psychiatric medication - integrated services for … · 2018-06-05 · psychiatric medication . ......
TRANSCRIPT

T R A I N I N G M O D U L E
PSYCHIATRIC MEDICATION

LEARNING OBJECTIVES
At the end of this module the learner will:
• Be familiar with commonly prescribed psychiatric
medications, intended benefits, and how they work
• Be familiar with common side effects, risks, and
contraindications for each medication
• Recognize signs of relapse or non-adherence to
medication prescriptions
• Be familiar with potential reactions between
prescription and nonprescription medications
• Be familiar with alcohol and opioid addiction
treatment medication

THE BASICS
• All actions of the brain – sensory, motor, and
intellectual – are carried out physiologically through
the interactions of nerve cells (neurons)
• Various areas of the brain are interconnected
structurally and functionally by a network of neurons
• Interaction of neurons involves:
• Impulse conduction,
• Neurotransmitter release, and
• Receptor response
• Alterations in these basic processes may lead to
mental disturbance

WHY IT IS IMPORTANT TO UNDERSTAND NEURONS, RECEPTORS, AND NEUROTRANSMITTERS
• Neurons (nerve cells) • Conduct electrical impulses
• Release chemicals called neurotransmitters
• Synapse (space between two neurons) • Neurotransmitters diffuse across a space, or synapse, to
adjacent postsynaptic neuron, where it attaches to receptors on the neuron’s surface
• Receptors (on the receiving neuron) • Neurotransmitters attach to receptors to stimulate or inhibit
the receiving neuron
• It is the interaction between neurotransmitter and receptor that is a major target of the drugs used to treat psychiatric disease
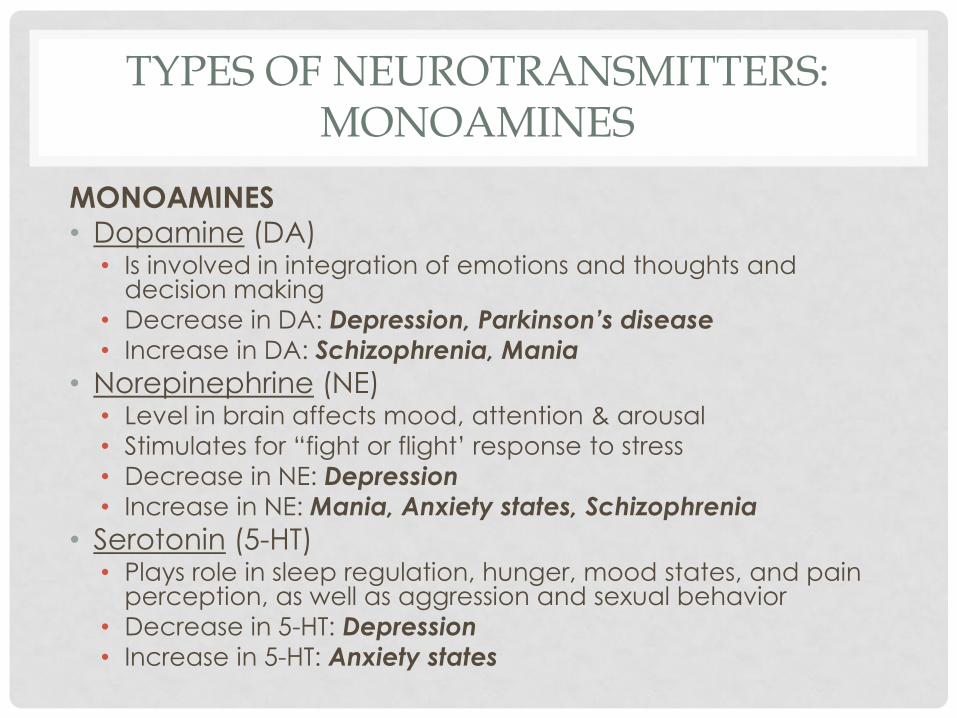
TYPES OF NEUROTRANSMITTERS: MONOAMINES
MONOAMINES • Dopamine (DA)
• Is involved in integration of emotions and thoughts and decision making
• Decrease in DA: Depression, Parkinson’s disease
• Increase in DA: Schizophrenia, Mania
• Norepinephrine (NE) • Level in brain affects mood, attention & arousal
• Stimulates for “fight or flight’ response to stress
• Decrease in NE: Depression
• Increase in NE: Mania, Anxiety states, Schizophrenia
• Serotonin (5-HT) • Plays role in sleep regulation, hunger, mood states, and pain
perception, as well as aggression and sexual behavior
• Decrease in 5-HT: Depression
• Increase in 5-HT: Anxiety states

