qual analysis standard 1 - ausl.re.it analysis standard 1... · 1. sustainable is an inappropriate...
TRANSCRIPT

QUALITATIVE ANALYSIS OF COMMENTS AND SUGGESTIONS FROM PILOT ORGANISATIONS
STANDARD -1-
STANDARD 1
2
CODES
CLARITY
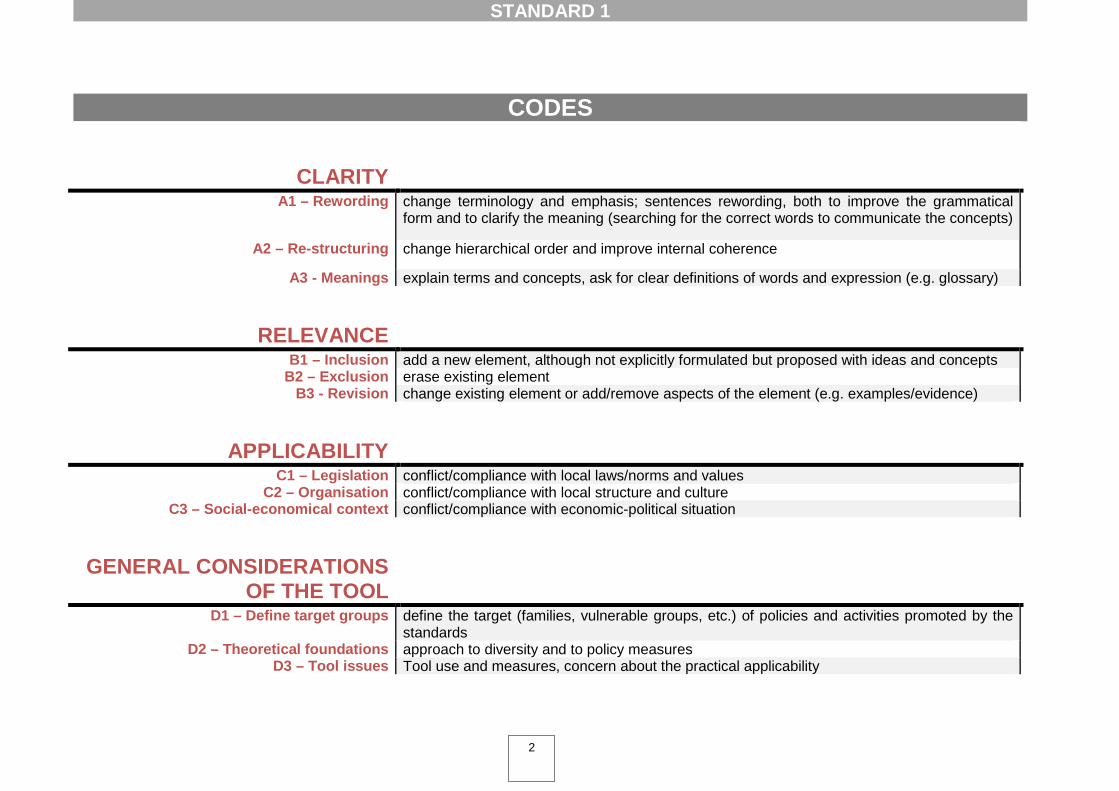
A1 – Rewording change terminology and emphasis; sentences rewording, both to improve the grammatical form and to clarify the meaning (searching for the correct words to communicate the concepts)
A2 – Re-structuring change hierarchical order and improve internal coherence
A3 - Meanings explain terms and concepts, ask for clear definitions of words and expression (e.g. glossary)
RELEVANCE
B1 – Inclusion add a new element, although not explicitly formulated but proposed with ideas and concepts B2 – Exclusion erase existing element
B3 - Revision change existing element or add/remove aspects of the element (e.g. examples/evidence)
APPLICABILITY
C1 – Legislation conflict/compliance with local laws/norms and values C2 – Organisation conflict/compliance with local structure and culture
C3 – Social-economical context conflict/compliance with economic-political situation
GENERAL CONSIDERATIONS OF THE TOOL
D1 – Define target groups define the target (families, vulnerable groups, etc.) of policies and activities promoted by the standards
D2 – Theoretical foundations approach to diversity and to policy measures D3 – Tool issues Tool use and measures, concern about the practical applicability

