pulmonary embolism
TRANSCRIPT

Pulmonary Embolism
Todd A. May, M.D.Todd A. May, M.D.Director, Family Practice Inpatient ServiceDirector, Family Practice Inpatient Service
San Francisco General HospitalSan Francisco General Hospital
Associate Clinical ProfessorAssociate Clinical Professor
University of California, San FranciscoUniversity of California, San Francisco

PE: A Clinical Challenge
Common: 250,000 cases/yearCommon: 250,000 cases/year Mimics many other illnessesMimics many other illnesses Potentially fatal (15%)Potentially fatal (15%) Treatment potentially dangerousTreatment potentially dangerous No single reliable diagnostic testNo single reliable diagnostic test Under- and over-diagnosedUnder- and over-diagnosed

Diagnostic Testing
NoNo single noninvasive test is single noninvasive test is sufficiently sensitive or specific to sufficiently sensitive or specific to diagnose or exclude PE in all diagnose or exclude PE in all patientspatients
No single test can reliably rule out No single test can reliably rule out PEPE
Yep, that includes CT Angio (right?)Yep, that includes CT Angio (right?)
Clinical Approach
Consider PE in DDxConsider PE in DDx Stratify risk for PE (H&P, initial lab)Stratify risk for PE (H&P, initial lab) Select appropriate diagnostic Select appropriate diagnostic
test(s)test(s) Interpret results in clinical contextInterpret results in clinical context Select therapy based on clinical Select therapy based on clinical
statusstatus

Risk Factors
GeneralGeneral HypercoagulabilityHypercoagulability StasisStasis Vascular injuryVascular injury
Clinical Presentation
97% with PE have at least one of 97% with PE have at least one of the following:the following: DyspneaDyspnea TachypneaTachypnea Pleuritic painPleuritic pain
Presence should trigger initial Presence should trigger initial suspicionsuspicion

Clinical Presentation
SymptomsSymptoms Dyspnea, pleuritic chest painDyspnea, pleuritic chest pain Cough, hemoptysis, syncopeCough, hemoptysis, syncope
SignsSigns Tachypnea, tachycardiaTachypnea, tachycardia JVD, loud PJVD, loud P22, TR murmur, rales, TR murmur, rales Signs of DVTSigns of DVT

Chest Radiograph

Electrocardiogram

Oxygenation
Pulse Oximetry (SpOPulse Oximetry (SpO22)) Normal SpONormal SpO22 does not exclude PE does not exclude PE Interpret with RRInterpret with RR
ABGABG
pOpO2 2 pCO pCO22
Increased A-a gradientIncreased A-a gradient

Risk Stratification
Determine probability of PEDetermine probability of PE LowLow ModerateModerate HighHigh
Overall clinical impressionOverall clinical impression Models/scoring systemsModels/scoring systems

PE Probability Prediction Rule
DVT signs/symptomsDVT signs/symptoms 3.03.0
HR > 100 HR > 100 1.5 1.5
Immobilization/Surgery < 4 wk Immobilization/Surgery < 4 wk 1.5 1.5
Previous DVT or PE Previous DVT or PE 1.5 1.5
Hemoptysis Hemoptysis 1.0 1.0
Malignancy (current) Malignancy (current) 1.0 1.0
Alternative Dx less likelyAlternative Dx less likely 3.0 3.0
Probability: Low<2, Moderate 2-6, High>6Probability: Low<2, Moderate 2-6, High>6

D-Dimers
Valuable screening testValuable screening test High sensitivity; low specificityHigh sensitivity; low specificity
Helpful only if Helpful only if NegativeNegativeStrong Negative Predictive Strong Negative Predictive Value-- Rules out PE when low Value-- Rules out PE when low probabilityprobability
Safe, noninvasiveSafe, noninvasive Rapid, inexpensiveRapid, inexpensive
D-Dimers
Available assaysAvailable assays Standard ELISAStandard ELISA Latex agglutinationLatex agglutination Erythrocyte agglutination (SimpliRED)Erythrocyte agglutination (SimpliRED) Turbidimetric assay (Liatest)Turbidimetric assay (Liatest) Rapid ELISA (VIDAS)Rapid ELISA (VIDAS) Immunofiltration (NycoCard)Immunofiltration (NycoCard)

