proton-pump inhibitors reduce gastrointestinal events ... investigations proton-pump inhibitors...
TRANSCRIPT
Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 7 , N O . 1 4 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 5 . 1 2 . 0 6 8
ORIGINAL INVESTIGATIONS
Proton-Pump Inhibitors ReduceGastrointestinal Events Regardlessof Aspirin Dose in Patients RequiringDual Antiplatelet Therapy
Muthiah Vaduganathan, MD, MPH,a Deepak L. Bhatt, MD, MPH,a Byron L. Cryer, MD,b Yuyin Liu, MS,c,dWen-Hua Hsieh, PHD,c Gheorghe Doros, PHD,c,d Marc Cohen, MD,e Angel Lanas, MD, DSC,f
Thomas J. Schnitzer, MD, PHD,g Thomas L. Shook, MD,h Pablo Lapuerta, MD,i Mark A. Goldsmith, MD, PHD,j
Loren Laine, MD,k,l Christopher P. Cannon, MD,a,c on behalf of the COGENT Investigators
ABSTRACT
FrobU
Re
BACKGROUND The COGENT (Clopidogrel and the Optimization of Gastrointestinal Events Trial) showed that proton-
pump inhibitors (PPIs) safely reduced rates of gastrointestinal (GI) events in patients requiring dual antiplatelet therapy
(DAPT). However, utilization of appropriate prophylactic PPI therapy remains suboptimal, especially with low-dose
aspirin.
OBJECTIVES The authors investigated the safety and efficacy of PPI therapy in patients receiving DAPT in low- and
high-dose aspirin subsets.
METHODS Randomized patients with available aspirin dosing information in COGENT (N ¼ 3,752) were divided into
“low-dose” (#100 mg) and “high-dose” (>100 mg) aspirin groups. The primary GI and cardiovascular endpoints were
composite upper GI events and major adverse cardiac events, respectively. All events were adjudicated by independent,
blinded gastroenterologists and cardiologists.
RESULTS Median duration of follow-up was 110 days. Low-dose aspirin users (n ¼ 2,480; 66.1%) were more likely to be
older, female, and have higher rates of peripheral artery disease, prior stroke, and hypertension, whereas high-dose
aspirin users (n ¼ 1,272; 33.9%) had higher rates of hyperlipidemia, smoking, a history of percutaneous coronary
intervention, and were more than twice as likely to be enrolled from sites within the United States (80.4% vs. 39.8%).
High-dose aspirin was associated with similar 180-day Kaplan-Meier estimates of adjudicated composite GI events
(1.7% vs. 2.1%; adjusted hazard ratio: 0.88; 95% confidence interval: 0.46 to 1.66) and major adverse cardiac events
(4.8% vs. 5.5%; adjusted hazard ratio: 0.73; 95% confidence interval: 0.48 to 1.11) compared with low-dose aspirin.
Randomization to PPI therapy reduced 180-day Kaplan-Meier estimates of the primary GI endpoint in low-dose
(1.2% vs. 3.1%) and high-dose aspirin subsets (0.9% vs. 2.6%; p for interaction ¼ 0.80), and did not adversely affect
the primary cardiovascular endpoint in either group.
CONCLUSIONS Gastroprotection with PPI therapy should be utilized in appropriately selected patients with
coronary artery disease requiring DAPT, even if the patients are on low-dose aspirin. (Clopidogrel and the Optimization
of Gastrointestinal Events Trial [COGENT]; NCT00557921) (J Am Coll Cardiol 2016;67:1661–71)
© 2016 by the American College of Cardiology Foundation.
m the aBrigham and Women’s Hospital Heart & Vascular Center and Harvard Medical School, Boston, Massachusetts;
niversity of Texas Southwestern and Veterans Affairs North Texas Health Care System, Dallas, Texas; cHarvard Clinical
search Institute, Boston, Massachusetts; dDepartment of Biostatistics, Boston University, Boston, Massachusetts; eNewark

ABBR EV I A T I ON S
AND ACRONYMS
CAD = coronary artery disease
CI = confidence interval
DAPT = dual antiplatelet
therapy
GERD = gastroesophageal
reflux disease
GI = gastrointestinal
HR = hazard ratios
IQR = interquartile range
NNT = number needed to treat
PCI = percutaneous coronary
intervention
PPI = proton-pump inhibitor
SODA = Severity of Dyspepsia
Assessment
Beth Israel
Investigaci
and RehabihParexel In
ceuticals, C
System, W
conducted
The study i
The sponso
Elsevier Pr
VA Researc
Committee
Research I
honoraria f
(editor in c
American C
mittee of C
Care (secre
funding fro
Sanofi, and
the Americ
Takeda. Dr
from Bayer
national. D
Dr. Laine s
boards of B
Boehringer
authors ha
Manuscript
Vaduganathan et al. J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6
PPIs and Aspirin Dose in COGENT A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1
1662
G iven similar antiplatelet inhibitionand theoretically lower bleedingrisk (1–3), lower-dose aspirin is
generally preferred for secondary preventionof cardiovascular events compared withhigher-dose aspirin (4), especially whenused in combination with more potent P2Y12
antagonists (5). Dual antiplatelet therapy(DAPT) poses significant risks of bleeding,particularly gastrointestinal (GI) bleeding,even with low-dose aspirin (6). GI bleedingin high-risk patients with coronary arterydisease (CAD) is independently associatedwith poor prognosis (7), and on-treatmentdyspepsia appears to be clinically importantand may influence compliance with anti-platelet therapy (8). As such, safe and effec-tive strategies limiting gastric toxicity are
much needed.
SEE PAGE 1672
The COGENT (Clopidogrel and the Optimizationof Gastrointestinal Events Trial; NCT00557921),despite being terminated prematurely due to loss offunding, demonstrated that omeprazole reducedrates of composite upper GI events (1.1% vs. 2.9%;p < 0.001) (9) and patient-reported dyspepsia (10)
Medical Center, Newark, New Jersey; fUniversity of Zaragoza, In
ón Biomédica en Red en Enfermedades Hepáticas y Digestivas, Z
litation and Internal Medicine—Rheumatology, Northwestern Univ
ternational, Waltham, Massachusetts; iLexicon Pharmaceuticals,
ambridge, Massachusetts; kYale School of Medicine, New Haven
est Haven, Connecticut. The COGENT was funded by Cogentus P
independently with biostatistical support from an independent te
nvestigators had full access to the trial database and retained com
r did not have right to review or approve the final manuscript.
actice Update Cardiology, Medscape Cardiology, and Regado Bios
h Institute and Society of Cardiovascular Patient Care; chairs
; is vice-chair of the ACTION Registry Steering Committee; serve
nstitute, Harvard Clinical Research Institute, Mayo Clinic, and
rom American College of Cardiology (senior associate editor, Clin
hief, Harvard Heart Letter), HMP Communications (editor in c
ollege of Cardiology (guest editor; associate editor), Population H
OMPASS), Slack Publications (chief medical editor, Cardiology To
tary/treasurer), and WebMD (CME steering committees); is deput
m Amarin, AstraZeneca, Bristol-Myers Squibb, Eisai, Ethicon, For
The Medicines Company; is a site co-investigator for Biotronik, B
an College of Cardiology; and performs unfunded research for Co
. Cryer has served as a consultant to Cogent Pharmaceuticals. D
Pharma AG; and has served on advisory boards for Bayer Pharm
r. Lapuerta is an employee of Lexicon Pharmaceuticals. Dr. Goldsm
erved on data safety monitoring boards for Bayer and Bristol-My
ristol-Myers Squibb, Lipimedix, and Pfizer; and has received resea
Ingelheim, CSL Behring, Essentialis, GlaxoSmithKline, Janssen
ve reported that they have no relationships relevant to the conte
received November 9, 2015; revised manuscript received Decem
at 180 days compared with placebo in patients withCAD requiring DAPT, and achieved this withoutincreasing rates of major adverse cardiac events(MACE) (9). Whether proton-pump inhibitor (PPI) usereduces GI risk consistently across aspirin doses hasnot definitively been established. Furthermore,utilization of appropriate prophylactic PPI therapyremains suboptimal, especially with low-dose aspirin(11). In this context, our post hoc analysis of theCOGENT aimed to determine the overall GI andcardiovascular safety and efficacy of PPI therapy inpatients on low-dose and high-dose aspirin.