STANDARD 1
3
STANDARD 1 The organisation promotes equity by providing fair opportunities in healthcare and contributes to reducing health inequities through the delivery of sustainable and cost effective policies. To define how the organization should develop policies, governance and performance monitoring systems, which promote equity.
Codes frequency: Code Freq. A3-Meanings 7
A1-Re-wording 6
B1-Inclusion 2
C1-Legislation 2
D2-Theoretical foundations 2
A2-Re-structuring 1
C3-Social-economical context 1
B2-Exclusion 1
B3-Revision 1
D1-Define target groups 1
D3-Tool issues 1
Quotations N = 25
Bold text = critical issue Red Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Sustainable is an inappropriate word in this settings. Should change to … delivery of operational/practical/functional … (Norway)
2. “Reducing health inequities” is more widely unde rstood here – this standard could be
strengthened if it simply said “The organisation contributes to reducing health ine quities through the delivery of sustainable and cost effect ive policies ”. (Australia)
3. Use the term ‘health disparities ’ rather than ‘health inequities ’. (Canada – Ontario)
4. Please consider the following rewording of the main standard definition: The organization
promotes equity by providing equal access to health care and contributes to reducing existing health disparities through the effective d elivery of sustainable polices . (Canada – Ontario)
5. […] Suggested rewording: “The organisation promotes access by providing equit able
opportunities in healthcare and contributes to redu cing health inequities through the delivery of sustainable policies ”. (Australia)
6. ‘Cost-effective’ could be considered redundant with ‘sustainable’ and appears out of place in
the context of a focus on equity standards. Cost effectiveness appears to be irrelevant at this point. (Switzerland)
• A2 – Re-structuring:
1. The order in which the substandards and associated measureable elements are presented is confusing and may result in organizations having difficulty in conducting an organizational equity assessment. It is recommended that the substandards and measureable elements be reordered as suggested so that the ordering reflect s a progression from high-level to specific equity policies and procedures . (Canada – Ontario)
STANDARD 1
4
STANDARD 1 The organisation promotes equity by providing fair opportunities in healthcare and contributes to reducing health inequities through the delivery of sustainable and cost effective policies. To define how the organization should develop policies, governance and performance monitoring systems, which promote equity.
• A3 – Meanings:
1. Explanation about the concept ‘Equity’ - Many hospital staff members only have a superficial
understanding of the concept of equity. (The Netherland and Norway)
2. “Providing fair opportunities in healthcare ” is open to very wide interpretation . (Australia)
3. Definition of key terms in the entire standard as to ensure a common understanding for all readers. (Norway)
4. The word ‘fair’ [opportunities] is vague and would require definition (Canada – Ontario)
5. The standard assumes promoting equity is the goal – this is not part of the discourse here
just yet so it may be difficult for this standard to be a) understood and b) valued. (Australia)
6. The main standard is lacking in clarity and international generalizability . (Canada – Ontario)
7. “Equity of Access ” is a guiding principle for the organisation , and is probably the closest
our organisation would come to “promoting equity by providing fair opportunities in healthcare”, however this is probably a narrower interpretation than is intended in this standard. (Australia)
B – RELEVANCE
• B1 – Inclusion:
1. Creating involvement in an organization is the key to success. If you skip that everything will fail. You can create involvement and support by means of communication. You have to explain your vision internally. After the standards CS asks ARA if it is important to insert a standard for personnel/staff policy on diversity because personnel policy is very import in their organization. ARA says that it is important but that the question is how to insert a standard for personnel policy. The proposal is: “the composition of the staff should be the same as the composition of the service area .” The idea is that not only a Turkish nurse should take care of Turkish elderly. However the Turkish nurse has to be part of the first contact so that she can get to know all the relevant information. The Turkish nurse should tell the other nurses the important information so that the other nurses can deliver good care. (The Netherlands)
STANDARD 1
5
STANDARD 1 The organisation promotes equity by providing fair opportunities in healthcare and contributes to reducing health inequities through the delivery of sustainable and cost effective policies. To define how the organization should develop policies, governance and performance monitoring systems, which promote equity.
2. Note that little attention is paid to equity indicators within the organisation , in the treatment of employees - for example, regarding needs associated with the life cycle. We also suggest that specific attention be paid to the gender factor , both with internal indicators (such as the extent to which women are penalised in the course of their careers) and external indicators (such as the extent to which health workers take this factor into account when treating patients). (Italy – Ferrara)
• B2 – Exclusion:
1. Should cut down the number of measurable elements : there are too many elements , they
could be summarized into two substandards without repeating the measurable elements. (Norway, Sweden,Spain ).
• B3 – Revision:
1. “Cost effectiveness ” is not addressed in the substandards and should be in the measurable
elements i.e., 1.1 […]. (Canada – Ontario)
C – APPLICABILITY
• C1 – Legislation:
1. Legislation in Finland lead healthcare actions a nd laws set up some limits for example data collection and statistics . The baseline is assumption that availability of treatment is equal and equitable for all. We also have guarantee of care by the law . Guarantee of care means that everyone have to get an appointment and treatment as soon as possible when they recognize need of treatment. In Finland we have the law about the good government. Equality have to take into account for example staff recruit ing . Decision making contrary to equality would be illegal. Constitutional law set up limits for data collection from medical records. We can register to patient medical report only age, se x and citizenship (when foreigner) . We have not separated budget for culturally competent health care. Each hospital district in Finland have Ombudsman. Ombudsman vacancy is further resource if patient is dissatisfied for the treatment. Ombudsman make reports about complaints. For patients safety reports we have electronic measuring system named HAIPRO. (Finland)
2. All substandards and measurable elements of this standard are linked to the organizational policy and, in our case, the development of implementation strategies corres ponds to the Ministry of Health and the Andalusian Health Servic e. From our hospital we can only adhere to them. We believe that this can be extended to the entire document. (Spain)
STANDARD 1
6
STANDARD 1 The organisation promotes equity by providing fair opportunities in healthcare and contributes to reducing health inequities through the delivery of sustainable and cost effective policies. To define how the organization should develop policies, governance and performance monitoring systems, which promote equity.
• C3 – Social-economical context:
1. The main standard is lacking in clarity and international generalizability. (Canada – Ontario)
D – GENERAL CONSIDERATIONS OF THE TOOL
• D1 – Define target groups:
1. Terminology varies in different countries and this can lead to different types of understanding of issues and which groups are included in the equity definition. It may be helpful to identify the population groups, as some organisations may uninte ntionally omit certain groups . Are these standards aimed at all groups or can specific measurable elements be applied to specific groups? More guidance is needed to organisations on how this can be achieved over time, as one approach is not suitable for all groups that may experience inequity. In addition, limited resources may impact on delivering on all these at once, even when there is good will. (Australia)
• D2 – Theoretical foundations:
1. The meaning of “cost effective policies ” is subjective and open to wide interpretation . It would be more relevant to refer to risk reduction rather than cost – it is costly to ensure all clients receive access to relevant language services, rather than using alternatives (such as utilising family members / unaccredited staff to provide interpreting for communication) but that puts clients/agencies at high risk when such strategies are used. The standard needs to be reconsidered in terms of risk minimisation rather t han “cost” related issues . […] (Australia)
2. ‘Cost-effective’ could be considered redundant with ‘sustainable’ and appears out of place in the context of a focus on equity standards . Cost effectiveness appears to be irrelevant at this point. (Switzerland)
• D3 – Tool issues:
1. [parlando delle modalità di risposta al questionario] Not three options , but four to promote the choice avoiding the neutral choice. (Italy – Cesena)
STANDARD 1
7
SUBSTANDARD 1.1 The organization can ensure that its plans, policies and decisions promote equity in all aspects of its activities. Codes frequency: Code Freq. A1-Re-wording 5
B1-Inclusion 2
C2-Organisation 2
A3-Meanings 1
B3-Revision 1
Quotations N = 11
Bold text = critical issue Blue Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: “The organisation has plans, policies and decisions that promote equity in all aspects of its activities ” (twice Norway)
2. Change to: “The organisation ensures that its steering document s and decisions promote equity in all aspect of its activities ” (twice Norway )
3. Stronger wording is needed: The organization “should” ensure …rather than “can” ensure … […] (Canada – Ontario)
4. The word "ensure " is problematic . Suggest: "Equity is promoted through the organization's plans, policies and decisions. " […] (Canada – Ontario)
5. […] The level of the activities is different from that of the policies and is therefore too specific, micro and not possible to contextualize in this point. (Italy – Ausl Re)
• A3 – Meanings:
1. "aspects of its activities " What is meant by plans? Activity plans or structured plans (e.g. maternity and children’s unit)? - We have interpreted it as general planning, not specific plans. (Italy – Cesena)
B – RELEVANCE
• B1 – Inclusion:
1. Also need to add a point around equitable representation at the leadership levels (e.g. senior management, boards, etc.). (Canada – Ontario)
2. Parts of diversity have to be part of the workplans . Diversity means a reflection of the population of the city of Amsterdam. Both clients and staff have to be a reflection of the city. The staff is our first target because clients can feel at home only after they can identify themselves with the staff. We focus on the selection of staff mainly from the four important language groups. (The Netherlands)
STANDARD 1
8
SUBSTANDARD 1.1 The organization can ensure that its plans, policies and decisions promote equity in all aspects of its activities.
• B3 – Revision:
1. This standard appears to be unrealistic , maybe some specific aspects should be selected .
(Switzerland)
C – APPLICABILITY
• C2 – Organisation:
1. Comments for UHN Health Equity Council: UHN provides unscheduled, emergency care for all patients regardless of country of origin, income, education, employment status, sexual orientation or other social determinants of health. In scheduled care we have less ability to review that aspect of UHN policy . (Canada – Ontario)
2. This works well for NHS Lothian as we have well-developed systems to capture this data. Less well-developed organisations might struggle with some of the terms and they may not translate well. (Scotland)

STANDARD 1
9
MEASURABLE ELEMENT 1.1.1 The organization has procedures in place to review the impact of its plans, policies and decisions on equity. [Evidence: Document setting out its process and tools for carrying out equity audit or impact assessment (e.g. Health Equity Audit; Equity Impact Assessment tool).] Codes frequency: Code Freq. A1-Re-wording 6
B3-Revision 5
C2-Organisation 2
C1-Legislation 1
C3-Social-economical context 1
Quotations N = 15
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. The element could be better described and clarified : […] (Italy – Cesena)
2. Comment: “…plans, policies and decisions ” should be replaced by “governing documents ”. (Norway)
3. Change to: The organisation has evident procedures to review t he impact of its plans,
policies and decisions on equity . (Norway)
4. Change to: The organization has procedures to review the impac t of its plans, policies and decisions on equity . (Norway)
5. The word ‘review’ does not adequately describe the evidence provided for this measureable
element. The word ‘evaluate’ is a more accurate alternative . Please consider the following rewording of measureable element 1.1.1: The organisation has procedures in place to evaluate the impact of its plans, policies, and dec isions on equity . (Canada – Toronto)
6. Unclear on what “procedures in place to review…” means. (Canada – Ontario)
B – RELEVANCE
• B3 – Revision:
1. Examples : include references to equity in three-year action plan and relative annual plan hospital board resolution on equity: regional and vast area work group on equity centre resolution passed by single guarantee committee inter-agency resolution on functionality of intercultural mediation hph hospital coordination group and hph agency network of health promoters three-year plan for equity and annual plan of action on equity; equity impact assessment; annual training plan on equity. (Italy – Ferrara)

