pulmonary function tutorial,bhutani
TRANSCRIPT

Tutorial: Pulmonary Function--Dr. Bhutani
Clinical Case695 g male neonate with RDS, treated with surfactant and on ventilatory support @ 18 hours age:
Settings: 18 / 5 cm H20 x 45 breaths / min; FiO2 = 0.65
Driving Pressure: 18-5 = 13 cm H20
Arterial Gas: pH = 7.3; PaO2 = 74; PaCO2 = 55 mmHg
Is this baby a candidate for permissive hypercapnia?

Normocapnia varies?
• Maternal: 32 - 34 mmHg (progesterone effect)
• Fetal: 40 - 42 mmHg
• At birthing: 45 - 65 mmHg
• First day : 34 mmHg (progesterone effect)
• After first week : 35 - 42 mmHg
• Term PCA: 35 - 42 mmHg (RR = 40-60/min)
• 52 wks PCA: 35 - 42 mmHg (RR = 20-30/min)

Strategies to Prevent Non-Permissive Hypercapnia
• Define optimum PaCO2 levels
• Level to at which you will intervene• Level to at which you will wean
• Ventilate at optimal FRC
• Continuous monitoring of tidal volume
• Use least pressure for maximal tidal volume
• Facilitate spontaneous breathing
• Consider “dual wean” of driving pressures
• Consider pseudo-adaptive strategies

Alveolar Algebra: Ventilation
• Alveolar Ventilation inversely correlated to PaCO2
• Alveolar Ventilation is (VT-VD) x rate• Provided dead space is constant: proportional
changes in VT or rate will lead to proportional changes in alveolar ventilation and PaCO2.
Based on Pulmonary Gas Law: in a steady state, when inspired CO2 is negligible, then PACO2 = 863 (VCO2 / VA); where, VCO2 is CO2 production; PACO2 is partial pressure of carbon dioxide; 863 is body temp. x std. pressure / standard temperature ( 310 X 760/273 = 863 )

Clinical Case695 g male neonate with RDS, treated with surfactant and on ventilatory support and is now about 18 hours age and has stable vital signs, normotensive and is normoglycemic:
Settings: PIP:18 cm H20; PEEP: 5 cm H20; SIMV: 45 br / min;
Arterial Gas: pH = 7.3; PaO2 = 74; PaCO2 = 55 mmHg
Is the Alveolar Ventilation compromised?
If so, by how much?
Clinical Case695 g male neonate with RDS, treated with surfactant and on ventilatory support and is now about 18 hours age and has stable vital signs, normotensive and is normoglycemic:
Settings: PIP:18 cm H20; PEEP: 5 cm H20; SIMV: 45 br / min;
Arterial Gas: pH = 7.3; PaO2 = 74; PaCO2 = 55 mmHg
PaCO2 = 55 mmHg is 35% higher than 40 mmHg
Alveolar Ventilation is decreased by 35%

Clinical Case695 g male neonate with RDS, treated with surfactant and on ventilatory support and is now about 18 hours age and has stable vital signs, normotensive and is normoglycemic:
Settings: PIP:18 cm H20; PEEP: 5 cm H20; SIMV: 45 br / min;
Arterial Gas: pH = 7.3; PaO2 = 74; PaCO2 = 55 mmHg
PaCO2 = 54 mmHg is 35% higher than 40 mmHg
Questions: Do we wean? Which option?