METHODS
STUDY POPULATION. The study design and primaryresults of COGENT have been previously described(9). In brief, the COGENT was a global, prospec-tive, phase III randomized, placebo-controlled,double-blind, double-dummy clinical trial of afixed-combination of clopidogrel 75 mg and omepra-zole 20 mg compared with clopidogrel 75 mg alone.Daily enteric-coated aspirin was administered to allstudy patients in open-label fashion, but specificdosing was left to the treating clinician. Patients olderthan 21 years of age requiring DAPT for at least12 months, regardless of indication, were included aslong as P2Y12 therapy was initiated #21 days before
stituto de Investigación Sanitaria Aragón, Centro de
aragoza, Spain; gDepartments of Physical Medicine
ersity Feinberg School of Medicine, Chicago, Illinois;
Basking Ridge, New Jersey; jConstellation Pharma-
, Connecticut; and the lVA Connecticut Healthcare
harmaceuticals; however, this post hoc analysis was
am from Harvard Clinical Research Institute (HCRI).
plete control on the decision to pursue publication.
Dr. Bhatt serves on the advisory boards of Cardax,
ciences; serves on the boards of directors of Boston
the American Heart Association Quality Oversight
s on data monitoring committees for Duke Clinical
Population Health Research Institute; has received
ical Trials and News, ACC.org), Belvoir Publications
hief, Journal of Invasive Cardiology), Journal of the
ealth Research Institute (clinical trial steering com-
day’s Intervention), Society of Cardiovascular Patient
y editor of Clinical Cardiology; has received research
est Laboratories, Ischemix, Medtronic, Pfizer, Roche,
oston Scientific, and St. Jude Medical; is a trustee of
gentus (chair of COGENT), FlowCo, PLx Pharma, and
r. Lanas has received an investigator-initiated grant
a AG. Dr. Shook is an employee of PAREXEL Inter-
ith is an employee of Constellation Pharmaceuticals.
ers Squibb. Dr. Cannon has served on the advisory
rch funding from Accumetrics, Arisaph, AstraZeneca,
, Merck Regeneron, Sanofi, and Takeda. All other
nts of this paper to disclose.
ber 13, 2015, accepted December 22, 2015.

J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6 Vaduganathan et al.A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1 PPIs and Aspirin Dose in COGENT
1663
enrollment. Exclusion criteria included anticipatedhospital discharge within 48 h, recent use of gastro-protection (including PPIs, H2-receptor antagonists,sucralfate, or misoprostol), known GI erosive esoph-agitis or variceal disease, prior non-endoscopic gastricsurgery, concomitant use of oral anticoagulationtherapy (which could not be safely discontinued atstudy entry), and recent exposure to fibrinolytictherapy. The ethics committees and institutional re-view boards of each individual site locally approvedthe study protocol, and all patients provided explicitinformed consent for trial participation.
STUDY ENDPOINTS. The pre-specified primary GIendpoint of the overall COGENT and the currentanalysis was composite upper GI clinical events(including overt upper GI bleeding of known orunknown origin, bleeding of presumed GI origin with aclinically significant reduction in hematocrit, symp-tomatic gastroduodenal ulcer, persistent GI pain withevidence of endoscopy-confirmed gastroduodenalerosions, obstruction, or perforation). The secondaryGI endpoint was symptomatic, endoscopy-confirmederosive esophagitis (gastroesophageal reflux disease[GERD]). Non–GI-related bleeding events werealso documented. The pre-specified primary cardio-vascular endpoint of the overall COGENT and the
FIGURE 1 Distribution of Aspirin Dosing Over Time
1500
1400
1300
1200
1100
1000
900
800
700
600
500
400
300
200
100
0
FREQ
UENC
Y
1300
1200
1100
1000
900
800
700
600
500
400
300
200
100
0
FREQ
UENC
Y
75mg 81mg 150mg 162mg 300mg 325mgDaily Aspirin Dose Administered at Baseline
75mg 81mDaily Aspirin
1415
1065
196
9730
949
1257
104
BaselineA B
Histogram illustrates the specific, open-label aspirin doses used in the C
COGENT ¼ Clopidogrel and the Optimization of Gastrointestinal Events
current analysis was the composite of cardiovasculardeath, nonfatal myocardial infarction, coronaryrevascularization, or ischemic stroke. All GI andcardiovascular events were blindly adjudicated byteams of independent gastroenterologists and cardi-ologists, respectively. Investigator-reported GI andcardiovascular events as well as patient-reporteddyspepsia symptoms, assessed using the Severity ofDyspepsia Assessment (SODA) questionnaire (12,13) at4- and 24-week follow-up, were also reported.
STATISTICAL ANALYSIS. Patients in the intention-to-treat population were divided into 2 groups:1) “low-dose” aspirin, defined as daily maintenancedoses of 75 mg or 81 mg; and 2) “high-dose” aspirin,defined as daily maintenance doses of 150 mg, 162 mg,300 mg, or 325 mg. Baseline characteristics, along withGI and cardiovascular outcomes, were compared inboth treatment arms in low- and high-dose aspirinsubsets. Discrete variables are presented as n (%)and compared using chi-square or Fisher exact tests,whereas continuous variables are presented asmean� SD andmedian (interquartile range [IQR]), andcompared using Student t tests. All clinical endpointsare presented as Kaplan-Meier estimates at 180 days.
Interaction analyses were performed to determinethe interaction between treatment assignment (with
1000
900
800
700
600
500
400
300
200
100
0
FREQ
UENC
Y
g 150mg 162mg 300mg 325mg Dose Administered at Week 4
75mg 81mg 150mg 162mg 300mg 325mgDaily Aspirin Dose Administered at Week 8
5
162
92
19
805
986 978
97 81
14
701
Week 4 Week 8C
OGENT at baseline (A), 4-week follow-up (B), and 8-week follow-up (C).
Trial.