STANDARD 1
10
MEASURABLE ELEMENT 1.1.1 The organization has procedures in place to review the impact of its plans, policies and decisions on equity. [Evidence: Document setting out its process and tools for carrying out equity audit or impact assessment (e.g. Health Equity Audit; Equity Impact Assessment tool).]
2. Many policies and procedures are under review cu rrently . Equity is applied through emphasis on best practices, communication, and the meeting of cultural and language needs of patients, as well as anti-violence and anti-racism procedures. Sociocultural Consultation and Interpretation services emphasizes Equity in its Mission Statement. Impact is measured through data collection , annual reports and impact assessment analyisis statements in preparation of new plans (Canada – Quebec)
3. It is a given that the plans themselves exist. it would be appropriate to request , as first evidence, an explanation of policies for equity , after the assessment is made. (Italy – Modena)
4. […] The element is only relevant and applicable with the indicated modifications and if the more specific and concrete part of the "decisions" is therefore removed . (Italy – Reggio Emilia)
5. We are just beginning to consider trialling use of an Aboriginal Health Impact assessment tool – our organisation would have a long way to go in meeting this element (Australia)
C – APPLICABILITY
• C1 – Legislation:
1. Apart from the political situation, this measurable element does not seem to be necessa ry in Spain , as it is supposed to be overcome under the Spanish Constitution and the General Health Law , which guarantee the equal and accessible assistance in the healthcare system for every resident in the country. (Spain)
• C2 – Organisation:
1. This is embedded in the organizational priorities , and the organization's values and core
competencies but there is not a formal process for reviewing the impact on equity . It is not clear if this type of consideration is relevant to the measurable element.(Canada – Ontario)
2. This is a good measure of a sophisticated healthcare organisation's capacity to address
inequality through its mainstream processes. (Scotland)
• C3 – Social-economical context:
1. Often this is linked to the funding requirements that specific organisations may have, and these may need to be considered as well (Australia)

STANDARD 1
11
MEASURABLE ELEMENT 1.1.2 The organization monitors the extent to which its plans, policies and decisions address equity issues for patients and staff. [Evidence: Report showing the extent to which equity issues are addressed by its management (e.g. The report shows that the organization acts on the findings of impact assessment).] Codes frequency: Code Freq. A1-Re-wording 7
B3-Revision 4
A2-Re-structuring 2
C1-Legislation 1
C2 – Organisation 1
D3-Tool issues 1
Quotations N = 16
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: The organisation monitors the equity issues for patients and staff through its plans, policies and decisions. (Norway)
2. Change to: The organisation monitors its steering documents addressing issues . (Norway)
3. "The organisation controls monitors the extent to which its plans, policies and decisions consider the outcomes of the equity evaluations for patients and staff ." - The element as it is expressed here is not very clear since “address” seems to be connected with point 1.3 on the equity plan , whereas it could be changed to “consider the outcomes of the equity evaluations” so that it is coherent with this area. (Italy – Ausl Re)
4. To include ...The organization monitors, addresses, and acts ....... for me to be clear, relevant and applicable. (Canada – Quebec)
5. Please consider the following rewording of measureable element 1.1.2: The organization has procedures in place to ensure that its plans, polices, and decisions address equity issues and this information is internally and publicly dis seminated . [Evidence : An infrastructure is in place that enables organizations to review the impact of its plans, polices, and decisions on equity issues and act on the findings. A process for disseminating these findings is in place (e.g., organisational equity reports, scorecards, etc.)]. (Canada – Ontario)
6. There may need to be guidance or a review of the language used to allow organisations to see the clear distinction and progression between t his element and the previous one . (Scotland)
7. This would be applicable if the evidence were explained more clearly . Or, a better alternative would be to explain the type of report more clearly . (Italy – Pisa)
• A2 – Re-structuring:
1. This could be the 1st question (Italy – Modena)
2. Mentioning both the patients and staff in the sa me indicator is not appropriate . The
measurable element should be split into two measurables – one for patients and one for staff (Twice Norway).

STANDARD 1
12
MEASURABLE ELEMENT 1.1.2 The organization monitors the extent to which its plans, policies and decisions address equity issues for patients and staff. [Evidence: Report showing the extent to which equity issues are addressed by its management (e.g. The report shows that the organization acts on the findings of impact assessment).]
B – RELEVANCE
• B3 – Revision:
1. [Evidence: An infrastructure is in place that enables organizations to review the impact of its plans, polices, and decisions on equity issues and act on the findings. A process for disseminating these findings is in place (e.g., organisational equity reports, scorecards, etc.)]. (Canada – Ontario)
2. Only makes sense if element 1.1.1 is in place (Australia)
3. Family members should be explicitly mentioned in this element as they are an important and
separate stakeholder. (Canada – Ontario)
C – APPLICABILITY
• C1 – Legislation:
1. It's a function of the services of the Regional Health Administration (Spain)
• C2 – Organisation:
1. No one is in charge of a sustainable monitoring of policies of the institution . but assessment have been carried out within specific projects (Switzerland)
D – GENERAL CONSIDERATIONS OF THE TOOL
• D3 – Tool issues:
1. We don't understand how this can be assessed . (Spain)

STANDARD 1
13
MEASURABLE ELEMENT 1.1.3 The organisation’s leaders and decision makers actively promote equity in their work. [Evidence: Equity is included in performance management arrangements for all leaders and decision makers (e.g. Guidance for managers requires them to have at least one performance indicator which addresses equity).] Codes frequency: Code Freq. A1-Re-wording 2
C2-Organisation 2
B3-Revision 2
A2-Re-structuring 1
C1-Legislation 1
B2-Exclusion 1
Quotations N = 9
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: The organisation’s leaders and staff actively promote equity in their work. Otherwise, it is very difficult to measure this indicator as there is no tool addressing this work. (Norway)
2. the following rewording of this measureable element: The organisation’s leaders and decision
makers actively promote and support equity in their work. (Canada – Ontario) • A2 – Re-structuring:
1. Please consider incorporating measureable element 1.1.3 into substa ndard 1.3 […]
(Canada – Ontario)
B – RELEVANCE
• B2 – Exclusion:
1. Unnecessary , covered by the elements above (Sweden)
• B3 – Revision:
1. e.g. equity performance indicators are included in perfo rmance management to ensure that equity in workplace is promoted. This allows for measuring.. (Canada – Quebec)
2. the level of satisfaction of the term "actively" must be explained to be able to create
measurable indicators of it. “being active” may only be the simple distribution of informative material or, on the other hand, it may mean the measurement of behaviours and results. examples: - include at least 1 equity among the assessment goal s and indicators of managers - equity goal and indicator in the annual budget - equity indicators in the hospital panel of strategic indicators (Italy – Aosp Fe)

