public health ethics (kfmc,11.05.2016)
TRANSCRIPT

PUBLIC HEALTH ETHICS: ETHICS OF PUBLIC HEALTH AND HEALTH PROMOTION
ETHICS OF DISASTERS AND EMERGENCY MEDICINE.
RESOURCE ALLOCATION
King Fahad Medical City (May 11, 2016)
Ghaiath Hussein, MBBS, MHSc. (Bioethics)
Doctoral Researcher, Uni. Of Birmingham
■ This presentation is based on Hussein GM, Alkabba AF, Kasule
OH. Professionalism and Ethics Handbook for Residents (PEHR):
A Practical Guide. Ware J, Kattan T (eds). 1st Edition. Riyadh,
Saudi Arabia: Saudi Commission for Health Specialties, 2015.
AND
■ Training material presented to the East Mediterranean Public
Health Network (EMPHNET) course on Public Health Ethics
(Amman, 2014)

■ The technical and ethical differences between clinical care and
public health practice
■ The importance of ethics in PH practice and research
■ concepts of surveillance, screening, and outbreak investigation
■ The ethical issues in surveillance and screening
■ Concepts and scope of health promotion
■ Discuss the ethical issues that arise from health promotion
■ Theoretical models for resource allocation
ETHICAL ISSUES IN PUBLIC HEALTH & HEALTH
PROMOTION

■Tell me
about public
health
Source: http://professiongal.com/

Aspect Clinical care Public health
Main aim Treat sick individuals (cure) Prevent healthy individuals from getting ill
(prevention)
Beneficiaries Individuals (healthy or sick) and families Population (community)
Scope Clinical care, diagnosis, and treatment Health education, health promotion, and community-
based interventions
Fields
(specialties)
Internal medicine, surgery, paediatrics,
obstetrics and gynecology, etc.
Epidemiology, health promotion, biostatistics
Occupational health, etc.
Guidance Clinical guidelines, hospital policies, etc. PH guidelines, regulations, laws
Examples of
ethical issues
and questions
Issues related to the individuals’ right to
decide (autonomy), privacy and
confidentiality, etc.
- When is it ethical to disclose a patient’s
medical information?
- How to decide which patient should
have which service (e.g. an ICU bed)?
Issues related to the tension between the individual
rights (interests) and the public good (interests)
- When is it ethical to limit the freedom of
movement of a patient with an infectious disease
(e.g. in case of pandemic)?
- Do parents have the right to refuse vaccinating
their children?

– the identification, analysis, and resolution of
ethical problems arising in public health practice
and research

■ In Countristan, treatment of all TB patients is free. Patients are expected to show to the nearest health center (HC) to receive the treatment under direct observation (DOTS).
■ The HC keeps a record of ‘which patient had which dose’.
■ The TB officer in that region of Coutristan noted that one of the TB patient, Mr. Contagious did not receive his doses for the last couple of weeks.
■ The Officer approached Mr. Contagious to persuade him to take the doses on time.
■ The patient refused. The Officer presented an official request to the Attorney General (AG) in the region saying that “Mr. Contagious presents danger to the public.”
■ The AG issued an Order of Arrest against Mr. Contagious for the whole duration of the TB treatment.
What are the ethical issues at stake here?

■ Public vs. individuals’ rights
■ Scarcity of resources
■ Socio-political factors:
– Poverty, illiteracy , minorities, vulnerability
– Abuse of power (‘Nanny State’ & public engagement)
■ Socio-cultural factors:
– Local beliefs vs. “international guidelines”
– Role of families and community leaders
■ Urgency to contain public health threats
■ Inequalities (national and international)

