quantiferon® testing of migrants: evidence, … · testing of migrants: evidence, ......
TRANSCRIPT

QuantiFERON® testing of migrants:
Evidence, Implementation, and Interpretation
L. Masae Kawamura, M.D.Senior Director, Medical and Scientific Affairs, Immune and Infectious Diseases, QIAGEN Clinician, San Francisco TB Clinic
Nduku NdundaAssociate Director, Medical and Scientific Affairs, Immune and Infectious Diseases, QIAGEN
March 2018

DISCLAIMER
I am employed by QIAGEN, manufacturer of QFT and other diagnostics, however the views expressed are my
own in keeping with my career as a TB clinician and formerTB Controller
Global Tuberculosis Report 2017, WHO

Sample to Insight
OVERVIEW
3
Why test for LTBI?
Why test with IGRAs?
Implementation
Result interpretation
QFT-Plus, 4th generation

TB and its all its consequences can be PREVENTED
LTBI Active TB
ACQUIRED DRUGRESISTANCE
http://www.unitaid.eu/tb-in-myanmar/ http://www.unitaid.eu/tb-in-myanmar/
http://www.unitaid.eu/tb-in-myanmar/
StigmaShame
Side effects
Financial losses
Irreversible Lung damage
TRANSMISSION
X
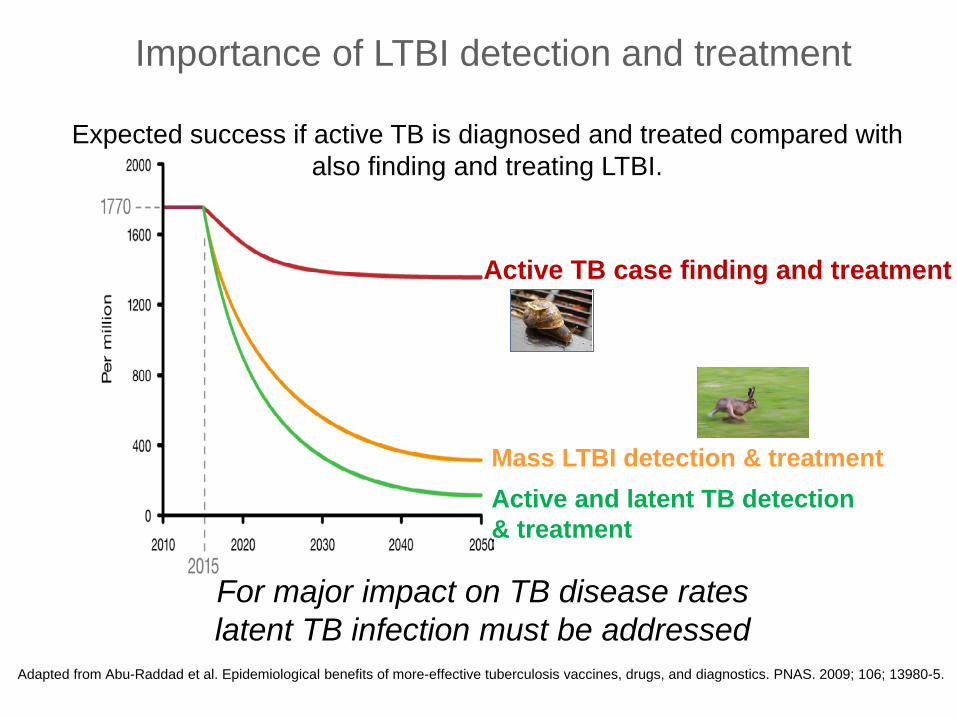
Importance of LTBI detection and treatment
Active TB case finding and treatment
Mass LTBI detection & treatmentActive and latent TB detection& treatment
Expected success if active TB is diagnosed and treated compared with also finding and treating LTBI.
For major impact on TB disease rateslatent TB infection must be addressed
Adapted from Abu-Raddad et al. Epidemiological benefits of more-effective tuberculosis vaccines, drugs, and diagnostics. PNAS. 2009; 106; 13980-5.

6
Full blown Active TBDogma: 10%
Diabetes
Aging
Immigration
The Global LTBI reservoir ensures future TB disease
HIV
Biologics

7
Great shift…• Passive TB case finding targeted active case finding• Ignoring LTBI prevention essential for TB elimination• IGRAs NO! IGRAs YES!• STOP TB END TB
2018 WHO updated and consolidated guidelines on the management of LTBI and prevention:

Sample to Insight
OVERVIEW
8
Why test for LTBI?
Why test with IGRAs?
Implementation
Result interpretation
QFT-Plus, 4th generation

9
Tuberculin skin test (TST) QuantiFERON-TB (QFT)
Can be fully automated Highly specific, not affected by BCG Results with one patient visit No inter-reader variability Electronic results (straight to EMR) Quality-assured laboratory test
Manual placement, reading and data entry Results affected by BCG vaccine and NTM Two patient visits required, high no-show rate Significant inter-reader variability Poor surveillance tool Often no quality control after initial training
TST is not patient or program-centered and least effective in the most vulnerable: BCG-vaccinated and “hard to reach” groups

The problem with the skin test: Purified Protein Derivative (PPD)
Prasad TSK, et al. Clinical Proteonmics 2013;10:8
Discovered by Robert Koch, 1890Mixture of denatured peptides/proteinsAutoclaving in vitro grown M. tuberculosis at 100° C for two hoursChemical composition: 93% proteins 1% nucleic acid 6% carbohydrate

Affect of BCG VaccinationPooled specificity for QFT-G and QFT-GIT 99% among non BCG vaccinated (8 studies) 96% among BCG vaccinated (8 studies)
Pooled specificity for TST 97% among non BCG vaccinated (6 studies) 59% among BCG vaccinated (6 studies)
Pai M, et al. Ann Intern Med 2008:149:177-184

Species Specificity of IGRA TB Antigens
Tuberculosis Complex
ESAT-6 CFP-10 TB7.7 Environmental Strains
ESAT-6 CFP-10 TB7.7
M tuberculosis + + + M abcessus - - -M africanum + + + M avium - - -M bovis + + + M branderi - - -
M celatum - - -BCG substrain M chelonae - - -
gothenburg - - - M fortuitum - - -moreau - - - M gordonii - - -tice - - - M intracellulare - - -tokyo - - - M kansasii + + -danish - - - M malmoense - - -glaxo - - - M marinum + + -montreal - - - M oenavense - - -pasteur - - - M scrofulaceum - - -
M smegmatis - - -M szulgai + + -M terrae - - -M vaccae - - -M xenopi - - -

QFT and BCG vaccinated
populations/migrants
13

Vietnam Immigrant Adults destined to the USAJohn A. Painter, Randall Reves et al, PLOS, December 2013 | Volume 8 | Issue 12
Tuberculosis Screening by Tuberculosis Skin Test or QuantiFERON®-TB Gold In-Tube Assay among an Immigrant Population with a High Prevalence of Tuberculosis and BCG
Vaccination
Vietnam Panel pre-entry screening of adults with BCG at birth TST and QFT results on 996 applicants with abnormal CXR 132 had TB, and 479 with normal CXR.
During 2-stage screening, QFT is as sensitive as TST in detecting TB with fewer requiring CXR and being diagnosed with LTBI. These data support the use of QFT
over TST in this population
14
Culture + M.tb (N=132) QFT TST at 5, 10 and 15 mmPositive (%) 86.4 89.4 vs 81 vs 52.3
Normal CXR (N=479) QFT TST at 5, 10 and 15 mmPositive (%) 33.6 71.0 vs. 49.3 vs. 23.0
Abn CXR culture- (N=864) QFT TST at 5, 10 and 15 mm
67.6 79.4 vs. 61.5 vs. 33.0

2015 US CDC pediatric study from panel sites in Mexico, Philippines and Vietnam
Howley et al, Pediatr Infect Dis J,2015 Jan;34(1):35-9
Evaluation of QuantiFERON-TB Gold In-Tube and Tuberculin Skin Tests among Immigrant Children being Screened for Latent
Tuberculosis Infection
Pre-entry screening of children age 2-14 from Mexico, Philippines and Vietnam entering the US
Comparison study of performance of IGRAs vs TSTs in foreign-born children.
15
N=2520 QFT TSTPositive 142 (5.6%) 664 (26%)
Indeterminate rate 13 (0.5%)1.4% (age 2-5)
All QFT indeterminatesTST negative
QFT-/TST+ QFT +/TST-
Discordant 553 (83%) 31 (2%)