TYPES OF NEUROTRANSMITTERS: AMINO ACIDS
AMINO ACIDS
• Gamma-aminobutyric acid (GABA) • plays a role in inhibition; reduces aggression, excitation, and
anxiety; anticonvulsant and muscle-relaxing properties; may play role in pain perception; may impair cognition and psychomotor functioning
• Decrease in GABA: Anxiety disorders, Schizophrenia, Mania
• Increase in GABA: Reduction of anxiety
• Glutamate • is excitatory; plays a role in learning and memory
• Decrease in glutamate: Psychosis
• Increase in glutamate: Neurodegeneration in Alzheimer’s disease

PHARMACOLOGICAL TREATMENT
• Pharmacological treatment of mental disturbances
is directed at the suspected neurotransmitter-
receptor problem
• For example:
• Anti-psychotic drugs decrease dopamine
• Anti-depressant drugs increase synaptic levels of serotonin
• Anti-anxiety drugs increase effectiveness of GABA or
increase serotonin
• Drugs used to treat the disturbance can affect
more than one area of brain activity (side effects)
• For example, basic drives, sleep patterns, or body
movement
ANTIANXIETY DRUGS
ANXIOLYT ICS

ANTIANXIETY DRUGS
• Benzodiazepines • Valium
• Klonopin
• Xanax
• Ativan
• Buspirone (BuSpar) • Nonbenzodiazepine
• Without strong sedative-hypnotic effect
• Antidepressants to treat anxiety • SSRIs
• SSNRIs
• TCAs
• MAOIs

BENZODIAZEPINES
• Quick onset of action
• Potential for dependence:
• Use for short periods only until other medications take effect
• Not recommended for patients with known substance
abuse problem
• Not for pregnant or breastfeeding women
• May cause withdrawal symptoms after 3-4 months
of daily use
• Drug interactions:
• Antacids delay absorption
• Alcohol/barbiturates cause increased sedation
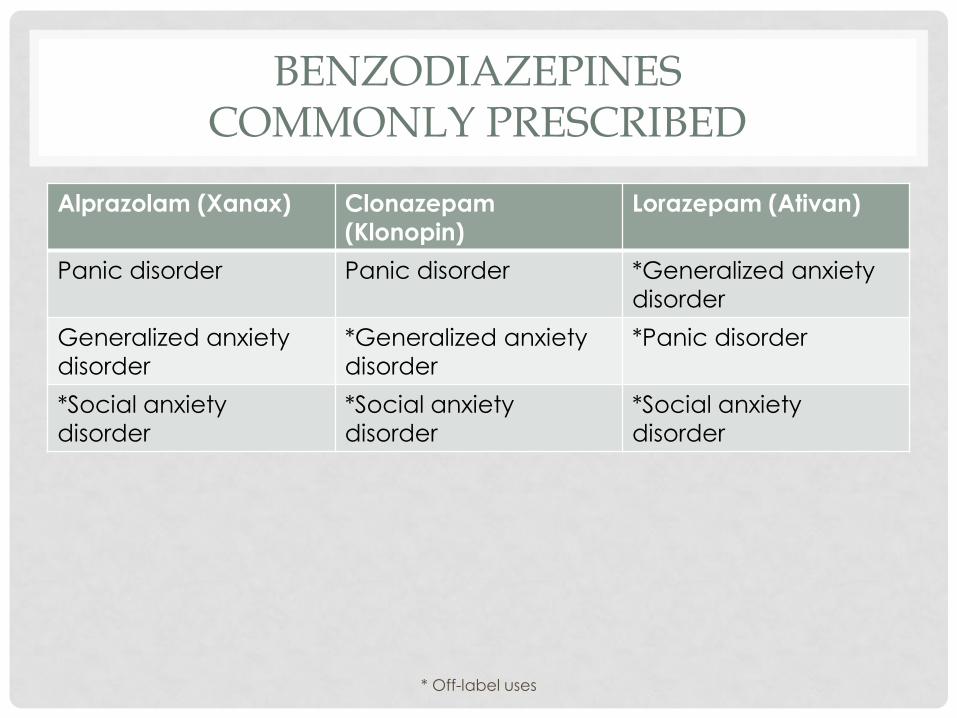
BENZODIAZEPINES COMMONLY PRESCRIBED
Alprazolam (Xanax) Clonazepam
(Klonopin)
Lorazepam (Ativan)
Panic disorder Panic disorder *Generalized anxiety
disorder
Generalized anxiety
disorder
*Generalized anxiety
disorder
*Panic disorder
*Social anxiety
disorder
*Social anxiety
disorder
*Social anxiety
disorder
* Off-label uses

