protocol - university of york · protocol prepared by: ... a single retrospective non-randomized...
TRANSCRIPT

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of
convalescent plasma for the treatment of severe acute respiratory infections of viral
aetiology: a systematic review
A project commissioned by the World Health Organization Pandemic and Epidemic Disease
Department
PROTOCOL
Prepared by: John Mair-Jenkins, Maria Saavedra-Campos, Dr Charles Beck
Senior Supervisor: Professor Jonathan S. Nguyen-Van-Tam
Project leads: John Mair-Jenkins1 and Maria Saavedra-Campos2
1 Specialty Registrar in Public Health 2Field Epidemiology Training Fellow
Clinical Sciences Building Nottingham City Hospital Hucknall Road, Nottingham NG5 1PB, United Kingdom Email: [email protected]; [email protected]
Document date: 20 January 2014
Version: 3
Project funding: World Health Organization Pandemic and Epidemic Diseases
Department

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 2
Contents
1. Background ............................................................................................................................................... 3
2. Review questions .................................................................................................................................... 4
3. Study selection ......................................................................................................................................... 6
4. Assessment of risk of bias and data extraction .............................................................................. 7
5. Data synthesis .......................................................................................................................................... 8
6. Dissemination ........................................................................................................................................... 8
7. Resource implications ............................................................................................................................ 8
8. Acknowledgments .................................................................................................................................. 8
9. References................................................................................................................................................. 9
10. Appendix 1 – search strategy ....................................................................................................... 11
11. Appendix 2 – data extraction form............................................................................................. 24

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 3
1. Background In September 2012 a novel human coronavirus was identified in two patients with severe respiratory disease in Saudi Arabia and the Middle East. The virus was later named Middle East Respiratory Syndrome coronavirus (MERS-CoV). As of 26 June 2013, the World Health Organization (WHO) has been informed of 77 laboratory-confirmed cases of MERS-CoV, 40 of whom died due to the infection. Laboratory-confirmed cases have predominately been identified in Jordan, Qatar, Saudi Arabia, and the United Arab Emirates. A small number of additional cases have so far been described in France, Germany, Italy, Tunisia and the United Kingdom. In these situations the index case was connected to the Middle East through travel or they were transferred outside of the Middle East for ongoing intensive care clinical management (1). Currently there is evidence of limited, non-sustained person-to-person transmission although potential exposures to a common source may also play a part. Transmission has been reported between close contacts and within family clusters in the Middle East. There has also been reports of nosocomial transmission in healthcare facilities from patient to patient and from patients to health care workers (1). In Europe and Northern Africa the known index cases have all had direct connections with the Middle East. Limited local transmission has been documented between close family contacts and nosocomial transmission has also been reported between patients (1). The current cases suggest that person-to-person transmission of MERS-CoV requires close contact, and that the virus may not be as readily transmissible or likely to develop epidemic potential as a fully adapted respiratory virus (2). However, this needs to be interpreted with caution as uncertainty remains about the behavior and epidemiology of the virus. For example, the full extent of geographical spread is not known and it is possible that only severe cases have been identified to date (3). The clinical presentation of MERS-CoV may include fever, cough, shortness of breath and myalgia although current working knowledge is limited and based on a small number of cases (4–6). A recent case identified in France with an initial presentation including diarrhoea, raising the possibility of non-respiratory symptoms, especially in the immunocompromised or those with underlying medical conditions (7). Most of the cases of MERS-CoV progressed to severe acute respiratory disease with some also developing an acute kidney injury, although it is unclear if this is a typical picture. Milder illness associated with MERS-CoV has also been identified (8). Despite admission to intensive care units and the use of resource intensive measures (such as mechanical ventilation and extracorporeal membrane oxygenation [ECMO] ) the case fatality rate across all cases is estimated at 59% (4,7). MERS-CoV shares virological and epidemiological characteristics with severe acute respiratory syndrome (SARS). This has raised concerns about the potential public health impact if wider community transmission occurs (3) especially when linked with international mass gatherings, such as the annual Hajj Pilgrimage that takes place annually in the Middle East which is attended by over three million people and therefore offers the propensity for wide geographical spread (9). The SARS outbreak caused over 8,000 probable or confirmed cases and 774 deaths, in 26 countries in five continents. The overall mortality rate during the outbreak was estimated at 9.6%. Of greater concern is that in 2003 SARS spread from Hong Kong to Vietnam, Singapore and Canada in a number of weeks, illustrating the potential for modern day air passenger movement to substantially accelerate international spread of a novel respiratory infection (10). Unfortunately no vaccine or specific treatment is available for MERS-CoV, nor is there any prospect of either in the foreseeable future. Interim guidance for the clinical management of severe acute respiratory infections (SARI) when novel coronavirus is suspected, have been produced by WHO (11). These guidelines recommend the use of supplemental oxygen therapy, empirical antimicrobials and