STANDARD 1
14
MEASURABLE ELEMENT 1.1.3 The organisation’s leaders and decision makers actively promote equity in their work. [Evidence: Equity is included in performance management arrangements for all leaders and decision makers (e.g. Guidance for managers requires them to have at least one performance indicator which addresses equity).]
C – APPLICABILITY
• C1 – Legislation:
1. This is a legal requirement in Australian hospitals . It is also achieved via the yearly mandatory Staff Performance Appraisals , the Staff Supervision Framework , and other training. (Australia)
• C2 – Organisation:
1. As previously stated – equity of access is articulated as a guiding princi ple but not as a core value . Values of the organisation include respect; compassion; integrity (including acting fairly); excellence and collaboration; so would be more likely to see these terms included in performance management arrangements rather than equity. (Australia)
2. The measurable element seems skewed towards organization's with large infr astructures and formalized processes . (Canada – Ontario)
STANDARD 1
15
SUBSTANDARD 1.2 The organization’s research, monitoring and evaluation systems can measure equity performance. Codes frequency: Code Freq. A1-Re-wording 4
B3-Revision 1
Quotations N = 5
Bold text = critical issue Blue Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: The organisation’s quality system measures equity performance. (Norway)
2. Please consider the following rewording of substandard 1.2: The organisation’s research, monitoring, and evaluation systems measure equity p erformance . (Canada – Ontario)
3. Change the wording to be more specific, e.g. the organization measures equity performance
through its research, monitoring, and evaluation sy stems . (Canada Ontario)
4. “Can” should be deleted . Revised substandard should read “The organisation’s research, monitoring and evaluation systems measure equity performance.” (Canada Ontario)
B – RELEVANCE
• B3 – Revision:
1. When conducting research and surveys, people from non-English speaking (NES) Backgrounds, particularly those with low English fluency, have to be included with the aim to work towards representational inclusion of all groups. A minimum of 25% of patients involved in research projects at Northern Health must be from NES background. The transcultural & Language Services (TALS) Department is consulted in the process to determine culturally appropriate strategies and provision of language services. (Australia)

STANDARD 1
16
MEASURABLE ELEMENT 1.2.1 The organization collects data on the way people access its services to understand how service utilization patterns reflect the demography and meet the needs of the catchment area. [Evidence: Data are available about who is and who is not using its services according to the same nee d (e.g. Compare data on access of service users with statistics about social stratification, gender, nationality, origin, religion, aboriginal, ethnicit y, disability and age breakdown of the population).] Codes frequency: Code Freq. C2-Organisation 9
A1-Re-wording 4
B3-Revision 2
C1-Legislation 2
A2-Re-structuring 1
B1-Inclusion 1
D2-Theoretical foundations 1
Quotations N = 20
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. The sentence is too long . (Norway)
2. "The organisation collects data on access to services considering the social-demogr aphic, cultural and vulnerability characteristics of the c itizens in the catchment area. " (Italy – Reggio Emilia)
3. Change to: The organisation provides health care adapted to demography and needs of the
catchment area. (Norway)
4. […] To reflect this standard’s focus on policy, please consider the following rewording of measureable element 1.2.1: The organisation has a policy and procedures to systematically collect and disseminate data on the way people acce ss its services to understand how service utilisation patterns reflect the demography and meet the needs of its client populations. [Evidence: Data are available about who is and who is not using its services according to the needs of the client populations (e.g. compare data on access of service users with statistics about social stratification, sex, gender, nationality, origin, religion, aboriginal status, ethnicity, disability and age breakdown of the population).] (Canada – Ontario)
• A2 – Re-structuring:
1. This substandard have much similarities with standards regarding access to the services.
(Finland)
B – RELEVANCE
• B1 – Inclusion:
1. Add another follow up point that the organization systematically reviews and acts on addressing gaps identified by the data . Often data is collected but never used and does not get translated into action. (Canada – Ontario)

STANDARD 1
17
MEASURABLE ELEMENT 1.2.1 The organization collects data on the way people access its services to understand how service utilization patterns reflect the demography and meet the needs of the catchment area. [Evidence: Data are available about who is and who is not using its services according to the same nee d (e.g. Compare data on access of service users with statistics about social stratification, gender, nationality, origin, religion, aboriginal, ethnicit y, disability and age breakdown of the population).]
• B3 – Revision:
1. Data needs to be collected in a cohesive manner at registration . Currently clientele is
identified by postal codes, by aboriginal status for remote users, by language for other language speakers. Many services collect their own data. Need to collect for race, ethnicity, literacy, language and SES on a global scale (Canada – Quebec)
2. Missing examples of the methods for collecting the data (Norway)
C – APPLICABILITY
• C1 – Legislation:
1. The Andalusian Digital Medical History partially records the indicators listed above. Maybe too much elements listed . We consider as mandatory to register the country of origin and religion. (Spain)
2. In the Catalan health system, this is done (partially) by the 'CatSalut ' (the health services
planning and purchasing institution- public organization reporting to the Department of Health). Public hospitals can access this information. (Spain)
• C2 – Organisation:
1. The field of application at the hospital is more limited and might require in-depth or ad hoc epidemiologic studies, not all statistics are current (Italy – Modena)
2. "The way people access" Difficult to get data and information on people who don’t access
and use the services . Easier to get data on users classified by sex, age, nationality….(Italy – Cesena)
3. There are data available on those who access the services but no data on those who do not
access them . (Italy – Reggio Emilia)
4. ‘Catchment area’ is not applicable to the Hospital for Sick Children as it does not have a discrete catchment area; patients come from local, national, and internation al origins . As an alternative, ‘client population ’ would be a more general term for organizations that do not have discrete catchment areas. […] (Canada – Ontario)
STANDARD 1
18
MEASURABLE ELEMENT 1.2.1 The organization collects data on the way people access its services to understand how service utilization patterns reflect the demography and meet the needs of the catchment area. [Evidence: Data are available about who is and who is not using its services according to the same nee d (e.g. Compare data on access of service users with statistics about social stratification, gender, nationality, origin, religion, aboriginal, ethnicit y, disability and age breakdown of the population).]
5. Although clear and relevant, difficult to meet. We collect much of the demographic information suggested, but do not have the resources to do more than a superfi cial analysis of how we compare to the population of Toronto.
6. Not clear how those not accessing services are being measured/accounted for (Canada – Quebec)
7. some data are collected, no systematism, important indicators are not collected on the administrative data base (spoken languages, country of birth) (Switzerland)
8. The Andalusian Digital Medical History partially records the indicators listed above. Maybe too much elements listed . We consider as mandatory to register the country of origin and religion. (Spain)
9. Discuss whether any special requirements should be recorded on all women. Currently, our IT system does not capture language proficiencies and disability data . (Ireland)
D – GENERAL CONSIDERATIONS OF THE TOOL
• D2 – Theoretical foundations:
1. ‘Catchment area ’ is not applicable to the Hospital for Sick Children as it does not have a discrete catchment area; patients come from local, national, and international origins. As an alternative, ‘client population ’ would be a more general term for organizations that do not have discrete catchment areas. […] (Canada – Ontario)