NON-BENZODIAZEPINE FOR ANXIETY DISORDER
Buspirone (BuSpar)
Generalized anxiety disorder
*Social anxiety disorder
*Obsessive-compulsive disorder
• Does not cause dependence
• 2-4 weeks required to reach full effects
• May be used for long-term treatment
*Off-label uses

ANTIDEPRESSANTS FOR ANXIETY DISORDERS
SSRIs SSNRIs MAOIs
Citalopram (Celexa) Duloxetine (Cymbalta) Phenelzine (Nardil)
Escitalopram (Lexapro) Venlafaxine (Effexor) Tranylcypromine (Parnate)
Fluoxetine (Prozac)
Fluvoxamine (Luvox)
Paroxetine (Paxil)
Sertraline (Zoloft)
First-line treatment for acute stress disorders and PTSD
Panic disorders, GAD, SAD, OCD, PTSD
Panic disorders, GAD, SAD, PTSD
Preferable to TCAs because they have a more rapid onset
of action & fewer
problematic side effects
Reserved for treatment-resistant conditions
Panic disorders, GAD, SAD, OCD, PTSD
Risk of life-threatening blood pressure crisis if dietary
restrictions are not followed

OTHER CLASSES OF MEDICATIONS FOR ANXIETY DISORDERS
• Often added if the first course of treatment is ineffective
• Beta-blockers • Atenolol (Tenormin)
• Propranolol (Inderal)
• Antihistamines – nonaddictive alternative to benzodiazepines to lower anxiety levels • Hydroxyzine hydrochloride (Atarax)
• Hydroxyzine pamoate (Vistaril)
• Anticonvulsants • Carbamazepine (Tegretol)
• Gabapentin (Neurontin)
• Valproic acid (Depakote)

DRUG TREATMENT FOR SLEEP DISORDERS

SLEEP DISORDERS RELATED TO OTHER MENTAL DISORDERS
• Most psychiatric disorders are associated with sleep disturbance. Two classifications: • Insomnia – most frequent complaint
• Hypersomnia
• There is evidence that sleep disruption itself may be a precipitating factor in triggering mood and other psychiatric disorders and increases the risk to relapse
• Insomnia is common with anxiety disorders and schizophrenia
• Hypersomnia is associated with mood disorders, personality disorders, bipolar disorder, and uncomplicated grief
MORE ON SLEEP DISORDERS RELATED TO OTHER MENTAL DISORDERS
• Patients tend to focus on their sleep and ignore the
symptoms of the related mental disorder
• For example, patients who wake up frequently at night and
awaken with a difficult mood report that if they could get a
good nights sleep their mood symptoms would improve.
• Poor health habits compound the problems:
• Excessive caffeine use, smoking, inattention to regular sleep
schedule