Howley et al Pediatric Infectious Disease Journal 2014,
Title, Location, Date 16
Mexico
Philippines
VIetnam
41% LTBI reductionby QFT
85% LTBI reductionby QFT
84% LTBI reductionby QFT

17
Lowenthal et al, PIDJ, Vol 35:3, P231-236, March 2016
• Retrospective review of the follow-up of TST+ children settling in California (2005-2013)
• Countries of origin: Philippines> Mexico> China > Vietnam• Cohort age: 2-14 year• Total: 12,544 immigrant children included: 7786 (62%) evaluated post-
entry• 5243 (67%) were tested with TST or IGRA• 33% not retested

Domestic follow up of TST positive children: Key findings
18ID Week, October 8, 2015 – San Diego, CA
• Among those retested with IGRA →75% had negative results
• TST+/QFT- discordance consistent with other studies
• TST results ≥20 mm (Pre-entry) predicted positive TST on retest (95%) but NOT for IGRA (44% positive)
• Nearly half had repeat CXRs post entry (almost all normal) → IGRAs would reduce CXRs by 75%
…”replacing TST with IGRA or adding IGRA as a second confirmatory test at preimmigration screening sites could reduce the number of unnecessary domestic examinations among immigrant children, diminishing the burden imposed on immigrants and US TB control programs”
Lowenthal et al, PIDJ, Vol 35:3, P231-236, March 2016

No gold Standard for LTBI: Hierarchy of reference standards for LTBI Dx Aids.
Zwerling A, van den Hof S, Scholten J, et al. Thorax (2011). doi:10.1136/thx.2010.143180 19

IGRAs in predicting TB disease progression
20
LTBI

Serial QuantiFERON testing and tuberculosis disease risk among young children: an observational cohort studyInvestigator: Jason Andrews et al, Lancet, 2017http://thelancet.com/journals/lanres/article/PIIS2213-2600(17)30060-7/fulltext
N=2512 healthy babiesStudy design: Longitudinal study on QFT negative infants enrolled in a randomized, double-blind, placebo-controlled vaccine trial of MVA85A conducted in rural South Africa. Retested at ~1 year after vaccination
Findings• 7% conversion with no difference in placebo and vaccinated arms
• Disease incidence• QFT negative (non-converters): 0.7/100 person years• QFT positive 0.35 – 4.0 IU/ml: 2.5/100 person years• QFT positive >4.0 IU/ml: 28/100 person years
• Negative predictive value: 99%
Filling the knowledge gap: Pediatric study from Stanford University on South African children less than age 2

QFT+(n=4455)
TST+(n=6404)
TST+/QFT-(n=3050)
TST-/QFT+(n=1101)
TST+/QFT+(n=3354)
Follow up (person yrs)
8597 12281.5 5817.3 2132.8 6464.3
Incidence n 75 62 9 22 53Cumulative incidence*(95% CI)
1.68%(1.31-2.06)
0.97%(0.73-1.21)
0.30%(0.10-0.49)
2.0%(1.17-2.82)
1.58%(1.16-2.00)
Incidence/100 person years* (95% CI)
0.87(0.68– 1.07)
0.50(0.38–0.63)
0.16(0.05–0.26)
1.03(0.60–1.48)
0.82(0.60–1.04)
*P=<0.0001
22
*P=<0.0001
Gao L et al, Lancet Infect Dis 2017; 17: 1053–61
NEW: Definitive evidence that QFT is more sensitive than TST – CHINA(Gao et al, Lancet ID 2017)
2 year follow up study on multi-center cohort: QFT+ or TST+ (≥10mm) 2013: Baseline LTBI prevalence (n=21,022)
• QFT 18% (13-20%)• TST 28% (15-42%)
2014-2015: tracked disease progression by test positivity n=7505
“key populations in communities in rural China…could be targeted for latent infection screening and treatment with an IGRA rather than the TST.”
23
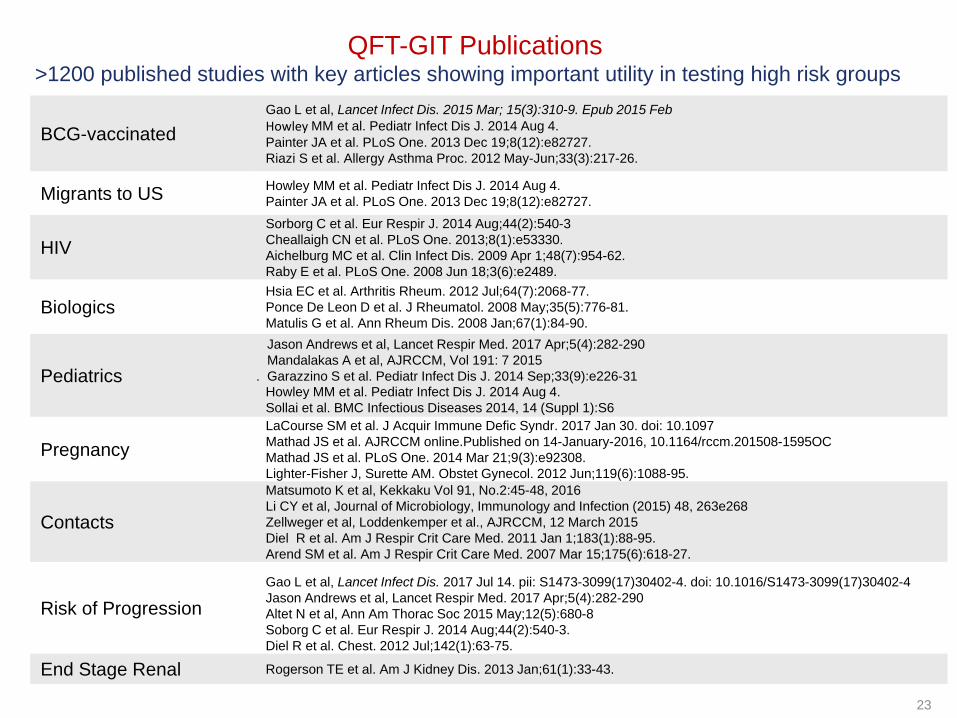
QFT-GIT Publications
BCG-vaccinatedGao L et al, Lancet Infect Dis. 2015 Mar; 15(3):310-9. Epub 2015 FebHowley MM et al. Pediatr Infect Dis J. 2014 Aug 4.Painter JA et al. PLoS One. 2013 Dec 19;8(12):e82727.Riazi S et al. Allergy Asthma Proc. 2012 May-Jun;33(3):217-26.
Migrants to US Howley MM et al. Pediatr Infect Dis J. 2014 Aug 4.Painter JA et al. PLoS One. 2013 Dec 19;8(12):e82727.
HIVSorborg C et al. Eur Respir J. 2014 Aug;44(2):540-3Cheallaigh CN et al. PLoS One. 2013;8(1):e53330.Aichelburg MC et al. Clin Infect Dis. 2009 Apr 1;48(7):954-62.Raby E et al. PLoS One. 2008 Jun 18;3(6):e2489.
BiologicsHsia EC et al. Arthritis Rheum. 2012 Jul;64(7):2068-77.Ponce De Leon D et al. J Rheumatol. 2008 May;35(5):776-81.Matulis G et al. Ann Rheum Dis. 2008 Jan;67(1):84-90.
Pediatrics
Jason Andrews et al, Lancet Respir Med. 2017 Apr;5(4):282-290Mandalakas A et al, AJRCCM, Vol 191: 7 2015
. Garazzino S et al. Pediatr Infect Dis J. 2014 Sep;33(9):e226-31Howley MM et al. Pediatr Infect Dis J. 2014 Aug 4.Sollai et al. BMC Infectious Diseases 2014, 14 (Suppl 1):S6
PregnancyLaCourse SM et al. J Acquir Immune Defic Syndr. 2017 Jan 30. doi: 10.1097Mathad JS et al. AJRCCM online.Published on 14-January-2016, 10.1164/rccm.201508-1595OCMathad JS et al. PLoS One. 2014 Mar 21;9(3):e92308.Lighter-Fisher J, Surette AM. Obstet Gynecol. 2012 Jun;119(6):1088-95.
Contacts
Matsumoto K et al, Kekkaku Vol 91, No.2:45-48, 2016Li CY et al, Journal of Microbiology, Immunology and Infection (2015) 48, 263e268Zellweger et al, Loddenkemper et al., AJRCCM, 12 March 2015Diel R et al. Am J Respir Crit Care Med. 2011 Jan 1;183(1):88-95.Arend SM et al. Am J Respir Crit Care Med. 2007 Mar 15;175(6):618-27.
Risk of ProgressionGao L et al, Lancet Infect Dis. 2017 Jul 14. pii: S1473-3099(17)30402-4. doi: 10.1016/S1473-3099(17)30402-4 Jason Andrews et al, Lancet Respir Med. 2017 Apr;5(4):282-290Altet N et al, Ann Am Thorac Soc 2015 May;12(5):680-8Soborg C et al. Eur Respir J. 2014 Aug;44(2):540-3.Diel R et al. Chest. 2012 Jul;142(1):63-75.
End Stage Renal Rogerson TE et al. Am J Kidney Dis. 2013 Jan;61(1):33-43.
>1200 published studies with key articles showing important utility in testing high risk groups

