questions of health and inequality in southern africa: the case of mozambique bridget o’laughlin...
TRANSCRIPT
Questions of health and inequality in Southern Africa:the case of Mozambique
Bridget O’Laughlin
IESE April 2011
Argument The areas of connection between governance and health
are wider and less specialized than we often assume, which becomes clear:
If we focus on the relation between health and inequality rather than just the relation between health and poverty;
If we focus on health at the level of social causes of health and disease rather at individual incidence of ill or good health;
If we recognize that questions of health and inequality in Southern Africa today have to do with broad historical processes, and specifically some particular aspects of the enduring political economy of this region.
The order of the lecture
Some illustrations of health inequalities in Mozambique: the problem of rural health
Different ways of thinking about the relation between social inequality and health
The political economy of inequality in health in southern Africa: the rural ‘subsistence-producing’ family can/must take care of itself?
The causes of Sick Populations: 3 examples
Health and the space of governance
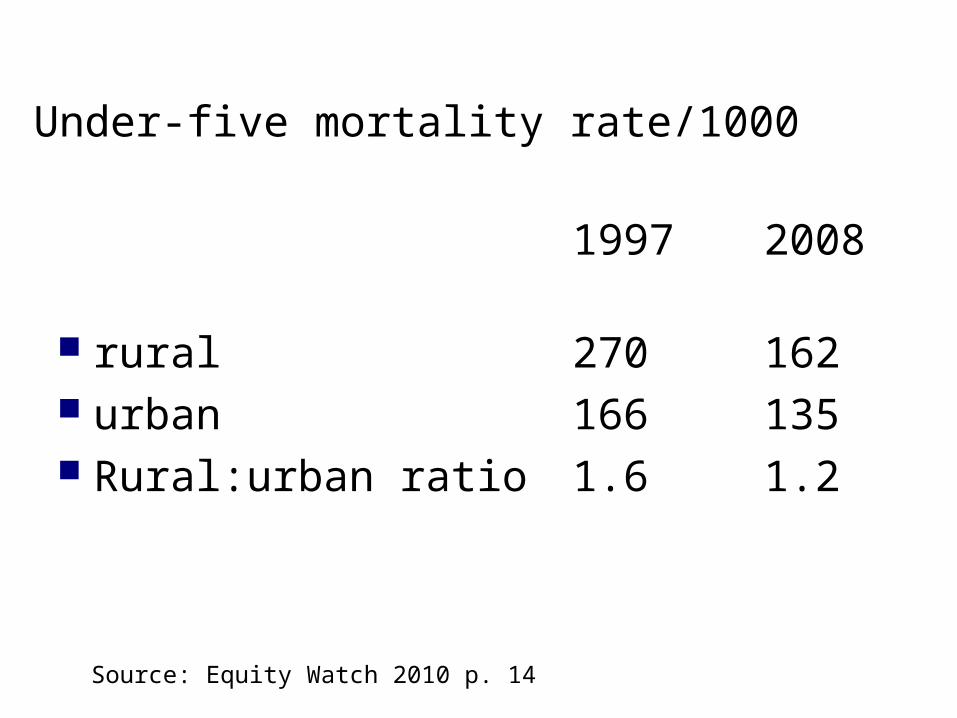
Under-five mortality rate/1000