SUBSTANCE-INDUCED SLEEP DISORDER
• Can result from use or recent discontinuance of a
substance or medication
• Over-the-counter (OTC) medications
• Alcohol
• Decreases deep sleep and REM sleep
• Middle-of-the-night awakenings, difficult returning to sleep
• Nicotine
• It is a stimulant, as levels decline overnight patients wake up
in response to mild withdrawal
• Caffeine
• Difficulty falling asleep, reduces slow wave sleep
• Diuretic – awaken for urination

DRUG TREATMENT FOR INSOMNIA
• Benzodiazepines used as sleep aids • Habit forming (Schedule IV)
• Dalmane
• Restoril
• Halcion
• Prosom
• Doral
• Short-Acting Sedative-Hypnotic Sleep Agents • “Z-hypnotics” are habit forming (Schedule IV)
• Ambien
• Sonata
• Lunesta
Continued…

DRUG TREATMENT FOR INSOMNIA
Continued:
• Melatonin Receptor Agonists
• Not habit forming
• Rozerem
• Antidepressants for insomnia
• Not habit forming
• Trazadone (Desyrel)
• Antihistamines for insomnia
• Tolerance to hypnotic effects develops in 1-2 weeks
• Diphenhydramine (in Benadryl)
• Doxylamine (Unisom)

MELATONIN FOR INSOMNIA
• Melatonin is a hormone naturally secreted in
response to dark to produce sensation of sleepiness
• Melatonin levels decline in the early morning and disappear
during the day to reverse the effect
• Synthetic melatonin is available OTC
• Research actually does not indicate melatonin is
useful in treatment of insomnia
• It does show some effectiveness in managing jet lag and
shift work disorder

MELATONIN, CONTINUED
• It is safe… maybe
• No documented reports of toxicity or overdose
• However:
• There is no identified effective dosage range
• Because it is available OTC and unregulated by the FDA, there is
no standardization of ingredients
• Side effects:
• Nausea
• Headache
• Blood pressure changes

ANTIDEPRESSANT DRUGS

3 HYPOTHESES OF ANTIDEPRESSANTS’ MECHANISM OF ACTION
1. There is a deficiency in one or more
neurotransmitter - 5-HT, NE, or DA (dopamine) –
and increasing these neurotransmitters alleviates
depression.
2. Low levels of neurotransmitters cause receptors to
be more sensitive. Increasing neurotransmitters
results in desensitizing receptors. May answer why
it takes so long for antidepressants to work.
3. Drugs increase production of neurotrophic factors
(to enhance survival of neurons and new synaptic
connections).

TARGET SYMPTOMS
• Antidepressant drugs target symptoms that include:
• Sleep disturbance
• Appetite disturbance
• (increase or decrease)
• Fatigue
• Decreased sex drive
• Psychomotor retardation or agitation
• Diurnal variations in mood
• (usually worse in the morning)
• Impaired concentration or forgetfulness
• Anhedonia
• (inability to experience joy or pleasure in living)

TYPES OF ANTIDEPRESSANTS: TCA
• Tricyclic Antidepressants (TCAs) • Used widely before SSRIs were developed
• Side effects are more prominent than SSRIs
• Some examples: • Amitriptyline (Elavil)
• Clomipramine (Anafranil)
• Imipramine (Tofranil)
• Some side effects & warnings: • Dry mouth
• Constipation
• Blurred vision
• Cardiac toxicity
• Sedation
• Lethal in overdose • Do not take with MAOIs