Sample to Insight
OVERVIEW
24
Why test for LTBI?
Why test with IGRAs?
Implementation
Result interpretation
QFT-Plus, 4th generation

Sample to Insight
Implementing QFT Plus at your panel site
CST001 overview, Aeras, July 30th 2014 25
What you need for your lab
37 0c IncubatorCentrifuge Plate washer
Reader FridgePipettes
Sample to Insight
Fully Automated ELISA Platforms available
Title, Location, Date 26
DS2 DSX

Sample to Insight
QFT on Automated Platforms
FOR INTERNAL USE ONLY QFT Product Training Tech Performance QM31635227A Approved 05/2013 27
QFT ELISA can be run on multiple platforms
Dynex DSX
Also known as BEST 2000
DiaSorin Eti-Max 3000
DadeBehring BEPIII
DadeBehring BEP2000
Grifols Triturus
Bio-Rad Evolis
Trinity Nexgen
Dynex DS2
Diamedix Mago Plus
ETI Max
Radim Alisei
Adaltis Personal Lab
ChemWell 2910
Inova QUANTA Lyser
Tecan Freedom EVO (75,100)

Sample to Insight
Evolution of QFT Technology
QFT blood collection tubes
QuantiFERON®-TB Gold Plus
QFT Plus ELISA
*Enzyme-Linked Immunosorbent Assay
QFT delivers advanced technology

Sample to Insight
Powered by QuantiFERON Technology
QuantiFERON® technology is a unique approach to disease detection and monitoring of the cell-mediated functions of the immune system from whole blood samples.
Advantage of QuantiFERON technology
Sample to Insight
Whole blood in tube Robust – Accurate Flexible workflow
Scalable Automated Rapid turn around

Sample to Insight
QFT System Overview
30
Nil (Grey cap) Negative control Adjusts for background noise or
non-specific IFN-γ in blood samples
TB Antigen TB1 (Green cap) Contains highly specific
CD4 antigens. TB2 (Yellow cap) Contains highly specific TB antigens:
combination of CD4 and CD8
Mitogen (Purple cap) Positive control May indicate:
- Decreased patient immune status, or- Incorrect blood handling & incubation
Blood collection tubes

Sample to Insight
Flexible blood collection options.
Title, Location, Date 31

Sample to Insight
Single Tube Blood Collection Process
Title, Location, Date 32
Collect 5ml blood byVenipuncture into one lithium Heparin tube. Maintain tubes at 22±5oC
Ship tube to laboratory.Blood must be incubated at 37oC (within 16 hours of collection).
Transfer 1ml of blood to each of the QFT Plus tubes.
Immediately after filling shake tubes 10 times.Label tubes.
Incubate blood as soon as possible (within 16 hours of collection). Incubate tubes for 16-24 hours.

Sample to Insight
Single Tube Blood Collection Process
Title, Location, Date 33
Collect 5ml blood byVenipuncture into one lithium Heparin tube. Maintain tubes at 4oC
Ship tube to laboratory.Blood must be incubated at 37oC (within 48 hours of collection).
Transfer 1ml of blood to each of the QFT Plus tubes.
Immediately after filling shake tubes 10 times.Label tubes.
Incubate blood as soon as possible (within 16 hours of collection). Incubate tubes for 16-24 hours.

Sample to Insight
QFT Plus Flexible Processing Options
Title, Location, Date 34
Option 2: Blood Incubated at collection site
Collect samples
Incubate within 16 hours
Send for analysis
calculation &Interpretation
Within 3 days send to lab
Standard blood handling precautions apply

Sample to Insight
QuantiFERON ELISA
*Enzyme-Linked Immunosorbent Assay
QFT delivers advanced technology

Sample to Insight
QuantiFERON Reagents Shelf Life
ELISA component Storage temperature
Storage time limit
ELISA kit 2ºC - 8ºC 36 months from date of manufacture
Reconstituted kit standard 2ºC - 8ºC 3 monthsFrom date of reconstitution
Reconstituted Conjugate100X Concentrate
2ºC - 8ºC 3 monthsFrom date of reconstitution
Working strength conjugate 17ºC - 27ºC 6 hours after dilution to working strength
Working strength wash buffer 17ºC - 27ºC 2 weeks after dilution to working strength
FOR INTERNAL USE ONLY QFT Product Training Tech Performance QM31635227A Approved 05/2013
Sample to Insight
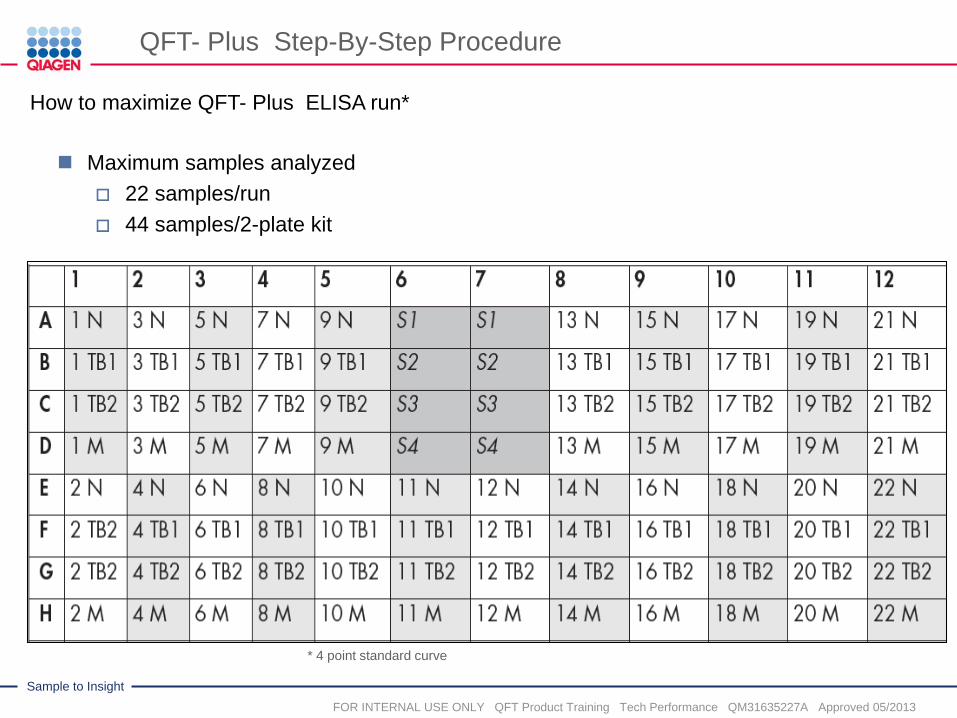
QFT- Plus Step-By-Step Procedure
Maximum samples analyzed 22 samples/run 44 samples/2-plate kit
FOR INTERNAL USE ONLY QFT Product Training Tech Performance QM31635227A Approved 05/2013
How to maximize QFT- Plus ELISA run*
* 4 point standard curve