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 4
conservative fluid management for patients presenting with SARI. The guidelines advise against the use of corticosteroids or other adjunctive therapies for viral pneumonitis unless they are indicated for another reason (e.g. underlying asthma). Close monitoring of patients for signs of clinical deterioration is recommended in order to apply supportive care interventions as early as possible. Public Health England and the International Severe Acute Respiratory & Emerging Infection Consortium have recently published a decision support tool for clinicians managing cases of MERS-CoV (12). This document includes a summary review of current treatments for MERS-CoV, predominately based on expert advice and clinical experience of treating patients with severe respiratory disease caused by other viruses including SARS and 2009 pandemic influenza A(H1N1). The authors report that current evidence is strongest for convalescent plasma or other therapeutics which contain neutralising antibodies (such as hyperimmune immunoglobulin) where a probable clinical effect exists for treatment of MERS-CoV. Due to uncertainties regarding the viral replication kinetics of MERS-CoV, the authors suggest that convalescent plasma may be considered for patients who are deteriorating (despite other specific and supportive therapy) and in whom the virus remains detectable (12). Convalescent plasma has previously been used for the treatment of novel viruses such as ‘Spanish influenza’ (1918-19 pandemic), 2009 influenza pandemic (A(H1N1)pdm09), avian influenza (A(H5N1))and SARS (13–16). In a meta-analysis performed on literature from 1918-19 pandemic influenza the analysis suggested that patients who presented with pneumonia and who received a transfusion with influenza convalescent human blood products may have experienced an important reduction in the risk of death and improvement in their clinical condition (14). More recent studies on the use of convalescent plasma in patients with severe A(H1N1)pdm09 infection including a randomised control trial suggested that treatment with convalescent plasma may have reduced respiratory tract viral load, serum cytokine response and mortality (13,17). A review of the treatment of SARS suggested that patients with SARS who continue to deteriorate and were treated with convalescent plasma had a shorter hospital stay and lower mortality (18). However, this was based on a single retrospective non-randomized study where the comparator group was formed from SARS cases treated with methylprednisolone. A further systematic review found that the studies identified were inconclusive, as the effect of convalescent plasma or intravenous immunoglobulin could not be differentiated from the effect of patient comorbidities or other treatments (19). In a number of case studies regarding SARS treatments, the authors commented that patients with severe presentation seemed to improve after treatment with convalescent plasma (20,21). The current evidence base for use of convalescent plasma for respiratory viruses is therefore inconclusive and comes from different periods with varying size and quality of studies. This highlights the need for a systematic review of the literature and meta-analysis of available data, which has not so far been performed, to help inform management of MERS-CoV cases. The systematic review will be conducted according to the requirements of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (22). This protocol will be registered and made available through the International Prospective Register of Systematic Reviews (PROSPERO, http://www.crd.york.ac.uk/Prospero/).
2. Review questions The aim of this review is to evaluate the clinical effectiveness of convalescent plasma, convalescent serum and hyperimmune immunoglobulin for the treatment of SARI cases with a viral aetiology, to help inform the evidence base for MERS-CoV treatment. This will be achieved by addressing the following questions:

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 5
1. What is the effect of treating SARI cases of viral aetiology with convalescent plasma, serum or
hyperimmune immunoglobulin on the all-cause case-fatality rate? 2. What is the effect of treating SARI cases of viral aetiology with convalescent plasma, serum or
hyperimmune immunoglobulin on the duration of hospital admission? 3. What is the effect of treating SARI cases of viral aetiology with convalescent plasma, serum or
hyperimmune immunoglobulin on the requirement for and duration of critical care support (e.g. rate of admission and length of stay in intensive care units [ICU] or high dependency units [HDU], rate of intubation, rate and duration of mechanical ventilation, rate and duration of ECMO and other rescue therapies for respiratory failure)?
4. What is the effect of treating SARI cases of viral aetiology with convalescent plasma, serum or hyperimmune immunoglobulin on the rate and severity of non-respiratory organ system involvement or sepsis (including severe sepsis and septic shock)?
5. What is the effect of treating SARI cases of viral aetiology with convalescent plasma, serum or hyperimmune immunoglobulin on the rate of hospital readmission or recurrence of severe disease?
6. What is the effect of treating SARI cases of viral aetiology with convalescent plasma, serum or hyperimmune immunoglobulin on viral antibody levels?
7. What is the effect of treating SARI cases of viral aetiology using convalescent plasma, serum or hyperimmune immunoglobulin on viral load and clearance in respiratory, faecal and blood samples?
8. What serious adverse events and intervention-related safety issues (e.g. anaphylaxis, transfusion-related effects, or secondary bacterial infections) have been associated with convalescent plasma, serum and hyperimmune immunoglobulin used therapeutically in SARI cases of viral aetiology?
The Population, Intervention, Comparators, and Outcomes (PICO) framework to inform the review objectives are as follows: Population: Human subjects of any age or either sex who have been hospitalised due to a severe
acute respiratory infection of viral aetiology. This study will adopt the epidemiological case definition of SARI in accordance with surveillance guidance published by WHO/Europe (23). Subjects presenting with the following clinical conditions will be included: Middle East respiratory syndrome, severe acute respiratory syndrome, pulmonary parenchymal disease, viral pneumonitis, viral pneumonia, acute lung injury, and acute respiratory distress syndrome (11)
Intervention: The use of convalescent plasma, convalescent serum and hyperimmune immunoglobulin derived from convalescent plasma
Comparators: Placebo, sham treatment, or no intervention where a comparator group has been studied. Case series or other studies with no comparator will also be included
Outcomes: Mortality at 30 days and by study end following onset of respiratory symptoms; length of stay in hospital; rate of admission to ICU/HDU; length of stay in ICU/HDU; rate of intubation; rate and duration of non-invasive and invasive mechanical ventilation; rate and duration of ECMO and other rescue therapies for respiratory failure; rate and severity of non-respiratory organ system involvement, sepsis, severe sepsis and septic shock; rate of hospital and ICU/HDU readmission, rate of severe disease recurrence; laboratory confirmed viral load and clearance in respiratory, faecal and blood specimens; laboratory confirmed viral antibody levels

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 6
of IgM and IgG pre and post treatment, seroconversion and seropositivity rates post treatment; serious adverse events and intervention-related adverse reactions, as defined by the International Conference on Harmonisation Guideline for Good Clinical Practice (24)
3. Study selection Inclusion criteria
Systematic reviews with or without meta-analysis, experimental studies, observational studies, and other literature sources reporting relevant outcome data on the effectiveness of convalescent plasma, convalescent serum or hyperimmune immunoglobulin for the treatment of SARI cases with a viral aetiology
Studies which recruited acutely hospitalised subjects of any age or sex whose clinical presentation was consistent with the WHO/Europe SARI case definition, of a viral aetiology. Symptoms or syndromes may include at least one of the following: (23) (11)
o Fever, cough, sore throat or dyspnoea (including shortness of breath or difficulty breathing)
o Middle East respiratory syndrome o Severe acute respiratory syndrome o Pulmonary parenchymal disease o Viral pneumonia o Viral pneumonitis o Acute lung injury o Acute respiratory distress syndrome o Opacities on imaging, pulmonary oedema (non-cardiogenic, not due to fluid
overload) or poor oxygenation
Studies of SARI cases with laboratory-confirmed or probable viral infection due to: o Coronavirus (including MERS-CoV and SARS) o Seasonal, avian or pandemic influenza o Adenovirus o Rhinovirus o Respiratory syncytial virus (RSV) o Parainfluenza virus o Human metapneumovirus o Varicella-zoster virus o Measles
Records reporting data pertaining to at least one of the outcome measures specified in the PICO framework
Records published up to June 2013
Records published in the English language and other languages (where the available resources allow access to multi-lingual translators or reviewers)
Exclusion criteria
Records reporting prophylactic interventions
Records where the intervention was a monoclonal antibody (licensed or experimental)
Records where convalescent plasma was used for treatment of infections other than viral infections of the respiratory system
Studies conducted in animals