Philosophical
•Deontological
•Utilitarian (act & rule)
•Rights-based
•Virtue
•Casuistry
•Social-contract
•Principlism
Religious
•Islamic ethics & jurisprudence (Purposes of Law ‘Sharia’)
•Christian ethics
•Jewish Ethics
•?Oriental Philosophies (Buddhist, Confucian, etc.)
Guiding Principles
•Utility
•Efficiency
•Liberty
•Transparency
•Participation
•Review and revisability
•Effectiveness
•Fairness
•Reciprocity
•Solidarity
■ Utility: acting so as to produce the greatest good.
■ Efficiency: calls for minimizing the resources needed to produce a
particular result or maximizing the result that can be produced
from a particular set of resources.
■ Liberty: one should impose the least burden on personal self-
determination that is necessary to achieve a legitimate goal
■ Fairness: “treating like cases alike”
■ Reciprocity: individuals (professionals) accept of the risk in
executing their duties would engender reciprocal duties on the
part of the community to them
■ Proportionality: actions taken proportional to need

Examples of ethical issues in public health
■Surveillance,
screening, &
outbreak
investigation
■Health Promotion

■ Definition:
– “the continuous, systematic collection, analysis and
interpretation of health-related data needed for the
planning, implementation, and evaluation of public
health practice.” (WHO)
■ Functions:
– early warning system;
– document the impact of an intervention, or track
progress towards specified goals; and
– monitor and clarify the epidemiology of health
problems

■ "the presumptive identification of unrecognized disease
or defect by the application of tests, examinations, or
other procedures which can be applied rapidly.” (ICC,
WHO)
■ Examples:
– Premarital genetic
– Prenatal genetic
– Paediatric genetic
– Cancer genetic

■ Definition
“activities undertaken to establish the existence of an outbreak, describe the outbreak, and to identify the source, transmission mechanism and contributory factors, as a basis for outbreak response.” (NZ CDC)
Steps:
1. Verify the diagnosis
2. Confirm the outbreak
3. Case definition
4. Descriptive epidemiology
5. Develop a hypothesis
6. Test the hypothesis
7. Refine hypothesis / Execute additional studies
8. Implement control and prevention measures
9. Communicate findings

•Privacy
•Confidentiality
•Autonomy (consent)
Data/sample collection
•Benefits
•Harms
•Autonomy (consent)Methods used
•Justice
•Trust Outcomes

‘Preventive’ Mastectomy ■ “I carry a “faulty” gene, BRCA1, which sharply increases my risk of developing
breast cancer and ovarian cancer.
■ My doctors estimated that I had an 87 percent risk of breast cancer and a 50
percent risk of ovarian cancer,
■ Once I knew that this was my reality, I decided to be proactive and to minimize
the risk as much I could.
■ I made a decision to have a preventive double mastectomy.
■ I am writing about it now because I hope that other women can benefit from my
experience.
■ I wanted to write this to tell other women that the decision to have a mastectomy
was not easy. My chances of developing breast cancer have dropped from 87
percent to under 5 percent.
■ I am fortunate to have a partner, Brad Pitt, who is so loving and supportive. Brad
was at the Pink Lotus Breast Center, where I was treated, for every minute of the
surgeries.
ETHICAL ISSUES IN DISASTERS
Let’s give it a thought …
■What do we mean by a disaster?
■Natural vs. manmade
■Any examples from EMR?

Disproportional burden
COI (®Tamiflu, vaccine)
Resource allocation
Consent
Public engagement
Sub-optimal products
Surveillance (research?)
Inequalities
Trials (review)
Loss of property &work hours
Access to care
Restricted movement
Confidentiality
Professional duty
■ Individual liberty
■ Protection of the public from harm
■ Proportionality
■ Reciprocity
■ Transparency
■ Privacy
■ Protection of communities from undue stigmatisation
■ Duty to provide care
■ Equity
■ Solidarity
(Singer et al., 2003)
■ Do (public) health
professionals have the
duty to provide
healthcare services
even if that would
endanger their lives?
■ What are the factors
that help us draw that
extent?