STANDARD 1
19
MEASURABLE ELEMENT 1.2.2 The organization collects data on the health status and inequalities in its catchment area. [Evidence: Data or information collection about the health needs of relevant populations which aloe health inequalitites to be identified (e.g. Epidemiological and socio-demographic data in relevant areas/districts and target population groups; Quantitative and qualitative information).] Codes frequency: Code Freq. C2-Organisation 6
A1-Re-wording 4
C1-Legislation 4
B3-Revision 1
A3-Meanings 1
D1-Define target groups 1
Quotations N = 17
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. To reflect this standard’s focus on policy, please consider the following rewording of measurable element 1.2.2: The organisation has a policy and procedures to systematically collect and disseminate data on the health status and inequalities of its client populations . (Canada – Ontario)
2. Also, not every organization has a well defined catchment area – specialty hospitals for example have a broader reach than community hospitals.
3. “catchment ”? (Canada – Quebec)
4. Suggested change: “The organisation collects and has access to data on the health status and inequalities in its catchment area.” (Canada Ontario)
• A3 – Meanings:
1. […] The use of the term “inequalities ” as opposed to “inequities ” makes the element unclear because they mean different things and it is unclear which one is intended. (Canada – Ontario)
B – RELEVANCE
• B3 – Revision:
1. This element should also include people with a disability, and GLBTI people . (Australia)
C – APPLICABILITY
• C1 – Legislation:
1. The ASMN hospital provides services based on the supply agreements established with the health care unit , its client. Therefore, the health care unit collects the data on the health status of the catchment area, based on which it decides what and how much to ask the ASMN for. (Italy – ASMN Re)

STANDARD 1
20
MEASURABLE ELEMENT 1.2.2 The organization collects data on the health status and inequalities in its catchment area. [Evidence: Data or information collection about the health needs of relevant populations which aloe health inequalitites to be identified (e.g. Epidemiological and socio-demographic data in relevant areas/districts and target population groups; Quantitative and qualitative information).]
2. The Health Districts collect specific data on so cial and health inequalities in the primary healthcare, where the health promotion is assumed. Conceptually it repeats the previous section. We believe it is more suitable for the Primary Healthcare . (Spain)
3. It's a function of the services of the Regional Health Administration (Spain)
4. We understand that this measurable element, in a planned health market as is Catalan, belongs to 'CatSalut' . (Spain)
• C2 – Organisation:
1. The ASMN hospital provides services based on the supply agreements established with the health care unit, its client . Therefore, the health care unit collects the data on the health status of the catchment area, based on which it decides what and how much to ask the ASMN for. (Italy – ASMN Re)
2. "health status and inequalities in " Lots of quantity data Less quality data collected Partially or
yes? We have chosen “yes” because we do as much as possible with the available resources; even if the information systems only collect some data ; only some of the available data is processed; not much quality data is collected . (Italy – Cesena)
3. Fulfilling the element: no but information from the Community Health Services about
contagious diseases which are detected in certain groups does reach us. (The Netherlands)
4. This is a difficult question to answer for our organization and may be for others. It isn’t done on a regular or formal basis by any of the departments responsible for reporting, although it may be done on an ad hoc basis as needs arise. […](Canada – Ontario)
5. mainly through specific research project (Switzerland)
6. The Health Districts collect specific data on social and health inequalities in the primary
healthcare, where the health promotion is assumed. Conceptually it repeats the previous section. We believe it is more suitable for the Primary Healthcare . (Spain)

STANDARD 1
21
MEASURABLE ELEMENT 1.2.2 The organization collects data on the health status and inequalities in its catchment area. [Evidence: Data or information collection about the health needs of relevant populations which aloe health inequalitites to be identified (e.g. Epidemiological and socio-demographic data in relevant areas/districts and target population groups; Quantitative and qualitative information).]
D – GENERAL CONSIDERATIONS OF THE TOOL
• D1 – Define target groups:
1. This element should also include people with a disability, and GLBTI people . (Australia)

STANDARD 1
22
MEASURABLE ELEMENT 1.2.3 The organization uses this data to continually improve equity in the accessibility and quality of health care. [Evidence: Evidence-based outcomes showing service equity improvements (e.g. Documented variation in the number and range of individuals accessing a diabetes or asthma clinic).] Codes frequency: Code Freq. C2-Organisation 5
A1-Re-wording 4
B3-Revision 2
C1-Legislation 1
D2-Theoretical foundations 1
B2-Exclusion 1
C3-Social-economical context 1
D3-Tool issues 1
Quotations N = 16
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. "to continually improve equity in the accessibility and quality " Clarify better what is meant by “continually ”: Monthly? Every three months? Annually? Every two years? Clarify better “this data ”: Which? All of it or part of it?
2. Or change to: the organisation uses this data to continually improve equity in health care .
(Norway)
3. To reflect this standard’s focus on performance monitoring systems, please consider the following rewording of measureable element 1.2.3: The organization has a quality improvement process which utilizes client health an d service utilization data to continually improve equity in the accessibility and quality of health care, and disseminate the results of this process . (Canada – Ontario)
4. I believe that accessibility and quality are 2 v ery different things . Perhaps they should not
be tied together as quality of health care is often expected by non-marginalized persons and is used as a barometer of health status (private bed vs ward, front-of-the-line vs a waiting list, full-service vs limited resources.) Even before quality, accessibility is often wished-for when it relates to marginalized groups. In an ideal situation we hope that high quality health care [when it exists] is fully accessible regardless of status. (Canada – Quebec)
B – RELEVANCE
• B2 – Exclusion:
1. Comment: This element should be removed if 1.2.1 is being changed.
• B3 – Revision:
1. Evidence and examples are not coherent with sub-standard (Italy – Lucca)

STANDARD 1
23
MEASURABLE ELEMENT 1.2.3 The organization uses this data to continually improve equity in the accessibility and quality of health care. [Evidence: Evidence-based outcomes showing service equity improvements (e.g. Documented variation in the number and range of individuals accessing a diabetes or asthma clinic).]
2. Good Need to add a point regarding acting on the evidence in a timely manner and having reporting/accountability mechanisms in place . Often the gaps are known for many years and there is an abundance of evidence to support it but the organization does not act on it. (Canada – Ontario)
C – APPLICABILITY
• C1 – Legislation:
1. This criteria is more applicable in Primary Healthcare Attention . (Spain)
• C2 – Organisation:
1. For specific groups of users (for example, maternity and children’s unit) (Italy – Modena)
2. "[Evidence: Evidence-based outcomes showing service equity improvements " - The definition of this element seems to refer to the fact that the outcomes of the monitoring are shared and are translated into specific objectives of the unit plan , and not that there are already results (Italy – Ausl Re)
3. however, as said, available data are limited (Switzerland)
4. This criteria is more applicable in Primary Healthcare Attention . (Spain)
5. It is difficult to collect these data on a regular basis . (Spain)
• C3 – Social-economical context:
1. […] Very challenging indicator and very difficult to fulfil in periods of economic cri sis and organisational difficulties within health care units and the health care system. (Italy – Ausl Cesena)

STANDARD 1
24
MEASURABLE ELEMENT 1.2.3 The organization uses this data to continually improve equity in the accessibility and quality of health care. [Evidence: Evidence-based outcomes showing service equity improvements (e.g. Documented variation in the number and range of individuals accessing a diabetes or asthma clinic).]
D – GENERAL CONSIDERATIONS OF THE TOOL
• D2 – Theoretical foundations:
1. I believe that accessibility and quality are 2 very different things . Perhaps they should not be tied together as quality of health care is often expected by non-marginalized persons and is used as a barometer of health status (private bed vs ward, front-of-the-line vs a waiting list, full-service vs limited resources.) Even before quality, accessibility is often wished-for when it relates to marginalized groups. In an ideal situation we hope that high quality health care [when it exists] is fully accessible regardless of status. (Canada – Quebec)
• D3 – Tool issues:
1. More information on how this can be measured would be helpful. (Australia)