1997 2008
rural 270 162 urban 166 135 Rural:urban ratio 1.6 1.2
Source: Equity Watch 2010 p. 14
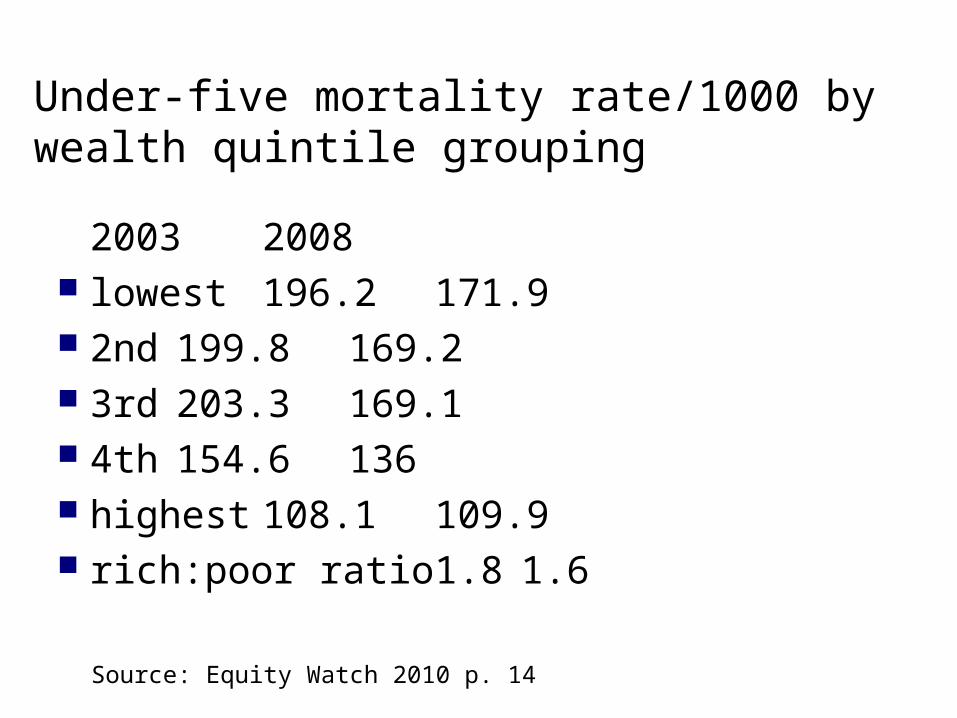
Under-five mortality rate/1000 by wealth quintile grouping
2003 2008 lowest 196.2 171.9 2nd 199.8 169.2 3rd 203.3 169.1 4th 154.6 136 highest 108.1 109.9 rich:poor ratio 1.8 1.6
Source: Equity Watch 2010 p. 14
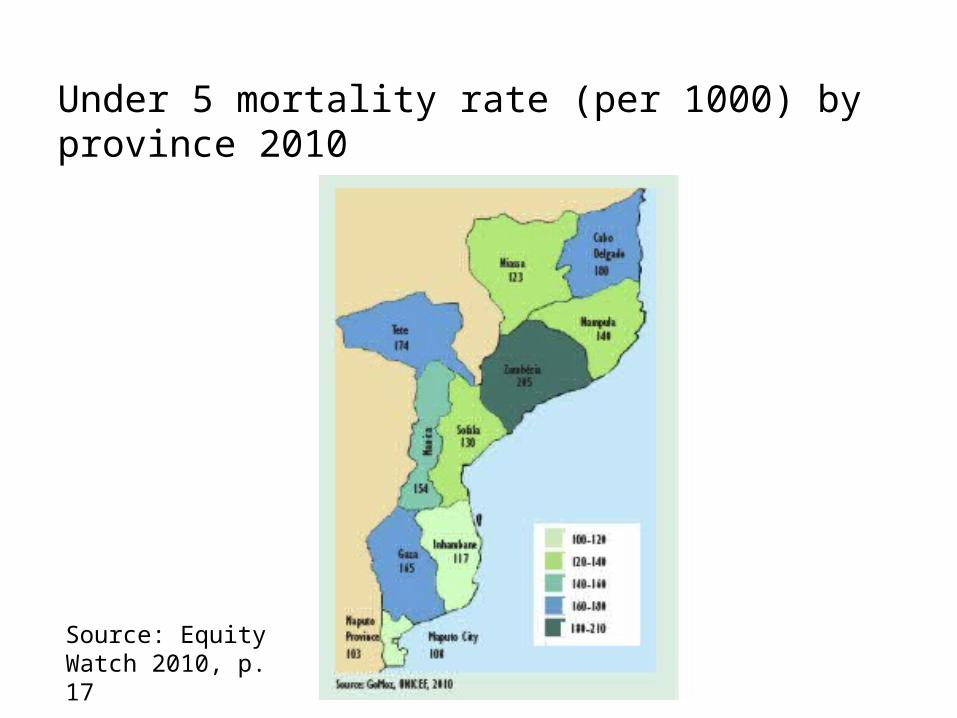
Under 5 mortality rate (per 1000) by province 2010
Source: Equity Watch 2010, p. 17
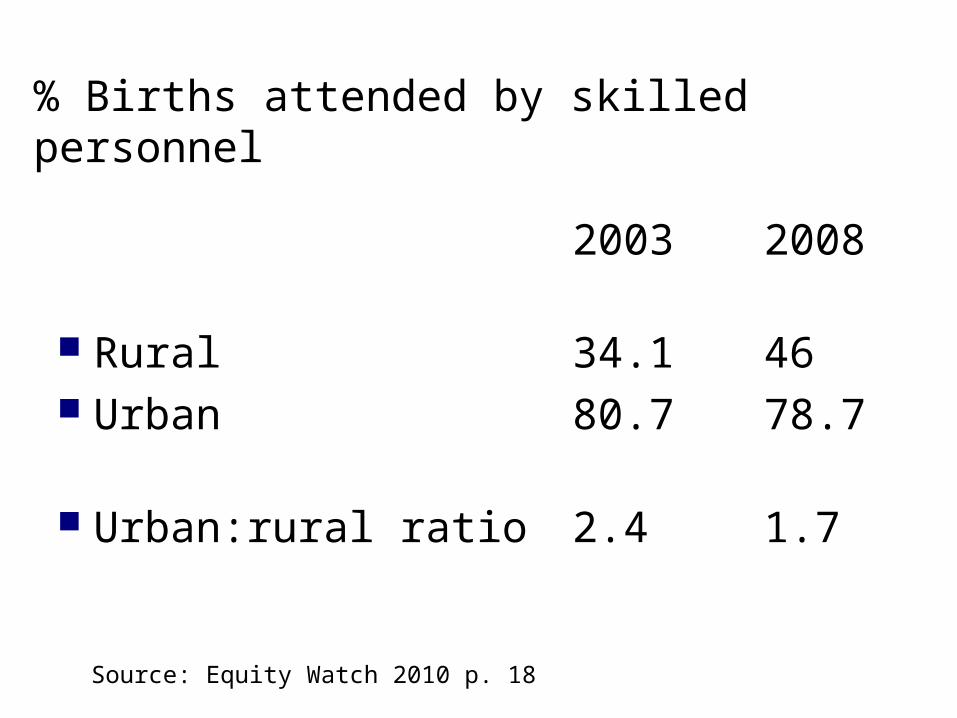
% Births attended by skilled personnel
2003 2008
Rural 34.146 Urban 80.778.7 Urban:rural ratio 2.4 1.7
Source: Equity Watch 2010 p. 18