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 7
Any systematic review with or without meta-analysis that has been superseded by an updated evidence synthesis
Two reviewers will conduct the literature search (see Appendix 1 – literature search strategy), these results will then be pooled and duplicates removed. Identified literature will be screened by two reviewers, applying the eligibility criteria using a three stage sifting approach to review literature title, abstract, and the full text. The number of papers screened out will be recorded at each stage. A PRISMA diagram will be produced and reasons for exclusion will be recorded when sifting at the full text stage. Any disagreement between the two reviewers will resolved by consensus, this may involve a third reviewer when required.
4. Assessment of risk of bias and data extraction The risk of bias in the study and outcome level of selected records will be assessed using the following tools:
Cochrane Collaboration tool (25) for assessing risk of bias in experimental and prospective cohort studies
Newcastle Ottawa scale (26) for other observational studies (excluding prospective cohort studies). This will be used to assess levels of confounding along with bias. The Cochrane Collaboration recommends the assessment of confounding due to the potential risk of selection bias in these studies, and importance in contributing towards heterogeneity between studies
United States Agency for Healthcare Research and Quality domain and element-based evaluation instrument (27) for Systematic reviews that meet the eligibility criteria
Outcome reporting bias will be assessed within each study using the above quality assessment tools. The result of each assessment will be presented per domain or per question, in line with recommendations of the Cochrane Collaboration and the PRISMA statement. Abstracts that are assessed to meet the study eligibility criteria for inclusion will be subject to data extraction only and not assessment for risk of bias. Reviewers will be required to identify the confounding factors stated in each study, describe the methodology used to measure them, and state how selection bias was controlled through any study design specific features and methods of statistical analysis. In compliance with the Cochrane collaboration, potential confounding factors anticipated to be of importance in the review are:
Demography of the study population
Differences in severity and presentation
Settings from which study population has been sampled
The range of interventions being given to a patient at the same time as the intervention of interest
Viral infection type (including virus co-infection)
Underlying medical history or comorbidities
Methodology used to assess study outcome measures
Duration of the follow up
Data extracted from records will be collected according to the PICO framework and in a predefined form which will be piloted until the final version is agreed (see Appendix 2 – data extraction form).

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 8
Data extraction and quality assessments will be conducted by reviewers that will be trained in the study protocol prior to undertaking any study related procedures. Any disagreements between reviewers will be recorded and resolved after discussion with a third reviewer.
5. Data synthesis Study characteristics and outcome measures will be tabulated to aid narrative synthesis. Statistical analyses will be performed where feasible to produce a random-effects meta-analysis of pooled estimates of effect size (including 95% confidence intervals). Heterogeneity will be assessed using I2 statistics. Primary narrative synthesis and meta-analysis results will be presented by virus aetiology. Sensitivity analyses are planned to explore the robustness of these estimates through studying the effect of treatment by age group (particularly adults vs. children), intervention characteristics, risk of bias and underlying meta-analysis model. Publication bias will be assessed for each outcome measure studied using funnel plots of effect size versus sample size for each included study (where sufficient data is available). Statistical tests for funnel plot asymmetry such as those proposed by Egger or Harbord may be conducted. A narrative approach will be used to synthesise quality assessments and extract data according to the following framework described by the Economic and social research council and recommended by the University of York Centre for Review and Dissemination (28).
Develop a theory of how the intervention works, why and for whom.
Develop a preliminary synthesis of findings of included records.
Exploring relationships within and between records.
Assessing the robustness of the synthesis.
6. Dissemination A report will be produced and submitted to WHO Pandemic and Epidemic Diseases Department (PED). The report will aim to be developed into a publication in a peer-reviewed journal. Presentation of the final version of this manuscript at appropriate conferences and meetings will also be considered.
7. Resource implications An Agreement for Performance of Work (APW) will be drawn up between WHO and the University of Nottingham. This agreement will incorporate a budget accounting for any resources deemed necessary for the completion of the project.
8. Acknowledgments We acknowledge and thank the following people for their contribution to the development of the protocol: Dr Kenneth Baillie (University of Edinburgh); Dr Paul Cleary, Dr Sophia Makki, Dr Fu-Meng Khaw (Public Health England); Dr Wei Shen Lim (Nottingham University Hospitals NHS Trust); Prof Kevin Rooney (University of West Scotland); Dr Nahoko Shindo (World Health Organization).