TABLE 1 Baseline Characteristics
Low-Dose Aspirin(75 mg or 81 mg)
High-Dose Aspirin(150 mg, 162 mg, 300 mg, or 325 mg)
p ValueHigh- vs. Low-Dose Aspirin†
p ValueInteraction BetweenAspirin Dose and
TreatmentGroup‡
Omeprazole(n ¼ 1,231)
Placebo(n ¼ 1,249) p Value*
Omeprazole(n ¼ 638)
Placebo(n ¼ 634) p Value*
Age, yrs
Mean � SD (n) 68.2 � 10.2 (1,230) 68.0 � 10.4 (1,245) 0.71 63.6 � 11.4 (638) 63.8 � 11.3 (634) 0.75 <0.001 0.62
Median (IQR) 69.0 (64.0–75.0) 69.0 (63.0–75.0) 65.0 (55.0–71.0) 66.0 (56.0–72.0)
Range, min, max 23.0, 94.0 31.0, 93.0 33.0, 94.0 28.0, 91.0
Male 64.2 (790/1,231) 66.0 (823/1,247) 0.34 71.9 (459/638) 76.3 (484/634) 0.07 <0.001 0.33
White race§ 93.8 (1,154/1,230) 94.5 (1,178/1,246) 0.44 93.4 (595/637) 92.9 (589/634) 0.72 0.16 0.45
United States 37.6 (463/1,231) 39.8 (497/1,249) 0.27 79.3 (506/638) 80.4 (510/634) 0.62 <0.001 0.90
Body mass index, kg/m2
Mean � SD (n) 28.5 � 5.1 (1,217) 28.7 � 5.0 (1,239) 0.28 30.4 � 5.9 (634) 30.3 � 8.9 (628) 0.70 <0.001 0.36
Median (IQR) 27.8 (25.0-31.2) 28.0 (25.3-31.5) 29.7 (26.5-33.2) 29.0 (25.9-33.5)
Range, min, max 16.5, 60.3 16.8, 55.9 14.4, 71.1 17.5, 202.9
Negative for H. pylori 44.5 (548/1,231) 44.5 (556/1,249) 1.00 67.1 (428/638) 65.9 (418/634) 0.66 <0.001 0.72
NSAID use 9.3 (114/1,231) 9.0 (112/1,249) 0.80 7.2 (46/638) 8.2 (52/634) 0.51 0.58 0.49
Major indications for dualantiplatelet therapy
PCIk 64.3 (784/1,220) 61.6 (758/1,231) 0.17 87.4 (554/634) 91.3 (577/632) 0.02 <0.001 0.01
ACS 43.6 (533/1,223) 43.5 (534/1,228) 0.96 39.2 (248/633) 40.9 (258/631) 0.54 0.28 0.59
Both PCI and ACS 27.7 (339/1,224) 27.6 (340/1,234) 0.94 35.3 (224/635) 37.8 (239/632) 0.35 <0.001 0.43
Cardiovascular history
MI 31.0 (379/1,223) 28.1 (345/1,229) 0.11 29.2 (185/634) 29.5 (186/631) 0.91 0.56 0.31
Peripheral artery disease 13.2 (161/1,223) 13.2 (162/1,231) 1.00 9.8 (62/635) 9.5 (60/631) 0.88 0.02 0.90
Stroke 9.1 (111/1,223) 9.9 (122/1,231) 0.48 3.6 (23/635) 4.6 (29/631) 0.38 <0.001 0.63
Other 47.5 (581/1,222) 49.7 (611/1,230) 0.29 52.3 (332/635) 53.2 (336/631) 0.73 0.14 0.74
Cardiovascular risk factors
Hypertension 81.7 (1,002/1,226) 82.9 (1,029/1,241) 0.44 76.7 (488/636) 78.5 (497/633) 0.45 0.02 0.90
Diabetes 30.6 (375/1,226) 28.4 (352/1,241) 0.23 33.8 (215/636) 29.1 (184/633) 0.07 0.75 0.45
Hypercholesterolemia 74.7 (916/1,226) 72.6 (901/1,241) 0.23 87.6 (557/636) 86.1 (545/633) 0.44 <0.001 0.91
Other 40.7 (498/1,225) 39.2 (486/1,239) 0.47 42.8 (272/636) 42.7 (270/633) 0.97 0.15 0.70
Current smoking¶ 12.7 (155/1,223) 14.7 (181/1,235) 0.15 15.8 (100/632) 16.6 (103/622) 0.72 0.28 0.56
Current alcohol use# 46.3 (567/1,224) 47.9 (596/1,245) 0.44 48.0 (306/637) 50.6 (320/632) 0.36 0.26 0.76
Follow-up days
Mean � SD (n) 98.7 � 73.0 (1,231) 96.4 � 73.0 (1,249) 0.44 133.5 � 87.6 (638) 129.1 � 78.1 (634) 0.34 <0.001 0.68
Median (IQR) 78.0 (54.0–136.0) 67.0 (52.0–126.0) 118.0 (58.0–175.0) 115.0 (57.0–178.0)
Range, min, max 0.0, 1,090.0 0.0, 840.0 0.0, 916.0 0.0, 484.0
History of GI bleedingor ulcer
4.1 (50/1,231) 3.8 (47/1,249) 0.70 4.1 (26/638) 5.0 (32/634) 0.41 0.19 0.37
Continued on the next page
Vaduganathan et al. J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6
PPIs and Aspirin Dose in COGENT A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1
1664
PPI or placebo) and aspirin dose using the Breslow-Day test for discrete variables, one-way analysis ofvariance tests for continuous variables, and Coxproportional hazards models for time-dependentvariables. Global region was categorized as UnitedStates- and non–United States-based on site of en-rollment. Cumulative incidence curves were con-structed for the primary GI and cardiovascularendpoints, stratified by treatment assignment (withPPI or placebo), separately for low- and high-doseaspirin dosing subsets. The number needed to treat(NNT) to prevent 1 major composite upper GI eventafter 6 months of PPI therapy was calculated usingthe formula: NNT ¼ 1 / absolute risk reduction (whereabsolute risk reduction was equal to Kaplan-Meier
estimates of event rates at 180 days in the placebogroup minus that in the omeprazole group). Major GIand cardiovascular events were also comparedbetween low- and high-dose aspirin groups. Toaccount for confounding by indication, Cox propor-tional hazards models were used to estimate effectsizes of high- versus low-dose aspirin, expressed ashazard ratios (HRs) and 95% confidence intervals (CI).Multivariate models accounted for a pre-determinedset of high-risk covariates including age, sex,region (United States vs. non-United States), percu-taneous coronary intervention (PCI), acute coronarysyndrome presentation, history of GI bleeding orulcer, and PPI treatment assignment. No adjustmentsfor multiple comparisons were made. A p value

TABLE 1 Continued
Low-Dose Aspirin(75 mg or 81 mg)
High-Dose Aspirin(150 mg, 162 mg, 300 mg, or 325 mg)
p ValueHigh- vs. Low-Dose Aspirin†
p ValueInteraction BetweenAspirin Dose and
TreatmentGroup‡
Omeprazole(n ¼ 1,231)
Placebo(n ¼ 1,249) p Value*
Omeprazole(n ¼ 638)
Placebo(n ¼ 634) p Value*
Medication at study entry
Aspirin 73.3 (902/1,231) 71.7 (896/1,249) 0.39 84.6 (540/638) 85.5 (542/634) 0.67 <0.001 0.43
Clopidogrel 57.0 (702/1,231) 55.6 (695/1,249) 0.49 79.3 (506/638) 81.7 (518/634) 0.28 <0.001 0.20
Other antiplatelet and oralanticoagulation agents
0.7 (9/1,231) 0.2 (2/1,249) 0.03 0.2 (1/638) 0.8 (5/634) 0.10 0.03 0.01
Baseline SODA scores
Pain intensity
Mean � SD (n) 5.9 � 7.3 (1,094) 6.3 � 7.5 (1,122) 0.27 5.5 � 7.0 (512) 6.5 � 7.7 (499) 0.02 0.49 0.20
Median (IQR) 2.0 (2.0–6.0) 2.0 (2.0–9.0) 2.0 (2.0–2.0) 2.0 (2.0–9.0)
Range, min, max 2.0, 37.0 2.0, 37.0 2.0, 33.0 2.0, 36.0
Non-pain symptom
Mean � SD (n) 11.0 � 3.5 (1,190) 10.9 � 3.5 (1,221) 0.41 10.7 � 3.3 (627) 10.7 � 3.5 (625) 0.88 0.21 0.54
Median (IQR) 12.0 (7.0–13.0) 10.0 (7.0–13.0) 10.0 (7.0–13.0) 10.0 (7.0–13.0)
Range, min, max 7.0, 24.0 7.0, 26.0 7.0, 20.0 7.0, 22.0
Satisfaction
Mean � SD (n) 17.9 � 5.2 (1,192) 18.0 � 5.3 (1,221) 0.65 17.8 � 5.5 (627) 17.2 � 5.7 (625) 0.09 0.01 0.09
Median (IQR) 20.0 (13.0–23.0) 20.0 (13.0–23.0) 20.0 (11.0–23.0) 18.0 (11.0–23.0)
Range, min, max 2.0, 23.0 2.0, 23.0 2.0, 23.0 2.0, 23.0
Values are % (n/N for characteristic) unless otherwise indicated. *Within-group, unadjusted comparison between omeprazole and placebo treatment arms. †Between-group, unadjusted comparisonbetween low-dose vs. high-dose aspirin groups in placebo patients alone. ‡Interaction testing between aspirin dosing group and treatment assignment (with proton-pump inhibitor or placebo). §Race wasreported by the investigator. kRecent PCI defined as occurring within 14 days of study randomization. ¶The numerator includes patients who are currently using cigarettes, cigars, pipes, or chewing tobacco.#The numerator includes patients who are currently having <1 drink weekly, 1 to 2 drinks weekly, 1 drink on most days, 2 drinks on most days, 3 or more drinks on most days, or having drinks occasionally.