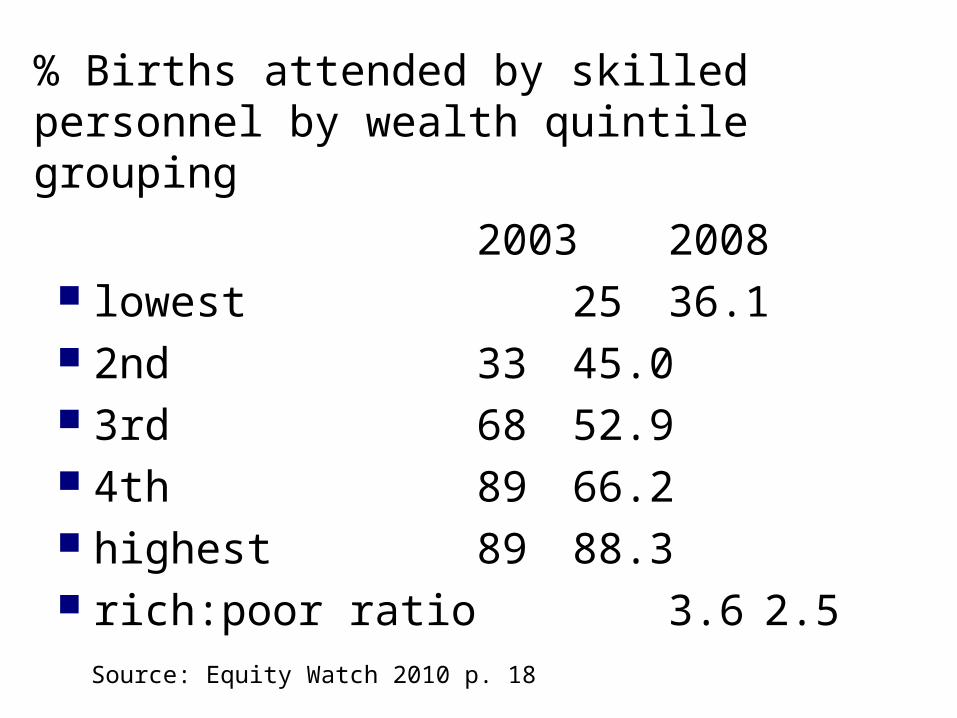
% Births attended by skilled personnel by wealth quintile grouping
2003 2008 lowest 25 36.1 2nd 33 45.0 3rd 68 52.9 4th 89 66.2 highest 89 88.3 rich:poor ratio 3.6 2.5
Source: Equity Watch 2010 p. 18
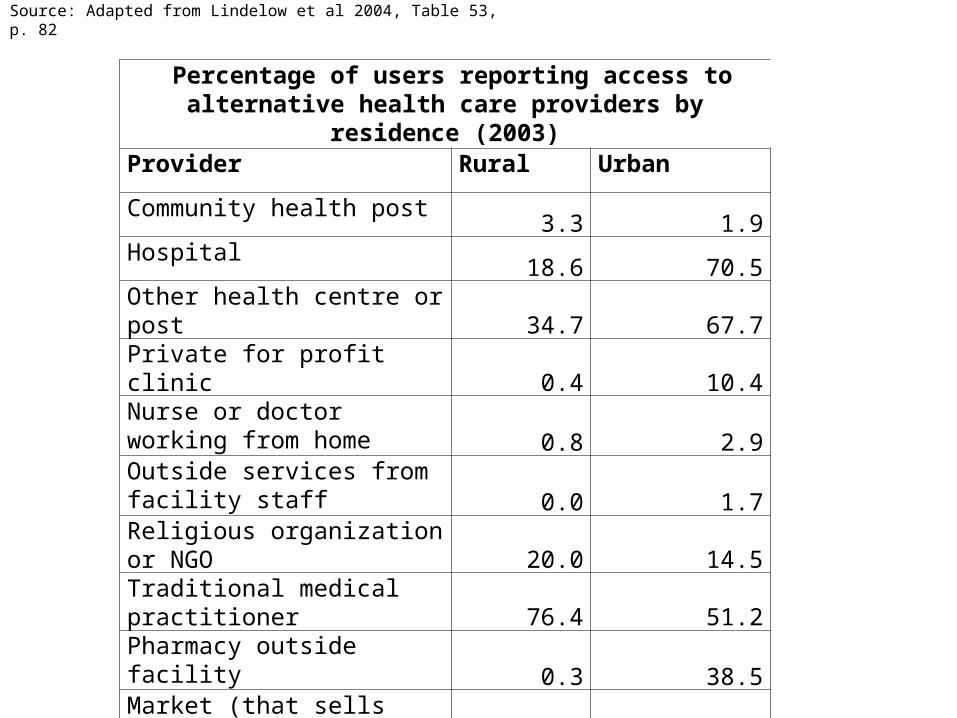
Percentage of users reporting access to alternative health care providers by residence (2003)
Provider Rural Urban
Community health post3.3 1.9
Hospital18.6 70.5
Other health centre or post34.7 67.7
Private for profit clinic0.4 10.4
Nurse or doctor working from home 0.8 2.9Outside services from facility staff 0.0 1.7Religious organization or NGO