Sample to Insight
QFT-Plus Software
QuantiFERON-TB Gold Blood Collection Refresher Training, Webinar PROM-9165-001 38

Sample to Insight
QuantiFERON-TB Gold Plus (QFT-Plus)
QuantiFERON-TB Gold Plus: the Most Accurate Test for TB Infection, Location, Date 39
Interpretation of QFT-Plus results (1)
Nil (IU/ml) TB1 minusNil (IU/ml)
TB2 minus Nil (IU/ml)
Mitogen minus Nil (IU/ml)
QFT-Plus result
Report/Interpretation
≤8.0 ≥0.35 and ≥25% of Nil
Any Any Positive M. tuberculosis infection likely
Any ≥0.35 and ≥25% of Nil
<0.35 OR ≥0.35 and <25% of Nil
≥0.5 Negative M. tuberculosis infection NOT likely
<0.5 Indeterminate Likelihood of M.tuberculosisinfection cannot be determined
>8.0 Any
Note: Cutoffs have not changed from QFT.
Positive results by TB1, TB2, or both are considered positive1. QuantiFERON-TB Gold Plus (QFT-Plus) ELISA Package Insert. Rev. 02. February 2015.1083163

Sample to Insight
Variability of IGRAS
Title, Location, Date 40
M.Pai, 2014 Clinical Microbiology

Sample to Insight
FAQ
Does Haemolysis affect QFT Test?

Sample to Insight
FAQ
How important is shaking the QuantiFERON tubes?
Complete mixing of the tubes is essential for proper performance of the QFT assay. During manufacture, the tube contents (TB-Specific antigens, Mitogen etc.) are spray dried onto the ENTIRE inner surface of the tube above the gel. Thus, blood needs to come into contact with the total inner surface to ensure that all reagents are rehydrated.

Sample to Insight
FAQ
Software uses the Optical density (OD) of S1 – S3 to generate a standard curve (outside USA)
From this curve an IFN-γ (IU/ml) value can be determined for each sample OD
Accuracy of test results depends on generation of an accurate standard curve
FOR INTERNAL USE ONLY QFT Product Training Tech Performance QM31635227A Approved 05/2013
S1
S2
S3Sample OD
IFN-γSample IU/ml
OD
Do I need standards for every run?
Sample to Insight
Resources available to help answer some of the FAQ
Title, Location, Date 44
http://www.quantiferon.com/products/quantiferon-tb-gold/clinical-resources/

Sample to Insight
OVERVIEW
45
Why test for LTBI?
Why test with IGRAs?
Implementation
Result interpretation
QFT-Plus, 4th generation

Let’s begin….Decision to test is a decision to
think! …..John Bernardo MD
46
Sample to Insight
QuantiFERON-TB Gold Plus (QFT-Plus)
QuantiFERON-TB Gold Plus: the Most Accurate Test for TB Infection, Location, Date 47
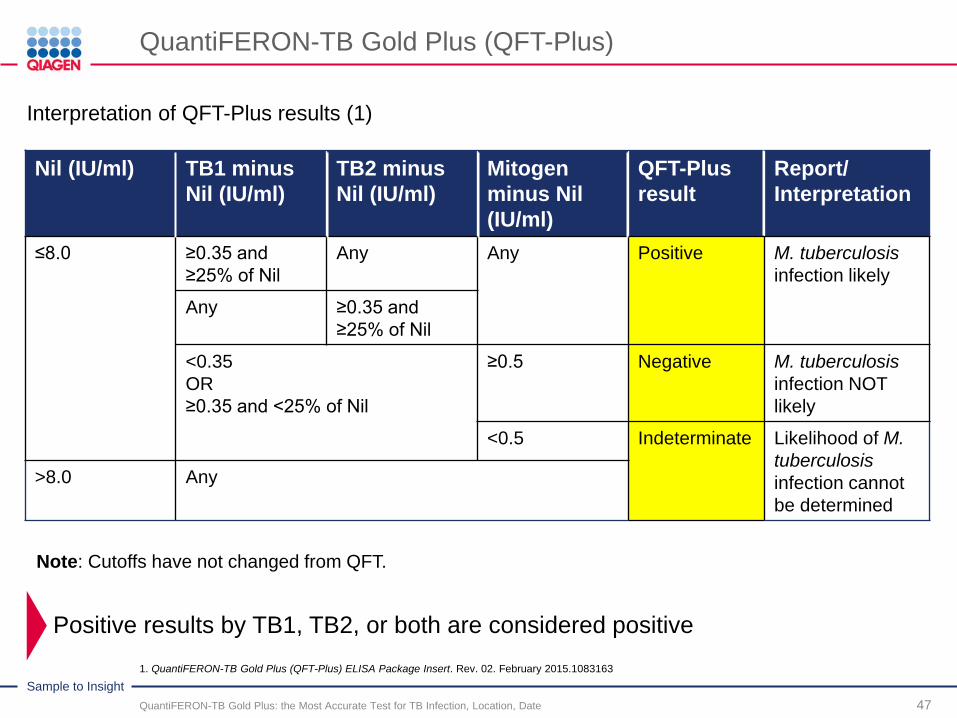
Interpretation of QFT-Plus results (1)
Nil (IU/ml) TB1 minusNil (IU/ml)
TB2 minus Nil (IU/ml)
Mitogen minus Nil (IU/ml)
QFT-Plus result
Report/Interpretation
≤8.0 ≥0.35 and ≥25% of Nil
Any Any Positive M. tuberculosis infection likely
Any ≥0.35 and ≥25% of Nil
<0.35 OR ≥0.35 and <25% of Nil
≥0.5 Negative M. tuberculosis infection NOT likely
<0.5 Indeterminate Likelihood of M.tuberculosisinfection cannot be determined
>8.0 Any
Note: Cutoffs have not changed from QFT.
Positive results by TB1, TB2, or both are considered positive1. QuantiFERON-TB Gold Plus (QFT-Plus) ELISA Package Insert. Rev. 02. February 2015.1083163

48
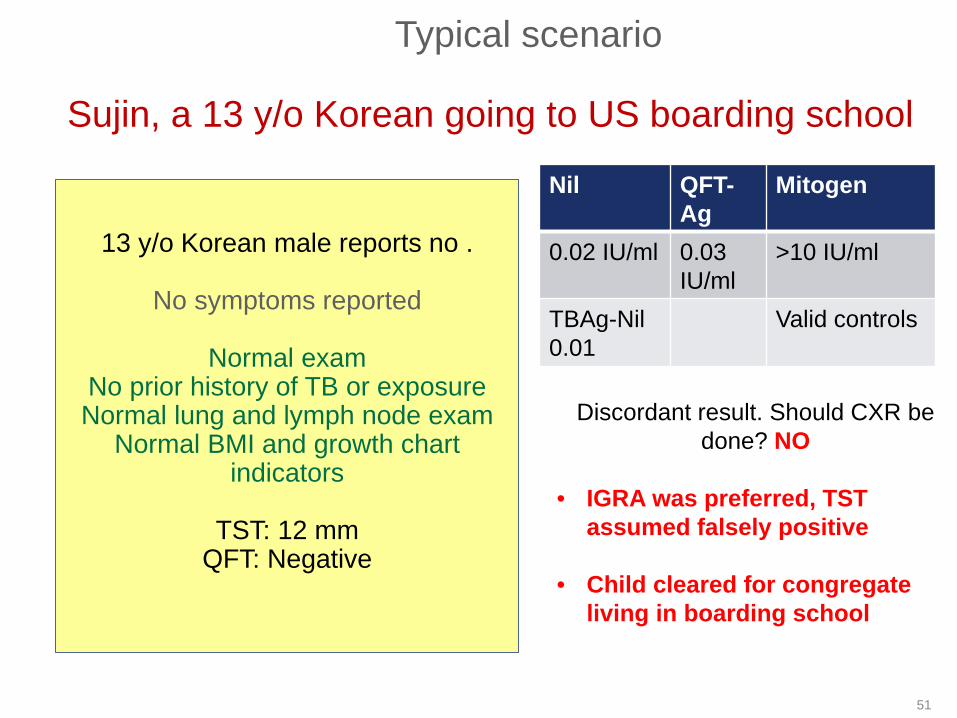
Sujin, a 13 y/o Korean going to US boarding school
13 y/o Korean male reports no .
No symptoms reported
Normal examNo prior history of TB or exposureNormal lung and lymph node exam
Normal BMI and growth chart indicators
TST: 12 mmIs retesting with IGRA advised?
Typical scenario
What test is preferred and why?
How do I manage this patient?