ACS ¼ acute coronary syndrome; GI ¼ gastrointestinal; IQR ¼ interquartile range; MI ¼ myocardial infarction; NSAID ¼ nonsteroidal anti-inflammatory drug; PCI ¼ percutaneous coronary intervention;SODA ¼ Severity of Dyspepsia Assessment.
J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6 Vaduganathan et al.A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1 PPIs and Aspirin Dose in COGENT
1665
of <0.05 was considered statistically significant. Allstatistical analyses were performed using SAS version9.4 (SAS Institute, Cary, North Carolina).
RESULTS
The COGENT was prematurely terminated due tothe sponsor filing for bankruptcy. From January 2008to December 2008, the COGENT randomized 3,761patients from 393 sites across 15 countries. Of thetotal randomized, intention-to-treat cohort, 3,752(99.8%) patients had available aspirin dosing infor-mation. Patients were divided into low-dose (#100mg; n ¼ 2,480; 66.1%) and high-dose (>100 mg;n ¼ 1,272; 33.9%) aspirin groups. Aspirin doses of75 or 81 mg daily were consistently the mostfrequently administered, followed by 325 mg, atbaseline and all major follow-up time points in theCOGENT (Figure 1).
BASELINE CHARACTERISTICS. The baseline charac-teristics of patients assigned to PPI and placebo armswere well-balanced in both aspirin subsets (Table 1).However, clinical profiles varied substantially byaspirin dosing. Low-dose aspirin therapy was morefrequently utilized in older patients, women, and
participants who were less overweight/obesecompared with high-dose aspirin. High-dose aspirintherapy was associated with a higher rate of docu-mented negative Helicobacter pylori infection (65.9%vs. 44.5%) compared with low-dose therapy.Low-dose aspirin users had higher rates of estab-lished peripheral artery disease, prior stroke, andhypertension, whereas high-dose aspirin users hadhigher rates of hyperlipidemia and a history of PCIwithin 14 days of randomization (91.3% vs. 61.6%).High-dose aspirin users were more than twice aslikely to be enrolled from sites within the UnitedStates compared with low-dose aspirin users (80.4%vs. 39.8%). There was no difference in history of GIbleeding or ulcer between the groups. Patients onhigh-dose aspirin during the study were more likelyto have been prescribed aspirin and clopidogrel(initiated within 21 days of randomization) beforestudy entry compared with patients on low-doseaspirin. High-dose aspirin users (median 115 days;IQR: 57 to 178 days) had longer follow-up durationscompared with low-dose aspirin users (median67 days; IQR: 52 to 126 days).GASTROINTESTINAL ENDPOINTS. Overall, medianduration of follow-up was 110 days (IQR: 55 to 167) for

Vaduganathan et al. J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6
PPIs and Aspirin Dose in COGENT A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1
1666
the entire analytic cohort. PPI use reduced rates ofthe primary GI endpoint in the low-dose (1.2% vs.3.1%; p ¼ 0.003) and high-dose aspirin subsets (0.9%vs. 2.6%; p ¼ 0.05) (Table 2). The corresponding NNTestimated to prevent 1 major composite upper GIevent with 6 months of PPI therapy was 52 in thelow-dose aspirin subset and 58 in the high-doseaspirin subset. Aspirin dosing did not appear tomodify the benefit of PPI therapy in reducing rates ofthe primary GI endpoint (interaction p ¼ 0.80).Kaplan-Meier analyses further demonstrated theconsistency of PPI benefit in reducing cumulativeincidence of GI events in low- and high-dose aspirinsubsets (Central Illustration). PPI use consistentlyreduced each of the components of the primary GIendpoint numerically in both aspirin dosing groups(interaction p range 0.67 to 0.99). Similarly, rates ofthe secondary GI endpoint were reduced by PPIs inthe low-dose (0.7% vs. 1.3%; p ¼ 0.10) and high-dose(0.2% vs. 1.6%; p ¼ 0.02; interaction p ¼ 0.33) aspiringroups. Investigator-defined GI events were alsoconsistently reduced by PPIs in both low-dose (2.6%vs. 5.2%; p ¼ 0.01) and high-dose (3.5% vs. 5.3%;p ¼ 0.13; interaction p ¼ 0.55) aspirin groups. At 4weeks, PPI therapy significantly reduced mean SODAscores for dyspepsia pain intensity in both aspirinsubsets (interaction p ¼ 0.13). Trends favoring PPIbenefit on pain-related SODA scores persisted at24 weeks, but these differences were not statisticallysignificant (Table 2).
CARDIOVASCULAR ENDPOINTS. PPI therapy did notsignificantly increase the primary cardiovascularendpoint in low-dose (5.6% vs. 5.5%; p ¼ 0.95) orhigh-dose (4.2%vs. 5.5%; p¼0.92; interaction p¼0.91)aspirin groups. Kaplan-Meier incidence curvesfor the primary cardiovascular endpoint by PPItreatment randomization are presented in Figure 2.Similarly, PPIs did not influence investigator-definedcardiovascular events in both aspirin dose subsets(interaction p ¼ 1.00). Rates of non-GI bleedingand all-cause mortality were low and were not in-fluenced by PPI therapy in either aspirin dosingsubset (Table 2).
EVENT RATES BY ASPIRIN DOSING. High-doseaspirin was associated with similar risks of adjudi-cated composite upper GI events (1.7% vs. 2.1%),GERD (0.9% vs. 1.0%), and MACE (4.8% vs. 5.5%)compared with low-dose aspirin at 180 days (Table 3).After accounting for baseline risk profiles, high-doseaspirin did not influence risk of adjudicated com-posite upper GI events (adjusted HR: 0.88; 95% CI:0.46 to 1.66), GERD (adjusted HR: 0.71; 95% CI: 0.28
to 1.77), or MACE (adjusted HR: 0.73; 95% CI: 0.48 to1.11) compared with low-dose aspirin (Table 3).
INDEPENDENT PREDICTORS OF ADJUDICATED
PRIMARY GASTROINTESTINAL EVENTS. Age remainedthe only significant independent predictor of adjudi-cated composite upper GI events in the final multi-variate model (adjusted HR: 1.03 per year; 95% CI:1.00 to 1.06), whereas randomization to omeprazole(vs. placebo) was independently associated withlower risk of the composite primary GI endpoint(adjusted HR: 0.33; 95% CI: 0.18 to 0.62).
DISCUSSION
In the context of a large, randomized clinical trialof PPI therapy in patients with CAD on DAPT, aspirindosing #100 mg was utilized in two-thirds of patientsand was associated with similar risks of GI eventsas higher-dose aspirin. Prophylactic PPI therapyconsistently reduced rates of adjudicated GI events at180 days and patient-reported symptoms, even withlow-dose aspirin therapy. In the COGENT, the NNTestimated to prevent 1 major composite upperGI event with 6 months of PPI therapy was 52 and58 in the low-dose and high-dose aspirin subsets,respectively.
COGENT represented an ideal setting to examineoptimal gastroprotection approaches by aspirin dosinggiven that the trial: 1) represented the only large,randomized placebo-controlled experience exam-ining PPI use in this setting; 2) included robustglobal participation, potentially capturing regionalvariation in aspirin dosing (5,14); and 3) specificallyadjudicated GI and cardiovascular events. The con-sistency of PPI benefit across aspirin doses maybe related to its potent effects on gastric acidsuppression.
