psychosocial support intervention for hiv-affected youth and their caregivers in haiti eddy...
TRANSCRIPT

Psychosocial Support Intervention for HIV-Affected
Youth and Their Caregivers in Haiti
Eddy Eustache, M.A.Director of
Psychological Services
Partners In Health/Zamni Lasante Sociomedical
Complex, Cange, Haiti

Key Collaborators
• Joia Mukherjee (PI), Cate Oswald, Ermaze Louis, Fiona Scanlan, Pamela Surkan, Sarah Hook, Anna Casey, Mary Smith Fawzi, and colleagues in Haiti
• Collaborators represent Zanmi Lasante/ Partners In Health; Department of Global Health and Social Medicine, Harvard Medical School; and the Division of Global Health Equity, Brigham and Women’s Hospital


Specific Aim 1• To document the feasibility of implementing a
psychosocial group support intervention for HIV-affected youth and their caregivers in a resource-poor setting

Specific Aim 2• To describe the preliminary findings of the effect of
this intervention on psychosocial health outcomes among HIV-affected youth and their parents

Cange

Standard of Care at PIH/ZL
• Comprehensive pediatric services to address the physical health problems
• Money for school fees and food for those children of HIV-positive parents in need
• Nutritional and/or financial support to affected families
• ART available for all parents and youth who need triple therapy

Methods
• Intervention introduced to168 high risk HIV-affected youth and their caregivers (n=130) recruited between February 2006 and January 2007
• Intervention based on “Project TALC”, developed by Dr. Mary Jane Rotheram-Borus, which demonstrated positive impact on youth affected by HIV. The intervention was adapted by Haitian social workers for use in central Haiti

Inclusion Criteria
• Child or Caregiver Reports:– Child’s psychological symptoms impacting
psychosocial functioning– Child does not live with mother and father– Child being underfed due to HIV-affected status
• Child Reports:– Having 0 friends
• Caregiver Reports:– Having “thoughts of suicide”
Methods• Pre- versus post-intervention assessments were
compared for levels of psychological symptoms, degree of psychosocial functioning, and extent of social support from friends and family among youth
• For caregivers, severity of depressive symptoms, level of role functioning, degree of social support, and HIV-related stigma were compared pre- and post-intervention

Assessment• Child:
– psychiatric symptoms and psychosocial functioning (youth and caregiver report)
– psychosocial functioning (youth and caregiver report)
– social support
• Parent/Caregiver:– depression symptoms– role functioning– HIV-related stigma– Social support (having a confidant, close
friends and relatives, instrumental support)
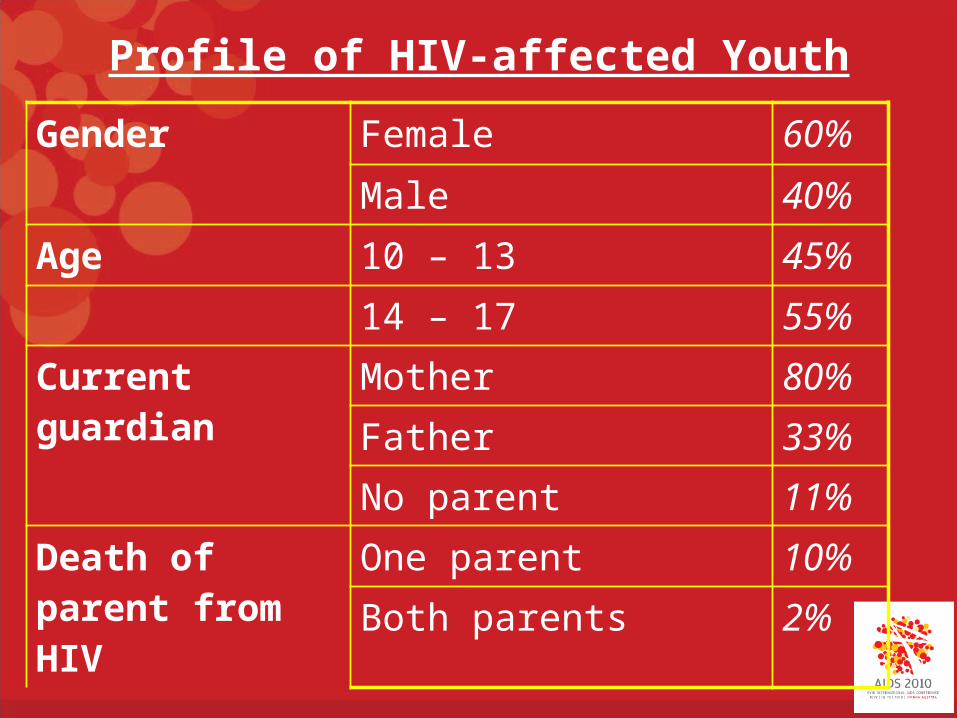
Profile of HIV-affected Youth
Gender Female 60%
Male 40%
Age 10 – 13 45%
14 – 17 55%
Current guardian Mother 80%
Father 33%
No parent 11%Death of parent from HIV
One parent 10%Both parents 2%

Profile of Caregivers of HIV-affected Youth
Gender Female 76%Male 24%
Age Mean 39.41
Education Level Never Attended School 41%HIV Status HIV Positive 95%