TYPES OF ANTIDEPRESSANTS: SSRI
• Selective Serotonin Reuptake Inhibitors (SSRIs)
• Do not have side effects common w/TCAs, but have other side effects
• Some examples:
• Citalopram (Celexa), Escitalopram (Lexapro), Fluoxetine
(Prozac), Fluvoxamine (Luvox), Paroxetine (Paxil), Sertraline (Zoloft)
• Some side effects & warnings:
• Agitation, insomnia
• Headache, nausea, vomiting
• Sexual dysfunction
• Withdrawal effects may occur with discontinuation
• Do not take with MAOIs

TYPES OF ANTIDEPRESSANTS: SNRI
• Serotonin-Norepinephrine Reuptake Inhibitors
(SNRIs)
• Some examples:
• Venlafaxine (Effexor) – popular next-step after trying SSRIs
• Duloxetine (Cymbalta) – also decreases neuropathic pain
• Some side effects & warnings:
• Hypertension (Effexor)
• Nausea
• Dry mouth
• Insomnia, agitation
• Sexual dysfunction
• May cause withdrawal

TYPES OF ANTIDEPRESSANTS: SNDI
• Serotonin-Norepinephrine Disinhibitors (SNDIs)
• Effects may be faster than SSRIs
• May be used for sleep disorders
• Only one:
• Mirtazapine (Remeron)
• Some side effects & warnings:
• Sleepiness
• Exaggerated by alcohol, benzodiazepines
• Do not take with MAOIs

TYPES OF ANTIDEPRESSANTS: MAOI
• Monoamine Oxidase Inhibitors (MAOIs)
• Some examples:
• Phenelzine (Nardil), Selegiline (EMSAM), Tranylcypromine
(Parnate)
• Some side effects & warnings:
• Insomnia, agitation
• Nausea
• Confusion
• Do not take with other antidepressants and check with
physician before taking any other prescribed or OTC meds
• Avoid tyramine-rich foods (for example, avacado, fig, aged
meats, most cheese, yeast, beer/wine, protein dietary
supplements)

TYPES OF ANTIDEPRESSANTS: NDRI
• Norepinephrine Dopamine Reuptake Inhibitor
(NDRI)
• Only one:
• Bupropion (Wellbutrin)
• Some side effects & warnings:
• Agitation, insomnia
• Stimulant action may reduce appetite
• Headache, nausea, vomiting
• Very small risk of seizure (at high doses)
• May increase sexual desire
• Used as an aid to quit smoking
• Do not take with MAOIs

PREGNANCY AND ANTIDEPRESSANTS
• SSRI and TCAs
• Risk of preterm birth
• Higher risk for spontaneous abortion
• TCAs
• Congenital malformations of the heart and limbs
• MAOIs
• Severe hypertension and stroke with pregnancy
• Breathing problems in infant
• Withdrawal in infant

MOOD STABILIZERS
TREATMENT OF B IPOLAR DISORDER

BIPOLAR DISORDER
• Episodes of mania alternates with major depression
• Rapid cycling – four or more mood episodes in a 12 month period
• Depressive episodes:
• Same symptoms as major depression, although more
intense
• Lithium & Lamictal are the first-line treatment for acute
depressive episode; Antidepressants are not recommended
(may result in mania)
• Atypical antipsychotics may be added if psychotic features
• Manic episodes:
• Persistent elevated, expansive, or irritable mood
• May necessitate hospitalization

LITHIUM
• Mechanism of action is not well understood
• Low Therapeutic Index – this means the blood level that can cause death is not far above the blood level required for drug effectiveness • Blood level of lithium must be MONITORED on a regular basis
• Adverse Effects: • Nervous/muscular - tremor, confusion, convulsions,
uncoordinated movement
• Digestive – nausea, vomiting, diarrhea
• Cardiac – arrhythmias
• Fluid/electrolyte – polyuria (large output of urine), polydipsia (excessive thirst), edema (swelling)
• Goiter, hypothyroidism

ANTICONVULSANT DRUGS
USED IN TREATMENT OF B IPOLAR DISORDER

VALPROATE (DEPAKOTE, DEPAKENE)
• Divalproex is recommended for mixed episodes
and has been useful for rapid cycling bipolar
disorder
• Common Side Effects:
• Tremor
• Weight gain
• Sedation
• Therapeutic blood level monitoring required
• Liver function tested before and throughout use