(Source: Case Studies of Ethics During a Pandemic, McDougall, 2010)
■ Maria is a 35-year-old family physician and mother of three children aged 4-8. She works in a primary care clinic in a main hospital and is one of 12 doctors practising in the clinic.
■ Her husband, hearing the media reports, is concerned that she may become ill or bring home illness to her family because of the increased exposure at work. He encourages her not to go to work. Maria is concerned for the care of her children. They attend a day care centre. Her husband works in an accounting firm. She is also worried about abandoning her patients and increasing the workload of her colleagues, many of whom, like her, have young families.
■ First Set of Questions
– What are your initial thoughts and feelings about this?
– What do you think are the most important considerations for Maria in making her decision?
– Would your opinion change if the day care centre was closed? Why?
■ Maria decides she will go to work. She is concerned that her clinic lacks the appropriate amount of protective equipment. The clinical group meets and decides that they are committed to providing care to people with influenza, but will only do so if the ministry of health provides appropriate protective equipment.
■ 2nd group of questions:
– What do you think of the clinical group's decision?
– Do you think society has an obligation to health care workers in the event of a pandemic outbreak?
– One of Maria's colleagues is close to retirement. He has diabetes and heart disease. He tells the clinic that he will not come to work as he feels the risk to his own health is too great.
– In your view, is the health status of a health care worker an acceptable reason not to respond to a pandemic virus?

The influenza outbreak is now well advanced. Many people are sick, including a large
number of health care workers. Many health care providers in hospitals and clinics are
not showing up for work. Many refuse to work because they fear infection.
■ Should health care providers face consequences for refusing to show up for work?
■ If no, why? If yes, what sorts of penalties do you think would be fair?
The government has now officially declared a health emergency. It is enacting
legislation mandating health care workers to participate in the efforts to control the
outbreak.
■ What do you think about this possibility?
■ Do you think such laws would violate the rights of health care workers?
Final Questions
– In your view, is it justifiable for health care providers to refuse to provide care?
– Who should make these kinds of decisions?
– How should these kinds of decisions be made? In the absence of a consensus, how should
these decisions be made?
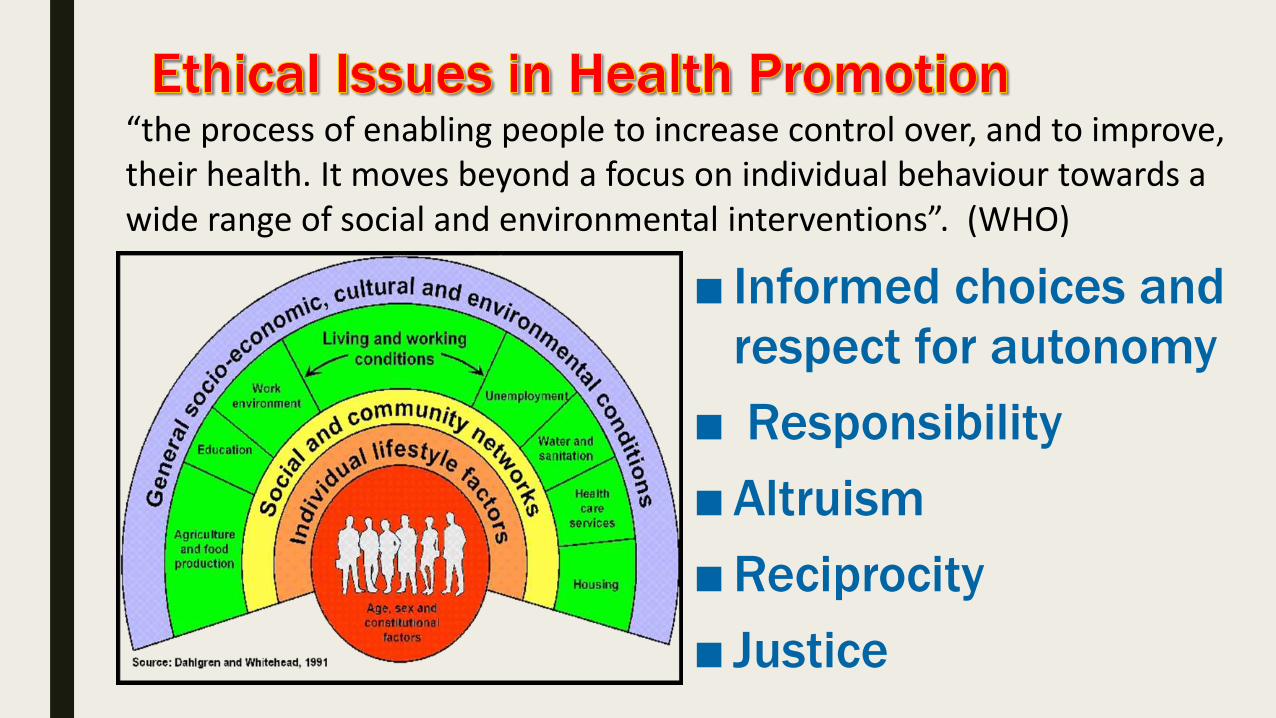
■ Informed choices and
respect for autonomy
■ Responsibility
■ Altruism
■ Reciprocity
■ Justice
“the process of enabling people to increase control over, and to improve, their health. It moves beyond a focus on individual behaviour towards a wide range of social and environmental interventions”. (WHO)