VARIATION IN ASPIRIN DOSING PRACTICES. Aspirinis widely prescribed for secondary prevention of car-diovascular events in patients with CAD. Substantialregional and practice-based variations exist regardingaspirin dosing regimens (14). Despite recent shiftstowards utilizing lower-dose aspirin therapy,higher-dose aspirin is still used in more than 60% of“real-world” patients discharged after acute myocar-dial infarction in theUnited States (15), and it continuesto be supported by guideline committees for selecthigh-risk settings. Even in well-selected patients inthis contemporary trial, one-third of CADpatients usedhigh maintenance aspirin doses. Data regarding the GIrisks associated with varying aspirin doses are limited(16), and meta-analyses have been contradictory(17,18). High maintenance aspirin doses ($300 mg)
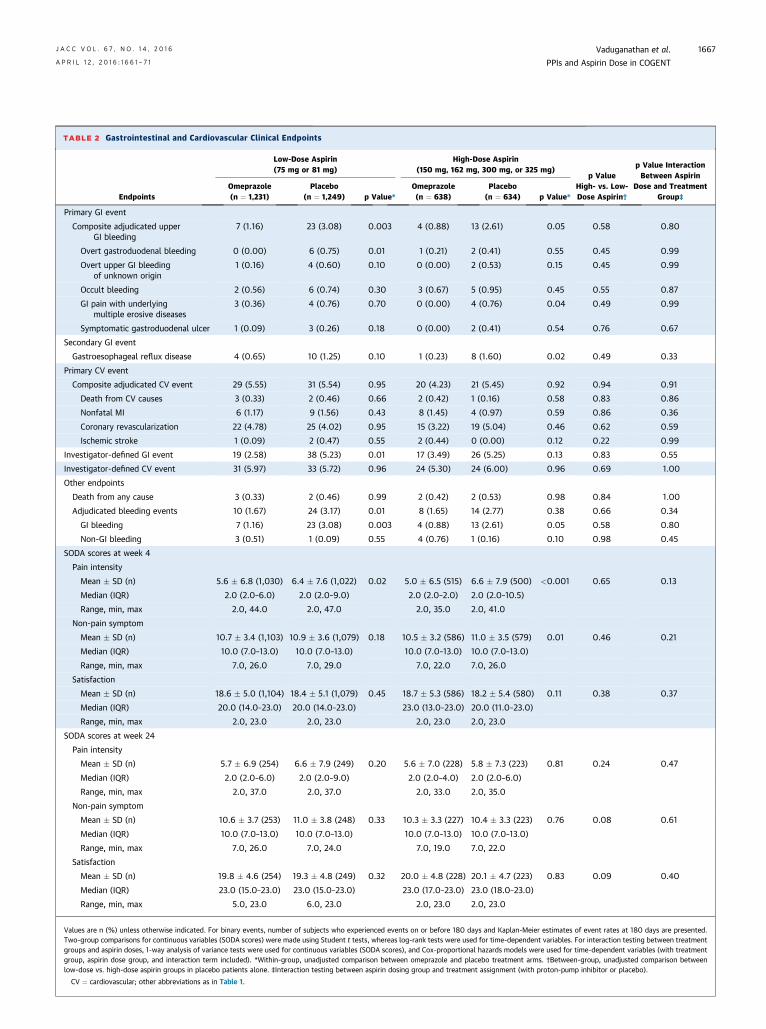
TABLE 2 Gastrointestinal and Cardiovascular Clinical Endpoints
Endpoints
Low-Dose Aspirin(75 mg or 81 mg)
High-Dose Aspirin(150 mg, 162 mg, 300 mg, or 325 mg)
p ValueHigh- vs. Low-Dose Aspirin†
p Value InteractionBetween Aspirin
Dose and TreatmentGroup‡
Omeprazole(n ¼ 1,231)
Placebo(n ¼ 1,249) p Value*
Omeprazole(n ¼ 638)
Placebo(n ¼ 634) p Value*
Primary GI event
Composite adjudicated upperGI bleeding
7 (1.16) 23 (3.08) 0.003 4 (0.88) 13 (2.61) 0.05 0.58 0.80
Overt gastroduodenal bleeding 0 (0.00) 6 (0.75) 0.01 1 (0.21) 2 (0.41) 0.55 0.45 0.99
Overt upper GI bleedingof unknown origin
1 (0.16) 4 (0.60) 0.10 0 (0.00) 2 (0.53) 0.15 0.45 0.99
Occult bleeding 2 (0.56) 6 (0.74) 0.30 3 (0.67) 5 (0.95) 0.45 0.55 0.87
GI pain with underlyingmultiple erosive diseases
3 (0.36) 4 (0.76) 0.70 0 (0.00) 4 (0.76) 0.04 0.49 0.99
Symptomatic gastroduodenal ulcer 1 (0.09) 3 (0.26) 0.18 0 (0.00) 2 (0.41) 0.54 0.76 0.67
Secondary GI event
Gastroesophageal reflux disease 4 (0.65) 10 (1.25) 0.10 1 (0.23) 8 (1.60) 0.02 0.49 0.33
Primary CV event
Composite adjudicated CV event 29 (5.55) 31 (5.54) 0.95 20 (4.23) 21 (5.45) 0.92 0.94 0.91
Death from CV causes 3 (0.33) 2 (0.46) 0.66 2 (0.42) 1 (0.16) 0.58 0.83 0.86
Nonfatal MI 6 (1.17) 9 (1.56) 0.43 8 (1.45) 4 (0.97) 0.59 0.86 0.36
Coronary revascularization 22 (4.78) 25 (4.02) 0.95 15 (3.22) 19 (5.04) 0.46 0.62 0.59
Ischemic stroke 1 (0.09) 2 (0.47) 0.55 2 (0.44) 0 (0.00) 0.12 0.22 0.99
Investigator-defined GI event 19 (2.58) 38 (5.23) 0.01 17 (3.49) 26 (5.25) 0.13 0.83 0.55
Investigator-defined CV event 31 (5.97) 33 (5.72) 0.96 24 (5.30) 24 (6.00) 0.96 0.69 1.00
Other endpoints
Death from any cause 3 (0.33) 2 (0.46) 0.99 2 (0.42) 2 (0.53) 0.98 0.84 1.00
Adjudicated bleeding events 10 (1.67) 24 (3.17) 0.01 8 (1.65) 14 (2.77) 0.38 0.66 0.34
GI bleeding 7 (1.16) 23 (3.08) 0.003 4 (0.88) 13 (2.61) 0.05 0.58 0.80
Non-GI bleeding 3 (0.51) 1 (0.09) 0.55 4 (0.76) 1 (0.16) 0.10 0.98 0.45
SODA scores at week 4
Pain intensity
Mean � SD (n) 5.6 � 6.8 (1,030) 6.4 � 7.6 (1,022) 0.02 5.0 � 6.5 (515) 6.6 � 7.9 (500) <0.001 0.65 0.13
Median (IQR) 2.0 (2.0–6.0) 2.0 (2.0–9.0) 2.0 (2.0–2.0) 2.0 (2.0–10.5)
Range, min, max 2.0, 44.0 2.0, 47.0 2.0, 35.0 2.0, 41.0
Non-pain symptom
Mean � SD (n) 10.7 � 3.4 (1,103) 10.9 � 3.6 (1,079) 0.18 10.5 � 3.2 (586) 11.0 � 3.5 (579) 0.01 0.46 0.21
Median (IQR) 10.0 (7.0–13.0) 10.0 (7.0–13.0) 10.0 (7.0–13.0) 10.0 (7.0–13.0)
Range, min, max 7.0, 26.0 7.0, 29.0 7.0, 22.0 7.0, 26.0
Satisfaction
Mean � SD (n) 18.6 � 5.0 (1,104) 18.4 � 5.1 (1,079) 0.45 18.7 � 5.3 (586) 18.2 � 5.4 (580) 0.11 0.38 0.37
Median (IQR) 20.0 (14.0–23.0) 20.0 (14.0–23.0) 23.0 (13.0–23.0) 20.0 (11.0–23.0)
Range, min, max 2.0, 23.0 2.0, 23.0 2.0, 23.0 2.0, 23.0
SODA scores at week 24
Pain intensity
Mean � SD (n) 5.7 � 6.9 (254) 6.6 � 7.9 (249) 0.20 5.6 � 7.0 (228) 5.8 � 7.3 (223) 0.81 0.24 0.47
Median (IQR) 2.0 (2.0–6.0) 2.0 (2.0–9.0) 2.0 (2.0–4.0) 2.0 (2.0–6.0)
Range, min, max 2.0, 37.0 2.0, 37.0 2.0, 33.0 2.0, 35.0
Non-pain symptom
Mean � SD (n) 10.6 � 3.7 (253) 11.0 � 3.8 (248) 0.33 10.3 � 3.3 (227) 10.4 � 3.3 (223) 0.76 0.08 0.61
Median (IQR) 10.0 (7.0–13.0) 10.0 (7.0–13.0) 10.0 (7.0–13.0) 10.0 (7.0–13.0)
Range, min, max 7.0, 26.0 7.0, 24.0 7.0, 19.0 7.0, 22.0
Satisfaction
Mean � SD (n) 19.8 � 4.6 (254) 19.3 � 4.8 (249) 0.32 20.0 � 4.8 (228) 20.1 � 4.7 (223) 0.83 0.09 0.40
Median (IQR) 23.0 (15.0–23.0) 23.0 (15.0–23.0) 23.0 (17.0–23.0) 23.0 (18.0–23.0)
Range, min, max 5.0, 23.0 6.0, 23.0 2.0, 23.0 2.0, 23.0
Values are n (%) unless otherwise indicated. For binary events, number of subjects who experienced events on or before 180 days and Kaplan-Meier estimates of event rates at 180 days are presented.Two-group comparisons for continuous variables (SODA scores) were made using Student t tests, whereas log-rank tests were used for time-dependent variables. For interaction testing between treatmentgroups and aspirin doses, 1-way analysis of variance tests were used for continuous variables (SODA scores), and Cox-proportional hazards models were used for time-dependent variables (with treatmentgroup, aspirin dose group, and interaction term included). *Within-group, unadjusted comparison between omeprazole and placebo treatment arms. †Between-group, unadjusted comparison betweenlow-dose vs. high-dose aspirin groups in placebo patients alone. ‡Interaction testing between aspirin dosing group and treatment assignment (with proton-pump inhibitor or placebo).