CARBAMAZEPINE (TEGRETOL)
• Useful in preventing mania and during episodes of
acute mania
• Common Side Effects:
• Dry mouth
• Constipation
• Urinary retention
• Blurred vision
• Sedation
• Rash
• Blood levels are monitored to avoid toxicity

LAMOTRIGINE (LAMICTAL)
• Approved by FDA for maintenance therapy of
bipolar disorder
• Works well in treating the depression without switching the
patient into mania, like other antidepressants
• Not effective in acute mania
• Promptly report rashes – could be a sign of life-
threatening Stevens-Johnson syndrome
• can be minimized by slow titration to therapeutic doses
OTHER ANTICONVULSANTS
• Other anticonvulsants used as mood stabilizers:
• Gabapentin (Neurontin)
• Topiramate (Topamax)
• Oxcarbazepine (Trileptal)
• None of them have FDA approval as mood
stabilizers
• Studies have not provided strong evidence for their
use as primary treatments for bipolar disorder
• Antipsychotic medications and clonazepam
(Klonopin) are used for calming effect during mania

ANTIPSYCHOTIC DRUGS

POSITIVE VS. NEGATIVE SYMPTOMS OF SCHIZOPHRENIA
Positive Symptoms
• Hallucinations
• Delusions
• Loose association of ideas
• Conversations derailed by unnecessary/tedious details
Negative Symptoms
• Uncommunicative/withdrawn
• Talks about self as “bad” or “no good”
• Extremely sensitive to real/perceived slights
• Lack of energy/motivation

CONVENTIONAL ANTIPSYCHOTICS
• Also known as:
• First-generation antipsychotic drugs
• Typical
• Standard
• These drugs block dopamine to reduce symptoms
• Overactivity of the dopamine system may be responsible for at least some of the symptoms of schizophrenia
• Reduces POSITIVE SYMPTOMS
• delusions (paranoid and grandiose ideas)
• Hallucinations
• These drugs are not first-line treatment anymore

CONVENTIONAL ANTIPSYCHOTICS
• Chlorpromazine (Thorazine)
• Thioridazine (Mellaril)
• Loxapine (Moban)
• Perphenazine (Trilafon)
• Trifluoperazine (generic only)
• Thiothixene (Navane)
• Fluphenazine (Prolixin)
• Haloperidol (Haldol)
• Pimozide (Orap)

SIDE EFFECTS OF CONVENTIONAL ANTIPSYCHOTICS
• Dry mouth
• Urinary retention/hesitancy and constipation
• Blurred vision
• Photosensitivity and dry eyes
• Impotence in men
• Pseudoparkinsonsim (Stiff/stooped posture, shuffling gait, tremor, “pill-rolling”)
• Dystonias (acute contractions of tongue, face, neck, or back)
• Akathisia (tapping foot incessantly, rocking, shifting weight side to side)
• Tardive Dyskinesia (protruding/rolling tongue, smacking, spastic facial distortion)
• Neuroleptic Malignant Syndrome (NMS) – rare, potentially fatal

ATYPICAL ANTIPSYCHOTICS
• These drugs target BOTH positive and negative
symptoms
• Produce fewer motor-related side effects
• For example, tardive dyskinesia and pseudoparkinsonism
• Often chosen as first-line treatment over
conventional drugs
• Increased risk of metabolic syndrome:
• Increased weight, blood glucose, and triglycerides
• Especially clozapine (Clozaril) and olanzapine (Zyprexa)
CLOZAPINE (CLOZARIL)
• Atypical antipsychotic
• Relatively free of motor side effects
• Patients are more likely to adhere to medication regimen than other atypical antipsychotics
• Increased risk of infection • Monitor blood work monthly
• Side Effects: • Drowsiness/Sedation
• Hypersalivation
• Weight gain
• Constipation
• Dizziness
• Dose-related risk of convulsions