Profile of Caregivers of HIV-affected Youth

Profile of Caregivers of HIV-affected Youth

Have
head
ache
s, s
tom
acha
ches
or s
ickne
ss**
Const
antly
fidg
eting
or s
quirm
ing
Restle
ss, c
anno
t sta
y st
ill*
Get a
long
bette
r with
adu
lts th
an c
hildr
en o
f own
age*
*
Have
man
y fe
ars,
eas
ily s
care
d*
Wou
ld ra
ther
be
alone
than
with
peo
ple o
f own
age*
*
Wor
ry a
lot
Easily
dist
ract
ed, d
ifficu
lt to
con
cent
rate
**0
10
20
30
40
50
60
70
80
90
100
Pre- and post-intervention assessment of psychological symp-toms among HIV-affected children
Baseline
Follow-up
Children's Psychological Symptoms
Per
cen
t o
f C
hil
dre
n R
epo
rtin
g S
ymp
tom
s (%
)
*p<.05**p<.01

Low in
ene
rgy*
Feelin
g ev
eryt
hing
is an
effo
rt**
Feelin
g sa
d**
Feelin
g lon
ely**
Crying
eas
ily**
Feelin
g ho
peles
s ab
out t
he fu
ture
*
Feelin
g wor
thles
s**
Difficu
lty fa
lling
or s
tayin
g as
leep*
*0
10
20
30
40
50
60
70
80
90
Pre- and post-intervention assessment of psychological symp-toms among caregivers of HIV-affected children
Baseline
Follow-up
Caregivers' Depressive Symptoms
Per
cen
t o
f C
areg
iver
s R
epo
rtin
g S
ymp
tom
s (%
)
*p<.05**p<.01

Results
• Significant increases from baseline to follow-up in:– youth reported social support– caregiver reported social support and support
from relatives
• Nearly 59% of youth reported having no friends at baseline compared with 30.9% at follow-up
Results• Caregivers reported significant changes from
baseline to follow-up:– decreased depressive symptoms– decreased perceived stigma– increase in social support
• 60% of caregivers indicated at baseline that their health kept them from work, whereas 46.3% reported this at follow-up

Results
• Significant decreases from baseline to follow-up in:– youth self-reported psychological symptoms– caregiver report on youth psychological
symptoms
• 53.6% of youth initially felt that the symptoms they reported resulted in difficulties in psychosocial functioning and only 25.2% indicated this feeling at follow up
Qualitative findings• Caregivers reported a renewed sense of hope and strength to
cope with their illness after the intervention:– My heart was closed, I had asked my body to die… The support
groups gave us courage to live with our illness, and they gave us hope– I used to feel sorry for myself, as if I was at a loss for life, but when I
started the groups I started listening to other people and that helped me a lot… the groups have helped me to learn how to cope with my problems
• HIV-positive parents also expressed a greater capacity to confront HIV-related stigma– I felt embarrassed because people said bad things about me, I was
very discouraged. Now I feel as though I have more strength, and I don’t think about what others have to say about me
– I had a lot of problems because my friends and neighbors talked badly about me. They called me ‘SIDAyis’ (person with HIV). Now I feel comfortable, I don’t let things like this give me problems anymore
Qualitative findings• HIV-affected youth also described a greater ability to
cope with adversity and plan for for the future– As a teenage girl, I learned how to protect myself and
cope with things on my own and continue school
– I learned so much in the support groups, such as how I can protect myself from illnesses you can get from having sex
– I learned so much in the support groups, such as how I can protect myself from illnesses you can get from having sex and how I can chase bad ideas from my head. I really liked the work that we did in the support groups. I now understand my mother better and I am able to better support her

Qualitative findings• Caregivers also expressed that the intervention helped reduce
conflict and strengthen their relationship– The support groups have given me strength… in the exchange of ideas
we’ve had I’ve come to realize that it is not only me who lives like this. The groups have helped me in how I relate to my children
– When [we] started coming to the support groups my children listened to the facilitators talking about how to better support their parents, this made them start to change their behavior, and now they are like different children and they listen to me more
– The support groups were really great, they helped us all, they showed us how we can live with our children. All of my children now listen to me more
– Before the [support groups] I used to treat my children very badly; I would hit them… and yell at them. But now, thanks to our good God, the support groups have brought a different feeling to me and my children are now my friends because I treat them much better.

Discussion• Psychosocial support group for HIV-affected youth and
their caregivers was feasible in rural Haiti
• Study presented a high retention rate. 95% of families completed the twelve month intervention Contributing factors were:– participants’ expressing interest in returning to learn and
to share their experiences– coverage of transportation costs– provision of food at the sessions
• The positive impact on psychological symptoms for HIV affected youth as well as caregivers were significant

Discussion
• Youth and caregivers both reported improvements in social support from friends and relatives
• Quantitatively and qualitatively, HIV-related stigma demonstrated a reduction
• Youth and caregivers demonstrated improvements in psychosocial and role functioning, respectively
Implications for Service
• The high levels of privation in this population may have caused higher levels of certain depressive symptoms
• Intervention increased quality of life for caregivers as rates of suicidal thoughts decreased from 27.7% to 8.1 %. This was achieved by:– Decreasing perceived stigma among HIV-
positive parents– Increasing social support
Implications for Service
• Qualitative findings reflected improvements in self-esteem
• HIV-affected youth described a greater ability to cope with adversity and plan for the future
• Youth also expressed interest in protecting themselves from HIV
Implications for Service
• Long-term psychosocial support interventions may reduce the burden of psychological symptoms and potentially impact psychosocial functioning
• Providing complementary psychosocial support group services in communities receiving an ART intervention may have an impact on psychosocial as well as physical health related outcomes