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 9
9. References
1 World Health Organization. WHO Coronavirus infections updates. WHO. http://www.who.int/csr/don/archive/disease/coronavirus_infections/en/index.html (accessed 5 Jul2013).
2 Breban R, Riou J, Fontanet A. Interhuman transmissibility of Middle East respiratory syndrome coronavirus: estimation of pandemic risk. The Lancet 2013;Early Online Publication. doi:10.1016/S0140-6736(13)61492-0
3 Joseph C, Malik MR, Mounts AW, et al. Highlights and conclusions from the technical consultative meeting on novel coronavirus infection, Cairo, Egypt, 14–16 January 2013. Eastern Mediterranean Health Journal 2013;19:1.
4 Drosten C, Seilmaier M, Corman VM, et al. Clinical features and virological analysis of a case of Middle East respiratory syndrome coronavirus infection. The Lancet Infectious Diseases 2013;Early Online Publication. doi:10.1016/S1473-3099(13)70154-3
5 Assiri A, McGeer A, Perl TM, et al. Hospital Outbreak of Middle East Respiratory Syndrome Coronavirus. New England Journal of Medicine 2013;Online Publication. doi:10.1056/NEJMoa1306742
6 Guery B, Poissy J, el Mansouf L, et al. Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome coronavirus: a report of nosocomial transmission. The Lancet 2013;381:2265–72.
7 ECDC. MERS-CoV novel coronavirus risk assessment. European Centre for Disease Prevention and Control 2013. http://www.ecdc.europa.eu/en/publications/Publications/MERS-CoV-novel-coronavirus-risk-assessment.pdf (accessed 24 Jun2013).
8 Memish ZA, Zumla AI, Al-Hakeem RF, et al. Family Cluster of Middle East Respiratory Syndrome Coronavirus Infections. New England Journal of Medicine 2013;368:2487–94.
9 Shafi S, Booy R, Haworth E, et al. Hajj: Health lessons for mass gatherings. Journal of Infection and Public Health 2008;1:27–32.
10 Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003. World Health Organization. http://www.who.int/csr/sars/country/table2004_04_21/en/ (accessed 19 Jun2013).
11 Clinical management of severe acute respiratory infections when novel coronavirus is suspected: What to do and what not to do. World Health Organization 2013. http://www.who.int/csr/disease/coronavirus_infections/InterimGuidance_ClinicalManagement_NovelCoronavirus_11Feb13u.pdf (accessed 5 Jul2013).
12 Treatment of MERS-CoV: Decision Support Tool. V1.0. London: : Public Health England 2013. http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1317139281416 (accessed 5 Jul2013).
13 Hung IF, To KK, Lee C-K, et al. Convalescent plasma treatment reduced mortality in patients with severe pandemic influenza A (H1N1) 2009 virus infection. Clin Infect Dis 2011;52:447–56.
14 Luke TC, Kilbane EM, Jackson JL, et al. Meta-analysis: convalescent blood products for Spanish influenza pneumonia: a future H5N1 treatment? Ann Intern Med 2006;145:599–609.
Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 10
15 Cheng Y, Wong R, Soo YOY, et al. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur J Clin Microbiol Infect Dis 2005;24:44–6.
16 Kong LK, Zhou BP. Successful treatment of avian influenza with convalescent plasma. Hong Kong Med J 2006;12:489.
17 Hung IFN, To KKW, Lee C-K, et al. Hyperimmune Intravenous Immunoglobulin Treatment: A Multicentre Double-Blind Randomized Controlled Trial for Patients with Severe A(H1N1)pdm09 Infection. Chest Published Online First: 28 February 2013. doi:10.1378/chest.12-2907
18 Lai ST. Treatment of severe acute respiratory syndrome. Eur J Clin Microbiol Infect Dis 2005;24:583–91.
19 Stockman LJ, Bellamy R, Garner P. SARS: systematic review of treatment effects. PLoS Med 2006;3:e343.
20 Yeh K-M, Chiueh T-S, Siu LK, et al. Experience of using convalescent plasma for severe acute respiratory syndrome among healthcare workers in a Taiwan hospital. J Antimicrob Chemother 2005;56:919–22.
21 Wong SSY, Yuen K-Y. The management of coronavirus infections with particular reference to SARS. J Antimicrob Chemother 2008;62:437–41.
22 Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009;339:b2700–b2700.
23 Caroline Brown, Pernille Jorgensen, Joshua A. Mott, et al. WHO Regional Office for Europe guidance for sentinel influenza surveillance in humans. World Health Organization 2011. http://www.euro.who.int/__data/assets/pdf_file/0020/90443/E92738.pdf (accessed 5 Jul2013).
24 International Conference on Harmonisation Working Group. ICH harmonised tripartite guideline: guideline for good clinical practice E6 (R1). In: International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. 1996.
25 Green S, Higgins JP, Alderson P, et al. Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons, Ltd 2008. http://onlinelibrary.wiley.com/doi/10.1002/9780470712184.ch1/summary (accessed 2 Jul2013).
26 P Tugwell W, G. A. The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed 20 Jun2013).
27 Systems to rate the strength of scientific evidence. Evidence report/technology appraisal No. 47. Available [online] from: http://archive.ahrq.gov/clinic/epcsums/strengthsum.pdf. Agency for Healthcare Research and Quality (2002)
28 Centre for Reviews and Dissemination. Systematic Reviews: CRD’s guidance for undertaking reviews in health care. York: University of York 2009.
Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 11
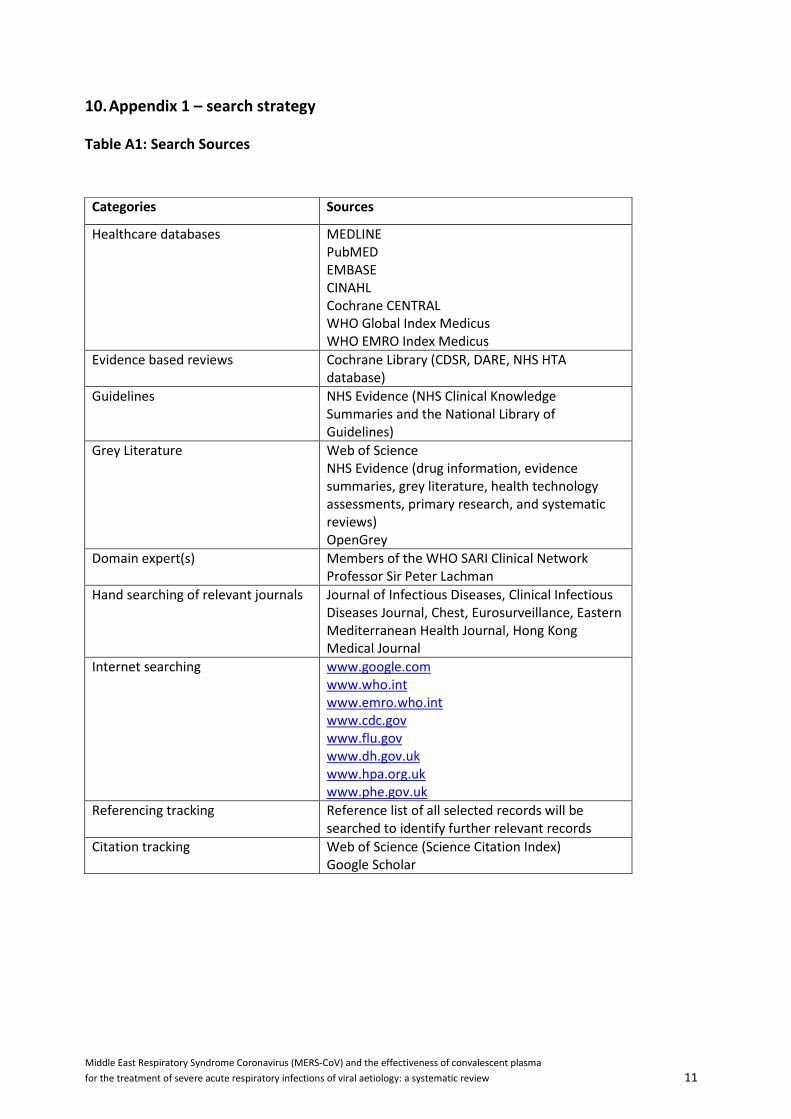
10. Appendix 1 – search strategy
Table A1: Search Sources
Categories Sources
Healthcare databases MEDLINE PubMED EMBASE CINAHL Cochrane CENTRAL WHO Global Index Medicus WHO EMRO Index Medicus
Evidence based reviews Cochrane Library (CDSR, DARE, NHS HTA database)
Guidelines NHS Evidence (NHS Clinical Knowledge Summaries and the National Library of Guidelines)
Grey Literature Web of Science NHS Evidence (drug information, evidence summaries, grey literature, health technology assessments, primary research, and systematic reviews) OpenGrey
Domain expert(s) Members of the WHO SARI Clinical Network Professor Sir Peter Lachman
Hand searching of relevant journals Journal of Infectious Diseases, Clinical Infectious Diseases Journal, Chest, Eurosurveillance, Eastern Mediterranean Health Journal, Hong Kong Medical Journal
Internet searching www.google.com www.who.int www.emro.who.int www.cdc.gov www.flu.gov www.dh.gov.uk www.hpa.org.uk www.phe.gov.uk
Referencing tracking Reference list of all selected records will be searched to identify further relevant records
Citation tracking Web of Science (Science Citation Index) Google Scholar

