radiation breast oncology highlights of sabc 2006
TRANSCRIPT

Radiation Breast Oncology Highlights of SABC 2006
Alison Bevan, MD PhD UCSF Radiation Oncology
January, 2007

TopicsI. Updates
a. Evaluating the impact of adjuvant radiation in older women with ER+ ESBC on Tamoxifen (# 11)b. Who needs a boost? Defining radiation dose (#10)c. MammoSite TM (ASTRO #52)
II. Newa. DCIS: Who can avoid RT (#29)b. EBCTCG Meta-Analysis (ASTRO #4, SABC #40) )
IV. Conclusions
• Ongoing
• Conclusions

Radiation dose: who needs a boost to decrease LRR?
• Whole breast radiotherapy is delivered over 5 to 6 weeks.
• Boost is delivered over the last 5-8 days to the tumor
bed
• Cost from patient’s point of view: time and toxicity
• Prior to EORTC trial, no guidelines

EORTC Boost TrialBartelink, H., et al. NEJM, 2001
• >5500 patients with stage I&II• 50Gy (5 weeks) ± 16Gy boost (8 days) after complete
excision• Systemic therapy decreased LRR (HR .75) but
disappeared in multivariate analysis
P<.0001 Boost No Boost
5y LRR 4.3% 7.3%

EORTC Boost TrialBartelink, H., et al. NEJM, 2001
• Benefit was age-related, particularly important for those younger than 50 years
• No difference in DM, OS
Boost No Boost p value
LRR 4% 7% <.001
<40y 10% 19.5% .002
>60y 2.5% 4% .14

Randomized trial evaluating 10 Gy boost (Lyon Trial)
Romestaing, P et al, JCO 1997
• 1024 women with tumors <3cm with negative margins
5 years Boost No boost
LRR 3.6% 4.5%

Impact of boost on LRR, cosmesis & survival10 year results
Bartelink H et al., EORTC 22881-10882 Abstract #10
• No difference in OS (82%, p.93)• Fibrosis increased with boost 4.4% v 1.6% p<.0001• Cumulative LRR 10% v 6%• All statistically significant
age Boost No Boost Absolute benefit
≤40 13.5% 24% 10.5%
41-50 9% 12.5% 4%
51-60 5% 8% 3%
>60 4% 7% 3%

Impact of boost on LRR, cosmesis & survival10 year results
Bartelink H et al., EORTC 22881-10882 Abstract #10
• Benefit in all ages
• Despite some poor boost techniques
• Is absolute benefit of 3% critical?

Impact of boost on LRR, cosmesis & survival10 year results
Bartelink, H et al., EORTC 22881-10882 Abstract #10
• The boost is very important for young patients <35y and less important with increasing age
• Also incomplete excision arm consisting of 255pts randomized to 10Gy v 26Gy with increased local control (NS) & severe fibrosis
• New studies: microarrays to distinguish pathological features

Early Breast Cancer Trialists Collaborative Group (EBCTCG)
Meta-analysis
1995
Post-operative radiation significantly reduced breast cancer deaths but increased non-breast cancer deaths resulting in no significant improvement survival.
2000
Significant reduction isolated local recurrence and breast cancer mortality with radiation but increase in non-breast cancer deaths with a non-significant benefit overall survival at 20 years.

Effects of radiotherapy and differences in the extent of surgery for early breast cancer on local recurrence and 15 year survival: An
overview of the randomized trials
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG)
Lancet 366: 2087-2106, 2005ASTRO abstract #4, 2006SABC abstract #40, 2006

EBCTCG: local therapies
No. Trials No. women
Total (by 1995) 78 42,080
CS +/- RT 10 7,311
Mastectomy +/- RT 36 16,177
Mastectomy vs. CS +/- RT 11 6,615
Nodal surgery vs. RT 9 4,550
Nodal surgery vs. none 8 2,502
RM vs. MRM 4 4,925

EBCTCG: endpoints for trial comparison
• 5 year isolated LRR (75% occurred within 5 years)
• 15 year breast cancer mortality
• 15 year all cause mortality

EBCTCG: breast cancer specific
survival benefit at 15 years Trials with <10% absolute difference in 5 year isolated
local-regional recurrence15 year breast cancer mortality benefit 1%(M±RT N-, MRM v RM, M v CS+R)
Trials with 10-20% absolute difference15 year breast cancer mortality benefit 4.5%(CS±R n-, M ±R n+, axillary dissection v no axillary treatment)
Trials with >20% absolute difference15 year breast cancer mortality benefit 6%(CS ±R n+, M without axilllary dissection ±R n+)

EBCTCG: BCS trials
• Radiotherapy After BCS, 10 trials with 7311 women
RT No RT absolute benefit
5y LRR 7% 26% 19%
15y breast ca mortality 30.5% 35.9% 5.4%
Overall mortality reduction 5.3%

LRR
N016%
N+30%
EBCTCG: BCS & RT
5%
7%
15y absolute survival benefit
(Mastectomy N+ 5%)