STANDARD 1
25
SUBSTANDARD 1.3 The organization has a plan, resources and budget to promote equity. This plan is integrated with existing performance management and accountability systems. Codes frequency: Code Freq. A2-Re-structuring 4
A1-Re-wording 2
C2-Organisation 1
B3-Revision 1
C1-Legislation 1
C3-Social-economical context 1
A3-Meanings 1
D1-Define target groups 1
B1-Inclusion 1
Quotations N = 13
Bold text = critical issue Blue Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: The organisation has an action plan, resources and budget to promote equity. This action plan is integrated with existing management systems . (Norway)
2. In university or large hospital, the standard should not restrict to head management but also to departments managements . (Switzerland)
• A2 – Re-structuring:
1. Move substandard 1.3 (equity strategy) to the very beginning , as this creates a more effective narrative for the rest of the standard.
2. It would be interesting that substandard 1.3 were at the beginning of the standard (it may be
more logical to ask first if there exist any equity strategy and then valuating if there is an impact assesment or improvement areas). (Spain)
3. To improve the narrative of the Standard, this should really be at the front - swap 1.3 for 1.1 .
(Scotland)
4. Plans and budgeting for resources are 2 separate issues and should be teased out more - plans can be written up but are often not achieved due to lack of realistic funding / budgets to meet the strategies, when disadvantaged groups are not given equal priority. (Australia)
• A3 – Meanings:
1. Clarify "a plan, resources and budget ".(Italy – Cesena)
STANDARD 1
26
SUBSTANDARD 1.3 The organization has a plan, resources and budget to promote equity. This plan is integrated with existing performance management and accountability systems.
B – RELEVANCE
• B1 – Inclusion:
1. […] The standards generally are weak on workforce equality. This standard is probably the most appropriate for inclusion of one or more substandards relating to how the organisation ensures that its employees are able to achieve their potential regardless of their equity characteristic. In addition, a substandard about dignity at work (being able to be oneself at work regardless of equality characteristic, with no risk of bullying or harassment) could usefully appear here. (Scotland)
• B3 – Revision:
1. In university or large hospital, the standard should not restrict to head management but
also to departments managements . (Switzerland)
C – APPLICABILITY
• C1 – Legislation:
1. Rather than one “Equity Plan” the organisation has several plans. This is partly due to government/funding body policy requirements . For example the organisation has a Cultural Responsiveness Plan, and an Aboriginal Health Outcomes Plan. Some program areas are required to have a separate Diversity Plan; the organisation does not yet have a Disability Action Plan. […] (Australia)
• C2 – Organisation:
1. Rather than one “Equity Plan” the organisation has several plans . This is partly due to
government/funding body policy requirements. For example the organisation has a Cultural Responsiveness Plan, and an Aboriginal Health Outcomes Plan. Some program areas are required to have a separate Diversity Plan; the organisation does not yet have a Disability Action Plan. […] (Australia)
STANDARD 1
27
SUBSTANDARD 1.3 The organization has a plan, resources and budget to promote equity. This plan is integrated with existing performance management and accountability systems.
• C3 – Social-economical context:
1. […] Hence it would be difficult for this sub-standard to be applicable while there are competing
compliance requirements that require resourcing, monitoring and reporting of mul tiple plans . (Australia)
D – GENERAL CONSIDERATIONS OF THE TOOL
• D1 – Define target groups:
1. In university or large hospital, the standard should not restrict to head management but also to departments managements . (Switzerland)

STANDARD 1
28
MEASURABLE ELEMENT 1.3.1 The organization has an equity plan or strategy which is rewiewed regularly. [Evidence: Written strategy or plan, which sets out the actions it will take to address equity issues ( e.g. The equity plan includes mission statement, objectives, allocation of resources, duration, responsabilities).] Codes frequency: Code Freq. A1-Re-wording 3
C2-Organisation 3
B3-Revision 1
Quotations N = 7
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. May be useful to define a timeframe instead of “regularly ” (Australia)
2. Please consider the following rewording of measurable element 1.3.1: The organisation has a specific equity plan, which is reviewed regularly. [Evidence: A written equity plan, which sets out actions that will be taken to address equity issues (e.g. The equity plan includes a mission statement, objectives, allocation of resources, duration, responsibilities).] (Canada – Ontario)
3. Recommend that “regularly ” be revised to “annually ” to motivate an action agenda on equity. (Canada – Ontario)
B – RELEVANCE
• B3 – Revision:
1. Somehow, the budget should be included in this indicator. (Norway)
C – APPLICABILITY
• C2 – Organisation:
1. Plan or strategy - We do not have a plan with these characteristics (Italy – Cesena)
2. Our organisation operates according to the guidelines and principles outlined in the CNCA Planning Document , as the latter ensure that the correct approach is taken to deal with problems of equity. From the standpoint of methods used, a basic requirement for all our actions is “suspending judgment” when dealing with our users - an element that guarantees the equal treatment of those who take advantage of our services (italy – Pisa)
3. there's no unified long-term policy but the head management is aware of this issue and
specific allowances for specific equity project have been distributed. (Switzerland)
STANDARD 1
29
MEASURABLE ELEMENT 1.3.2 Implementation of the organisation’s equity plan is included in the overall strategy of the organisation. [Evidence: The overall strategy makes specific reference to the equity plan (e.g. The equity plan has equal weight to quality improvement and risk management objectives and is integrated with them).] Codes frequency: Code Freq. C2-Organisation 2
B2-Exclusion 2
A1-Re-wording 1
A2-Re-structuring 1
B1-Inclusion 1
C1-Legislation 1
Quotations N = 8
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: Implementation of the equity plan is included in the overall strategy of the organisation. (Norway)
• A2 – Re-structuring:
1. Please consider dividing this measureable element into the followin g 2 measureable
elements to clarify the progression of steps an organization may take to adopt equitable policies and practices. [1] An equity strategy is included in the overall strategy of the organization. [Evidence: The overall strategy makes specific reference to the equity priorities.] [2] The organization had a procedure for implementing an equity plan and eva luating its impact . [Evidence: There is a written procedure for implementing the equity plan and a process for evaluating the plan which is integrated into the general quality improvement and risk management processes of the organization.] (Canada – Ontario)
B – RELEVANCE
• B1 – Inclusion:
1. Please consider dividing this measureable element into the followin g 2 measureable elements to clarify the progression of steps an organization may take to adopt equitable policies and practices. [1] An equity strategy is included in the overall strategy of the organization. [Evidence: The overall strategy makes specific reference to the equity priorities.] [2] The organization had a procedure for implementing an equity plan and eva luating its impact . [Evidence: There is a written procedure for implementing the equity plan and a process for evaluating the plan which is integrated into the general quality improvement and risk management processes of the organization.] (Canada – Ontario)
• B2 – Exclusion:
1. Unnecessary , 1.3.1. is sufficient (Sweden) 2. This is very similar to the previous item . Perhaps a single measurable element could be
developed. (Italy – Pisa)

STANDARD 1
30
MEASURABLE ELEMENT 1.3.2 Implementation of the organisation’s equity plan is included in the overall strategy of the organisation. [Evidence: The overall strategy makes specific reference to the equity plan (e.g. The equity plan has equal weight to quality improvement and risk management objectives and is integrated with them).]
C – APPLICABILITY
• C1 – Legislation: 1. The unit strategy is strongly connected in our case to regional planning which promotes the
development of equity policies. (Italy – Ausl Re)
• C2 – Organisation:
1. Agree integration of the equity plan (and/or related/similar plans) as part of the organisational strategy is essential (Australia)
2. This element is key to ensuring that the organisation's equity plans are mainstreamed into its strategic objectives. (Scotland)