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 12
Table A2: Search Limits
Limit Category Specified Limit
Languages All languages (English title/abstract)
Publication type None
Date of publication All publications up to date of search
Study design None
Other limits Human data
Search Construct MeSH thesaurus headings and free text terms may be amended to maintain compatibility with databases which do not use MeSH or include non-English language records. Search interfaces with limited functionality (for example those which support single line searches only, small number of search terms etc.) may be initially searched using broad terms followed by longer search strings. Literature searches will be documented (including but not limited to the terms used, sources interrogated and hits identified) such that these may be replicated. The scope of each free text search will include the study title and abstract where available, when the search strategy is executed. Individual MeSH thesaurus headings and free text terms will be searched for within each group of the PICO statement. However, no terms have been described for the comparator element of the search, as records with no comparator will also be included. Search terms across the PIO groups will be combined along with terms for the viral infections of interest. Search results will be extracted to produce the final list of search hits from each database. All search hits will be imported into reference management software to collate the identified literature and remove duplicates entries prior to conducting the three-stage sifting process. Where search interfaces do not allow the export of search hits to reference management software, search hits may be sifted using alternative electronic or paper-based methods.

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 13
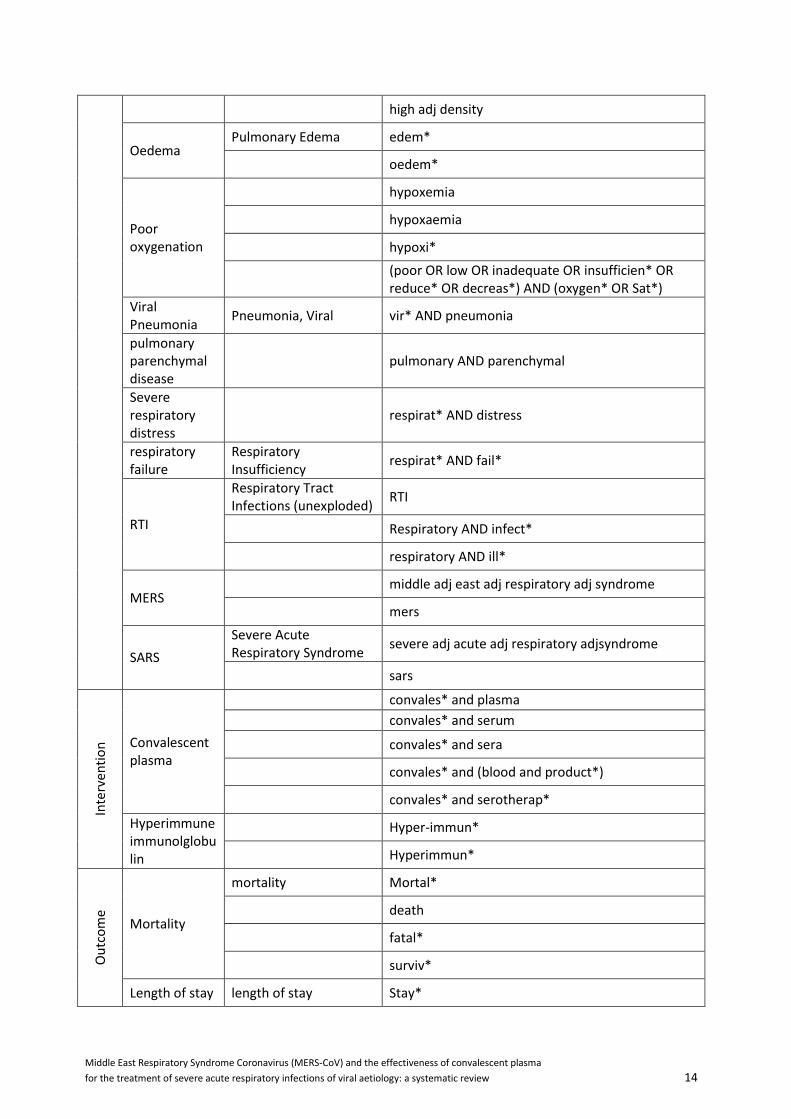
Table A3 – Search terms
PIO Concept MeSH Text
Po
pu
lati
on
Severe Acute respiratory Infection
Severe and Acute and respiratory and Infection*
SARI
Fever Fever Fever*
Pyrexia*
Short of breath
Dyspnea SOB
Dyspnoea OR Dyspnea
Short* AND Breath*
Difficult* AND breath*
Cough Cough Cough
Tussis
Sore throat
Pharyngitis Sore AND throat
Pain AND Throat
Inflam* AND throat
Infect* AND throat
Irritat* AND throat
pharyngiti*
Hospital admission
Hospitalization Hospital OR Health*
inpatient* OR in-patient*
hospitali*
admission* OR admit*
Acute Respiratory distress Syndrome
Respiratory Distress Syndrome, Adult
Acute adj respiratory adj distress adj syndrome*
ARDS
double adj pneumonia
ALI
Acute adj lung adj injury
Imaging
Radiography, Thoracic opacit*
Tomography, X-Ray Computed
consolidat*
Magnetic Resonance Imaging
shadow*
infiltrat*
ground adj glass
Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 14
high adj density
Oedema Pulmonary Edema edem*
oedem*
Poor oxygenation
hypoxemia
hypoxaemia
hypoxi*
(poor OR low OR inadequate OR insufficien* OR reduce* OR decreas*) AND (oxygen* OR Sat*)
Viral Pneumonia
Pneumonia, Viral vir* AND pneumonia
pulmonary parenchymal disease
pulmonary AND parenchymal
Severe respiratory distress
respirat* AND distress
respiratory failure
Respiratory Insufficiency
respirat* AND fail*
RTI
Respiratory Tract Infections (unexploded)
RTI
Respiratory AND infect*
respiratory AND ill*
MERS middle adj east adj respiratory adj syndrome
mers
SARS
Severe Acute Respiratory Syndrome
severe adj acute adj respiratory adjsyndrome
sars
Inte
rven
tio
n Convalescent
plasma
convales* and plasma
convales* and serum
convales* and sera
convales* and (blood and product*)
convales* and serotherap*
Hyperimmune immunolglobulin
Hyper-immun*
Hyperimmun*
Ou
tco
me
Mortality
mortality Mortal*
death
fatal*
surviv*
Length of stay length of stay Stay*