Clinical Case
OPTIONS:
1. No Change
2. Reduce PIP by I cm H20 (17/5) :
Driving Pressure = 12 cm H20
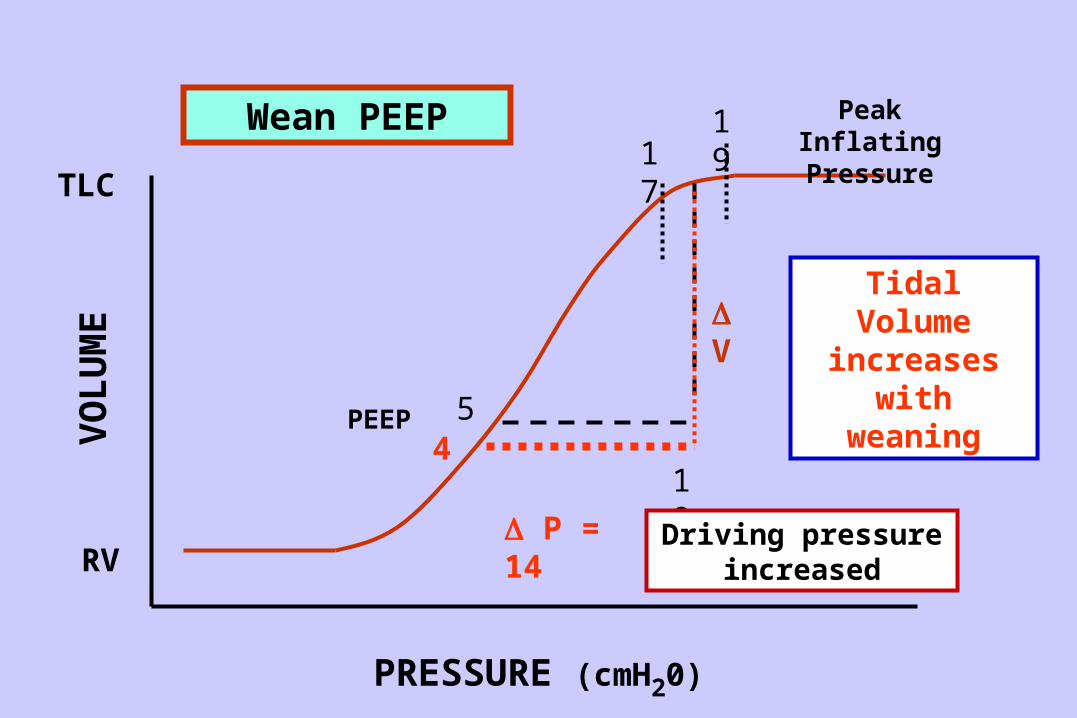
3. Reduce PEEP by I cm H20 (18/4):
Driving Pressure = 14 cm H20
4. Reduce SIMV: Decrease minute ventilation

Clinical Case: Use of Tidal Volume
695 g male neonate with RDS, treated with surfactant and on ventilatory support:
Settings: 18 / 5 cm H20 x 35 breaths / min
Driving Pressure: 18-5 = 13 cm H20
Tidal Volume (measured): = 4 ml (5.7ml/kg)
Effective Compliance: = V / P ; 5.7 / 13 ml/cm H20/kg
Arterial Gas: pH = 7.3; PaO2 = 74; PaCO2 = 55 mmHg

Clinical Case
695 g male neonate with RDS, treated with surfactant and on ventilatory support:
Settings: 18 / 5 cm H20 x 35 breaths / min
Driving Pressure: 18-5 = 13 cm H20
Tidal Volume (measured): = 4.0 ml (5.7 ml/kg)
Effective Compliance: = V / P ; 5.7 /13
= 0.44 ml / cm H20/kg
Arterial Gas: pH = 7.3; PaO2 = 74; PaCO2 = 55 mmHg

Relationship to FRC

Least Intervention or Barotrauma
• Increase Lung Volume : CPAP
• Adequate Lung Inflation : T insp.
• Adequate Lung Deflation : T exp.
• Adjust T insp. / T exp. : by estimating Time Constants
Ventilate at Optimal FRC
Clinical Case
695 g male neonate with RDS, treated with surfactant and on ventilatory support:
Settings: 18 / 5 cm H20 x 45 breaths / min
Driving Pressure: 18-5 = 13 cm H20
Tidal Volume (measured): = 4.0 ml (5.7 ml/kg)
Effective Compliance: = V / P ; 5.7 /13
= 0.44 ml / cm H20
Arterial Gas: pH = 7.3; PaO2 = 74; PaCO2 = 55 mmHg

(PEEP) 5 18 (PIP)
P = 13 cm H20
V = 5.7 ml/kg
Graphic Representation of Ventilator Settings

(PEEP) 5 18 (PIP)
P = 13 cm H20
V = 5.7 ml/kg
V / P = 5.7 / 13 = 0.44 ml/cm H20 /kg
Graphic Representation of Ventilator Settings