RATIONING AND RESOURCE ALLOCATION

■ Utilitarianism:– Theory: resources being allocated to less expensive treatments or services that provide the greatest
benefit.
– Practice: QALY.
■ Equity and Distributive Justice– Theory: “equals should be treated equally, and unequals treated unequally in proportion to the
relevant inequalities”. The need not only the benefit gained from an intervention.
– Practice: ensure that those in poorest health, or greatest need
■ Autonomy:
– individuals have a right to determine/choose what is in their own best interest
■ Beneficence/Non-maleficence:
– Healthcare providers should act in the interest of their clients/patients and NOT to harm them
■ ‘distributive’ Justice/fairness:
– All groups have an equal right to health services regardless of race, gender, age, income, or any other characteristic.
How should we decide on who gets what?
■Concept of need
■Concept of utility
■Non-comparative concept
■Privileging concept or ‘social worth’

■ What does resource allocation affect? How?
Breadth
• the population covered?
• application of criteria
• means-testing (e.g., excluding those with higher incomes),
• employment (e.g., excluding self-employed people),
• excluding people from eligibility (e.g., those who do not meet certain requirements),
• or by allowing people to opt out.
Scope
• Which services?
• excluding services from the benefits package
• effectiveness,
• comparative effectiveness,
• cost-effectiveness,
• health technology assessments (HTAs),
• clinical guidelines or quality assurance
Depth
• extent or cost share to which services are covered
• selective charges (co-payments) for inefficient services,
• reduced charges for especially valuable ones (value-based insurance design)