49
Sujin, a 13 y/o Korean going to US boarding school
Nil QFT-Ag
Mitogen
0.02 IU/ml 0.03 IU/ml
>10 IU/ml
TBAg-Nil0.01
Valid controls
Typical scenario
Discordant result. Should CXR be done?
13 y/o Korean male reports no .
No symptoms reported
Normal examNo prior history of TB or exposureNormal lung and lymph node exam
Normal BMI and growth chart indicators
TST: 12 mmIs retesting with IGRA advised?

50
When to do the CXR when IGRAs are the preferred test?Algorithm for the use of the TST and IGRAs in children – excerpt from
2014 AAP Technical report
AAP Technical Report:Interferon-γ Release Assays for Diagnosis ofTuberculosis Infection and Disease in Children
Pediatrics 2014;134:e1763–e1773
51
Nil QFT-Ag
Mitogen
0.02 IU/ml 0.03 IU/ml
>10 IU/ml
TBAg-Nil0.01
Valid controls
Typical scenario
Discordant result. Should CXR be done? NO
• IGRA was preferred, TST assumed falsely positive
• Child cleared for congregate living in boarding school
Sujin, a 13 y/o Korean going to US boarding school
13 y/o Korean male reports no .
No symptoms reported
Normal examNo prior history of TB or exposureNormal lung and lymph node exam
Normal BMI and growth chart indicators
TST: 12 mmQFT: Negative

52
Han, 17 y/o Vietnamese unaccompanied minor
17 y/o Vietnamese-born female enters the US through the Mexican-US
border. Reports her and her family beaten by the police. She escaped her
country by foot to Thailand before arriving in Mexico.
Minimal cough for 2 weeks, no fever, night sweats or weight loss. Feels fine
No prior history of TB or exposureNormal lung and lymph node exam
Height: 5’0” Weight: 91 lbsNo prior TB testingCXR: LUL infiltrate
Sputum X3: smear negativeBronchial lavage: smear negative
Scenario 2:
Does she need a TB skin test?
Now what? Does she needIGRA?
TST done before CXR. 43 mm

53
Han, 17 y/o Vietnamese unaccompanied minor
17 y/o Vietnamese-born female enters the US through the Mexican-US
border. Reports her and her family beaten by the police. She escaped her
country by foot to Thailand before arriving in Mexico.
Minimal cough for 2 weeks, no fever, night sweats or weight loss. Feels fine
No prior history of TB or exposureNormal lung and lymph node exam
Height: 5’0” Weight: 91 lbs)No prior TB testingCXR: LUL infiltrate
Sputum X3: smear negativeBronchial lavage: smear negative
Nil IU/ml QFT- Ag TBAg-Nil0.03 IU/ml 1.5 IU/ml 1.2 IU/ml
Positive?
Scenario 2:
Is TB ruled in?

LIMITATIONS of IGRAs are the same as the TST …..
CANNOT distinguish between active and latent TB
CANNOT distinguish between remote and new infection
CANNOT determine efficacy of treatment
SHOULD NOT be used to rule out active TB or LTBI in severely immunosuppressed persons
However, IGRAs CAN distinguish between BCG and true TB infection

55
Han, 17 y/o Vietnamese unaccompanied minor
17 y/o Vietnamese-born female enters the US through the Mexican-US
border. Reports her and her family beaten by the police. She escaped her
country by foot to Thailand before arriving in Mexico.
Minimal cough for 2 weeks, no fever, night sweats or weight loss. Feels fine
No prior history of TB or exposureNormal lung and lymph node exam
Height: 5’0” Weight: 91 lbs)No prior TB testingCXR: LUL infiltrate
Sputum X3: smear negativeBronchial lavage: smear negative
Scenario 2:
SYNOPSIS1. Symptoms should’ve triggered
CXR as first test2. Abnormal CXR is TB until
proven otherwise -TREAT3. Negative smears do not rule-
out active TB4. TST or IGRA results would
not change management unless active TB ultimately ruled out

56
Elena, 12 y/o Honduran female applicant
12 y/o Honduran female
No symptoms reported
Normal exam except foot lacerationNo prior history of TB or exposureNormal lung and lymph node exam
Normal BMI and growth chart indicators
No prior TB testing
Do a CXR now?Is retesting with IGRA advised?
Nil QFT-Ag
Mitogen
0.00 IU/ml 0.03 IU/ml
0.1 IU/ml
TBAg-Nil0.03
indeterminate
Scenario 3
What could be the cause these indeterminate results?

Sample to Insight
QuantiFERON-TB Gold Plus (QFT-Plus)
QuantiFERON-TB Gold Plus: the Most Accurate Test for TB Infection, Location, Date 57
Interpretation of QFT-Plus results (1)
Nil (IU/ml) TB1 minusNil (IU/ml)
TB2 minus Nil (IU/ml)
Mitogen minus Nil (IU/ml)
QFT-Plus result
Report/Interpretation
≤8.0 ≥0.35 and ≥25% of Nil
Any Any Positive M. tuberculosis infection likely
Any ≥0.35 and ≥25% of Nil
<0.35 OR ≥0.35 and <25% of Nil
≥0.5 Negative M. tuberculosis infection NOT likely
<0.5 Indeterminate Likelihood of M.tuberculosisinfection cannot be determined
>8.0 Any
Note: Cutoffs have not changed from QFT.
Positive results by TB1, TB2, or both are considered positive1. QuantiFERON-TB Gold Plus (QFT-Plus) ELISA Package Insert. Rev. 02. February 2015.1083163

Mitogen – Nil < 0.5 IU/ml- technical errors are the most common cause in healthy patients
Indeterminate QFT results – technical errors
May indicate:
Incorrect sample handling > 16 hours from blood specimen draw to incubation Transportation / incubation at incorrect temperature
Inadequate shaking of tubes- most common cause
Overfilling of tubes
What to do when a healthy person has an indeterminate result? Per TI instructions –no retest, treat as negative When should a program suspect a technical issue and seek help? Healthy outpatient populations should not have a indeterminate rate that exceeds 4%
59
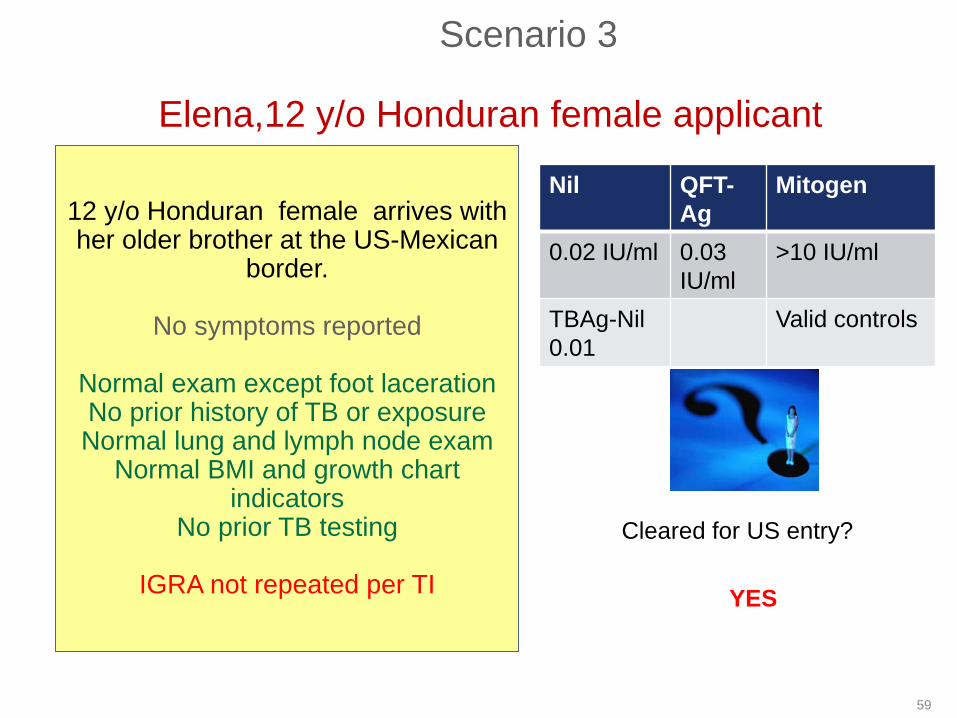
Elena,12 y/o Honduran female applicant
12 y/o Honduran female arrives with her older brother at the US-Mexican
border.
No symptoms reported
Normal exam except foot lacerationNo prior history of TB or exposureNormal lung and lymph node exam
Normal BMI and growth chart indicators
No prior TB testing
IGRA not repeated per TI
Nil QFT-Ag
Mitogen
0.02 IU/ml 0.03 IU/ml
>10 IU/ml
TBAg-Nil0.01
Valid controls
Scenario 3
Cleared for US entry?
YES