20.0 14.5Traditional medical practitioner
76.4 51.2Pharmacy outside facility
0.3 38.5Market (that sells medicine)
5.0 12.2
Source: Adapted from Lindelow et al 2004, Table 53, p. 82
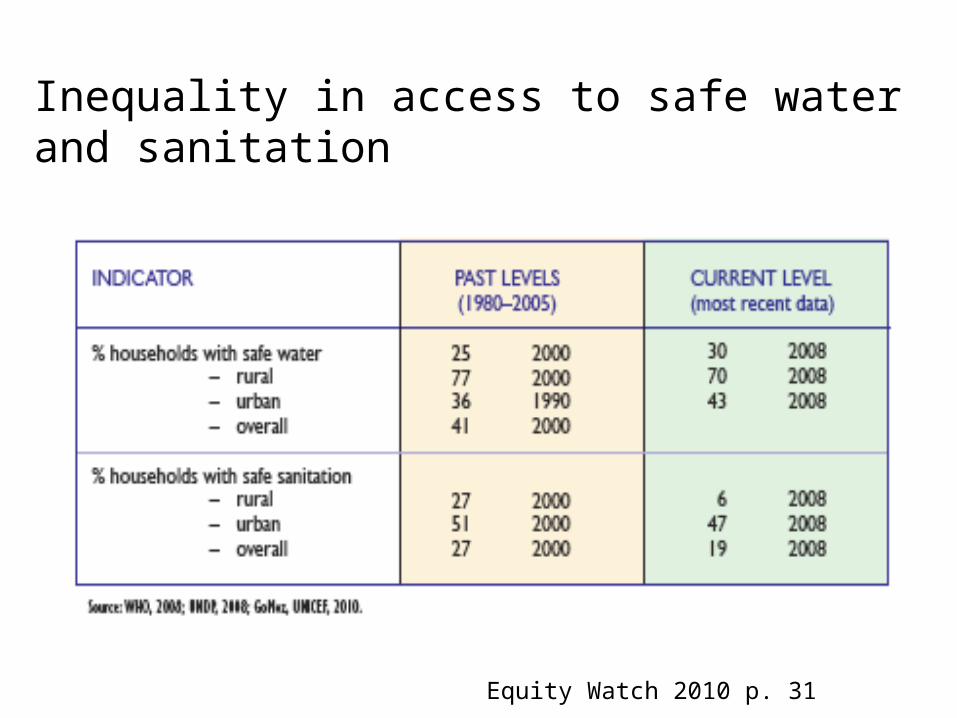
Inequality in access to safe water and sanitation
Equity Watch 2010 p. 31
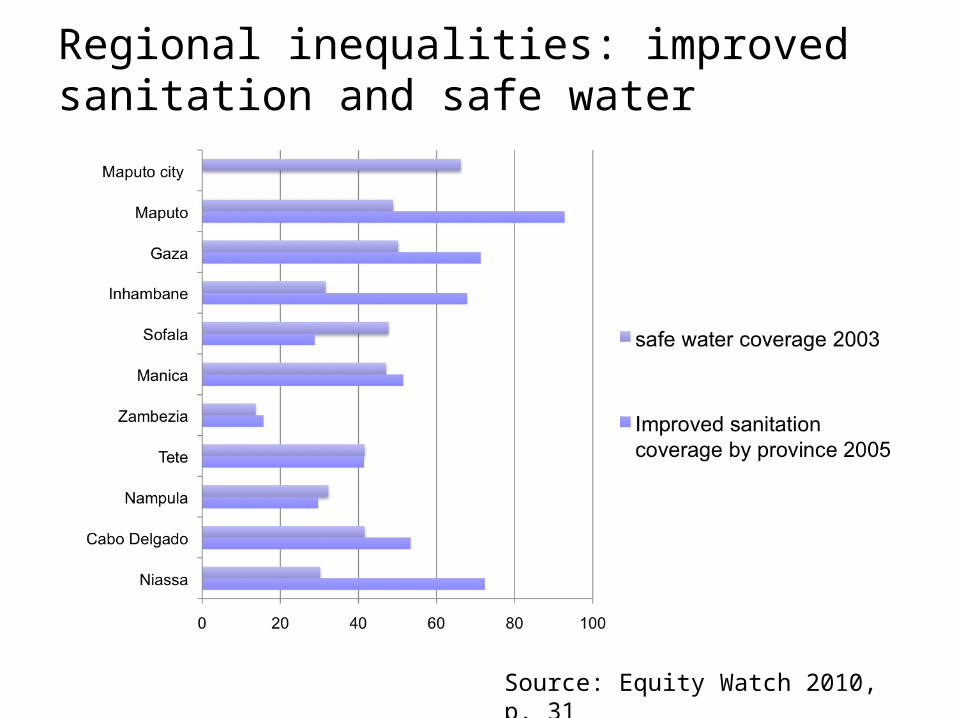
Regional inequalities: improved sanitation and safe water
Source: Equity Watch 2010, p. 31
Rose’s distinction
‘Aetiology confronts two distinct issues: the determinants of individual cases and the determinants of the rate of incidence’.