5
TLC
RV
19
P = Driving pressure
V
PRESSURE (cmH20)
VO
LU
ME
Peak Inflating Pressure
PEEP
1817
Linear Change in V/ P
V / P = 5.7 / 13 = 0.44 ml/cm H20

5
TLC
RV
19
P = Driving pressure
V
PRESSURE (cmH20)
VO
LU
ME
Peak Inflating Pressure
PEEP
1817
Imaginary P-V relationship

Clinical Case
OPTIONS:
1. No Change
2. Reduce PIP by I cm H20 (17/5) :
Driving Pressure = 12 cm H20
3. Reduce PEEP by I cm H20 (18/4):
Driving Pressure = 14 cm H20
4. Reduce SIMV: Decrease minute ventilation

5
17
18
TLC
RV
19
16
P = 12
V
PRESSURE (cmH20)
VO
LU
ME
Peak Inflating Pressure
PEEP
Wean Peak Inflating Pressure
Tidal Volume decreases
with weaning
Driving pressure decreased
Clinical Case
OPTIONS:
1. No Change
2. Reduce PIP by I cm H20 (17/5) :
Driving Pressure = 12 cm H20
3. Reduce PEEP by I cm H20 (18/4):
Driving Pressure = 14 cm H20
4. Reduce SIMV: Decrease minute ventilation
5
18
TLC
RV
1917
P = 14
V
PRESSURE (cmH20)
VO
LU
ME
Peak Inflating Pressure
PEEP4
Wean PEEP
Tidal Volume increases with
weaning
Driving pressure increased

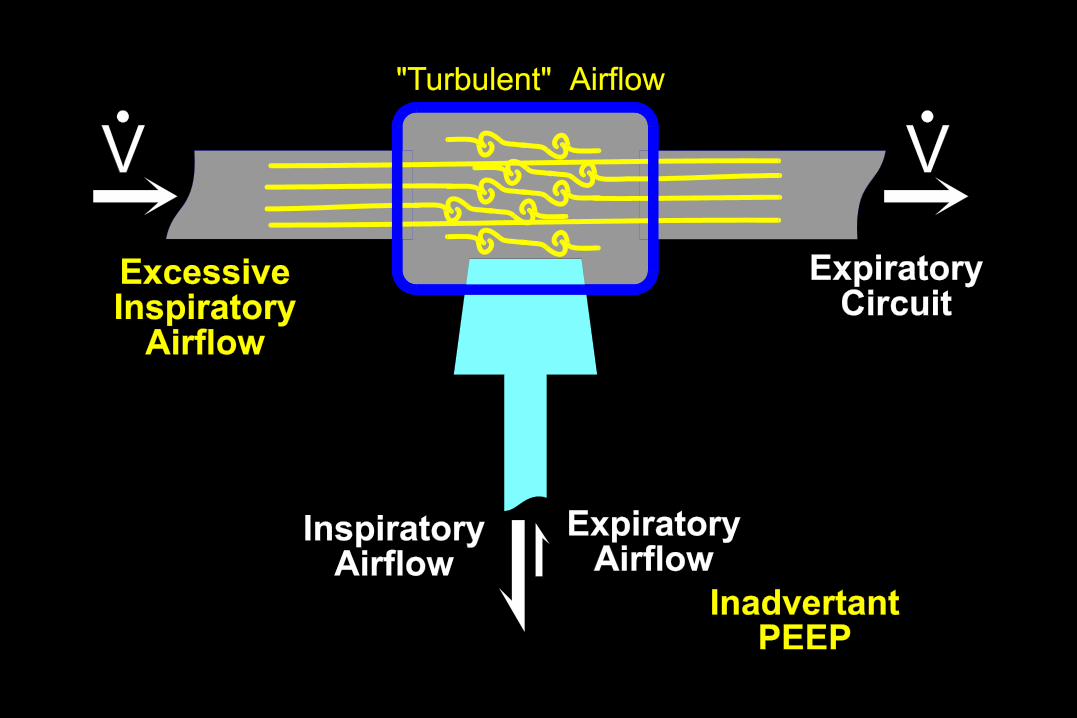
Circuit Airflow
• Airflow that is set, at operator’s discretion, to flow from inspiratory to expiratory circuits.
• Magnitude dependent on patient’s minute ventilation
• Excessive circuit airflow can lead to turbulence and may impede expiratory flow from the patient
• Low flow may limit inspiratory airflow
• Optimal circuit flow is about 5 to 8 fold minute ventilation