V/Q Scan

V/Q Lung Scan
Normal V/Q Sensitivity 99%Normal V/Q Sensitivity 99% Rules Rules outout PE PE
High Prob V/Q Specificity 96%High Prob V/Q Specificity 96% Rules Rules inin PE PE
But, >60% nondiagnosticBut, >60% nondiagnostic Takes >2 hr to performTakes >2 hr to perform Not available at all timesNot available at all times

V/Q Lung Scan
V/Q ResultV/Q Result True PE True PE (+Angio)(+Angio)
PPV if prob PPV if prob concordant concordant
High probabilityHigh probability 87%87% 96%96%
IntermediateIntermediate 30%30% 33%33%
LowLow 14%14% 4%4%
NormalNormal <2%<2% <2%<2%
PIOPED. PIOPED. JAMAJAMA. 1990; 263:2753-59. 1990; 263:2753-59

Ultrasound for DVT
Positive testPositive test Inability to compress femoral or Inability to compress femoral or
popliteal veinpopliteal vein Positive Predictive Value 97%Positive Predictive Value 97%
Negative testNegative test Full compressibilityFull compressibility Negative Predictive Value 98%Negative Predictive Value 98%
Kearon et al. Kearon et al. Ann Intern MedAnn Intern Med. 1998; 129:1044-49. 1998; 129:1044-49
Ultrasound and PE
US +DVT in 30-50% with PEUS +DVT in 30-50% with PE Positive US—confirms PEPositive US—confirms PE Negative ultrasoundNegative ultrasound
PE less likely, but not excludedPE less likely, but not excluded Sequential ultrasoundSequential ultrasound
Persistently negativePersistently negative ultrasound at ultrasound at 1-2 wks 1-2 wks <2% DVT/PE at 6mos <2% DVT/PE at 6mos
Hull et al. Hull et al. J. ThrombJ. Thromb 1996; 3:5-8. 1996; 3:5-8.
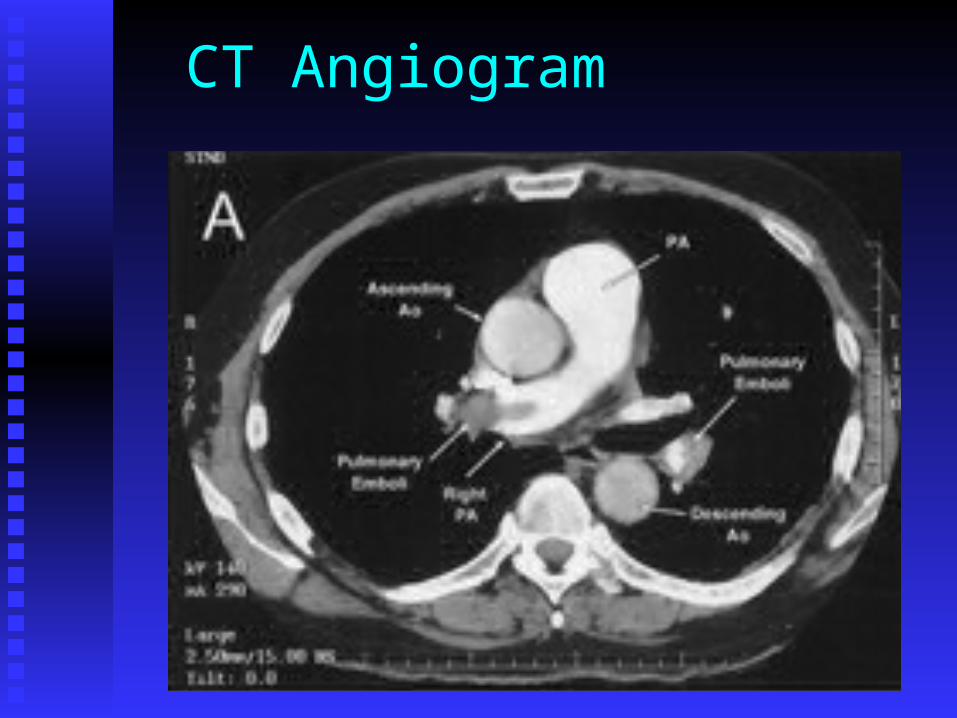
CT Angiogram
CT Angiogram
BenefitsBenefits AvailableAvailable Direct imageDirect image Alternative DxAlternative Dx Pelvic/leg veinsPelvic/leg veins
LimitationsLimitations IV contrastIV contrast ExpensiveExpensive Patient Patient
cooperationcooperation Uncertain Uncertain
sens/specsens/spec

