questions what are the histological differences between atypical ductal hyperplasia (adh), ductal...
TRANSCRIPT


QuestionsWhat are the histological differences
between atypical ductal hyperplasia (ADH), ductal carcinoma in-situ (DCIS), atypical lobular hyperplasia (ALH) and lobular carcinoma in-situ (LCIS)? How do they each behave?
What are the management options for DCIS and what is the evidence?
What surveillance is recommended for DCIS?

Benign Breast DiseaseNonproliferativeProliferative without atypiaProliferative with atypia
ADH ALH LCIS
Considered “high risk” as they are associated with an increase in the patient’s future risk of developing breast cancer
Not “premalignant”

Aytpical Hyperplasia (AH)Atypical Ductal Hyperplasia
(ADH)Characterised by proliferation
of uniform epithelial cells with monomorphic round nuclei filling part, but not all of the involved duct
Shares some of the cytologic and architectural features of low-grade DCIS
Atypical Lobular Hyperplasia (ALH)Characterised by proliferation
of monomorphic, evenly spaced, dyshesive cells filling part, but not all, of the involved lobule
Can also involve ductsShares some cytologic and
architecural features of LCIS

ADHDCIS and invasive breast cancer is identified
in 33-87% of subsequent excision biopsies reported as ADH in the core biopsy

Risk of Cancer After AHAH (especially multifocal lesions)
Increased risk (RR 3.7-5.3) in ipsilateral and contralateral breast (higher in ipsilateral)
Conflicting data to suggest that the risk is higher with ALH than ADH
Relative risk increases when ADH occurs in women with a family history of breast cancer in a 1st degree relative to 10 times that of the general population with no family history
Lobular NeoplasiaSpectrum of proliferative changes within the
breast lobule that includes both atypical lobular hyperplasia (ALH) and LCIS
Both associated with increased risk of invasive breast cancer
LCIS is non-invasive, multicentric proliferation of the epithelial cells in the lobules and terminal ducts of the breast

HistologyLCIS diagnosed when all of the following
occur:Cellular proliferation is characterised by
round, cuboidal or polyganal cells that are regularly arranged and evenly spaced
Cell nuclei are predominantly round, monotonous and hyperchromatic
Proliferation involves, distends and distorts at least half the acini in the terminal duct-lobular unit and fills involved lobular spaces, resulting in the absence of central lumia
ALH is diagnosed with a lesion fails to meet at least one of the diagnostic criteria for LCIS in over 50% of acini within a lobular unit
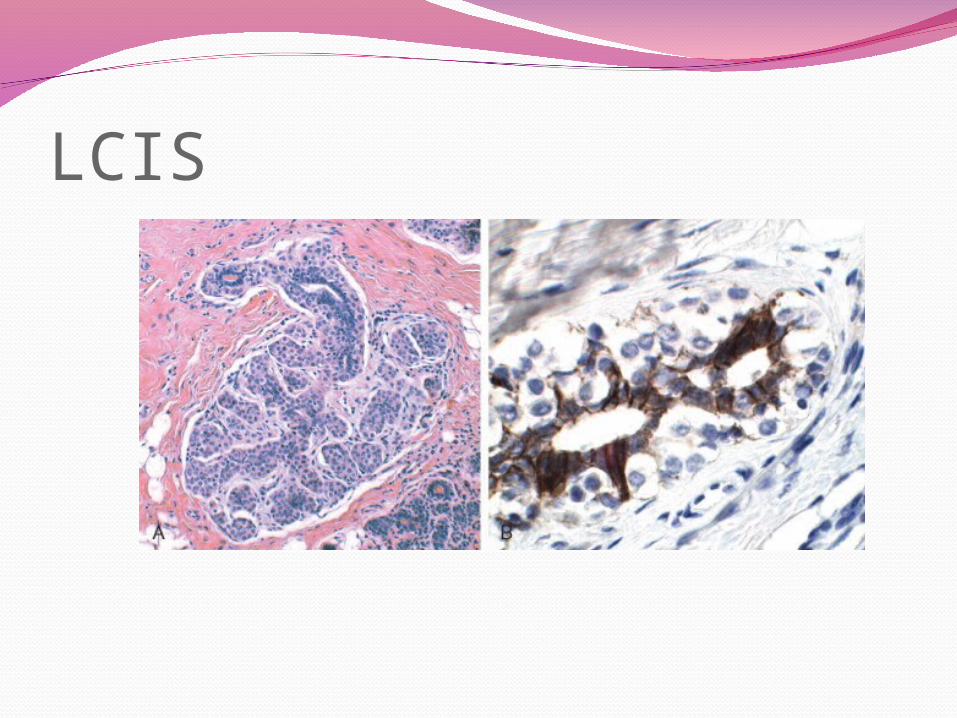
LCIS

Cancer RiskALH RR 3-4 (compared with general
population)Greater risk in ipsilateral breast
LCIS RR 7-9Appears to be as common in the contralateral
breast as in the ipsilateral breastPleomorphic variant appears to have an
aggressive biologic profile

Management and Follow-UpCore Bx of ADH excision biopsy due to
association with DCIS or invasive breast cancer
No strong evidence about whether to perform excision biopsy on women with LCIS or ALH on core Bx
Surveillance appears to be best the best management option for women who have been diagnosed with ADH, LCIS or ALH as the only abnormality (annual clinical examination, annual bilateral mammography for at least 15 years following diagnosis)