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 15
LOS
Patient Discharge discharge*
Readmission/reccurence
Patient Readmission readmi* or re-admi*
Recurrence recur* or relaps*
Interventions
Respiratory Therapy extracorporeal adj membrane adj oxygenation
ecmo
pumpless adj adj extracorporeal adj lung adj assist
PECLA
Novalung
Nitric adj oxide
respirat*
ventilat*
cpap or bipap or bi-pap
positive adj airway adj pressure
Tracheostomy trache*
Intubation intubat*
Healthcare utilisation
Intensive Care (critic*) AND (care OR treat*)
Intensive Care units (intens*) AND (care OR treat*)
high adj dependency
step adj down
ITU OR ICU OR CCU OR HDU
ward* or unit* or department* or centre*
Patient antibodies
Antibodies, Viral antibod*
immunoglobulin*
IGG
IGM
sero*
Viral load Viral Load vir* AND (load OR Concentrat* OR titre OR titer)
Viral shedding
Virus Shedding vir* AND shed*
resp* AND shed*
(stool* OR faec* or fec*) AND shed*
Secondary organ involvement
Renal Insufficiency kidney*
liver failure renal*

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 16
Heart Diseases nephro*
Multiple Organ Failure liver*
hepat*
heart*
cardi*
organ and (fail* or collaps* or damag* or injur*)
multi-organ and (fail* or collaps* or damag* or injur*)
Systemic Inflammatory Response Syndrome
sepsis or septic
SAE
Patient Safety SAE
Blood Safety (side adj effect*) or side-effect
harm*
danger*
adverse or untoword
safe* OR unsafe
life-threat* OR life adj threat*
disab* or incapacit*
(congenital adj anomaly) or (birth adj defect)
anaphylaxis
transfus*
infect* AND bacteria*
Vir
use
s
Coronavirus
coronavirus (unexploded)
corona*
coronavirus 229e cov
sars virus mers-cov
coronavirus oc43, human
sars-cov
coronavirus nl63, human
Coronavirus Infections
Influenza
influenza, human Influenza*
Influenzavirus A Flu
Influenzavirus B
Rhinovirus rhinovirus Rhinovirus
Rhino adj virus
Adenovirus Adenovirus Infections, Adenovirus

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 17
Human
Adenoviruses, Human Adeno adj virus
Respiratory syncytial virus
Respiratory Syncytial Virus, Human
Respiratory adj syncytial adj virus
Respiratory Syncytial Virus Infections
RSV
Parainfluenza virus
Parainfluenza Virus 1, Human
Parainfluenza
Parainfluenza Virus 2, Human
Parainfluenza Virus 3, Human
Parainfluenza Virus 4, Human
Human metapneumonovirus
Metapneumovirus Metapneumovirus
Meta-pneumovirus
Varicella-zoster virus Herpes Zoster
varicella* or herpes*
Herpesvirus 3, Human zoster*
vzv or hzv
Measles Measles virus measles
Measles
Respiratory virus
Respiratory AND vir*
Pulmonary AND vir*

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 18
Table A4 – Sample Search
Database: Ovid MEDLINE(R) Daily Update <July 10, 2013>, Ovid MEDLINE(R) In-Process & Other
Non-Indexed Citations and Ovid MEDLINE(R) <1946 to Present>
Search Strategy:
--------------------------------------------------------------------------------
1 (Severe and Acute and respiratory and Infection*).ti,ab. (4536)
2 SARI.ti,ab. (227)
3 exp Fever/ (34167)
4 Fever*.ti,ab. (122431)
5 Pyrexia*.ti,ab. (3392)
6 exp Dyspnea/ (15316)
7 SOB.ti,ab. (279)
8 (Dyspnoea or Dyspnea).ti,ab. (30892)
9 (Short* and Breath*).ti,ab. (10976)
10 (Difficult* and breath*).ti,ab. (4314)
11 exp Cough/ (12054)
12 Cough.ti,ab. (29820)
13 Tussis.ti,ab. (8)
14 exp Pharyngitis/ (13111)
15 (Sore and throat).ti,ab. (3366)
16 (Pain and Throat).ti,ab. (1296)
17 (Inflam* and throat).ti,ab. (727)
18 (Infect* and throat).ti,ab. (4320)
19 (Irritat* and throat).ti,ab. (489)
20 pharyngiti*.ti,ab. (4244)
21 exp Hospitalization/ (155645)
22 (Hospital or Health*).ti,ab. (2114630)
23 (inpatient* or in-patient*).ti,ab. (1165789)
24 hospitali*.ti,ab. (148367)
25 (admission* or admit*).ti,ab. (234990)
26 exp Respiratory Distress Syndrome, Adult/ (14830)
27 (Acute adj respiratory adj distress adj syndrome*).ti,ab. (7201)
28 ARDS.ti,ab. (7374)
29 (double adj pneumonia).ti,ab. (3)
30 ALI.ti,ab. (3675)
31 (Acute adj lung adj injury).ti,ab. (9188)
32 opacit*.ti,ab. (13524)
33 consolidat*.ti,ab. (26720)
34 consolidat*.ti,ab. (26720)