THEORETICAL MODELS FOR RESOURCE
ALLOCATIONEzekiel J. Emanuel" Justice and Managed Care: Four Principles for the Just Allocation of Health Care
Resources,” Hastings Center Report 30, no. 3 (2000): 8-16. Daniels N, Sabin JE. The ethics of accountability in managed care reform. Health Aff (Millwood) 17[5],
50-64. 1998
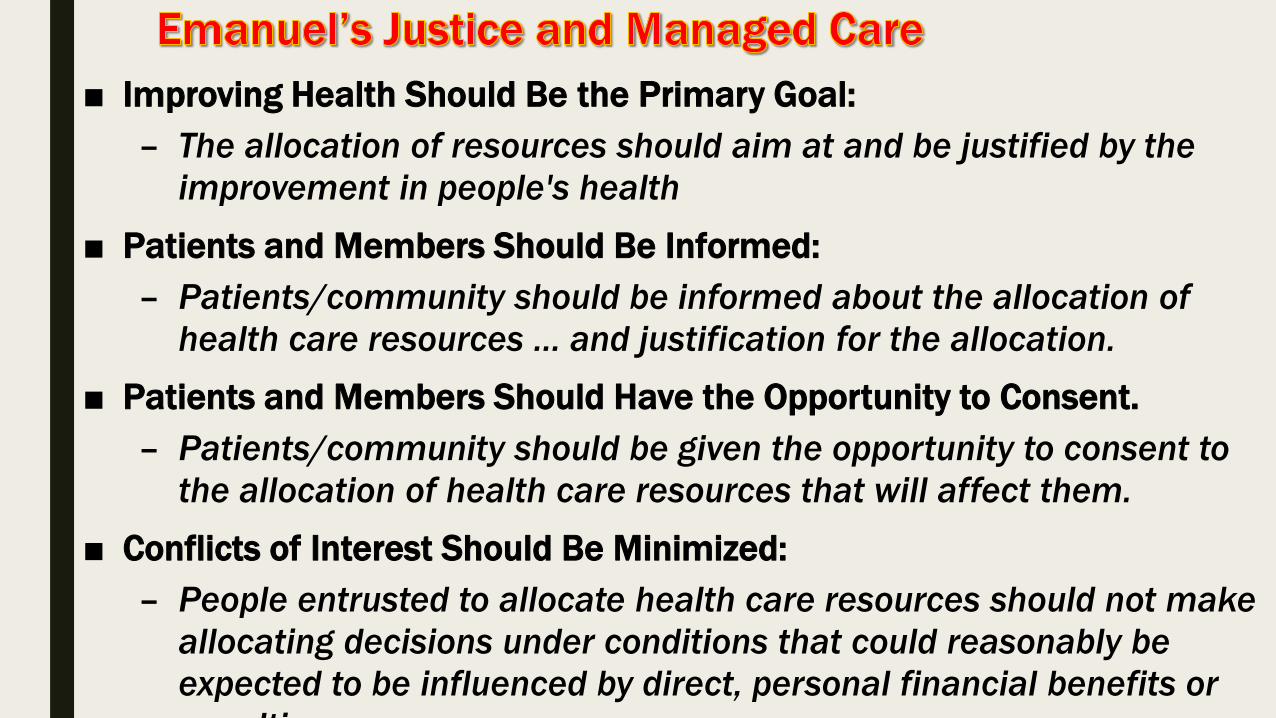
■ Improving Health Should Be the Primary Goal:
– The allocation of resources should aim at and be justified by the
improvement in people's health
■ Patients and Members Should Be Informed:
– Patients/community should be informed about the allocation of
health care resources … and justification for the allocation.
■ Patients and Members Should Have the Opportunity to Consent.
– Patients/community should be given the opportunity to consent to
the allocation of health care resources that will affect them.
■ Conflicts of Interest Should Be Minimized:
– People entrusted to allocate health care resources should not make
allocating decisions under conditions that could reasonably be
expected to be influenced by direct, personal financial benefits or
penalties.

Condition Description
Relevance • Priority setting decisions must rest on reasons (including
evidence and principles) that fair-minded participants
(stakeholders) can agree are relevant
• These can involve managers, clinicians, patients, and
consumers in general (three key foci are underlined)
Publicity Priority setting decisions and their rationales must be
publicly accessible
Appeals The priority setting process must include a mechanism for
revising decisions in light of further evidence or principles
that other stakeholders might contribute
Enforcement There must be voluntary or public regulation of the
process to ensure that the first three conditions are met
■ Within its efforts to control the spread of Pandemic
Influenza A H1N1 during the Hajj season (2010), the
Saudi government was able to provide a total of
2,500,000 doses of the newly produced vaccine.
■ The pilgrims are estimated to be 3,500,000; the
working staff who are in contact with pilgrims (entries,
security & health) are about 120,000 persons
■ Who should have the vaccine? Who’s first?
■ Frank JR. The CanMEDS 2005 physician competency framework: Better standards, better physicians, better care. Royal College of Physicians and Surgeons of Canada; 2005
■ Principles of the Ethical Practice of Public Health; Public Health Leadership Society (2002)
■ Ethics and Public Health: Model Curriculum. Ed. Bruce Jennings et al. (2003)
■ Childress JF, Faden RR, Gaare RD, Gostin LO, Kahn J, Bonnie RJ, Kass NE, Mastroianni AC, Moreno JD, Nieburg P: Public health ethics: mapping the terrain. J Law Med Ethics 2002, 30:170-8.
■ Public health: disconnections between policy, practice and research. Jansen et al. Health Research Policy and Systems 2010, 8:37
■ Ethical issues in epidemiologic research and public health practice. Steven S Coughlin. Emerging Themes in Epidemiology 2006, 3:16
■ Accountability for reasonableness. Norman Daniels, BMJ 2000;321:1300-1301