CT Angiogram
““Helical CT is a reliable Helical CT is a reliable imaging tool for imaging tool for excluding clinically excluding clinically important PE”important PE”
Goodman LR et al. Radiology 2000;215:535-42.
CT Angiogram
1015 patients evaluated for PE1015 patients evaluated for PE Nonrandomized, not controlled Nonrandomized, not controlled
Two diagnostic arms “recommended”Two diagnostic arms “recommended” Substantial differences between groupsSubstantial differences between groups
285 patients with negative CT Angio285 patients with negative CT Angio 22% were treated anyway22% were treated anyway
< 2% risk of subsequent PE in 3 months< 2% risk of subsequent PE in 3 months Only 70% completed 3mo f/u!Only 70% completed 3mo f/u!

CT Angiogram
Prospective study of consecutive, Prospective study of consecutive, nonselected patients in a Geneva nonselected patients in a Geneva ER included 299 with suspected PEER included 299 with suspected PE
39% had confirmed PE39% had confirmed PE High prob V/Q, +US, or +AngioHigh prob V/Q, +US, or +Angio
CT Sensitivity 70%CT Sensitivity 70% CT Specificity 91%CT Specificity 91%
Perrier et al. Perrier et al. Ann Intern MedAnn Intern Med. 2001; 135:88-97. 2001; 135:88-97

CT Angiogram 35 35 false negativefalse negative on CT on CT
1919 High prob V/QHigh prob V/Q 1212 +DVT on US+DVT on US 33 +Angio+Angio 11 Dx at f/uDx at f/u
““CT should not be used alone for CT should not be used alone for suspected PE, but combining tests suspected PE, but combining tests improves accuracy and reduces need improves accuracy and reduces need for angiography”for angiography”
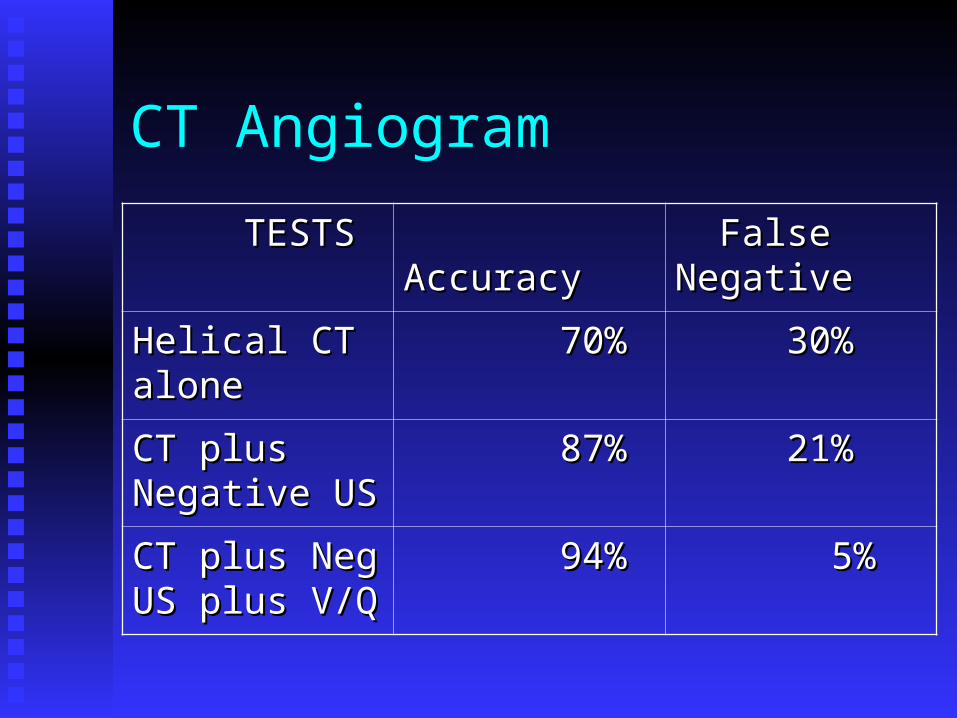
CT Angiogram
TESTSTESTS AccuracyAccuracy False False NegativeNegative
Helical CT Helical CT alonealone
70%70% 30%30%
CT plus CT plus Negative USNegative US
87%87% 21%21%
CT plus Neg CT plus Neg US plus V/QUS plus V/Q
94%94% 5%5%
CT Angiogram
New Systematic ReviewNew Systematic Review 15 studies met criteria15 studies met criteria VTE after negative CT Angio:VTE after negative CT Angio:
NLR 0.07NLR 0.07 NPV 99.1%NPV 99.1%
““The clinical validity of using CT to r/o The clinical validity of using CT to r/o PE is similar to that reported for PE is similar to that reported for pulmonary angiographypulmonary angiography””
Quiroz R et al. JAMA 2005;293:2012-17.