If we focus on the first issue, sick individuals, we will try to protect high-risk individuals against infections, whereas if we focus on the second issue and follow a population approach we will seek to control the causes of incidence.
Source: Rose 2001: p. 427
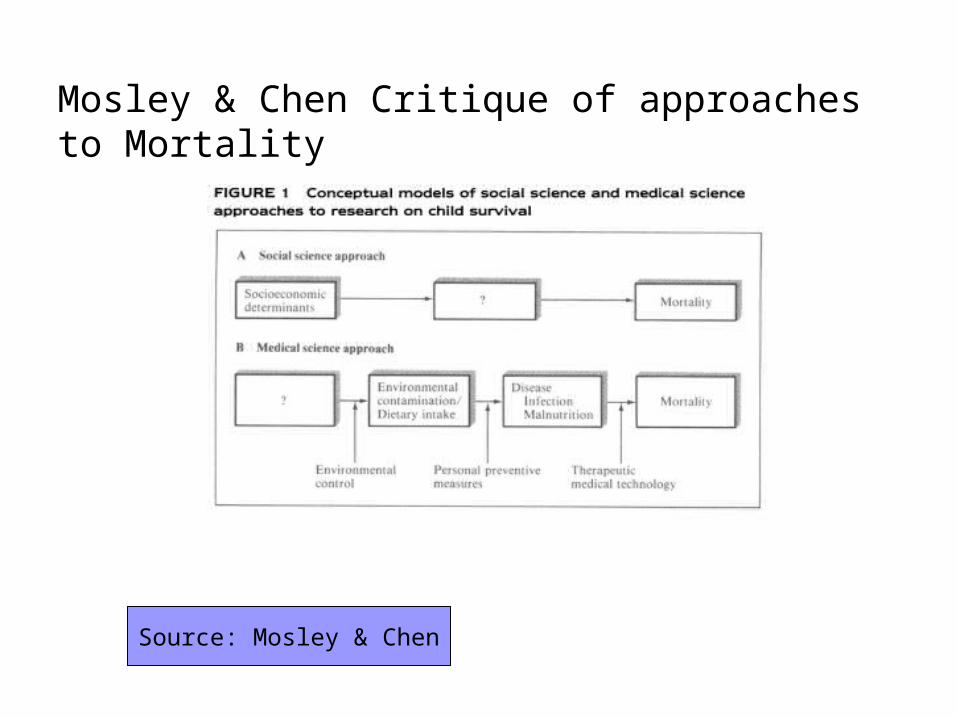
Mosley & Chen Critique of approaches to Mortality
Source: Mosley & Chen
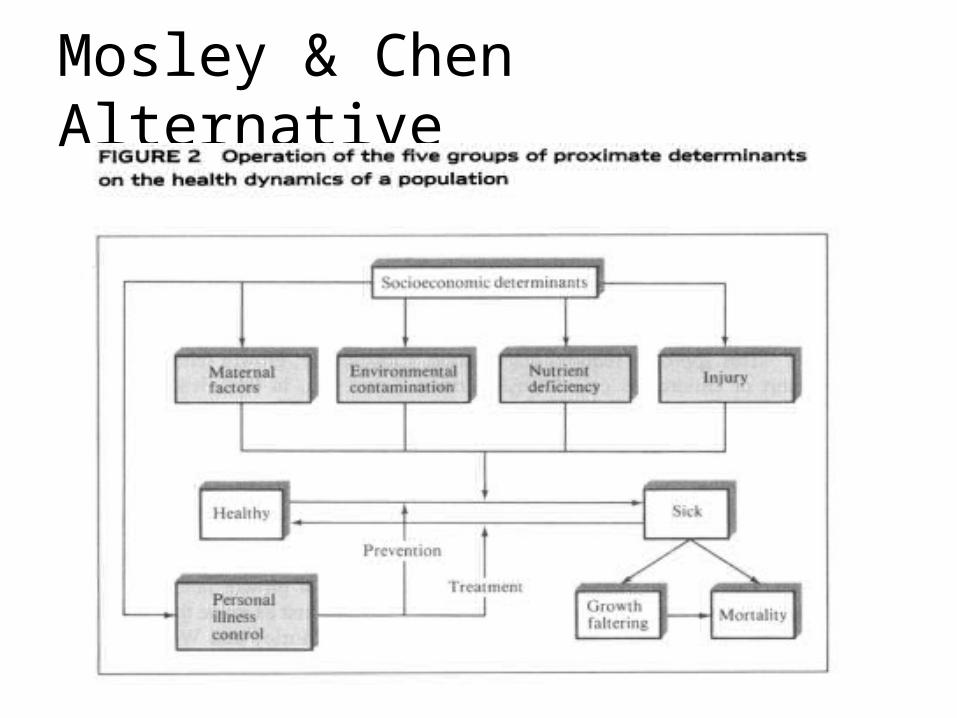
Mosley & Chen Alternative
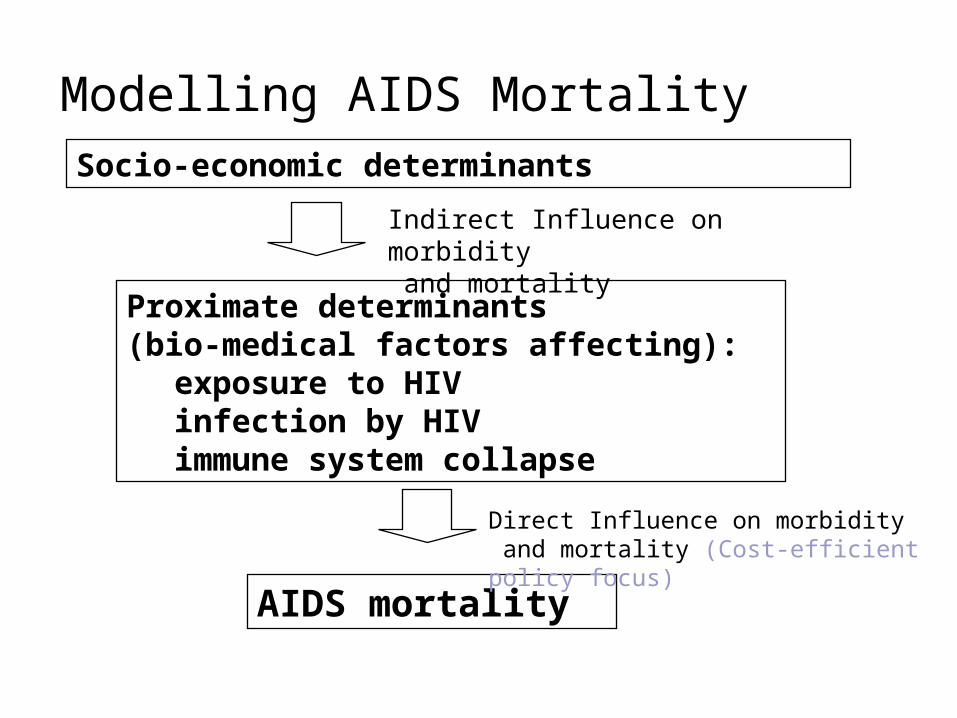
Modelling AIDS MortalitySocio-economic determinants
Proximate determinants (bio-medical factors affecting):
exposure to HIVinfection by HIVimmune system collapse
AIDS mortality
Indirect Influence on morbidity and mortality