CV ¼ cardiovascular; other abbreviations as in Table 1.
J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6 Vaduganathan et al.A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1 PPIs and Aspirin Dose in COGENT
1667
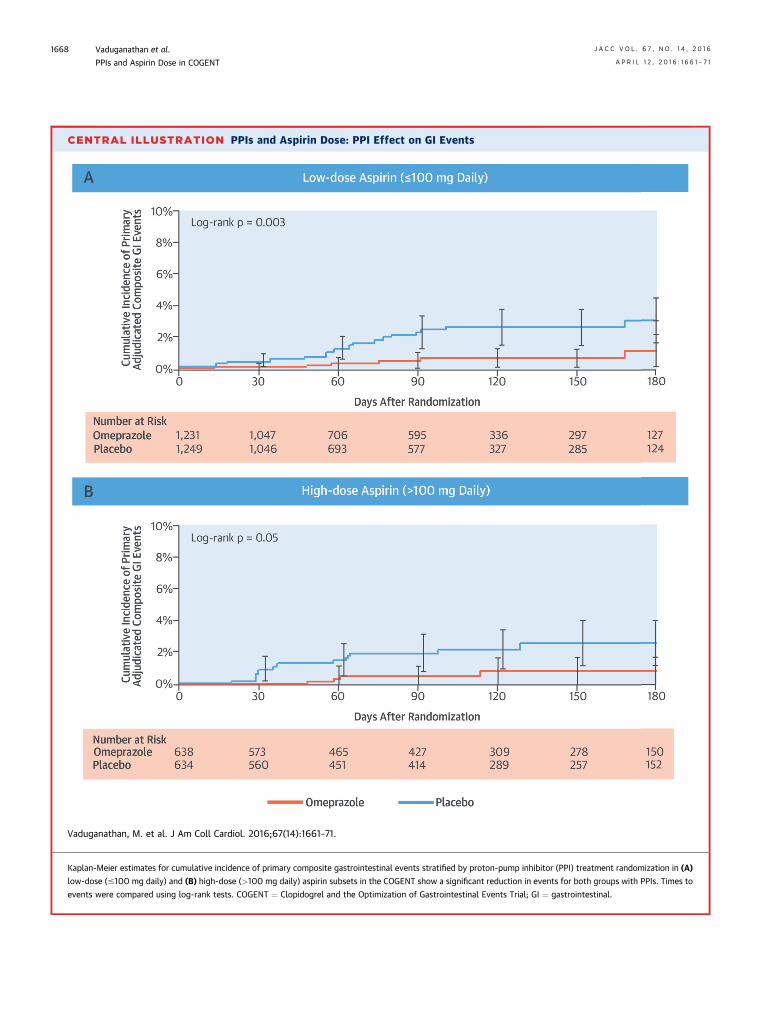
CENTRAL ILLUSTRATION PPIs and Aspirin Dose: PPI Effect on GI Events
A
B
Vaduganathan, M. et al. J Am Coll Cardiol. 2016;67(14):1661–71.
Kaplan-Meier estimates for cumulative incidence of primary composite gastrointestinal events stratified by proton-pump inhibitor (PPI) treatment randomization in (A)
low-dose (#100 mg daily) and (B) high-dose (>100 mg daily) aspirin subsets in the COGENT show a significant reduction in events for both groups with PPIs. Times to
events were compared using log-rank tests. COGENT ¼ Clopidogrel and the Optimization of Gastrointestinal Events Trial; GI ¼ gastrointestinal.
Vaduganathan et al. J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6
PPIs and Aspirin Dose in COGENT A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1
1668
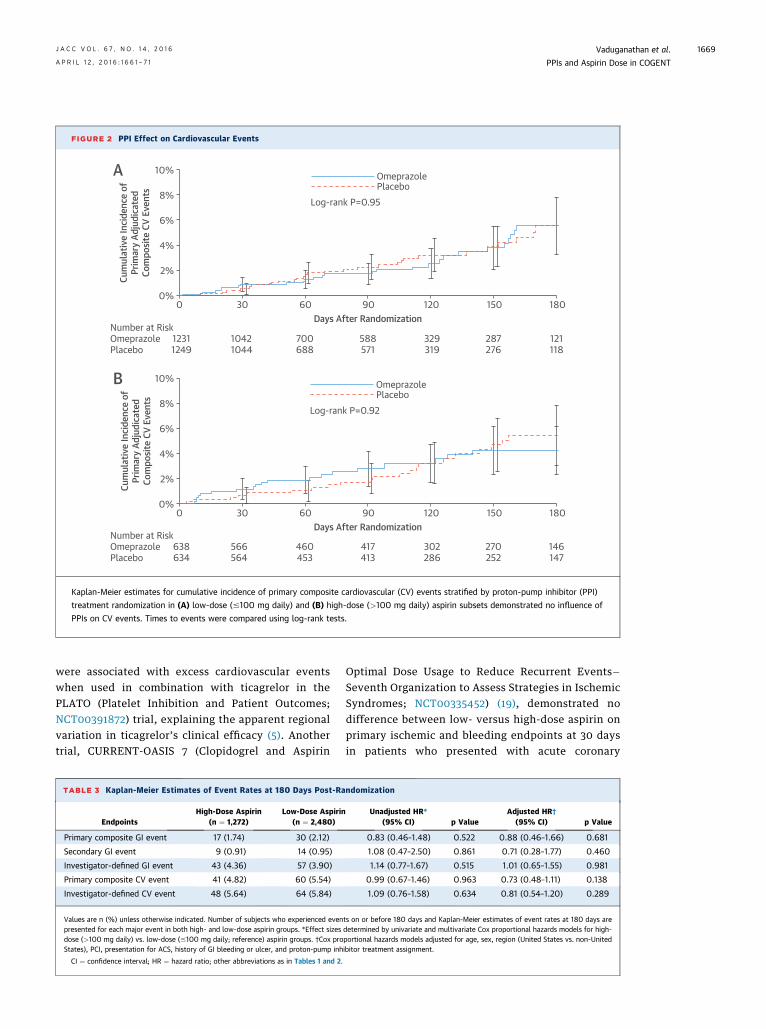
FIGURE 2 PPI Effect on Cardiovascular Events
10%
8%
6%
4%
2%
0%0 30 60 90 120 150 180
Days After Randomization
Cum
ulat
ive
Inci
denc
e of
Prim
ary
Adju
dica
ted
Com
posit
e CV
Eve
nts
10%
8%
6%
4%
2%
0%0 30 60 90 120 150 180
Days After Randomization
Cum
ulat
ive
Inci
denc
e of
Prim
ary
Adju
dica
ted
Com
posit
e CV
Eve
nts
OmeprazolePlacebo
Log-rank P=0.95
OmeprazolePlacebo
Log-rank P=0.92
Number at RiskOmeprazolePlacebo
12311249
10421044
700688
588571
329319
287276
121118
Number at RiskOmeprazolePlacebo
638634
566564
460453
417413
302286
270252
146147
A
B
Kaplan-Meier estimates for cumulative incidence of primary composite cardiovascular (CV) events stratified by proton-pump inhibitor (PPI)
treatment randomization in (A) low-dose (#100 mg daily) and (B) high-dose (>100 mg daily) aspirin subsets demonstrated no influence of
PPIs on CV events. Times to events were compared using log-rank tests.
