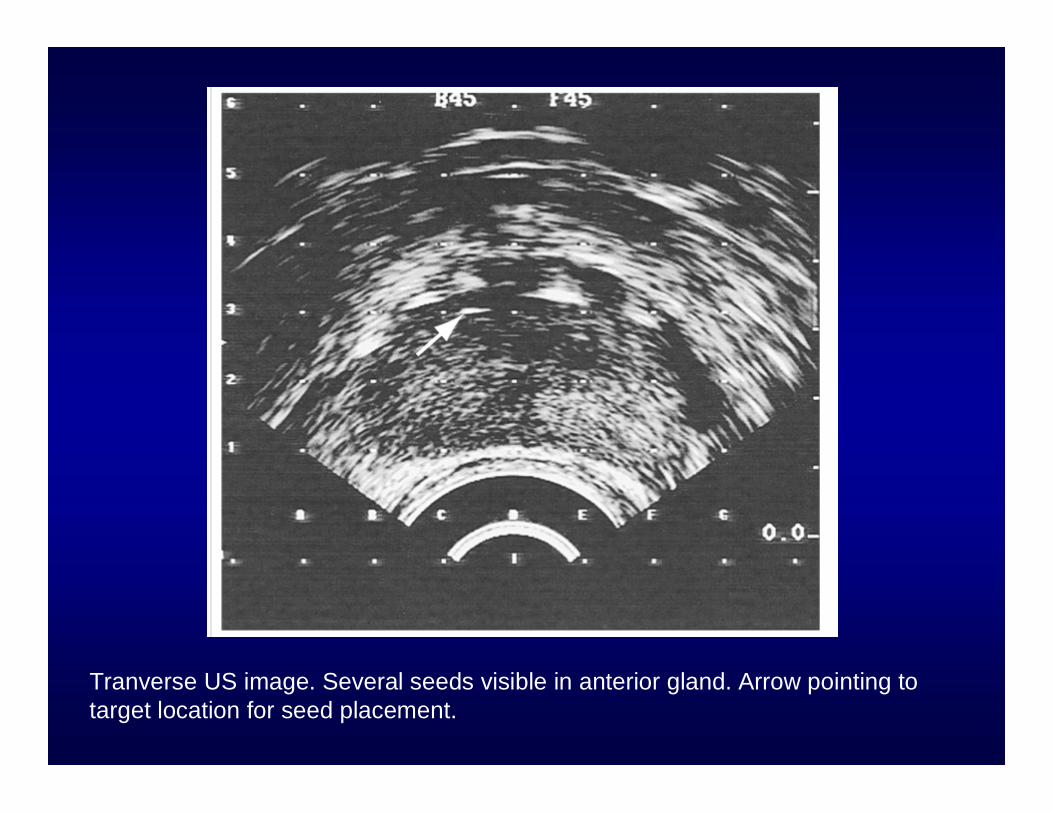
Tranverse US image. Several seeds visible in anterior gland. Arrow pointing to target location for seed placement.

Parasagittal US image. Arrow demonstrates needle depth goes to the prostatic capsule before deploying radioactive seeds.

Intraoperative fluoroscopic image of the prostate demonstrating placement of palladium 103 seeds.