Direct Influence on morbidity and mortality (Cost-efficient policy focus)
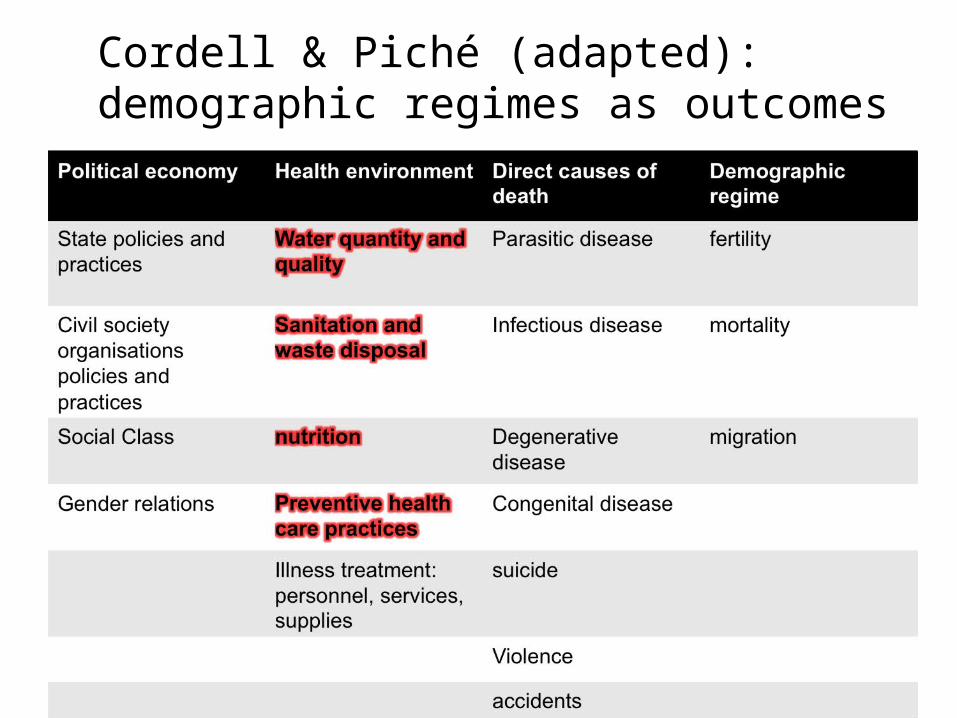
Cordell & Piché (adapted): demographic regimes as outcomes
Social costs of production
the ones normally counted as factors of production AND
a wide range of costs which in some societies and at some times are counted as production costs, and at other times are borne by the state, or workers' families, or the entire population.
Source: Feierman 1985
Southern Africa: ‘Africa of the Labour Reserves’
Migrant labour Small-holder cash-cropping and livestock
production The myth of subsistence farming Who bears/pays the social costs of
production?