Goldhaber, S. Z. N Engl J Med 2005;352:1812-1814
Two Cases of Pulmonary Embolism as Shown on Contrast-Enhanced 16-Slice Multidetector-Row Computed Tomography

Multidetector-Row CT
756 consecutive pts; 194 with PE756 consecutive pts; 194 with PE 82 High Prob: 78/82 +CT, 1 +US/-CT82 High Prob: 78/82 +CT, 1 +US/-CT 674 Lower Prob:674 Lower Prob:
232 neg D-dimer 232 neg D-dimer no TE no TE 109 +CT109 +CT 318 neg dimer and CT 318 neg dimer and CT 3 TE at 3mo 3 TE at 3mo
Neg CT plus Neg D-dimer: ~1% risk for Neg CT plus Neg D-dimer: ~1% risk for TE at 3 monthsTE at 3 months
Perrier A et al. NEJM 2005;352:1760-8.
CT Angiogram
My ConclusionsMy Conclusions CT Angio is good and getting CT Angio is good and getting
betterbetter It’s not perfect, so don’t over-rely It’s not perfect, so don’t over-rely
on iton it Do additional testing if clinical Do additional testing if clinical
suspicion is highsuspicion is high Neg D-dimer plus neg MDR CT may Neg D-dimer plus neg MDR CT may
be best to confidently r/o PEbe best to confidently r/o PE
MRI/MRA
No radiation or contrast exposureNo radiation or contrast exposure ExpensiveExpensive Not uniformly availableNot uniformly available Limited dataLimited data Role not establishedRole not established
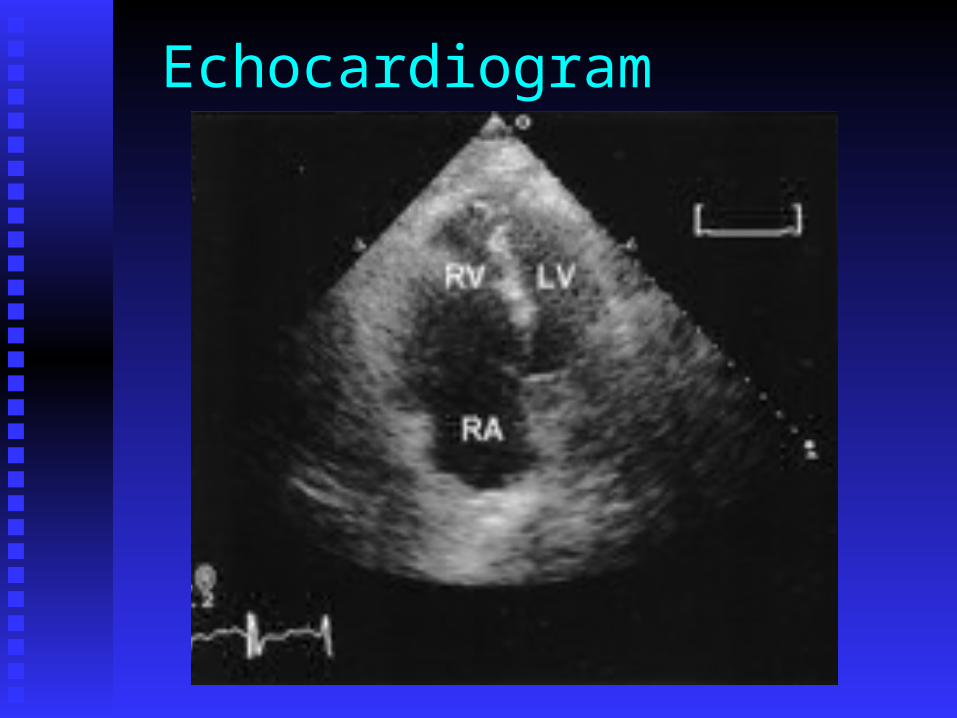
Echocardiogram