STANDARD 1
31
MEASURABLE ELEMENT 1.3.3 The organization includes progress on equity in its mainstream performance reports. [Evidence: Mainstream reports include specific equity measures (e.g. Equity measures in patient satisfaction, complaints and patient safety reports ).] Codes frequency: Code Freq. A1-Re-wording 4
A3-Meanings 4
B2-Exclusion 2
C2-Organisation 1
B3-Revision 1
C3-Social-economical context 1
Quotations N = 13
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: Equity is included in management (mainstream perfor mance) reports . Or: Progress may be replaced with achievement – The organisation includes achievement on equity in its mainstream performance reports. (Norway)
2. The tools must be explained clearly (Italy – Modena)
3. Change to: The organisation demonstrates the progress on equity in its mainstream
performance reports. (Norway)
4. Please consider the following rewording of measureable element 1.3.3: Progress on equity indicators is presented in organizational performan ce reports . [Evidence: Organizational progress reports include specific equity performance measures (e.g. Use of interpreter services, patient satisfaction measures i.e., patients perceptions of staff’s cultural sensitivity, accessibility of services, inclusiveness of service delivery, patient safety reports, patient complaint reports).] (Canada – Ontario)
• A3 – Meanings:
1. "progress " - "performance reports ". Clarify better what is meant by “progress” and what type
of performance indicators to analyse (Italy – Cesena)
2. Use of the term "mainstream " is ambiguous and should be defined / clarified for this context. (Canada – Ontario)
3. What is “progress on equity”? could not ansie (Canada – Quebec)
4. Need to clarify what “mainstream ” means . (Canada – Ontario)
B – RELEVANCE
• B2 – Exclusion:
1. Comment: This element can be used as an example to 1.2.3 (Norway)
STANDARD 1
32
MEASURABLE ELEMENT 1.3.3 The organization includes progress on equity in its mainstream performance reports. [Evidence: Mainstream reports include specific equity measures (e.g. Equity measures in patient satisfaction, complaints and patient safety reports ).]
2. As above, unnecessay (Sweden)
• B3 – Revision:
1. Good. “Family experience ” should be included in the evidence example as a comprehensive performance measure. (Canada – Ontario)
C – APPLICABILITY
• C2 – Organisation:
1. We use tools for measuring Customer Satisfaction and receive complaints while managing our services. Their use also depends on the commissioning agency agreeing to this type of survey and to the sharing of the relative tools. (Italy – Pisa)
• C3 – Social-economical context: 1. Equity measures in patient satisfaction reports difficult to assess when numbers of
respondents in rural areas from some demographic groups are so low – hard to apply. (Australia)
STANDARD 1
33
SUBSTANDARD 1.4 The organization ensures that staff at all levels has awareness and competence to address inequities in health care. Codes frequency: Code Freq. A1-Re-wording 2
C2-Organisation 1
B3-Revision 1
D3-Tool issues 1
Quotations N = 5
Bold text = critical issue Blue Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: The organisation facilitates that staff at all levels has awareness and competence to address inequities in health care. (Norway)
2. Maybe, it would be interesting to say 'staff at all leves ENHANCES awareness…' It is a never-ending process. (Spain)
B – RELEVANCE
• B3 – Revision:
1. Include reference to specific training (Australia)
C – APPLICABILITY
• C2 – Organisation:
1. This is an extremely difficult task with the number of staff in the organisation – not all have access to computers - & with regular staff turnover . The “competence” issues that we concentrate on are mainly related to language services, gender issues related to access of interpreter, spiritual needs and dietary preferences, BUT at an organisational level the leaders have not been able to understand that staff “competence” cannot occur, or is badly hampered, when the organisation is not committed enough to make the resources available for staff to be “competent” i.e. commitment to an adequate language service budget, IT systems that support identification & timely tracking of clients needing interpreters or the ability to capture “religious affiliation” data, resources to ensure “chapel” type facilities are inclusive of the needs of Moslems by provision of separate prayer space & ablutions areas. Too much emphasis is being placed on staff being culturally “competent”, when this cannot occur without the organisation first being culturally “competent” . (Australia)

STANDARD 1
34
SUBSTANDARD 1.4 The organization ensures that staff at all levels has awareness and competence to address inequities in health care.
D – GENERAL CONSIDERATIONS OF THE TOOL
• D3 – Tool issues:
1. Is it possible to combine all different competence issues under one s tandard ? Now there are one part here and another elsewhere. This does not give good tool to improve staff competence comprehensively. (Finland)
STANDARD 1
35
MEASURABLE ELEMENT 1.4.1 The organization has a comprehensive programme for equity training and challenging attitudes towards equity issues for all staff. [Evidence: Training plans show appropriate training is delivered to all staff, including senior staff ( e.g. The plan sets out which staff should receive basic awareness training, and which should receive more advanced training on specific).] Codes frequency: Code Freq. A1-Re-wording 5
C2-Organisation 3
D2-Theoretical foundations 2
A3-Meanings 1
Quotations N = 11
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Change to: The organisation has a programme for equity training and raising awareness of equity issues for all staff. (Norway)
2. Change to: The organisation has an equity training programme for all staff that promotes
positive attitudes . (Norway) 3. Remove "comprehensive" . Remove "challenging attitudes towards" and replace with
"promoting " (Norway) 4. Equity training includes ‘challenging attitudes towards equity issues’ and thus should
not be presented as a separate component from the overall training. In addition, ‘equity education ’ is a more accurate term as it includes awareness raising, knowledge acquisition, and skill building, whereas training often focuses on skill building alone. Please consider using the term ‘equity education’, rather than ‘equity training’. Please consider the following rewording of measureable element 1.4.1: The organisation has a comprehensive programme for equity education . [Evidence: Education plans show appropriate education is delivered to all staff, including senior staff, and is reflective of the education needs of different staff groups (e.g., The plan sets out which staff should receive basic awareness training and which staff should receive more advanced training on specific equity issues).] (Canada – Ontario)
5. Change “challenging ” to “challenges ”. (Canada – Ontario) • A3 – Meanings:
1. "a comprehensive programme for equity training " clarify (Italy – Cesena)
STANDARD 1
36
MEASURABLE ELEMENT 1.4.1 The organization has a comprehensive programme for equity training and challenging attitudes towards equity issues for all staff. [Evidence: Training plans show appropriate training is delivered to all staff, including senior staff ( e.g. The plan sets out which staff should receive basic awareness training, and which should receive more advanced training on specific).]
C – APPLICABILITY
• C2 – Organisation:
1. Standard is OK so long as the definition of equity training is understood broadly. Some staff have undertaken equity training, but our major training priority and investment at prese nt is in cultural competence and cultural safety training for staff and managers . Once again, application of the element is likely to be constrained by competition for staff time and resources needed to comply with specific equity related policy e.g. Cultural Responsiveness, Improving Care for Aboriginal Patients etc. (Australia)
2. The measurable element seems to be very ambitious . (Spain) 3. at the moment, there is no unified program for all but different teaching activities for different
audiences exist (Switzerland)
D – GENERAL CONSIDERATIONS OF THE TOOL
• D2 – Theoretical foundations:
1. Standard is OK so long as the definition of equity training is understood broadly. Some staff have undertaken equity training , but our major training priority and investment at present is in cultural competence and cultural safety training for staff and managers. Once again, application of the element is likely to be constrai ned by competition for staff time and resources needed to comply with specific equity rel ated policy e.g. Cultural Responsiveness, Improving Care for Aboriginal Patients etc. (Australia)
2. Equity training includes ‘challenging attitudes towards equity issues’ and thus should not be
presented as a separate component from the overall training. In addition, ‘equity education’ is a more accurate term as it includes awareness raisi ng, knowledge acquisition, and skill building, whereas training often focuses on skill b uilding alone . Please consider using the term ‘equity education’, rather than ‘equity training’. […] (Canada – Ontario)
STANDARD 1
37
MEASURABLE ELEMENT 1.4.2 The organisation’s mainstream training includes learning about equity. [Evidence: Mainstream training is reviewed for inclusion if equity issues where this is appropriat e (e.g. Equity is part of the core induction training and training updates).] Codes frequency: Code Freq. B2-Exclusion 5
A3-Meanings 4
A1-Re-wording 3
D2-Theoretical foundations 1
D3-Tool issues 1
Quotations N = 14
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Prefer to call it “education ” rather than “training ” as the main emphasis is to get a staff “awakening” about their own cultural beliefs / prej udices and start treating individuals rather than stereotypes of “cultural groups”, which has occurred over decades in Australia. The education sessions are based on human rights and cultural humanism rather than “training” , which in the health industry is closely aligned to the ability to do certain tasks & use checklists – not an approach that works well when dealing with concepts of equity. (Australia)
2. "(e.g. Equity is part of the core induction training and cross-sectional courses ).]" (Italy – Ausl
Re)
3. It is recommended to use the word ‘core ’ rather than ‘mainstream’ . It is recommended that ‘education’ be added to this measureable element . Please consider the following rewording of measureable element 1.4.2: The organization’s core education and training includes learning about equity. [Evidence: Core education and training are reviewed and modified for inclusion of equity issues where appropriate (e.g. Equity is part of the core induction training and training updates).] (Canada – Ontario)
• A3 – Meanings:
1. "Mainstream training " clarify (Italy – Cesena)
2. Mainstream should be defined / clarified (Canada – Ontario)
3. Good but the use of the term “mainstream ” is problematic because it positions equity training
as marginalized training when the assumed intent is for equity to be part of all training inclusive of specific and separate training on equity issues. This step needs to be integrated in a systematic way rather than being left to individual trainers/course developers’ discretion. There needs to be some monitoring to ensure this does happen. (Canada – Ontario)
4. Clarify meaning of “mainstream ” (Canada – Ontario)
STANDARD 1
38
MEASURABLE ELEMENT 1.4.2 The organisation’s mainstream training includes learning about equity. [Evidence: Mainstream training is reviewed for inclusion if equity issues where this is appropriat e (e.g. Equity is part of the core induction training and training updates).]
B – RELEVANCE
• B2 – Exclusion:
1. This indicator should be included in 1.4.1 as an example (Norway)
2. Overlapping with 1.4.1.? (Finland)
3. Comment: Should be included as an example to 1.4.1 (Norway)
4. Include this indicator as an example for 1.4.1 (Norway)
5. We can't see the differences between this and the previous measurable element. (Spain)
D – GENERAL CONSIDERATIONS OF THE TOOL
• D2 – Theoretical foundations:
1. Prefer to call it “education” rather than “training” as the main emphasis is to get a staff “awakening” about their own cultural beliefs / prej udices and start treating individuals rather than stereotypes of “cultural groups”, which has occurred over decades in Australia . The education sessions are based on human rights and cultural humanism rather than “training” , which in the health industry is closely aligned to the ability to do certain tasks & use checklists – not an approach that works well when dealing with concepts of equity. (Australia)
• D3 – Tool issues:
1. Not clear how to measure (Canada – Quebec)