Clinical Case
OPTIONS:
1. Dual Wean: Reduce both PIP/PEEP
Dual Wean: 18/5 to 17/4 cm H20
= Driving Pressure
= 13 cm H20

5
17
18
TLC
RV
19
16
P = 13
V
PRESSURE (cmH20)
VO
LU
ME
Peak Inflating Pressure
PEEP
4
DUAL WEAN: concurrent wean of both PIP and PEEP
Tidal Volume increases with
weaning
Tidal Volume increases with
weaning
Driving pressure unchanged
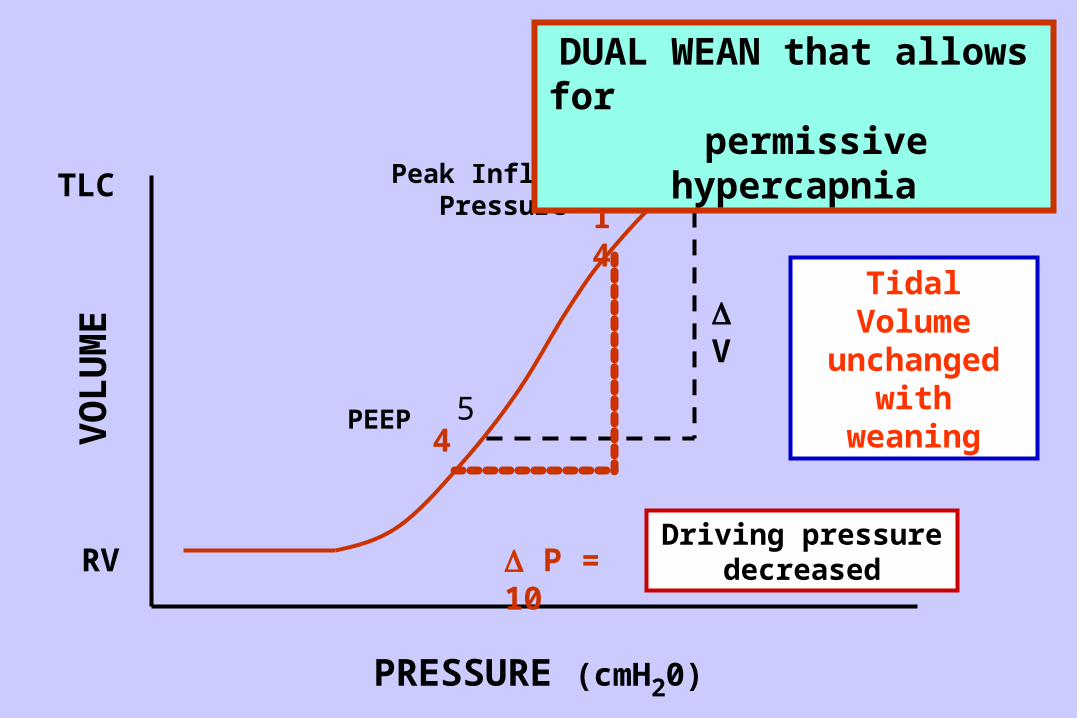
5
18TLC
RV
14
P = 10
V
PRESSURE (cmH20)
VO
LU
ME
Peak Inflating Pressure
PEEP4
DUAL WEAN that allows for permissive
hypercapnia
Tidal Volume unchanged
with weaning
Driving pressure decreased

Clinical Case • PaCO2 = 55 torr at 18/5:
• IATROGENIC HYPERCAPNIA secondary to ventilation at “flattened” portion of the P-V relationship
• After Dual Wean, PaCO2 will be lowered provided ventilation is occurring closer to total lung capacity.
• Subsequent weaning to 14/4 may result in a PaCO2 = 55 torr
• PERMISSIVE HYPERCAPNIA

45
17
18
TLC
RV
19
16
P
V
PRESSURE (cmH20)
VO
LU
ME
Peak Inflating Pressure
PEEP
Iatrogenic hypercapnia with inappropriate Dual
Wean
Tidal Volume decreases
with weaning