RISPERIDONE (RISPERDAL)
• Atypical antipsychotic
• Very low potential for infection risk or convulsions
• High therapeutic doses may cause motor difficulties
• Side Effects:
• Bouts of low blood pressure (fall risk)
• Weight gain
• Sedations
• Sexual dysfunction
• Available as long-acting injection (every 2 weeks)

QUETIAPINE (SEROQUEL)
• Atypical antipsychotic
• High sedation
• Side Effects:
• Weight gain/ risk of metabolic syndrome
• Low risk of motor difficulties

OTHER ATYPICAL ANTIPSYCHOTICS
• Olanzapine (Zyprexa)
• Side effects: sedation, weight gain, high blood glucose w/type 2 diabetes onset, higher risk of metabolic syndrome
• Ziprasidone (Geodon)
• Side effects: dizziness, moderate sedation
• Aripiprazole (Abilify)
• Little sedation or weight gain
• Side effects: insomnia, akathisia
• Paliperidone (Invega)
• Side effects: sedation, orthostasis

DRUG TREATMENT FOR ATTENTION DEFICIT HYPERACTIVITY DISORDER
FOR CHILDREN & ADULTS WI TH ADHD

SYMPTOMS OF ADHD
• Short attention span
• Difficulty listening, even with prompts or redirection
• Easily distracted, loses things, forgetful
• Impulsivity
• Unable to sit still or play quietly
• Acts as if “driven by a motor”
• Talk excessively, blurts out answers before question
is finished, interrupts, intrudes
• Difficulty waiting for own turn

STIMULANT DRUG THERAPY
• Paradoxically, the treatment for ADHD is stimulant drugs:
• Methlphenidate (Ritalin, Concerta & Metadate - longer acting)
• Dextroamphetamines (Adderall)
• Lisdexamfetamine (Vyvanse)
• Side effects:
• Insomnia
• Agitation
• Exacerbation of psychotic thought processes
• Hypertension
• Long-term growth suppression
• Potential for abuse of the drugs

NONSTIMULANT DRUG THERAPY
• Atomoxetine (Strattera)
• Approved for children and adults
• Eliminates risk of abuse, but may not be as effective as
stimulants
• Response developed slowly (up to 3 weeks)
• Common Side Effects:
• Gastrointestinal disturbances
• Reduced appetite, weight loss
• Dizziness
• Fatigue
• Insomnia

INTEGRATIVE THERAPY

EXERCISE
• Exercise
• counteracts symptoms of depression, enhances mood
• increases available serotonin
• Has fewer side effects than antidepressants
• Effects of exercise are:
• Biological
• Social
• Psychological
• A combination of exercise and meditation is helpful
• Clients should consult with a medical professional
before starting an exercise program

DIET
• Nutritional disturbances are common among
people with a mental illness
• Diabetes and obesity are prevalent in people with
psychiatric disorders and require dietary
management
• Nutritional states may cause psychiatric
disturbances
• Lower rates of depression are reported in
vegetarians
• Anemia is often accompanied by depression

NUTRITIONAL SUPPLEMENTS
• Omega 3 fatty acids may be recommended as
adjunct therapy for persons with depression and
bipolar disorder
• Nutritional supplements, SAMe and B vitamins (B6
and folic acid), may improve depression
• B vitamins and Folic acid may be useful for
management of bipolar illness and schizophrenia
• These vitamins augment, rather than replace,
conventional medication therapy
• Research results vary, and results should be
carefully reviewed considering design of the study
and populations examined

RISKS VS. BENEFITS: HERBALS & SUPPLEMENTS
• Many people believe herbal treatments are safer because they are “natural” or may have fewer side effects
• Research has yet to determine their mechanisms of action
• Some herbal treatments, vitamin supplements, herbal preparations, and protein supplements are not safe: • Interactions with conventional drugs
• Detrimental long-term effects to nerves, kidneys, and liver
• May reduce effectiveness of conventional drugs
• No regulation by FDA
• Inconsistent quality or dosing
• We should be discussing herbal supplements with persons served: • Do they help? How much are you taking? How long have you
been taking them?