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 19
35 shadow*.ti,ab. (13295)
36 infiltrat*.ti,ab. (151624)
37 (ground adj glass).ti,ab. (3217)
38 (high adj density).ti,ab. (60558)
39 exp Pulmonary Edema/ (15033)
40 edem*.ti,ab. (81912)
41 oedem*.ti,ab. (22307)
42 exp Radiography, Thoracic/ (32569)
43 exp Tomography, X-Ray Computed/ (293871)
44 exp Magnetic Resonance Imaging/ (307997)
45 hypoxemia.ti,ab. (11566)
46 hypoxaemia.ti,ab. (2963)
47 hypoxi*.ti,ab. (92822)
48 ((poor or low or inadequate or insufficien* or reduce* or decreas*) and (oxygen* or Sat*)).ti,ab.
(282860)
49 exp Pneumonia, Viral/ (4580)
50 (vir* and pneumo*).ti,ab. (19322)
51 (pulmonary and parenchymal).ti,ab. (3588)
52 (respirat* and distress).ti,ab. (28427)
53 exp Respiratory Insufficiency/ (50820)
54 (respirat* and fail*).ti,ab. (38128)
55 Respiratory Tract Infections/ (31178)
56 RTI.ti,ab. (1348)
57 (Respiratory and infect*).ti,ab. (69600)
58 (respiratory and ill*).ti,ab. (20169)
59 (middle adj east adj respiratory adj syndrome).ti,ab. (8)
60 mers.ti,ab. (1595)
61 exp Severe Acute Respiratory Syndrome/ (4403)
62 (severe adj acute adj respiratory adjsyndrome).ti,ab. (0)
63 sars.ti,ab. (6905)
64 (convales* and plasma).ti,ab. (591)
65 (convales* and serum).ti,ab. (2482)
66 (convales* and sera).ti,ab. (2055)
67 (convales* and (blood and product*)).ti,ab. (171)
68 (convales* and serotherap*).ti,ab. (3)
69 Hyper-immun*.ti,ab. (323)
70 Hyperimmun*.ti,ab. (5429)
71 exp mortality/ (279378)
72 Mortal*.ti,ab. (458666)
73 death.ti,ab. (463792)

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 20
74 fatal*.ti,ab. (103119)
75 surviv*.ti,ab. (730864)
76 exp length of stay/ (56598)
77 Stay*.ti,ab. (111444)
78 LOS.ti,ab. (16495)
79 exp Patient Discharge/ (18502)
80 discharge*.ti,ab. (160659)
81 exp Patient Readmission/ (7583)
82 (readmi* or re-admi*).ti,ab. (14840)
83 exp Recurrence/ (158952)
84 (recur* or relaps*).ti,ab. (489593)
85 exp Respiratory Therapy/ (87634)
86 (extracorporeal adj membrane adj oxygenation).ti,ab. (4379)
87 ecmo.ti,ab. (3091)
88 (pumpless adj extracorporeal adj lung adj assist).ti,ab. (45)
89 PECLA.ti,ab. (22)
90 Novalung.ti,ab. (53)
91 (Nitric adj oxide).ti,ab. (113823)
92 respirat*.ti,ab. (347771)
93 ventilat*.ti,ab. (120013)
94 (cpap or bipap or bi-pap).ti,ab. (5487)
95 (positive adj airway adj pressure).ti,ab. (6765)
96 exp Tracheostomy/ (5106)
97 trache*.ti,ab. (72648)
98 exp Intubation/ (43379)
99 intubat*.ti,ab. (38986)
100 exp Intensive Care/ (19127)
101 (critic* and (care or treat*)).ti,ab. (146392)
102 exp Intensive Care units/ (54697)
103 (intens* and (care or treat*)).ti,ab. (206688)
104 (high adj dependency).ti,ab. (768)
105 (step adj down).ti,ab. (2324)
106 (ITU or ICU or CCU or HDU).ti,ab. (29779)
107 (ward* or unit* or department* or centre*).ti,ab. (943083)
108 exp Antibodies, Viral/ (90952)
109 antibod*.ti,ab. (709919)
110 immunoglobulin*.ti,ab. (126466)
111 IGG.ti,ab. (112696)
112 IGM.ti,ab. (55850)
113 exp Viral Load/ (22904)

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 21
114 (vir* and (load or Concentrat* or titre or titer)).ti,ab. (89882)
115 exp Virus Shedding/ (2291)
116 (vir* and shed*).ti,ab. (8125)
117 (resp* and shed*).ti,ab. (16012)
118 ((stool* or faec* or fec*) and shed*).ti,ab. (3398)
119 kidney*.ti,ab. (326122)
120 renal*.ti,ab. (446551)
121 nephro*.ti,ab. (119135)
122 liver*.ti,ab. (611359)
123 hepat*.ti,ab. (521578)
124 heart*.ti,ab. (621580)
125 cardi*.ti,ab. (823864)
126 exp Renal Insufficiency/ (121863)
127 exp liver failure/ (17896)
128 exp Heart Diseases/ (879970)
129 exp Multiple Organ Failure/ (8522)
130 (organ and (fail* or collaps* or damag* or injur*)).ti,ab. (49903)
131 (multi-organ and (fail* or collaps* or damag* or injur*)).ti,ab. (1955)
132 exp Systemic Inflammatory Response Syndrome/ (95181)
133 (sepsis or septic).ti,ab. (88084)
134 exp patient safety/ (3098)
135 SAE.ti,ab. (852)
136 exp blood safety/ (241)
137 ((side adj effect*) or side-effect).ti,ab. (176139)
138 harm*.ti,ab. (97236)
139 danger*.ti,ab. (44698)
140 (adverse or untoward).ti,ab. (286966)
141 (safe* or unsafe).ti,ab. (499239)
142 ((life-threat* or life) adj threat*).ti,ab. (52393)
143 (disab* or incapacit*).ti,ab. (137725)
144 ((congenital adj anomaly) or (birth adj defect)).ti,ab. (5346)
145 anaphylaxis.ti,ab. (10878)
146 transfus*.ti,ab. (81439)
147 sero*.ti,ab. (327022)
148 (infect* and bacteria*).ti,ab. (134139)
149 coronavirus/ (1216)
150 corona*.ti,ab. (328699)
151 exp coronavirus 229e/ (202)
152 cov.ti,ab. (2790)
153 exp sars virus/ (2945)