J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6 Vaduganathan et al.A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1 PPIs and Aspirin Dose in COGENT
1669
were associated with excess cardiovascular eventswhen used in combination with ticagrelor in thePLATO (Platelet Inhibition and Patient Outcomes;NCT00391872) trial, explaining the apparent regionalvariation in ticagrelor’s clinical efficacy (5). Anothertrial, CURRENT-OASIS 7 (Clopidogrel and Aspirin
TABLE 3 Kaplan-Meier Estimates of Event Rates at 180 Days Post-Ra
EndpointsHigh-Dose Aspirin
(n ¼ 1,272)Low-Dose Aspirin
(n ¼ 2,480)
Primary composite GI event 17 (1.74) 30 (2.12)
Secondary GI event 9 (0.91) 14 (0.95)
Investigator-defined GI event 43 (4.36) 57 (3.90)
Primary composite CV event 41 (4.82) 60 (5.54)
Investigator-defined CV event 48 (5.64) 64 (5.84)
Values are n (%) unless otherwise indicated. Number of subjects who experienced evenpresented for each major event in both high- and low-dose aspirin groups. *Effect sizesdose (>100 mg daily) vs. low-dose (#100 mg daily; reference) aspirin groups. †Cox proStates), PCI, presentation for ACS, history of GI bleeding or ulcer, and proton-pump inh
CI ¼ confidence interval; HR ¼ hazard ratio; other abbreviations as in Tables 1 and 2.
Optimal Dose Usage to Reduce Recurrent Events�Seventh Organization to Assess Strategies in IschemicSyndromes; NCT00335452) (19), demonstrated nodifference between low- versus high-dose aspirin onprimary ischemic and bleeding endpoints at 30 daysin patients who presented with acute coronary
ndomization
Unadjusted HR*(95% CI) p Value
Adjusted HR†(95% CI) p Value
0.83 (0.46–1.48) 0.522 0.88 (0.46–1.66) 0.681
1.08 (0.47–2.50) 0.861 0.71 (0.28–1.77) 0.460
1.14 (0.77–1.67) 0.515 1.01 (0.65–1.55) 0.981
0.99 (0.67–1.46) 0.963 0.73 (0.48–1.11) 0.138
1.09 (0.76–1.58) 0.634 0.81 (0.54–1.20) 0.289
ts on or before 180 days and Kaplan-Meier estimates of event rates at 180 days aredetermined by univariate and multivariate Cox proportional hazards models for high-portional hazards models adjusted for age, sex, region (United States vs. non-Unitedibitor treatment assignment.

PERSPECTIVES
COMPETENCY IN PATIENT CARE AND
PROCEDURAL SKILLS: Gastrointestinal toxicity is
common in patients treated with DAPT even when low
doses of aspirin are utilized, and prophylactic adminis-
tration of a PPI is effective regardless of aspirin dosing.
TRANSLATIONAL OUTLOOK: Further investigation
is needed to evaluate the risks of gastrointestinal
bleeding and effectiveness of protective strategies
using newer combinations and longer durations
of DAPT.
Vaduganathan et al. J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6
PPIs and Aspirin Dose in COGENT A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1
1670
syndromes referred for an invasive strategy, thoughthere was a lower rate of GI bleeding with low-doseaspirin. Our study demonstrated that risk-adjustedGI and cardiovascular events were similar in subsetsof CAD patients prescribed varying aspirin doses.We eagerly await comparative effectiveness data fromtheADAPTABLE trial (AspirinDosing: A Patient-centricTrial AssessingBenefits andLong-TermEffectiveness),which will compare low- versus high-dose aspirinstrategies in patients with CAD (20).PPI EFFICACYWITH LOW-DOSEASPIRIN. Using low-doseaspirin appears to provide effective antiplatelet pro-tection, but still confers a substantial risk of GIbleeding. These randomized data support the role ofprophylactic use of PPIs to attenuate this excess riskwithout heterogeneity by aspirin dosing in patientsrequiring DAPT. Consistently, prior small trials havedemonstrated efficacy of PPIs with low-dose aspirinin secondary prevention of GI bleeding in otherhigh-risk cohorts, such as patients with a prior historyof GI ulcers (21,22). Despite this, PPI use appears tobe underutilized for prevention of GI events (11),perhaps related to underestimated clinician estimatesof GI risks related to low-dose aspirin. ProphylacticPPI therapy is a data-driven, expert-recommended(6,23), and cost-effective approach to gastroprotection(24) in appropriately selected patients (25–27), eventhose on low-dose aspirin. Enteric-coated aspirin wasprotocol-specified in COGENT, but these preparationsmay be associated with variable drug absorption(28) and antiplatelet effects (29), without significantlyattenuating attendant GI bleeding risks (30), com-pared with standard dispersible aspirin. Definitivecardiovascular outcome data are lacking regardingthe use of enteric-coated versus immediate-releasepreparations of aspirin in patients with CAD.Enteric-coating may decrease dyspepsia and, as such,may have led to some underestimation of omepra-zole’s potential benefits in reducing dyspepsia in thistrial. New formulations of aspirin may limit GI toxicity(31,32), but further data are required. Ongoing inves-tigation is needed to evaluate the differential GIbleeding risks and effective gastroprotection strate-gies with newer combinations and longer durationsof DAPT (33).
STUDY LIMITATIONS. There are several limitations tothis post hoc analysis. The overall trial was notpowered to detect differences in safety and efficacy of
PPI therapy by aspirin dosing. Comparisons of clinicaloutcomes between different aspirin dosing regimenswere nonrandomized and thus may be subject to re-sidual confounding by indication. The point esti-mates for GI and cardiovascular risks by aspirindosing should be interpreted with caution, given thewide CIs. No statistical adjustments were made formultiple comparisons. We used baseline aspirin doseat the time of enrollment in our models; however,aspirin dosing did not appear to change substantiallyduring follow-up. The specific preparation of theclopidogrel–PPI combination used in the COGENTis not commercially available, though that is unlikelyto affect the study findings. Although the originaltrial was prematurely terminated due to loss offunding, it met its initial target sample size, withrobust follow-up available in the high-risk periodpost-randomization. More potent P2Y12 inhibitors,such as prasugrel and ticagrelor, were not widelyused in this trial.
CONCLUSIONS
These data from COGENT suggest that gastro-protection with PPI therapy should be utilized inappropriately selected patients with CAD requiringDAPT, even if on low-dose aspirin.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Deepak L. Bhatt, Brigham and Women’s Hospital Heart &Vascular Center, 75 Francis Street, Boston, Massachu-setts 02115. E-mail: [email protected].
RE F E RENCE S
1. Eikelboom JW, Hirsh J, Spencer FA, et al.Antiplatelet drugs: Antithrombotic Therapy andPrevention of Thrombosis, 9th ed: American
College of Chest Physicians Evidence-BasedClinical Practice Guidelines. Chest 2012;141:e89S–119S.