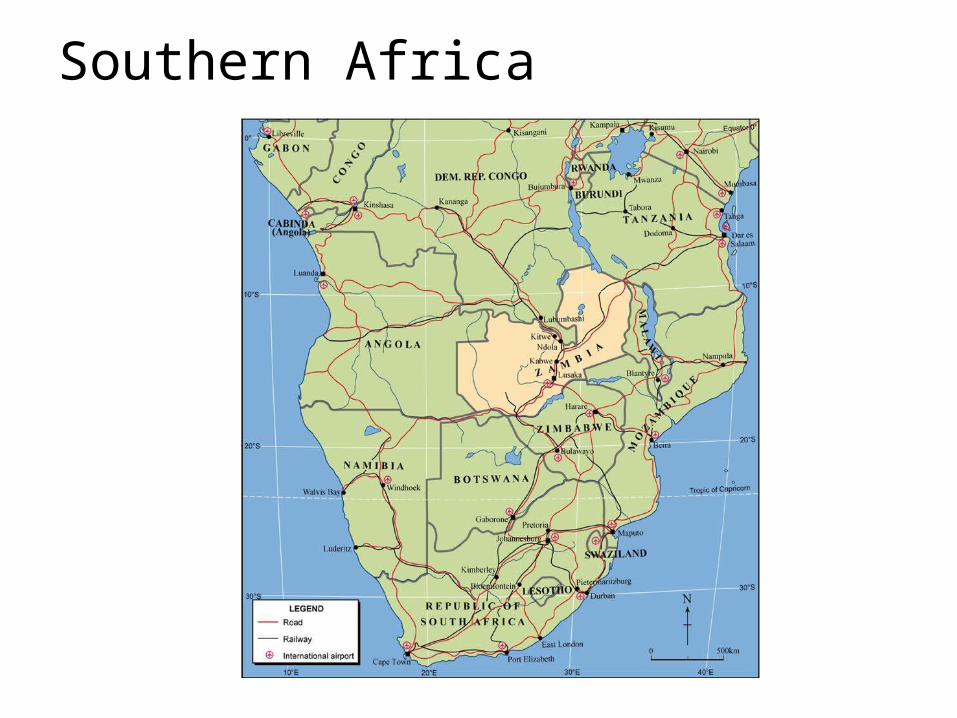
Southern Africa
Causes of cases and causes of incidence The development of endemic tuberculosis
in Southern Africa The elimination and recurrence of malaria
in Swaziland The mystery of konzo paralysis
Health and the space of governance
The health of populations is determined by a terrain much broader than formal health care (preventive and curing) : nutrition, work, environment
Strategies of accumulation Strategies of redistribution
the instruments of governance of the state include all those of particular relevance in approaching social inequality
tax policy, industrial relations policy, corporate governance policy, financial regulation social transfers
The space of health governance is a terrain of struggle reaching civil society and the state
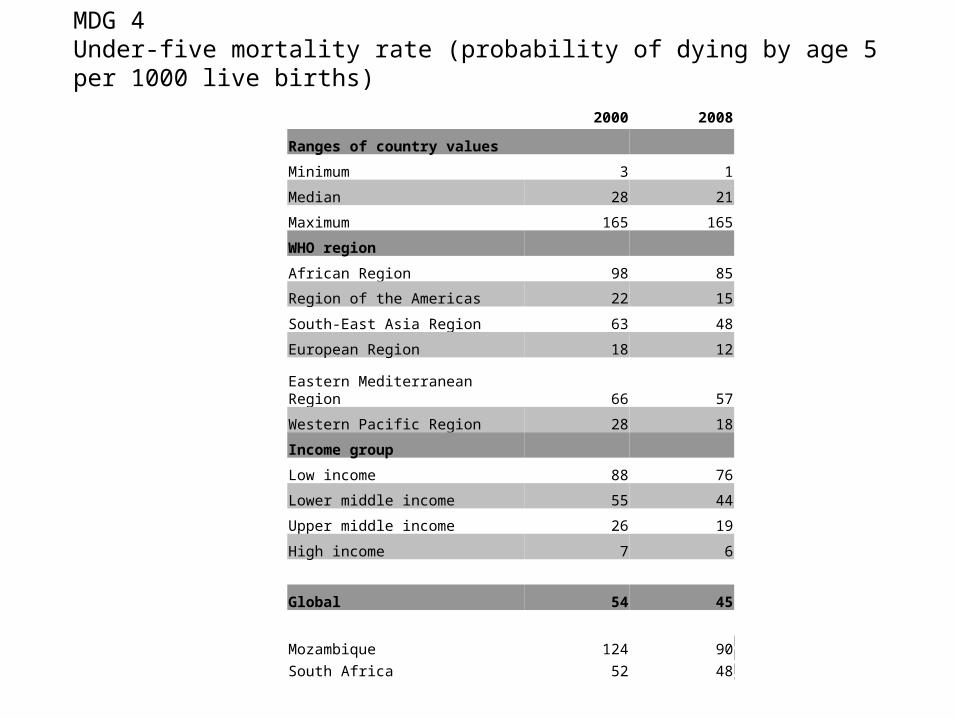
2000 2008
Ranges of country values
Minimum 3 1
Median 28 21
Maximum 165 165
WHO region
African Region 98 85
Region of the Americas 22 15
South-East Asia Region 63 48
European Region 18 12
Eastern Mediterranean Region 66 57
Western Pacific Region 28 18
Income group
Low income 88 76
Lower middle income 55 44
Upper middle income 26 19
High income 7 6
Global 54 45
Mozambique 124 90
South Africa 52 48
MDG 4 Under-five mortality rate (probability of dying by age 5 per 1000 live births)