ST. JOHN’S WORT
• May have serious interactions with a number of conventional medications
• Taking St. John’s Wort with SSRIs or triptans can cause serotonin syndrome: • Abdominal pain, diarrhea
• Sweating, fever
• High heart rate, high blood pressure
• Delirium
• Muscle spasm
• Mood changes (hostility, irritability)
• Death
• It may reduce effectiveness of other medications by reducing blood levels of the drugs

ADDICTION PHARMACOLOGY
ALCOHOL & OPIOID ADDICT ION TREATMENT

ADDICTION PHARMACOLOGY
• Alcohol and drug use affects neurotransmitters and
areas of the brain.
• Medication Assisted Treatment/Pharmacology
Interventions used:
• To manage withdrawal
• To alter drug use

ALCOHOL WITHDRAWAL TREATMENT
• Not all persons who stop drinking require management of withdrawal
• Depends on: • Overall health
• Prior history of withdrawal complications
• Amount person has been drinking
• Length of time drinking
• Naltrexone • Manage level of craving and somatic symptoms
• Disulfiran (Antabuse) • Works on inhibiting drinking because the patient tries to
avoid the unpleasant physical effects caused by antabuse-alcohol reaction

TREATMENT OF OPIOID ADDICTION
• Methadone • Blocks the cravings for and effects of heroin
• Taken every day and is highly addicting
• Levo-alpha-acetylmethadol (LAAM) • Alternative to Methadone effective for 72-96 hours
• Side effects: dizziness, light headedness, constipation, sedation
• Naltrexone • Blocks euphoric effects of opioid for up to 72 hours
• Low toxicity and few side effects
• Buprenorphine (Subutex) • Partial opioid agonist blocks signs and symptoms of opioid
withdrawal
• Suboxone (buprenorphine + naloxone/Narcan) • Supresses withdrawal symptoms and cravings

THE CLINICIAN’S ROLE

WHEN YOUR CLIENT IS ON MEDICATION
• Know the current medication list
• Medication type
• Dose
• Administration times/when it is supposed to be taken
• Common side effects
• Discuss side effects with the agency nurse
• Monitor medication compliance
• Communicate with agency nurse with any concerns
• Watch for abuse or addiction
• Refer the client to the agency nurse if
• he/she has any questions about their medication
• Becomes pregnant/thinking of becoming pregnant
ADHERENCE
• The clinician should emphasize the importance of taking
medications as prescribed
• Help the client identify and resolve obstacles to adherence
• Potential obstacles to adherence:
• Cost of medication
• Negative attitudes of self or family towards taking medications
• Frequent dosing/many pills
• Side effects
• Consider depot injection or extended release patches,
when it is an option
• Involve the doctor in discussion of any fears or problems
in the use of medication and management of side
effects

OTHER CONSIDERATIONS RELATED TO ADHERENCE
• Patient family education is significantly related to
adherence with medication regimen
• Medications may be needed over long periods of
time
• Therapeutic interventions should be made to assist
the persons served maintain occupation and social
relationships

RECOGNIZING SIGNS OF RELAPSE OR NONADHERENCE
• Be aware that the medication may take 2 or more weeks to become effective
• The key to adherence is: • Shared decision making between the person served and
psychiatrist
• The person served perspective of their diagnosis is critical in their acceptance and ability to manage symptoms
• Research demonstrates people want more than watered-down, simplistic information • Persons served need current, evidence-based information
• Nurses and physicians are in a position to help to recognize side effects and interactions among drugs that are prescribed for physical and mental illness

HANDLING THE COSTS OF MEDICATION
• The doctor should be alerted to restrictions in
inability to pay
• They may prescribe an equally effective medication that
costs less money
• Coordinate with the pharmacist to enroll the client
in drug company assistance programs