60
Mr. Lee, Majong champion applying to go to the US
62 y/o Chinese male heavy tobacco user is an applicant in Guanjou. He is retired and is joining his family in the
USReports no symptoms except unknown
weight loss Unknown family history of TB or
exposureNormal lung and lymph node exam
Hght: 5’10” Weight: 120 lbs (BMI17.2)Malnourished appearance NAD
No prior TB testing
CXR: RUL fibrotic infiltrateSputum smear negative X3
Nil QFT-Ag
TBAg-Nil
Mitogen
0.00 IU/ml
0.3 IU/ml
0.3 IU/ml
.5 IU/ml
Indeterminate
Scenario 4
Does he need IGRA?
Is TB ruled out?
What could be the potential causes of these results?
TST: 0 mm

TST and IGRA test interpretation: false-negative or indeterminate results
Host factors affecting TST and likely IGRAs HIV- low CD4, no ARVs Recent TB infection (<8 weeks) Infections (viral, fungal, bacterial) Other illness affecting lymphoid organs Live virus vaccination Immunosuppressive drugs Overwhelming TB Malnutrition Age (newborn, elderly)

62
Scenario 4
SYNOPSIS1. TB suspect Probable false
negative TST from malnutrition and/or TB
2. TB tests are immunologic assays impacted by anything that impacts the immune system
3. TB tests never rule out TB in a person who is a TB Suspect
4. An Indeterminate result can sometimes be meaningful
Mr. Lee, Majong champion applying to go to the US
62 y/o Chinese male heavy tobacco user is an applicant in Guanjou. He is retired and is joining his family in the
USReports no symptoms except
unknown weight loss Unknown family history of TB or
exposureNormal lung and lymph node examHght: 5’10” Weight: 120 lbs (MBI
17.2)Malnourished appearance NAD
No prior TB testingTST=0mm
CXR: RUL fibrotic infiltrateSputum smear negative X3

Sample to Insight
OVERVIEW
63
Why test for LTBI?
Why test with IGRAs?
Implementation
Result interpretation
QFT-Plus, 4th generation

Evolution of QFT Technology
64
QuantiFERON-TB to QuantiFERON-TB Gold
1st Generation 2nd Generation 3rd GenerationQuantiFERON-TB Gold In tube
• 2007 U.S. FDA approval• Logistical advantage –
remote incubation• New benchmark: Scalable
and easily automated• >1200 peer reviewed
publicatoins• >30 million tests sold
QuantiFERON-TB Gold
• 2004 U.S. FDA approval• “Liquid antigen” version• Antigens specific for M.tb
with 99% specificity• New benchmark: No cross
reactivity with BCG
QuantiFERON-TB
• 2001 U.S. FDA approval• Measured cell-mediated
immunity to tuberculin purified protein derivative (PPD)
• Breakthrough: TST becomes a blood test

4th Generation: QuantiFERON-TB Gold Plus
65
SAME test principle-procedure …..SAME technology of QFT
QFT-Plus is an improved version of QFT that will replace QFT-GIT :• Sensitivity of ~94% in registration trials• Specificity of >97%• Innovative CD8+ T-cell technology
– Optimized for CD4+ and CD8+ response
• Improvements in test formulation and manufacturing• NEW: options for blood draw and work flow flexibility
• One Li-heparin tube draw approved for transfer into QFT-Plus tubes
• 48 hour time limit for blood transfer to QFT tubes if Li-heparin tube stored between 2-8 degrees C.
QFT-Plus: potential test evolution – CD8 potential
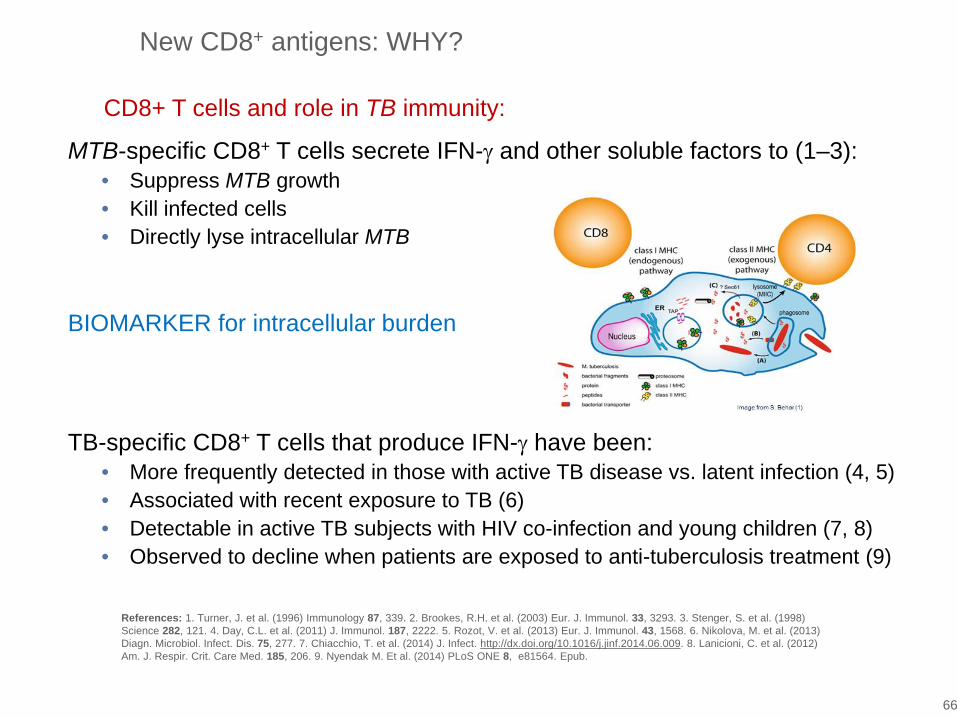
New CD8+ antigens: WHY?
66
CD8+ T cells and role in TB immunity:
MTB-specific CD8+ T cells secrete IFN-γ and other soluble factors to (1–3):• Suppress MTB growth• Kill infected cells • Directly lyse intracellular MTB
BIOMARKER for intracellular burden
TB-specific CD8+ T cells that produce IFN-γ have been:• More frequently detected in those with active TB disease vs. latent infection (4, 5)• Associated with recent exposure to TB (6)• Detectable in active TB subjects with HIV co-infection and young children (7, 8)• Observed to decline when patients are exposed to anti-tuberculosis treatment (9)
References: 1. Turner, J. et al. (1996) Immunology 87, 339. 2. Brookes, R.H. et al. (2003) Eur. J. Immunol. 33, 3293. 3. Stenger, S. et al. (1998) Science 282, 121. 4. Day, C.L. et al. (2011) J. Immunol. 187, 2222. 5. Rozot, V. et al. (2013) Eur. J. Immunol. 43, 1568. 6. Nikolova, M. et al. (2013) Diagn. Microbiol. Infect. Dis. 75, 277. 7. Chiacchio, T. et al. (2014) J. Infect. http://dx.doi.org/10.1016/j.jinf.2014.06.009. 8. Lanicioni, C. et al. (2012) Am. J. Respir. Crit. Care Med. 185, 206. 9. Nyendak M. Et al. (2014) PLoS ONE 8, e81564. Epub.

