psoriatic arthritis - boca raton regional hospitalweb.brrh.com/msl/im2019/im saturday/saturday - 2 -...
TRANSCRIPT

©2017 MFMER | slide-1
Psoriatic Arthritis
Benjamin Wang, M.D., FRCPC Division of Rheumatology
Mayo Clinic Jacksonville, FL
Boca Raton Regional Hospital Internal Medicine Conference 2019

©2017 MFMER | slide-2
Disclosures
Nothing to disclose

©2017 MFMER | slide-3
Outline
• Clinical features
• Pathophysiology
• Treatment

©2017 MFMER | slide-4
• Inflammatory arthritis
• Many variants and clinical forms
• Seronegative
• Destructive, disabling
• Occurs in up to 30% of persons with psoriasis
• Arthritis precede skin disease
• Increased cardiovascular mortality
© Merck Manual

©2017 MFMER | slide-5

©2017 MFMER | slide-6
Arthritis
• Symmetric polyarthritis
• Asymmetric oligoarthritis
• DIP-included arthritis
• Spondylitis
• Arthritis mutilans
Papazoglou A et al. “Psoriasis” in Brent LH, SG Arthritis (2016)
Torpy JM et al. JAMA. 2011;306(8):896

©2017 MFMER | slide-7
Symmetric Polyarthritis • May be mistaken for rheumatoid arthritis
• “Seronegative RA” may actually be psoriatic arthritis
• More joint erythema than RA
• Less periarticular osteopenia on x-ray than rheumatoid arthritis
Papazoglou A et al. “Psoriasis” in Brent LH, SG Arthritis (2016)

©2017 MFMER | slide-8
Asymmetric Oligoarthritis • Monoarthritis of a large joint (knee, hip, elbow, ankle) – often associated with spondylitis
• Oligoarthritis, often asymmetric, of large joints
• Small joint oligoarthritis
• May evolve into a symmetric polyarthritis
Michet CJ et al. Ann Rheum Dis 2005;64:1068–1070. Emad Y et al. J Rheum 2005;39(10):1979-1986

©2017 MFMER | slide-9
Spondylitis
• Back pain Inflammatory characteristics
• prolonged AM stiffness
• better with use
• responsive to anti-inflammatories and corticosteroids
• May be asymptomatic
• May accompany peripheral arthritis
• Always worth doing: SI joint x-rays
Baraliakos X et al. Clin Exp Rheumatol 2015; 33 (Suppl. 93):S31-S35.
© eMedicine 2005

©2017 MFMER | slide-10
DIP-included Polyarthritis
• May be mistaken for OA (Heberden nodes) and vice-versa
• Look for nail dystrophy, pitting and onycholysis
• Look for periungual erythema Martel W et al. AJR 1980;134:125-135
Sandre MK. Sem Arthritis Rheum 2014; 44:162-169

©2017 MFMER | slide-11
Arthritis Mutilans
• Aggressive, destructive form (1%)
• May affect all joint areas
• “Telescoping digits” and “flail joints”
• Advanced osteolysis Alejandra-Lopez R et al. Int. J. Clin. Rheumatol. (2018) 13(6), 384-387
Butendieck Jr RR and Abril A. J Rheum 2013; 40:1921-1922

©2017 MFMER | slide-12
Enthesitis
• Enthesis: a bone-tendon or bone-ligament interface
• Specialized histology
• Inflammatory potential
• History of heel pain or Achilles insertional pain
• Inflammation leads to new bone formation—osteophytes, syndesmophytes

©2017 MFMER | slide-13
Tendonitis and Dactylitis
McGonagle D et al. Nature Rev Rheumatology 2019; 15:113-121
Kaeley GS et al. Sem Arthritis Rheum 2018;48:35–43.
© American Academy of Dermatology

©2017 MFMER | slide-14
Combinations of the Above
• Polyarthritis with spondylitis
• Oligoarthritis with spondylitis
• DIP-only with spondylitis (uncommon)
• Spondylitis
• Enthesitis and/or tendonitis and/or dactylitis may accompany any of the above
• Other: uveitis, IBD and enteropathic arthritis

©2017 MFMER | slide-15
How is Psoriatic Arthritis Classified?
• No autoantibody production yet inflammatory
• Involvement of innate immune system more than adaptive immunity
• A member of a broad family of ‘seronegative’ conditions
• Ankylosing spondylitis • Reactive arthritis • Psoriasis • Uveitis • Inflammatory bowel
disease
Generali E et al. Autoimmunity Reviews 17 (2018) 935–941

©2017 MFMER | slide-16
HLA-B27 and Psoriatic Arthritis
• Prevalence of HLA-B27 varies according to the clinical presentation:
• Psoriasis: 5% (increases risk of developing PsA)
• Psoriatic arthritis (peripheral): 20%
• Psoriatic arthritis (axial): 70%
• HLA-C06 is a biomarker of skin disease, with no influence on the development of joint disease

©2017 MFMER | slide-17
Genetic Contributions

©2017 MFMER | slide-18
Gene-Environment Interactions
• Trauma and the Koebner phenomenon: local trauma found in 25% on patients prior to disease onset
• Streptococcal antibodies: triggers shift in CD8/CD4 balance
• Microbiota: significant reductions in Akkermansia, Ruminococcus, and Pseudobutyrivibrio species; increased soluble IgA and decreased RANKL concentrations.
• Smoking
Veale DJ and Fearon U. Lancet 2018; 391: 2273–84