STANDARD 1
39
MEASURABLE ELEMENT 1.4.3 The organization monitors and evaluates the effectiveness of its equity training. [Evidence: Data is available on the number of staff who has completed equity training. Mechanisms are in place to evaluate changes in staff attitudes, knowledge and skills (e.g. Credit system for on going learning and professional development; Pre and post assessment of training; Mystery shoppers; Patient feedback; Complaints or other similar sources to evaluate training).] Codes frequency: Code Freq. C2-Organisation 6
A3-Meanings 2
A1-Re-wording 2
B3-Revision 2
B2-Exclusion 1
C3-Social-economical context 1
Quotations N = 14
Bold text = critical issue Green Bold text = proposal
A – CLARITY
• A1 – Re-wording:
1. Evaluating effectiveness is rather demanding . We suggest using term input instead of effectiveness . (Finland)
2. Please consider the following rewording of measureable element 1.4.3: The organisation
monitors and evaluates the effectiveness of its equity education . (Canada – Ontario) • A3 – Meanings:
1. Clarify the examples better (what is mystery shopping?)
2. Mystery Shopper - what is it? needs to be defined (Canada – Quebec)
B – RELEVANCE
• B2 – Exclusion:
1. Comment: Should be included as an example to another element . (Norway) • B3 – Revision:
1. The examples are too general and vague . That puts you on the wrong foot (The Netherlands) 2. Family members should be explicitly mentioned as an evidence example . They are an
important and separate stakeholder. (Canada – Ontario)
C – APPLICABILITY
• C2 – Organisation:
1. Measuring change of attitudes can be infeasible ? Otherwise, it seems to be a very difficult and complicated process. (Norway)

STANDARD 1
40
MEASURABLE ELEMENT 1.4.3 The organization monitors and evaluates the effectiveness of its equity training. [Evidence: Data is available on the number of staff who has completed equity training. Mechanisms are in place to evaluate changes in staff attitudes, knowledge and skills (e.g. Credit system for on going learning and professional development; Pre and post assessment of training; Mystery shoppers; Patient feedback; Complaints or other similar sources to evaluate training).]
2. Very ambitious sub-standard! The element is theoretically applicable, but in practice difficult to apply because thinking about measuring changes in attitudes and knowledge on equity is really difficult! (Italy – Cesena)
3. It is difficult to measure (monitor and evaluate) the change of attitude. (Norway) 4. through research projects onlx, evaluation of effectiveness can't be done through a n
administrative intern monitoring (Switzerland) 5. This is another good one for more sophisticated organisations . (Scotland) 6. Difficult to implement in the present healthcare environment. Excessive requirement for
healthcare organizations . (Spain) • C3 – Social-economical context:
1. Difficult to implement in the present healthcare environment . Excessive requirement for
healthcare organizations. (Spain)
STANDARD 1
41
[MEASURABLE ELEMENT 1.4.4] New Measurable Element suggested Codes frequency: Code Freq. B1-Inclusion 2
C3-Social-economical context 1
Quotations N = 3
Bold text = critical issue Green Bold text = proposal
B – RELEVANCE
• B1 – Inclusion:
1. It is recommended that the following measureable element be included within substandard 1.4 (substandard 1.4 as defined in the supplement document): The organization has procedures in place to continually monitor and eval uate the quality of the health care provision environment . (Canada – Ontario)
2. Suggestion for one more MEASURABLE ELEMENT 1.4.4: "The organisation has a conflict
of interest free method by which disadvantaged grou ps are able to provide feedback on the effectiveness of laws, policy that affect their access to services including the negative consequences (complaints office are not ne cessarily conflict free) -Does the org have a method by which information about its policies or rights adherence effectiveness is made transparent and available? -Are those in leadership roles responsible for implementing and overseeing the law required to regularly report on their activities and the effectiveness with which the law or policy is administered? -Is there regular review of the effectiveness of rights/equity implementation and whether the aims of the law/policy are being achieved? -Are the resources allocated to the law or policy regularly reviewed to ensure that they remain appropriate for its effective implementation? (Canada – Ontario)
C – APPLICABILITY
• C3 – Social-economical context:
1. Improving Include question on if the organisation’s health equity strategy/plan aligns w ith broader framework of funder, province/state, countr y…etc […] (Canada – Ontario)