Pulmonary Angiogram
Gold standardGold standard 98% Sensitive98% Sensitive 97% Specific97% Specific ComplicationsComplications
Death 0.5%Death 0.5% Major non-fatal 1%Major non-fatal 1% Minor 5%Minor 5%

Diagnostic Summary
Determine pre-test probability—Determine pre-test probability—be be selective when deciding to w/uselective when deciding to w/u
D-Dimers to r/o PE if low prob.D-Dimers to r/o PE if low prob. CT or V/Q (US CT or V/Q (US firstfirst if DVT likely) if DVT likely) Bilat. LE US if V/Q non-diagnostic and/or Bilat. LE US if V/Q non-diagnostic and/or
CT neg. and suspicion persistsCT neg. and suspicion persists Then, Then,
Serial US if moderate/high prob.Serial US if moderate/high prob. Angiogram if still high prob.Angiogram if still high prob.

Treatment

Unfractionated Heparin
Weight-based dosingWeight-based dosing (nomogram) (nomogram) IV bolus, then infusionIV bolus, then infusion Monitor PTT (1.5-2.0 x), CBCMonitor PTT (1.5-2.0 x), CBC Continue Continue 4-5d and therapeutic on 4-5d and therapeutic on
Warfarin for 2d (INR>2.0)Warfarin for 2d (INR>2.0)
Low Molecular Weight Heparin
Alternative regimenAlternative regimen Better bioavailability, longer half-Better bioavailability, longer half-
life, more predictable effectlife, more predictable effect No monitoring of PTT (follow CBC)No monitoring of PTT (follow CBC) Contraindications: renal failure Contraindications: renal failure
(CrCl<30), weight extremes(CrCl<30), weight extremes

Warfarin
Start when therapeutic on Start when therapeutic on HeparinHeparin
Monitor INR dailyMonitor INR daily Goal: INR 2.0-3.0 for Goal: INR 2.0-3.0 for
3-6 months3-6 months

Duration of anticoagulation
Identified precipitantIdentified precipitant 3 mos3 mos First idiopathic episodeFirst idiopathic episode 6 mos6 mos Prolonged/indefinite:Prolonged/indefinite:
2 thrombotic episodes2 thrombotic episodes 1 spont. life-threatening episode1 spont. life-threatening episode Anti-phospholipid antibody Anti-phospholipid antibody
syndrome, ATIII deficiencysyndrome, ATIII deficiency
Thrombolysis
Massive PEMassive PE Acute pulmonary hypertensionAcute pulmonary hypertension RV dysfunctionRV dysfunction Systemic hypotensionSystemic hypotension
All age groups benefitAll age groups benefit Addition to Heparin therapyAddition to Heparin therapy Various agents appear equivalentVarious agents appear equivalent

Thrombectomy
Surgical or transvenous (catheter)Surgical or transvenous (catheter) When thrombolysis unsuccessful or When thrombolysis unsuccessful or
contraindicated, orcontraindicated, or Massive PEMassive PE

Vena Cava Filters
Indications:Indications: Contraindication to anticoagulationContraindication to anticoagulation Recurrent PE on anticoagulationRecurrent PE on anticoagulation Complications from anticoagulationComplications from anticoagulation Massive PE with poor reserveMassive PE with poor reserve
Problems with filter thrombosisProblems with filter thrombosis