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 22
154 mers-cov.ti,ab. (9)
155 exp coronavirus oc43, human/ (122)
156 sars-cov.ti,ab. (2082)
157 exp coronavirus nl63, human/ (35)
158 exp Coronavirus Infections/ (7016)
159 exp influenza, human/ (36278)
160 Influenza*.ti,ab. (86080)
161 exp Influenzavirus A/ (33346)
162 Flu.ti,ab. (8777)
163 exp Influenzavirus B/ (3127)
164 exp rhinovirus/ (3013)
165 Rhinovirus.ti,ab. (3176)
166 (Rhino adj virus).ti,ab. (8)
167 exp Adenovirus Infections, Human/ (2060)
168 Adenovirus.ti,ab. (35679)
169 exp Adenoviruses, Human/ (6863)
170 (Adeno adj virus).ti,ab. (54)
171 exp Respiratory Syncytial Virus, Human/ (1557)
172 exp Respiratory Syncytial Virus Infections/ (4854)
173 (Respiratory adj syncytial adj virus).ti,ab. (9496)
174 RSV.ti,ab. (8230)
175 exp Parainfluenza Virus 1, Human/ (2807)
176 Parainfluenza.ti,ab. (4190)
177 exp Parainfluenza Virus 2, Human/ (270)
178 exp Parainfluenza Virus 3, Human/ (1047)
179 exp Parainfluenza Virus 4, Human/ (33)
180 exp Metapneumovirus/ (997)
181 Metapneumovirus.ti,ab. (1298)
182 Meta-pneumovirus.ti,ab. (2)
183 exp Herpes Zoster/ (9583)
184 (varicella* or herpes*).ti,ab. (76077)
185 exp Herpesvirus 3, Human/ (5465)
186 zoster*.ti,ab. (13974)
187 (vzv or hzv).ti,ab. (3885)
188 exp measles virus/ (5959)
189 exp measles/ (13195)
190 measles.ti,ab. (19015)
191 (Respiratory and vir*).ti,ab. (35615)
192 (Pulmonary and vir*).ti,ab. (12217)

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 23
193 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19
or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36
or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53
or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 (4481427) –Population terms
194 64 or 65 or 66 or 67 or 68 or 69 or 70 (9794) – Intervention terms
195 71 or 72 or 73 or 74 or 75 or 76 or 77 or 78 or 79 or 80 or 81 or 82 or 83 or 84 or 85 or 86 or 87
or 88 or 89 or 90 or 91 or 92 or 93 or 94 or 95 or 96 or 97 or 98 or 99 or 100 or 101 or 102 or 103
or 104 or 105 or 106 or 107 or 108 or 109 or 110 or 111 or 112 or 113 or 114 or 115 or 116 or
117 or 118 or 119 or 120 or 121 or 122 or 123 or 124 or 125 or 126 or 127 or 128 or 129 or 130
or 131 or 132 or 133 or 134 or 135 or 136 or 137 or 138 or 139 or 140 or 141 or 142 or 143 or
144 or 145 or 146 or 147 or 148 (7421879) – Outcome terms
196 149 or 150 or 151 or 152 or 153 or 154 or 155 or 156 or 157 or 158 or 159 or 160 or 161 or 162
or 163 or 164 or 165 or 166 or 167 or 168 or 169 or 170 or 171 or 172 or 173 or 174 or 175 or
176 or 177 or 178 or 179 or 180 or 181 or 182 or 183 or 184 or 185 or 186 or 187 or 188 or 189
or 190 or 191 or 192 (600446) – Virus terms
197 193 and 194 and 195 and 196 (732)
198 limit 197 to humans (574)

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 24
11. Appendix 2 – data extraction form
A pre-piloted electronic form will be used to record the outcomes of risk of bias assessments and for data extraction for each study meeting inclusion criteria. The data items to be extracted are listed below. For each study there may be multiple population groups, treatments and outcomes.
Study eligibility
Reviewer
Study ID (supplied by JMJ/MSC)
Citation
Eligible for review
Comments - if study is not eligible, state reason(s) why
Study Characteristics
Reviewer
Study ID
Author
Year of publication
Type of publication (journal article etc..)
Country(ies) where conducted
Study objectives (Primary, secondary and further objectives)
Study design
Total study sample size
Power calcuation performed?
Methods of recruitment / selection
Inclusion criteria used in study
Exclusion criteria used in study
Sequence Generation (random or not random)
Allocation (blinded or not blinded)
Selection bias and confounding variables
Type and source of funding / sponsorship
Respiratory virus(es) considered
Comments Population
Reviewer
Study ID
Description of study group
Citation of original data source (for referenced data)
Sample size of group
Setting
Average age and measure of spread

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 25
Sex (male or female)
Diagnosis method within each group (clinical case definition or laboratory confirmed)
Clinical / treatment / socioeconomic characteristic (1)
Clinical / treatment / socioeconomic characteristic (2)
Clinical / treatment / socioeconomic characteristic (2)
Comments Treatment
Reviewer
Study ID
Intervention description
Route of administration
Patient status at time of intervention
Criteria for intervention
Timing of intervention (inc. measure of spread)
Dose
Dosing schedule
Number allocated to treatment
Number received treatment
Serious adverse events or treatment effects
Comments Outcomes
Reviewer
Study ID
Definition
Measurement tool (if used)
Timing of measurement
Unit of measurement
Blinding
Duration of follow-up
Method of analysis
ITT / PP
Number included
Withdrawals - intervention
Withdrawals - comparator
Exclusions - intervention
Exclusions - comparator
Loss to FU - intervention
Loss to FU - comparator
Data for future meta-analysis: Result - intervention (+ive)
Data for future meta-analysis: Result - intervention (-ive)
Data for future meta-analysis: Result - comparator (+ive)
Data for future meta-analysis: Result - comparator (-ive)
Data for future meta-analysis: Result - statistical output

Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and the effectiveness of convalescent plasma
for the treatment of severe acute respiratory infections of viral aetiology: a systematic review 26
Data for future meta-analysis: Control for selection bias and confounding
Data for narrative analysis: Result - intervention
Data for narrative analysis: Result – comparator
Comments