ToxicititiesToxicitities
•• UrinaryUrinary–– 37% with grade I toxicity 37% with grade I toxicity
in 1in 1stst 60 days60 days–– 68% resolution of grade 68% resolution of grade
II toxicity at 36moII toxicity at 36mo–– 11--5% require CIC5% require CIC–– 22--3% overall significant 3% overall significant
urinary obstruction urinary obstruction (refractory to medical (refractory to medical mgmt) mgmt) s/ps/p brachytherapybrachytherapy
•• RectalRectal–– 11--4% minor rectal 4% minor rectal
bleedingbleeding–– Rate of toxicity related to Rate of toxicity related to
dose and length of rectal dose and length of rectal wall receiving dosewall receiving dose
•• WallnerWallner (1995): keep (1995): keep rectal dose to 85% of rectal dose to 85% of prescribed doseprescribed dose
PotencyPotency
•• ZelefskyZelefsky reported improved rates of reported improved rates of potency over EBRT potency over EBRT **
–– 53% 53% vsvs 43% (p= 0.52)43% (p= 0.52)•• Rate of potency decreases with longer Rate of potency decreases with longer
followupfollowup–– 50% of potent men pre50% of potent men pre--treatment will be treatment will be
potent 6 years postpotent 6 years post--treatmenttreatment
Zelefsky MJ, et al. Comparison of 5yr outcome and morbidity of 3DCR vs transperineal permanent I-125. J Clin Oncol 1999; 17:517-22.
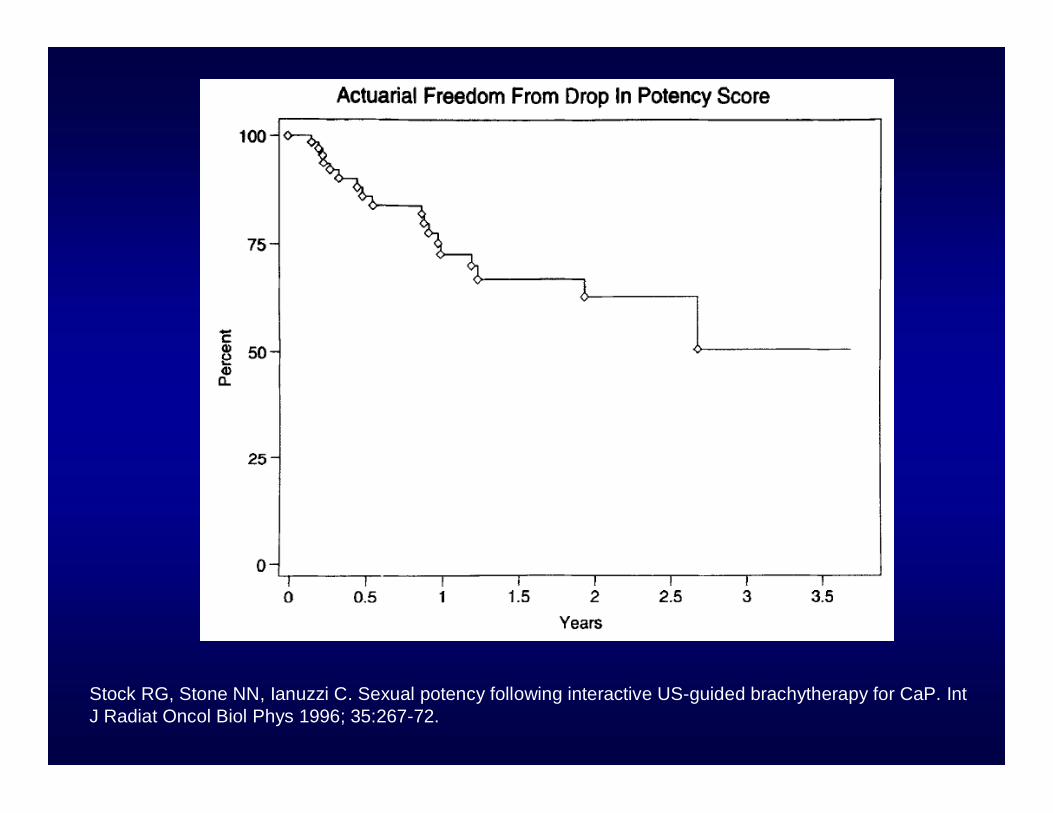
Stock RG, Stone NN, Ianuzzi C. Sexual potency following interactive US-guided brachytherapy for CaP. IntJ Radiat Oncol Biol Phys 1996; 35:267-72.
Comparison of treatments
• Cleveland Clinic, Kaiser Permanente– Looked at 5 year biochemical relapse free
survival– T2b, T2c, gleason 7- intermediate risk CaP– Open prostatectomy, laparoscopic
prostatectomy, EBRT, or brachytherapy– 79.9% vs 60.2% vs 85.7 % vs 89.5%
(p<0.0001)
Vassil AD, et al. A comparison of BRFS and initiation of salvage therapy in patients with intermediate risk CaP treated with open RP, lap RP, EBRT or PSI. IJ Rad Onc Biol Phys 2008; 72(1): s286.