QuantiFERON® TB Gold In tube QuantiFERON® TB Gold Plus
Title, Location, Date 67
Cells stimulated
Nilcontrol
Mitogen control
Nil control
Mitogen control
noneCD4+ andCD8+ T-Cells
CD4+T-Cells
TBAntigen
TB 1Antigen
TB2Antigen
CD4+T-Cells
none AllAll
Long peptides (MHC class II)•ESAT-6 •CFP-10 •TB7.7+Additional short peptides(MHC class I)
Long peptides (MHC class II)•ESAT-6 •CFP-10 •TB7.7
Long peptides (MHC class II)•ESAT-6 •CFP-10 •TB7.7
Polypeptide Antigens
2 Antigen tubes:• More information: 2 data points instead of 1• Allows the calculation of CD8 response

Additional analysis of TB Antigen Tube values – Package Insert data
TB2 Minus TB1 (i.e. CD8/CD4 – CD4)
68
TB2 – TB1 (Nil subtracted)Surrogate for isolated CD8 response
Potential for additional valuable information for risk stratification?
Does this information help inform clinical practice?
Is this is recent infection?
Are they more likely to progress?
n=733 n=588 n=357

QFT PLUS Publications growing
69
Title/Authors
First independent evaluation of QuantiFERON-TB Plus performanceBARCELLINI et al
Published – ERJ 2016
Equal sensitivity of the new generation QuantiFERON-TB Gold plus in direct comparison with the previous test version QuantiFERON-TB Gold IT.HOFFMANN et al.
Published – CMI 2016
First evaluation of QuantiFERON-TB Gold Plus performance in contact screeningBARCELLINI et al
Published – ERJ 2016
Preliminary data on precision of QuantiFERON-TB Plus (QFT-Plus) performance. GALLAGHER et al
Published- ERJ 2016
CD8 response is associated to active TB and to the response to TB2 in the QuantiFERON-TB Plus kit.PETRUCCIOLI et al
Published– J of Infection 2016
Evaluation of QuantiFERON-TB Gold Plus for Detection of Mycobacterium tuberculosisinfection in JapanYI et al
Published-Scientific Reports 2016
QuantiFERON-TB® Gold Plus as a potential tuberculosis treatment monitoring toolKAMADA et al
Published –ERJ 2017
The sensitivity of the QuantiFERON®-TB Gold Plus assay in Zambian adults with active tuberculosis TELISINGHE et al
Published–IJTLD 2017
QFT-Plus: a plus in variability? – Evaluation of new generation IGRA in serial testing of students with a migration background in GermanyKNIERER et al
Published – J of Occ Med and Tox
Evaluation of QuantiFERON®-TB Gold-Plus in Healthcare Workers in a Low-Incidence Setting. MOON et al
JCM 2017
Prevalence of latent tuberculosis infection among foreign students in Lübeck, Germany tested with QuantiFERON-TB Gold In-Tube and QuantiFERON-TB Gold PlusMORALES et al
Journal of Occ Med and Toxicology 2017

70
Area of study Authors Finding
Sensitivity (culture proven TB)Italy, England, Germany, Japan
BARCELLINI et al,(n=116) HOFFMANN et al. (n=24)YI et al (n=162)PETRUCCIOLI et al, (n=69)TAKASAKI et al, (n=99)
88%-96% (indeterminate results excluded)Package insert: 94%
Specificity (low-no risk of exposure) Italy, USA
BARCELLINI et al (n=106)MOON et al (n=626)TAKASAKI et al, (n=117)
97-99% (99% if using conservative definition of both Ag tubesconcordant positives)
Contact investigationQFT-GIT vs. QFT-PlusItaly
BARCELLINI et al,N=119 TST+ contactsPIETERMAN et al,N=127 contacts
QFT-Plus results more closely associated with exposure risk. 15-33% with CD8 signal
HIV infected persons with microbiological proven TBZambia
TELISINGHE et aln=108 (63% HIV+)
QFT-Plus sensitivity not impacted by HIV status. HIV+ (85%) vs HIV negative (80%) Sensitivity 89% if indeterminate results excluded
Treatment monitoringJapan
KAMADA et aln=38, pansusceptible TB
CD8 but not CD4 responsedecreasing through end of treatment
Laboratory Precision QFT-GIT vs. QFT-Plus UK
GALLAGHER et aln=20 samples from 2 donors
CV: 9.60% (QFT-Plus) vs.18.25% (QFT-GIT)
QFT-Plus 2016–2018 key publications

71
Area of study Authors FindingComparison StudyLTBI- Immunocompromised:RA (on immunosuppressants)Japan
IGARI et al (n=154)Average age: 66.5 yrsBackground LTBI (2015)10.6% -15% for age 60-79 yrs
QFT-Plus vs. TSPOT*9.7% vs. 4.5% (P < 0.01)
*cut point- 6 spots, blood age <8 hrs
3-way Comparison studyActive TB sensitivity(Culture proven) and SpecificityJapan
TAKASAKI et al,Active TB (n=99)Controls (n=106)
QFT-Plus vs .QFT vs. TSPOT*Sensitivity98.9% vs. 97.9% vs. 96.9%Specificity 98.1% vs. 99% vs 98.1%No statistical differenceZero indeterminates QFT
*8-spot cut point but blood age not revealed
QFT-Plus 2016–2017 comparison studies
2017 unpublishedArea of study Authors FindingComparison studyActive TB sensitivity(Culture proven)Japan
FUKUSHIMA et al, (n=77) QFT-Plus vs. QFT vs. TSPOT*93.9% vs. 90.9% vs. 74%No statistical difference between QFTsBoth QFTs vs. TSPOT: p<0.0006 and P<0.004
*cut point- 8 spots, blood age >8 hrs, with T-Cell Xtend® product added

72
QuantiFERON-TB Gold Plus: Potential to better identify risk for progression
QuantiFERON-TB Gold Plus: Gaining attention in 2016 WHO TB report
Barcellini L, Borroni E, Brown J, Brunetti E, Campisi D, Castellotti PF et al. First evaluation of QuantiFERON-TB Gold Plus performance in contact screening. Eur Respir J. 2016:ERJ-00510-02016.
CD8 and CD4 T-cell response
“Current IGRA assays primarily detect a CD4 T-cell response. However, a new generation assay, the QuantiFERON-TB Plus (QFT-Plus, Qiagen, Hilden, Germany), has been developed to stimulate gamma interferon production by both CD4 and CD8 T-cells. First results indicate that the CD8 T-cell response may be able to identify people at greater risk of progression to active TB”.

First evaluation of QuantiFERON-TB Gold Plus performance in contact screening
Study design: Prospective recruitment of TST-positive adult contacts (TST ≥5 mm)• Average age of 39 (30-79) • 26%(n=61) non-European born, 78.85% (n=82) BCG vaccinated • 9.24% (n=11) were immunocompromised (HIV and other)• Contact screening based on NICE TB guidelines 2011 and Italian guidelines
Results
RESULTS
Barcellini et al, Eur Respir J. 2016 Jul 7. pii: ERJ-00510-2016. doi: 10.1183/13993003.00510-2016. Epub ahead of print]

Barcellini et al, 2016: Results continued…
74
Strong overall agreement (ĸ = 0.8) and QFT-Plus with higher positive rate◦ QFT-GIT: 47% (56/119)◦ QFT-Plus: 57% (68/119) – all except one with TST>10mm◦ Two QFT-GIT conversions upon retesting at 10–12 weeks. Both initially positive
by QFT-Plus
QFT-Plus with stronger risk association • QFT-Plus showed a stronger risk association to aggregate exposure time than QFT:
Odds ratio 6 QFT vs. 14 QFT-Plus
• QFT-Plus showed a stronger risk association to index case proximity than QFT:
Odds ratio 4 QFT vs. 6 QFT-Plus
“…our data show that QFT-Plus in contact screening has improved performance compared to QFT-GIT...”
Barcellini et al, Eur Respir J. 2016 Jul 7. pii: ERJ-00510-2016. doi: 10.1183/13993003.00510-2016. Epub ahead of print]