©2017 MFMER | slide-19
Pathophysiology
• Macroscopic vascular pattern
• The presence of immature vessels suggests that many of the vessels remain in a plastic state and, thus, primed for endothelial cell activation and sprouting
• Relative hypoxia induces upregulation of key metabolic pathways
• Increased expression of vascular growth factors permits ingress of inflammatory cells
Veale DJ and Fearon U. Lancet 2018; 391: 2273–84

©2017 MFMER | slide-20
• A variety of cell types are active to mediate tissue inflammation and destruction
• A combination of innate and adaptive immunity
Pathophysiology
Veale DJ and Fearon U. Lancet 2018; 391: 2273–84

©2017 MFMER | slide-21
Drug Therapy
• Symptom relief
• NSAIDs
• Corticosteroids
• Disease-modifying antirheumatic drugs (DMARDs)
• Methotrexate
• Sulfasalazine
• Hydroxychloroquine
• Leflunomide
• Azathioprine
• Mycophenolate

©2017 MFMER | slide-22
Biologic DMARDs for Psoriatic Arthritis
• Directed at cytokines
• TNF inhibitors: etanercept (Enbrel®), infliximab (Remicade ®), adalimumab (Humira®), golimumab (Simponi®), certolizumab (Cimzia®)
• IL-12/23 antagonist: uskekinumab (Stelara®)
• IL-17 antagonists: secukinumab (Cosentyx®), ixekizumab (Taltz®)
• Directed at cells:
• T cell-directed therapy: abatacept (Orencia®)
• Small molecules:
• Phosphodiesterase-4 antagonist: apremalast (Otezla®)
• Tofacitinib (Xeljanz®)

©2017 MFMER | slide-23
Coates LC et al. Semi Arthritis Rheum 2016; 46:291–304

©2017 MFMER | slide-24
Infliximab – IMPACT2 Trial (2005)
Antoni C et al. Ann Rheum Dis 2005;64:1150–1157.
©2017 MFMER | slide-25
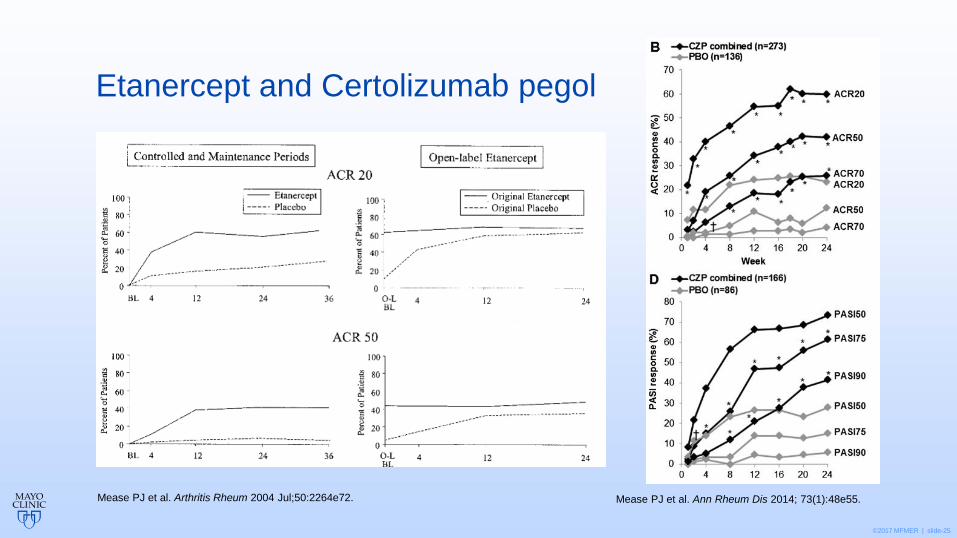
Etanercept and Certolizumab pegol
Mease PJ et al. Arthritis Rheum 2004 Jul;50:2264e72. Mease PJ et al. Ann Rheum Dis 2014; 73(1):48e55.

©2017 MFMER | slide-26
Secukinumab (Cosentyx®)
• FUTURE2 Trial
• 76 center multinational RCT
• 397 patients randomized in 1:1:1:1 ratio
• SCK 300 mg/mo
• SCK 150 mg/mo
• SCK 75 mg/mo
• Placebo
• SCK 300 mg and 150 mg doses similar
• In TNF nonresponders, SCK 300 mg was superior
McInnes IB et al. Lancet 2015;386(9999):1137e46.

©2017 MFMER | slide-27
Apremilast (Otezla®) Tofacitinib (Xeljanz®)
Gladman D et al. N Engl J Med 2017 19;377(16):1525e36. Kavanaugh A et al. Ann Rheum Dis 2014;73:1020–6.
©2017 MFMER | slide-28
Summary
• An inflammatory, erosive form of arthritis accompanied by psoriasis
• Occurs in 30% of people with psoriasis
• Varied clinical manifestations
• Cellular and cytokine-mediated pathophysiology
• Growing selection of directed biologic therapy encompassing various mechanisms of action