EBCTCG: local therapy comparisons
For the women who received adjuvant systemic therapy:
5y isolated LRR
No Systemic therapy 28%
Systemic therapy 8%
15y reduction breast ca mortality 6%
Better local treatment adds to the effects of systemic therapy on LR and breast cancer mortality

EBCTCG: local therapy comparisons
5 yr. Isolated Loc-reg Node - Node +
Decrease breast cancer mortality 15 yr.Node - Node +
Mastectomy +/- RT Mastectomy Mastectomy + RT
6% 23% 2% 6% +4% - 5%
Mastectomy, CS+RT Mastectomy CS+RT
5% 8% 9% 5% +1% -2%
CS +/- RT CS CS + RT
23% 41% 7% 11% -5% - 7%

EBCTCG: toxicity & OS
Radiotherapy was associated with a significant increase in contralateral breast cancer at 15 years (7.5% vs. 9.3%)
Radiotherapy was associated with a significant increase in non-breast cancer deaths at 15 years (14.6% vs. 15.9%)
The excess mortality was primarily from heart disease and lung cancer

EBCTCG: local therapy comparisons
Rule of 4
Proportional relationship between effects on local control and breast cancer mortality:
“One breast cancer death (in the absence of any other causes of death) would be avoided for every 4 local recurrences prevented.”
4:1 local recurrence benefit/breast cancer survival benefit

EBCTCG: local therapy comparisons
Rule of 4
For example: LRR without RT 26%LRR with RT 10%
Absolute benefit = 16% at 5 years then survival benefit 4% at 15 years

Lumpectomy + Tamoxifen with & without XRT for Women ≥70 years with Early Stage Breast Cancer
Hughes, KS et al. CALGB 9343, RTOG, ECOG Abstract #11
• 8.2 year follow-up (5yr NEJM, 2004)
• About 200pts in each group had no axillary exploration
≤2cm, cN0, ER+
TamRT Tam
≥70 years
Lumpectomy (631pts)

Lumpectomy + Tamoxifen with & without XRT for Women ≥70 years with Early Stage Breast Cancer
Hughes, KS et al. CALGB 9343, NEJM, 2005
5 year TamRT Tam p value
LRR 1% 4% p<0.0001
OS 87% 86% p=0.94
FFDM 99% 98% p=0.97
Mastectomy Free
99% 98% p=0.15

Lumpectomy + Tamoxifen with & without XRT for Women ≥70 years with Early Stage Breast Cancer
Hughes, KS et al. CALGB 9343, RTOG, ECOG Abstract #11
8.2 years TamRT Tam p value
LRR 1% (4) 7% (23) <.001
In-breast 1% (4) 6.3% (20) sig
Axillary rec 0 1.2%(4) sig
Mastectomy rate 1% 3% NS
Distant mets 3% 3% NS
BSS 2% 2% NS
Mortality 27% 26% NS

Lumpectomy + Tamoxifen with & without XRT for Women ≥70 years with Early Stage Breast Cancer
Hughes, KS et al. CALGB 9343, RTOG, ECOG Abstract #11
• Absolute LRR difference of 5-6%
• No statistical difference in mastectomy rate, distant metastases, BSS, OS
• Cosmesis inferior in TamRT arm
• No thromboembolic events
• Conclusion: reasonable option for some patients
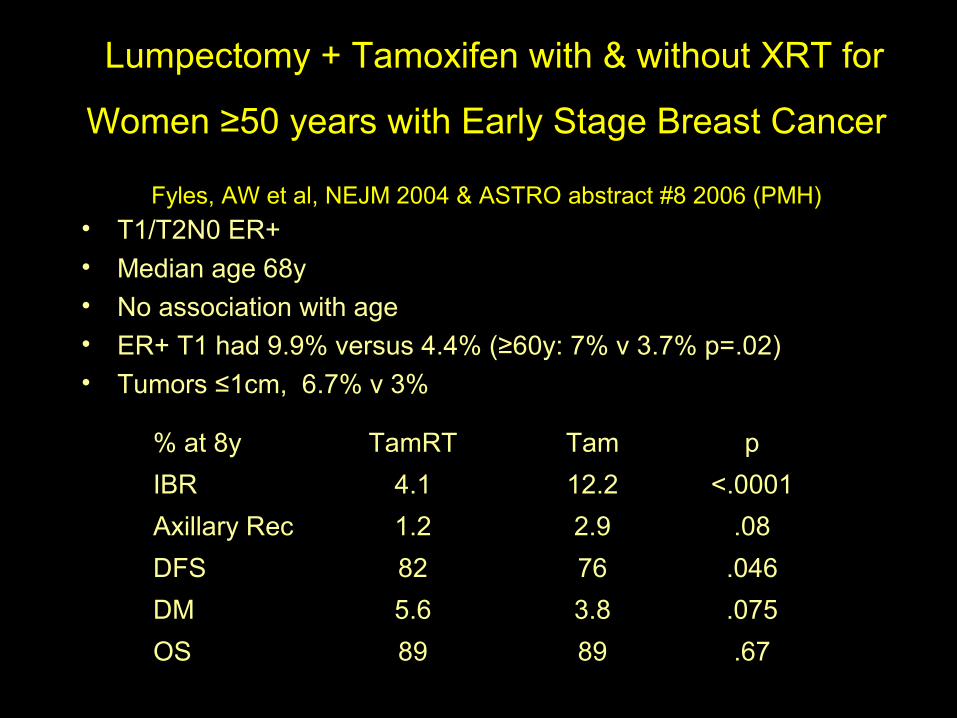
Lumpectomy + Tamoxifen with & without XRT for
Women ≥50 years with Early Stage Breast Cancer Fyles, AW et al, NEJM 2004 & ASTRO abstract #8 2006 (PMH)
• T1/T2N0 ER+• Median age 68y• No association with age• ER+ T1 had 9.9% versus 4.4% (≥60y: 7% v 3.7% p=.02)• Tumors ≤1cm, 6.7% v 3%
% at 8y TamRT Tam p
IBR 4.1 12.2 <.0001
Axillary Rec 1.2 2.9 .08
DFS 82 76 .046
DM 5.6 3.8 .075
OS 89 89 .67