TB2:TB1 differential as a surrogate measure for CD8 stimulation
75
15% of QFT+ contacts had TB2-TB1 values >0.6 IU/mL• Significantly associated with proximity to the index case
◦ p = 0.0029• Significantly associated with European origin
◦ p = 0.043
“[QFT-Plus performance] suggests a role for the differential value between the two tubes as a proxy for recent infection.”
Barcellini et al, Eur Respir J. 2016 Jul 7. pii: ERJ-00510-2016. doi: 10.1183/13993003.00510-2016. Epub ahead of print]
Barcellini et al, 2016: Results continued…
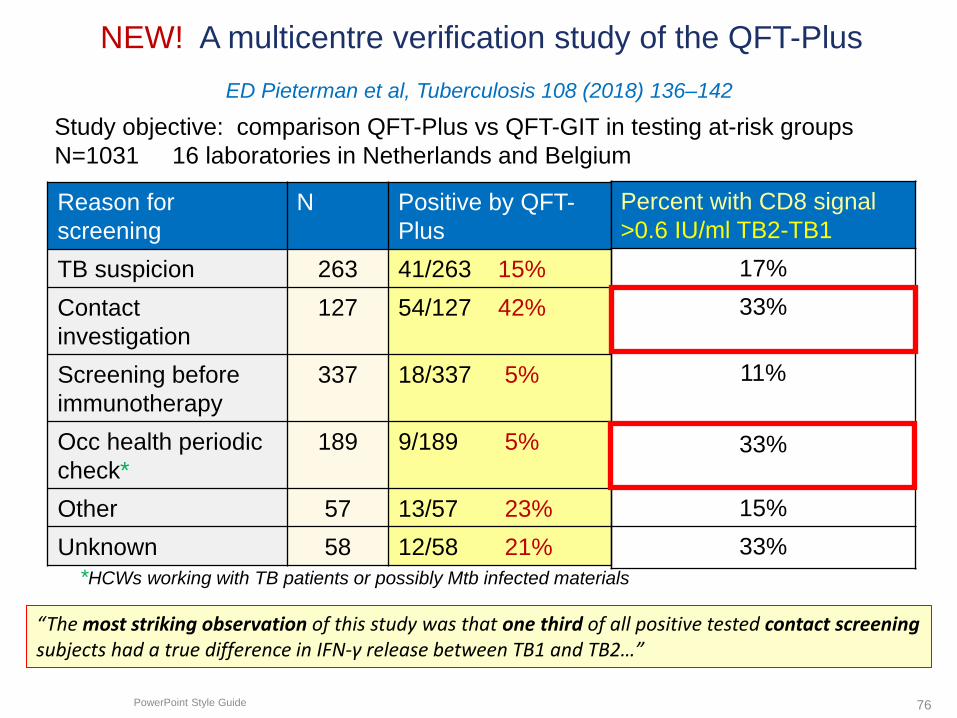
NEW! A multicentre verification study of the QFT-Plus
PowerPoint Style Guide 76
ED Pieterman et al, Tuberculosis 108 (2018) 136–142
Study objective: comparison QFT-Plus vs QFT-GIT in testing at-risk groupsN=1031 16 laboratories in Netherlands and Belgium
Reason for screening
N Positive by QFT-Plus
TB suspicion 263 41/263 15%Contact investigation
127 54/127 42%
Screening before immunotherapy
337 18/337 5%
Occ health periodic check*
189 9/189 5%
Other 57 13/57 23%Unknown 58 12/58 21%
*HCWs working with TB patients or possibly Mtb infected materials
Percent with CD8 signal >0.6 IU/ml TB2-TB1
17%33%
11%
33%
15%33%
“The most striking observation of this study was that one third of all positive tested contact screening subjects had a true difference in IFN-γ release between TB1 and TB2…”

1st evaluation of QFT-Plus performance in PLHIV (high-burden setting)
Study design: Prospective recruitment of Zambian patients with pulmonaryTB• Mean age of 32, 73% male; 63% HIV infected, BMI <18.5 (>50%)• 108 consecutive smear or Xpert +
Results
RESULTS
Telisinghe et al, INT J TUBERC LUNG DIS 21(6):690–696

QFT-Plus results not affected by HIV status
78
• Median IFN γ was higher in TB2 than in TB1 irrespective of HIV status
• Value of TB2: Among HIV negative, 20% of negative/indeterminate results on TB1 were positive on TB2, and among PLHIV, 29% of patients with negative/indeterminate results on TB1 were positive on TB2.
• QFT Plus negative/indeterminate (n=18) were underweight (76%), and 56% of those patients were HIV positive
• Compared to prior study in their institution with similar cohorts (Raby 2007) QFT not affected by HIV status and less affected by low CD4 count (results in % below)
Telisinghe et al, INT J TUBERC LUNG DIS 21(6):690–696
Telisinghe et al, 2017: Results continued

79
Scenario 1: TB2 equal TB1…Does it mean anything?
TB EXPOSURE SCENARIO: CONTACT INVESTIGATION
Contact investigation: Husband with cavitary MDR-TB ….
38 y/o Russian-born female with no cough, weight loss or fever
No medical problemsNon-smoker, no alcohol
Work: postal workerNormal lung and lymph node examGrandfather had TB when she was
age 9
CXR: Normal
QFT-PLUS RESULTTB1-Nil TB2-Nil0.46 0.50 Positive

Additional analysis of TB Antigen Tube values – Package Insert data
TB2 Minus TB1 (i.e. CD8/CD4 – CD4)
80
TB2 – TB1 (Nil subtracted)Surrogate for isolated CD8 response
Potential for additional valuable information after risk stratification?
n=733 n=588 n=357
FOR INTERNAL USE ONLY QFT Product Training
?

1. This Russian postal worker with new and remote contact to active TB and therefore a high probability (predictive value) for a positive QFT-Plus result.
2. Quantitative values are consistent with TB infection
3. TB2 = TB1 Does that mean anything? Yes, perhaps. It may impact preventive treatment decision including drug choice.
81
0.45 0.50
Near equal quantitative values. Lack of CD8 signal, history of childhood TB exposure, places her at lower risk of recent infection with MDR-TB
TB EXPOSURE SCENARIO: CONTACT INVESTIGATION

82
Scenario 2: Discordant positive….TB2 higher than TB1…Does it mean anything?
Contact investigation: Russian father with cavitary MDR-TB….
12 y/o daughter with probable anorexia and chronic anemia but no cough, reported weight loss or fever. However, she notes a cold 2 weeks
ago
Ballet dancerno medical problems
Normal lung and lymph node examNo prior TB testing
Mother and brother with +QFT
CXR: left lower lobe infiltrate with effusion
QFT-PLUS RESULTTB1 TB20.34 2.5 Positive
TB EXPOSURE SCENARIO: CONTACT INVESTIGATION

Additional analysis of TB Antigen Tube values – Package Insert data
TB2 Minus TB1 (i.e. CD8/CD4 – CD4)
83
TB2 – TB1 (Nil subtracted)Surrogate for isolated CD8 response
Potential for additional valuable information after risk stratification?
?
n=733 n=588 n=357
FOR INTERNAL USE ONLY QFT Product Training
?

1. This high-risk 12 y/o has a discordant positive and strong CD8 signal and abnormal chest X-ray consistent with early TB disease
2. In the context of recent TB exposure and CXR results, findings are consistent with both recent infection and disease
3. Does TB2>TB1 value mean anything? Yes probably increase risk of TB disease suspicion and need for immediate empiric TB treatment.
84
0.34 2.5
High PPV: CD8 signal (TB2—TB1) =2.16 IU/ml
TB EXPOSURE SCENARIO: CONTACT INVESTIGATION

QFT-Plus: the latest evolution of QFT technology
85
SummaryQFT-Plus is here
New flexibility for blood draw
Higher sensitivity than available metaanalysis
Maintenance of high specificity (independent studies)
The PLUS: Innovative CD8+ T-cell technology – Optimized for CD4+ and CD8+ response– Independent studies showing CD8+ correlation to
new infection and burden of TB– Numerous studies ongoing around the world– Each QFT-Plus test provide 2 data points with new dimension of insight
QFT-Plus: setting a new benchmark in TB infection testing
CD8 and CD4 T-cell response

Summary.
• Performance: QFT has higher specificity and LTBI sensitivity compared to the TB skin test
• QFT is the IGRA with the most evidence in multiple risk groups• QFT is the preferred test by the best TB programs in the US
and most advanced programs in Asia (Korea, Singapore, and Taiwan)
• QFT has been successfully implemented and studied by panel physicians in Latin America, Asia, and Eastern Europe

Sample to Insight
Thank you for your attention
87