Management and Follow-UpNo role for CLE or mastectomy in the
management of ADH, LCIS or ALHInsufficient evidence to recommend the use
of tamoxifen for prevention of invasive breast cancer following a diagnosis of ADH, LCIS or ALH (Australian Guidelines)

DCISDefinition
Abnormal proliferative condition of epithelial cells in the mammary ducts
Cells display cytological features of malignancy but unlike invasive cancer, DCIS is confined within the ducts
Why is it clinically significant?Historically data suggests that 20-30% of
untreated DCIS progresses to invasive cancer

No reliable predictors for probability to progression to invasive carcinoma
Risk may be greater when DCIS displays features such as comedo necrosis or high nuclear grade
Natural history is largely unknown

Histology5 architectural subtypes: comedocarcinoma, solid, cribiform, papillary and micropapillary
Majority show a mixture of patterns
Malignant polyclonal population of cells limited to ducts and lobules by the basement membrane


Paget’s DiseaseDCIS arising within the
ductal system that extends up the lactiferous ducts and into the skin of the nipple without crossing the basement membrane

DiagnosisMost commonly detected as
mammographic caclificationBI-RADS Classification
0. Incomplete1.Negative2.Benign3.Probably benign4.Suspicious5.Highly suggestive of malignancy6.Known biopsy-proven malignant


General Principles of ManagementSmall, mammographically detected lesions should be
treated with complete local excisionIf disease is extensive, total mastectomy may be a
more reliable treatmentRCTs demonstrate a reduction in DCIS recurrence
and invasive breast cancer if radiotherapy is performed after CLE
ALND is not indicatedChemotherapy has never been investigatedTamoxifen in the adjuvant setting reduces risk of
DCIS recurrence and invasive breast cancerMDT

•Surgery (breast and axilla)•Radiotherapy•Chemoprophylaxis

SurgeryAim is to ensure complete excision with best
possible cosmetic resultPre-operative localisation is essential for a
mammographically detected impalpable lesionOptimal margins
No reliable definitionMust be completely excised“Clear margins” (no DCIS at section edge) provides
acceptable local control when combined with radiotherapy
<1mm considered inadequate

SurgeryAxillary Dissection
No place for ALNDWhat about SLNB?
High suspicion for invasive cancer Large size Aggressive histologic features Palpable mass
Surgery that will compromise ability to perform SLNB in the future
SurgeryMastectomy
Widespread contiguous or multi-focal DCISWidespread microcalcification in the presence
of proven DCISRecurrence of DCIS following initial treatmen
when either of the above indiciations is presentWoman’s choiceOther relevant risk factors for breast cancer

RadiotherapyLower recurrence rate demonstrated (4 RCTs)
when DCIS is treated with complete local excision (CLE) and adjuvant radiotherapy compared with CLE alone regardless of grade and pathological subgroup
Insufficient statistical power to detect small differences in survival
2009 Meta Analysis of RTx compared to no further treatment following excision showed RTx resulting in reduction in risk of all ipsilateral breast events (HR 0.49; 95% CI 0.41-0.58)

Risk of RecurrenceRelatively low for DCIS with good prognostic
pathological featuresClear marginsLow-gradeNo necrosisSmall extent (<10mm)
High grade DCIS with necrosis, close margins and larger size should have radiotherapy

Systemic TreatmentChemotherapy
Never investigated or used in treatment with DCIS

Systemic TreatmentTamoxifen
Must have ER + diseaseIn women who have breast conservation treatment,
postoperative tamoxifen is more effective than placebo in reducing the risk of invasive breast cancer (NSABP B-17 and B-24) (8.5 vs 10%
Meta-analysis (2009): Tamoxifen reduces recurrence risk of ipsilateral breast (HR 0.75, 95%CI 0.60-.092), trend to reduction in risk of invasive carcinoma (HR 0.79, 95%CI 0.60-1.01), lower risk for contralateral carcinoma (HR 0.57, 95%CI 0.39-0.83)
No apparent survival benefitRisks: endometrial cancer, VTE

Systemic TreatmentNCCN 2013 Guidelines
Consider tamoxifen for 5 years: Patients treated with breast conservation, especially if
ER + Patients treated with surgery alone and ER +
Australian Guidelines 2003Further research required, tamoxifen may
reduce risk of subsequent local invasive breast cancer in women who have had breast conservation treatment
No data for aromatase inhibitorsLimited data for HER2-directed therapy

The EvidenceLocal Recurrence Rates (%)
Trial No. of Patients
Follow up (yr)
CLE CLE + XRT
CLE + XRT + Tam
p value
NSABP B-17
818 12 30.8 14.9 <0.000005
EORTC 10853
1010 4.25 16 9 <0.005
UK ANZ 1707 5 20 8 6 <0.0001
SweDCIS
1067 5 7 22 <0.0001
NSABP B-24
1807 7 9 6 0.04

Post Treatment SurveillanceOverall survival for women >67 is similar to
those without breast cancerWomen >67 are more likely to die of
cardiovascular disease than breast cancerAustralian Guidelines
No evidence defining optimum follow-up protocol
Consensus recommendation is for annual review with examination and mammography indefinitely

Post Treatment SurveillanceNCCN Guidelines
Interval history and physical examination every 6-12 months for 5 years then anually
Mammogram annually and 6-12 months post radiation therapy if breast conserved
Breast awarenessIf treated with tamoxifen
Annual gynae assessment Opthalmology exam Manage symptoms as per guidelines