Comparison of Trials
author years characteristics LRR
Hughes 8 ≥70, T1 ER+ cN0 7% v 1%
Fyles 8 ≥60, T1 ER+ cN ± 9.9% v 4.4%
Veronesi 10
Quad, ±N, ≤2.5cm>65≤70 56-65
(low numbers n=80, 25)
4.4% v 4%12.1%v 2.4%

Considerations
• Age
• Hormone Receptor +
• Toxicity of Tamoxifen
• Co-morbidities
• Life expectancy
• Patient preference

MammoSiteTM : multi-institutional 2 year experience with ESBCCuttino, LW, et al ASTRO abstract #52
• 9 institutions, 2000-2004
• 483 patients with stage 0, I, II
• In-breast failure in 6 pts, 4 outside lumpectomy site
• Closed cavity placement reduced risk of infection from 9% to 4.8%
• Infection related to overall cosmesis being fair to poor
• Cosmesis good/excellent in 91%

Lumpectomy alone for low risk DCIS 5 year results of intergroup trial E5194
Hughes, L et al., ECOG, NCCTG Abstract #29
• 711 patients with DCIS enrolled from 1997-2002 (29 ineligible)
• Median age 60 years (range 28-88)
• Median f/u was 4.96 years
• Adjuvant Tamoxifen allowed in 2000 (ER status testing routine)
• All pathology reviewed at Vanderbilt University
• 89% acceptable for study after central review (excluded size
<3mm)

Lumpectomy alone for low risk DCIS 5 year results of intergroup trial E5194
Hughes, L et al., ECOG, NCCTG Abstract #29
DCIS
Group I Group II
Lumpectomy (711 pts)
Low/int grade <2.5cm High grade <1cm
Observation30% Tamoxifen
Post-op mammogram clear for calcificationsMargins>3mm

Lumpectomy alone for low risk DCIS 5 year results of intergroup trial E5194
Hughes, L et al., ECOG, NCCTG Abstract #29
Low-Int grade(580 pts) •median tumor size 6mm •18% >1cm. •median margin 5-10mm. •31% declared intention for
TAM
High grade (102 pts) •median tumor size 7mm•Median margin 5-10mm •30% declared intention to take
TAM
Ipsi breast events
13.7%6.8%
50% DCIS and 50% InvasiveContralateral events 3.5% & 4.2%

Lumpectomy alone for low risk DCIS 5 year results of intergroup trial E5194
Hughes, L et al, ECOG, NCCTG Abstract #29
1. Observation is acceptable for rigorously evaluated and selected patients with low to intermediate grade DCIS of the breast
2. For high grade lesions (Grade 3), excision is inadequate
3. Early data, need longer f/u
4. Who got Tam, LRR with grade, age and margins status?

Prospective Study of Wide Excision Alone for DCIS of the Breast
Dana Farber/Brigham and Woman’s CC
• 158 pts, median age 51• ≥1cm margins, Grade 1/2 (50/50), ≤2.5cm by
mammo• No Tamoxifen• Rate of ipsi recurrence was 2.4% per year• 5 year rate of 12%• Closed early--met stopping rules• 84% re-excision, 6% multiple re-excisions
Wong, J et al. JCO, 2005
?younger, larger tumors, no Tamoxifen?

Conclusions• Boost: benefit in all age groups
• Tamoxifen without radiation after local excision for some ≥ 70 years women with ER+ ESBC may be acceptable
• EBCTCG: local control benefits breast cancer survival at 15 years
• Low-risk DCIS: no adjuvant radiation may be needed for
small tumors with wide margins
• MammoSiteTM trials are immature; closed technique superior in reducing infection

DCIS Collaborative GroupCS+RT in 1003 pts
LRR 5y 10y 15y
Solin 5% 10% 19%