Prevention
Identify and minimize risk factorsIdentify and minimize risk factors Pneumatic compression devicesPneumatic compression devices S.Q. HeparinS.Q. Heparin
UnfractionatedUnfractionated Low molecular weightLow molecular weight
Thrombophilia evaluation
Hypercoagulable statesHypercoagulable states
Thrombophilia evaluation
Why test for hypercoagulability?Why test for hypercoagulability? May affect intensity/duration of May affect intensity/duration of
treatmenttreatment Family counseling about risksFamily counseling about risks Identify need for prophylaxis in Identify need for prophylaxis in
higher risk situationshigher risk situations
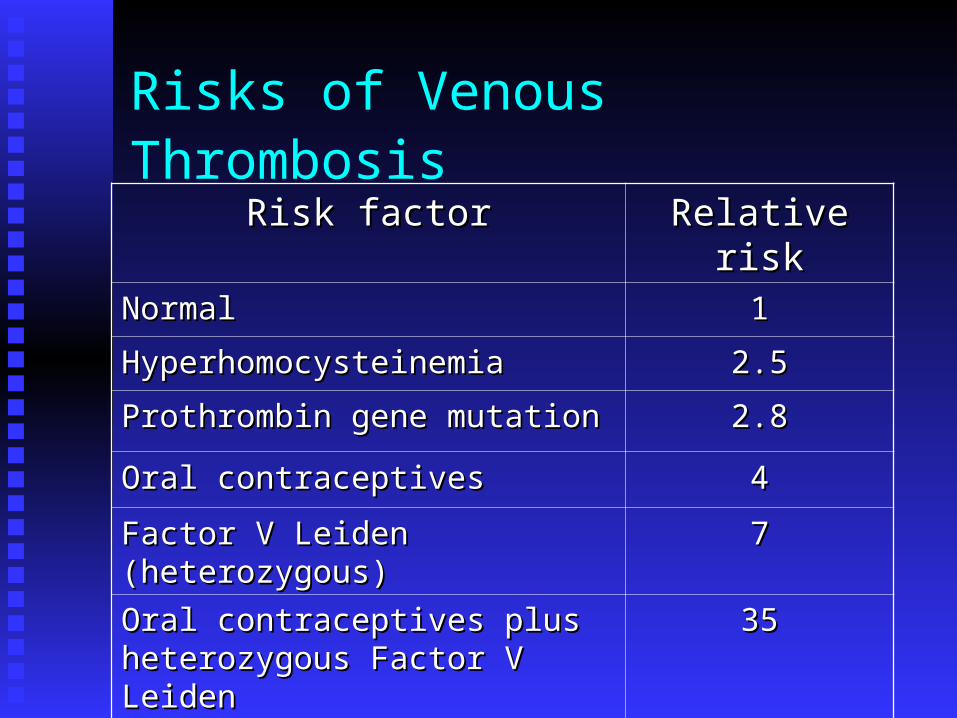
Risks of Venous Thrombosis
Risk factorRisk factor Relative riskRelative riskNormalNormal 11
HyperhomocysteinemiaHyperhomocysteinemia 2.52.5
Prothrombin gene mutationProthrombin gene mutation 2.82.8
Oral contraceptivesOral contraceptives 44
Factor V Leiden (heterozygous)Factor V Leiden (heterozygous) 77
Oral contraceptives plus heterozygous Oral contraceptives plus heterozygous Factor V LeidenFactor V Leiden
3535
Factor V Leiden (homozygous)Factor V Leiden (homozygous) 8080

Thrombophilia evaluation
Unprovoked thrombotic event andUnprovoked thrombotic event and Age < 45 yrsAge < 45 yrs Recurrent eventRecurrent event Family history of thrombosisFamily history of thrombosis Cerebral/visceral thrombosisCerebral/visceral thrombosis Fetal demiseFetal demise 3 or more SABs3 or more SABs
Thrombophilia evaluation
First unprovoked eventFirst unprovoked event Provoked by pregnancyProvoked by pregnancy Provoked by OCs or HRTProvoked by OCs or HRT

Thrombophilia evaluation
Testing caveatsTesting caveats C, S, ATIII C, S, ATIII in acute thrombosis in acute thrombosis Heparin interferes with ATIII, Heparin interferes with ATIII,
lupus anticoagulant, Factor VIII, lupus anticoagulant, Factor VIII, and some APC resistance testsand some APC resistance tests
Warfarin decreases C & SWarfarin decreases C & S
Thrombophilia evaluation
Tests performed acutelyTests performed acutely Leiden Factor V (APC resistance)Leiden Factor V (APC resistance) Prothrombin G20210A mutationProthrombin G20210A mutation Increased homocysteineIncreased homocysteine Anti-cardiolipin antibodiesAnti-cardiolipin antibodies
Thrombophilia evaluation
Consider testing laterConsider testing later Lupus anticoagulantLupus anticoagulant Decreased Proteins C & SDecreased Proteins C & S Decreased Anti-thrombin IIIDecreased Anti-thrombin III Increased Factor VIIIIncreased Factor VIII
Summary
Have index of suspicion for PEHave index of suspicion for PE Develop clinical probabilityDevelop clinical probability Interpret all tests in context of pre-Interpret all tests in context of pre-
test probabilitytest probability Selectively w/u for thrombophiliaSelectively w/u for thrombophilia Choose therapy based on clinical Choose therapy based on clinical
statusstatus