2. Peters RJ, Mehta SR, Fox KA, et al. Effectsof aspirin dose when used alone or in combi-nation with clopidogrel in patients with acute

J A C C V O L . 6 7 , N O . 1 4 , 2 0 1 6 Vaduganathan et al.A P R I L 1 2 , 2 0 1 6 : 1 6 6 1 – 7 1 PPIs and Aspirin Dose in COGENT
1671
coronary syndromes: observations from theClopidogrel in Unstable angina to preventRecurrent Events (CURE) study. Circulation2003;108:1682–7.
3. Steinhubl SR, Bhatt DL, Brennan DM, et al.Aspirin to prevent cardiovascular disease: the as-sociation of aspirin dose and clopidogrel withthrombosis and bleeding. Ann Intern Med 2009;150:379–86.
4. Smith SC Jr., Benjamin EJ, BonowRO, et al. AHA/ACCF secondary prevention and risk reductiontherapy for patients with coronary and otheratherosclerotic vascular disease: 2011 update: aguideline from the American Heart Association andAmerican College of Cardiology Foundationendorsed by the World Heart Federation and thePreventive Cardiovascular Nurses Association. J AmColl Cardiol 2011;58:2432–46.
5. Mahaffey KW, Wojdyla DM, Carroll K, et al.Ticagrelor compared with clopidogrel bygeographic region in the Platelet Inhibition andPatient Outcomes (PLATO) trial. Circulation 2011;124:544–54.
6. Bhatt DL, Scheiman J, Abraham NS, et al. ACCF/ACG/AHA 2008 expert consensus document onreducing the gastrointestinal risks of antiplatelettherapy and NSAID use: a report of the AmericanCollege of Cardiology Foundation Task Force onClinical Expert Consensus Documents. J Am CollCardiol 2008;52:1502–17.
7. Moukarbel GV, Signorovitch JE, Pfeffer MA,et al. Gastrointestinal bleeding in high risk survi-vors of myocardial infarction: the VALIANT trial.Eur Heart J 2009;30:2226–32.
8. Martin Merino E, Johansson S, Nagy P, GarcíaRodríguez LA. Effect of baseline gastrointestinalrisk and use of proton pump inhibitors on fre-quency of discontinuation of aspirin for secondarycardiovascular prevention in United Kingdom pri-mary care. Am J Cardiol 2013;112:1075–82.
9. Bhatt DL, Cryer BL, Contant CF, et al. Clopi-dogrel with or without omeprazole in coronaryartery disease. N Engl J Med 2010;363:1909–17.
10. Vardi M, Cryer BL, Cohen M, et al. The effectsof proton pump inhibition on patient-reportedseverity of dyspepsia when receiving dual anti-platelet therapy with clopidogrel and low-doseaspirin: analysis from the Clopidogrel and theOptimization of Gastrointestinal Events Trial.Aliment Pharmacol Ther 2015;42:365–74.
11. de Jong HJ, Korevaar JC, van Dijk L, et al.Suboptimal prescribing of proton-pump inhibitorsin low-dose aspirin users: a cohort study in primarycare. BMJ Open 2013;3.
12. Rabeneck L, Wristers K, Goldstein JL, et al.Reliability, validity, and responsiveness of severityof dyspepsia assessment (SODA) in a randomizedclinical trial of a COX-2-specific inhibitor andtraditional NSAID therapy. Am J Gastroenterol2002;97:32–9.
13. Rabeneck L, Cook KF, Wristers K, et al. SODA(severity of dyspepsia assessment): a new effec-tive outcome measure for dyspepsia-relatedhealth. J Clin Epidemiol 2001;54:755–65.
14. Cannon CP, Rhee KE, Califf RM, et al. Currentuse of aspirin and antithrombotic agents in theUnited States among outpatients with athero-thrombotic disease (from the REduction of Athe-rothrombosis for Continued Health [REACH]Registry). Am J Cardiol 2010;105:445–52.
15. Hall HM, de Lemos JA, Enriquez JR, et al.Contemporary patterns of discharge aspirin dosingafter acute myocardial infarction in the UnitedStates: results from the National CardiovascularData Registry (NCDR). Circ Cardiovasc Qual Out-comes 2014;7:701–7.
16. McQuaid KR, Laine L. Systematic review andmeta-analysis of adverse events of low-doseaspirin and clopidogrel in randomized controlledtrials. Am J Med 2006;119:624–38.
17. Derry S, Loke YK. Risk of gastrointestinalhaemorrhage with long term use of aspirin: meta-analysis. BMJ 2000;321:1183–7.
18. Laine L, McQuaid K. Bleeding complicationsrelated to aspirin dose. Am J Cardiol 2005;96:1035–6.
19. Mehta SR, Bassand JP, Chrolavicius S, et al.Dose comparisons of clopidogrel and aspirin inacute coronary syndromes. N Engl J Med 2010;363:930–42.
20. Hernandez AF, Fleurence RL, Rothman RL.The ADAPTABLE trial and PCORnet: shining lighton a new research paradigm. Ann Intern Med 2015;163:635–6.
21. Chan FK, Ching JY, Hung LC, et al. Clopidogrelversus aspirin and esomeprazole to prevent recur-rent ulcer bleeding. N Engl JMed 2005;352:238–44.
22. Lai KC, Lam SK, Chu KM, et al. Lansoprazolefor the prevention of recurrences of ulcer com-plications from long-term low-dose aspirin use.N Engl J Med 2002;346:2033–8.
23. Abraham NS, Hlatky MA, Antman EM, et al.ACCF/ACG/AHA 2010 expert consensus documenton the concomitant use of proton pump inhibitorsand thienopyridines: a focused update of theACCF/ACG/AHA 2008 expert consensus documenton reducing the gastrointestinal risks of anti-platelet therapy and NSAID use: a report of theAmerican College of Cardiology Foundation Task
Force on Expert Consensus Documents. J Am CollCardiol 2010;56:2051–66.
24. Saini SD, Schoenfeld P, Fendrick AM,Scheiman J. Cost-effectiveness of proton pumpinhibitor cotherapy in patients taking long-term,low-dose aspirin for secondary cardiovascularprevention. Arch Intern Med 2008;168:1684–90;discussion 1691.
25. Depta JP, Bhatt DL. Omeprazole and clopi-dogrel: should clinicians be worried? Cleve Clin JMed 2010;77:113–6.
26. Moukarbel GV, Bhatt DL. Antiplatelet therapyand proton pump inhibition: clinician update. Cir-culation 2012;125:375–80.
27. Banerjee S, Weideman RA, Weideman MW,et al. Effect of concomitant use of clopidogrel andproton pump inhibitors after percutaneous coro-nary intervention. Am J Cardiol 2011;107:871–8.
28. Grosser T, Fries S, Lawson JA, et al. Drugresistance and pseudoresistance: an unintendedconsequence of enteric coating aspirin. Circulation2013;127:377–85.
29. Cox D, Maree AO, Dooley M, et al. Effect ofenteric coating on antiplatelet activity of low-doseaspirin in healthy volunteers. Stroke 2006;37:2153–8.
30. Kelly JP, Kaufman DW, Jurgelon JM, et al. Riskof aspirin-associated major upper-gastrointestinalbleeding with enteric-coated or buffered product.Lancet 1996;348:1413–6.
31. Cryer B, Bhatt DL, Lanza FL, et al. Low-doseaspirin-induced ulceration is attenuated byaspirin-phosphatidylcholine: a randomized clinicaltrial. Am J Gastroenterol 2011;106:272–7.
32. Whellan DJ, Goldstein JL, Cryer BL, et al.PA32540 (a coordinated-delivery tablet of enteric-coated aspirin 325 mg and immediate-releaseomeprazole 40 mg) versus enteric-coated aspirin325mgalone in subjects at risk foraspirin-associatedgastric ulcers: results of two 6-month, phase 3studies. Am Heart J 2014;168:495–502, e494.
33. Vaduganathan M, Bhatt DL. Revisiting theclopidogrel-proton pump inhibitor interaction:from bench to bedside. Circ Cardiovasc Interv2015;8:e003208.
KEY WORDS bleeding, clinical outcomes,clinical trials, coronary artery disease
APPENDIX For a full list of investigators,please see the online version of this article.